Drugs & Behavior Exam 3
1/110
Earn XP
Description and Tags
incomplete done through 3/29/24
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
111 Terms
Alcohol History
fermentation dev with society
ethanol → fruit is ripe but not rotten → greater use
~1000 BCE China, remedy for diseases
Usquebaugh
Gaelic “water of life”, whiskey derived from, major ingredient of tonics & elixirs
Wood Alcohol
Methyl, synthetic, antifreeze, fuel
Grain Alcohol
Ethyl, fermentation product, drinkable
Rubbing Alcohol
isopropyl, wound disinfection
How to Make Alcohol
Fermentation
organic high sugar material + yeast
1 molecule sugar → 2 molecules alcohol, 2 molecules CO2
Distillation
heat fermentation product to vapor then cool, concentrate
Change in Average American Drinking
1800s: 4-5 standard drinks a day
Now: 3-4 standard drinks a day
US Alcohol Use
48.7% 12+ yrs old used in past month
79.7% M and 77.3% F lifetime use
Standard Drink
12 oz beer ~ 8-9 oz malt liquor ~ 5 oz wine ~ 1.5 oz spirits
~30mg/dL alcohol
Alcohol %’s of Common Beverages
Wine - 7-15%
Beer - 4-6%
Liquor - 40-95%
Alcohol Broad Scope
$200 bil/yr, 100,000 deaths/yr, 15.1 mil (1:20) Alcohol Use Disorder, hard to get treatment for, stigma
Alcohol Absorption Types
need LARGE amounts (~14 g standard drink)
Oral most often, other kinds banned in most states
AWOL (inhale, vaportini, alc wo liquid)
Palcohol (powdered)
Alcohol Absorption Molecular Basis
simple small molecule, soluble in water and lipids, neutral
rapidly absorbed (small intestine faster than stomach) into body water (~90% to brain)
food slows down ethanol absorption → lower BAL
Blood Alcohol Level/Concentration (BAL/BAC)
concentration of alcohol in blood
80mg/dL = 0.08g/100mL = 0.08% = 17mM
Metabolic Process of Alcohol
alcohol dehydrogenase (redox) : ethanol → acetaldehyde +water
Aldehyde dehydrogenase : acetaldehyde → acetate, NADH out
alcohol levels below 0.1g/dL (22mM)
Else- Microsomal Ethanol Oxidizing system : ethanol → acetaldehyde
NADPH → NADP+, cytochrome P450
byproducts: toxins, free radicals, H2O2
Acetate → water & CO2 or acetyl-CoA
Disulfiram
antabuse, blocks aldehyde dehydrogenase, increases hangover effects from acetaldehyde
negative reinforcement, people avoid taking (attrition)
Alcohol & the Liver
fatty acid buildup leads to cell death, alcoholic hepatitis → cirrhosis → liver failure
SOME alcohol breakdown in the stomach (more for males)
Alcohol Excretion
unchanged through lungs (~2-8%, breathalyzers)
90-95% slowly oxidized through the kidneys
increased urination, suppresses antidiuretic hormone
Alcohol Pharmodynamics
Nonspecific: disturbs P-membrane, polar phospholipid head, alters lipid comp
Specific: acts as NT at binding site, mods channel gating mech, channel P change, stim Gs-adenylyl cyclase
dirty drug. many assorted effects. GABA- DA, opioid peptides, glutamate input
Alcohol Mechanism of Action
increases GABA(A), up inhibition, decreases glutamate, alters function of many proteins at once
acts on ligand-gated ion channels (nicotinic actylcholine, 5-HT3), metabotropic (da and opioid), and voltage gated ion channels (Ca2+, Na+)
Alcohol Behavioral effects
BAC (g/dL): 0.05-0.1 (11-22mM) : subjective high “buzz”, anxiolysis, sedation
0.1-0.2 g/dL (22-44mM) : motor impairment, slurred speech, blackout
0.2-0.3 (44-66 mM) : emesis (vomiting), stupor (near unconsciousness)
0.3-0.4 (44-99 mM) : coma
>0.5 (110mM) : respiratory depression, death
takes more alcohol to kill chronic users
Alcohol Peripheral Effects
dilates blood vessels, dec body temp
increases other depressant drug effects
perception change
Alcohol Tolerance & Withdrawal
acute (one sitting), chronic, and metabolic
sleep disruption, ANS (sympathetic NS) activation, tremors, seizures, psychological dependence
~10-15% use at detrimental levels
Alcohol Reinforcing Effects
Positive: slow (PK), pleasure, altered consciousness, peer conformance
Negative: relief of stress, negative emotions, pain, and withdrawal symptoms
damage PFC → compromised decision making, emotional effect, and executive function
Korsakoff Syndrome
brain damage from alcohol, leading cause of dementia, loss of white and gray matter → brain shrinks!!!
greater risk for older people and the frontal lobes
Negative Alcohol Effects
J shaped cardiovascular - helps (10-40% reduced risk) then worsens in higher amts
coronary heart diseases (sat fat & cholesterol), arrhythmias, cardiomyopathy hemorrhagic stroke
hypertension, esophagus reflux or cancer, stomach gastritis, pancreas inflammation and pain
intestine chronic diarrhea, malabsorption
Naltrexone
Revia, opioid antagonist, ant-alcohol treatment, reduces craving
blocks reinforcing effects, reduces relapse, works better with behavioral therapy combo
Acamprosate
may block NMDA receptors, alcohol pharmacotherapy
Behavioral Alcohol Treatment
alcoholics anonymous - 26-50% success rate after 1 yr, abstinence, self recognized helplessness
behavioral therapy - controlled drinking, mod/control amt and frequency ingested
adverse therapy - pair alcohol with unpleasant consequences (psychosocial)
Papaver somniferm
opium plant, frost tolerant annuals, sleep related
found in the middle east/mediterranean sea and cultivated in Asia
Opium Extraction
petals off to egg sized seedpod
lightly score seedpod and collect white sap (opium)
dry the sap → thick & gummy can be smoked or ingested
Opium History of Use
6000 yrs ago Sumerian s and Assyrians
3500 yrs ago Egypt (Therapeutic Papyrus of Thebes)
~150 CE greeks and romans pancea (Galen)
widespread use in Islamic cultures and china
19th cent → western use
Morphine
F.W. Serturner id as active component
10x as potent as opium
hypodermic syringe, 1800s, civil war’s soldier’s disease
Opium Derivatives Potency
opium < morphine(x10) < heroin(x2) < fentanyl
Diacetylmorphine (heroin)
Alder Wright, cough suppressant and pain killer, 1874
Harrison Narcotic Act (1914)
beginning of US drug crime, up prices
addendums of prescribe only with reducing doses, no prescription to addicts, and never prescribing heroin
Prescription Opiates
Poppy (opium, morphine)
Codeine, dilaudid (semi-synth),
oxycodone/oxycontin (semi-synth)
Percodan (aspirin + oxycodone)
Percocet (acetaminophen + oxycodone)
Vicodin (acetaminophen + hydrocodone)
Synthetic Opiates
higher rates of OD deaths
oxycontin (extended release ~12hrs but people crush & snort & die.)
fentanyl (SEVERE pain, actiq, duragesic, sublimaze, high potency, reduces therapeutic window, more sedative)
Opium Absorption
oral - gastronintestinal
injected - intravenous quicker (mainlining)
‘smoked’ (inhaled) - through nasal mucosa & lungs
Opium Distribution/Metabolism/Excretion
morphine - small amt cross BBB
heroin - more lipid soluble, prodrug, converted to morphine in brain
liver metab ~2 hrs, some to normorphine
codeine → morphine
kidneys/urine eliminate, sex/age/diet/genetics/disease states/meds influence
Opioid Neurotransmitters
Naloxone (1960s, sim to morphine)
blocks effects, reverse overdoses
antagonist, narcan
Endorphins (endogenous morphine, 70s)
Pert & Snyder, NT opiates mimic
beta- , enkephalin, dynorphin
Endorphins
brain’s natural pain-relief. released from injury
acupuncture and placebos release
naloxone blocks
Opiates Brain Effects
mimic endorphins (endogenous opioid peptides)
agonist
directly effect activity, uses intrinsic pain-modulating circuitry, additional therapeutic effects
Opioid Systems of Effect
sensory - pain inhibition
modulatory - gastrointestinal, endocrine, autonomic
emotional - rewarding & addicting
cognitive - mods learning and memory
Mu μ Opioid Receptor
endorphin, agonist
analgesia (supraspinal), euphoria, down GIT, miosis, respiratory depression, physical dependence
Delta δ Opioid Receptor
enkephalin, agonist, analgesia (spinal & supraspinal), growth hormone, affective behavior, limbic system
Kappa κ Opioid Receptor
dynorphin, agonist, analgesia (spinal), sedation, miosis
Opioid Receptors Overall
metabotropic (g-protein coupled), agonist, inhibit neurons, activate K+, inhibit Ca2+ & neurotransmitter release
Opioid Pharmacological Effects
euphoria, analgesia, drowsiness, reduced anxiety, ‘heavy’ limbs, respiration depression, cough suppression, miosis (pupillary constriction), nausea, vomiting, impotence, loss of desire, vivid dreams
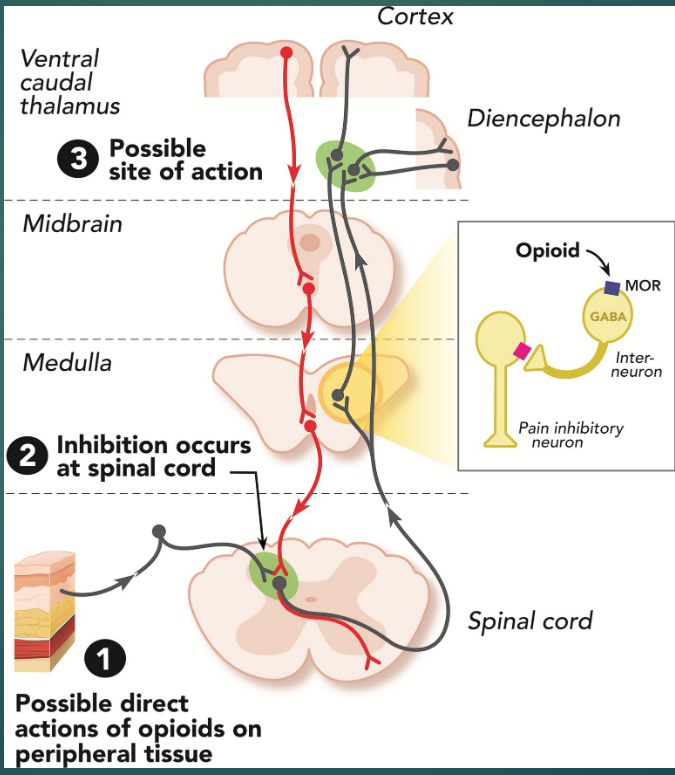
Opiate Pain Signalling
GABA-ergic, pain inhibitory
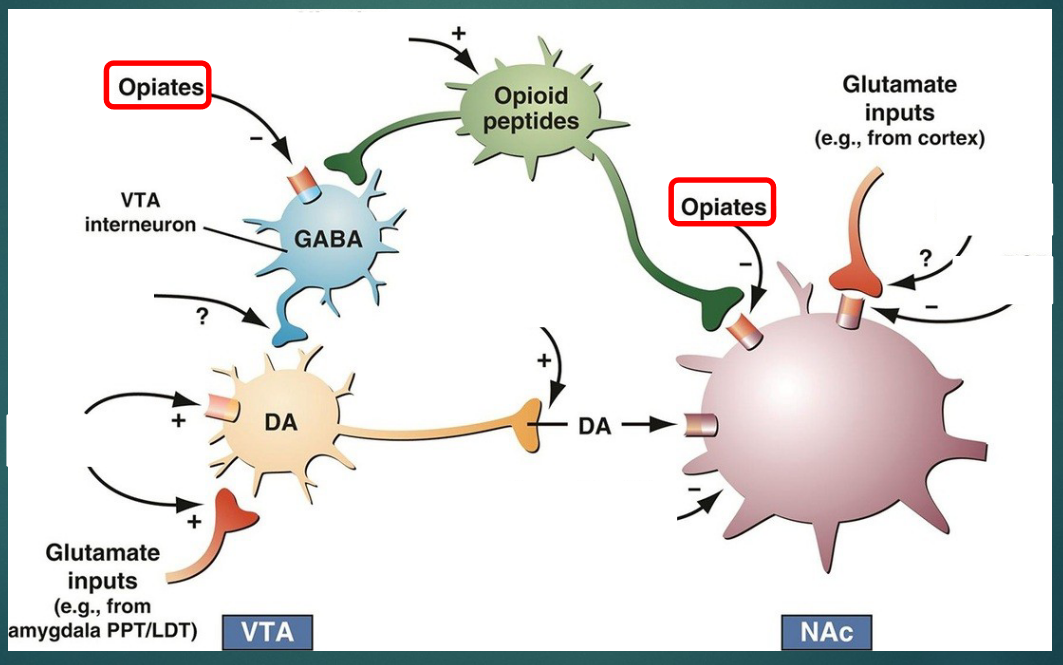
Opiates on Reward System
Opiate Tolerance And WIthdrawal
decreased receptors, increased liver enzymes, conditioned tolerance
depression, crying, high anxiety, irritability, panting, diarrhea, pos → neg reinforcement, flu like symptoms ~6-12hrs after last dose
HIGH relapse, environmental and pavlovian (‘nam vets 21% addiction rate, few relapses at home)
Opiates Medical Use
pain without unconscious (heroin schedule I)
end stage cancer (w low dose Naltrexone)
diarrhea, cough (dextromethorphan)
opioid use disorder
Opioid Lethality
no organ damage
OD deaths. small LD/ED ratio. unstable tolerance
toxic substances combined with, mixing (speedball - heroin & cocaine)
Opioid Replacement Therapy
Methadone - maintain, harm reduction, individualized, up abstinence down crime, HIV, death
Naloxone (narcan) - reverse effects, pops opioid off receptor antagonist, full affinity
Buprenorphine (suboxone) - best of both, partial agonist / antagonist
Cannabis Sativa
“intoxicant”, marijuana leaf, hashish = dust/resin for plant protection
Marijuana Historical Use
stone age pots
Shen Nung for medicinal (sedation, analgesia, psychoactive)
India religious use
ME and North Africa speed up child birth
~1800s Western, medical & mental illness (Moreau)
Marijuana Regulation
Marijuana Tax Act 1937 - criminalization, weed → harmful actions
LaGuardia Committee Report 1944 → multidisciplinary, weed not harmful, no aggression with. mental confusion, delirium, excitation, and anxiety noted
US National Academy of Science → treatment for pain, nausea, and vomiting
Marijuana Use
most widely used elicit drug in the western world
3rd most common (alcohol first nicotine second)
~3-4% worldwide, inverse to perceived risk
Marijuana Absoption
chew leaves or smoke
joint = cig, blunt = emptied out cigar, vapor = vape/pipes/bong
peak ~30 minutes, lasts 2-4 hours
potency, ~20% active ingredient absorbed
Marijuana Distribution & Metabolism & Elimination
highly lipid soluble, into fatty tissues. detectable when blood lvl = 0
liver & organs → less active compounds
feces/urine (half life 1 week), detectable up to 30 days later (single use)
Marijuana Structure
more than 60 compounds
delta-9-tetrahydrocannabinol (THC) = psychoactive component
Marijuana Potency
highest sinsemilla (seedless) - 10-30% THC
lower US - from ~2% → 8-10%
hash oil → ~20%, max ~60%
Marijuana Pharmacodynamics
CB1 (CNS) and CB2 (PNS/immune system)
metabotropic, natural receptors
postsynaptic synthesis, presynaptic receptors (retrograde)
inhibit release of glutamate, GABA, noradrenaline, dopamine, 5-HT
Endocannabinoids
endogenous, Anandamide (bliss) and 2-arachidonoyl-glycerol (2-AG)
Marijuana Effects
acute - differ per user, benign, thirst, down motor & REM, up talking and hunger, nausea/headache
cardiovascular - red eyes (conjuctiva), vasidilation (after 1 hr), dose dependent
Some reactions learned, experienced more sensitive
Learning Effects on Marijuana
Mechanical - inhalation & increased absorption
Perceptual - perceive physical and psychological effects
Labeling - label pleasant effects
Marijuana Behavioral Effects
decreased psychomotor, relaxed/tranquil. keener perception, down sensitivity to pain, varied effect on sexual function (but long term to impotent or disinterest)
Marijuana Cognitive Effects
impaired short term memory (in encoding, consolidation, and information retrieval. greater for teens)
reduced neurotransmission - impaired long term potentiation (inc synapse strength) and long term depression (decrease synapse strength)
lengthened sense of time (decreased)
down critical thinking, judgement, and attention/vigilance
Marijuana Emotional Effects
carefree, relaxed, euphoric, content, excited
~1/3rd → anxiety, dysphoria, suspicion, paranoia
inconclusive links to schizophrenia/psychosis, depression, and anxiety
Marijuana Physiological Effects
up hr and bp (after 20mins last 1hr)
decreased proper lung function (reversible?)
weed cigs have more tar and carcinogens, hold smoke in longer, varied results per symptom of worse
emphysema, no long term cardiovascular effects, some immunosuppressant but nothing long term
reduced sperm count/motility, non-ovulatory menstrual cycles
Marijuana Addictive
activates reward pathway, tolerance in animal
withdrawal - sleep disturb, nausea, restless with heavy use
neuroadaptations. yes addictive.
Amotivational Syndrome
controversial theory that weed → unmotivated and lazy
likely from pre-existing personality characteristics
Marijuana Gateway Drug?
no. stepping stone like: ethanol/nicotine → marijuana → hard drugs.
90% cocaine users done weed not converse
correlative vulnerability - general predisposition to use drugs
Cannabis Medical Uses
schedule I drug (no med use). historically used
reduces vomiting and stimulates appetite, for cancer
cachexia (stim appetite), pain, epilepsy, hypertension, asthma, anxiety, alzheimer’s, depression
glucoma (reduce eye pressure, side effects)
Synthetic Cannabinoids
schedule III (med use allowed)
more specified, only target one receptor type, fewer side effects, more potent, stable, and soluble. slow
marinol (dronabinol), cesamet (nabilone), sativex (oral spray → pain killer sclerosis arthritis)
rimonabant (inverse agonist, obesity, alzheimers)
CBD
cannabidiol
self admin, little reinforcement, psychoactive side effects
Hallucinogens
change mental state by distorting perception of reality
illusionogenic, psychotomimetic, psychedelic, mind expanding
Serotonergic Hallucinogens
LSD (lysergic acid diethylamide), mescaline (peyote cactus), psilocybin, lysergic acid amide (morning glory seeds), DMT (dimethyltryptamine),
change serotonin transmission
Hallucinogens History
religious ceremonies, shrooms before 1000 bce, rituals in Mexico
Switzerland Hoffman, 1938, derivative of fungus ergot, for psychotherapy
60s: western culture, ~2 mil tried LSD in the US, claims of health risks (insanity, suicide, violence)
Methylated Amphetamines
MDA, MDMA (ecstasy)
Anticholinergic Hallucinogens
mandrake, henbane, belladonna, jimsonweed
Dissociative Anesthetics
angel dust, ketamine
LSD
potent, 50-150 microgram street dose, effective dose 10 micrograms
similar structure to serotonin
Serotonin
regulation of sleep, mood, impulsivity, cognition
blood, brain, GI tract, 7 receptor classes, 14 subtypes
produced in the raphe nucleus → central nervous system
analgesia, sleepiness, change in appetite
most metabotropic, some ionotropic, hormonal messenger traits
LSD Mechanism of Action
serotonin receptor partial agonist
mimics serotonin, alters system
higher affinity for 5HT2A, cross tolerance
Mescaline Mech of Action
psychoactive compound in peyote cactus
different structure, acts on 5-HT receptors
cross tolerance
Serotonin Hallucinogens
LSD most potent - ~20 min, lasts 8-12hrs
Morning glory seeds (lysergic acid amide) - ~10% LSD potency
Psilocybin - variable, ~1% LSD
Mescaline - ~10-14 hour trip, ~1/3000 LSD
DMT (dimethyltryptamine) - plant used to make tea, least potent, ~1 min kick in, ~1 hr trip
Hallucinogen Psychotherapeutic Use
Past- produce model psychosis, induce hallucinogens, destroy ego defenses, visual (drugs) vs auditory (schizo). risks outweighed benefits
Hallucinogen Effects
sim to stimulants, sympathomimetic (up HR and BP and body temp, pupil dilation)
visual, vivid, dream like hallucinations, synthesia, labile mood (magical thinking, cosmic sig)
altered cognitive experiences
Hallucinogen Side Effects
bad trips - acute paranoia, psychotic state
flashbacks (months/years later)
psychiatric disorders - manson family/cult, prepsychotic symptoms
Hallucinogens Tolerance
cross btwn hallucinogens
LSD hallucinogens and physical within days of use
days of abstinence to return of effect; days to complete tolerance
MDMA
ecstasy, club drug, high use in the 90s
schedule I ‘85
Methylated Amphetamines
intake: oral, inject, snort
effect last 6-8 hours
MDMA 75-150 mg, MDA 50-150 mg
Methylated Amphetamines Pharmacodynamics
blocks serotonin transporters (reuptake), and a bit of dopamine. Increase monoamine release
sympathomimetic, like stimulants
followed by a low
Methylated Amphetamines Physical Effects
Suppressed appetite, elevated heart rate
Increased blood pressure and body temp
Sweating and salivation, insomnia
Muscle tension
Bruxism (teeth grinding), trismus (lockjaw)
Methylated Amphetamines Psychological Effects
Euphoria, up emotional warmth and empathy, up talking
Down defensiveness, hallucinations are NOT common
Effects from drug AND environment
Methylated Amphetamine Withdrawal
Drowsiness, muscle pain, depression, paranoia, anxiety
Methylated Amphetamine Toxicity
Dehydration, heatstroke, heat exhaustion, muscle breakdown, kidney failure, stroke, seizure, heart attack - sympathomimetic effects
combo effects (envi too) - adulteration from more
after mult. high doses, synergistic effects with other drugs
Methylated Amphetamine Long Term Effects
Depletion of 5-HT and/or loss of 5-HT nerve terminals
(after single high dose or multiple low doses)
depression and cognitive deficits ??