6 - OCD & Related
1/18
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
19 Terms
What is the difference in diagnosis for OCD in DSM-IV and DSM5?
Used to be part of anxiety disorders
New category: OC & RD
Also: body diysmorphic, body-focused repetitive behaviours, olfactory reference disorder
What is excoriation disorder and explain the DSM-5 criteria
skin picking disorder, under OCRD
Skin lesions due to skin picking
Attempts to decrease/stop
Causes clinically significant distress/impairment in functioning
Not attributed to substance/other medical condition, not better explained by other mental disorder
What is olfactory reference syndrome and explain the DSM-5 criteria
false belief of emitting foul body odor
Culture-related (japan) - expanded
What is hoarding and explain the DSM-5 criteria
accumulation of possessions due to ↑ acquisition or difficulty discarding possessions
Excessive acquisition = repetitive urge to buy
Difficulty discarding = distress w discarding, perceived need to save
Results in clutter, safety compromised, significant distress/impairment
What are intrusive thoughts?
unwanted thoughts that cause distress
94% of participants experienced in last 3 months
Intrusive thoughts become obsessional for OCD
What is OCD characterised by? What are the criteria?
intrusive, recurring, unpleasant thoughts (obsessions)
Repetitive, irrational behaviours (compulsions)
Time consuming (more than 1 hr), significant distress/impairment
1.6~2.3 lifetime prevalence, fairly equal gender ratio, chronic
cultural differences (diff OCD compulsions)
What are rituals and how do they differ from OCD?
rituals are developmentally normal
E.g. children (2-6 y/o) with rituals
Adults also have ritualised behaviours
Becomes issue of concern if causes distress/impairment
Obsessions vs Compulsions
obsessions: unwanted thoughts, pictures, urges
Unpleasant, repetitive - feel out of control, uncomfortable, anxious
E.g. violent urges, religious thoughts, need for order, doubts about locking the door
Compulsions: repetitive physical/mental behaviours/avoidance
Feeling of need to do smthn over again, even if you don’t want to or doesn’t make sense
E.g. prayer, checking doors, counting/repeating everything
Behaviours = safety strategies / neutralising actions (to feel less responsible) / looking for danger (attention/reasoning biases)
Four common OCD themes
contamination
Harm
Order and symmetry
Unacceptable thoughts
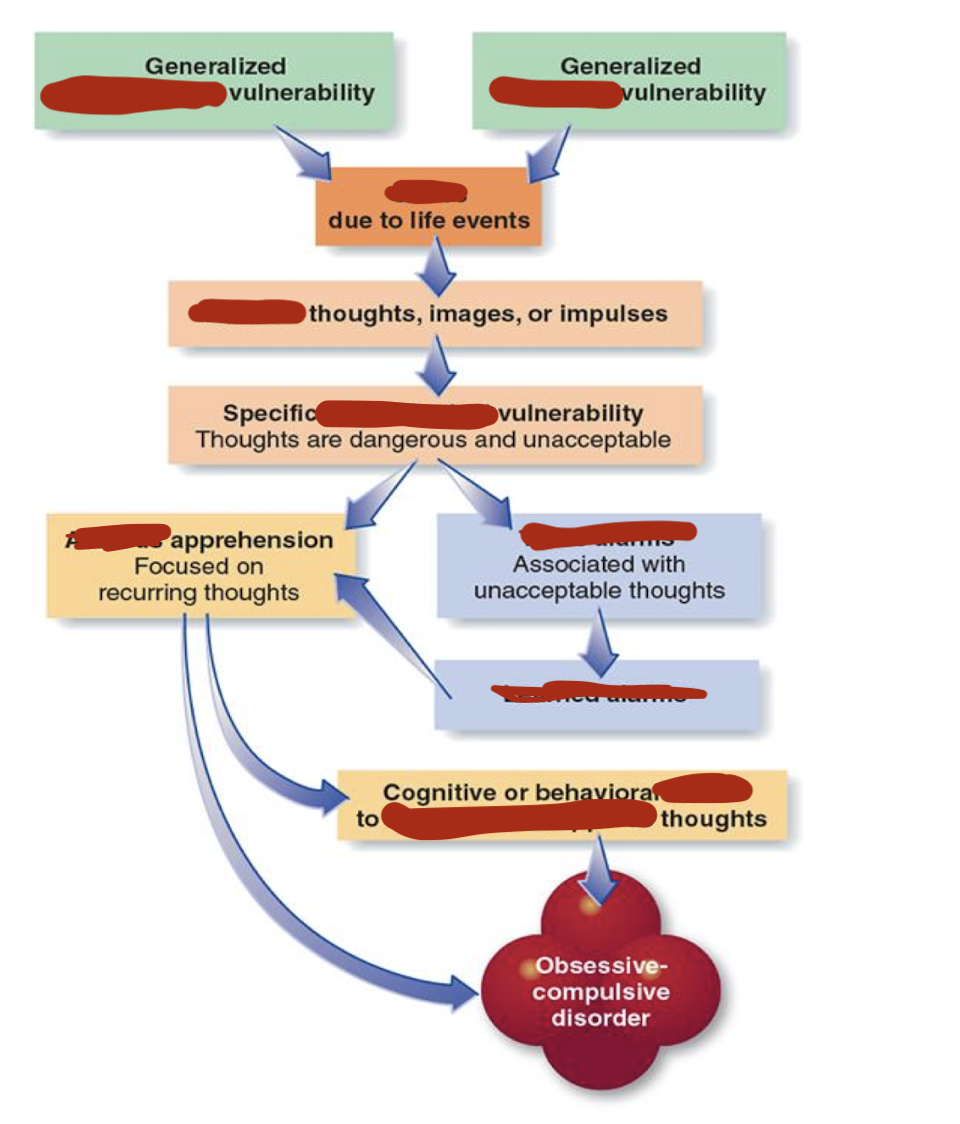
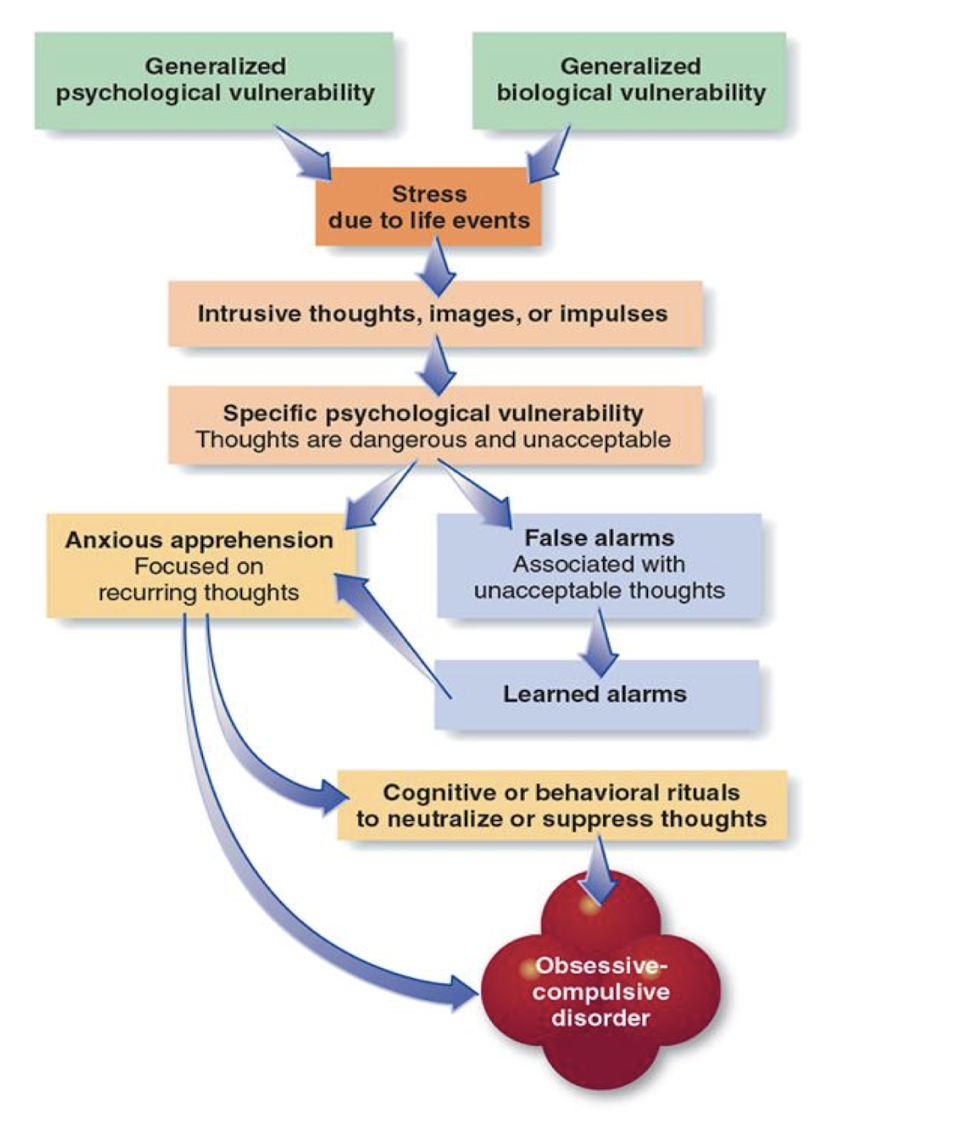
Explain the model of causes of OCD
generalised psych + bio vulnerability → stress → intrusive thoughts/images/impukses
Specific psych vulnerability → anxious apprehension / false alarm + learned alarms
Anxious apprehension → cognitive/behavioural rituals → OCD
Causes OCD
biological
Stressful/unpleasant event - learned experience
Assumptions & belief - cognitive style
What is meant by over valued ideas and how does it contribute to OCD?
strongly held, rigid/consistent abnormal belief, preoccupying life
Idealised value, identified with self, fail to adapt
Examples: hoarding, appearance, order, symmetry
What is meant by an over inflated sense of responsibility and what ole does it play in OCD?
obsessions 0 intrusive thoughts
Vulnerable indv interpret as indicating they may be responsible for serious harm
Explain the cognitive model for checking
Perceived responsibility + probability of harm + seriousness of harm → anxiety → preventative checking ↑ responsibility & uncertainty → consequences = feeling out of control, lack focus, more careful → strengthen belief about incompetence
Explain how obsession, anxiety, and compulsion interact with each other
obsessions → anxiety → compulsion → short term relief → obsession …
Vicious cycle
What is meant by thought action fusion?
Likelihood TAF = belief that simply having thought about even = more likely to occur
Moral TAF = thinking about action is morally equivalent to actually performing action
(Emotional reasoning - reasoning based on presence of emotion)
Two main treatment methods for OCD
medication (SSRI) - high relapse when discontinued
CBT (exposure and response prevention - ERP)
What are some problems with medication
40-60% patients remain symptomatic/no improvement - non-response
Side effects with clomipramine
High rates of relapse after discontinuation
Explain the exposure and response prevention treatment
Hierarchy of fears
Exposure - habituation (getting used to feeling)
Prevent compulsion, aversion, neutralisation
Task list created, gradual steps