L1. Opioid Analgesics I
1/153
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
154 Terms
What. are the 3 types of opioid receptors?
mu, kappa, delta
Opioid receptors are --- coupled receptors
GPCR
Endogenous opioid peptide are --- produced by the body and act similarly to ---
naturally produced
act similarly to opioids
Endogenous opioid peptides: 3 genes encode 3 precursor peptides
proenkephalin
prodynorphin
proopiomelanocortin
Proenkephalin binds with high affinity to --- and --- receptors
mu and delta
Proenkephalin functions as a ---
neurotransmitter
True / False: Proenkephalin are widely distributed in brain, spinal cord, adrenal medulla, and gastrointestinal tract
true
Where are prodynorphins distributed?
Brain and spinal cord
Dynoprhin ---- has a high affinity for kappa opioid receptors
A 1-17
Prodynorphins function as ---
neurotransmitters
Beta-endorphins function as --- or ---
neuromodulators or neurohormones
What is released in response to stress?
beta-endorphins
Beta endorphins have high affinity for -- and -- receptors
mu and delta
Proopiomelanocortin can be processed into
1. ACTH
2. a-MSH
3. beta-endorphin
Proopiomelanocortin has limited distribution of cell bodies to the --- and ---
intermediate lobe of pituitary gland
arcuate nucleus of hypothalamus
Proopiomelanocortin has axonal projections to
amygdala
periaquaductal gray (pain modulation)
brainstem and spinal cord
Opiod receptors are mainly in the
brain
brainstem
spinal cord
peripheral neurons
intestines
Mechanism of action of opioids
inhibit adenylyl cyclase = no cAMP
close voltage gated Ca channels = inhibits neurotransmitter release
open K channels = increase hyper-polarization
What happens when opioids inhibit adenylyl cyclase and reduce cAMP?
decrease cell excitability
Pharmacological effects of opioids
analgesia
Analgesia effects can be --
central, spinal, or peripheral
Periaquaductal gray (PAG) is in the ---- and activates descending pain inhibition pathways
midbrain
Central (supra spinal) analgesia is pain modulation in the ---
brain
Spinal analgesia is pain modulation in the --- neurons of the spinal cord
dorsal horn
Peripheral analgesia is activation of opioid receptors located on --- and --- fibers
alpha delta and C fibers
Pain transmission pathway from peripheral receptors
dorsal root ganglion
tract of lissaur
dorsal horn of spinal cord (decussate in anterior white commissure)
travel up neospinothalamic or paleospinothalamic pathway to VPL of thalamus
Pain transmission pathway from periaquaductal gray
PAG receives input from cortex/amygdala/hypothalamus
sends transmission to rostral ventral medulla
RVM sends 5-HT and norepinephrine to interneurons in dorsal horn of spinal cord
Interneurons inhibit pain
Central effects of opioids
Respiratory depression
Cough suppression
Miosis
Euphoria
Nausea/vomiting
How do opioids cause respiratory depression?
decrease brainstem centers response to CO2
decrease pontine/medullary centers
What do pontine and medullary centers regulate?
Respiratory rate, frequency, tidal volume
How do opioids cause cough suppression?
depress cough reflex in brainstem
How do opioids cause miosis?
central effect on oculomotor nerve = depress sphincter pupillae muscle
cause pupil dilation / no pupil constriction
How do opioids cause nausea / vomiting?
stimulates chemoreceptor trigger zone inthe medulla
Peripheral effects of opioids
Constipation
Cardiovascular effects
Pruritis
How do opioids cause constipation?
increase smooth muscle tone
decrease propulsive motility though GI
True / False: urinary retention sometimes occurs with opioid due to increased smooth muscle tone
true
How do opioids cause pruritis?
Histamine release and central action on central pruritocetive neural circuits
How do opioids cause cardiovascular effects?
cause histamine release = peripheral vasodilation / orthostatic hypotension
True / False: opioids have minimal direct effects on heart rate and blood pressure
true - effects are secondary due to histamine release
Cerebral vasodilation is ---- to --- depression.
Can also increase ---
secondary to respiratory depression
can also increase CSF
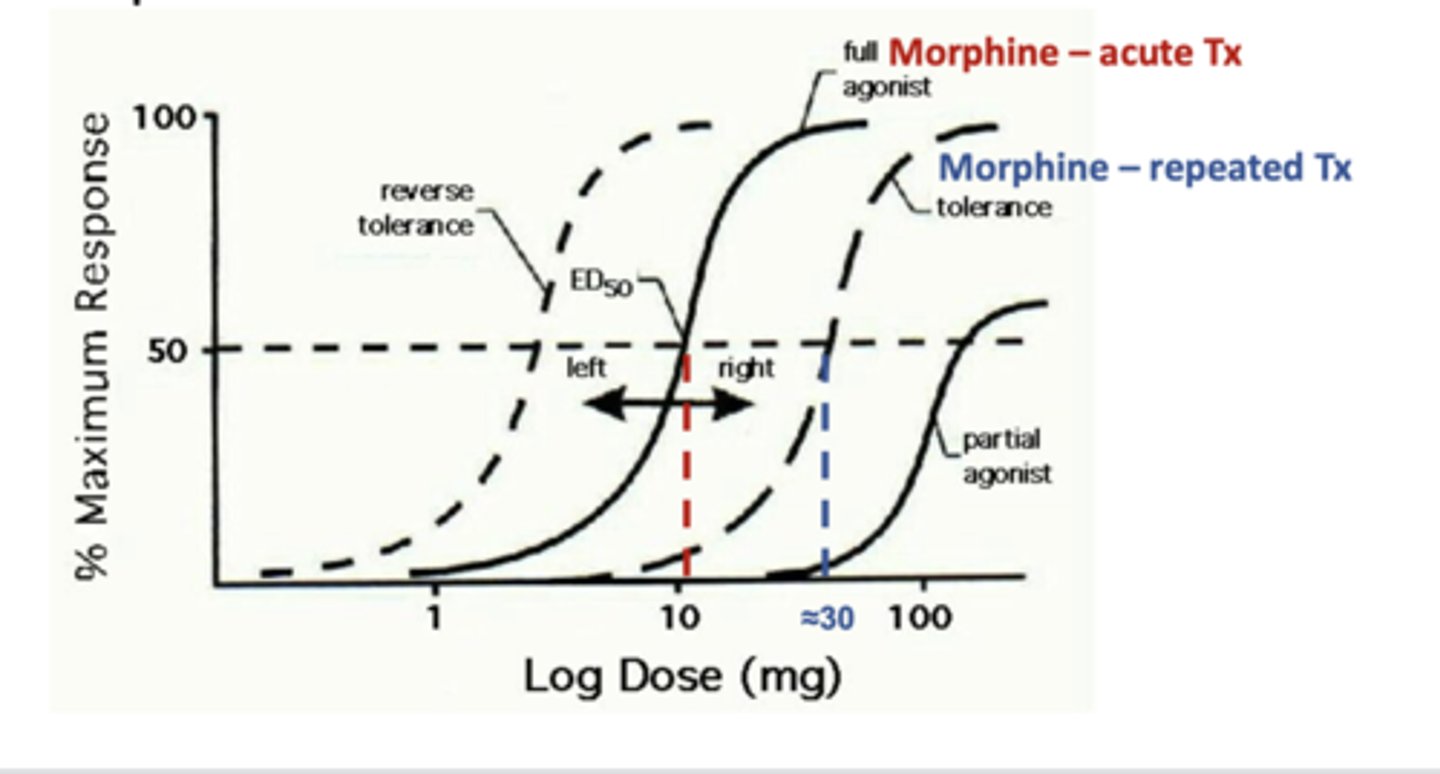
Tolerance is a ---- of a drug as a consequence of prior exposure to that drug
decreased efficacy
Tolerance results in a --- shift of the dose response curve
rightward
True / False: Tolerance can develop to some effects of opioids but not to others
true
Tolerance can be overcome by --- the dose
increasing
Tolerance occurs when repeated use of opioids leads to a --- response to the same dose. Over time, --- are needed to achieve the same analgesic (pain-relieving) effect
reduced response
higher doses
What causes tolerance?
reduced efficacy
short duration of action
True / False: tolerance remains when the opioid is discontinued
false - tolerance is lost
What happens when opiates are given together?
cross tolerance
---- refers to the development of a new, atypical physiological state produced by repeated administration of a drug, which then makes its continued use necessary to prevent the appearance of a withdrawal syndrome
Physical dependence
Withdrawal reactions are usually the --- of the physiological effects produced by acute administration of the drug
opposite
Physical dependence --- after opioid is discontinued
decreases
Addiction is associated with significant --- dependence and is accompanied by compulsive drug --- and drug taking behaviors
psychological
drug seeking
---- alone does not fulfill the criteria for drug addiction
physical dependence
What is needed for an individual to be considered addicted to opioids?
psychological dependence
physical dependence
What is the diagnosis for opioid addiction?
opioid use disorder
What does profound opioid toxicity cause?
respiratory depression / cough suppression
Signs of an opioid overdose include ---, --- and decreased ---
stupor, miosis, and decreased respirations
What opioid receptor antagonist is administered to restore ventilation?
naloxone
Morphine is a --- receptor agonist
mu
Morphine is a --- and --- receptor agonist at high doses
kappa and delta
Morphine is a natural --- from opium derived from the poppy plant
phenanthrene alkaloid
Morphine is ---- absorbed after oral administration
well
What is the first pass effect of morphine?
large first metabolism in liver
How does first pass metabolism for oral medications occur?
drug travels from stomach to small intestine
absorbed in small intestine
takes portal vein to liver
metabolized by liver
reduced amount of active drug reaches circulation
What opioid has a large first pass metabolism?
morphine
What beta blocker has large first pass metabolism?
propranolol = b1/b2 nonselective antagonist
True / False: Like all opioid analgesics, morphine provides symptomatic pain relief only
true
How is morphine metabolized in the liver?
by glucoronidation
What does morphine become after glucoronidation by the liver?
morphine 6 glucoronide
Morphine 6 glucoronide has high affinity for --- opioid receptors
mu
What happens to morphine metabolites with chronic oral dosing of morphine?
morphine 6 glucoronide can exceed morphine
How is morphine eliminated?
glomerular filtration
What must happen to mophine 6 glucoronide before it is eliminated via glomerular filtration?
must be conjugated
True / False: morphine can accumulate in the tissues
false - once elimination is complete by glomerular filtration there is no morphine left
Morphine half life
2-4 hours
Morphine duration of action
3-5 hours
Morphine recommended dosing interval
q 4hours
Morphine IV to PO ratio
1:3
True / False: morphine causes increased biliary tract pressure
true
Opioid induced hyperalgesia
increased sensation of pain
Opioids induced hyperalgesia is associated with chronic administration of opioid analgesics especially --- and ---
morphine and fentanyl
Potential mechanisms of opioid induced hyperalgesia involve involve --- and activation of --- and --- receptor
spinaldynorphin
bradykinin and NMDA
Why is morphine not given during compromised respiratory status?
depresses pontine and medullary respiratory receptors
depresses brainstem center response to CO2
Why is morphine not given to patients with liver and kidney disease?
metabolized by liver
eliminated by glomerular filtration
Why is morphine not given to patients with head trauma?
indirectly increases CSF
impairs clinical picture
Why are opioids contraindicated in pregnancy?
cause physical dependence / respiratory depression
Why are opioids contraindicated in paralytic ileus and GI obstruction?
increase smooth muscle tone
decrease propulsive motility though GI
What happens to opioids if there is liver dysfunction?
increases plasma levels of opioid
not metabolized
What happens to opioids if there is a kidney dysfunction?
increases plasma levels of opioid metabolites
morphine --> morphine 6 glucoronide
morphine 6 glucoronide is not eliminated by the kidneys
Administration of a drug with mu opioid receptor agonist properties can produce which of the following effects?
A. Diarrhea
B. Mydriasis
C. Hypertension
D. Nausea
E. Anxiety
D. Nausea
Death due to acute opioid overdose is due to which of the following?
A. Convulsions leading to status epilepticus
B. Myocardial infarction
C. Respiratory depression
D. Atrial fibrillation leading to stroke
E. Acute pulmonary edema
C. Respiratory depression
Mu receptor activation causes:
respiratory depression
cough depression
miosis
euphoria
nausea / vomiting
what is the difference between chemical structure of morphine and codeine?
morphine = hydroxy group at 3 position = OH
codeine = methoxy group at 3 position = OCH3
Codeine is a natural --- from opium
phenanthrene alkaloid
What provides greater oral bioavailability of codeine compared to morphine?
methoxy (OCH3) instead of hydroxy group (OH)
Codeine is metabolized by ---
liver
Codeine can be metabolized to ---
morphine
Codeine is eliminated via ---
glomerular filtration (kidneys)
Indications / clinical use for codeine
oral analgesic for mild to moderate pain for ambulatory patients
antitussive
What is effective for relief of mild to moderate pain in ambulatory persons: morphine or codeine?
codeine