CSB330 All Content
1/105
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
106 Terms
principles of a paramedic
Integrity and impartiality
Promoting the public good
Commitment to the system of government
Accountability and transparency
professional boundaries
the clear separation that should exist between professional conduct (meeting a patient's health needs) and a practitioner's own personal wants, needs, views and feelings
Office of the Health Ombudsman (OHO)
the first place to contact for health service complaints regarding registered and non-registered practitioners
mandatory notifications
practised the practitioner's profession while intoxicated by alcohol or drugs; or
engaged in sexual misconduct in connection with the practice of the practitioner's profession; or
placed the public at risk of substantial harm in the practitioner's practice of the profession because the practitioner has an impairment*; or
placed the public at risk of harm because the practitioner has practised the profession in a way that constitutes a significant departure from accepted professional standards.
practising within your scope
you have to be trained, competent and authorised
harm
An outcome that negatively affects the patient's health and/or quality of life, impairment of structure or function of the body and/or deleterious effect arising there (WHO).
error
a preventable adverse effect on the patient's healthcare.
coroners
the state coroner,
the deputy coroner,
two Brisbane-based coroners and
three regional coroners.
open disclosure
the open discussion of adverse events that result in harm (real or potential) to a patient while receiving health care.
Open disclosure usually takes place with the patient and their family/carers present for support.
Open disclosure ensures that honest, open, timely and empathetic discussions occur between the healthcare provider and the patient following a clinical incident.
WHS
involves the identification and management of hazards and risks to the health and safety of everyone in your workplace, yourself, your colleagues, bystanders, and patients.
risk
probability of harm being caused by a hazard
diagnostic errors
Incorrect or significantly delayed diagnosis leading to patient harm e.g. Bias errors
treatment errors
Medication and/or procedure errors resulting in harme.g. Wrong dose
failure errors
Failure of equipment or systems to function as designed e.g. radio error, stretcher collapse
preventative errors
When drugs/procedures known to reduce harm, are not implemented
why errors happen
Organisation; Poor clinical governance, poor oversight, poor safety culture
Teamwork; Poor communication, poor tasking, poor safety environment
Individual paramedic; Experience, personal beliefs and attitudes, fatigue, stress
Task and equipment design; Difficult to use equipment or procedures, effort involved
Patient; Individual characteristics, typical disease presentations, poor hygiene, mental health/behavioural issues
Australian Commission on Safety and Quality in Health Care
ACSQHC's purpose is to contribute to better health outcomes and experiences for all patients and consumers and improve value and sustainability in the health system by leading and coordinating national improvements in the safety and quality of healthcare.
National Safety and Quality Health Service (NSQHS) Standards
Clinical Governance
Preventing and Controlling Infections
Comprehensive Care
Blood Management
Partnering with Consumers
Medication Safety
Communicating for Safety
Recognising and Responding to Acute Deterioration
informed consent
a person's decision, given voluntarily, to agree to healthcare treatment, procedure or other intervention.
health care rights
access, safety, respect, communication, participation, privacy, comment
6Rs
Right Paitent
Right Drug (Verbalise and confirm the medication name, indication for use, medication is unused and expiry date.)
Right dose (Check the right dose has been Calculated correctly + Prepared and drawn up correctly)
Right Route (method of administration)
Right Time (Drugs that can be repeated often have set periodic intervals, to avoid accidental overdose/adverse effects)
Right to refuse
clinical reasoning
the process of thinking and decision-making in clinical practice
improved by Engaging in reflective practice and self-assessment
requires Technical proficiency in medical procedures, Patient communication and anatomy/ physiology
snake bite
immoblise paitent
reassure
remove jewlery
cut off clothes
pressure bandage (distal to proximal)
splint
check circulation
report (photo of dead snake etc)
use for haemostatic dressing
If there is severe, life-threatening bleeding from a wound site not suitable for tourniquet, or from a limb when a tourniquet has failed to stop the bleeding
haemostatic dressing application
Haemostatic dressings must be applied as close as possible to the bleeding point, held against the wound using local pressure (manually initially) then held in place with the application of a bandage (if available). Haemostatic dressings should be left on the bleeding point until definitive care is available
direct pressure method for a bleed
Applying firm, direct pressure sufficient to stop the bleeding. Pressure can be applied using a pad over the bleeding point.
If bleeding continues, apply a second pad and a tighter bandage over the wound. If bleeding still continues, check that the pad and bandage are correctly applied, directly over the bleeding.
Applying firmer pressure, only using 1 to 2 pads over a small area, will achieve greater pressure over the bleeding point than continuing to layer up further pads
embeded object
Do not remove the embedded object because it may be plugging the wound and restricting bleeding.
Apply padding around or on each side of the protruding object, with pressure over the padding.
Arterial tourniquets
should only be used for life-threatening bleeding from a limb, where the bleeding cannot be controlled by direct pressure. Ideally, a tourniquet should not be applied over a joint or wound, and must not be covered up by any bandage or clothing.
follow instructions or 5 cm above the bleeding point if no instructions
inital torniquet fails can add another/ try combo of tourniquet and homeostatic dressing
internal bleeding
may be difficult to recognise, but should always be suspected where there are symptoms and signs of shock.
Internal bleeding includes bruising, locally contained bleeding (e.g. an "egg on the head") and the bleeding associated with injury or disease of organs in the abdomen or chest, as well as fractures. Severe bleeding may also occur from complications of pregnancy.
Symptoms and signs may include:
pain, tenderness or swelling over or around the affected area
the appearance of blood from a body opening
nose bleed
Pressure must be applied equally to both sides of the nose, over the soft part below the bony bridge (usually between the thumb and index finger).
The person should lean with the head forward to avoid blood flowing down the throat.
Encourage the person to spit out blood rather than swallow it as swallowed blood irritates the stomach, and causes vomiting which can worsen the bleeding.
The person should remain seated at total rest for at least 10 minutes. On a hot day or after exercise, it might be necessary to maintain pressure for at least 20 minutes.
airway obstruction
Airway obstruction may be partial or complete, and present in the conscious or the unconscious person. Typical causes of airway obstruction may include, but are not limited to:
relaxation of the airway muscles due to unconsciousness
inhaled foreign body
trauma to the airway
anaphylactic reaction
obstruction
5 back blows checking if obstruction has been removed after each
if ineffective identify compression point as for CPR and give up to five chest thrusts
encourgae active coughing
An infant may be placed in a head downwards position prior to delivering back blows
breathing
LOOK for movement of the upper abdomen or lower chest
LISTEN for the escape of air from nose and mouth
FEEL for movement of air at the mouth and nose.
location for chest compressions
the lower half of the sternum
lace the heel of hand in the centre of the chest with the other hand on top
Avoid compression beyond the lower limit of the sternum. Compression applied too high is ineffective and if applied too low may cause regurgitation and/or damage to internal organs.
compressions
2 finger technique for infants
Either a one or two hand technique can be used for performing chest compressions in children
person needs to be on back on firm surface
remember full recoil of chest
lower half of the sternum should be depressed approximately one third of the depth of the chest with each compression. This equates to more than 5cm in adults
perform chest compressions for all ages at a rate of 100 to 120 compressions per minute (almost 2 compressions/second)
swap after 2mins
compressions for pregnant people
place padding such as a towel, cushion or similar object under the right hip to tilt the woman's hips (approximately 15-30 degrees) to the left but leave her shoulders flat to enable good quality chest compressions. The reason for this position in pregnant women is to move the weight of the pregnant uterus off of her major blood vessels in the abdomen
Basic Life Support (BLS)
taught in first aid and CPR classes
Primary Survey
Danger
Response (AVPU)
Haemeorage
Airway
Breathing
Circulation (if unresponsive do DRXCABDE)
AVPU
Alert - patient's eyes are open spontaneously.
Verbal - The patient opens their eyes to verbal stimuli/voice (COWS)
Pain - The patient opens their eyes to a painful stimulus. (eg Trap Squeeze)
Unresponsive - The patient does not respond to any stimuli. (does not necessarily mean they are unconscious)
Airway manoeuvres
Head tilt is used to straighten the airway and is conducted by using two hands to gently place the head in the sniffing position. (dont do if suspeted c-spine injury)
Jaw thrust is used to move the tongue anterior (forward) in the mouth so as not to cause further obstruction and to assist in visualising the airway. It is conducted by the paramedic using the fingers of both hands on either side of the patient's jaw, hooking the fingers under the angle of the jaw and lifting anteriorly.
Chin lift / opening the mouth involves the paramedic using their thumbs to open the jaw while maintaining the jaw thrust. This allows for clear visualisation of the airway.
clearing airway
Liquid obstructions can sometimes be cleared by positioning the patient on their side, opening their mouth, and allowing gravity to clear the airway. This is otherwise known as the 'recovery position'. Alternatively, or in conjunction with positioning, oral suctioning can be done to clear the liquid.
Soft solids and liquids can be removed either through positioning and digital external scraping where the paramedic strokes the downward-facing cheek of the patient to encourage the object to loosen and fall out of the oral cavity, through oral suctioning, or removal utilising Magill's forceps.
Solid obstructions will often be removed utilising Magill's forceps, occasionally assisted with a laryngoscope.
checking equipment
At the beginning of each shift, the suction equipment should be checked for serviceability by the oncoming crew. This should include: checking the level of gas available in the oxygen cylinder, ensuring all connections are tight, tubing and equipment are clean and ready for use, and suction pressures are set to the required adult setting. The suction pressure should be checked to ensure it is working correctly.
breathing interventions
Manual ventilation via a bag-valve-mask (BVM), administering intermittent positive pressure ventilation (IPPV). This is colloquially referred to as 'bagging'.
Supplemental oxygen is delivered through a BVM or another type of mask (e.g. a simple face mask, nasal prongs, non-rebreather mask).
checking pulse
The radial pulse is the least invasive and, therefore, most often used. However, it can be difficult to assess if the patient has very low blood pressure.
the carotid pulse is more easily palpated and quickly identified. This makes the carotid favoured when no radial pulse can be confidently identified or the patient appears unresponsive.
The brachial is typically reserved for assessing blood pressure. the femoral pulse is typically only palpated during indirect haemorrhage control techniques. This is due to the particularly invasive nature of the location.
The pulse check should only take ten seconds to complete. The paramedic is simply checking to see if a pulse is present. If a pulse is present, the paramedic will take note of the regularity, strength, and speed of the pulse. If no pulse is present, this will indicate the need for CPR to commence.
SITREP
confirm your crew number, clinical and/or operational situation, resources required, and at what speed
Oropharyngeal airway devices (OPA)
patient can be sitting in any position for insertion
measured from central incisor to angle of jaw or tragus to corner of mouth
for adults inserted opposite way up for half its length then rotated 180, however dont invert for kids
if gagging, remove
Nasopharyngeal airway devices (NPA)
measure from tragus to nostril on that side
lube before inserting
place bevel inside nose facing septum
inserted until flange rests just outside nostril
Intermittent positive pressure ventilation
size mask correctly (better to have slightly bigger than too small)
ensure seal using C3/ CE grip
compress bag 1/3 slowly, let expriy take x3 to 4 longer
oxygen delivery
nasal prongs (small FiO2 increase 1-4L/min)
simple mask (6-8L/min)
nebuliser mask (6-8L/min)
non-rebreather/ resviour mask (bag attached, 8-10L/min)
Manual ventilation bag (8-15L/min)
oxygen uses
hypoxia associated with physical trauma or respiratory emergencies or critical state patient
has immediate effect but lasts <5mins
AVPU equivalence with GCS
Alert (15-12)
Verbal (14-10)
Pain (10-5)
Unresponsive (5-3)
using magill's forceps
put patient in sniffing position
follow laryngoscope towards object
open blades when within 1-2cm
after removal sweep left + right with lyrgoscope to ensure no further obstructing material
visualise glottis to ensure its clear
suction
direct oropharynx suctioning usually requires Yankauer sucker
test before use with container of water (also use water for cleaning throughout)
insert along laryngoscope blade
cover top hole for suction (uncover to withdraw)
collect suctioned liquid for evaluation
sucker can be disregarded if no sufficient reciprocal or potentially reused
laryngoscope
make sure patient is in sniffing position (sometimes need to elevate)
blade inserted on the right side of mouth to displace tounge to the left
advance down the tongue with blade until glottis is located
if using a curved blad, place tip in vecular grove at junction of the tongue and epiglottis
to move mandible, move the laryngoscope up and away, in line with the handle
straight blade moves epiglottis against the tongue to expose glottis
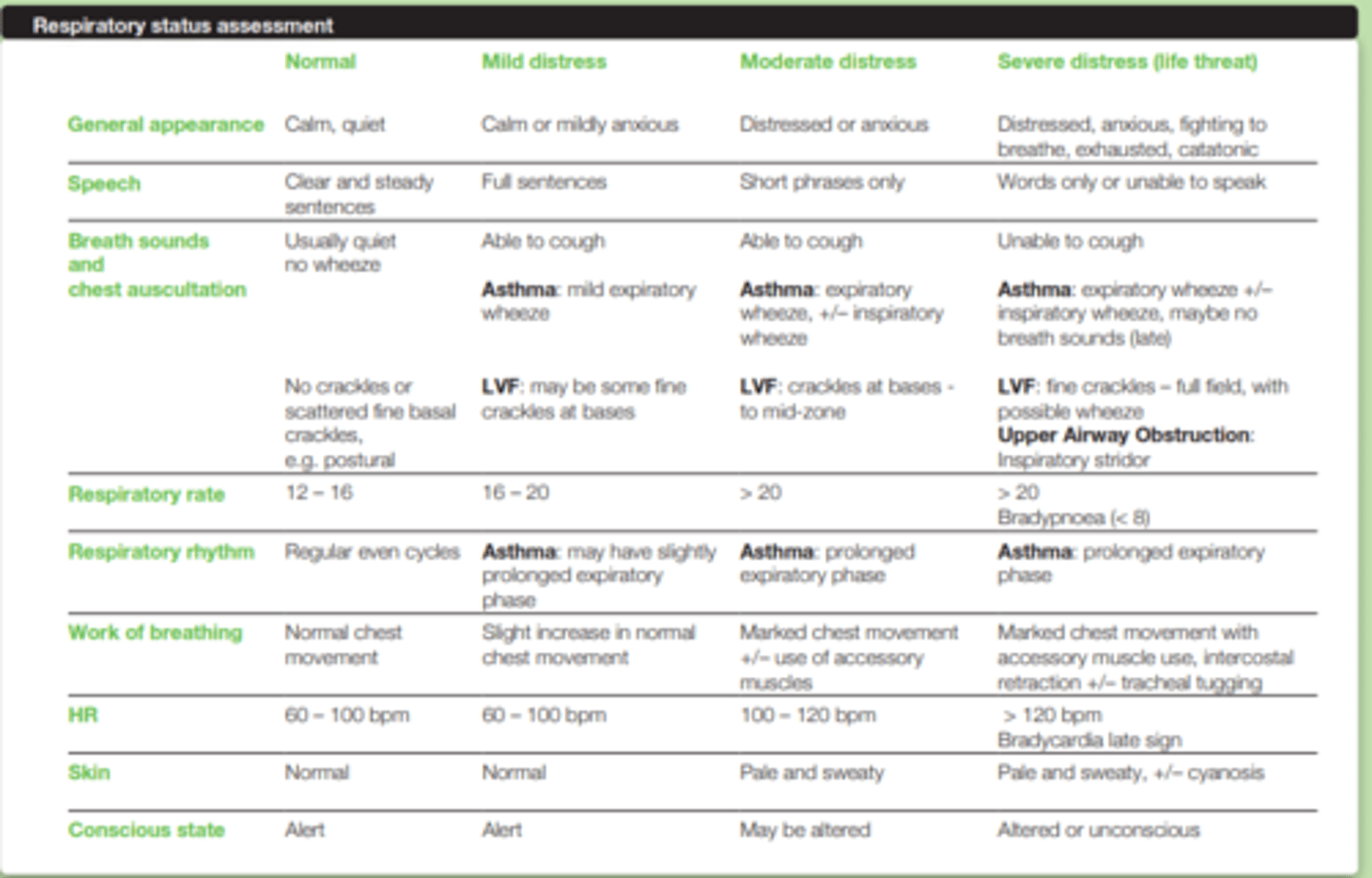
Respiratory status assessment (RSA)
Conscious state
Appearance
Pulse rate
Effort
Respiratory rate
Rhythm
Sounds
Speech
Skin
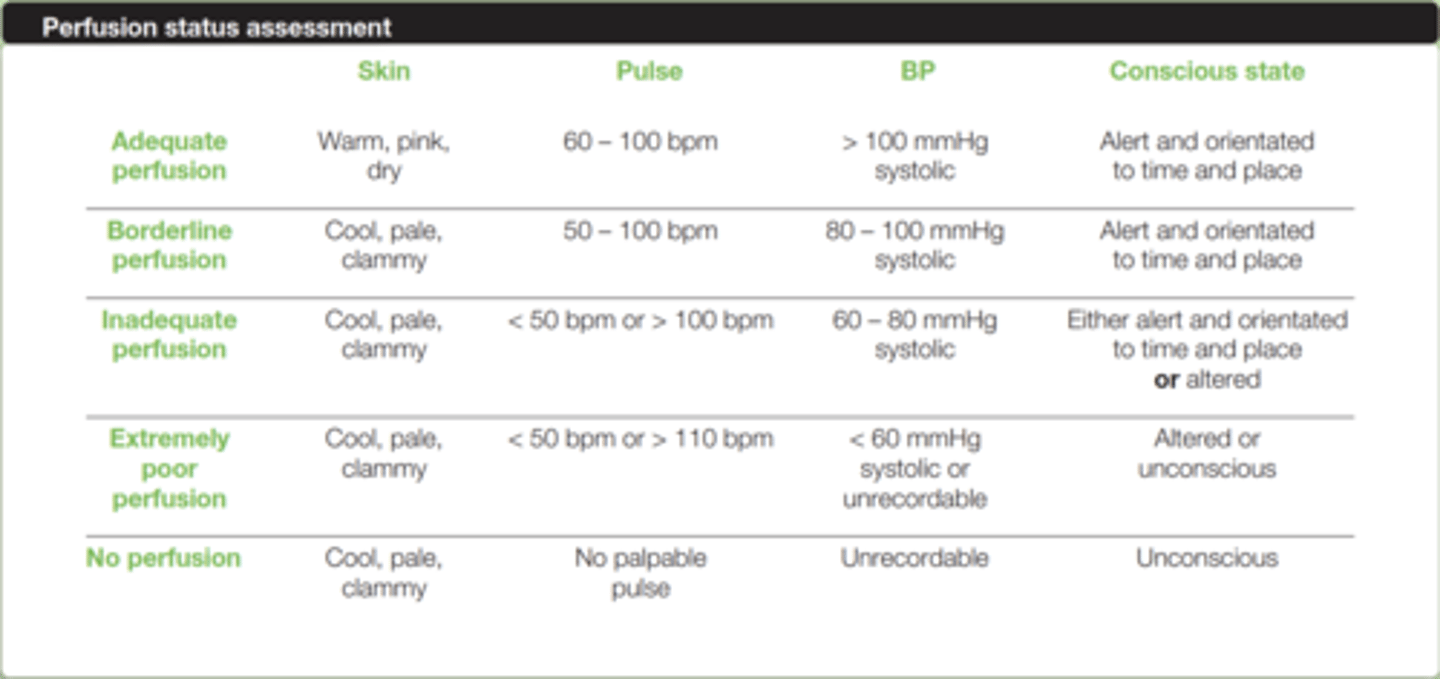
Perfusion Status Assessment (PSA)
history taking (SAMPLE)
Signs + symptoms
Allergies + Adverse reactions
Medication
PHMx
Last ins/ outs
Events Leading up
Assessing symptoms (OPQRST)
O NSET (mode of onset and time, rapid or gradual? )
P ROVOCATION/PALLIATION (what makes it worse, what makes it better)
Q UALITY (what does it feel like, descriptive)
R ADIATION /REFERRED (localised, travels, felt elsewhere)
S EVERITY (subjective, 0-10, does it interfere with ADLs/Sleep)
T IMING (when did it first start, has it happened before, how long has it lasted, consistent or intermittent?)
hypertension meds
Diuretics: lasix, frusemide, spironolactone
Beta-blockers/β-blockers: "olol's"
ACE inhibitors: "pril's"
Angiotensin II receptor blockers: "sartan's"
Calcium channel blockers: "ipine's"
Alpha-blockers: "azosin's"
Alpha-2 Receptor Agonists: "idine's"
Combined alpha and beta-blockers
diabetes meds
insulin injections
Oral tablets:
Metformin
Glipizide
Jardiance
Januvia
Epilepsy meds
Anti Epileptic Drugs (AEDs) - used to managage long-term
sodium valproate: epilem, valpro
carbamazepine: tegratol, curatil
lamotrigine: lamictal
levetiracetam: keppra
topiramate: Topamax
cannabinoids
Seizure termination drugs:
First line: Benzodiazapines (midazolam, diazepam, lorazepam)
Second line: AEDs (Keppra, phenytoin, sodium valproate)
Third line: Barbituates (phenobarbital), propofol.
anticoagulants
Warfarin: The reversal agent is Vitamin K, has a very small therapeutic window, and requires regular blood tests to monitor to ensure pt is appropriately dosed.
Rivaroxaban: Xarelto
Dabigatran: Pradexa
Apixaban: Eliquis
Clopidogrel:
antibiotics
Penicillins; flucloxacillin, amoxicillin
Cephalosporins: cefalexin, Keflex, ceflex
Tetracyclines; doxycycline
Aminoglycosides; gentamicin
Macrolides; azithromycin, erythromycin, clarithromycin Metronidazole; Flagyl
Quinolones ciprofloxacin
pulse oximetry
can be attached to fingers (no nail polish), ear lobes, sometimes foreheads and infant foots
chose correct paediatric/ adult size
blood pressure can be assed concurrently (different limb)
allow 5-10secs for readings to stabilise
Assessing blood pressure
place stethoscope bell over brachial artery, inflate until 40mmHg over when Korotkoff sounds heard
deflate the cuff, sounds will be heard again when pressure is approx. equal to systolic blood pressure
when sounds disappear again pressure is equal to approx. diastolic pressure
assessing respiratory rate/ rhythm
try and make sure patient doesnt know what your doing
start timing and count inspirations over a 30sec period (x2 for per minute)
temperature sites
rectal (invasive), oral (varies), temporal (variation), axillary (sweating effects), tympanic (in the ear, most easy/reliable)
tympanic assessment
for adults outer ear usually needs to be pulled upwards and for infants pull posteriorly to align ear canal
change probe tip each time
measuring blood glucose
clean finger with antiseptic wipe and allow to dry
draw a drop of blood using a lancet from the side of a finger near the tip (less painful)
test strip is used to absorb the correct amount of blood
glucometer gives results in mmol/L or mg/dL
blood glucose readings
4-7mmol/L normal
<4 hypoglycaemia
>7 hyperglycaemia
signs of acutely ill patient
delirium
Respiratory Signs
cardiovascular signs
neurgolical signs
delirium
Acute change to cognitive function over hours or a few days.
A recent change in mental status, has it fluctuated? Is it worse at night (a.k.a. Sundowner Syndrome)?
Difficulty concentrating, following instructions, easily distracted?
Incoherent thinking, rambling conversation, flight of ideas?
Alert, drowsy, comatose, or increased alertness (agitation, irritable)?
Respiratory Signs
Stridor and intercostal recession
Accessory muscle use
Unable to speak in sentences
SpO2 <90%
Angiooedema
cardiovascular signs
Absent pulse (peripheral or central)
HR <40bpm or >180bpm
SBP <100 mmHg (where previously within normal range)
Poor peripheral perfusion (tissue hypoxia):
neurological signs
Absent gag reflex (airway threatened)
Not obeying commands
Unresponsive to painful stimuli
Moving only one side (stroke, cerebral haemorrhage)
Reduced respiratory rate
Sudden reduced LOC (AVPU)
Pupils size and reaction to light (pinpoint, unequal, dilated, unresponsive, sluggish)
Seizure activity
GCS <10
sepsis
Temperature >38 or <36
Tachycardia >90bpm
Tachypnoea >20breaths/min
SBP <100mmHg
BGL >10mmol
ALOC
Non-blanching petechial (pinpoint) or purpuric rash/bruising:
head-to-toe examination
Inspect the area for obvious injury or deformity
Palpate for pain and/or crepitus
Where applicable, assess passive and active movement (i.e. can I move it for you without pain, can you move it yourself without pain).
assessment of limb
pulse
pallor
perishing cold
pain
paralysis
Paraesthesia
nexus c-spine rule
C-Spine Injury CANNOT be ruled out if ANY of the following are present:
Midline cervical tenderness
Altered mental status (GCS <15)
Focal neurological deficits
Intoxication
Painful and/or distracting injury
Canadian c-spine rule
C-Spine injury CANNOT be ruled out if ANY of the following are present:
HIGH-RISK FACTORS (cannot rule out injury):
>65 years old
Dangerous mechanism of injurya. Fall from height (2m or >5 stairs)b. Axial load to head (e.g. diving)c. High-speed RTC (>60km/hr, rollover, or ejection)d. Motorised recreational vehicles (e-bikes/e-scooters, quadbikes, etc.)e. Bicycle struck, or collision
Parastheasias in extremities
Neurological Status Assessment (NSA)
level of conciousness (GCS)
Cranial Nerve (CN) Assessment
speech
Peripheral motor and sensory function
GCS Scores
3-8 = Severe impairment/injury, <8 = Loss of gag reflex, airway risk!
9-12 = Moderate impairment/injury
13-15 = Mild impairment/injury, you can have a GCS 15 and still have a brain injury/neurological deficit
GCS Adjustments Paediatrics
use baby sounds to determine conscious state
5- orientated + spontaneous
4- inappropriate but spontaneous
3- only after verbal stimuli
2- only after pain
1- not at all
cranial nerve assessment
assessing the level of functioning of the 12 nerves that are located across the ventral surface of the brain. These nerves represent the functioning of several important motor and sensory functions, particularly those that relate to the eyes.
Dysfunction is highly correlated to underlying central nervous system injury. While the ability to complete a full cranial exam would be impressive, it would also be time-consuming. In paramedic care, it would be sufficient to carry out the assessment outlined in your readings:
PEARL (Pupils Equal And Reactive to Light) CN II-IV
Face and Shoulders CN VII, XI
Swallowing CN IX, XDysphagia (difficulty swallowing)
Smell and Taste CN I
speech conditions
Dysphasia = Difficulty in the generation of speech
Dysarthria = Difficulty articulating speech
Peripheral motor and sensory function
important in the assessment of spinal cord injury.
What can the patient feel?Numbness, decreased sensation, burning, tingling, pins and needles?
How can the patient move, power, and gait?
Is there symmetry?
Is there weakness, or hypersensitive reflexes?
Non-pharmacological interventions for pain
cognitive: music, distraction, hypnosis, guided imagery
behavioural: relaxation techniques, biofeedback exercises, breathing control
physical: heat and cold (cryoanalgesia) application, massage or touch, position and comfort, temperature regulation, transcutaneous electrical nerve stimulation (TENS), acupuncture, chiropractic, immobilisation.
pelvic binding
bring legs together and secure at the knees and ankles
apply over greater trochanters (not illiac crests)
only release after definitive examination
informed consent
Benefits
Risks
Alternatives
Intuition (how the paitent feels)
Nothing (what happens if they refuse/ wait)
things causing altered level of consciousness (AEIOUTIPS)
Alcohol/ Acidosis
epilepsy
infection
overdose/ oxygen deficiency
uraemia
Trauma/ tumer
Insulin
Psychogenic/ poison
stroke/ shock
cardiac arrest
the heart is unable to beat and therefore pump adequate amounts of oxygenated blood throughout the body
chain of survival
Recognition of cardiac arrest and activation of additional resources required on scene.
Early cardiopulmonary resuscitation (CPR) with an emphasis on high-quality chest compressions
Rapid defibrillation
CPR
30 compressions to 2 breaths
swap every 2mins during defibulation
100-120 compressions per min
1/3 depth and full recoil of chest
COACHED
Continue chest compressions
Oxygen away (if required)
All others stand clear (the person performing compressions continues to do CPR)
Charging defibrillator
Hands off (order to person performing CPR) & "I'm Safe" "All hands off" (confirmation of hands-off chest, person to do visual and hand sweep to ensure no one is touching the patient)
Evaluate Rhythm
Deliver shock (shockable rhythm, 200J for adult 4J/per kg for paed) or Dump the charge (non-shockable rhythm)
pad placement
centre of the apex (lateral) pad is positioned over the 5th intercostal space on the mid-axillary line (the position of V6 when a 12-Lead is performed). The sternal pad should be positioned to the right of the sternum, below the clavicle.
shockable rhythms
Ventricular Tachycardia (VT):
- can only defib if they're Unconscious/ Pulseless (possible to be neither for a bit but still VT)
- Looks; Regular (each complex is identical and follows the same pattern) Broad complex (the QRS complex is wide), Tachycardia (>100bpm)
ventricle fibulation
- Irregular/chaotic (the complexes have no pattern of varying amplitude)
- Tachycardia (>100bpm)
- Fibrillations/fibrillatory waves can be coarse (jagged and tall) or fine (wide and small)
non-shockable
Asystole: flat/ish line
pulseless electrical activity (PEA): electrical activity is there, but there's no mechanical output to produce a pulse
bias
Attribution bias - defining/diagnosing a person's presentation due to characteristics
Confirmation bias - tendency to search for, interpret or favour in a way that confirms or supports one's prior beliefs
Implicant bias - implicit bias or stereotype is the attribution of qualities by an individual to a member of a social group.
Hypotheticodeductive Reasoning (HR)
Hypothesis generation: Dependent on information gathered during the systematic assessment
hypothesis testing: Further assessment, or intervention/s
Hypothesis verification: Change in patient status or results of furthertesting
who's considered a paediatric
paediatric assessment generally refers to the assessment of patients aged 1 to approximately 14 years.
In Queensland alone, the public system varies greatly on when they consider the paediatric cut-off age. For example, the QAS drug dosage calculations consider the cut-off for a paediatric patient to be 12. However, Queensland public emergency departments accept patient presentations/admissions until the 16, however public mental health, oncology and complex care presentations will accept patients up to 18.
This subject will focus on paediatrics up until 12 years of age.