Lecture 12 - Clinical Psychology
1/57
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
58 Terms
conduct disorder
• A disorder of childhood and adolescence characterized by a repetitive and persistent pattern of behavior in which the basic rights of others or major age‑appropriate societal norms or rules are violated (e.g., aggression, destruction of property, deceitfulness, serious rule violations).
parent management training (PMT)
• A behavioral intervention for conduct problems in which parents are taught to modify their child’s behavior through consistent monitoring, clear rules, positive reinforcement of prosocial behavior, and noncoercive discipline.
multisystemic treatment (MST)
• An intensive, time‑limited treatment for severe conduct problems in adolescents that intervenes in multiple systems (family, peers, school, neighborhood), using family‑based and community‑based strategies to reduce delinquency and improve functioning.
personality (3)
• individual’s characteristic way of behaving, experiencing life, and of perceiving and interpreting themselves, other people, events, and situations
→ relatively stable over time and situations
→ affects cognition, emotion, behavior
The Big 5 (and their opposites)
• Neuroticism - Emotional stability
• Extraversion - Introversion
• Openness to Experience - Traditionalism
• Agreeableness - Antagonism
• Conscientiousness - Heedlessness
personality disorders
• Extreme, dysfunctional, and inflexible patterns of inner experience and behavior that deviate markedly from cultural expectations, are stable over time, and lead to distress or impairment.
→ typically ego-syntonous (vs. ego-dystonous)
General criteria for personality disorders (7)
enduring pattern of inner experience and behavior that deviates markedly from expectations of the individual’s culture, manifests on 2 or more of 4 domains:
• cognition
• affectivity
• interpersonal functioning
• impulse control
→ 3 Ps
→ not better explained by substance/somatic/other disorder
What are the 3 Ps and what do they mean?
→ pervasive: inflexible, in many different situations
→ persistent: stable, long term, start early adulthood
→ pathological: distress/dysfunction
polythetic criteria
• when there’s multiple diagnostic criteria, which don’t all have to be fulfilled (e.g. “shows at least 5 of following symptoms” when there’s 9 possible symptoms)
• leads to heterogenous clinical pictures, because some people may exhibit some symptoms that other’s don’t show, while they have other symptoms
How are PDs conceptualized in the DSM? (4)
• almost all disorders seem dimensional in nature
• but: threshold determined by decision/consensus → arbitrary
• PD-NOS one of most frequently used
• alternative model (AMPD) included as appendix for research in DSM 5 for more dimensional approach → ICD-11 fully switched to it
Clusters in personality disorders (3)
• Cluster A: “Odd, eccentric”
• Cluster B: “dramatic, emotional, erratic”
• Cluster C: “anxious, fearful”
Disorders in cluster A (3)
• paranoid PD (distrusting)
• schizotypal PD (strange perceptions + behavior)
• schizoid PD (distant)
Disorders in cluster B (4)
• histrionic PD (emotional, attention seeking)
• narcissistic PD (inflated ego)
• antisocial PD (violating other’s rights)
• borderline PD (instability of self image, relations, emotions)
Disorders in cluster C (3)
• avoidant PD (socially inferior)
• dependent PD (submissive, clinging)
• obsessive-compulsive PD (perfectionistic, controlling)
DSM Alternative Model (4)
• DSM AMPD: hybrid
• 5 dimensions (clinical version of big 5)
• 25 facets
• 7 categorical classifications retained
Epidemiology of personality disorders (4)
• general population: 9-13 % → mostly mild though
• outpatient care: 30-50%
• inpatient clinics: 50-70%
• prisons: 60-70%
Consequences of personality disorders (4)
• high disease burden
• high consumption of care
• low quality of life
• high societal costs
→ but treatable
Comorbidities of personality disorders (5)
• often other PDs: cluster B → antisocial + borderline, cluster C → dependent + avoidant, but also between clusters→ borderline + dependent
→ other syndromal disorders:
• avoidant + alcohol abuse
• OCPD + depression
• borderline + PTSD
• PD + anxiety/depression/addiction
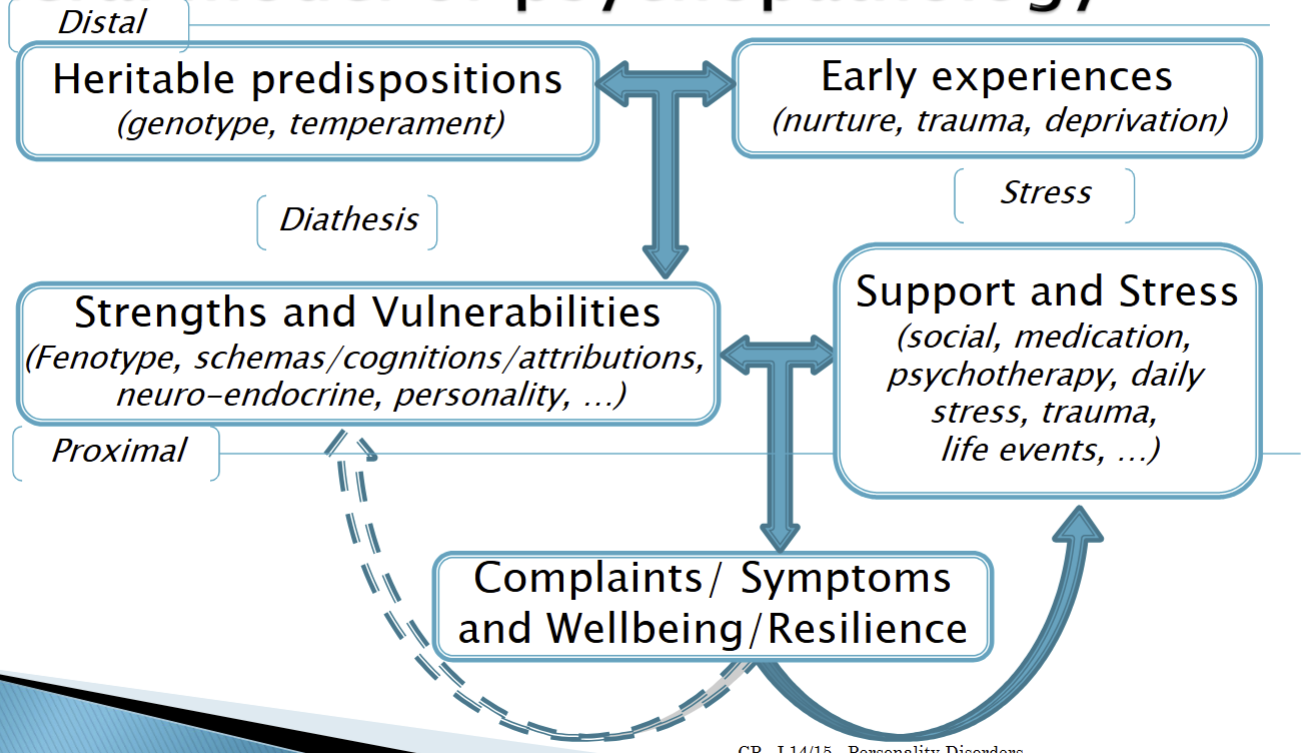
How is personality produced?
Early environmental factors as etiologies of personality disorders (5)
• abuse
• maltreatment
• aversive parental behavior
• lack of parental affection
• neglect
Biological factors as etiologies of PDs (3)
• genetic heritability → heritability estimates: ~0.35-0.7
• neurotransmitter systems
• brain areas
Neurotransmitter systems as etiologies of PDs (3)
→ dopamine (cognitive problems, cluster A)
→ serotonin (anger, impulse control)
→ mono-amine oxydase (MAO; aggression)
Brain areas as etiologies of PDs (2)
→ lack of frontal cortical control: impulses and emotions (mid brain)
→ dysfunction amygdala (hyper-emotionality; hypo-emotionality)
Psychological levels of description that may play role in PDs (3)
• attachment
• attributional style
• coping style
Process levels of description that may play role in PDs (4)
• cognitive biases (attention, interpretation, …)
• core assumptions/beliefs/schemas
• emotion regulation
• impulsivity
Biological levels of description that may play role in PDs (3)
endophenotypes:
• neural circuits: size, organization, connectivity
• neurotransmitter systems
• neuro-endocrine (e.g. HPA-axis tuning)
paranoid personality disorder
• A personality disorder characterized by pervasive distrust and suspiciousness of others, such that their motives are interpreted as malevolent.
schizoid personality disorder
• A personality disorder marked by detachment from social relationships and a restricted range of emotional expression in interpersonal settings.
histrionic personality disorder
• A personality disorder involving excessive emotionality and attention‑seeking behavior, including rapidly shifting emotions and a strong desire to be the center of attention.
dependent personality disorder
• A personality disorder characterized by an excessive need to be taken care of, leading to submissive and clinging behavior and fears of separation.
avoidant personality disorder
• A personality disorder marked by social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation, leading to avoidance of social situations despite a desire for close relationships.
obsessive-compulsive personality disorder
• A personality disorder characterized by a preoccupation with orderliness, perfectionism, and mental and interpersonal control, at the expense of flexibility, openness, and efficiency.
schizotypal personality disorder
• A personality disorder involving acute discomfort in close relationships, cognitive or perceptual distortions (e.g., odd beliefs, unusual perceptual experiences), and eccentric behaviors.
Etiology and prognosis of schizotypal PD (7)
• multi-genetic vulnerability
• biochemical deviations
• neurobiological deviation (endo-phenotypes)
→ but protective factors also play role!
• schizotypal traits, and/or
• psychotic decompensation: Psychotic disorders, Schizophrenia
• paranoid PD: most heterogenous group?
antisocial personality disorder (APD)
• A personality disorder defined by a pervasive pattern of disregard for and violation of the rights of others since age 15, including behaviors such as deceitfulness, impulsivity, irritability and aggression, irresponsible behavior, and lack of remorse; requires evidence of conduct disorder before age 15.
Psychopathic subgroup of antisocial PD (4)
• 15-25% of antisocial PD also psychopathic
• measure: Psychopathy Checklist-revised (PCL-R) → evaluation of interview by therapist + facts (file)
• Factor 1: Affect/Interpersonal → callous/unemotional, glib
• Factor 2: Behavior → antisocial/impulsive
psychopathy
• A construct related to antisocial personality disorder, emphasizing affective and interpersonal traits (e.g., lack of empathy or remorse, shallow affect, superficial charm) along with impulsive and antisocial behaviors.
triarchic model of psychopathy
• A model that conceptualizes psychopathy in terms of three core trait dimensions: boldness (social dominance and fearlessness), meanness (callousness and lack of empathy), and disinhibition (impulsivity and poor behavioral control).
borderline personality disorder (BPD)
• A personality disorder characterized by instability in interpersonal relationships, self‑image, and affect, along with marked impulsivity, recurrent self‑harm or suicidal behavior, intense anger, and frantic efforts to avoid abandonment.
Models that could explain PDs(3)
• learning/behavioral models
• cognitive models
• psychodynamic models
Learning/behavioral models (2)
• conditioning, modeling, contingencies
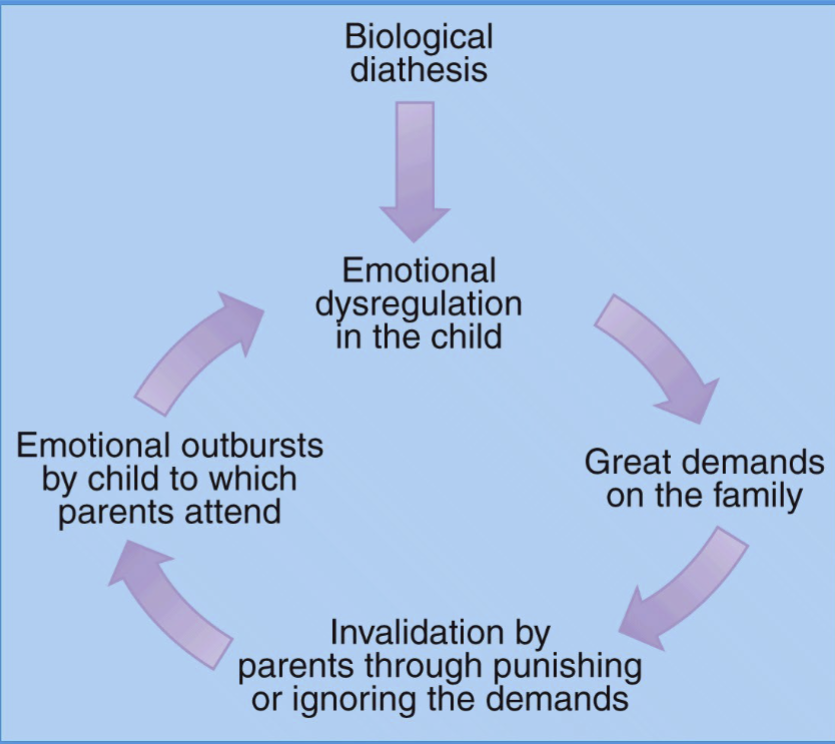
• Linehan: emotion-regulation
Cognitive models (2)
• Cognitive model (Beck)
• Maladaptive schema’s (Young)
Psychodynamic models (2)
• Mentalization
• Object-Relations (e.g. Kernberg)
Linehan’s emotional dysregulation model of BPD
Cognitive Model (Beck)
• schemas affect appraisal of ambiguous situation and thus influence thoughts + behavior
Schema theory (Young) (7)
• extension on Beck’s cognitive theory
• basic needs not met (e.g. safety, autonomy, boundaries, etc.)
→ “early maladaptive schemas”
• schemas useful/adaptive in past
• ~18 schemas proposed (e.g. abuse/mistrust, abandonment/instability)
• coping with schemas (e.g. submission, avoidance, overcompensation)
• coping results in multiple modes (e.g. vulnerable child, angry child, detached protector, demanding parent, healthy adult)
Mentalization
• understanding behavior of other (and yourself) in terms of their mental states
• hypothesis: mentalization is learned as primary caretakers mirror and name child’s emotions → if that doesn’t happen: PD
Object-relations
• internalized representation of self in relation to object (another person, men, etc.)
• in PD immature defence mechanisms (e.g. “splitting”: all good, all bad”)
narcissistic personality disorder
• A personality disorder marked by grandiosity, need for admiration, and lack of empathy, often accompanied by a sense of entitlement and exploitative behavior toward others.
personality trait domains
• In the DSM‑5‑TR alternative model for personality disorders, five broad dimensions (e.g., negative affectivity, detachment, antagonism, disinhibition, psychoticism) that capture major areas of maladaptive personality functioning.
personality trait facets
• In the alternative model for personality disorders, the more specific trait components (25 facets) that make up the broader personality trait domains (e.g., anxiousness, hostility, impulsivity).
Problems in treatment of PDs (3)
• life threatening behaviors
• therapy damaging behaviors
• motivation
Requirements for treatment (3)
• safety/safe environment → clear structure, attachment figure(s)
• incentive/invitation to revise coping → clear rationale
• possibility of new (positive experiences)
Treatment options for PDs (4)
• dialectical behavior therapy
• schema (focused) therapy
• mentalization based treatment (MBT)
• transference focused psychotherapy (TFP)
dialectical behavior therapy (DBT) (2)
• CBT treatment originally developed for BPD that emphasizes acceptance and change, teaching skills in emotion regulation, distress tolerance, interpersonal effectiveness, and mindfulness.
• stabilizes, works well in auto-mutilation
schema (focused) therapy (ST) (3)
• integrative in foundations: attachment theory, experiential therapy, cognitive therapy
• integrative in techniques: limited reparenting, imagery rescripting, chair dialogue
• wide scope, demanding of capacities
mentalization-based therapy (2)
• for BPD that aims to improve the person’s capacity to understand their own and others’ behavior in terms of underlying mental states (thoughts, feelings, intentions) → modelling, small steps
• simple, works well perhaps also for severe cases
transference-focused therapy (2)
• psychodynamic treatment for BPD that uses therapist–patient relationship (transference, object-relations) to help the patient understand and change maladaptive internal representations of self and others.
• drop-out might be higher