Glucose, kidneys, liver (wk 3/4)
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
What is Glucose
The primary source of energy for body cells, tissues, and the brain
We consume carbohydrates in our food
→ Carbs are broken down into glucose by enzymes
→ Glucose then diffuses into our cell following the concentration gradient
Is hydrophobic (repels water) -> cannot travel through membranes
Use transport proteins
SGLT transporters -> cotransport on ion of sodium and one molecule glucose
In intestine and kidneys
GLUT (2 and 4) transporters -> allow glucose to diffuse through
in muscles (GLUT4)
fat tissue (GLUT4)
liver (GLUT2)
Diffusion will reduce changes in blood glucose levels (BGLs)
Brain burns the most glucose in body
Tolerance range for BGLs
Regulation Needed for BOTH Storage & Release
Glucose diffusion alone doesn't provide enough control for level BGLs
Want BGLs to stay at ~5 millimolar
Regulation after a meal (fed state)
Think: rIse = Insulin, risE = bEta
• Insulin is a Protein Encoded by the INS Gene
• Only released when BGLs are too high
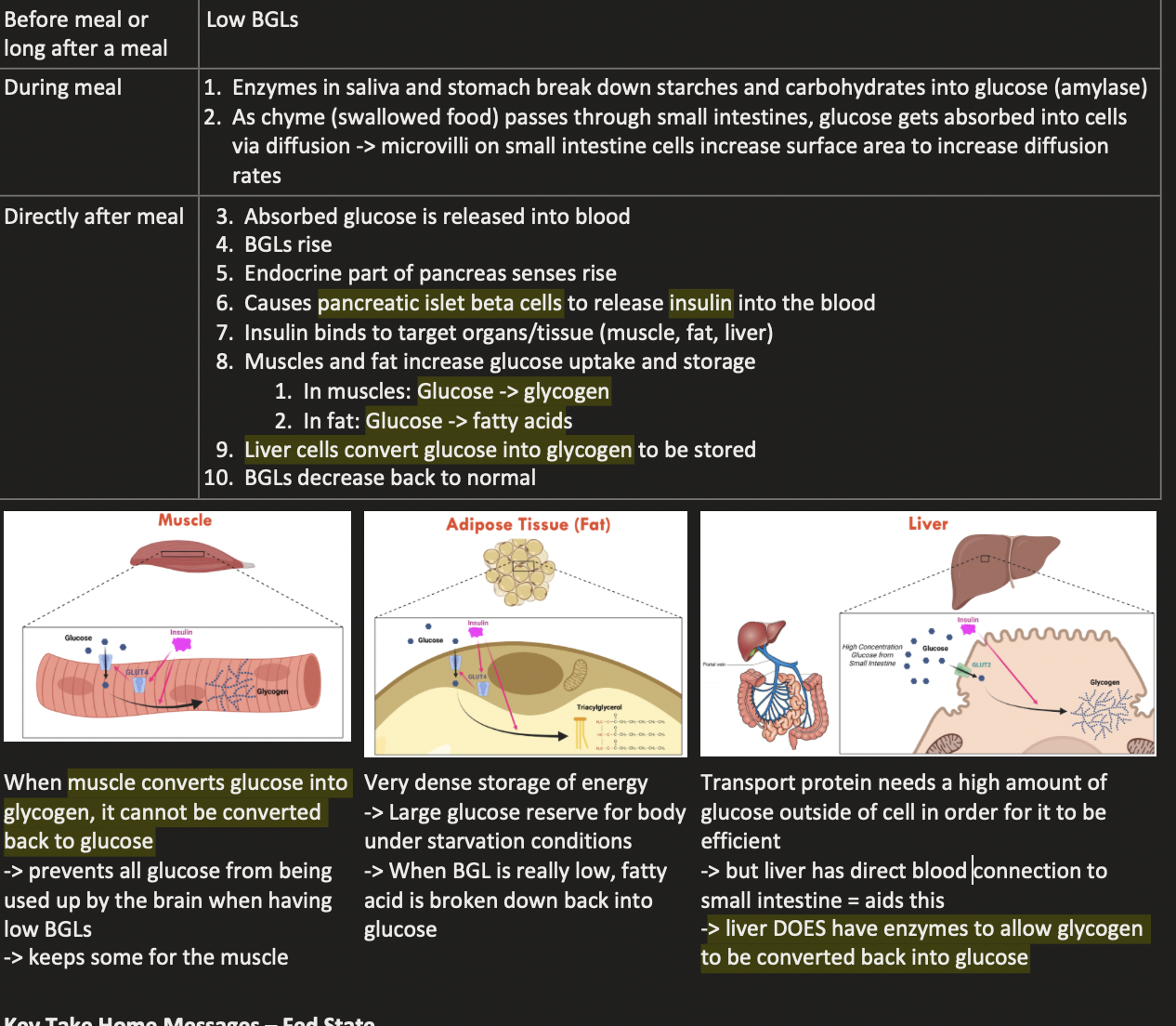
Key Take Home Messages – Fed State
Glucose is transported into cells by diffusion through glucose transporter proteins
Negative feedback loops -> keep BGLs close to ~5 mM
After a carbohydrate containing meal -> high BGLs -> stimulates insulin secretion into the blood from the beta cells of the pancreas
In muscle and fat cells: insulin -> stimulates glucose uptake into the cells (through GLUT4 protein) -> glucose converted into glycogen in muscles and into fatty acids in fat cells
In the liver: insulin -> lowers affinity glucose transporter GLUT2 at the cell surface & stimulates the storage of glucose as glycogen
Glucose uptake is facilitated by blood flow directly from the small intestine
Provides a very high glucose concentrations after a meal
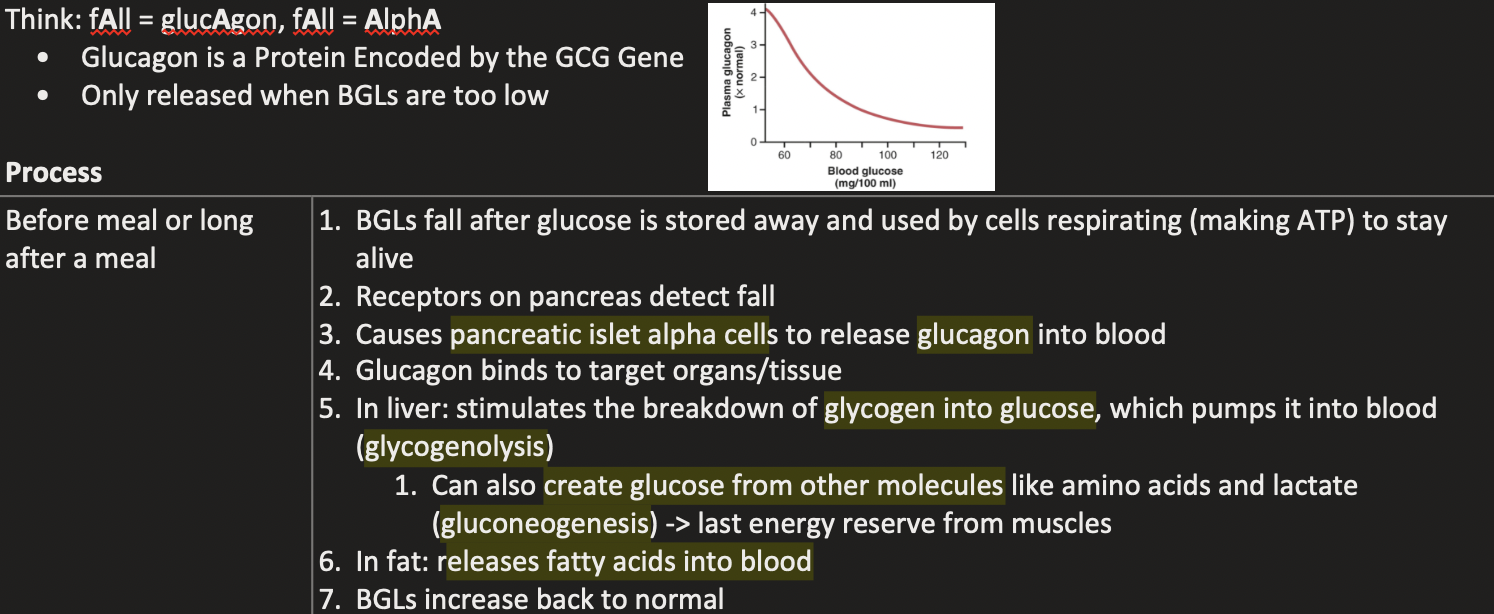
Regulation in the fasted state -> before the meal
Main Glucose Source Human First 24 h
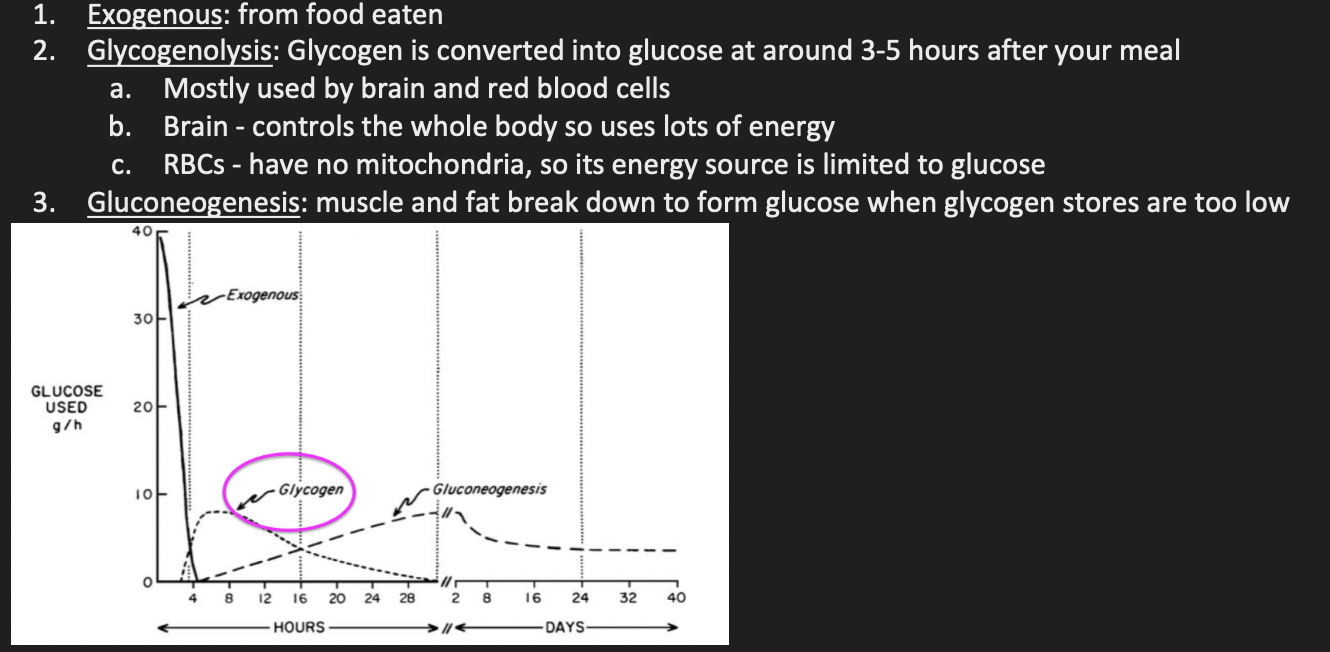
Key Take Home Messages – Fasted State
Low BGLs -> stimulate glucagon secretion from the alpha cells of the pancreas
In the liver
Glucagon -> stimulates glycogen breakdown (glycogenolysis) into glucose -> released into the blood ->maintain BGLs
Glucagon -> stimulates glucose synthesis (gluconeogenesis) from amino acids, glycerol and lactate -> released into the blood -> maintains BGLs
In fat cells: glucagon -> stimulates triglyceride breakdown (lipolysis) -> releases fatty acids and glycerol into the blood for use by the liver and other organs
function of pancreas
Endocrine
Alpha and beta islet cells secreting hormones
Regulates BGLs
Exocrine (most function of the pancreas)
To make enzymes for digestion
E.g. protease, lipases
Secrete them through their duct and it arrives in lumen of small intestines
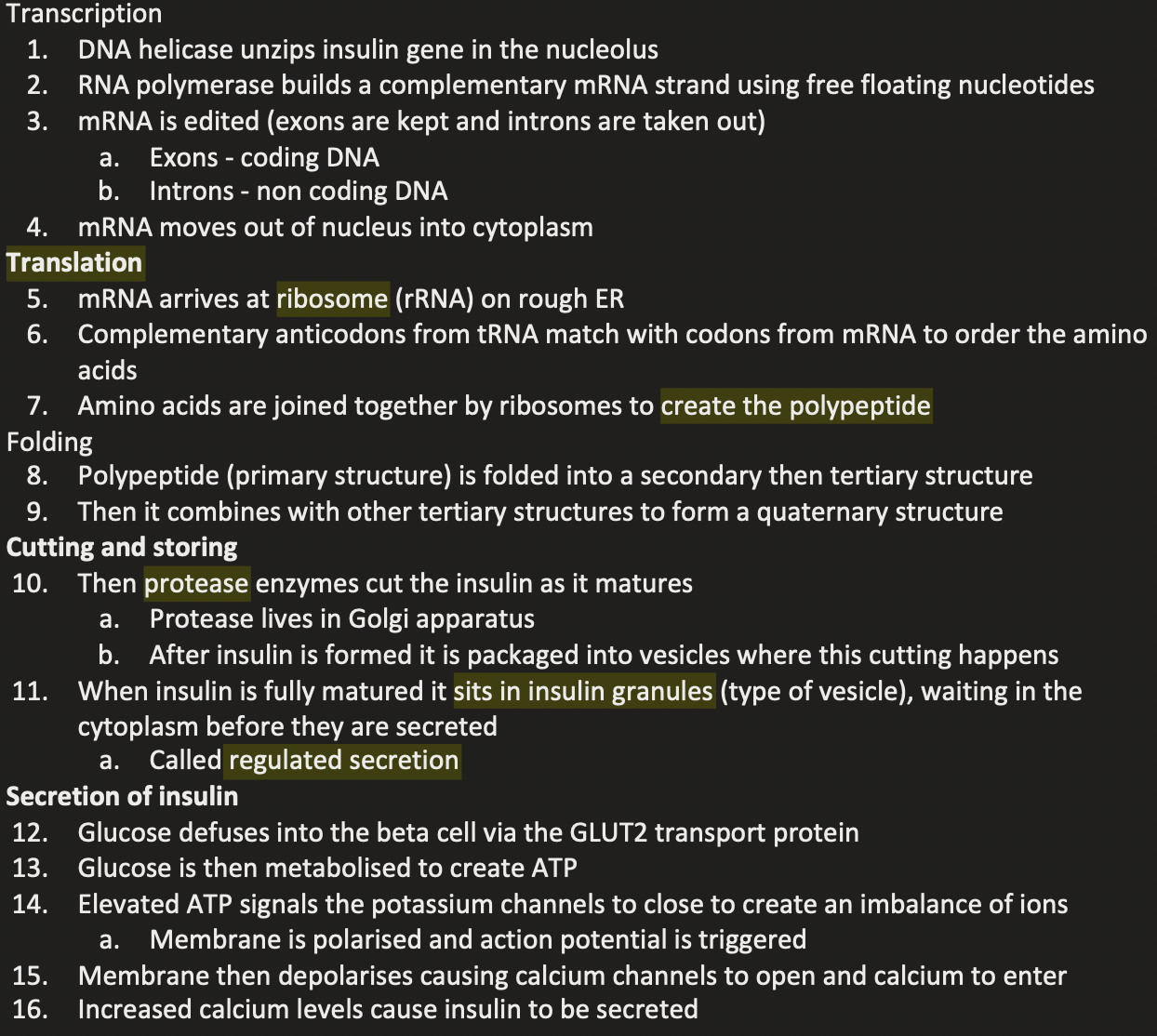
Making Insulin and secreting
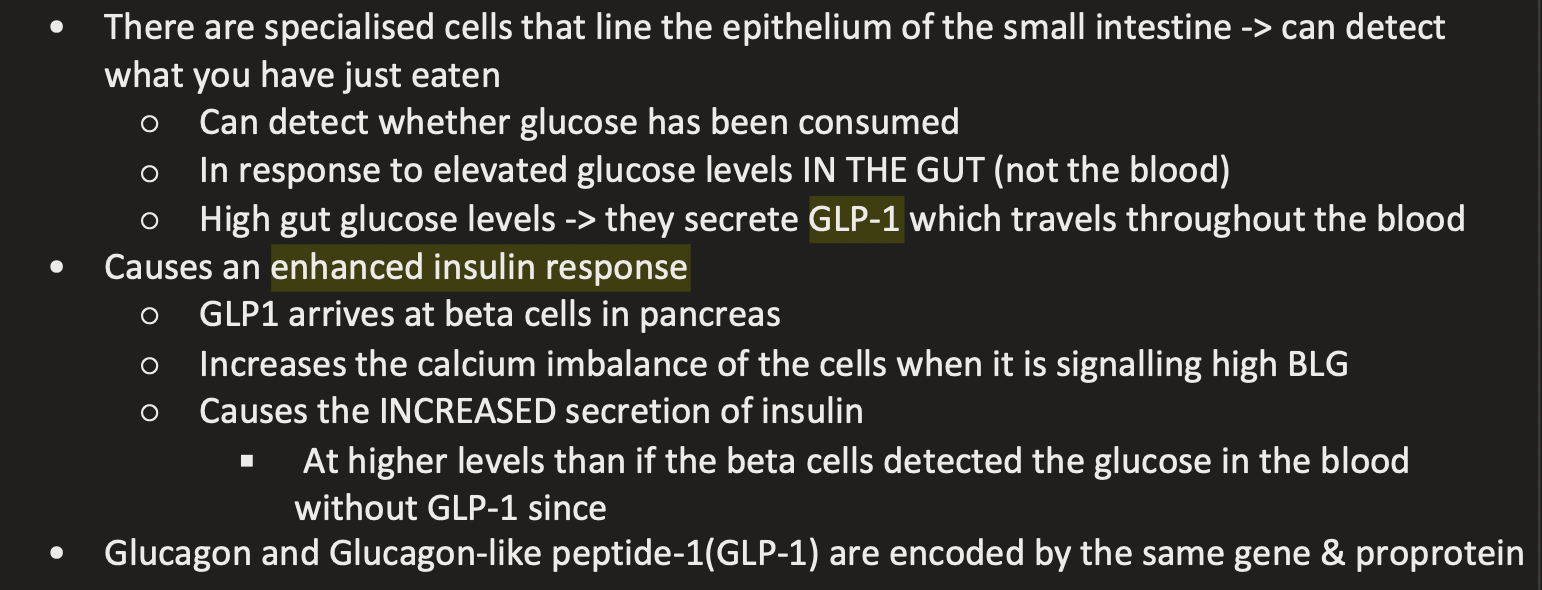
what is the Incretin Effect
• When we drink 100mL of glucose, insulin produced is higher than injecting 100mL of glucose directly into the blood (even though it spikes BGLs higher)
Due to another hormone called GLP-1
How GLP-1 works
Using GLP-1 in medicine
• We can synthesis GLP-1 and give it to people as a drug
• Ozempic contain chemically modified human GLP-1
Used to treat diabetes by stimulating insulin secretion
Key Take Home Messages – Insulin Secretion
Insulin is produced in cells
Regulated protein secretion starts with protein synthesis in the rough endoplasmic reticulum
Proteins are trafficked through Golgi
Pro-proteins (pre-matured insulin) is processed by proteases
Insulin is packaged into vesicles ready for a stimulus to trigger their secretion
High BLGS = beta cells secrete insulin into the blood
Via a multi-step mechanism
Receptors -> signal transduction -> signalling cascade -> second messenger molecules (calcium) -> response
Insulin secretion involves uptake in glucose via GLUT2 protein
Glucose metabolised into ATP
ATP-responsive potassium channels in the cell membrane cause membrane potential to change
Membrane depolarisation opens of calcium channels
Calcium levels increases in the cytoplasm
Triggers secretion of insulin.
Glucose taken orally stimulates secretion of GLP-1 into the blood by the small intestine
Co-stimulates the beta cells alongside glucose to maximise insulin secretion and subsequent glucose uptake in muscle and fat tissues
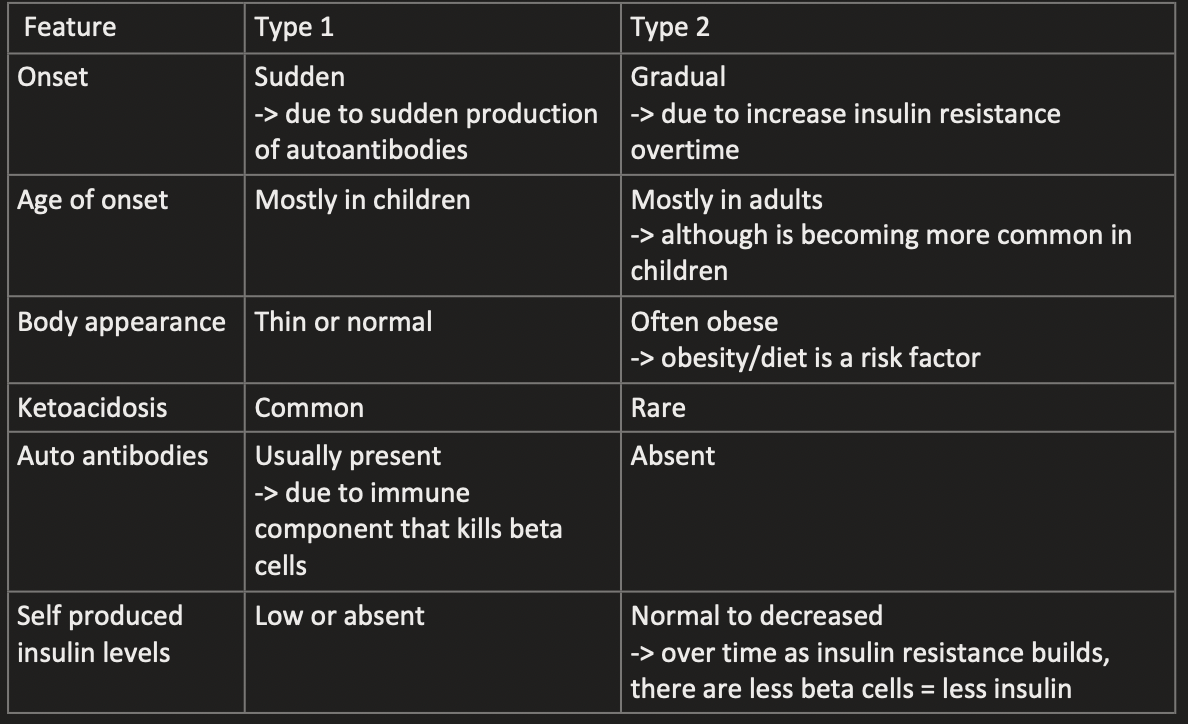
What is it type 1 diabetes
Is an autoimmune disease -> kills beta cells in the pancreas
Due to production of antibodies against beta cell specific proteins (e.g. insulin)
The immune system kills most or all of beta cells
○ Kill beta cells = lack or complete absence of insulin
Patients cannot store glucose in muscle or fat tissue
○ Lead to high BGLs if not controlled
○ Leads to high glucose in urination since there is no other way to get rid of glucose
Mostly first diagnosed in younger people
Environmental factors are strong contributors to getting this disease
With identical twins, only 20-30% both have type 1 diabetes
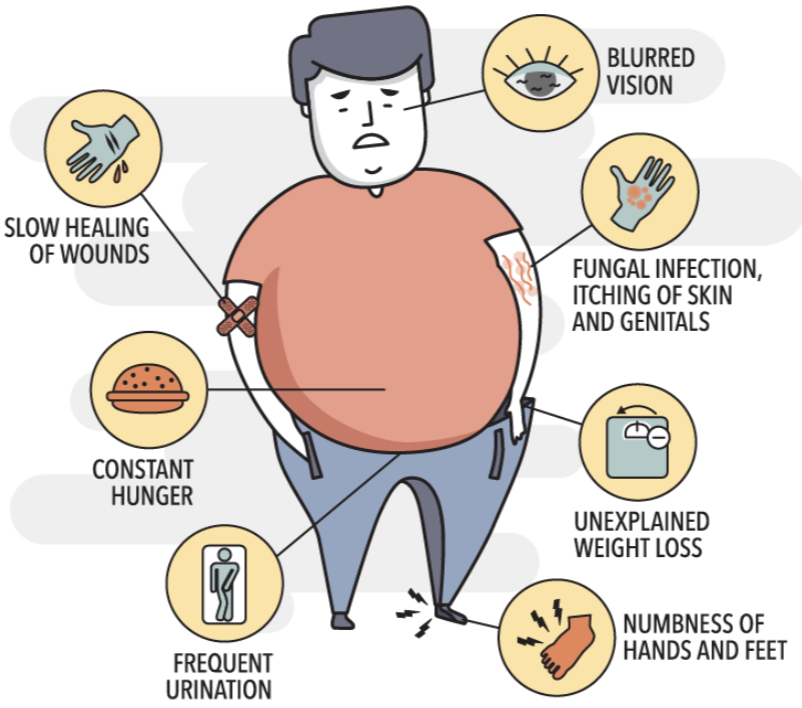
Symptoms of type 1 diabetes
• Frequent Urination: kidneys work overtime to excrete excess glucose.
• Excessive Thirst: Constant urination leads to dehydration
• Weight Loss: Without insulin, the body breaks down muscle and fat tissue, leading to weight loss
• Fatigue: Muscle cells are not receiving the glucose needed for energy, resulting in extreme lethargy
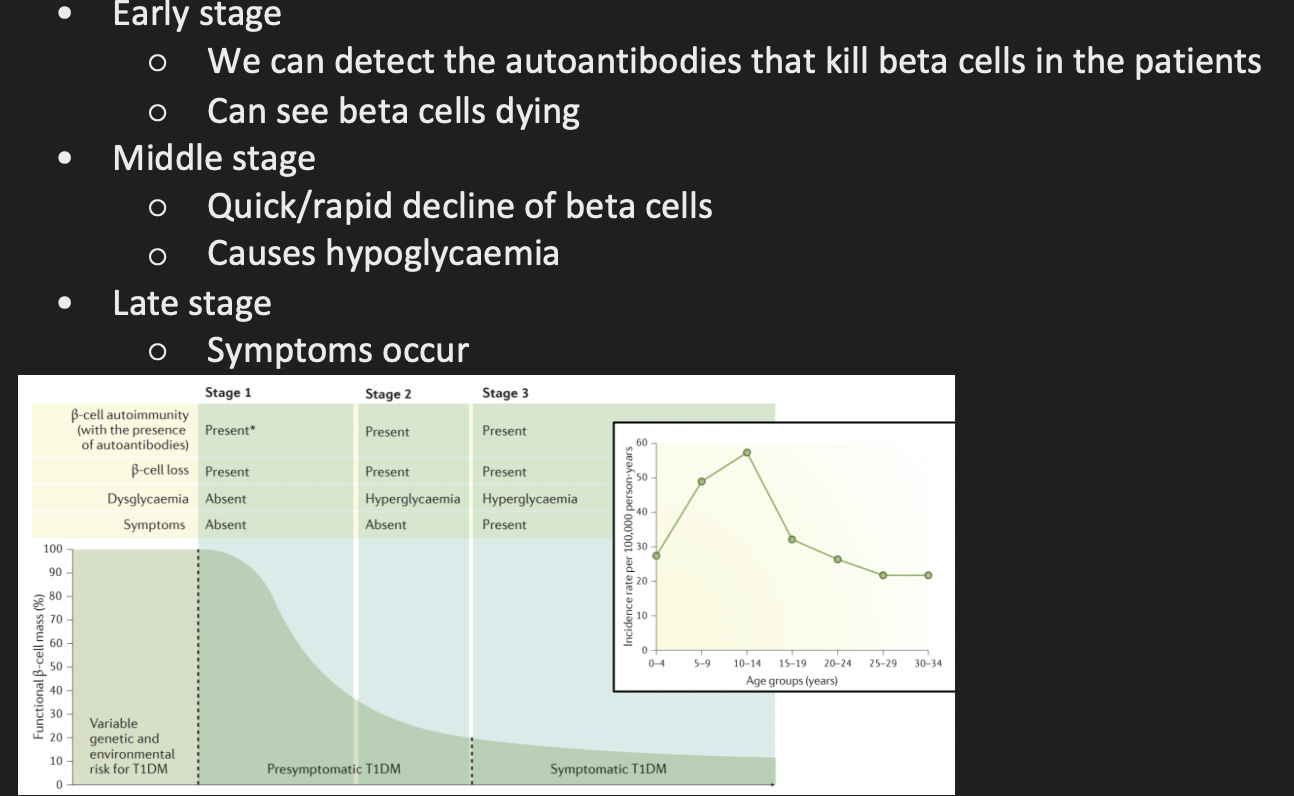
Progression of Type 1 Diabetes
Treatment for type 1 diabetes
Type II Diabetes symptoms
How it is developed: type 2 diabetes
Liver, muscle and adipose tissue becomes resistant to the effects of insulin
Signalling inside cell when insulin binds to receptor is not as effective
Cascade is not as great
Insulin resistance
Pancreas loses the capacity to secrete enough insulin in response to glucose
Beta cells have to increase amount of insulin they secrete to get the normal response of insulin
Challenging to produce all this extra insulin
Causes them to die -> could lead you to end up being like in type 1 diabetes
Type 1 vs Type 2 Diabetes