DBB: 18 - Theories of addiction: dependency models
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
why do people take drugs
experimentation
pleasure
medication
circumstance - e.g. WWII pilots staying awake
peer pressure
what are the 4 top positive reasons for alcohol use people describe
increase feeling of sociability
makes me feel euphoric
enables me to go along with friends
enables me to experience different states of consciousness
what are the top 6 negative reasons fro alcohol use people describe
relieves anxiety or tension
makes me less inhibited
makes me less inhibited sexually
enables me to stop worrying
alleviates depression
makes me less self-conscious
what are the two opposing views for alcohol use
disease model: addicts are victims of a chronic brain disease that leads to difficulty stopping
failure of choice/moral failure: addicts are people who choose drugs (over family, health) because they are selfish, weak, antisocial, irresponsible
give an example of why these might co-ocur as time goes on
idea that most people drink (but why) → but most people dont get addicted (so maybe its something outside of peoples control)
what is support for the disease model and how does it explain relapse rates
when you look at a healthy brain Vs diseased → there is decreased activity in diseased
ideas of relapse rates for drugs are similar to other diseases (asthma, diabetes) → same prognosis, hence addiction is a disease)
what is an opposing view on relapse rates for drugs
if you look at remission rates in wider population (like will get high relapse rates in people who received treatment and were administered)
in this case, remission is actually quite high (in all age groups)
drug dependence Vs average psychiatric disorders is a lot higher in comparison
what’s an example of drug use in soldiers in Vietnam
soldiers who went to Vietnam (where opioid use is high) many started taking them when deployed
most reported being addicted while out these
but when they come back most go into remission (but obviously addicted ones go into treatment)
what does this tell you about set and setting
how important it is for drug use
can’t just understand addiction from the drug alone - need the set and setting to get the whole complete picture
massive determinant
define addiction
a syndrome manifested by behavioural patten in which the use of a drug is given higher priority than other behaviour that once had higher value
at the extreme the dependence syndrome is associated with compulsive drug using behaviour
explain negative reinforcement models
drugs serve to increase the probability of further drug-seeking and drug-taking behaviour
because of their ability to alleviate unpleasant states
how does this apply to food - what is drive theory
food promotes food-seeking and eating as it alleviates aversive states if hunger
excitatory potential (sEr) = habit strength (sHr) X drive strength (D)
what is the self-medication hypothesis
drugs are used to self-medicate (relive symptoms that occur independently from drug use)
usually com orbit with psychiatric disorders
people who have a drug disorder/dependency → more likely to have mood disorder/anxiety
what is the physical dependent hypothesis
with the development of tolerance and physical dependence drug use is sustained in order to avoid the unpleasant consequence associated with withdrawal
what are distress syndrome reduction theories
people who continue to take drugs to ease ‘distress’ syndrome associated with cessation of drug use
perhaps due to adaptations in brain reward systems or opponent process
but withdrawal is typically transient
why was conditioned withdrawal model of drug addiction proposed - what does it explain
because many people (opioid addicts) report feelings if withdrawal when in therapy even after physical dependence has been gone for a while (as they’re talking about it)
explains why people who are in remission for months, years may still relate → because of the brain process involved in learning
what are the four basic tenets:
withdrawal produces aversive state
drug use rapidly relieves withdraw
withdrawal is ‘conditionable’, through Pavlovian conditioning, to internal and external cues
conditioned and unconditioned withdrawal act to stimulate drug-seeking behaviour
explain the seitan experiment on heroin
rats placed in 3 groups:
1: given morphine and withdrawal in same test environment
2: given morphine and withdrawal in home environment
3: no morphine given
found:
high response when expose to environment → not even when exposed to drug
don’t see withdrawal symptoms really at all when tested in new environment
how is environment important for drug use in relation to lethality
drug tolerance can be specific to particular context → taking the same amount in a new place is lethal (found with heroin use)
conditioning (CS) can evoke drug like or drug opposite effects
what’s a study that explains this
rats were give high doses of drug (alcohol, barbs, heroin)
rats who never had drug → high rate of death
dependent rats, but in a new place → less high rate but still high
dependent rats, but in same place → less high than both
explain the study with monkeys and morphine self-administration
nalorphine (antagonist) induce withdrawal in dependent subjects
trained with flashing light 10 minutes before nalorphine injection (US) and 30 minutes after
tested with flashing light (CS)
found:
large increase in morphine taking after nalophine injection and during 30 minutes following light
association of red light with precipitated withdrawal syndrome which enhances morphine taking
what aer some strengths for the conditioned withdrawal model
can account for (long-term) relapse
could apply to any drug which has a withdrawal syndrome
what are some weakness of the conditioned withdrawal model
cannot explain the maintenance of drug taking before physical dependence
not all drug cues trigger (physical) drug-opposite/withdrawal signs e.g. cocaine
no straightforward explanation why they’re is selective conditioning to withdrawal effects
define homeostasis
organisms maintain equilibrium in all systems, including brain reward systems, to function within appropriate limits of physiology
negative feedback = a process whereby the effects produced by an action serves to diminish or terminate that action
what is the opponent process model of addiction (conditioned opponent process model)
taking drugs to counteract negative effects (reach homeostasis - maintain balance)
drug gets you high → when it stops → give you the full drop/opposite effect → cycle
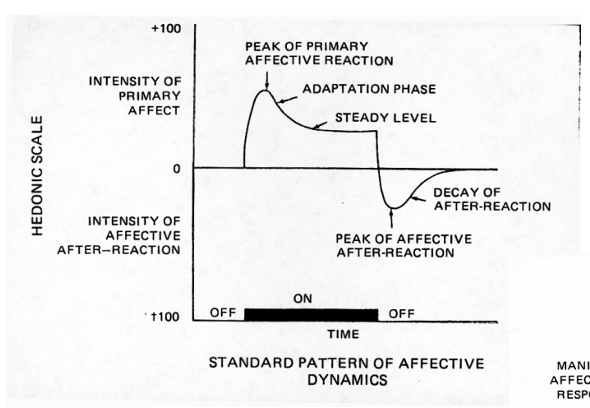
what is the homeostatic model of motivation
stimulus (drug) triggers A-process which in turn triggers a slave B-process (negative feedback) that is opposite to A to re-establish homeostasis
B is dependent on A → when A stops → B continues and overshoots (the low)
repeated stimulation makes B-process, but not A-process, grow
the A starts to draw out as B starts to overpower it
how can this process explain craving and relapse
drug seeking cues can trigger (small) A and (large) B states to induce drug craving and release
if cue is triggering A its also triggering B (aka the mini withdrawals people experience in remission)
explain the homeostatic dysregulation model based on this
neural system underlying A (reward) and B (anti-reward) process separate
B continuously grows in addiction resulting in lowered (allostatic) set-point and permanent anhedonic state → spiralling
progressively greater anhedonic/distress state ‘drives’ addict to seek and compulsively consume drugs
what are some neurological views on this
A-process = GABA, dopamine etc. going up
B-process = NPY (the stress response) which makes you go down, and gets bigger
what is the hypothesis that the B-process is the CRF system
increases are seen in extracellular CRF levels in the central amygdala during withdrawal from cocaine and ethanol
increase in heart rate, blood pressure, behavioural response to stressors etc.
what’s a study to support this
rats with a history of cocaine or alcohol taking require higher electric current for brain self-stimulation suggesting a state of anhedonia
more willing compared to controlled to give themselves brain shocks when in withdrawal → higher threshold in response to choking before responding (aka craving drug/sensation)
so turn up threshold to overcome the aversive effects of withdrawal
what are the 4 views of addiction from negative reinforcement
self-medication hypothesis: addicts take drugs to relieve (pre-existing) or medicate aversive state (e.g. co-morbidity)
conditioned withdrawal hypothesis: cues trigger physical or psychological ‘mini-withdrawals’ that lead to drug taking
conditioned opponent-process theory: aversive B-process
Allostasis theory of addiction: spiralling aversive state by change in ‘setting-point’
what are some weaknesses to these views
drugs of abuse vary dramatically in how much withdrawal they produce
while cues associated with opiate abuse produce drug-opposite reactions, this is not seen for other abused drugs
many opiate addicts deny feeling conditioned withdrawal, and those that do often deny that this provides relapse
there is a poor correlation between craving and the occurrence of withdrawal or conditioned withdrawal