Lecture 10: Collateral & Multiple Ligament Injury/Meniscal Injury
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
collateral ligament injury
complete or partial tear of medial or lateral collateral ligament
ligament injury =>
sprain!
1st, 2nd, 3rd degree sprains
1st = mild
2nd = moderate
3rd = complete
muscle tendon unit =>
strain!
no grading
most resolve with conservative management with rest
general considerations
medial and lateral collateral ligament function
limit varus-valgus motion of stifle joint
isolated medial or lateral collateral ligament tears rare in small animal
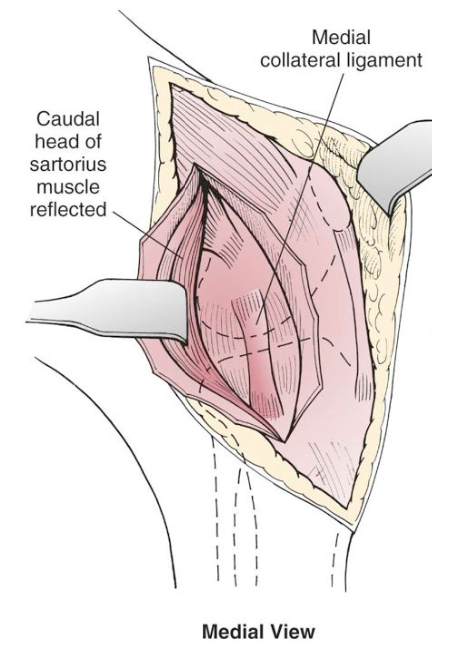
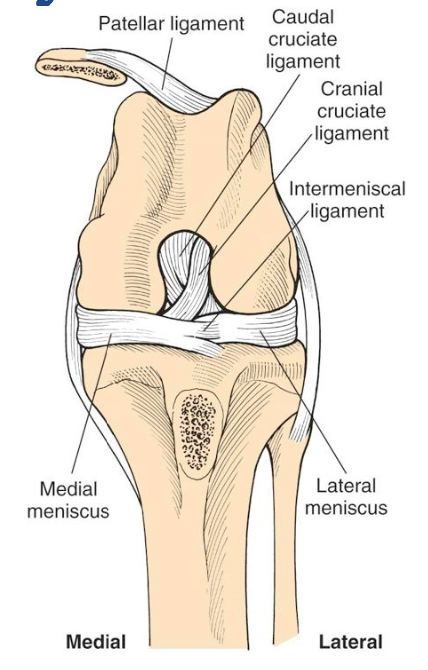
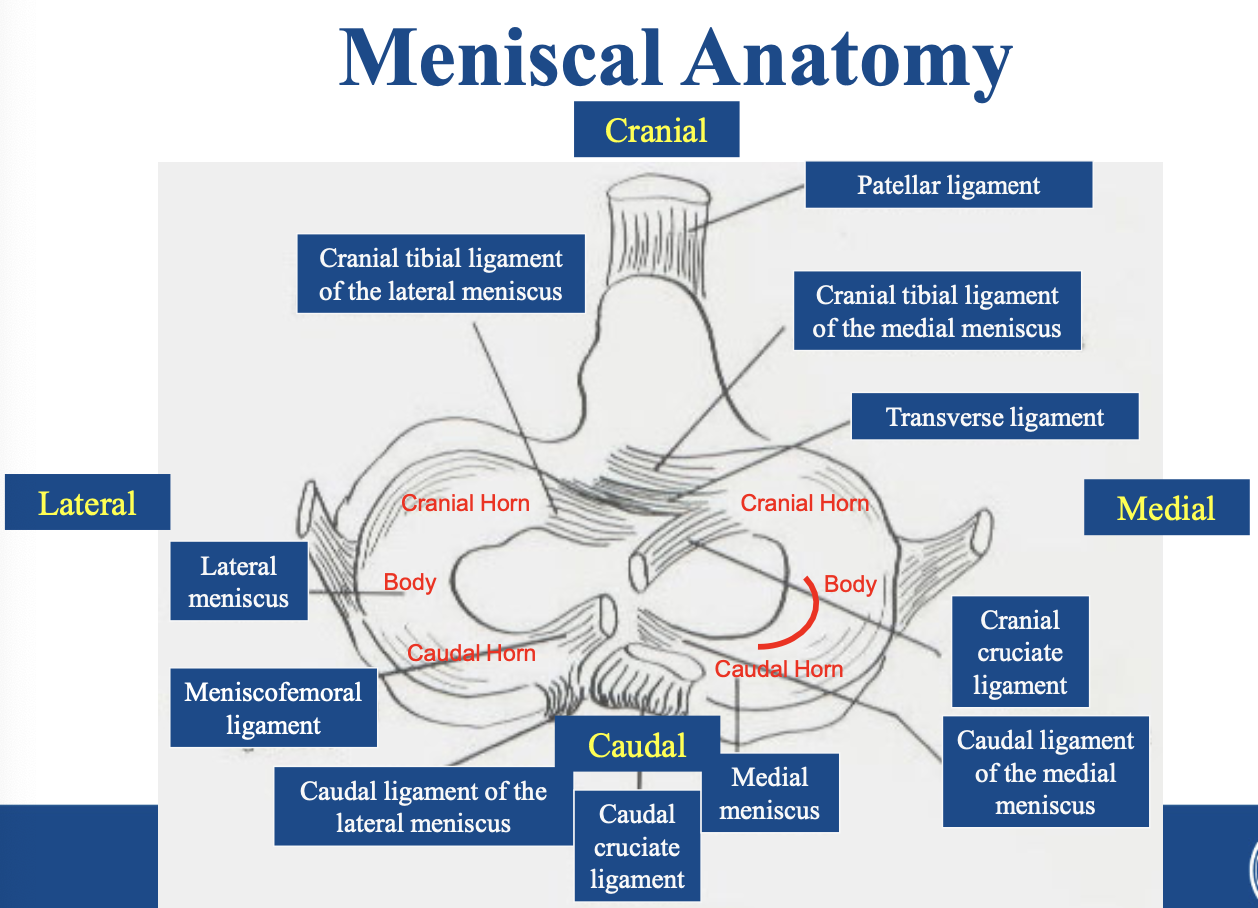
medial view anatomy
injuries to medial or lateral collateral ligaments:
occur with injury to other primary and secondary restraints of stifle joint
multiple ligament injuries result from:
severe trauma to stifle joint
involve injury to other stifle joint ligaments
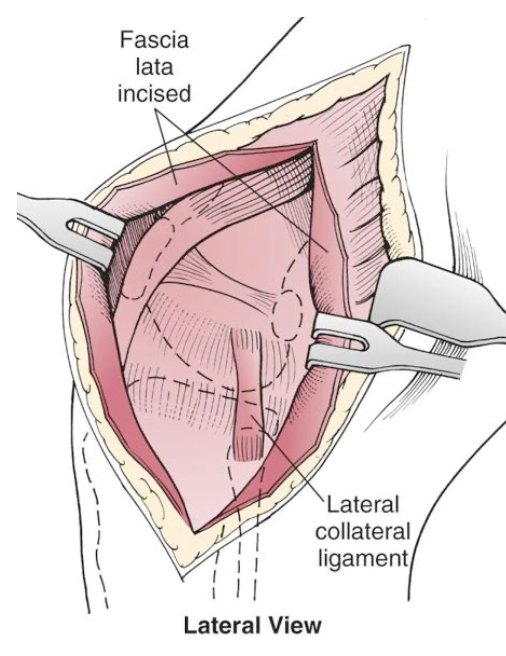
lateral view anatomy
signalment
dog or cat
any age or breed
either breed
hx of collateral and multiple ligament injury
may occur while exercising - w/o evidence of trauma
traumatic incident (vehicular accident) where animal has sustained major injuries
PE with collateral and multiple ligament injury
dx of collateral ligament injury
based on palpation
stifle joint extended to examine for collateral injury
cranial view anatomy
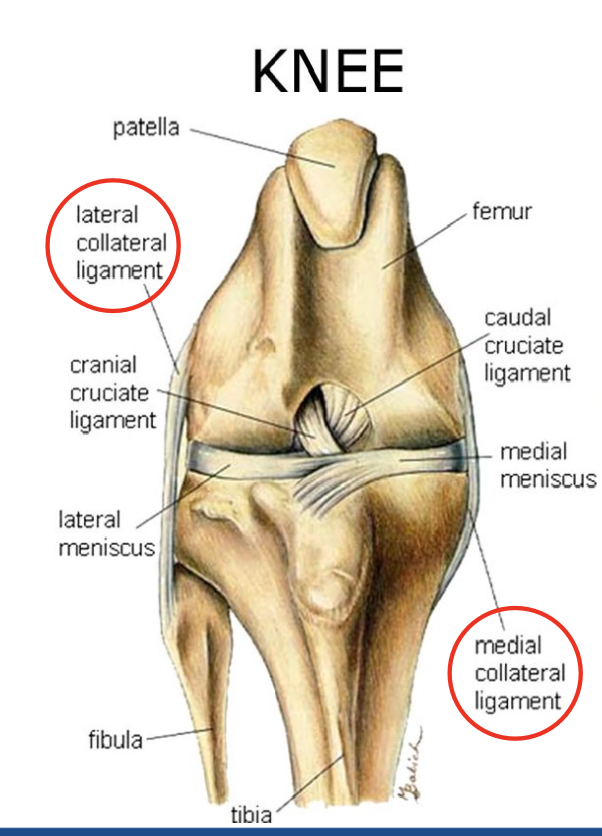
the valgus stress test evaluates the
medial collateral ligament
the varus stress test evaluates the
lateral collateral ligament
to examine the collateral ligaments:
apply medial and lateral pressure to tibia
assess integrity of collateral ligaments

how to perform the valgus stress test:
P in lateral recumbency
one hand stabilizes femur-other hand grasps distal tibia and applies upward force (abduction)
if medial joint restraints torn
see opening of medial joint line
medial collateral ligament (MCL), joint capsule, peripheral meniscal ligaments
how to perform the varus stress test
P in lateral recumbency
one hand stabilizes femur-other hand grasps distal tibia and applies inward force (adduction)
if lateral joint restraints are torn
see opening of lateral joint
lateral collateral ligament (LCL), joint capsule, peripheral meniscal ligaments
MCL tear

isolated tears show minimal opening
obvious opening occurs with more extensive injuries
radiographs for collateral and multiple ligament injuries
determines if bone fragments associated with ligament damage
craniocaudal and medial-lateral radiographs indicated: confirm presence or absence of bony avulsion
stress radiographs: show increase in medial or lateral joint space

note severity of joint opening
valgus stress applied to joint
stress radiograph of cat w/ MCL injury
laboratory findings:
consistent lab findings not seen
lab evaluation depends on signalment and physical findings in animals w/ trauma
diff. diagnosis
muscle strains
cranial or caudal cruciate ligament tears
nondisplaced physeal fractures in immature animals
medical management
conservative or surgical treatment for isolated collateral ligament injury based on degree of injury
collateral ligament itself
secondary joint restraints (joint capsule, peripheral meniscal ligaments)
assessment based on palpation and radiographs
criteria for medical management:
minimal swelling and only slight opening of joint space with stress test
indications for conservative treatment
1st degree sprain
fiberglass cast applied for 2 weeks
followed by controlled activity for 6 additional weeks
surgical treatment criteria:
moderate to severe swelling and significant opening of joint space with stress test
indicates greater injury to collateral restraints
2nd and 3rd degree sprains
treatment includes reconstruction:
collateral ligament(s)
meniscocapsular ligaments
joint capsule
be sure to repair all injured ligaments, tendons, and joint capsule
LITERALLY DON’T FORGET THIS BEAUTIFUL PEOPLE
primary repair of collateral ligaments done if:
point of failure is origin or insertion of ligament
an intrasubstance tear with large segments of ligament intact
occasionally small fragment of bone present on ligament
can be incorporated into repair
preoperative management
to prevent additional damage to articular cartilage or menisci:
place modified Robert Jones bandage on limb
Limit activity to leash walking
=> until surgery
animal evaluated for evidence of trauma to other ligaments or bones
preoperative management, P criteria:
Patients w/ injuries by HBC
thoracic, cardiovascular, and abdominal evaluation
perioperative antibiotics and and preemptive pain management
NSAIDS
Opioids
epidural analgesia
=> indicated for animals undergoing stifle reconstruction
surgical anatomy
medial collateral ligament
knowledge of origin and insertion points of collateral ligament is important
medial collateral ligament
originates from medial femoral epicondyle
runs distally to insert onto proximal tibial metaphysis
as ligament crosses medial joint line
strong attachment to joint capsule and medial meniscus
lies deep to caudal sartorius muscle
lateral collateral ligament
surgical anatomy
originates from oval area on lateral femoral epicondyle
runs distally to insert onto fibular head
lies deep to fascia late
careful when dissecting near lateral collateral ligament!
preserve peroneal (fibular) nerve!!!
peroneal (fibular) nerve
surgical anatomy
branch of sciatic nerve
obliquely crosses distal aspect of stifle joint
superficial to gastrocnemius muscle
sends articular branch to lateral collateral ligament
patient positioning for lateral collateral ligament injury
position patient in lateral recombancy with affected leg up
patient positioning for medial collateral ligament injuries
position animal in dorsal recumbency
patient positioning for multiple ligament tears
dorsal recumbency to facilitate exposure of both sides of limb
suspend limb and prepare for aseptic surgery
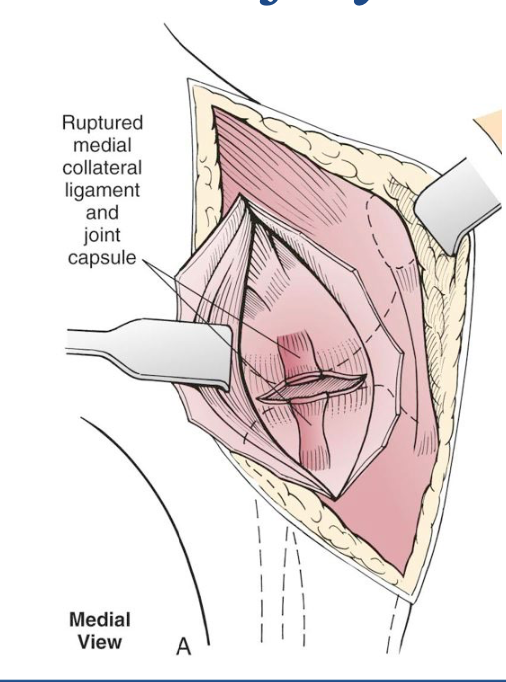
repair of a medial restraint injury
step 1:
incise insertion caudal head of sartorius muscle and deep fascia along craniomedial border of proximal tibia
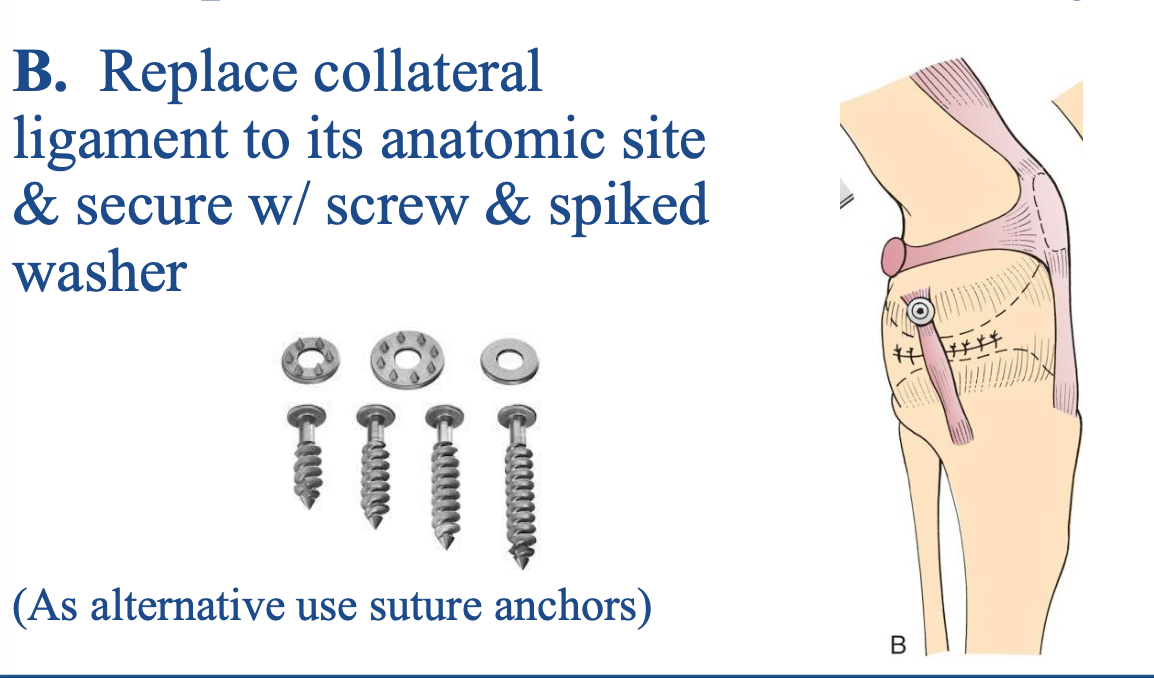
repair of a medial restraint injury
step 2:
replace collateral ligament to its anatomic site and secure with screw and spiked washer
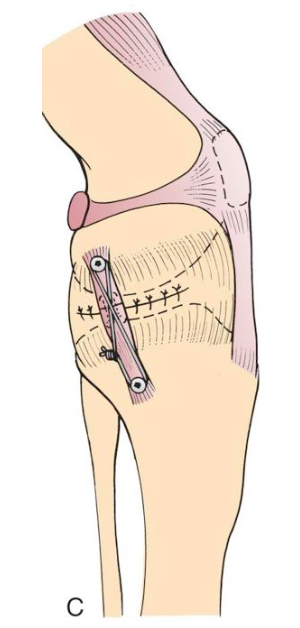
repair of medial restraint injury
step 3:
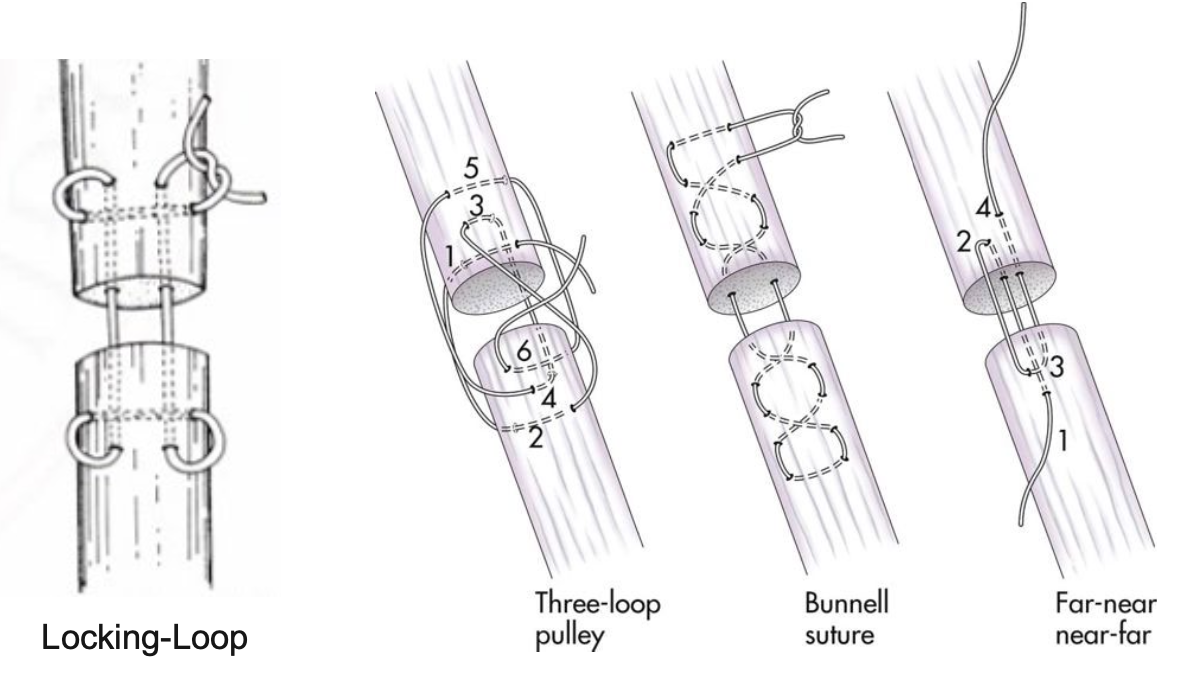
if ligament injury is intrasubstance tear:
primary repair by suturing ligament ends with locking-loop suture pattern
supplement primary repair with screws and figure-eight support
ligament and tendon sutures
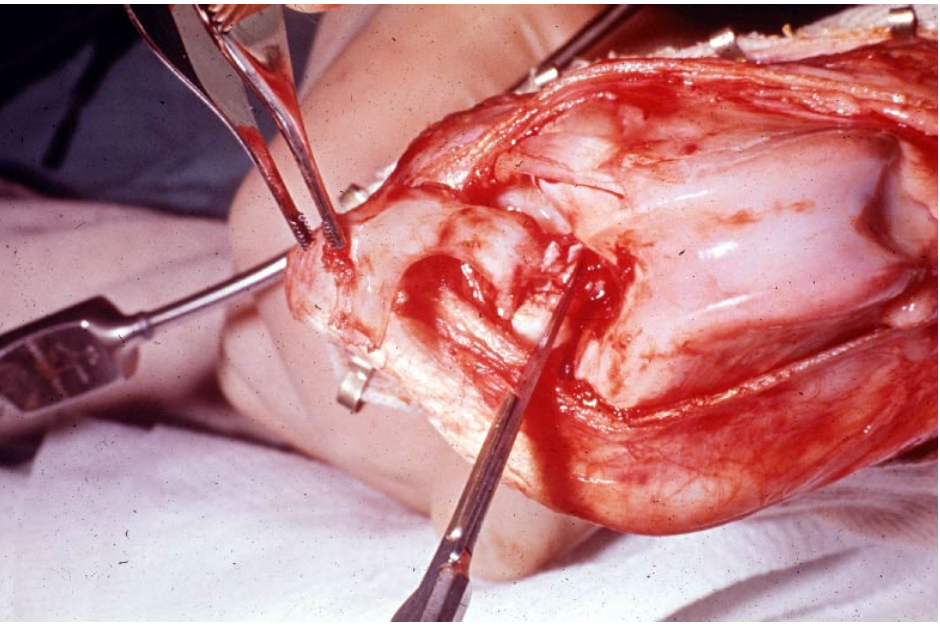
repair of a lateral restraint injury
craniolateral approach to expose lateral collateral ligament
make proximal-to-distal parapatellar incision through fascia lata
continue incision distally 4 cm below tibial crest parallel to joint line
use caution isolate and protect peroneal nerve
reflect fascia lata caudally
expose collateral ligament and lateral joint capsule
repair ligament as described for MCL
Prognosis of isolated collateral ligament tears is:
good to excellent
prognosis if multiple ligaments are torn prognosis is:
fair
multiple ligament injuries are:
injuries where cranial or caudal cruciate ligaments and collateral ligaments damaged simultaneously
caused by HBC or other major trauma
surgical anatomy for multiple ligament injuries
moderate to severe swelling and bruising of soft tissue surrounding joint seen
torn collateral ligaments difficult to identify because often encased in edematous connective tissue
menisci often displaced from normal positions and folded cranially or caudally
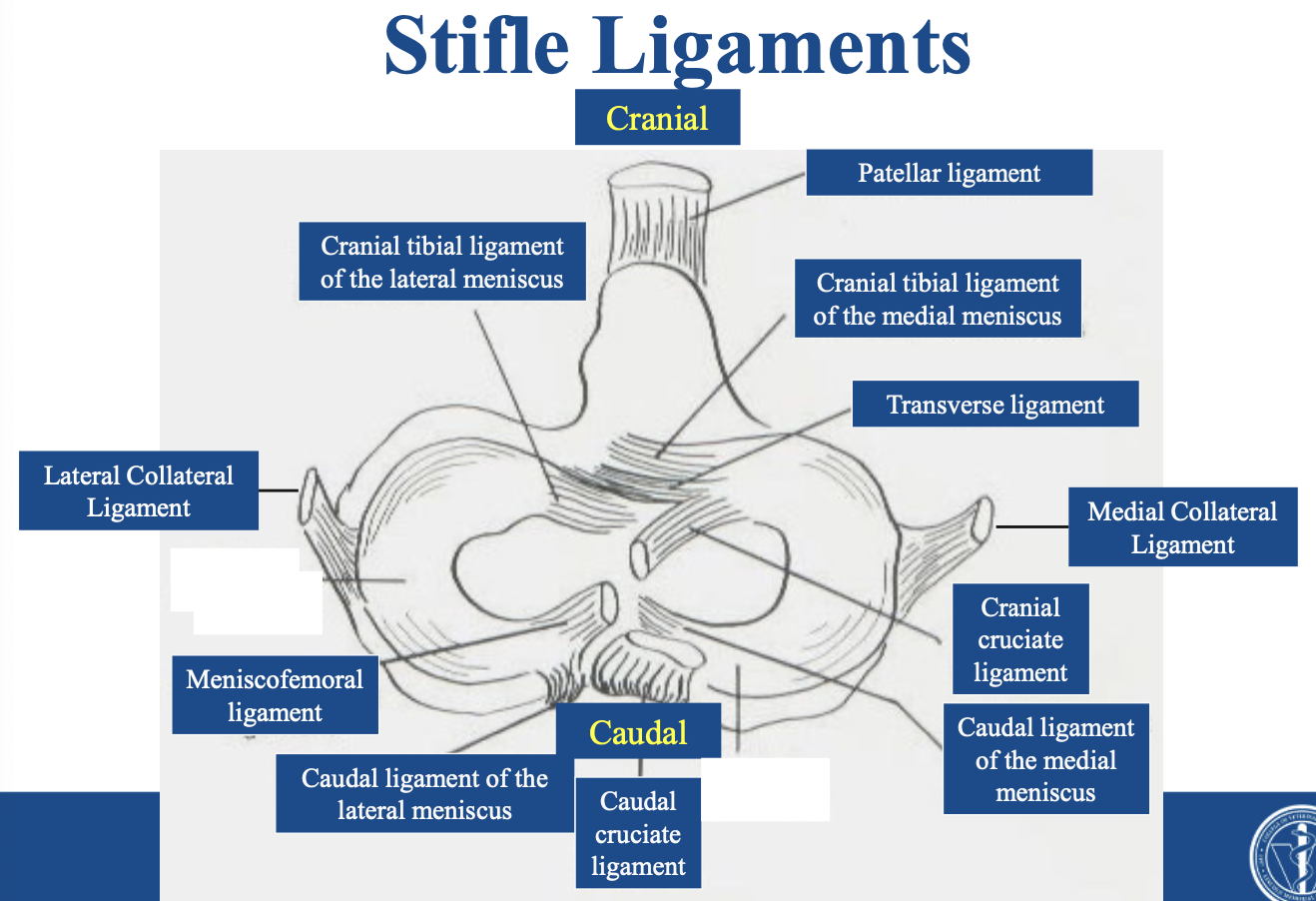
knowledge of normal origins and insertions of ligaments in joint required:
collateral ligaments
meniscocapsular ligaments
structures commonly injured with multiple ligament derangement of the stifle joint
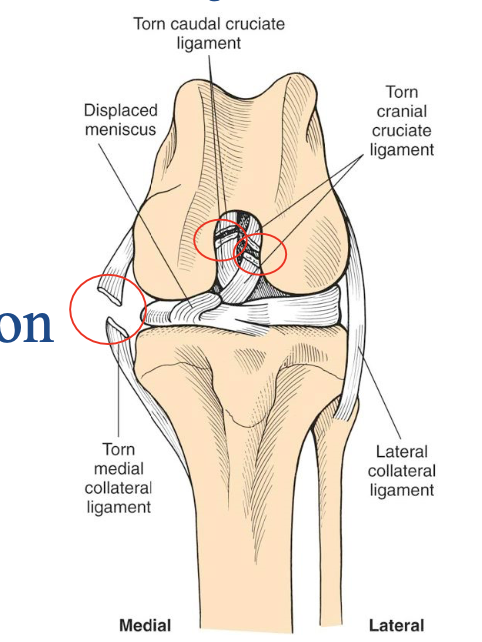
note loss of cranial and caudal cruciate ligaments and disruption of the medial restraints
multiple ligament injuries
common triad of injuries includes:
cranial and caudal cruciate ligament tears
failure of primary and secondary medial restraints
peripheral medial meniscal tears
prognosis is fair
deranged stifle
when there are multiple ligamentous injuries
often with meniscal injury
resulting in luxation of stifle joint
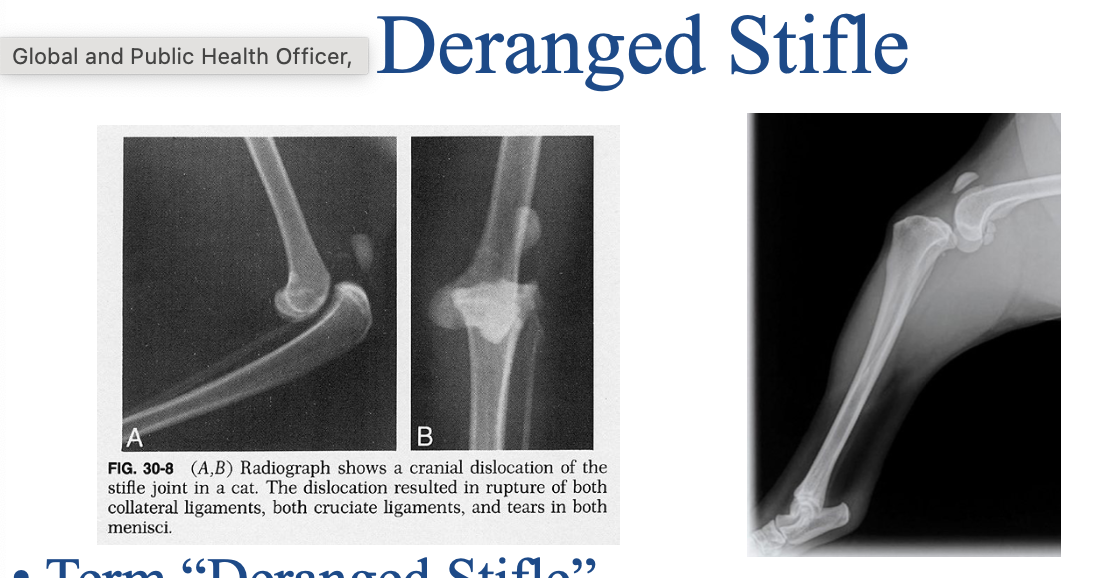
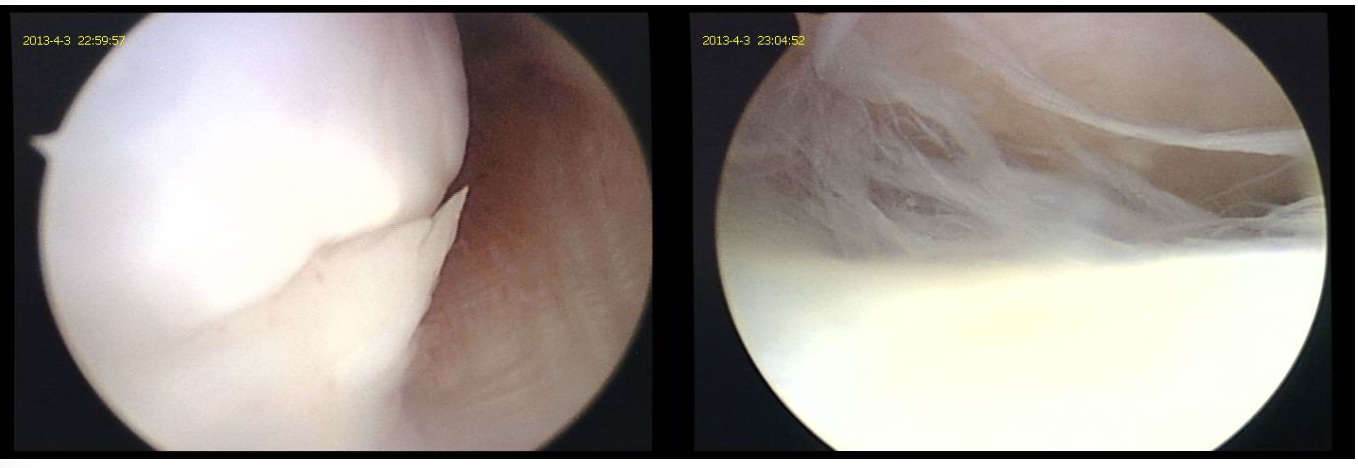
deranged stifle
FOR THE LOVE OF GOD, KNOW THIS IMAGE
meniscal tear image
meniscal release - locations:
A. transection of meniscotibial ligament
B. transection of midbody of meniscus
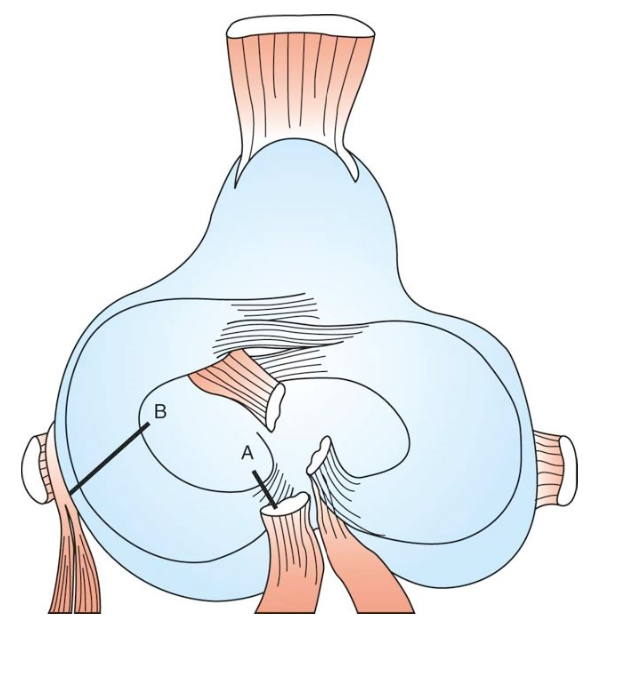
meniscal release
what does meniscal release mean:
“protecting” medial meniscus following surgical stabilization of stifle
developed in association with TPLO
meniscal release
controversial based on effects on meniscus and cartilage and uncertain efficacy
by transecting meniscus
function of meniscus is compromised by elimination of hoop stresses
with midbody meniscal release or transection of meniscotibial ligament:
femoral condyle increases contact with articular cartilage of tibial plateau
contributes to osteoarthritis
impairs functions of meniscus to provide stability and congruence
no clinical studies demonstrate efficacy of meniscal release in decreasing incidence of post TPLO meniscal injury; but technique remains in widespread use
medical management of meniscal injuries:
conservative treatment is not an option!
continued back-and-forth sliding of torn meniscus:
causes severe pain
will not improve with conservative management
accelerates DJD
conservative meniscal injuries tx
rest-plus or minus splint?
may be appropriate in stable joint

surgical treatment of meniscal injuries
1) partial meniscectomy
2) primary repair of peripheral meniscal injuries
3) total meniscectomy
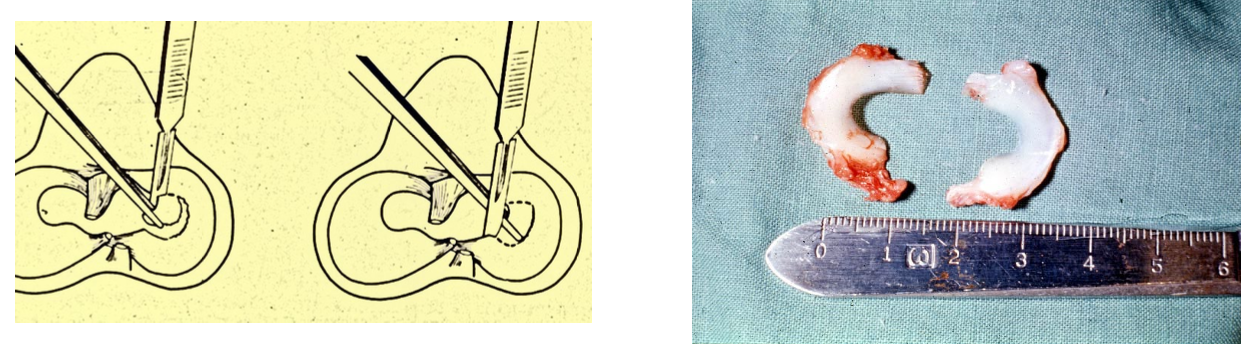
partial meniscectomy can be done by lateral approach:
removal of caudal horn
bucket handle tear excision
medial meniscectomy is easiest to perform through a medial surgical approach
partial meniscectomy:
removal of torn section of meniscus
experimentally: partial meniscectomy carries less morbidity than a total meniscectomy
treatment of choice for bucket handle tears of medial meniscus
primary repair of peripheral meniscal injuries
in human orthopedics: some surgeons advocate primary repair of torn meniscal body
in dogs: primary repair reserved for peripheral tears!
uncommon!
difficulty in suturing meniscal body tears in dogs
low morbidity associated with partial meniscectomy
repair with absorbable interrupted sutures
allowed meniscocapsular tissue to heal
challenging!
meniscal injuries treatment - general
damaged meniscus may not heal (likely not!)
total or partial removal may be indicated
total meniscal removal induces severe DJD in stifle!
total meniscectomy
when is a total meniscectomy indicated?
only when peripheral rim of meniscus is so damaged that primary suturing of meniscocapsular tissue is not possible
the more meniscal tissue removed the more rapidly OA develops