USMLE Step 1 Hematology
1/328
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
329 Terms
What transporter is found on Erythrocytes and what is the function?
HCO3-/Cl- antiporter
HCO3- leaves the RBC and Cl- moves into RBC (chloride shift)
Source of energy for RBC and how is it used?
GLUCOSE
- 90% in glycolysis
- 10% in HMP shunt
Platelets
a. Life span
b. Function
c. Where are they stored?
a. 8-10 days
b. Primary hemostasis (forms platelet plug by aggregating and sticking to fibrinogen)
c. Spleen (1/3 of them are there)
Granules of Platelets contain
Dense granules: ADP, Ca+2. TXA2
alpha granules: vWF, Fibrinogen
Thrombopoietin
a. Made where?
b. Function
a. Liver and kidney
b. Causes megakaryocytes to proliferate/differentiate and make platelets
vWF receptor on platelet
Gp Ib
Fibrinogen receptor on platelet
Gp IIb/IIIa
Thrombocytopenia results in ____.
Petechiae
Neutrophilic specific granules contain what?
ALP (alkaline phosphatase)
Lysozyme
Collagenase
Lactoferrin
Neutrophilic Lysosomes contain what?
Myeloperoxidase
Beta-glucuronidase
Acid phosphatase
Proteinases
Neutrophilic chemotactic agents
C5a
LTB4 (leukotriene)
IL-8
Platelet-activating Factor (PAF)
Kalikrein
Band Cells have decreased _____ receptors.
Fc receptors (CD16)
Hyper segmented PMNs are seen in ______.
B12/Folate deficiency
Increased band cells are seen in _____.
Myeloid proliferation
Causes of neutrophilia
- Leukocyte adhesion deficiency
- Corticosteroid use
- Acute bacterial infections
- Tissue necrosis
Agranulocytosis
a. What is it?
b. Etiology
c. S/S
a. Extremely low neutrophil count (near absent) w/ normal Hb and platelet count
b. (Agranulocytosis Certainly Causes Pretty Major Collapse To Defense Cells)
- Clozapine
- Colchicine
- Propythiouracil
- Methimazole
- Chloramphenicol
- Ticlopidine
- Dapsone
- Carbamazepine
c.
- Necrotizing ulcers in mouth and throat
- Increased risk of life-threatening infections
Inherited Neutrophil Abnormalities
- Leukocyte adhesion deficiency
- Chronic Granulomatous Disease
- Myeloperoxidase Deficiency
- Chediak-Higashi Syndrome
Function of Eosinophils
- Defend against helminthic infections by secreting Major Basic protein (helminthotoxin)
- Regulates immediate type hypersensitivity reactions by releasing histaminase to inactivate histamine and leukotrienes
Causes of Eosinophilia
(NAACP)
- Neoplasia (hodgkin lymphoma due to increased IL-5)
- Allergies/Asthma
- Addison's Disease, Athero-embolic Disease
- Chronic adrenal insufficiency, Collagen Vascular Disease
- Parasites (invasive)
Function of Basophils
Mediate allergic reactions
What do Basophils secrete?
- Histamine (in granules)
- Heparin (in granules)
- Leukotrienes (synthesize on demand)
Causes of Basophilia
- CML ****
- Hypersensitivity reactions
Types of Lymphocytes
B cells
T cells
NK cells
What do lymphocytes produce?
Hematopoietic growth factors
Causes of lymphocytosis other than cancer.
- Viral infections (CD8 T cells)
- Bacterial infections (esp pertussis)
B cells differentiate into what?
Plasma cells
Memory cells
B cells antigen-present via MHC ___.
II
B cells originate in the _____ and mature in the ____.
Bone marrow
Bone marrow
B cells, after maturation, migrate to...
- Cortex of Lymph node follicles
- Spleen (white pulp)
- Unencapsulated lymphoid tissue
What surface markers do B-cells express?
CD 19
CD 20
CD 21
What organelles are well-developed in plasma cells?
RER
Golgi apparatus
What is the name for the cancer of plasma cells?
Multiple Myeloma
T cells originate in the _____ and mature in the ____.
Bone marrow
Thymus
What surface marker do all T-cells express?
CD3
What co-signal is necessary for T-cell activation
CD28
T cells, after maturation, migrate to...
- Paracortex in lymph node follicles
- Periarterial sheath in spleen
Monocytes on peripheral blood smear look like what?
Large kidney-shaped nucleus
Macrophages antigen-present via MHC ___.
II
Macrophages are activated by..
Gamma-interferon
_____ from bacterial LPS binds to _____ on macrophages to initiate ______.
Lipid A
CD14
Septic shock
Mast cells mediate ....
Allergic reactions
Mast cells bind _______ which causes ________ leading to the release of ____.
1. IgE
2. Degranulation
3.
- Histamine
- Heparin
- Eosinophil Chemotactic factors
Mast cells contain ________ (eosinophilic/basophilic) granules and originate from _____.
Basophilic
Same precursor as basophils
________ prevents mast cell degranulation.
Cromolyn Sodium
Dendritic cells antigen-present via MHC ___.
II
_____ are a link between the innate and adaptive immune systems.
Dendritic cells
Dendritic cells are called _____ in the skin.
Langerhans Cells
_____ antibodies are made in ABO classification. ____ are made in Rh classification
1. IgM
2. IgG
A Blood
a. Group antigens on RBC surface
b. Antibodies in plasma
c. What will cause hemolytic reaction in these patients
a. A
b. Anti-B (IgM)
c. B blood, AB blood
B Blood
a. Group antigens on RBC surface
b. Antibodies in plasma
c. What will cause hemolytic reaction in these patients
a. B
b. anti-A (IgM)
c. A blood, AB blood
AB Blood
a. Group antigens on RBC surface
b. Antibodies in plasma
c. What will cause hemolytic reaction in these patients
a. A and B
b. NONE
c. Nothing
O Blood
a. Group antigens on RBC surface
b. Antibodies in plasma
c. What will cause hemolytic reaction in these patients
a. NONE
b. Anti-B, Anti-A
c. All blood types other than O
_______ is considered universal donor blood.
O blood
_______ is considered universal recipient patients for blood
AB patients
_______ is considered universal donor of plasma.
AB patients plasma
_______ is considered universal recipient patients for plasma.
O blood patients
______ crosses the placenta. _______ doesn't cross the placenta.
IgG crosses
IgM doesn't
Rh(+) Blood
a. Group antigens on RBC surface
b. Antibodies in plasma
c. Clinical Relevance
a. Rh (D)
b. None
c. No issues
Rh (-) Blood
a. Group antigens on RBC surface
b. Antibodies in plasma
c. Clinical Relevance
a. None
b. Anti-D (IgG)
c. If mother is exposed to Rh(+) fetal blood during delivery, her body will start making Anti-D IgG which will result in hemolytic disease of newborn if her next pregnancy is w/ an Rh+ fetus. To prevent this formation of Anti-D IgG, mom is given Rh(D) immunoglobulin that can bind the fetal blood from first pregnancy before her body makes Anti-IgD
In Hemolytic Disease of Newborn, What happens?
Mom's Anti-D IgG crosses the placenta and "attacks" fetus in utero
Prevention of Hemolytic Disease of Newborn?
Administer RhoGAM to Rh (-) pregnant women during 3rd trimester/after each pregnancy to prevent anti-Rh IgG formation
- RhoGAM is a anti-D IgG
Primary Hemostasis
a. What is it?
b. What initiates it?
c. What are the components?
a. Platelet plug formation (weak) at site of injury
b. Vascular injury (exposure of collagen, basement membrane)
c.
- Since blood vessel is anti-coagulant surface, any disruption is possible for clot formation
- Platelets form a plug at injured site
vWF
a. Function
b. Produced by?
a. Acts as a linker molecule for platelets to bind to during plug formation
b.
- Alpha granules of platelets
- Weibel-Palade bodies of endothelial cells
Weibel-Palade bodies of endothelial cells contain what?
- vWF
- P-Selectin
Endothelin
Released by damaged endothelial cells
- Causes vasoconstriction
ADP
a. Function
b. Produced by?
a. Binds platelets and increases platelet expression of Gp IIb/IIIa
b. In granules in platelets
Gp IIb/IIIa
Platelet receptor that binds fibrinogen which is necessary for platelet aggregation
Steps of Plug Formation
1. Injury to endothelium causes transient vasoconstriction mediated by Endothelinand neural stimulation reflex
2. vWF binds to exposed sub endothelial collagen
3. Platelet binds to vWF via Gp Ib and undergoes conformational change and degranulation releasing ADP, Ca+2, TXA2
4. ADP binds Platelet, increases Gp IIb/IIIa expression
5. Fibrinogen binds Gp IIb/IIIa and links platelets for aggregation
Aggregation is mediated by ______ resulting in _____ blood flow.
TXA2
decreased
Anti-Aggregation is mediated by ______ resulting in _____ blood flow.
NO and PGI2
Increased
Secondary Hemostasis
a. Initiated by
b. Function
a. Activated platelets
b. Produce fibrin to stabilize platelet plug (fibrin can be cross linked)
Coagulation Factors
Produced in liver in an inactivated state
What activates coagulation factors?
Ca+2
Phospholipid surface (platelet)
Hageman Factor
Coagulation factor activated by sub endothelial collagen
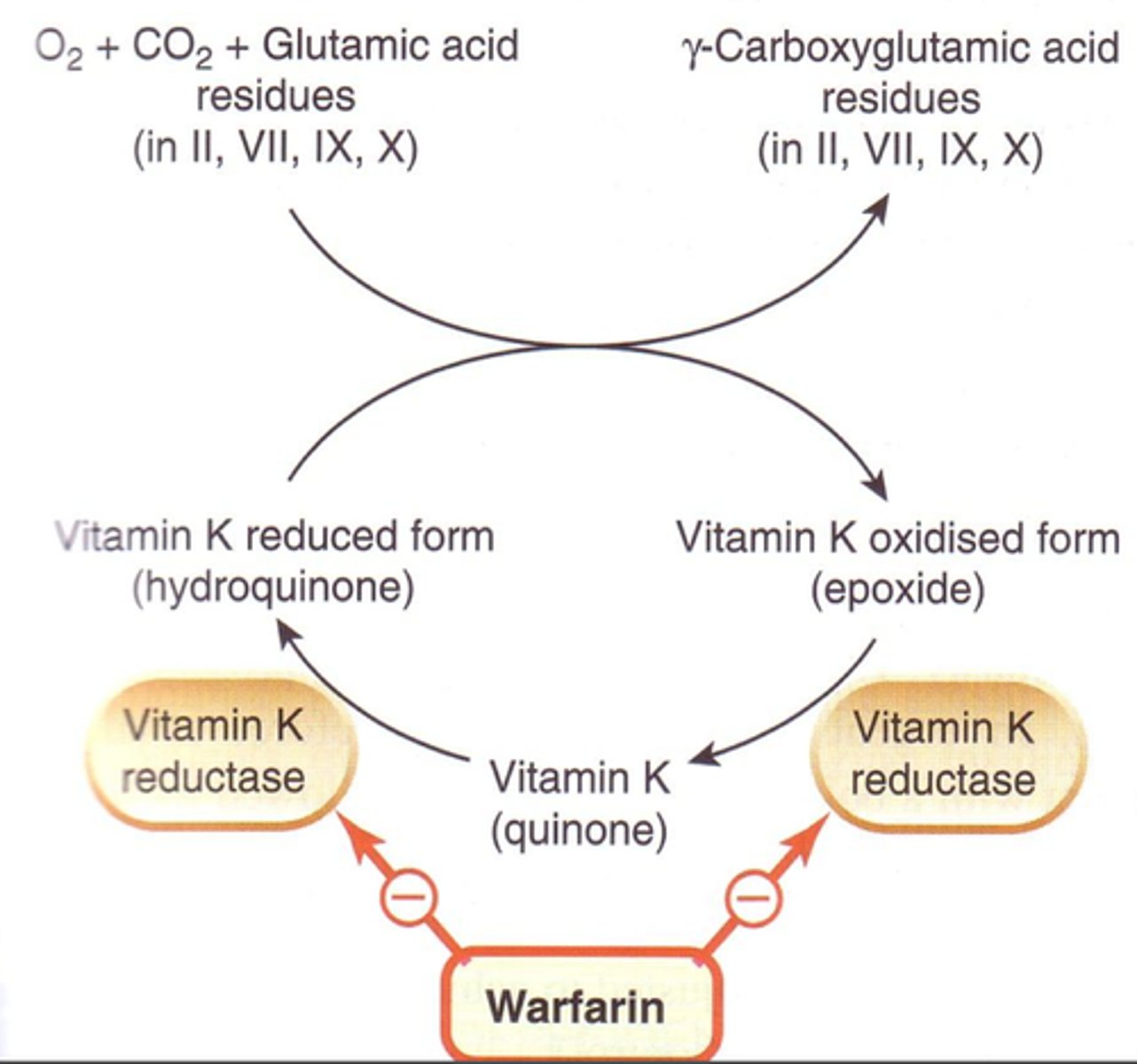
Vitamin K Dependent Factors
2, 7, 9, 10
Protein C
Protein S
Coagulation Cascade
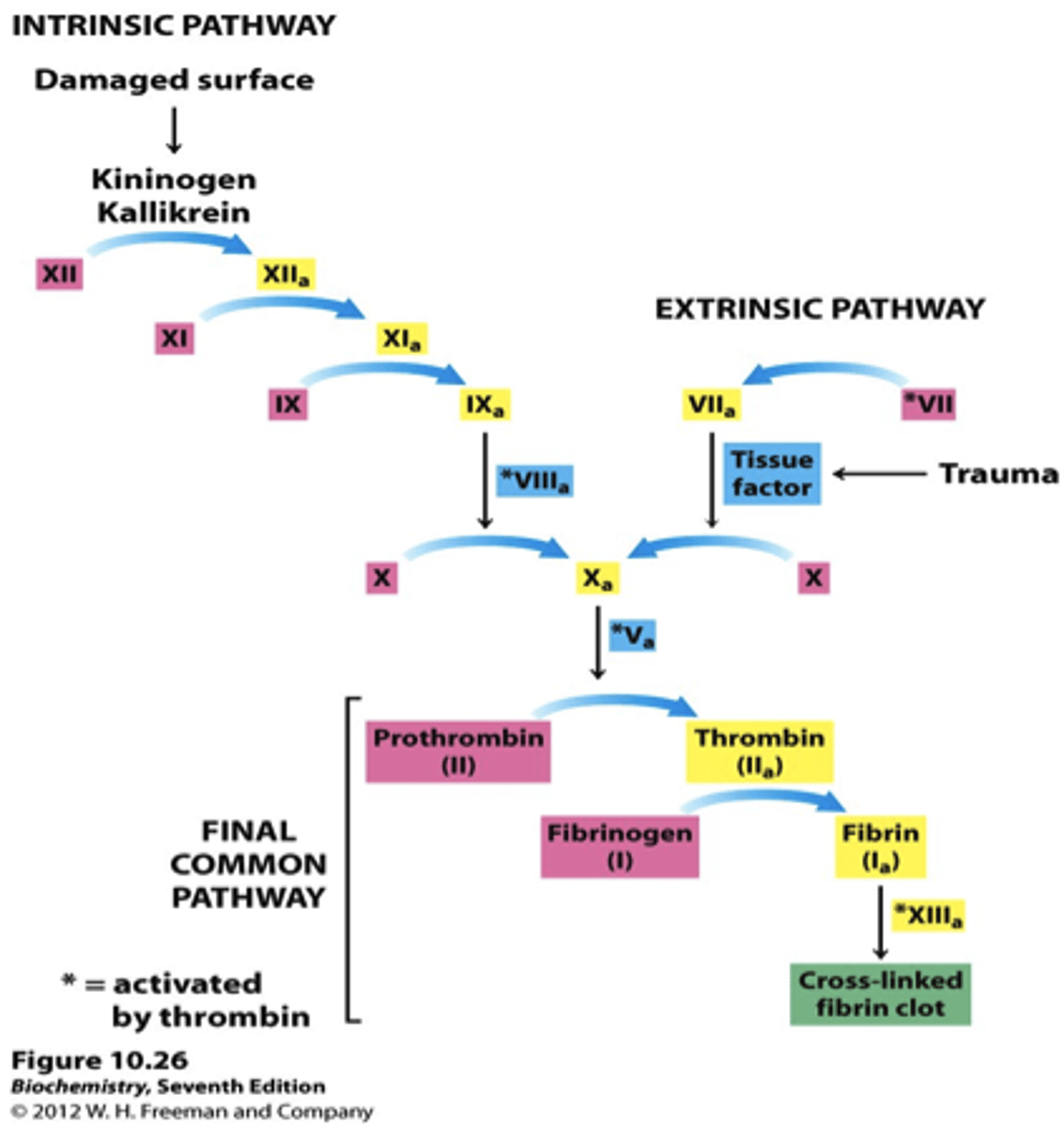
Thrombin
- End product of coagulation cascade
- Activated Prothrombin
- Converts fibrinogen to fibrin
Anti-Coagulants
- Anti-thrombin
- Heparin
- tPA
- Protein C
- Protein S
Anti-Thromibin
- Inhibits activated forms of factors 2, 7, 9 ,10, 11, 12
- Targets Thrombin and Factor Xa
Heparin
Enhances the activity of anti-thrombin
tPA
Used clinically as a thrombolytic
- Converts plasminogen to plasmin
Protein C and Protein S
Activated Protein C and Protein S cleave and inactivate Factors 5a and 8a
Plasmin
- Anti-coagulant
- Cleaves cross-linked fibrin and serum fibrinogen
- Destroys coagulation factors
- Blocks platelet aggregation
_____ inactivates Plasmin.
Alpha-2 Anti-Plasmin
vitamin K metabolism
Requires glutamate!
Kinin Cascade
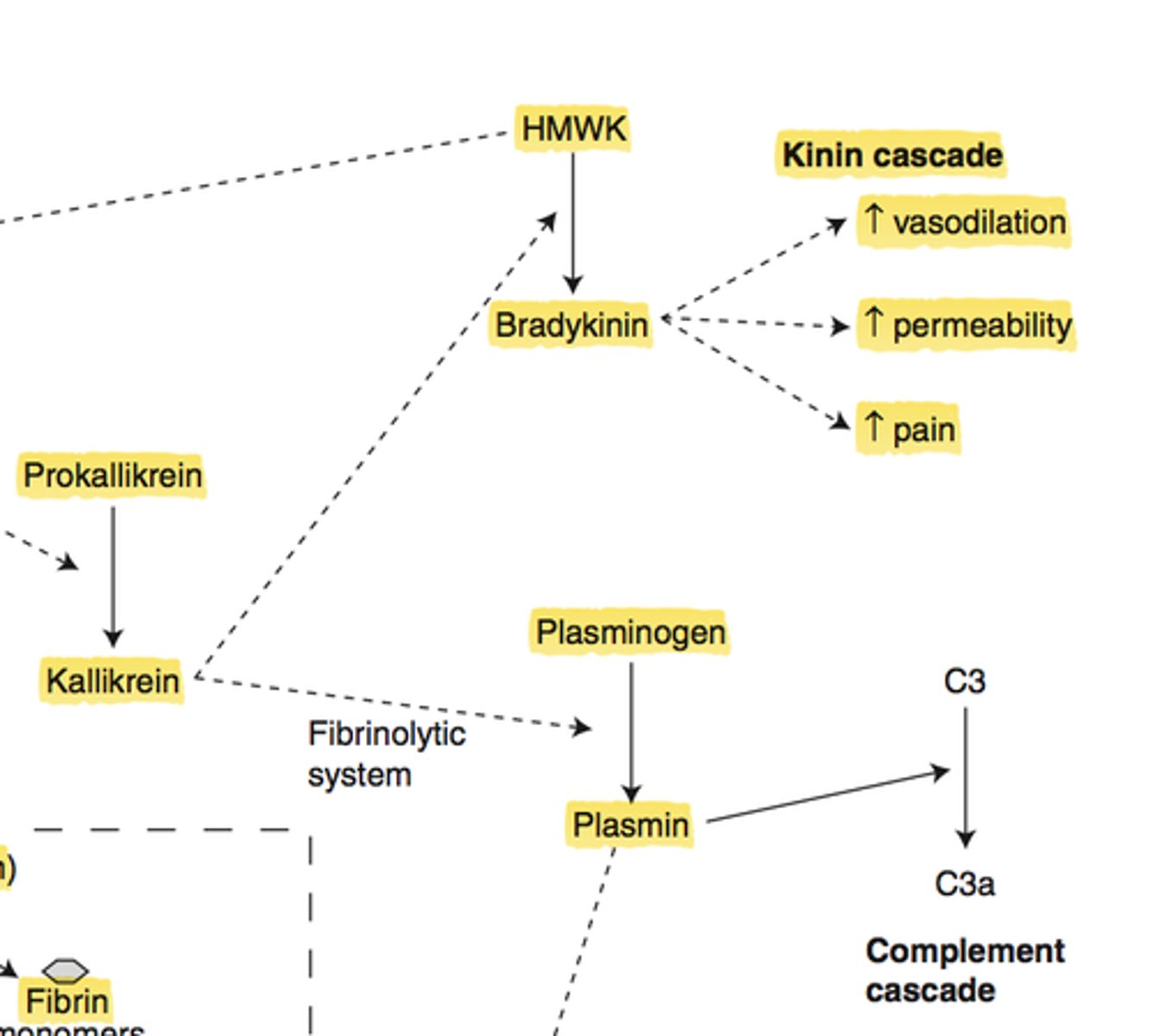
How is HMWK important for coagulation cascade?
It activates Factor 12 to initiate the intrinsic part
Kalikrein
Converts HMWK to Bradykinin
Function of Bradykinin
Increases vascular permeability, pain, vasodilation
Normal Adult Bone marrow
- 50% fat cells
- Myeloid:Erythroid ratio = 2:1 - 7:1
Reticulocytes have a bluish color due to...
RNA remnants
Myeloblasts differentiate into ...
Basophils/mast cells
Eosinophils
Neutrophils
Sources of Iron
Heme = meat (more readily absorbed)
Non-Heme (veggies)
Steps of Iron Absorption
1. Iron binds to brush border and enters enterocyte
2. Iron leaves enterocyte via Ferroportin and enters blood stream
3. Binds to transferrin once in blood
(if iron need is low, it binds to ferritin and is stored intracellularly)
Iron absorption
a. Location of intestine
b. Requires what state of iron
a. Duodenum
b. Fe+2 state (more readily absorbed than Fe+3)
Why is iron always bound to transferrin in blood?
Can form free radicals if not bound
Ferroportin
Transport of iron into and out of cells
Hepcidin
Blocks ferroportin and lowers serum iron concentrations
(prevents duodenal enterocyte uptake of iron. also prevents recycling via macrophages)
When are levels of Hepcidin increased?
- when transferrin bound iron increases
- In iron overloading diseases
- In chronic inflammatory diseases
Transferrin
- Binds iron in blood and transports it to cells (liver and macrophages for storage)