Chapter 6: Voice Disorders
Basic Vocabulary
Words
- Edema - Swelling
- Velum - Soft Pallet
- Aphonia - Loss of Voice
- Atrophy - Reduction in Tissue
- Hyperfunction - Increased Muscle Activity
- Hypofunction - Reduced Muscle Activity
Prefixes
- A - total loss
- Dys - abnormal
- Hyper - over/excessive
- Hypo - under/inadequate
- Ad - to/toward
- Ab - away from
Voice quality can be described:
Harsh - excessive muscle tension
Breathy - partial whisper
Hoarse - voice that is both harsh and breathy, irregular vocal fold vibrations
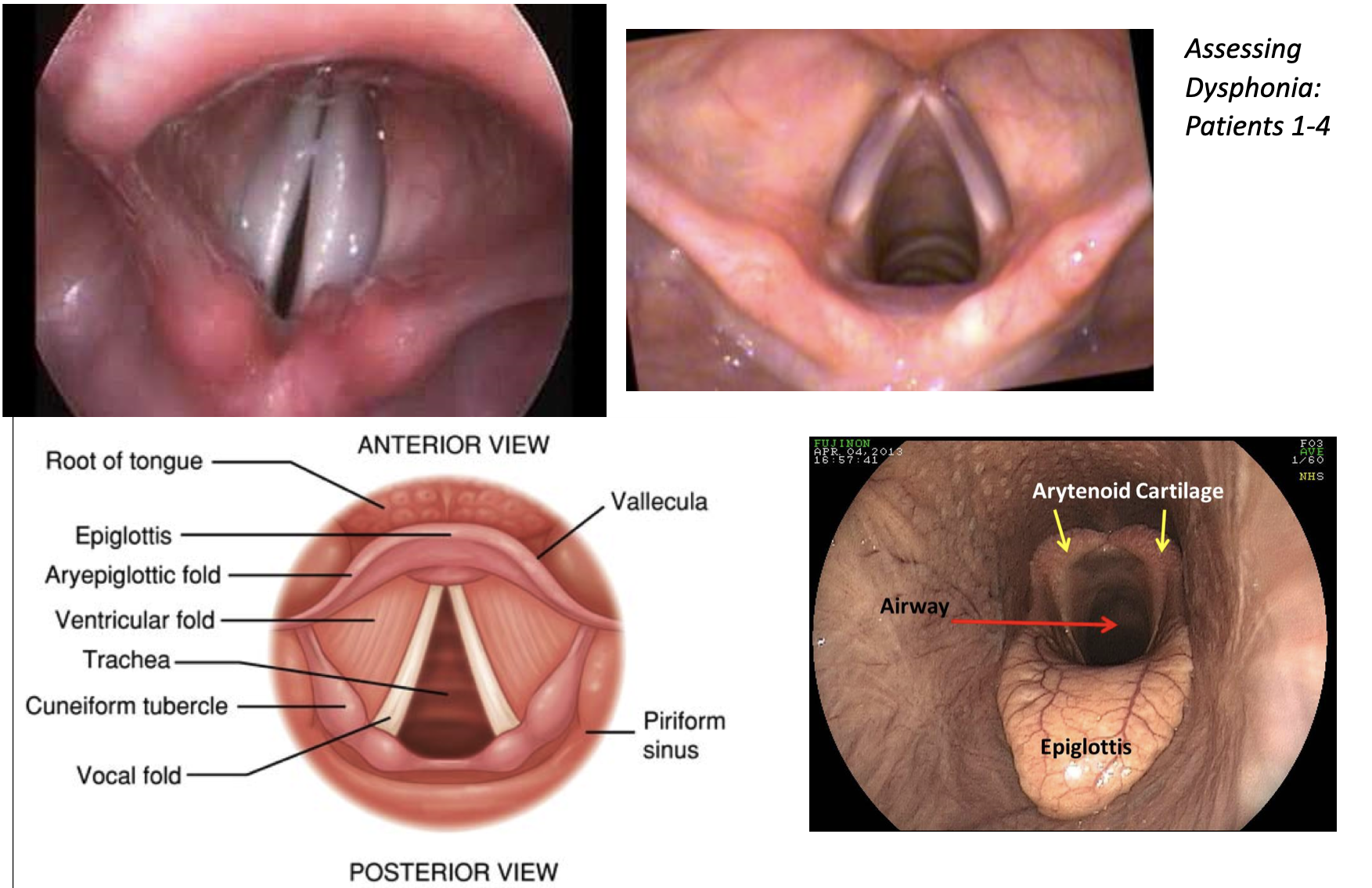
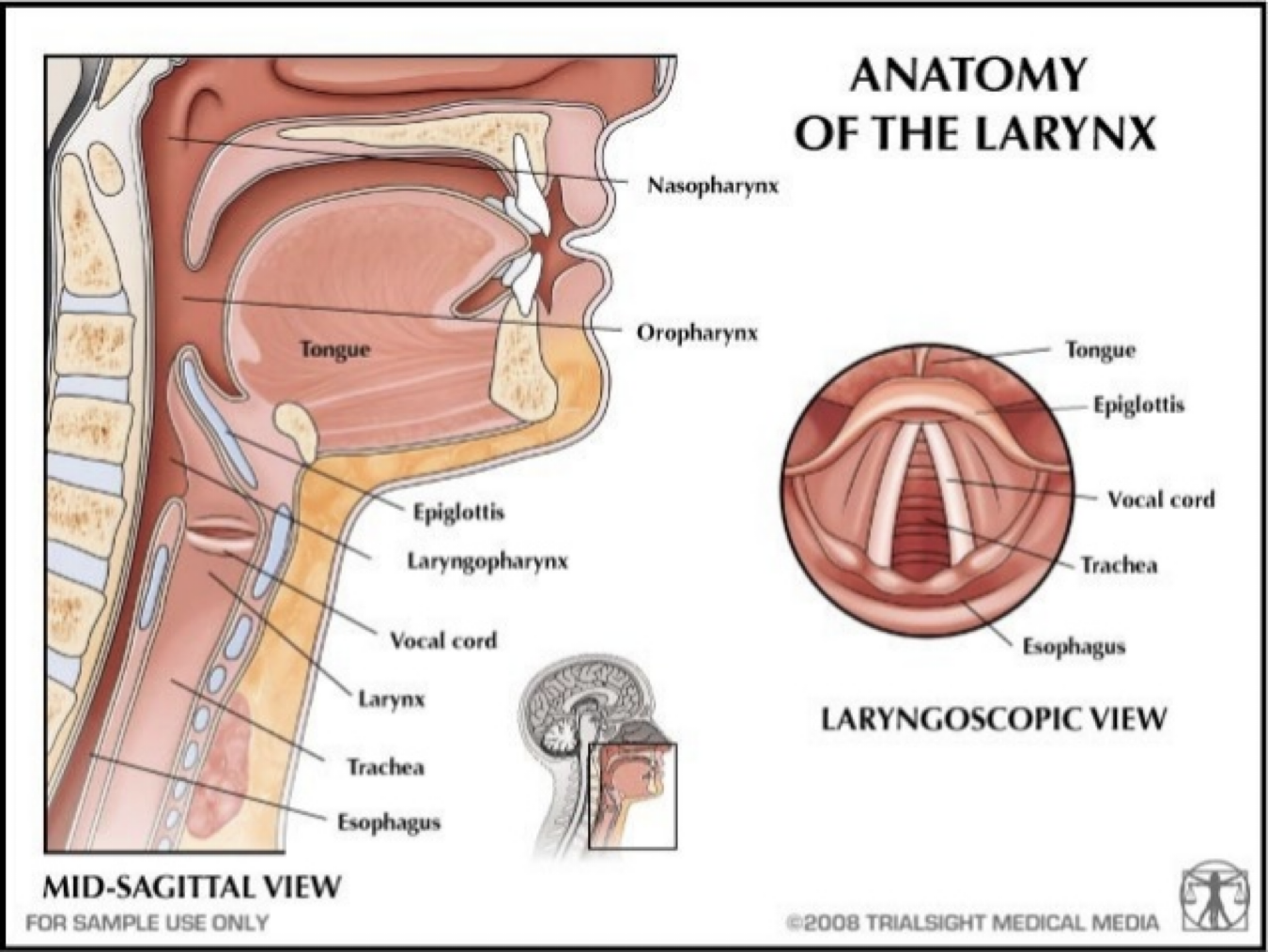
Speech Language Pathology - vocal folds in action
Vocal Fold Abnormalities that Affect Voice
- a variety of structural changes in the vocal folds can affect the voice
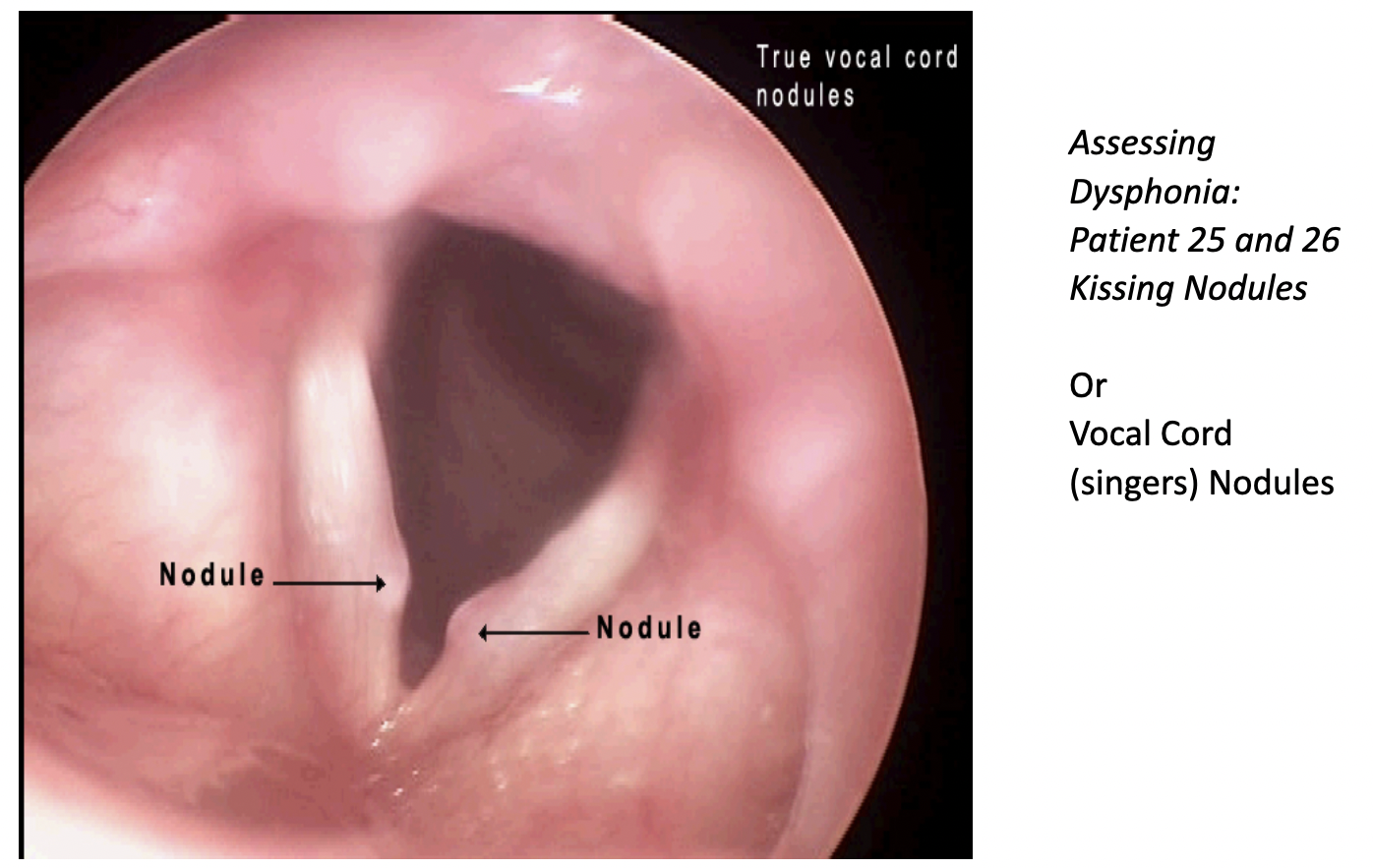
- Nodules - calluses that develop on the vocal folds
- Most common form of vocal fold abnormality
- Male children 5-10 years old and adult females
- Extroverted, “talkers”
- Hoarse voice quality
- Nodules form in pairs at the point of maximum contact along the length of the vocal fold where the amplitude of vibration is greatest
- Patient alters phonatory behavior to eliminate vocal abuse, the nodules will almost always be eliminated
Vocal Misuses and Abuses of the Larynx
- Talking in a noisy environment
- Yelling, screaming, or cheering
- Frequent coughing or clearing of the throat
- Giving speeches or lectures
- Using caffeine products
- Spending time in smoky environments
Treatment Techniques
- Yawn-Sigh
- Vocal folds are abducted during a yawn and they are not fully adducted during a sigh
- Helps patient feel/hear/produce a less tense sounds
- Extend breathy phonation into vowels, open syllables, words, phrases, and sentences
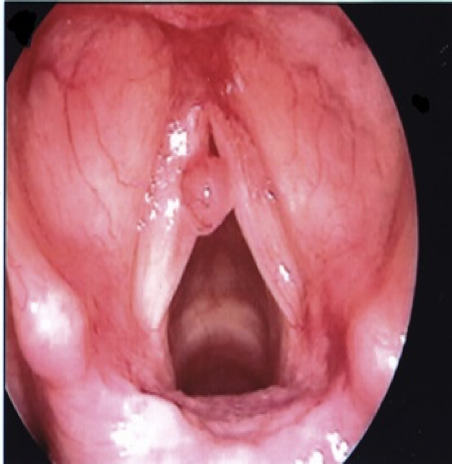
Polyps
- Polyps - Blisters
- Polyps are relatively common
- Shapes:
- Pedunculated - small balloons connected to the vocal fold by a narrow foot
- Sessile [ˈseˌsīl] - spread over a relatively large area of the vocal fold
- Abuse (one time), unilateral, breathy/hoarse
- Voice therapy to reduce vocal misuse/abuse, surgery
Contact Ulcers
- Contact ulcers and the granulomas that develop at sites of ulceration arise at the vocal processes (on the vocal folds between the arytenoids cartilages)
- Site is further back than the midpoint where nodules and polyps typically form
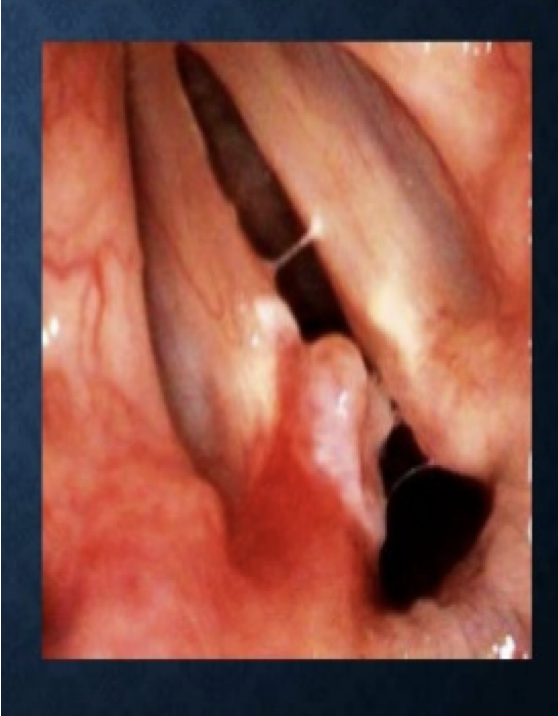
- Causes:
- Excessive slamming together of the arytenoid cartilages during the production of low pitches
- Frequent nonproductive coughing and throat clearing
- Gastric reflux
- Intubation trauma
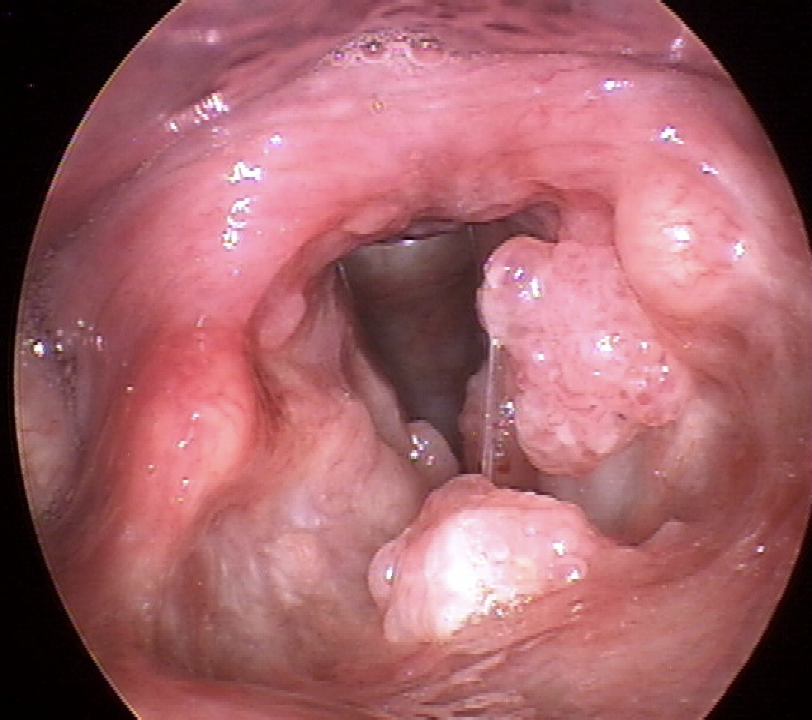
Papilloma
- The human papillomavirus can cause warts on the vocal folds
- Grow large
- Not common
- Hoarse voice quality
- Surgery, developing good vocal hygiene
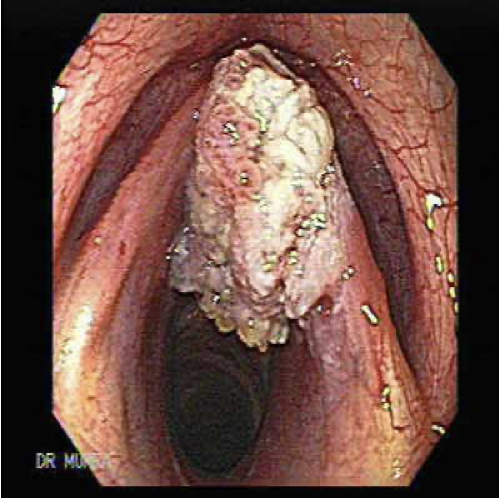
Carcinoma
- Carcinoma - Cancer of the larynx
- Frequently arises from exposure to inhaled smoke
- Preoperative and postoperative care is laryngectomy is needed
Voice Disorders Resulting from Neurological Impairment
- Paresis - partial loss of the capacity to carry out a voluntary movement
- Paralysis - total loss of the capacity to carry out a voluntary movement
Paralysis
- Paralysis Causes - Cranial nerve cut in surgery (usually vegas), Stroke
Treatment for Unilateral Vocal Fold Paralysis
- Unaffected side “overadducts” to approximate the paralyzed fold
- Surgery involves physically moving the affected vocal fold closer to midline so that the unaffected fold can contact it during phonation
Bilateral Paralysis
- Bilateral paralysis is less frequent
- Results from CNS damage
- If neural input to both recurrent laryngeal nerves is eliminated both fold assume a static position, glottis is compromised resulting in difficulty breathing (dyspnea)
- Surgery
- Voice typically remains functional
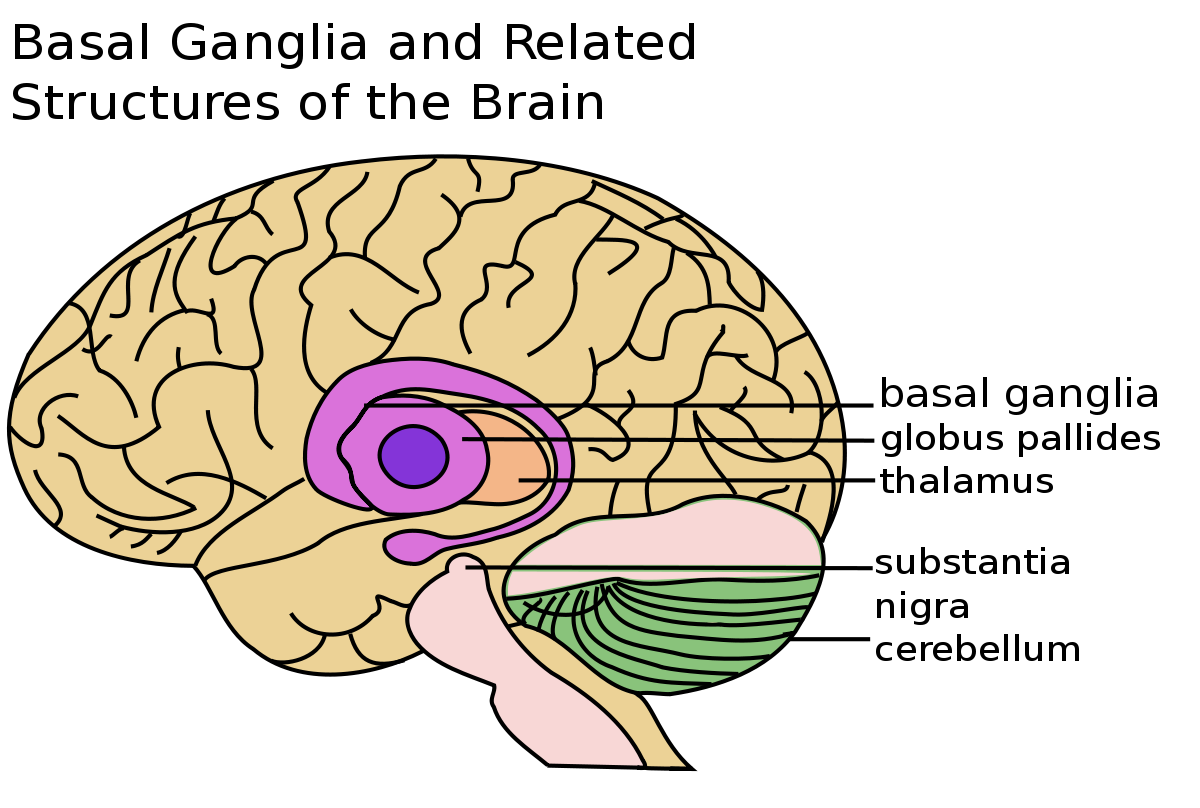
Spasmodic Dysphonia
- Rare disorder
- Accepted as a neurological problem involving a disturbance in the basal ganglia that causes disordered muscle tonicity
- Types:
- Adductor spasmodic dysphonia - strain-strangled voice quality, uncontrolled contractions of the adductor muscles
- Abductor spasmodic dysphonia - causes inappropriate contraction of the laryngeal abduction muscles, periods of aphonia
- Mixed spasmodic dysphonia - sudden abductions as well as sudden adductions
- Dysphonia Treatment - Botox into the vocal folds
Vocal Abnormalities Unrelated to Structural Change
- Conversion Aphonia/Dysphonia - patient reports change/loss of voice but medical examination fails to uncover an organic cause for the problem
- Psychogenic cause of the voice disorder may be suspected
- Sudden onset
- Careful interview
- Restored within an hour
- Referral to a mental clinician
Voice Disorders
- Puberphonia - mutational falsetto involves the continued use of a high-pitched voice by a post pubertal male
- Functional disorder
- Easy correction
- Muscle Tension Dysphonia - caused by inordinate tension in the laryngeal muscles
- Result from the simultaneous contraction of the muscles that close and open the vocal folds
- Hypertensive, “knots”
- Benefits from laryngeal massage
- Hoarse
- Report fatigue and laryngeal discomfort
- Hard driven, upwardly mobile, Type A personalities
Voice Evaluation
- Voice Evaluation Team - otolaryngologist, speech therapist
- Voice Evaluation Interview - History (how voice disorder started, etc.)
- Perceptual Assessment - clinician makes judgements regarding the pitch, volume, and quality of voice during a variety of tasks (sometimes recorded)
- Clinicians use scales for grading vocal parameters
- Assessments
- The Consensus Auditory Evaluation of Voice (CAPE-V)
- The Voice Handicap Index (VHI)
- Instrumental Evaluation
- Flexible videoendoscopy
- Stroboscopy - slow motion technique that allows the clinician to examine closely the movement characteristics of the vocal folds
- Visi-Pitch - provides objective data on a number of acoustic parameters
Laryngectomy
- Laryngectomy - removal of the larynx (cancer)
- Surgical removal of the larynx requires that the trachea be redirected to an opening on the front of the neck known as the tracheal stoma
- Artificial larynx
- Electrolarynx
Esophageal Speech
- Esophageal Speech - air is actively injected down the esophagus past an area known as the pharyngeal-esophageal (PE) segment
- Air is released and passes by the PE segment and draws the walls of the esophagus into vibration, much like air passing through the true vocal cords
- Esophageal walls are much larger in mass - esophageal speech is much lower in pitch
Tracheoesophageal Speech
- Tracheoesophageal Speech - air is routed from the lungs into the esophagus via a tracheoesophageal speech prosthesis
- Additional surgery to create a small opening between the trachea and esophagus in which the prosthesis is inserted
- Cover the stoma or be fitted with a valve
- Most natural speech with the least therapy
Prevention of Voice Disorders
- Vocal Hygiene is daily regimen of good habits to maintain the health of your vocal folds
- These include eliminating inappropriate vocal habits and situations that place unnecessary wear and tear on the voice and common-sense behaviors which contribute to efficient voice production and overall voice health
- The following is a list of some tips for keeping your voice healthy:
- Avoid irritants:
- cigarettes and secondhand smoke
- manage reflux with over the counter (OTC) medication/see an ENT who specializes in voice disorders for prescription medications which may be less drying
- Take care of your body:
- Maintain good hydration: Drink 6-8 ounce glasses of water/day
- Rest
- Exercise
- Good Nutrition
- Maintain good vocal habits:
- Avoid throat clearing and coughing
- Avoid whispering
- Warm up your voice before making big demands on it
- Avoid repeated stress on the voice
- Use good posture
- Control environmental factors that may negatively impact your voice