
peds exam 1 notes
Pediatric Exam 1 Study Guide
KEY: Memorization = blue
Unit 2: Health Promotion: Infant, Toddler, Preschooler, School Age and Adolescent (20 questions) - Review along with the TABLES listed and the Major Theories of Development document. | |
Health promotion | Focuses on maintaining or enhancing the physical and mental health of children Partnership development is the key strategy for success when implementing a health promotion activity. |
Principles of Health Supervision | - Providing services proactively - Optimizing child’s level of functioning - Ensuring child is growing and developing appropriately - Promoting best possible health of child - Preventing injury and illness through child teaching |
Three Components of Health Supervision | - Developmental surveillance and screening - Injury and disease prevention - Health promotion |
Health Promotion | - Growth - Developmental Milestones - Physical Systems Focused - Nutritional Requirements - Anticipatory Guidance - Immunizations ______________________________________________ - Newborn/Infant - Neonate (birth to 27/28 days) - Infant (1 month to 12 months) - Toddler - Preschooler - School Age - Adolescent |
Developmental Changes in the Newborn/Infant *difference between growth, development, and maturation. | Growth ○ increase in physical size (doubles birth weight by 6 months of age and triples birth weight by 12 months of age) Development ○ sequential process by which infants and children gain various skills and functions Maturation ○ increase in functionality of various body systems of developmental skills |
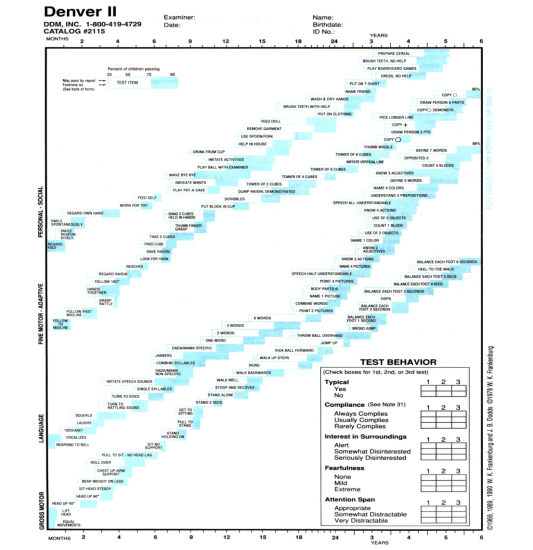
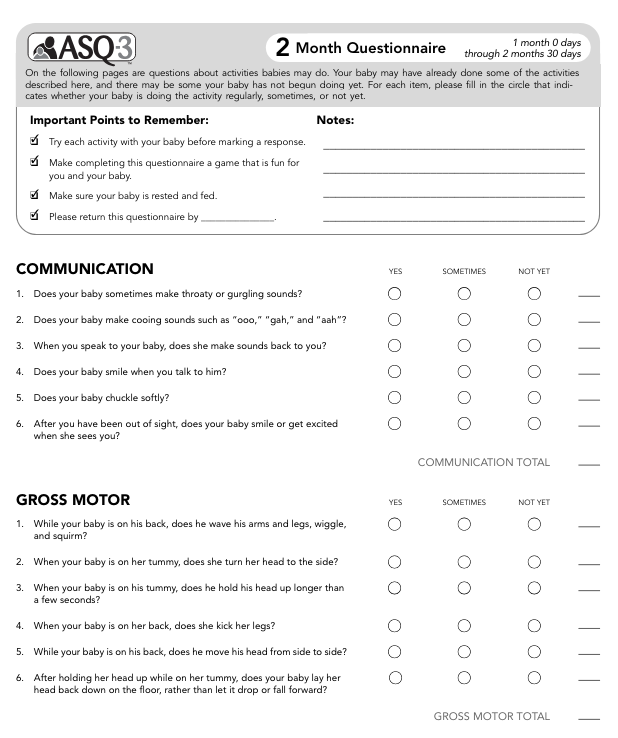
Assessing Newborns and Infants for Developmental Milestones | Nurse may ask the parent if the skill is present or the infant may demonstrate the skill during the assessment The nurse may elicit the skill from the infant Screening tools may be used to assess development: ○ Denver II Developmental Screening Test: a quick screen to determine whether a child is achieving developmental milestones in the areas of gross motor, fine motor, language, and personal social skills. It can be used with children from birth to 6 years of age. ○ Ages and Stages: identifies infants and young children whose social and emotional development requires further evaluation to determine if referral for intervention services is necessary. Example: ○ Learn the Signs. Act Early: From birth to 5 years, your child should reach milestones in how he plays, learns, speaks, acts and moves. (it’s like a CDC website w/ resources) |
Assessing growth and development of a premature infant | Use the infant’s adjusted age to determine expected outcomes
Plot growth parameters and assess developmental milestones based on adjusted age |
Newborn Reflexes: Sucking, Rooting, Grasp, Babinski, Moro, Tonic neck, Dance/step *Know how to assess newborn reflexes and at what age they are expected to disappear | |
Dance/Step
**they are instinctively trying to walk | |
Sucking
**helps latch on to nipple so they can feed | |
Rooting/root reflex
**helps find a nipple to feed | |
Moro
**occurs when they are startled or feel like they are falling | |
Tonic neck/Asymmetric tonic neck reflex
**idk why but they look like superman about to take off. | |
Grasp/Palmar grasp
**motor development and facilitate bonding. | |
Plantar reflex
**motor development also | |
Babinski
**reflects immature corticospinal tract - normal for them before 12 months | |
Infant Milestones TABLE 9.1 (info from this table that is on the study guide) Fine pincer grasp | Posterior fontanel closes by 8 weeks Social smile occurs by 2 months Head turns to locate sounds by 3 months Steady head control is achieved by 4 months Able to roll from tummy to back and from back to tummy by 5-6 months Plays “peek-a-boo” after 6 months Able to transfer objects from hand to hand by 7 months Able to sit unsupported at 8 months Able to crawl at 10 months Waves “bye-bye” at 10 months Fine pincer grasp appears at 10-12 months Able to walk with assistance at 10-12 months Says a few words in addition to “mama” and/or “dada” at 12 months Can sit down from standing position without help at 12 months |
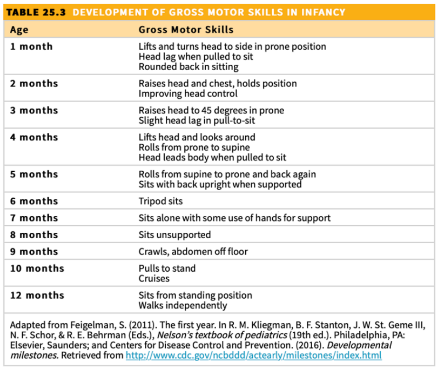
Table 25.3 - Development of gross motor skills in infancy **cruising - walking holding something to support themselves | |
Infant safety | Infant car seat rear facing in the back seat, BACK to sleep, crib rails up, never leave child alone on a raised, unguarded surface, never leave infant alone in bath, fence swimming pools, fence stairways, baby proof the home (keep all medications & household cleaning items high and locked, cover electrical outlets). |
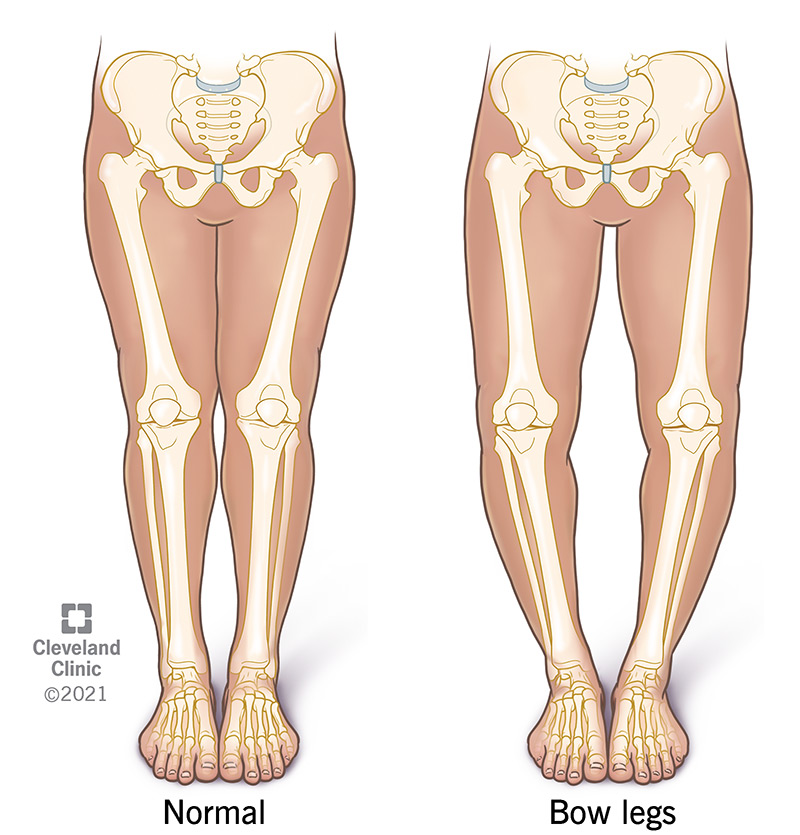
Toddler/Preschooler Milestones Table 11.1 and 12.1 (info from this table that is on the study guide) Bowlegged Potbellied | Temper tantrums are common Appears bowlegged and potbellied (lordosis) Anterior fontanel closed between 12 and 18 months Throws ball overhand by 18 months ⚽ Kicks ball by 24 months Can walk up and down the stairs by 24 months (2 feet on each step) Walks with wide stance at 24 months **things w their feet by 24 mo Feeds self with spoon and cup at 2 years Daytime toilet training can begin by age 2 years Two-to three- word sentences are spoken by 2 years **eating, speaking, and pooping (essentials) accomplished by 2 years Own first and last name can be stated by 2 ½ to 3 years All primary teeth (20) are present by 3 years Three-to four- word sentences are spoken by 3 years Names what has been drawn by 3 years Copies a circle (drawing) with facial figures by 3 years Rides Tricycle by 3 years Stands on one foot for a few seconds by 3 years Uses sentences of four or five words by 4 years Draws 3-part stick figures by 4 years Can walk up and down the stairs using alternate footing by 4 years Can skip and hop on one foot by 4 years Uses sentences of 6-8 words by 5 years Can tie shoelaces by 5 years Throws and catches ball well by 5 years Skates with good balance by 5 years |
Toddler safety: | Leading cause of death in toddlers/preschooler is unintentional injury. MUST focus on safety education. Car seats and booster seats must be used in the backseat of the car at all times. Swimming lessons and Pool fences for drowning prevention Curious about the world around them and like to explore. Accidental poisoning is a safety issue. Use of ipecac syrup is NO LONGER recommended (rapid-acting emetic) → Teach parents that it is NOT recommended to induce vomiting in any way because it may cause more damage. CALL Poison control center. |
School-age and Adolescents Milestones Tables 14.1, 15.1 and 15.2 (info from this table that is on the study guide) | Develops concepts of numbers by 6 years Knows right and left hands by 6 years Likes table games and simple card games by 6 years Uses table knife for cutting meat by 7 years Mechanical in reading by 7 years Can count backwards from 20 by 8 years Likes the reward system by 8 years Puberty: Girls sequence of maturational changes/puberty: can begin anytime between 8-13 years old in this order: breast changes, rapid increase in height and weight, growth of pubic hair, appearance of axillary hair, menstruation 2 years after first signs (breast changes) Boys sequence of maturational changes/puberty: can begin anytime between 9 ½ and 14 years old in this order: enlargement of testicles, growth of pubic hair/axillary hair/hair on upper lip/hair on face, rapid increase in height, changes in larynx causing voice changes, nocturnal emissions ( also known as wet dreams or nocturnal orgasms) |
School age/adolescent safety: | Leading cause of death is unintentional injury. MVA (motor vehicle accidents) refuse to ride with an impaired person or one who is driving recklessly, ALWAYS wear a seatbelt, passenger seat for 12 years of age or older, discourage distractions while driving-cell phones, texting, eating or smoking; if drinking alcohol or any drugs call someone to pick you up, never drive under the influence Learn how to swim and basic water safety rules Ask about depression (sadness, withdrawn) and thoughts of suicide or hurting self/others |
Growth milestones | When does birth weight double? 5-6 months When does birth weight triple? 12 months When does birth length double? 4 years When does a child use scissors? 4 years When does a child tie his/her own shoes? 5 years |
Concepts of bodily injury | Infants: remember pain after 6 months Toddlers: fear intrusive procedures Preschoolers: fear of body mutilation School-age: fear of loss of control over their bodies Adolescent: concerned about change in body image |
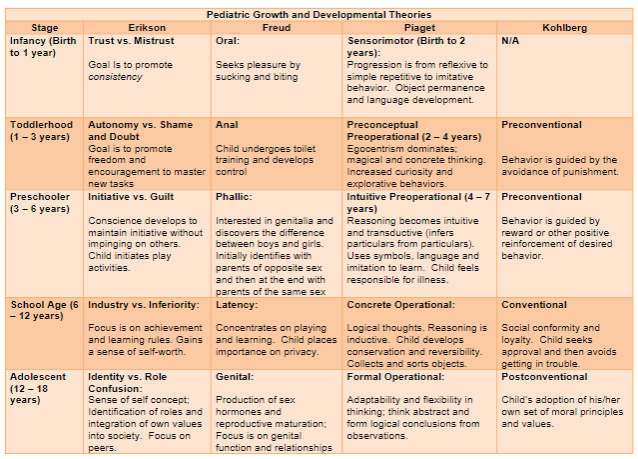
Review Pediatric Growth and Developmental Theories: Erikson, Freud, Piaget, Kohlberg FROM BIRTH TO ADOLESCENCE | |
Erikson 1 is a bun - rust colored bun 2 is a shoe - shane is sitting in his auto inside of a shoe 3 is a tree - there is an inn & tia sitting on a tree covered by a quilt 4 is a dinosaur - the dinosaur is dusty and he feels inferior 5 is a skydive - skydiver falls and dents the car and is confused | Trust vs mistrust
Autonomy vs shame and doubt
Initiative vs guilt
Industry vs inferiority
Identity vs role confusion
|













Unit 3: Medication Dosage Calculations (5 questions) | |
Unit 4: Care of the Hospitalized Child (8 questions) | |
Slide 5: Stressors and nursing interventions | Two main stressors seen across age groups: Separation anxiety
Loss of control
|
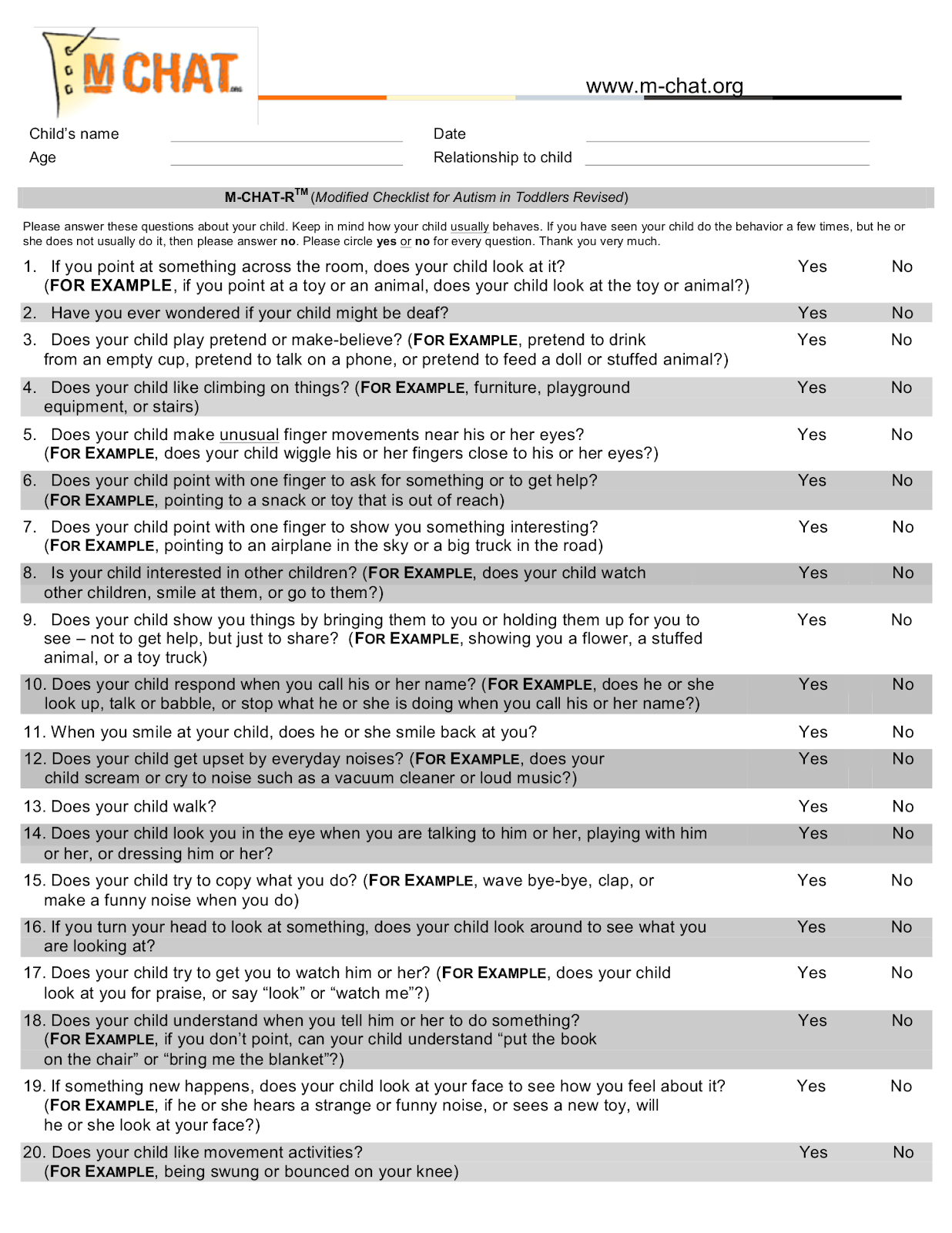
Slide 17: Autism | What is it?
Occurs in
Etiology
Clinical manifestations
Diagnostic evaluation
Prognosis Early identification and intervention (i.e. therapy) are key Nursing care management
|
Slide 26: Hearing impairment | When caring for a child who is hearing impaired, the nurse should do the following:
|
Slide 28: Visual impairment | Working with a Child who has a visual impairment
|
Slide 29: Nursing assessment of child w/ disability | Nursing assessment of the child with disabilities
|
Slide 37: Minors who may give consent | Emancipated minor - has established independence from his/her parents through marriage, pregnancy, or service in the armed forces, or by a court order. Emancipated minor is considered legally capable of signing an informed consent. |
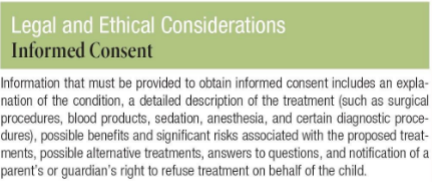
Slide 38: Legal and ethical considerations of informed consent | |
Slide 44: IV access | Site selection and equipment Provide atraumatic care: use topical anesthetic (for IV access and IM)
Maintenance Complications (requires frequent assessment for infiltration: redness, swelling, leaking) Removal |
Unit 5: Pain Management, Chronic Illness and End of Life (7 questions) | |
Chronic illness | |
Slide 21: Developmental factors | Effect on understanding of death Effect on behavioral response to death Effect on ability to communicate about death By 6 years of age, children recognize death as permanent By ages 9-10, children understanding of death is the same as an adult (inevitable, universal and irreversible) |
Slide 24: Nursing management for child that's dying | Be verbally supportive Do not reinforce denial Do not argue Recognize anger as normal response (do not take it personally) Actively listen, use stillness Encourage expression of feelings Offer spiritual support if appropriate Assist with grieving process and support resources Encourage family to create memories Allow progression through stages of grieving Encourage family participation in care and activities as appropriate |
Pain (5 questions) | |
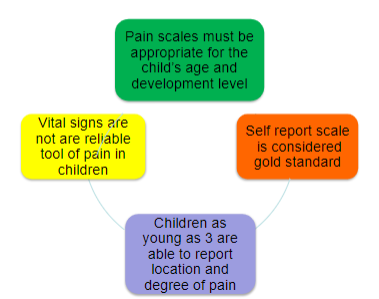
Slide 9: Pain assessment scales | |
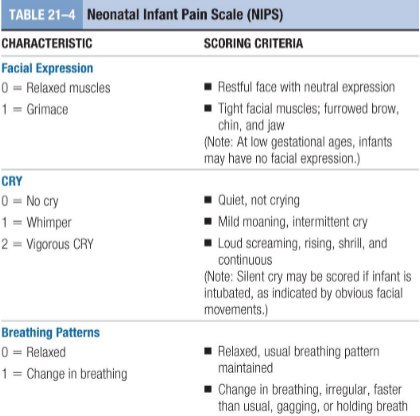
Slide 10: Tools bv age | Neonatal Infant Pain Scale (NIPS)
|
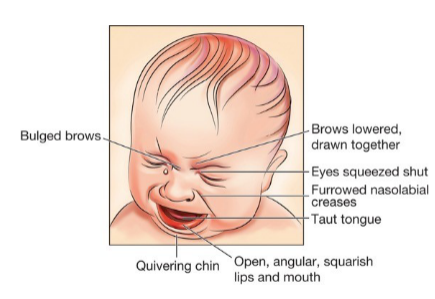
Slide 11: Signs an infant is in pain | |
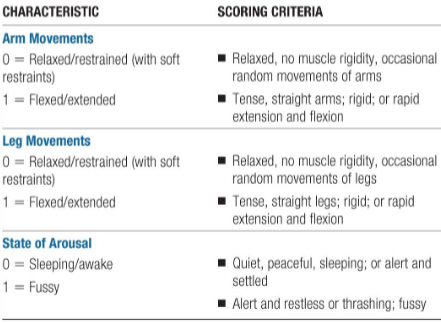
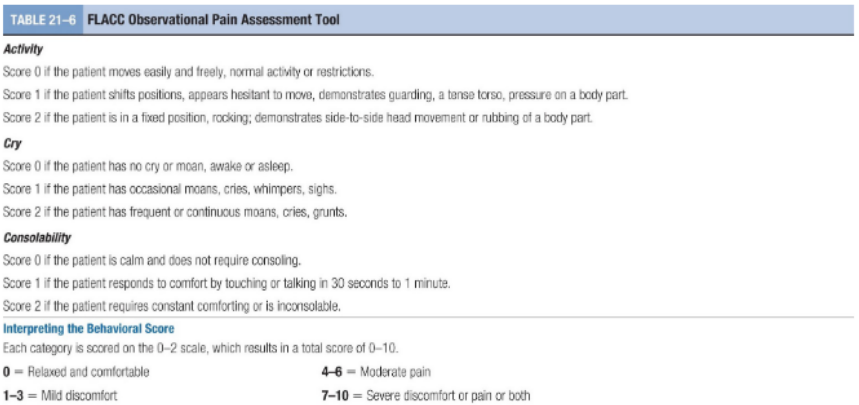
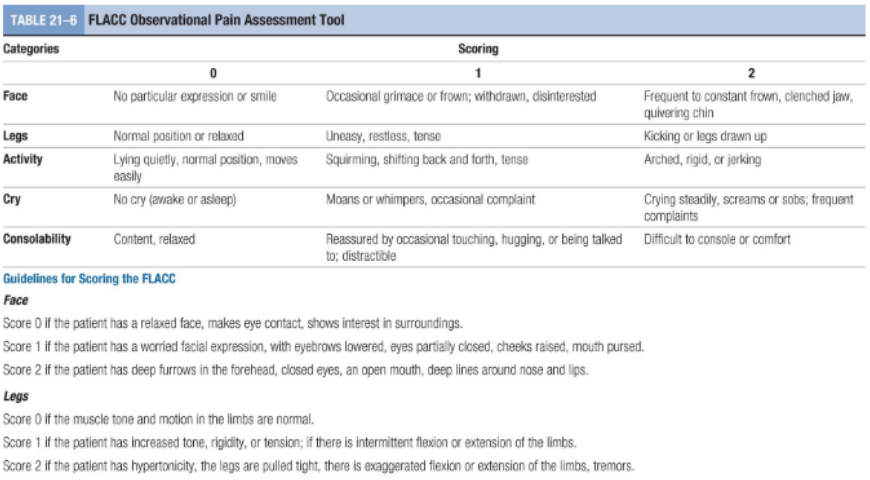
Slide 12: Face, Legs, Activity, Cry, Consolability (FLACC) | Face, Legs, Activity, Cry, Consolability (FLACC)
|
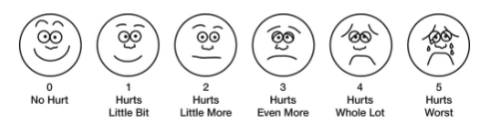
Slide 13: FACES | Wong Baker FACES Pain Rating Scale
|
Slide 14: Numeric pain scale | Numeric pain scale
|
Summarizing the pain scales | NIPS: Neonatal infant pain scale
FLACC: Face, legs, activity, cry, consolability
FACES
Numeric pain scale
|
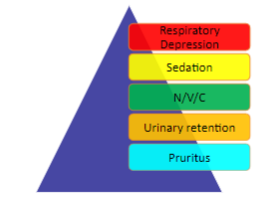
Slide 18: opioid SE | |
Slide 20: Non opioid analgesic | Nonsteroidal Anti-inflammatory Agents (NSAID’s):
Acetaminophen
|
Slide 26: Pediatric Pain Pearls | Pain assessment is considered the 5th vital sign. Guidelines are available regarding when you should treat pain. Morphine sulfate is the gold standard for sedation/pain Naloxone is the reversal agent for the opioid agents. Be consistent with using the same pain scale (must be appropriate for age and developmental level). IV narcotics are second witness medications at most institutions. |
Units 6 and 7: Respiratory Dysfunctions (10 questions) ** It is highly recommended that you read the material in the book if you are not understanding any concept from the slides. This will help reinforce learning. | |
Assessing respiratory function in children history | Pattern of Respirations – Rate (rapid (tachypnea), normal, slow (bradypnea)) – Depth (normal, shallow (hypopnea), too deep (hyperpnea)) – Ease (effortless, labored (dyspnea), difficulty breathing except in upright position (orthopnea), retractions → inspiratory or expiratory, nasal flaring) – Labored Breathing (continuous, intermittent, worsening, sudden onset, at rest or on exertion, associated with wheezing, grunting or chest pain) Cough – When is the cough heard (night, early am, daytime) – Nature/character of cough (croupy, wheezy, dry, wet, productive) – Frequency of cough Cyanosis, halitosis (associated with sore throat, lung infections), chest pain |
Effective auscultation | Make certain the child is relaxed and not crying, talking, or laughing. Record if child is crying. Check that room is comfortable and quiet. Warm stethoscope before placing it against skin. Apply firm pressure on chest piece but not enough to prevent vibrations and transmission of sound. Avoid placing stethoscope over hair or clothing, moving it against the skin, breathing on tubing, or sliding fingers over chest piece, which may cause sounds that falsely resemble pathologic findings. Use a symmetric and orderly approach to compare sounds on each side. |
Lung sounds | – Inspiration and expiration (all lung fields) – Wheezing: produced as air passes through narrowed passageways (obstruction) → sounds like high pitched whistling noise. – Crackles: result from the passage of air through fluid or moisture (fluid in lungs) → sounds like popping or crackling |
Acute infectious disorders | |
Nasopharyngitis (common cold) | Common Cold definition: –Viral upper respiratory infection Pathophysiology: –RSV –Influenza –Rhinovirus –Adenovirus Epidemiology • Toddlers get 6-9 colds per year • Immunity increases with repeated exposure to viral organisms and children will get fewer respiratory tract infections Signs and symptoms Fever, Headache, malaise, Nasal congestion, Rhinorrhea (thin watery discharge), Thick and purulent (the color is not an accurate indicator of viral vs bacterial), Nasal blockage, Irritable/restless, Decreased activity, Sore throat, Poor feeding (anorexia), Cough, Muscle aches, Abdominal pain, V/D Nursing interventions No specific treatment, Comfort measures, Antipyretics, Rest, Increase fluids, NO decongestants under 4 years old, Saline + suction Influenza positive? – Antivirals Teaching! –Hand washing , –Elbow cough/sneeze |
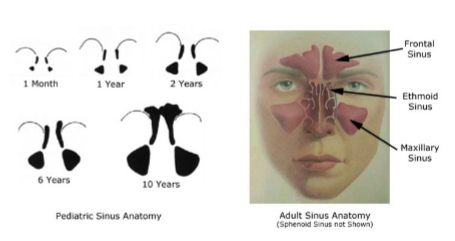
Sinusitis | Sinusitis definition: – Bacterial infection of the paranasal sinuses Pathophysiology: – Mucosal swelling – Decreased ciliary movement – Thickened nasal discharge – Young children
– >10 years
Signs and symptoms Greater than 10 days of: – Cough, Nasal congestion, Fever, Halitosis, Facial pain, Irritability, Poor appetite Nursing interventions Antibiotics as ordered, Normal saline nasal spray, Increased fluids, Comfort measures, Teaching → Handwashing & Elbow cough/sneeze |
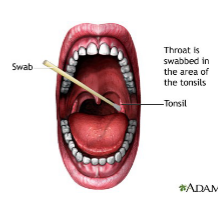
Pharyngitis & Tonsillitis –aka sore throat and inflamed tonsils Ice collar | Pharyngitis/Tonsillitis definition: – Inflammation of the throat mucosa and/or tonsils Pathophysiology: – Viral process – Group A beta-hemolytic strep (bacterial) – Gonorrhea Signs and symptoms Abrupt onset: Fever, Sore throat, Headache Anterior cervical adenopathy Abdominal pain Tonsils/pharynx with inflammation, redness, exudate, petechiae Strep throat mimics → common cold virus, COVID, flu, croup, mononucleosis, measles, chicken pox Nursing interventions Diagnosis – Rapid strep – Culture Treatment Bacterial
Viral
Nursing care post tonsillectomy Promoting airway clearance
Maintaining fluid volume
Minimize blood loss
Pain management
NPO until child is fully alert and able to swallow
TEACHING
|
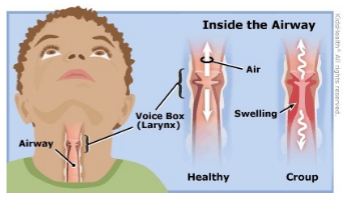
Croup syndromes
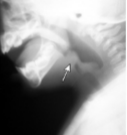
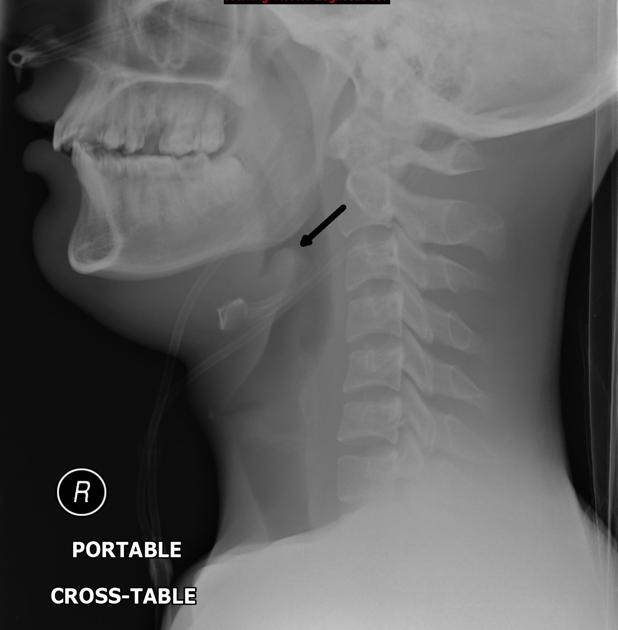
Toxic appearing child in tripod positioning | ACUTE EPIGLOTTITIS
Bacterial croup – Haemophilus influenza type b Pathophysiology – Inflammation of the epiglottis
Signs and symptoms High fever TOXIC appearing (can indicate shock presenting as lethargy, cyanosis, abnormal breathing, irritability, tachypnea, tachycardia) Tripoding → Leaning forward, Holding body up with hands, Open mouth with chin out Dysphonia → Muffled voice Dysphagia → Painful swallowing Dyspnea → Trouble breathing Drooling Nursing management of epiglottitis Do NOT attempt to visualize the throat (could cause complete obstruction) • Do NOT leave the child unattended • Do NOT place the child in a supine position • Provide 100% oxygen in the least invasive manner • If complete airway occlusion occurs, tracheostomy may be necessary • Ensure emergency equipment is available (resuscitation equipment and suction) LIFE THREATENING • Absence of spontaneous cough • Presence of drooling • Agitation
____________________________________________________ ACUTE LARYNGOTRACHEOBRONCHITIS
Viral croup – Inflammation of the upper airway Pathophysiology – Parainfluenza – RSV – Influenza Characteristic of croup Night-time cough Barky cough Signs and symptoms Monitor for respiratory distress – Inspiratory stridor – Suprasternal retractions – Nasal flaring – Decreased pulse-ox Nursing interventions Home Management such as: – Cool mist vaporizer – Elevate Head of Bed – Shower steam – Keep comfortable – Increase PO fluids Hospital Management – Monitor for respiratory distress – Provide cool mist humidified oxygen – Elevate HOB – Medications as ordered
____________________________________________________ ACUTE SPASMODIC LARYNGITIS aka “spasmodic croup”
|
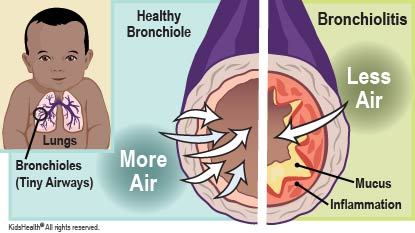
Acute infectious disorders: Bronchiolitis | Bronchiolitis – Inflammation of the bronchioles Pathophysiology: – RSV – Adenovirus – Parainfluenza Signs and symptoms • Tachypnea • Wheezing • Cough • Rhinorrhea • Sneezing • Difficulty feeding Nursing interventions • Nasal and/or nasopharyngeal suctioning • Frequent respiratory assessments • ?RR <60, O2 sats 90% or > • Positioning • Monitor pulse oximeter • Saline nebulizer • Oxygen as ordered (if O2 sats <90%) • Oral and/or IV hydration • Rarely is inhaled bronchodilator, racemic epinephrine is needed • NO antibiotics • NO cough suppressants |
Respiratory syncytial virus (RSV) bronchiolitis PREVENTION | Palivizumab (Synagis) – Humanized monoclonal antibody – Given IM monthly – Starts at the beginning of RSV season – Maximum of five doses Candidates – Infants born before 29 weeks of gestation – Infants in the first year of life with significant heart disease – Preterm infants (<32 weeks) with chronic lung disease |
Acute infectious disorders: Pneumonia | Pneumonia definition: – Inflammation/infection of the alveoli and the pulmonary parenchymal Pathophysiology: – Viral – Bacterial – Aspiration Signs and Symptoms – Fever – Cough – Tachypnea – Decreased breath sounds – Crackles – Difficulty feeding Nursing interventions • Administer Oxygen as ordered • Administer Antibiotics as ordered • Chest PT • Monitor Pulse Ox • Lay on affected side • Monitor s/s of dehydration |
Acute Non-Infectious Disorder: Foreign Body Obstruction | Foreign Body (FB) Obstruction definition – Occlusion to lungs due to offending object Pathophysiology: – Lodged in the main stem or lobar bronchus Signs and symptoms Cough Gagging Wheezing Stridor (FB is lodged in the upper airway) Asymmetric breath sounds Inability to speak (complete obstruction) Unresponsive (complete obstruction) Nursing interventions Prevention/Teaching – Dangers of certain foods (hotdogs, grapes, round candies, popcorn) – Toy age requirements (beads, small magnets) – Heimlich maneuver (>1 year old) Emergency measures – Activate emergency response – Perform Heimlich maneuver – Place IV – Prepare for endoscopy – X-ray |
Chronic respiratory disorders | |
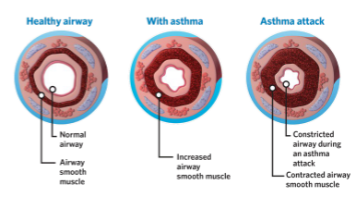
Asthma | Asthma definition: – Chronic airway inflammation with heightened airway reactivity (smooth muscle spasms and constriction) causing airway obstruction, bronchial hyper-responsiveness and recurring symptoms Status Asthmaticus definition: – Medical emergency – Respiratory distress even with treatment Epidemiology More than 7 million children in the US have asthma Primary cause of school absences Third leading cause of hospitalizations in children under 15 years Signs and Symptoms – Dyspnea: shortness of breath – Wheezing – Chest tightness – Non-productive cough (especially at night and early morning) – Tachypnea – Hypoxia – Prolonged expiration – Retractions – Nasal flaring Triggers Allergens – Outdoor: trees, shrubs, weeds, grasses, molds, pollen, air pollution, spores – Indoor: dust/dust, mites, mold, cockroach, antigen Changes in weather or temperature Irritants – Tobacco smoke, wood smoke, odors, sprays Cold air Animals – cats, dogs, rodents, horses Medications – aspirin, NSAID, antibiotics, beta-blockers Foods – nuts, milk/dairy Nursing intervention Avoid triggers Monitor pulse ox Administer oxygen/medications as per orders – Short acting beta-2 agonist: Albuterol
– Inhaled corticosteroids: Pulmicort (budesonide) or Flovent (fluticasone)
– Systemic corticosteroids: Prednisone (PO) or solumedrol (IV) – Airway Tray available Teaching – Asthma action plan – Medication administration – Avoiding triggers
|
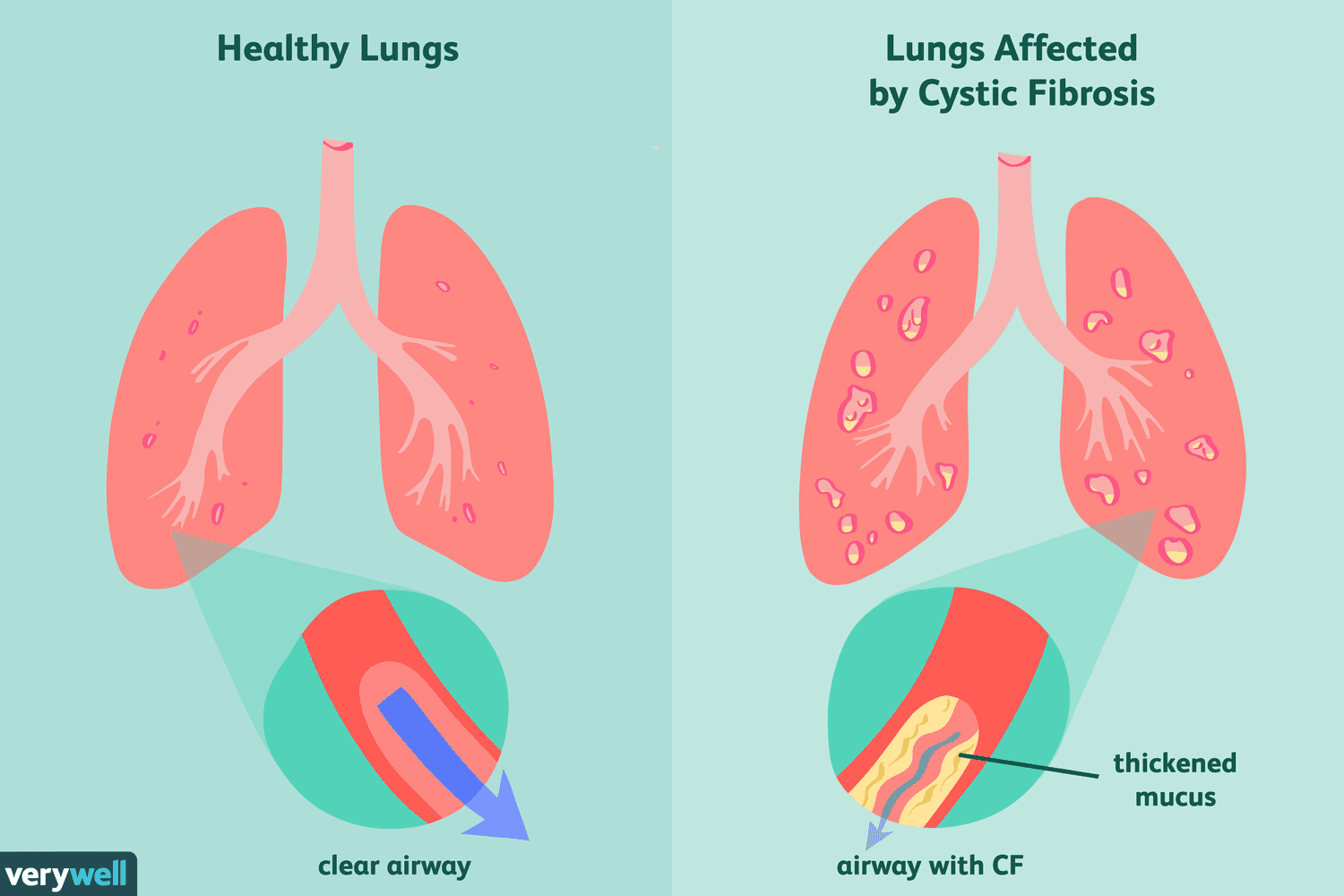
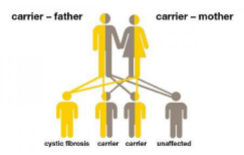
Cystic fibrosis | Cystic Fibrosis definition: – Multisystem autosomal recessive trait disorder Pathophysiology: – Over production of thick mucous resulting in insult to the respiratory, GI and reproductive systems
– The epithelial cells fail to conduct chloride and water transport abnormalities occur – The sweat glands build a larger amount of chloride leading to a salty taste of the skin and alterations in electrolyte balance and dehydration Signs and symptoms • Cough • Recurrent URI • Clubbing (associated with chronic hypoxia) • Barrel chest (indicates air trapping) • Intestinal obstruction • Frothy/foul-smelling stool (steatorrhea) • Failure to thrive Nursing interventions Diagnoses – Positive Newborn screening – Confirmed by sweat chloride test Management – Chest PT – Monitor pulse ox – Administer oxygen as per orders – Medication administration as per orders
– Monitor signs and symptoms of dehydration Diet – High-calorie – High-protein |





https://create.kahoot.it/share/pediatric-respiratory-disorders/a65ee247-30c4-47c6-bd81-2744142e7aa7
peds exam 1 notes
Pediatric Exam 1 Study Guide
KEY: Memorization = blue
Unit 2: Health Promotion: Infant, Toddler, Preschooler, School Age and Adolescent (20 questions) - Review along with the TABLES listed and the Major Theories of Development document. | |
Health promotion | Focuses on maintaining or enhancing the physical and mental health of children Partnership development is the key strategy for success when implementing a health promotion activity. |
Principles of Health Supervision | - Providing services proactively - Optimizing child’s level of functioning - Ensuring child is growing and developing appropriately - Promoting best possible health of child - Preventing injury and illness through child teaching |
Three Components of Health Supervision | - Developmental surveillance and screening - Injury and disease prevention - Health promotion |
Health Promotion | - Growth - Developmental Milestones - Physical Systems Focused - Nutritional Requirements - Anticipatory Guidance - Immunizations ______________________________________________ - Newborn/Infant - Neonate (birth to 27/28 days) - Infant (1 month to 12 months) - Toddler - Preschooler - School Age - Adolescent |
Developmental Changes in the Newborn/Infant *difference between growth, development, and maturation. | Growth ○ increase in physical size (doubles birth weight by 6 months of age and triples birth weight by 12 months of age) Development ○ sequential process by which infants and children gain various skills and functions Maturation ○ increase in functionality of various body systems of developmental skills |
Assessing Newborns and Infants for Developmental Milestones | Nurse may ask the parent if the skill is present or the infant may demonstrate the skill during the assessment The nurse may elicit the skill from the infant Screening tools may be used to assess development: ○ Denver II Developmental Screening Test: a quick screen to determine whether a child is achieving developmental milestones in the areas of gross motor, fine motor, language, and personal social skills. It can be used with children from birth to 6 years of age. ○ Ages and Stages: identifies infants and young children whose social and emotional development requires further evaluation to determine if referral for intervention services is necessary. Example: ○ Learn the Signs. Act Early: From birth to 5 years, your child should reach milestones in how he plays, learns, speaks, acts and moves. (it’s like a CDC website w/ resources) |
Assessing growth and development of a premature infant | Use the infant’s adjusted age to determine expected outcomes
Plot growth parameters and assess developmental milestones based on adjusted age |
Newborn Reflexes: Sucking, Rooting, Grasp, Babinski, Moro, Tonic neck, Dance/step *Know how to assess newborn reflexes and at what age they are expected to disappear | |
Dance/Step
**they are instinctively trying to walk | |
Sucking
**helps latch on to nipple so they can feed | |
Rooting/root reflex
**helps find a nipple to feed | |
Moro
**occurs when they are startled or feel like they are falling | |
Tonic neck/Asymmetric tonic neck reflex
**idk why but they look like superman about to take off. | |
Grasp/Palmar grasp
**motor development and facilitate bonding. | |
Plantar reflex
**motor development also | |
Babinski
**reflects immature corticospinal tract - normal for them before 12 months | |
Infant Milestones TABLE 9.1 (info from this table that is on the study guide) Fine pincer grasp | Posterior fontanel closes by 8 weeks Social smile occurs by 2 months Head turns to locate sounds by 3 months Steady head control is achieved by 4 months Able to roll from tummy to back and from back to tummy by 5-6 months Plays “peek-a-boo” after 6 months Able to transfer objects from hand to hand by 7 months Able to sit unsupported at 8 months Able to crawl at 10 months Waves “bye-bye” at 10 months Fine pincer grasp appears at 10-12 months Able to walk with assistance at 10-12 months Says a few words in addition to “mama” and/or “dada” at 12 months Can sit down from standing position without help at 12 months |
Table 25.3 - Development of gross motor skills in infancy **cruising - walking holding something to support themselves | |
Infant safety | Infant car seat rear facing in the back seat, BACK to sleep, crib rails up, never leave child alone on a raised, unguarded surface, never leave infant alone in bath, fence swimming pools, fence stairways, baby proof the home (keep all medications & household cleaning items high and locked, cover electrical outlets). |
Toddler/Preschooler Milestones Table 11.1 and 12.1 (info from this table that is on the study guide) Bowlegged Potbellied | Temper tantrums are common Appears bowlegged and potbellied (lordosis) Anterior fontanel closed between 12 and 18 months Throws ball overhand by 18 months ⚽ Kicks ball by 24 months Can walk up and down the stairs by 24 months (2 feet on each step) Walks with wide stance at 24 months **things w their feet by 24 mo Feeds self with spoon and cup at 2 years Daytime toilet training can begin by age 2 years Two-to three- word sentences are spoken by 2 years **eating, speaking, and pooping (essentials) accomplished by 2 years Own first and last name can be stated by 2 ½ to 3 years All primary teeth (20) are present by 3 years Three-to four- word sentences are spoken by 3 years Names what has been drawn by 3 years Copies a circle (drawing) with facial figures by 3 years Rides Tricycle by 3 years Stands on one foot for a few seconds by 3 years Uses sentences of four or five words by 4 years Draws 3-part stick figures by 4 years Can walk up and down the stairs using alternate footing by 4 years Can skip and hop on one foot by 4 years Uses sentences of 6-8 words by 5 years Can tie shoelaces by 5 years Throws and catches ball well by 5 years Skates with good balance by 5 years |
Toddler safety: | Leading cause of death in toddlers/preschooler is unintentional injury. MUST focus on safety education. Car seats and booster seats must be used in the backseat of the car at all times. Swimming lessons and Pool fences for drowning prevention Curious about the world around them and like to explore. Accidental poisoning is a safety issue. Use of ipecac syrup is NO LONGER recommended (rapid-acting emetic) → Teach parents that it is NOT recommended to induce vomiting in any way because it may cause more damage. CALL Poison control center. |
School-age and Adolescents Milestones Tables 14.1, 15.1 and 15.2 (info from this table that is on the study guide) | Develops concepts of numbers by 6 years Knows right and left hands by 6 years Likes table games and simple card games by 6 years Uses table knife for cutting meat by 7 years Mechanical in reading by 7 years Can count backwards from 20 by 8 years Likes the reward system by 8 years Puberty: Girls sequence of maturational changes/puberty: can begin anytime between 8-13 years old in this order: breast changes, rapid increase in height and weight, growth of pubic hair, appearance of axillary hair, menstruation 2 years after first signs (breast changes) Boys sequence of maturational changes/puberty: can begin anytime between 9 ½ and 14 years old in this order: enlargement of testicles, growth of pubic hair/axillary hair/hair on upper lip/hair on face, rapid increase in height, changes in larynx causing voice changes, nocturnal emissions ( also known as wet dreams or nocturnal orgasms) |
School age/adolescent safety: | Leading cause of death is unintentional injury. MVA (motor vehicle accidents) refuse to ride with an impaired person or one who is driving recklessly, ALWAYS wear a seatbelt, passenger seat for 12 years of age or older, discourage distractions while driving-cell phones, texting, eating or smoking; if drinking alcohol or any drugs call someone to pick you up, never drive under the influence Learn how to swim and basic water safety rules Ask about depression (sadness, withdrawn) and thoughts of suicide or hurting self/others |
Growth milestones | When does birth weight double? 5-6 months When does birth weight triple? 12 months When does birth length double? 4 years When does a child use scissors? 4 years When does a child tie his/her own shoes? 5 years |
Concepts of bodily injury | Infants: remember pain after 6 months Toddlers: fear intrusive procedures Preschoolers: fear of body mutilation School-age: fear of loss of control over their bodies Adolescent: concerned about change in body image |
Review Pediatric Growth and Developmental Theories: Erikson, Freud, Piaget, Kohlberg FROM BIRTH TO ADOLESCENCE | |
Erikson 1 is a bun - rust colored bun 2 is a shoe - shane is sitting in his auto inside of a shoe 3 is a tree - there is an inn & tia sitting on a tree covered by a quilt 4 is a dinosaur - the dinosaur is dusty and he feels inferior 5 is a skydive - skydiver falls and dents the car and is confused | Trust vs mistrust
Autonomy vs shame and doubt
Initiative vs guilt
Industry vs inferiority
Identity vs role confusion
|
Unit 3: Medication Dosage Calculations (5 questions) | |
Unit 4: Care of the Hospitalized Child (8 questions) | |
Slide 5: Stressors and nursing interventions | Two main stressors seen across age groups: Separation anxiety
Loss of control
|
Slide 17: Autism | What is it?
Occurs in
Etiology
Clinical manifestations
Diagnostic evaluation
Prognosis Early identification and intervention (i.e. therapy) are key Nursing care management
|
Slide 26: Hearing impairment | When caring for a child who is hearing impaired, the nurse should do the following:
|
Slide 28: Visual impairment | Working with a Child who has a visual impairment
|
Slide 29: Nursing assessment of child w/ disability | Nursing assessment of the child with disabilities
|
Slide 37: Minors who may give consent | Emancipated minor - has established independence from his/her parents through marriage, pregnancy, or service in the armed forces, or by a court order. Emancipated minor is considered legally capable of signing an informed consent. |
Slide 38: Legal and ethical considerations of informed consent | |
Slide 44: IV access | Site selection and equipment Provide atraumatic care: use topical anesthetic (for IV access and IM)
Maintenance Complications (requires frequent assessment for infiltration: redness, swelling, leaking) Removal |
Unit 5: Pain Management, Chronic Illness and End of Life (7 questions) | |
Chronic illness | |
Slide 21: Developmental factors | Effect on understanding of death Effect on behavioral response to death Effect on ability to communicate about death By 6 years of age, children recognize death as permanent By ages 9-10, children understanding of death is the same as an adult (inevitable, universal and irreversible) |
Slide 24: Nursing management for child that's dying | Be verbally supportive Do not reinforce denial Do not argue Recognize anger as normal response (do not take it personally) Actively listen, use stillness Encourage expression of feelings Offer spiritual support if appropriate Assist with grieving process and support resources Encourage family to create memories Allow progression through stages of grieving Encourage family participation in care and activities as appropriate |
Pain (5 questions) | |
Slide 9: Pain assessment scales | |
Slide 10: Tools bv age | Neonatal Infant Pain Scale (NIPS)
|
Slide 11: Signs an infant is in pain | |
Slide 12: Face, Legs, Activity, Cry, Consolability (FLACC) | Face, Legs, Activity, Cry, Consolability (FLACC)
|
Slide 13: FACES | Wong Baker FACES Pain Rating Scale
|
Slide 14: Numeric pain scale | Numeric pain scale
|
Summarizing the pain scales | NIPS: Neonatal infant pain scale
FLACC: Face, legs, activity, cry, consolability
FACES
Numeric pain scale
|
Slide 18: opioid SE | |
Slide 20: Non opioid analgesic | Nonsteroidal Anti-inflammatory Agents (NSAID’s):
Acetaminophen
|
Slide 26: Pediatric Pain Pearls | Pain assessment is considered the 5th vital sign. Guidelines are available regarding when you should treat pain. Morphine sulfate is the gold standard for sedation/pain Naloxone is the reversal agent for the opioid agents. Be consistent with using the same pain scale (must be appropriate for age and developmental level). IV narcotics are second witness medications at most institutions. |
Units 6 and 7: Respiratory Dysfunctions (10 questions) ** It is highly recommended that you read the material in the book if you are not understanding any concept from the slides. This will help reinforce learning. | |
Assessing respiratory function in children history | Pattern of Respirations – Rate (rapid (tachypnea), normal, slow (bradypnea)) – Depth (normal, shallow (hypopnea), too deep (hyperpnea)) – Ease (effortless, labored (dyspnea), difficulty breathing except in upright position (orthopnea), retractions → inspiratory or expiratory, nasal flaring) – Labored Breathing (continuous, intermittent, worsening, sudden onset, at rest or on exertion, associated with wheezing, grunting or chest pain) Cough – When is the cough heard (night, early am, daytime) – Nature/character of cough (croupy, wheezy, dry, wet, productive) – Frequency of cough Cyanosis, halitosis (associated with sore throat, lung infections), chest pain |
Effective auscultation | Make certain the child is relaxed and not crying, talking, or laughing. Record if child is crying. Check that room is comfortable and quiet. Warm stethoscope before placing it against skin. Apply firm pressure on chest piece but not enough to prevent vibrations and transmission of sound. Avoid placing stethoscope over hair or clothing, moving it against the skin, breathing on tubing, or sliding fingers over chest piece, which may cause sounds that falsely resemble pathologic findings. Use a symmetric and orderly approach to compare sounds on each side. |
Lung sounds | – Inspiration and expiration (all lung fields) – Wheezing: produced as air passes through narrowed passageways (obstruction) → sounds like high pitched whistling noise. – Crackles: result from the passage of air through fluid or moisture (fluid in lungs) → sounds like popping or crackling |
Acute infectious disorders | |
Nasopharyngitis (common cold) | Common Cold definition: –Viral upper respiratory infection Pathophysiology: –RSV –Influenza –Rhinovirus –Adenovirus Epidemiology • Toddlers get 6-9 colds per year • Immunity increases with repeated exposure to viral organisms and children will get fewer respiratory tract infections Signs and symptoms Fever, Headache, malaise, Nasal congestion, Rhinorrhea (thin watery discharge), Thick and purulent (the color is not an accurate indicator of viral vs bacterial), Nasal blockage, Irritable/restless, Decreased activity, Sore throat, Poor feeding (anorexia), Cough, Muscle aches, Abdominal pain, V/D Nursing interventions No specific treatment, Comfort measures, Antipyretics, Rest, Increase fluids, NO decongestants under 4 years old, Saline + suction Influenza positive? – Antivirals Teaching! –Hand washing , –Elbow cough/sneeze |
Sinusitis | Sinusitis definition: – Bacterial infection of the paranasal sinuses Pathophysiology: – Mucosal swelling – Decreased ciliary movement – Thickened nasal discharge – Young children
– >10 years
Signs and symptoms Greater than 10 days of: – Cough, Nasal congestion, Fever, Halitosis, Facial pain, Irritability, Poor appetite Nursing interventions Antibiotics as ordered, Normal saline nasal spray, Increased fluids, Comfort measures, Teaching → Handwashing & Elbow cough/sneeze |
Pharyngitis & Tonsillitis –aka sore throat and inflamed tonsils Ice collar | Pharyngitis/Tonsillitis definition: – Inflammation of the throat mucosa and/or tonsils Pathophysiology: – Viral process – Group A beta-hemolytic strep (bacterial) – Gonorrhea Signs and symptoms Abrupt onset: Fever, Sore throat, Headache Anterior cervical adenopathy Abdominal pain Tonsils/pharynx with inflammation, redness, exudate, petechiae Strep throat mimics → common cold virus, COVID, flu, croup, mononucleosis, measles, chicken pox Nursing interventions Diagnosis – Rapid strep – Culture Treatment Bacterial
Viral
Nursing care post tonsillectomy Promoting airway clearance
Maintaining fluid volume
Minimize blood loss
Pain management
NPO until child is fully alert and able to swallow
TEACHING
|
Croup syndromes
Toxic appearing child in tripod positioning | ACUTE EPIGLOTTITIS
Bacterial croup – Haemophilus influenza type b Pathophysiology – Inflammation of the epiglottis
Signs and symptoms High fever TOXIC appearing (can indicate shock presenting as lethargy, cyanosis, abnormal breathing, irritability, tachypnea, tachycardia) Tripoding → Leaning forward, Holding body up with hands, Open mouth with chin out Dysphonia → Muffled voice Dysphagia → Painful swallowing Dyspnea → Trouble breathing Drooling Nursing management of epiglottitis Do NOT attempt to visualize the throat (could cause complete obstruction) • Do NOT leave the child unattended • Do NOT place the child in a supine position • Provide 100% oxygen in the least invasive manner • If complete airway occlusion occurs, tracheostomy may be necessary • Ensure emergency equipment is available (resuscitation equipment and suction) LIFE THREATENING • Absence of spontaneous cough • Presence of drooling • Agitation
____________________________________________________ ACUTE LARYNGOTRACHEOBRONCHITIS
Viral croup – Inflammation of the upper airway Pathophysiology – Parainfluenza – RSV – Influenza Characteristic of croup Night-time cough Barky cough Signs and symptoms Monitor for respiratory distress – Inspiratory stridor – Suprasternal retractions – Nasal flaring – Decreased pulse-ox Nursing interventions Home Management such as: – Cool mist vaporizer – Elevate Head of Bed – Shower steam – Keep comfortable – Increase PO fluids Hospital Management – Monitor for respiratory distress – Provide cool mist humidified oxygen – Elevate HOB – Medications as ordered
____________________________________________________ ACUTE SPASMODIC LARYNGITIS aka “spasmodic croup”
|
Acute infectious disorders: Bronchiolitis | Bronchiolitis – Inflammation of the bronchioles Pathophysiology: – RSV – Adenovirus – Parainfluenza Signs and symptoms • Tachypnea • Wheezing • Cough • Rhinorrhea • Sneezing • Difficulty feeding Nursing interventions • Nasal and/or nasopharyngeal suctioning • Frequent respiratory assessments • ?RR <60, O2 sats 90% or > • Positioning • Monitor pulse oximeter • Saline nebulizer • Oxygen as ordered (if O2 sats <90%) • Oral and/or IV hydration • Rarely is inhaled bronchodilator, racemic epinephrine is needed • NO antibiotics • NO cough suppressants |
Respiratory syncytial virus (RSV) bronchiolitis PREVENTION | Palivizumab (Synagis) – Humanized monoclonal antibody – Given IM monthly – Starts at the beginning of RSV season – Maximum of five doses Candidates – Infants born before 29 weeks of gestation – Infants in the first year of life with significant heart disease – Preterm infants (<32 weeks) with chronic lung disease |
Acute infectious disorders: Pneumonia | Pneumonia definition: – Inflammation/infection of the alveoli and the pulmonary parenchymal Pathophysiology: – Viral – Bacterial – Aspiration Signs and Symptoms – Fever – Cough – Tachypnea – Decreased breath sounds – Crackles – Difficulty feeding Nursing interventions • Administer Oxygen as ordered • Administer Antibiotics as ordered • Chest PT • Monitor Pulse Ox • Lay on affected side • Monitor s/s of dehydration |
Acute Non-Infectious Disorder: Foreign Body Obstruction | Foreign Body (FB) Obstruction definition – Occlusion to lungs due to offending object Pathophysiology: – Lodged in the main stem or lobar bronchus Signs and symptoms Cough Gagging Wheezing Stridor (FB is lodged in the upper airway) Asymmetric breath sounds Inability to speak (complete obstruction) Unresponsive (complete obstruction) Nursing interventions Prevention/Teaching – Dangers of certain foods (hotdogs, grapes, round candies, popcorn) – Toy age requirements (beads, small magnets) – Heimlich maneuver (>1 year old) Emergency measures – Activate emergency response – Perform Heimlich maneuver – Place IV – Prepare for endoscopy – X-ray |
Chronic respiratory disorders | |
Asthma | Asthma definition: – Chronic airway inflammation with heightened airway reactivity (smooth muscle spasms and constriction) causing airway obstruction, bronchial hyper-responsiveness and recurring symptoms Status Asthmaticus definition: – Medical emergency – Respiratory distress even with treatment Epidemiology More than 7 million children in the US have asthma Primary cause of school absences Third leading cause of hospitalizations in children under 15 years Signs and Symptoms – Dyspnea: shortness of breath – Wheezing – Chest tightness – Non-productive cough (especially at night and early morning) – Tachypnea – Hypoxia – Prolonged expiration – Retractions – Nasal flaring Triggers Allergens – Outdoor: trees, shrubs, weeds, grasses, molds, pollen, air pollution, spores – Indoor: dust/dust, mites, mold, cockroach, antigen Changes in weather or temperature Irritants – Tobacco smoke, wood smoke, odors, sprays Cold air Animals – cats, dogs, rodents, horses Medications – aspirin, NSAID, antibiotics, beta-blockers Foods – nuts, milk/dairy Nursing intervention Avoid triggers Monitor pulse ox Administer oxygen/medications as per orders – Short acting beta-2 agonist: Albuterol
– Inhaled corticosteroids: Pulmicort (budesonide) or Flovent (fluticasone)
– Systemic corticosteroids: Prednisone (PO) or solumedrol (IV) – Airway Tray available Teaching – Asthma action plan – Medication administration – Avoiding triggers
|
Cystic fibrosis | Cystic Fibrosis definition: – Multisystem autosomal recessive trait disorder Pathophysiology: – Over production of thick mucous resulting in insult to the respiratory, GI and reproductive systems
– The epithelial cells fail to conduct chloride and water transport abnormalities occur – The sweat glands build a larger amount of chloride leading to a salty taste of the skin and alterations in electrolyte balance and dehydration Signs and symptoms • Cough • Recurrent URI • Clubbing (associated with chronic hypoxia) • Barrel chest (indicates air trapping) • Intestinal obstruction • Frothy/foul-smelling stool (steatorrhea) • Failure to thrive Nursing interventions Diagnoses – Positive Newborn screening – Confirmed by sweat chloride test Management – Chest PT – Monitor pulse ox – Administer oxygen as per orders – Medication administration as per orders
– Monitor signs and symptoms of dehydration Diet – High-calorie – High-protein |
https://create.kahoot.it/share/pediatric-respiratory-disorders/a65ee247-30c4-47c6-bd81-2744142e7aa7