HESP 415 Final Exam
Introduction to Intervention 8/28/24
Medical Model of Disability
Deficit-based, biomedical perception of disability. Something is wrong with the body or the mind, we need to make it right to fulfill the ultimate quality of life.
Social Model of Disability
Systemic structures, societal attitudes, and prejudices. Deficits are within society that impact quality of life for disabled individuals and solutions should focus on addressing those systems and attitudes.
The Risks of Ableist Practices
Masking: Therapies and messaging that promote masking of neurotypes have significant consequences on mental health
Suppression: Therapies that train suppression of behaviors can dampen important outlets for stress and dysregulation
Denial of functional resources: Prioritizing neurotypical standards can result in reduced access to technology that can support functional goals
Principles of Intervention
Dynamic (not static):
constantly providing stimuli and analyzing the results
Client considerations:
what helps a participant perform best? How to adjust to their interests, sensory needs
Functional strategies (not isolated skills)
Saying real sounds. Building on things that drive communication
Emphasis on communication
Emphasis on success
Choosing targets and implementing them in the therapy room
Challenge clients and push them out of their comfort zone
Preparation for discharge
We want clients to develop skills and go out into the world without constant help/intervention
Evidence-based practice
Cultural sensitivity
Make sure what the cultural background of the client and their family.
What changes are needed in our therapy
Essential Clinical Skills
Programming
How to program a session
Therapeutic programming of scheduling goals and how to treat them
Behavior Modification
Emphasizing the trust and safety of a client
Teaching Strategies
Skills that need to be supported
How to build upon these skills
Session Design
How to plan our session
How is it structured
Data Collection
Record and report on the client's progress in a session
9/4 - Building Rapport | Treatment Approaches for Articulation
The Clinician-Client Relationship:
Building Rapport and a Therapeutic Alliance
Establishing Rapport
Data Collection
Programming
Behavior
Teaching Strategies
Session Design
Building Rapport
The importance of therapist effects
Clinical factors
Therapist effects vs. intervention
The importance of rapport
Trust, safety, comfort in the therapeutic setting
Session engagement
Motivation and agency
It is the clinician's responsibility to build the relationship between client and therapist
Three main elements:
Interpersonal bond
Agreement between clinician and client, family regarding long-term goals
Agreement between clinician and client/family regarding therapeutic tasks
Interpersonal Bond
Striking the tone
Therapeutic Relationship:
Not personal, is professional
Personal interests
Following leads and establishing boundaries
Building connections and trust
Interest in person
Checking in every day
What are they looking forward to
Body language
Speaking style
Feedback
Agreement on Long-Term Goals
Solicit client priorities
Asking the client what they would like to accomplish
Seeing how the client interacts with their family (if nonverbal)
Solicit family priorities
What are some challenges the client experiences
Create goals that incorporate clinician expertise, the needs of the client, and the desires of stakeholders
Agreement on Treatment Activities
Incorporate interests
Consider client and family preferences
Consistently establish expectations and review rationales
understanding why you are doing a treatment session
Honor family requests
family understand why you are incorporating teaching strategies
listen to family requests - boundaries, preferences of language use, or types of play
Session Dynamics
The pace of the session
Start-up of therapy is successful
Material selection
Proxemics
The client and the clinicians’ literal position from each other
How it allows you to maintain materials
Questions:
When does rapport building start? When does it end?
It starts when you begin therapy and it is ongoing
What are the risks of foregoing rapport-building?
Maintaining trust from therapists - mainly kids
Adults may not know why they are there
May be reluctant to change - adults
How can rapport be restored?
Keeping consistent boundaries so it is easier to get back on track
Refresh the client's goals
Articulation and Treatment Approaches
Nature of Articulation Differences and Disorders
Functional: No known pathology is causing articulation errors
Absence of: hearing impairment, intellectual differences, structural abnormalities, neurological dysfunction
Organic: known physical causes of articulation errors
Presence of hearing impairment, structural abnormalities, neurological dysfunction
Both
Treatment Approaches
Traditional
Motor Kinesthetic
Distinctive Features
Paired Oppositions
Phonological Processes
Cycles Approach
Core Vocabulary
Metaphon
Traditional (Van Riper, 1978)
Sensory perceptual or motor-based approach
Incorporates auditory discrimination, motor placement, and gradual increase in complexity
GILCU: Gradually increasing in length and complexity
Traditional: Sequence
Speech sound discrimination training
a. Identification, isolation, and bombardment
Phonetic placement of the articulators
Producing the sound in isolation
Producing sound in nonsense syllables
Producing sound in initial, medial, and final positions
Producing sound in phrases and sentences
Producing sounds in conversation
Motor Kinesthetic
Emphasizes development of movement patterns
Clinician manipulation of articulators
Prioritizes kinesthetic and tactile feedback
A lot of touch to stimulate feedback between the client
Emphasis on the isolated sound
Distinctive Features
Emphasizes the distinctive features of the targeted sounds for training
Clinician selects a feature for training
Discussion of feature
Auditory discrimination activities
Return to traditional speech production hierarchy (GILCU)
Paired Oppositions
No explicit instruction on placement or production
Minimal or Maximal Pairs
Minimal Pairs: Differ on only one feature (/van/ vs /ban/)
Maximal Pairs: Difer on several features (e.g. /sad/ vs /bad/)
Provide opportunities for natural consequences of mispronunciation and repair in functional activities
Phonological Processes
Based on phonological simplification strategies that begin as typically developing
Does not target individual phonemes but rather entire class of speech errors
Cycles Approach
Intended for individuals with highly unintelligible speech
Determine multiple phonological patterns to be addressed, individually, for a determined amount of time (cycle)
Progression is based on cycle duration, not achieving mastery of speech sound
Internalization of speech pattern even as clinician introduces new targets
Core Vocabulary
SLP selects 50-70 “functionally powerful” words
Up to 10 words are targeted simultaneously
Emphasizes the ability to generate consistent motor plans for words
Clinician provides detailed, specific feedback about the limited number of words
Metaphon
“Philosophy” rather than program
Provides client with explicit information, development awareness, and understanding of detailed aspects of speech sounds to facilitate accurate production.
No specific or corrective feedback
The environment is structure for repeated opportunities for intentional production and repair
Treatment Efficacy and Evidence-Based Practice
There is minimal consensus evidence to indicate one articulation approach is more effective than the other
How do we choose?
Clinical expertise
Client considerations
Dynamic assessment and problem-solving
Remember the importance of clinical factors
9/11 - Programming | CLD Considerations
Programming
The selection and sequencing of specific behaviors for targeting in treatment
Programming Progression
New behavior is introduced
Behavior is taught with maximum structure and prompting
Progress through hierarchy of difficulty and complexity
Client demonstrates generalization of behavior
Plan for discharge
Social Model of Intervention
Does not focus on how to bring the client skills up to typical societal expectations
Identifies ways to modify the attitudes and structures of society to accommodate the client's communication profile
Focuses on reducing barriers to successful communication in the individual's environment or interpersonal relationships
Providing support and modifications to address physical, environmental, and sensory barriers experienced by the client
Therapeutic Targets: First Steps
Analyze assessment data
Review diagnostic findings to determine areas for further investigation
Gather pre-treatment baselines (no prompting/teaching)
Provide a number of stimuli to determine a baseline accuracy
Under 75%…. Over 50%…. Lowest accuracy
Incorporate clinical judgement
Goals and Objectives
Long-term goals: The determined communication behavior(s) to be acquired over the course of the treatment program
Short-Term Objectives: The stepping-stones or collection of behaviors to achieve long-term goals
Selecting Therapy Targets
Developmental/Normative Strategy
Known normative sequences of communicative behaviors are used to inform target selection
The earliest emerging behaviors are selected as the first therapy objectives
Most applicable for children
Client-Specific Strategy
Consider the client's unique needs rather than norms
Frequency of a specific communication behavior in daily activities
Relative importance of the communication behavior
Client's potential mastery of the skill (stimulability)
Stimulability: The client's ability to achieve the communication behavior through imitation
Effective for both pediatric and adult populations
Sequencing Therapy Targets
Developing a logical sequence of steps to accomplish each goal. Involves three factors:
Stimulus type
Task mode
Response level
Stimulus Type: The more explicit and direct a stimulus, the greater the level of support from the clinician
Direct physical manipulation
Concrete Symbols
Objects
Photographs/color pictures
Black and white line drawings
Abstract symbols
Oral language
Written language
Task Mode
Imitation
Cue/prompt
Spontaneous
Response Level (GILCU)
Isolation
Syllable
Word
Carrier phrase
Phrase
Sentence
Text
Complexity Hierarchies
Complexity hierarchies will vary based on population, skill, etc
Modifying level of support
Modifying level of complexity
All should gradually build in independence and functionality
Use pretreatment baselines…
Scores under 50% accuracy: begin at the level of difficulty just below the baseline stimuli
Scores between 50% and 75%: Begin at the same difficulty level as baseline stimuli
Branching: Modifying the difficulty level (branch up, branch down) to achieve a greater level of success
Generalization/Carryover
Programming for transfer of a newly mastered communicative behavior to the everyday environment
Should be incorporated throughout programming
Build variation into therapeutic activities
stimuli
environment
audience
Termination of Therapy
Discharge is based on clinical judgement
Consider
Attainment of skills that are commensurate with chronological, developmental, or premorbid status
Attainment of communication skills that permit functioning in their daily environment
Lack of discernible progress beyond a predetermined time period
How many black/POC are in this field?
About 3% black SLPs
Racial Concordance
The matching of patient/client and clinician across cultural variables
In primary care relationships, racial concordance is connected to increases in..
Client-clinician communication
client participation
information-giving
improved show-rates
overall satisfaction
In the absence of concordance
All clinicians need to be intentional about prioritizing:
Cultural Competence
Ongoing self-assessment, continuous cultural education, openness to others’ values and beliefs, and willingness to share one's values and beliefs
Cultural Responsiveness
Understanding and appropriately including and responding to the combination of cultural variables and the full range of dimensions of diversity that an individual brings to interactions
Cultural Humility:
“A personal examination of one's own beliefs and cultural identities to better understand the beliefs and cultural identities of others”
Cultural Dimensions
Family Life
Child-rearing practices
Education
Employment
Health Care Practices
Value Orientations
Verbal Communication
Nonverbal communication
Relational Communication Norms
Cultural Dimensions and the Individual
Cultural Dimensions exist on a continuum that will look different for each individual
Emphasize ethnogenetic views: Groups, cultures, and their individuals are fluid and complex
Being mindful of essentialism: Defining whole groups as essentially different, without regard for variations
Unlearning Ethnocentrism
Belief that your habits or viewpoints are superior
Willingness to approach all beliefs with flexibility
Acknowledging impacts of long-standing value systems
Monitoring for microaggressions
Responsiveness vs. Stereotyping
Consider how norms and values are uniquely shaped
Monitor for preconceptions of a particular population
Come prepared with cultural competence, adjust and nuance with cultural responsiveness
Difference vs. Disorder
A speech-language disorder..
Impacts storage, retrieval, and/or execution of behaviors related to communication
Results in a communication breakdown that is sufficient to negatively influence the effective communication in the language used by the speaker
A difference…
Reflects a variation of the behaviors which are rule-based, not disordered
May result from cultural variables impacting a variety of behaviors
May vary in degree based on exposure, assimilation, and acculturation
Pursuing a Culturally Responsive Practice
Solicit resources to build cultural competence
Differences across cultural dimensions in a particular population
Seek out support from other professionals who share concordance with your client
Establish a sensitive and responsive rapport with your client to ask questions and receive feedback on cultural dimensions
Mindful creation and modification of materials and therapeutic activities
9/18 - Behavioral Objectives
Goals vs. Objectives
Long Term Goals (LTG)
Written with the overall skill in mind
May not have a stated criterion
Short Term Objectives
The necessary sub-skills to achieve the LTG
May work in a gradual approximation of the LTG
May include a collection of steps in any order
Anatomy of an Objective
Given no more than verbal prompts, client will produce /s/ in initial position of words with 80% accuracy over two consecutive sessions
Condition: what support will be provided (“Given Statement")
Task: what will the client do
Criterion: the success level and time element (timing is optional)
Importance of an Objective
Allows the client and clinician to know
The exact therapy target
How it is to be accomplished
What defines successful performance
Allows new clinicians to implement programming immediately
Condition
The situation in which the target behavior will be performed
Specifies…
When the behavior will occur
Where it will be performed
In whose presence
Materials to elicit the target
Prompting to elicit the target
Important consideration for
generalization
independence
functionality
"Do” Statement
The specific action the client is expected to perform
Use terminology that is observable and measurable
Will I be able to tally when the behavior occurs?
Determines the action that will be measured through data collection
Do's and Not Do's
Do's
Point
Say
Label
Write
Name
Ask
Vocalize
Not Do's
Learn
Know
Remember
Apply
Comprehend
Improve
Understand
Criterion
How successfully the target behavior must be performed to achieve the objective
May specify
Ratio/percentage of “correct” or successful responses
Minimum number of successful responses
Maximum number of errored responses
Within a given time period
Examples
99% accuracy
8 out of 10 trials
Less than four errors over three consecutive sessions
80% accuracy over two consecutive sessions
Continuously over a 2-minute period
SMART Goals
Good objectives with a snappy title
Specific
Measurable
Achievable
Relevant and Realistic
Time based
Early Childhood Language
The Intentions of Early Intervention
Emphasize family involvement and education
Promote participation in the natural environment
Integrate multiple disciplines and lanes of development
Primary therapy strategies highlight authentic learning experiences and modeling/stimulation
Prelinguistic and Early Language skills
Localization: turning toward and visually searching for the source of a sound
Joint/Shared Attention: directing attention to a shared object, event, or individual
Mutual Gaze: eye contact between child and caregiver
Joint Action and Routines
A predictable play sequence with a clear progression of events
Facilitates anticipation by the child and increases the potential for successful interaction
Supports first interactions, turn-taking, role shifting
Communication Behavior Progression
Intentional Gestures
Movement of the body with the intent to be understood
Head shake, reach, raising arms up
Vocalizations
Reflexive → Cooing → Vocal play, laughter → Babbling → Jargon and Protowords
Symbolic communication
Consistent, intelligible signing
Words or word-approximations
Other symbols (photographs, line-drawn symbols)
Communicative Intentions
The meaning that the speaker wishes to convey
Preverbal
Attention Seeking
Requesting
Greetings
Protesting
Responding
Informing
Single-Word Level
Naming
Commenting
Requesting (object, action)
Responding
Protesting
Attention seeking
Greetings
The Importance of Play
Children learn and practice through play
Development of social communication skills and natural language learning
Nonsymbolic Play
Exploratory: dropping, mouthing, transferring
Functional: Using an item for its intended purpose as well as gross motor play
Symbolic Play
Substitution of objects, assigning roles
First Lexicon
Typical lexicons are based around social and physical events that are understandable and in the immediate environment
Choosing targets:
Words that can be used in many different contexts within the child's day
Words that are important to the child
Words that represent references that can be acted on or manipulated
Tier 1: Common, everyday words that most children known before entering school
Tier 2: Academic vocabulary that is common across all topic areas, but not part of everyday social language
Tier 3: Low-frequency, subject-specific words
Intervention for Birth-3 Intervention
Capitalizing on natural contexts for skill development
Creating natural contexts for skill development
Utilizing predictable routines
Imitating the child's behavior
Mirroring back vocalizations; playing their way
Flooding of the target (vocabulary, skill)
Incorporating family and key caregivers
Supporting for necessary changes in caregiver behavior
Intervention for Infants, Toddlers, and Pre-K
Focused Stimulation
Incidental Teaching
Floortime/Developmental Individual-Difference Relationship (DIR) Based
Family Centered
Focused Stimulation
Clinician provides concentrated exposure to a linguistic target form in a variety of contexts
High concentration throughout natural and meaningful interactions
Child is not required to imitate or produce
Can target vocabulary, grammatical morphemes, syntax
Can be included as individual words, within sentences, or in short stories
Incidental Teaching
Naturalistic approach encourages child to initiate communication by arranging the environment to increase the likelihood they will produce the targeted behavior
Verbal or non-speaking communication behaviors
Natural consequences as rewards
Clinician may respond to communicative attempts with models for expansion or elaboration
Floortime/DIR
Building foundations for social, emotional, and intellectual capacities
Does not target isolated skills
Emphasis on developmental milestones and individual differences
Highlights relationship between child and others in the environment
Family engagement is critical
Family Centered
Trains parents and caregivers to foster development of language and communication in natural settings
Family members are the “agents of change"
Building and responding in mutually reinforcing communicative interactions
SLP is an indirect support during interactions with heavy focus on parent education
Can be utilized to target variety of speech and language skills
9/25 - Behavior Modification | School-Age Language
Behavior Modification Intentions
Intended for:
Developing new speech, language, and communication behaviors
Increasing likelihood of success
Improving relationship and therapeutic alliance
Not intended for:
Maintaining control
Meeting NT expectations
Keeping materials or space clean and tidy
Establishing compliance
Tolerating non-preferred tasks or environments
Terminology
Operant Conditioning: Utilizing the relationship between a stimulus, response, and consequent event
Stimulus: An event that precede and elicits a response
Response: The behavior that is exhibited by the individual on presentation of the stimulus
Consequence: An event that immediately follows the response
Reinforcement: Consequences that increase the probability that a particular behavior will recur
Reinforcement and Punishment
Positive Reinforcement: The addition of a reward consequence that it is intended to increase the likelihood of a behavior
Negative reinforcement: The removal of an aversive consequence that is intended to increase the likelihood of a behavior
Punishment: The addition of an aversive consequence or removal of reward consequence intended to decrease the likelihood of a behavior
Positive Reinforcement: Reinforcement
Primary Reinforcers: Contingent events that are favorable due to the biological need or physiologic predisposition of the individual
Secondary Reinforcers: Consequences that must be perceived or interpreted as rewarding
Social
Token
Performance feedback
Negative Reinforcement: Reinforcer Types
Escape: Requires the presence of a condition that is perceived as aversive
Avoidance: A performance of the behavior prevents the occurrence of an anticipated aversive condition
Punishment: Types
Type I: Presentation of an aversive consequence after a unwanted behavior is exhibited
Type II: Withdrawal of a pleasant condition after an unwanted behavior is exhibited
Reinforcement Schedules:
Continuous: 1:1 reinforcement
Helpful for shaping new communication behaviors
Can be utilized for transitioning a skill to a greater level of difficulty
Not sustainable for long-term
Intermittent: Lower density reinforcement based on number of executions or duration of a behavior
Effective in strengthening responses, promote maintenance
More sustainable in creating behaviors less susceptible to extinction
Intermittent Reinforcement: Types
Fixed Ratio
Fixed Interval
Variable Ratio
Variable Interval
Behavior Modification and ND Populations
If expectations can be met without disconnection, set them!
ND Populations present with variations in preferences, regulation, and past experiences
Do not withhold contingent rewards that are used/can be used to establish regulation
Be mindful token reinforcement systems
Analyze your session design and response styles to ensure you are serving the needs of your client, not the needs of the clinician
School-Age Language and Literacy
Characteristics of Students Ages 5-10
Oral Language Development:
Vocabulary increases in size and depth
Utterance length increases
Changes in syntactic growth
Metalinguistic awareness
Reading Development:
Decoding: Knowledge of letter-sound correspondence
Word Recognition and Fluency: Rapid, automatic identification of written words
Comprehension: Processes by which print language is understood
Writing Development:
Spelling: The forming of words from letters
Written Composition: Writing at the text level
Writing Process Development:
Planning: Generating and organizing ideas
Drafting/Composing: Putting ideas into words/text
Revising: Reviewing and evaluating text
Editing: Polishing flow and format
Characteristics of Students Ages 10-18
Early Adolescence (10-14): Promote communication skills for academic and personal-social purposes
Mid-Adolescence (14-16): Promote communication skills for vocational purposes
Late Adolescence (16+): Promote communication skills for career purposes
Communication skills are refined
Development of higher-order language abilities
Growth in the metalinguistic area of figurative language
Develop conversational maturity
Increase the length of utterance
Increased comprehension and production of complex sentences
Advances in written language
Development of metacognitive and executive functioning abilities
Language Learning Disabilities
Overflow impact of language-learning differences in writing products, including:
Lack of planning
Reduced use of background knowledge
Lack of revision and editing
Reduced sense of audience
Reduced sentence complexity
Grammatical and punctuation errors
Intervention for School-Age and Adolescents
Developmental → Functional
Goals and objectives will begin to transition to more functional application
Consider program goals that incorporate demands and expectations of the educational curriculum
Oral Language x Literacy: As needs begin to impact academic progress, a greater focus on this relationship is necessary
Service Delivery:
Pull-out | Push-in | Consultation and collaboration
Shocking: No one delivery model is best!
Treatment Approaches
When the transition is made from developmental programming to functional, treatment approaches will emphasize deeper interaction with content and planning; habit-building; and compensatory strategies
Previewing: Planning strategy for oral and written texts
Examples of Oral Participation:
Topic identification; vocabulary; brief synopsis
Examples for written text:
Section headings; captions
Predicting: Use of subject matter knowledge to:
Make predictions about content and vocabulary
Check comprehesion
Think-Aloud : Students engage in self-talk throughout the learning task to improve comprehension/monitoring of oral and written material
K-W-L Procedure : Focuses on comprehension of oral and written language
K = what we KNOW
W = What we WANT to know
L = What we have LEARNED
Metacognitive Stems : Students are provided with a structure to improve their organization for completion of an assignment
Discussion-Oriented Approach: Whole classroom or groups talk about word meanings in a conversational context
Social Stories :
Focus on improving pragmatic language skills
Clinician develops written or pictorial scripts that explain appropriate communication interaction behaviors in given social situations
Computer-Driven Therapy: Use of personal computers to present therapeutic stimuli and feedback
10/2/24 - Teaching Strategies | Autism
Teaching and Scaffolding Strategies
Direct Modeling
Indirect Modeling
Shaping
Prompts
Fading
Expansion
Recast
Negative Practice
Target-Specific Feedback
Teaching Strategies: Direct Modeling
The clinician demonstrates a specific behavior to provide an exemplar for the client to imitate
Beneficial for early stages of therapy
Also utilized for shifting to a higher response difficulty
Provides maximum support by the clinician
Minimizes likelihood of errored responses
Teaching Strategies: Fading
The stimulus or consequence manipulations (e.g. modeling, prompting, reinforcement) are reduced in gradual steps while maintaining the target response
Initiated once a client is able to produce some consecutive correct responses at imitation
Process
Increase number of client productions following one model
Decrease length of model provided by clinician
Teaching Strategies: Prompts
The clinician provides additional verbal or nonverbal cues to facilitate a client's production of a correct response
Attentional: Cues to improve performance by focusing a client's concentration on the task
Instructional: Provide information directly related to the specific target behavior
Verbal reminders (“Remember to keep your tongue behind your teeth”)
Nonverbal reminders (A signal to adjust loudness)
Teaching Strategies: Shaping by Successive Approximation
A target behavior is broken down into small components and taught in an ascending sequence of difficulty
Utilized when a direct model of a complete behavior is insufficient
Each successive step moves progressively closer to the final form of the desired response
Teaching Strategies: Negative Practice
The client is required to intentionally produce a target behavior using a habitual error pattern
Facilitates learning by highlighting contrasts
Implemented after a client demonstrates capacity to produce the behavior consistently with imitation
Powerful on a short-term basis
Teaching Strategies: Target-Specific Feedback
The clinician provides information regarding the accuracy or inaccuracy of a client's response
Useful throughout all phases of therapy
Three primary functions
Provides precise information regarding why or how a response was correct
Maintains client's awareness of the exact response being targeted
Maintains client's focus on the target during a therapy activity
Teaching Strategies: Indirect Modeling
The clinician demonstrates a specific behavior frequently to expose a client to numerous well-formed examples of the target behavior
Can be employed at any stage in the therapy process
Increase exposure to positive speech, language, or communication behaviors
Not intended to elicit immediate responses
Teaching Strategies: Expansion and Recasting
The clinician reformulates a client's utterance into a more mature version (expansion) or difference sentence type (recasting)
Primarily used in language and communicative therapy
Increase exposure to positive speech, language, or communication behaviors
Teaching Strategies: Homework
Assigned to strengthen the response and facilitate generalization outside of the clinical setting
Should target an existing skill
Client should be able to evaluate their own performance
Assigned in manageable amounts
Assigned on a regular basis
Should include written instructions
Autistic Learner: Sensory Processing
Basic Senses
Auditory, Visual, Gustatory, Tactile, Olfactory
Invisible Senses
Vestibular: Sense of body in motion across a variety of planes (via semicircular canals)
Proprioceptive: Sense of body movements in relationship to one another (via stretch receptors in joints)
Interoception: Sensations related to internal body states (via organs)
Threshold: The level of input at which the sensory system registers and/or responds
Low Thresholds: May result in over-reactivity, frequent responses to stimuli, frequent distraction or loss of regulation
High Thresholds: May result in missing important cues or information about the environment
Purposes of each sensory system
Arousal (or alerting): To generate awareness
Discrimination (or mapping): To gather information to make maps of self and environment
Active Self-Regulation: The individual actively controls input to establish equilibrium
Passive Self-Regulation: Allows changes to environment and responds
Common Sensory Characteristics:
Sensitivity to touch, auditory, and oral sensory input
Low registration of environment until threshold, then resulting in overwhelm
Use of repetition and rituals to establish comfort to reduce triggering of lower thresholds
Interventionists (with the support of an OT) will need to learn the sensory profile of the individual to provide both alerting and calming stimuli to support trust, safety, and participation
Autistic Learner: Sensory Patterns
Seeking: High thresholds, active self-regulation, independently incorporate movement, touch, sound, and visual stimuli in their activity.
Low Registration: High thresholds, passive self-regulation. Do not actively seek changes to input, can appear withdrawn
Sensitive: Low thresholds, passive self-regulation. Easily disrupted and distracted by change that does not go unnoticed
Avoiding: Low thresholds, active self-regulation. Independently attempt to reduce input. May be resistant to participation
Autistic Learner: Cognitive Differences
Memory for complex material (scenes, stories)
Working memory (maintaining information for execution)
Concept formation (insight, judgment)
Face recognition
Executive functioning
Response to social consequences
Managing abstract concepts, such as time, unspoken rules
Autistic Learner: Mental Health
Reduce stress and demands by following the client's lead
Allow ample wait time over the course of an interaction, a session, an episode of care, to build trust and opportunity for initiation
Know your client's history with therapy and behavior interventions
Autistic Learner: Supports for Intervention
Incorportation of preferred sensory input: Create an environment that is conducive to the seeker, not punitive
Modulation of aversive sensory input: Monitor for aversive lighting, smells, auditory input. Prevent the need for avoidance
Utilze visual supports: Support for receptive language differences, preparation and frontloading, social stories
Utilize visual schedules: Support for impacted skills such as time-blindness, prediction, insight
Autistic Communicator: Social Differences
Impacted joint attention
Delayed pointing and use of gestures
Stereotypical play
Impacted perspective-taking (Theory of Mind)
Autistic Communicator: Language Development
Aberrant vs. Delayed: Language development may follows an atypical pattern
Use of immediate and delayed echolalia
Less-robust communicative intents
Difficulty interpreting nonverbal communication
Difficulty with higher-order language skills
Topic maintenance
Inferencing
Figurative language
Presupposition
Autistic Communicator: Echolalia
Echolalia: The partial or full repetition of the speech of others
A hallmark characteristic to autism (although not unique to autism)
May also be referred to as gestalts or scripts
Noteworthy in their adherence to melody and intonation
Characterized by timing:
Immediate: The repetition occurs immediately after perception
Delayed: The script is retained and produced at a later time
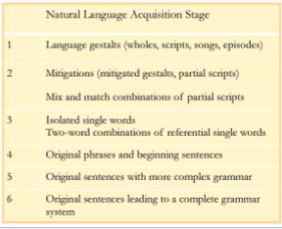
Autistic Communicator: Natural Language Acquisition
Natural Language Acquistion: The process of acquiring language in entire units, marked by natural boundaries (a breath, a pause, an end of an episode) and coded by experience
Individuals exhibiting signs of NLA (Gestalt Language Processors) will be slow to respond to therapy techniques that are based in analytical language processes
At any given time, a GLP individual may utilize utterances that represent different a variety of stages
Supporting GLPs in Early Stages:
Investigate the meaning of existing gestalts
Acknowledge all gestalt use as meaningful, even during the investigative phase, to build trust and reciprocity
Respond to current gestalts with a mitigated close relative
Reuse mitigations with a variety of “chunks”
Provide redundant models of new gestalts that are easily mitigated
Utilize rich intonation and stimulating, emotional contexts to support imprinting
Allyship: Mind Your Language
Rebuke deficit-based language and sweeping generalizations
Be mindful of word-choice and messaging that implies blame, lack of effort, or a conniving nature of the individual
He can do it, he just won't
They're just being lazy
She's manipulating you
Avoid “leveling” and functioning labels
Allyship: Disrupt NT Standards
We can support autistic individuals to develop skills that will help them establish joyful communication and participation in predominantly NT communities, without:
Disrupting play preferences
Interpreting with self-regulation attempts
Enforcing uncomfortable boundaries
Rebuking special interests
We can support NT communities to develop skills that will help them establish joyful communication and participation with autistic individuals
Provide counseling and support to families
Provide education to stakeholders on the micro and macro level
Encourage changes to environment and caregiver responsiveness
10/9 - Midterm Review
Sequencing Therapy Targets
Developing a logical sequence of steps to accomplish each goal. Involves three factors:
Stimulus Type
Task Mode
Response Level
The therapy target is what you are taking data on
Stimulus type: the more explicit and direct a stimulus, the greater the level of support from the clinician
Direct physical manipulation
Concrete symbols
Objects
Photographs/color pictures
black and white line drawings
Abstract symbols
Oral language
Written language
Task mode: how the therapy activity is designed
Imitation: Client repeats what is said
Cue/prompt: Provide an instruction/something that stimulates a behavior
Spontaneous:
Response Level
Length and Complexity (GILCU)
Isolation
Syllable
Word
Carrier Phrase
Phrase
Sentence
Text
Response Latency: how long it takes for the client to give a response
10/23/24 - Materials Selection | Aphasia and TBI
Material Selection
The vehicle of you therapeutic task
The most-likely determinant of stimulus type
Commercial materials
Therapeutic
Recreational
Created materials
Materials Considerations
What You Use
Consider client profile
Age
Developmental level
Language level
Foster engagement
Promote generalization
How You Use It
Address the target
As is
With clinician mods
Permit branching
Promote high frequency of targets
Can incorporate additional stimuli
Material Use
How do we put materials to use to accomplish therapeutic targets:
Use as directed
Incorporate additional demands or stimuli
Create the materials we need
Material Use: Use as Directed
Highlight the communication target that is naturally stimulated or easily prompted when interacting with the material
Material Use: Incorporating Additional Demands
Earn Your Turn
After 10 accurate productions of /s/ at word level, take your turn in Trouble
Incorporate a Target
Use past tense marker -ed to describe the turn (“You moved 2 spaces”)
Support a Functional Target
Engineer opportunities to demonstrate a social target (advocacy sportsmanship, compliments, etc)
Material Use: Creation
Create materials specific to the client's needs and preferences
Finding and Creating Materials
ChatGPT
Search Engines
Pinterest
Teachers Pay Teachers
Interactive sites
Closets
CLD Considerations
Exercise cultural sensitivity
Do not assume holiday observations or traditions
Be mindful of current events
Use materials and stimuli that are representative
Toys
Books and other media
AAC and visual supports
Resist poor or stereotypical representations
The Last Word
Consider the pictured material:
Determine a use for the material in treatment
The last student to contribute wins
Aphasia and TBI
Aphasia
A language disorder due to brain damage that results in impaired comprehension and/or formulation of language
Can impact both spoken and written modalities
May co-occur with motor impairments
Hemiplegia or hemiparesis
Hemianopsia
Possible Etiologies
Hemorrhage or blockage of blood flow to the brain
Strokes/cerebrovascular accidents (CVA)
Tumors
Head trauma
Certain disease processes
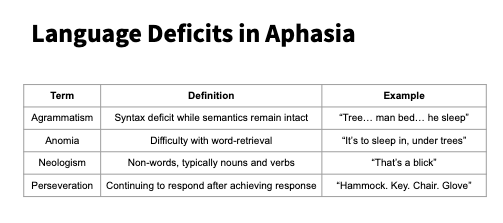
Classification of Aphasia Symptoms
Nonfluent Aphasia: Poor verbal/written output with relatively spared comprehension
Reduced vocabulary
Agrammatism
Impairments of articulation, rate, and prosody
Labored and effortful production
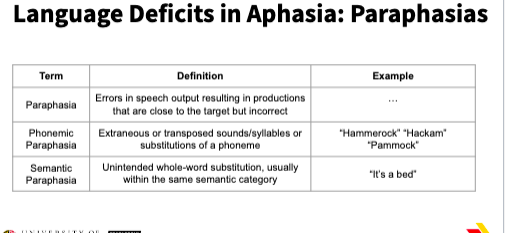
Fluent Aphasia: Impaired language comprehension with maintenance of normal melodic speech contour
Word-retrieval deficits
Paraphasias
Neologisms
Perseveration
Melodic, natural quality to speech production
Nonfluent Aphasias
Broca's: Agrammatism, effortful articulation of short utterances, impaired prosody and intonation, apraxia of speech, good comprehension
Transcortical Motor: Little to no initiation of spontaneous speech, but excellent imitation. Good comprehension
Global: severe deficits in all areas of language comprehension and production
Fluent Aphasias
Wernicke's: Fluent but meaningless speech articulation, intonation, and prosody are good. Comprehension is impaired.
Conduction: relatively fluent speech, frequent phonemic paraphasias, marked difficulty with imitation. good comprehension
Anomic: Significant word-finding difficulties with otherwise fluent and grammatical speech. good comprehension
Spontaneous Recovery
Occurs if at all, to the greatest extent during the first two to three months post injury/insult
Influenced by several factors
Lesion characteristics (size, location, etiology)
Type and severity of initial aphasia
Age at onset
Overall premorbid health
Prognosis is more favorable for younger clients without additional medical concerns
Neuroplasticity
The brain's ability to restructure its neural networks in response to internal and external stimuli
Neural regions adjacent to the lesion may adopt functions of the affected area
Right-hemisphere sites that parallel the affected left hemisphere may take over functions of the affected area
Neuroplasticity is a key theoretical underpinning to therapy and rehabilitation for patients with acquired neurological impairments
Intervention Timing
Delayed option: initiating treatment once the effects of spontaneous recovery have likely run their course
Early Intervention: Initiating treatment close to onset/injury to accelerate the natural process of spontaneous recovery
Delayed treatment has not been shown to improve treatment effects.
Most clinicians will recommend early intervention
Positive Indicators for Treatment
Age: Individuals under 65 make greater gains in therapy
Intensity: A total of 20-50 intervention hours resulted in better outcomes
Duration: Continuation beyond a 4-week episode of care results in better outcomes
Maintenance: longer-term gains were noted for individuals with milder aphasia symptoms and no deficits in executive functioning