topic 11
Ergogenic – to increase work, especially to increase potential for work output
Nutritional Agents:
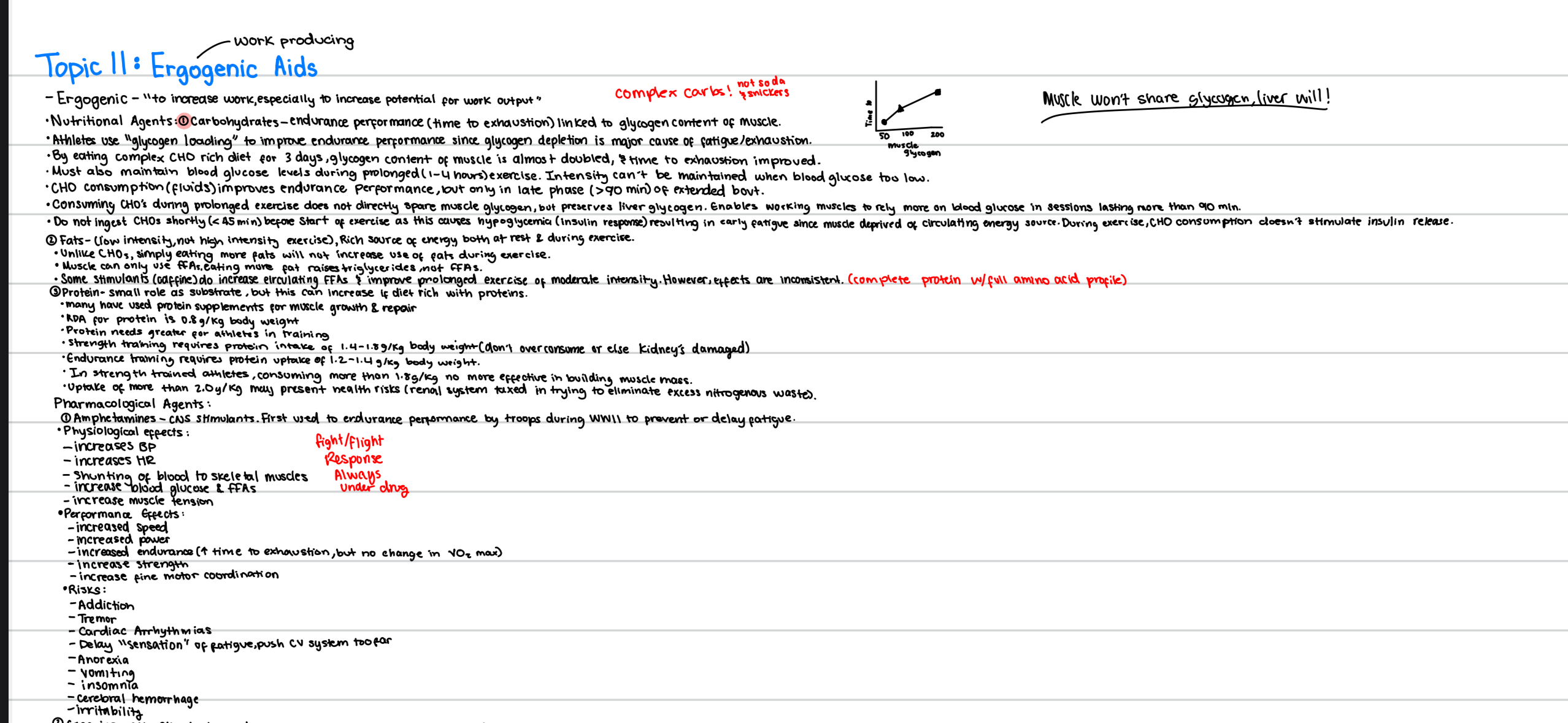
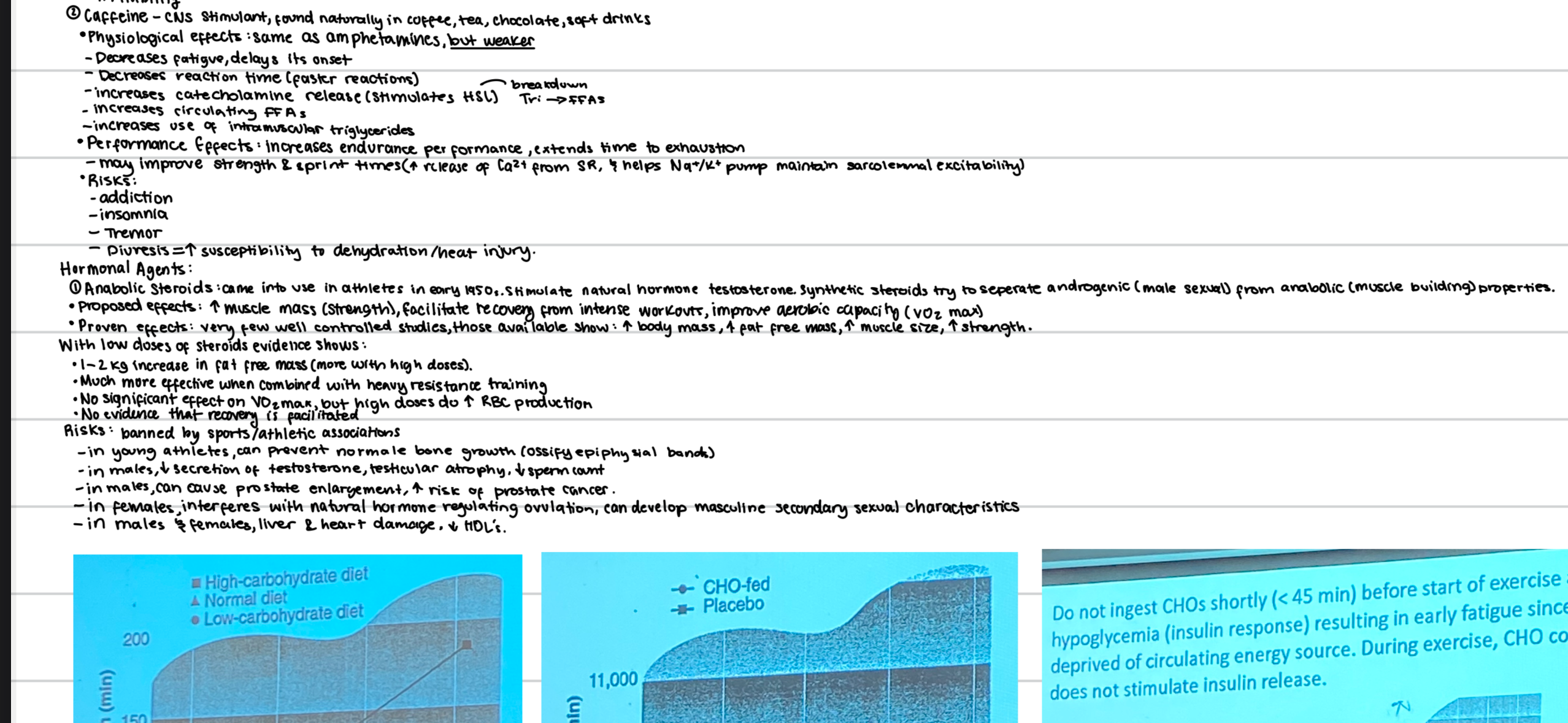
🍞 Carbohydrates – endurance performance (time to exhaustion) linked to glycogen content of muscle.
Athletes use "glycogen loading" to improve endurance performance since glycogen depletion is a major cause of fatigue/exhaustion.
By eating complex CHO rich diet for 3 days, glycogen content of muscle is almost doubled, and time to exhaustion improved.
Must also maintain blood glucose levels during prolonged (1–4 hours) exercise. Intensity can’t be maintained when blood glucose is low.
CHO consumption (fluids) improves endurance performance, but only in late phase (>90 min) of extended bout.
Consuming CHOs during prolonged exercise does not directly spare muscle glycogen, but preserves liver glycogen. Enables working muscles to rely more on blood glucose in sessions lasting more than 90 min.
Do not ingest CHOs shortly (<45 min) before start of exercise, as this causes hypoglycemia (insulin response), resulting in early fatigue since muscle deprived of circulating energy source. During exercise, CHO consumption doesn’t stimulate insulin release.
🥑 Fats – (low intensity, not high intensity) exercise. Rich source of energy both at rest & during exercise.
Unlike CHOs, simply eating more fats will not increase use of fats during exercise.
Muscle can only use FFAs. Eating more fat raises triglycerides, not FFAs.
Some stimulants (e.g., caffeine) do increase circulating FFAs & improve prolonged exercise of moderate intensity. However, effects are inconsistent. (complete protein w/ full amino acid profile)
Protein – small role as substrate, but this can increase if diet rich with proteins.
Many have used protein supplements for muscle growth & repair.
RDA ( recommended dietary allowance) for protein is 0.8 g/kg body weight.
Protein needs greater for athletes in training.
Strength training requires protein intake of 1.4–1.8 g/kg body weight (don’t overconsume or else kidneys damaged)
Endurance training requires protein uptake of 1.2–1.4 g/kg body weight.
In strength trained athletes, consuming more than 1.8 g/kg no more effective in building muscle mass.
Uptake of more than 2.0 g/kg may present health risks (renal system taxed in trying to eliminate excess nitrogenous waste).
Pharmacological Agents:
1) Amphetamines – CNS stimulants. First used to enhance endurance performance by troops during WWII to prevent or delay fatigue.
Physiological effects:
↑ BP
↑ HR
Shunting of blood to skeletal muscles
↑ blood glucose & FFAs
↑ muscle tension
Fight/Flight Response – Always Under Drug
Performance effects:
↑ speed
↑ power
↑ endurance ( ↑ time to exhaustion, but no change in VO₂ max)
↑ strength
↑ fine motor coordination
Risks:
Addictive
Tremor
Cardiac arrhythmias
Delay "sensation" of fatigue, push CV system too far
Anorexia
Vomiting
Insomnia
Cerebral hemorrhage
irritability
2) Caffeine – CNS stimulant, found naturally in coffee, tea, chocolate, soft drinks.
Physiological effects: Same as amphetamines, but weaker
↓ fatigue, delays its onset
↓ reaction time (quicker reactions)
↑ catecholamine release (stimulates HSL) → breakdown of tg into FFAs
↑ circulating FFAs
↑ use of intramuscular triglycerides
Performance effects:
↑ endurance performance, extends time to exhaustion
May improve strength & sprint times (↑ release of Ca²⁺ from SR; helps Na⁺/K⁺ pump maintain sarcolemmal excitability)
Risks:
Addiction
Insomnia
Tremor
Diuresis (inc production of urine)→ ↑ susceptibility to dehydration/heat injury
Hormonal Agents:
1) Anabolic Steroids
Came into use in athletes in early 1950s. Stimulate natural hormone testosterone.
Synthetic steroids try to separate androgenic (male sexual) from anabolic (muscle building) properties.
Proposed effects:
↑ muscle mass (strength), facilitate recovery from intense workouts, improve aerobic capacity (VO₂ max)
Proven effects:
Very few well-controlled studies, those available show:
↑ body mass
↑ fat-free mass
↑ muscle size
↑ strength
With low doses of steroids, evidence shows:
1–2 kg increase in fat-free mass (more with high doses)
More effective when combined with heavy resistance training
No significant effect on VO₂ max, but high doses do ↑ RBC production
No evidence that recovery is facilitated
Risks:
Banned by sports/athletic associations
In young athletes, can prevent normal bone growth (ossify epiphyseal bands)
In males, ↓ secretion of testosterone, testicular atrophy, ↓ sperm count
In males, can cause prostate enlargement, ↑ risk of prostate cancer
In females, interferes with natural hormone regulating ovulation, can develop masculine secondary sexual characteristics
In males & females, liver & heart damage, ↓ HDL’s
2) Human Growth Hormone (HGH)
Naturally secreted by pituitary gland. Once had to be obtained from cadavers. Since 1985, can be produced with recombinant DNA technology; use among athletes begins.
Proposed Effects:
Stimulates protein synthesis & muscle growth
Elongation of long bones in young athletes
↑ lipolysis leading to ↓ body fat + ↑ circulating FFAs
↑ blood glucose (prevents glucose uptake by liver & stimulates gluconeogenesis)
Improved healing from musuloskeletal injury
Proven Effects:
In older men (without training): ↑ fat-free mass (9%), ↓fat mass (14%), bone density ↑(2%)
In young men (with resistance training): ↑ fat-free mass, whole body protein synthesis ↑
→ No significant impact on muscle size, muscle protein synthesis, or strength.
Risks:
Acromegaly (bones thicken after fusion of growth plates)
Internal organs enlarge
Cardiomyopathy:a disease of the heart muscle. It causes the heart to have a harder time pumping blood to the rest of the body
Hypertension
Type II Diabetes
→ ex. Andre the Giant (7ft, 500lbs)
Physiological Agents:
1) Blood Doping
Athlete's total volume of RBCs increased with infusion of his own blood (autologous) or with another person's with same blood type (homologous).
Whole blood (≈1 liter) removed, stored refrigerated, & infused shortly before endurance event.
Must wait 5–6 weeks (time needed for body to produce new RBCs) before infusing blood, so that total # of RBCs is higher.
Proposed Effects:
↑ O₂ carrying capacity of blood
↑ VO₂max
↑ endurance performance
Proven Effects:
Research shows that with proper volume of blood & waiting period, VO₂max ↑ by 6% & time to exhaustion by almost 50%.
Ergogenic effect increases with length of endurance event
Risks:
Infusing too much blood thickens blood (viscosity), increasing resistance to heart’s pumping, can lead to heart failure.
Mismatching blood is possible as is HIV infection.
2) Erythropoietin (EPO)
Hormone naturally produced in kidneys that works on bone marrow to stimulate production of RBCs.
Currently, it is easily produced with recombinant DNA.
Proposed Effects:
Similar to blood doping, but “EPO” specifically increases hematocrit levels.
this ↑ oxygen carrying capacity of blood, VO₂max, & endurance performance
Proven Effects:
First tested scientifically in 1991. 6 weeks after erythropoetin given. Found:
→ ↑ hemoglobin & hematocrit (10%)
→ ↑ VO₂max (6-8%)
→ ↑ time to exhaustion (13–17%)
Risks:
Less controlled than with blood doping
Can ↑ blood viscosity (heart failure)
Some deaths among competitive cyclists linked to its use (not medically confirmed)
3) Bicarbonate Loading
Bicarbonates (HCO₃⁻) are buffering substances to hold pH constant & prevent acidosis.
They occur naturally & can be ingested as sodium bicarbonate (baking soda)
Proposed Effects:
Buffer lactic acid produced during anaerobic metabolism & improve performance in short term, high intensity events (sprints)
Proven Effects:
Oral intake of sodium bicarb ↑ plasma bicarbonate levels but has no effect on intracellular levels.
raises pH of blood
More extracellular buffering capacity, but not more intracellular buffering.
As result, originally thought to enhance only anaerobic efforts of more than 2 min duration, when lactate’s protons get into bloodstream.
Initially, researchers believed sodium bicarb was only helpful after ~2 minutes, when these acidic byproducts (like lactate and H⁺) exit the muscle and enter the bloodstream.
Later, Brooks indentified lactate transporter on sarcolemma that is driven by pH gradients
These transporters move lactate + H⁺ ions out of the muscle, and they are stimulated by pH gradients.
That is: the greater the difference in pH between inside and outside the muscle, the faster these waste products can be cleared.
As result: by increasing extracellular pH, bicarb helps transport lactate (proton) out of myofiber in events shorter than 2 min.
increase the pH gradient between inside and outside the muscle.
This accelerates the export of lactate and H⁺ ions through MCTs, even in shorter efforts (< 2 minutes).
Research:
Shows positive effects during intense exercise lasting 1–7 min, but only if dose is proper (300 mg/kg body weight)
Risks:
GI tract discomfort (tums/rollos) → antiacid
Nausea
diarrhea
Creatine Supplementation (Performance)
Type of exercise most effective: explosive, high intensity work of short duration
→ ex., 30 sec of work = 200% VO₂max
→ Glycolysis = 55% of required ATP
→ PCr hydrolysis = 25% of ATP
→ Oxidative phosphorylation = 20% of ATP
→ ex. 6 sec sprint at 250% VO₂max
→ Glycolysis = 50% of ATP
→ PCr hydrolysis = 50% of ATP
Sprint & strength increases 3–8%. May be greater with continuous repetitions
Creatine benefits evident during repeated exercise sprints
Performance benefits not achieved without proper training (no acute effect)
Great variability in performance effects (non-responders)
Performance benefits specific to muscle trained
Performance improvements greatest in untrained *vegetarians
Weight training benefits? Allow greater training volume & thus greater strength gains. Expectation: Pearson Study; with volume held constant, Cr group still showed greater strength gains.
Creatine Supplementation (Physiology)
Early weight gain of 3–6 lbs due to water retention
Not all creatine taken up by muscle converted to PCr
Not all creatine consumed gets into muscle
Supplementation usually decreases PCr:Cr ratio in muscle
relative proportion
total energy reserved still increase
Greater creatine uptake by muscle when consumed w/ high doses of CHO
Consuming creatine with a high-carbohydrate (CHO) meal or drink (e.g., juice or sports drink) boosts uptake efficiency.
In general, supplementation increases total muscle Cr by 0–40% (typically 15–20%)*non-responders*
Increased total Cr specific to muscle trained (upper limit)
Creatine does not directly stimulate muscle protein synthesis, or muscle hypertrophy
It doesn’t trigger muscle growth directly like hormones do.
However, it may allow you to train harder or with more volume, which indirectly leads to hypertrophy.
Initial, high “loading dose” of 20g/day not necessary; 5g/day just as effective; maintenance dose can be just 2g/day
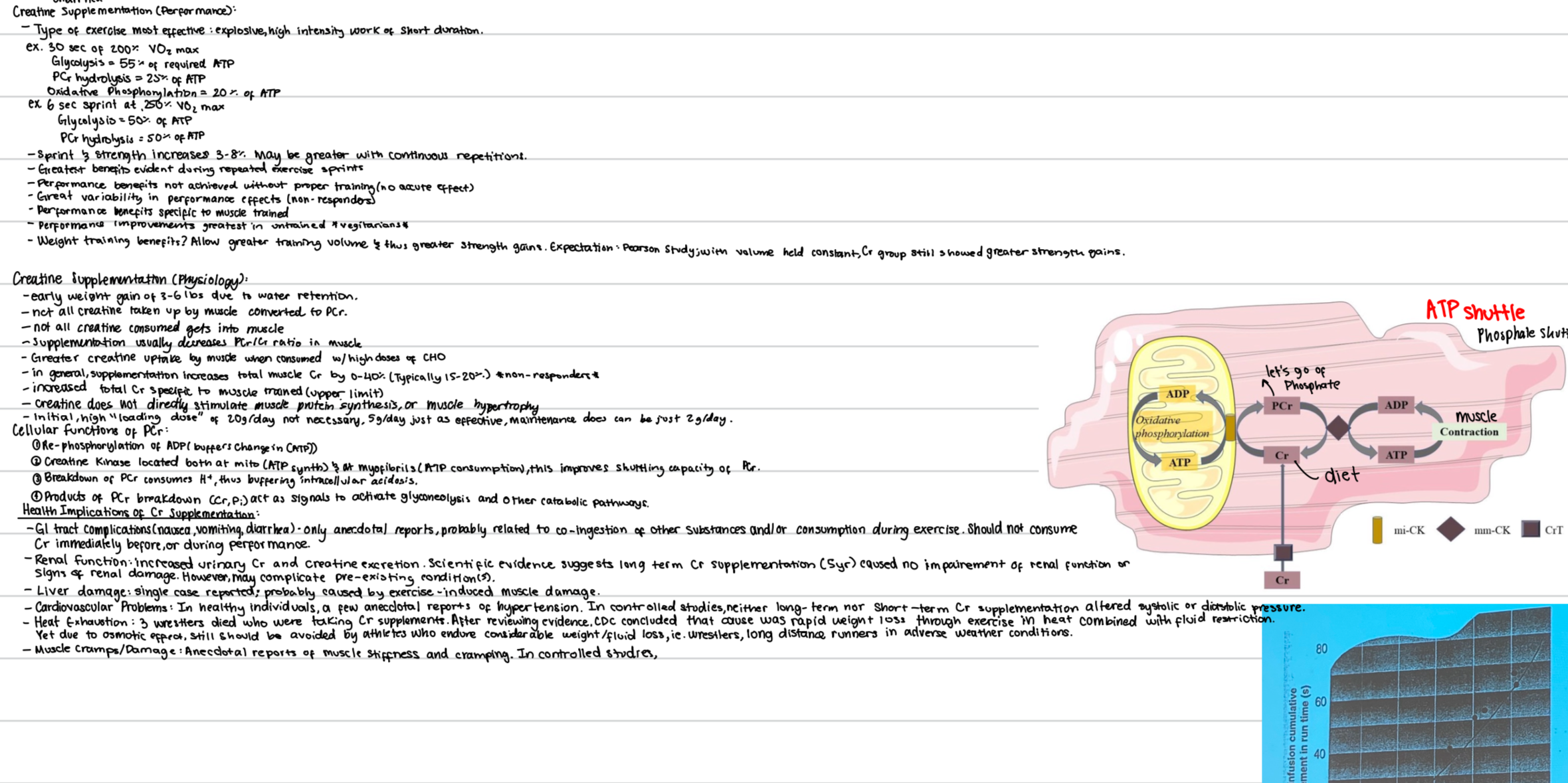
Cellular Functions of PCr:
Re-phosphorylation of ADP (buffers change in [ATP])
PCr + ADP → ATP + Cr
Creatine kinase located both at mitochondria (ATP synth.) & myofibrils (ATP consumption), this improves shuttling capacity of PCr
Mitochondria: where ATP is made → CK regenerates PCr here
Myofibrils (contractile machinery): where ATP is used → CK uses PCr to regenerate ATP on-site
Breakdown of PCr consumes H⁺, thus buffering intracellular acidosis
Products of PCr breakdown (Cr, Pi) act as signals to activate glyconeolysis and other catabolic pathways
Health Implications of Cr Supplementation
GI tract complications (nausea, vomiting, diarrhea) - only anecdotal reports, probably related to co-ingestion of other substances and/or consumption during exercise. Should not consume Cr immediately before, or during performance.
Renal function: increased urinary Cr and creatine excretion. Scientific evidence suggests long-term Cr supplementation (5 yrs) caused no impairment of renal function or signs of renal damage. However, may complicate pre-existing condition(s)
Liver damage: single case reported; probably caused by exercise-induced muscle damage
Cardiovascular problems: In healthy individuals, a few anecdotal reports of hypertension. In controlled studies, neither long-term nor short-term Cr supplementation altered systolic or diastolic pressure.
Heat exhaustion: 3 wrestlers died who were taking Cr supplement. After reviewing evidence, CDC concluded that cause was rapid weight loss through exercise in heat combined with fluid restriction.
→ Due to osmotic effect, still should be avoided by athletes who endure considerable weight /fluid loss, i.e., wrestlers, long distance runners in adverse weather conditions.Muscle cramps/damage: Anecdotal reports of muscle stiffness and cramping.