Hospital Theory
The History of Hospitals
- The concept of hospital began in Indian and Egyptian cultures
- Early hospitals were only for the insane, incurable and contagious
- The military was the major face for the recent development of hospitals with need to look after the wounded
- Now we have the Canadian Health Act which was enacted in Parliament in 1984
Health Care in Canada
- Predominantly publicly financed
- Medicare is also known as the Health Care Act founded by Tommy Douglas
- Management and delivery is the responsibility of the individual province/territory
- Federal Government gives the provinces money and they decide how to allocate it
- Federal setting and administering of national principles
Principles of Medicare
- Public Administration: nonprofit accountable to the provincial government ex. Hospitals
- Comprehensiveness: all medically necessary services are offers by nurses and physicians
- Universality: 100% of the population is insured (eligible residents)
- Accessibility: reasonable access to hospitals and physicians without barriers; providing care regardless of where you live
- Portability: ability to move to another province in Canada
Funding
- Primarily taxation (money taken out of paychecks)
- Provincial and federal (sales taxes,)
- Sales taxes, payroll levels, lottery proceeds
Pharmacoeconomics
- Relatively new
- Pharmacoeconomics: analytical methods are used to identify, measure and compare costs and consequences of pharmacy products and services
- Refers to the scientific discipline that can play compares the value of one pharmaceutical drug therapy to another drug therapy
- Help make decisions on
- Formulary inclusions
- Drug-use policies
- Clinical practice guidelines
- Reimbursement and individual patient therapies
- Used to compare cost and consequences of two or more competing products services and programs
- Look at value for the money
- Comparative effectiveness
- Cost effectiveness
- Value for money
- Managed Care: Is quality care that uses only the most cost effective treatment and encourages preventative health strategies
Managed Care
- Is quality care that uses only the most cost-effective treatments and encourages preventative health strategies
Health Care in Canada
- cost escalated and the health of Canadians has not dramatically increased accordingly
- cash starved provinces examining privatizations of services or user fees
- not covering some services
Canadian Institution for Health Information (CIHI)
- non-profit
- collect and disseminate health information
- data shows 331 billion of healthcare in 2022 (8,563 per Canadian)
- Slowdown in economy and increase in healthcare spending
- spending of drugs is 2nd largest portion of 26.1 billion in 2011 (84% Rx)
- payment to physicians is 3rd (26.6 billion)
Factors' Affecting Spending
- Geographic distribution
- models of care
- salary
- benefits levels
- age structure of provinces population
Suggested Overhaul of Medicare by Commissions Report
- 5 key areas
- rural and remote access fund
- diagnostic services fund
- primary health care transfer
- home care transfer
- catastrophic drug transfer
Quebec Ruling
- lengthy wait times unacceptable
- currently prohibited people from buying insurance for services by health plan
- court ruled it is unconstitutional ban private insurance where public system fails
Local Health Integration Networks
- Transferer power to provinces
- cannot run from one head office
- Designed to plan, integrate and fund local health services including
- Hospitals
- Community Care Centers
- Home Care
- Longer- term care
- Mental health services
Health Systems should be
- safe
- effective
- patient centered
- accessible
- efficient
- equitable
- integrated
- appropriately resourced
- focuses on Population Health
What Can We Do as Consumers to reduce cost medication spending"?
- newer drug not always better
- entire quantity of Rx medication need to be taken
- directions need to be clear
- physician or pharmacist provide info on drug
- fill all medications at same pharmacy
Inventory Management
Inventory
- up to 70% of a hospital pharmacy budgets is spend on pharmaceuticals
- inventory budget includes IV solutions, sets, pumps, and other medical supplies
- buyer manages inventory
- works under the supervision of the pharmacist
Bidding and Purchasing Contracts
- confidential process by which the pharmacy “locks in” medication costs from a prime wholesale vendor for one year
- Pharmacy also bids with manufacturers of drugs and IV solutions. with longer contracts (5 years)
- Buyer makes an accurate estimation of formulary medication use for the next calendar year
Ordering the Pharmaceuticals
- Ordered from wholesaler such as McKesson Provider Technologies or Cardinal Health
- IV solutions ordered from a medical device company such as Baxter or Hospira
- Procedures for ordering non-formulary drugs and borrowing from other facilities vary from hospital to hospital
Receiving and Storage
- Inventory control technician orders medications, all technicians assist in receiving and restocking orders
- check order against invoice upon receipt
- discrepancies must be resolved
- Check for damaged goods
- check for items not received due to drug shortages
- pharmaceutical should be placed on inventory shelves or in the refrigerator
- storage guidelines available in package inserts or some reference texts
Special Handling of certain pharmaceuticals
- Narcotics
- Controlled Substance ordering system
- must be kept in a locked cabinet
- physical inventory required every two years
- destructions must be witnessed and documented
- Investigational Drugs
- separate, secure storage area
- supplied directly from the manufacturer
- not usually labeled with name and strength
- packaging labeled with the lot number and expiration date
Performing Ongoing Inventory Responsibilities
- Rotating Inventory
- place drugs so that the products expiring first are used first
- document the inspection of expired drugs
- Checking for drug recalls
- recall notice from the wholesaler/manufacturer will list the drug and lot number to be recalled
- technician pulls drugs from the shelves, unit dose carts, crash carts, automated dispensing cabinets
- technicians completes and signs a return from to the wholesaler to receive credit from wholesaler
- copy the form kept in the pharmacy
Other Institutional Pharmacy Practice Settings
- Specialized pharmacies provide residents of long-term care facilities (LCTFs) with unit doses medications, IV medications
- Health Maintenance Organizations may have in-house pharmacies that serve their hospital facilities and clinics
- Home infusions pharmacies supply sterile preparations such as TPNs to patient who are not living in institutions
A Dose of Medical Ethics
- Top 10 Dilemmas
- Conflict pitting doctors against pat/fam
- Setting priorities related to medical waiting
- Access to needed health-care resources
- Shortage of family physicians Medical errors
- Palliative treatment
- Achieving informed consent
- Issues related to research
- Substitute decision-making Surgical innovations
…
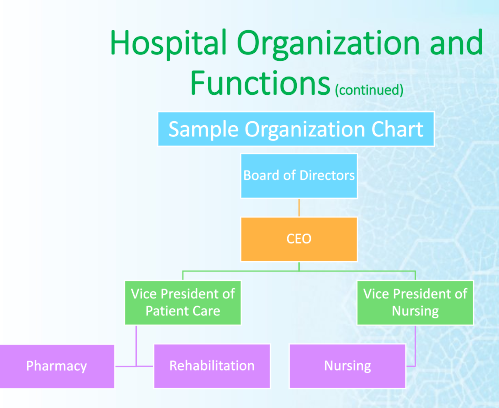
Organisation and function
- diagnosis and testing
- treatment and therapy
- patient processing
- public health and wellness
- preventative health initiatives
- training health care professionals
- CONDUCTING RESEARCH
- Hospitals are classified according to certain characteristics
- bed capacity
- targeted patent population
- type of service
- affiliation
- ownership
- urban versal rural
- financial status
- Common Hospital Departments and their Acronyms
- Ambulatory Patient Care (APC)
- Emergency Room/Department (ER/ED)
- Intensive Care Unit (ICU)
- Labor and Delivery (L&D)
- Neonatal Intensive Care Unit (NICU)
- Operating Room (OR)
- Transitional Care Unit (TCU)
Pharmacy and Therapeutics Committee (P&T)
- Reviews, approves, and revises the hospital’s drug formulary
- maintains hospital drug use policies
- reviews studies on appropriate use of drugs within hospital
- reviews investigational drugs for hospital use
- monitors medication error reports
- part of maintaining accreditation from the Joint Commission
- Representatives form medical staff, hospital and nursing administration
- director of pharmacy: records and disseminates meeting minutes
- drug-information pharmacist: researches and makes objective drug formulary recommendations
- Pharmacy Technician: collects data and performs audits for the drug-information pharmacist
Drug Formulary
- List of drugs approved for use in the hospital
- Provides most effective medications while limiting costs
- To add a medication to formulary, physician submits a medication application form
- Drug-information pharmacist reviews literature and compares cost, advantage, and disadvantage to existing formulary drug
- Approval sometimes restricted to a specific medical service
- If physician writes for nonformula drug, may need to justify use to P&T committee
Medication Error Reports
- drug information pharmacist collects and analyzes reports from pharmacy, nursing, and medicine
- Adverse drug events tabulated
- identify and correct the system’s problem to prevent recurrence
- required to maintain hospitals accreditation
Institutional Review Board
- Reviews the use of investigational drugs or procedures in the hospital
- investigational drug: used in clinical trials; not approved by the FDA
- Representative from medicine, pharmacy, nursing, and hospital administration, and the public
- Clinical research investigational study
- requires IRB approval before it can begin
- investigator submits application and informed consent
- informed consent: document written in understandable language about the study for patient participants
- IRB protects patients by ensuring adequate knowledge of study risks and confidential of medical information
- IRB collects information on adverse reactions to investigational medications, evaluates whether studies with severe adverse reaction should continue
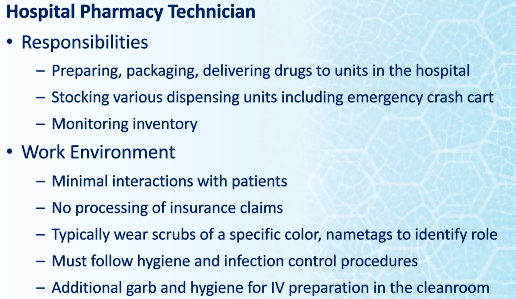
The Hospital Pharmacy Department
- Services
- administration (formulary, budget, inventory)
- distribution (filling, delivering, medications)
- clinical (consulting with prescribers, patients)
- Educational ( training pharmacies, patients, public, other personnel)
- Specialty services may include: satellite pharmacies located at patient care units, clinical pharmacists making rounds with physicians, drug information center
- Location and Structure
- designated areas such as unit dose cart fill, repackaging, narcotic and investigational drug storage, preparation of sterile products
- typically staffed 24 hours a day 7 days a week
- Director of Pharmacy responsibilities
- pharmacist-in-charge oversees the day-to-day operations
- determines the level and scope of pharmacy services
- plans and monitors the budget
- makes staffing decisions
- develops the Policy and Procedure Manual

- Specializing Pharmacists
- clinical pharmacists go on rounds with doctors, nurses
- in larger hospitals, specialist pharmacists are found in different departments including the emergency department, the neonatal Intensive Care Unit
- Specialties include compounding, chemotherapy, or IV medications
- Technician Training and Orientation
- require additional training on the job and regular retraining
- train to perform all major department functions
- most do not rotate through the cleanroom or hazardous compounding without specialized training
- Technician Advancement and Specializations
- medication reconciliation
- sterile compounding
- inventory management
- training other staff
- TCT Programs, technicians check each other’s work, adding an additional layer of medication safety
Types of Hospital and Institutional Pharmacy and Dispensing/ Returns
Long-Term care facilities
- Provides rehabilitative services
- restorative
- ongoing skilled nursing care to individuals
Hospices
- Provide palliative care and support services to individual at the end of their lives
- also serves patients families
- Open 24/7
- Inpatients home and facilities
- Provides pharmaceutical, physical, social, spiritual, and emotional care during last stages of life and bereavement period
Nursing Homes
- Offer skilled and custodial care to older people who do not need the intensive acute care of a hospital
- Wide range of medical conditions
- Known as
- Health Centers
- Havens
- Manors
- Nursing Centers
- Can range from 25-500 residents
Correctional Facilities
- Prisons
- Individual are physically confined and deprived of personal freedom
- part of the criminal justice system
- oversee the provision of pharmaceutical service to those confined to the facility
Hospital Pharmacies
- Most prevalent type of health-system pharmacy
- began as a charitable institution for the needy, aged, infirm or very young
- Now where sick or injured people receive many levels of medical or surgical care
- range from outpatient services to long-term care and intensive care
Types of Pharmacies
- Centralized: is operated out of one primary location, the inpatient
- all patient operations in one location
- medications delivered through in one location
- Decentralized (satellite): can consist of a central with multiple satellite pharmacies and outpatient pharmacy; typically specialized such as coagulation therapy
- disadvantage is duplication of staff. inventory, and equipment
- Medium and large facilities usually have to use this system
- Inpatient Pharmacy
- responsible for
- Medication packaging
- Centralized inventory
- Sterile product preparation
- Preparation and delivery of medication carts
- Service to patients admitted to a facility
- Outpatient: available to patients being discharged from the hospital
- or being treated by physician but do not require overnight admission
- retail-style pharmacy in hospital facility
- CIVA Centers (sterile prep): responsible from processing and dispensing medication orders for individual patients
- generally provide initial doses and emergency medications after which medications may be dispensed from floor stock
- number and scope of practice varies by facilities
- some for specific patient care areas
- some have satellites based on location and access not by scope of service
Health-Systems Pharmacies Returns
- returns are permitted if unused, unopened products
- not permitted everywhere
- safe
- no waste
- cost-effective
New Brunswick Prescription Drug Program
- NBPDP
- NB Electronic Health records
- one patient, one record
- web enabled application that will 24/7 Rx history access
Role of Hospitals
- They are vital part of Canadian healthcare system
- They provide
- Emergency Services
- Medical or surgical treatments
- rehabilitation services
- ongoing medical care
- Patient Care
- diagnostic and testing
- treatment and therapy
- Patient processing
- teaching
- research
- public health promotion
- GOALS OF PHARMACY
- Promote the rational use of medications
- Establish the value of pharmacy services
- to enhance the health of patients
About Horizon Health Network
- A billion dollar organization
- responsible for 14,000 staff including 1,00 physicians and 4,600 volunteers
- Operates 12 hospitals and more than 100 facilities, community health centers and clinics, addiction services, mental health services, public health, and extra mural program
- 20 foundations and 19 auxiliary and Alumnae supporting our organization
- Horizon provides major critical and trauma services and is responsible for unique programs such as:
- Heart Center
- Prenatal
- Trauma
- Rehabilitation
Vitalite Health Network
- $660 million
- 1,197 beds
- 399,322 patients
- 21,232 surgery’s
- 245,180 Emerge visits
- 2,029 births
- 186,561 Extra Mural Program
Classification System of Hospital
- teaching hospital
- types of care provided
- accreditation
- length of stay: less time more patient treated
- less time more prescriptions
- less admission, longer waits for surgery
- fewer services for tax dollar
- Home Care: if downsizing is to work. must be services waiting for people who are discharges patients
- Long-term care
- 65 licensed nursing homes in NB
- NBANH.com
- not enough
- fill many hospital bed waiting for home
- Ownership
- most owned by public
- some private in Canada
- Some operated by religious orders
Collaborative Practice
- Organizational Chart
- Technicians are intricate part of organizational structure
- Mission Statement of Pharmacy
- Accountability to hospitals and Patients
- Commitment to providing good working environment for its staff
- Ultimate goal is safe use of drugs by the public
- Pharmaceutical Care
- A relationship between a patient and a pharmacist in which the pharmacist accepts responsibility for drug use control functions and provides those services governed by awareness of, and commitment to, the patient’s interests’
- Pharmacist, patient, and physical make a therapeutic plan
- provide “definite outcomes which improve a patient’s quality of life”
- Provide pharmacist follow-up
- call patient at home
- ask patient to call at specific dates
- return to pharmacy
- routine discussion with physician
- Document follow-up activities
- Role of technician in Pharmaceutical Care
- helping pharmacists
- order-entry
- “first dose” fills
- Prepare and check all IV and chemo
- Note missed Doses
- Self-medication reporting and filling
- Other functions of the pharmacy department
- drug procurement
- safe preparation and distribution 5 rights
- drug information
- monitoring of appropriate drug use
- monitoring ADR’s
- Development of formulary
- monitoring of drug expenditures
- patient medication profiles
- pharmacotherapy
- investigational/ special release drugs
- Pharmacy’s responsibility to administration
- Annual reports must be submitted to inform admin of activities and achievements
- Financial reports
- staffing
- supplies
- workload monitoring
- medication incident/errors
- activity reports
- critical indicators
- measure taken for quality insurance
- detection of major deviations
- accreditations
- Drug related Problem’’
- Any physical or psychological signs or symptoms which is undesirable to the patient and which is in some way related to drug therapy
- Eight General Ways drugs can cause problems in patients
- taking drugs for no medically valid reason
- need drug and one has not been suggested or prescribed
- taking the wrong drug
- taking too little of the drug
- taking too much of the drug
- needs a drug, has been prescribed, but not taking or taking inappropriately
- experiencing adverse effects
- experiencing drug reaction
- Health Care Team
- Medical Staff
- MD or nurse practitioner
- Therapy and other personnel
- RT, PT, OT
- Nursing Personnel
- RN, LPN, Health Care Aid
- Pharmacy Personnel
- Pharm D, R.Ph, Technician, clerks
Formulary Medications
- Formulary Drugs: Narcotics
- Ordering by pharmacist or approved technician
- May or may not be patient specific
- Security: locked vault or acudose with a locked pocket (two people)
- Physician's orders- signed within 24 hours
- Prepackaging
- Narcotics stored and dispensed from separate Narcotic room in pharmacy
- Perpetual Inventory done regularly
Narcotics
- Many institutional pharmacies require pharmacy technicians to carry out all aspects of pharmaceutical controlled substance-related duties:
- Ordering Paling
- Counting
- Record keeping
- Ming
- Delivering
- providing quality assurance
- Placing the stock in s secure
Perpetual Inventory
- Computer keeps track of medications going in and out
- Some facilities manually record all withdrawals and additions in perpetual log books. The technician is often responsible for the record keeping (recording all controlled substance withdrawals and additions. perpetual log books,)
- The perpetual log book is an official, legal record of all activity relating to medications stored in the narcotic cabinet/room.
- The perpetual log book contains pages entitled Perpetual Inventory Record forms or Controlled Substance Record forms.
- Make all entries or additions into the perpetual log in black pen.
- Record withdrawals and negative balances in ==red pen==.
- Note errors by drawing a single line through the entire line entry. The initials of the person making the correction should be written next to the strikethrough and circled.
- Errors in the narcotic records must remain traceable and legible. Never cross or scribble out errors; note that it is never acceptable to use white-out or similar products.
- Always record information in the perpetual log on the next available line. There should never be an open or empty line in the perpetual log
- Never write information on the bottom of a perpetual log sheet below the preprinted spaces. Once you have filled the last available line on the page, you want start a new sheet.
- To start a new sheet, transfer the drug name, strength, dosage form, manufacturer, and DIN number from the drug bottle onto the appropriate space at the top of the new sheet. Transfer the balance or actual count number into the first available balance space on this new sheet.
Formulary Drugs: IPOs
- Individual prescription orders
- Patient name appears on package
- For 1-30+ days (most hospitals run on 24 hour patient supply)
- May be packaged as unit dose, various quantities in prescription vials, baggies, or blister packs.
Formulary Drugs: Night Cabinet
- General stock available in an area outside the pharmacy for access by approved nursing staff when the pharmacy is closed
- Not patient specific
- Usually a blinded system or automated dispensing cabinet
- Procedure
- When the pharmacy is closed there is a procedure to be followed to access the meds in the night cabinet.
- A copy of the physician’s order to be verified by pharmacist (or if CPOE it will be in the system to verify next morning)
- A record log is kept of all issues, indicating the patient, nursing unit, drug & strength, number of pre packaged units obtained.
- A pharmacist is always on call after hours. Some drugs are monitored or restricted, therefore a pharmacist must give authorization.
- Some hospitals the night cabinet is located in the SPD dept. which is open 24/7 and they are responsible for obtaining and delivering the med to the nursing unit.
Technicians Role- Night Cupboard
- Replace all stock taken from the previous night.
- Check the dating every month or week (items with shorter times, i.e. premixed IV bags) and replace any that will expire before the end of the month
- Making sure the stock is appropriately rotated.
Sample Night Cabinet Report from Automated Cabinet
- You will see here it tells you the medication that was taken and the amount you need to refill. You would pick the items needed in the stockroom and then go deliver and replenish the stock in the automated cabinet. Either by scanning the barcode or by typing in the drug name.
- blank slide (15)
- Some institutions store floor stock items in an automated dispensing machine (ADM).
- Turnaround times can be long when pharmacies are busy.
- The need to administer "STAT," "now," and initial doses quickly is the main reason for having floor stock.
- Pharmacy technicians are responsible for timely and accurate filling and checking of floor stock items on the Floor Stock Request Form (FSRF).
Medications not included in Floor Stock
- Critical care medications are commonly kept in a crash cart brought to the bedside for emergencies.
- Medications requiring pharmacy compounding
- Creams, ointments, special oral solutions, and IV solutions with additives that require compounding in the pharmacy are prepared as needed
- Narcotics
- These are kept in a separate, high-security area.
- Access to narcotics is restricted to authorized personnel.
- Special record keeping is required for their administration.
Sample Manual Method Floor Stock Request Form
- In this example you have Par level or your possibly and min and max column. For the manual method this would involve going to the unit and counting what is on hand and then replenishing what is needed. Typically would have different days scheduled for each unit/floor. Some high volume areas may get checked 2 to 3 times per week. An emergency department would be a high volume area.
- This is how the automated dispensing cabinet let's us know it needs replenishing
- These reports will print in the pharmacy alerting the technician's that the medication needs replenishing and which unit it is. Also note it tells you the quantity needed.
Formulary Drugs: Emergency Box (specialty Carts)
- OR (operating room) cart
- ER (emergency room) cart
- Crash (for codes) cart
- All contain medications, pertinent to their area, in forms/packaging that is quick and easy to administer in critical situations
- Meds are usually on a portable cart with drawers / shelves
- Technicians responsibilities
Pediatric Crash Cart
- Crash carts are kept on hand for treating respiratory or cardiac arrest and other potentially fatal emergency conditions.
- Many large facilities keep a crash cart on each floor or nursing unit.
- Contents of crash carts are tailored to the types of patients in the facility.
- Due to differences in body size and physiology, the types and strengths of medications in adult facilities would be different from those used in pediatrics.
- Most of the items in the crash cart will be for parenteral use, meaning any route of administration other than sublingual, enteral, or topical, such as intravenous or intramuscular.
- Generally, adult crash carts are stocked with emergency medications such as epinephrine, atropine, and nitroprusside.
- The cart may also contain standard IV base solutions, IV tubing, and a limited supply of syringes, needles, and other medications or supply items.
- Facilities often use tamper-evident plastic locks, which can be easily opened in emergency situations.
- When a hospital patient goes into cardiac or respiratory arrest, a code is called.
- A code is a life-threatening situation when a patient is in cardiac or respiratory arrest.
- code blue respiratory arrest
- code red: fire
- yellow missing persons
- A code team responds and assumes treatment of the patient, unlocking the crash cart.
- Except during code use, the crash cart must remain locked.
- Once the code has ended, the crash cart is returned to the pharmacy to be refilled.
- Define:
- crash cart: also known as "crash tray.” "code cart," "tackle box" or other term that individual facilities may develop
- parenteral: also known as "crash tray." "code cart," "tackle box" or other term that individual facilities may develop
- code: a life-threatening situation when a patient is in cardiac or respiratory arrest
- code team: a group of doctors and nurses trained in emergency medical care
- par level: the amount of a certain medication normally kept in the crash cart
Alcohol and Spirits
- Pharmacy responsible to order and dispense
- Perpetual inventory
- Document when used in compounds
- Beer can be ordered to patients on physicians' orders, with appropriate records maintained in a perpetual inventory log book.
Formulary Drugs: Weekend Passes
- Patient orders which are needed for a limited time period, outside the hospital
- label must contain information required by law in NB community pharmacies (including auxiliary, safety caps and directions)
- Patient specific
Patient Prescriptions
- Most inefficient because of waste and inability of the pharmacy department to properly monitor it
- After reviewing medication orders for a floor, the technician takes the medication is filled and checked and then taken to the floor
- Orders can be for several days supply
- Once opened cannot be returned to the pharmacy because it has left the closed system of the pharmacy
- Not prepackaged or unit dose medication
- Being dispensed in vials
Inventory Management
- Inventory
- Up to 70% of a hospital pharmacy budget is spent on pharmaceuticals
- Inventory budget includes IV solutions, sets, pumps, and other medical supplies
- Buyer managers inventory
- Works under the supervision of the pharmacists
- Bidding Pharmaceuticals and Purchasing Contracts
- Confidential process by which the pharmacy locks in medication costs from a prime wholesale vendor for one year
- pharmacy also bids manufacturers of drugs and IV solution, with longer contracts 5 years
- Buyer makes an accurate estimate of formulary medication use for the next calendar year
- give ordering card to buyer ordering box
- Ordering the Pharmaceuticals
- Ordered from wholesaler such as Mckesson Provider Technology or Cardinal Health
- IV solutions ordered from a medical device company such as Baxter or Hospira
- Procedures for ordering non formulary drugs and borrowing from other facilities vary from hospital to hospital
- Receiving Storage
- Inventory control technicians orders medications, all technicians assist in receiving and restocking orders
- check order against invoice upon receipt
- discrepancies must be resolved
- Check for damaged goods
- check for items not received due to drug shortages
- pharmaceuticals should be placed on inventory shelves or in the refrigerator
- storage guidelines available in package inserts or some reference texts
- Special Handling of certain pharmaceuticals
- Narcotics
- must be kept in a locked cabinet
- physical inventory required every two years
- destruction must be witnessed and documented
- INvestigational Drugs
- Separate, secure storage area
- supplied directly from the manufacturer
- not usually labeled with the name and strength
- package labeled with the lot number and expiration date
- Performing Ongoing Inventory Responsibilities
- Rotating Inventory
- Place new drug In front and old drug in the back
- document the inspection of expired drugs
- Checking for drug recalls
- recall notice form the wholesaler/ manufacturer will list the drug and lot number will be recalled
- Technician pull drugs from the shelves, unit dose carts, crash carts, automated dispensing cabinets
- technicians complete and signs a return form to the wholesaler to receive credit from wholesaler
- copy of the form kept in the pharmacy
Electronic Hospital Records and Medication Orders
- Electronic Health Records allow for easier communication about a patient within a health system
- Immediate access to patient’s medical records
- Improve documentation
- Enhanced coordination of patient care
- Intake Records
- Upon admission to a hospital, patient interviews about his medication his history by admitting staff or nurse
- some pharmacy technicians specialize to identify unknown medications brought from home (home meds)
- Patients is given a wrist band
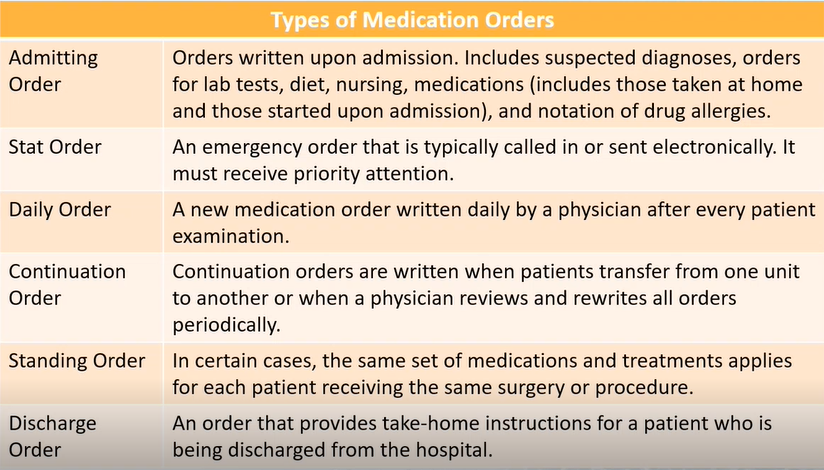
- Medication Orders
- Ordered by the prescriber for a patient
- received electronically, by fax, pneumatic tube, phone, or hand delivery
- written in the medical chart
- entered by the hospital pharmacist
- Computerized Prescriber Order entry
- Prescriber directly enters into the electronic health record using a mobile device or laptop
- a pharmacist checks and verifies the order
- Advantages of CPOE
- Efficient medication order completion
- allows for prescriber entry off-site
- simplifies inventory ordering and posting of patient hospital charger
- improved medication safety
- reduces transcription errors
- includes safeguards that identify duplicate drugs, incorrect doses, and laboratory test results that may affect drug or dose
- Handwritten Orders
- Input by pharmacist into the pharmacy software
- Verified for accuracy by the pharmacist if the pharmacy technician has entered the order
- Electronic Medication Administration Record (eMAR)
- all electronic record of the administration time of each drug
- reduces medication error
- increased nurse productivity
- Benefits of eMAR
- Enhances communication among healthcare team members
- reduces medication errors
- provides a way to meet documentation guidelines
- All information collected using automation must be used in a way that protects patient privacy according to HIPAA
Formular Drugs: Weekend Pass
- Patient Order which are needed for a limited time period, outside the hospital
- label must contain information required by law in NB community pharmacies (aux. safety caps and directions
- patient specific
- cannot be taken out of the acudose
INvestigational Drugs
- Not approved by the health protection branch for general use by the public
- two types of investigation drugs
- clinical
- SAP drugs (special access program)
- Emergency (covid vacc)
- Written consent have to be signed by the patient
- Technical Duties
- Clinical Trials
- released by health protection branch of health canada
- released to a qualified investigator who is experienced and trained
- why: to investigate the safety and the effectiveness of a drug to be evaluated. It is the final stage of human testing
- It would be a current drug that is in use but a different form or indication of it
- Emergency Status
- How are these Drugs different from the Rx drugs
- not available in canada but are approved by some health protection branch somewhere else
- who gives permission to use these drugs
- Health Canada
- who can order these drugs
- Doctors or Pharmacist a form has to be filled out why they want this drug then it has to be approved by health canada
- these drug are not for general use
- Released to a specific doctor, patient and use
- Investigational Drugs Consent
- required before administration of the drug
- written consent by the patient or power of attorney
- part of the permanent health record and a copy is given to the patient
- INvestigational Drugs Records
- investigation drugs must be stored separately from the other drugs in the pharmacy
- pharmacy department is responsible for
- separate storage and dispensing
- records must be accurate, complete,and up to date
Specialty Carts
- is a tray put on a cart
- Emergency Box
- OR cart
- ER Cart
- Crash Cart for all codes
- All contain medications, pertinent to their area, in forms/ packaging that is quick and easy to administer in critical situations
- technicians responsibilities
- •Meds include seizures, anaphylactic reaction, respiratory and cardiac arrest meds
- On all nursing units
- Back-up in night cabinet
- Immediately replaced when used extra in pharmacy when open in morning for immediate replacement
- Secured with a one-time use padlock if broken must be rechecked and re-sealed
- Typically uses pull tabs or sealed bags
- Unit3-20 sample of order for potassium may need to get from night cabinet
- Page 21 usage record
- Page 22 chart of how nc gets replenished
- Page 23-27 sample emergency box and list and chart of how replenishment is done
- Inventory approved by P&T
- Use prefilled syringes whenever possible for time
- Inventory list in box indicates quantity, strength, packaging and name of drug in alphabetical order all injectables
- Most often code is cardiac arrest
Most commonly used drugs are sodium bicarbonate, lidocaine, atropine and epinephrine * Must be in date sticker on outside with the earliest item to expiry
BPMH Medication Reconciliation
Medication Reconciliation
- PROCESS INTENDED TO PREVENT MEDICATION ERRORS AT TRANSITION POINTS IN PATIENT CARE
- Errors result of failure in communication about medications, especially at vulnerable transition points.
- Transition points
- Admission
- Discharge
- transfer between care settings
- CREATING MOST COMPLETE AND ACCURATE LIST OF ALL MEDIATIONS A PATIENT IS CURRENTLY TAKING
- USING THIS LIST WHEN WRITING MEDICATION ORDERS
- COMPARING THE LIST AND THE MEDIATION ORDERS
- PATIENT SAFETY INITIATIVE IN CANADA
- 50 % OF PATIENTS HAVE AT LEAST 1 UNINTENTIONAL MEDICATION DISCREPANCY IN HOSPITAL ADMISSION ORDERS
- HIGH INCIDENT WHEN TRANSFERRED FROM INTENSIVE CARE TO A WARD SETTING
- TRANSFER BETWEEN LONG-TERM CARE AND ACUTE CARE
- DISCHARGE FROM HOSPITAL
- Post-hospital medication discrepancies increase the risk of readmission within 30 days
- Discrepancies that exist at admission but remain unresolved can create confusion
- Medication reconciliation program can reduce time that physicians, nurses and pharmacists spend sorting out the medication problems at the transition of care
- component of seamless care initiative in 1998
- One of six targeted interventions in Safer Healthcare Now!
- Unintentional Discrepancy
- Ordered a grey thong instead of grey pants
- Forgot to reorder your belt
- Undocumented Intentional Discrepancy
- Blue a better color for you so substituted in place of red shirt but nobody was told
- Intentional Discrepancy
- Everyone told you that you had the legs for a dress so we replaced your pants
Medrec Background
- MEDICATION RECONCILIATION
- IS A REQUIRED ORGANIZATIONAL PRACTICE (ROP) FOR ALL HOSPITALS IN CANADA
- IS A VERY IMPORTANT PATIENT SAFETY INITIATIVE AND IMPACTS OUR PATIENTS THROUGHOUT THEIR HOSPITAL STAY, FROM ADMISSION TO DISCHARGE.
- NEEDS TO BE A PRIORITY IN OUR QUALITY IMPROVEMENT PLANS FOR EACH NURSING UNIT
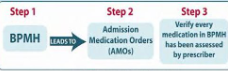
- IT IS A FORMAL PROCESS COMPARING:
- A PATIENT’S ACCURATE AND COMPREHENSIVE MEDICATION HISTORY (BPMH) AND
- MEDICATIONS PRESCRIBED AT ADMISSION, TRANSFER AND DISCHARGE
- Why is it important
- TRANSITIONS FROM ONE HEALTHCARE SETTING TO ANOTHER CAN LEAD TO ERRORS IN PATIENT’S MEDICATION REGIMENS
- THESE ERRORS CAN POTENTIALLY LEAD TO:
- ADVERSE EVENTS
- PROLONGED HOSPITAL STAYS
- RE-ADMISSIONS BACK TO HOSPITAL
- Transition of Care
- TRANSITIONS OR TRANSFERS BETWEEN INTERFACES OF CARE CAN INCLUDE PATIENTS MOVING BETWEEN:
- UNITS IN THE SAME HOSPITAL
- ICU TO GENERAL WARD
- ORHTOPEDICS TO CARDIOLOGY
- ONE HEALTHCARE FACILITY TO ANOTHER
- HOSPITAL TO HOSPITAL
- HOSPITAL TO REHAB
- ONE HEALTHCARE SECTOR TO ANOTHER
- LONG TERM CARE TO HOSPITAL
- HOSPITAL TO COMMUNITY
- Why is there a Problem
- A REVIEW OF PUBLISHED ARTICLES FOUND THAT 10-67% OF PATIENTS HAD AT LEAST ONE PRESCRIPTION MEDICATION HISTORY ERROR AT THE TIME OF HOSPITAL ADMISSION
- WHEN NON-PRESCRIPTION MEDICATIONS WERE INCLUDED THE FREQUENCY OF ERRORS WAS 25-83%
- What are the Discrepancies
- EX: UNINTENTIONAL DISCREPANCIES
- COMMON TYPES OF MEDICATION DISCREPANCIES:
- **OMISSION:**
- HOME MED NOT LISTED
- HOME MED NOT ORDERED
- DISCHARGE MED NOT INCLUDED IN INSTRUCTIONS
- COMMISSION
- DISCONTINUED MED IS LISTED OR ORDERED
- THERAPEUTIC DUPLICATION DUE TO FORMULARY SUBSTITUTION
- DOUBLE-DOSING VIA TWO ROUTES (IV AND PO)
- DESCRIPTION
- DOSE TIME MISSED
- DOSE INAPPROPRIATE
- EXTRA DOSE GIVEN
- DIFFERENT FREQUENCY
- Where is MEDREC Done
- Hospitals within 24 hours
- Ambulatory Visits
- day surgery, various clinics
- Community pharmacy
- Long term care homes
- home Care
- Admission: The goal reconciliation of admission is to ensure medication there is a conscious decision on the part of the patient's prescriber to continue, discontinue or modify the medication regimen that a patient has been taking at home.
- Compare BPMH vs. AMO (Admission medication orders)
- identify and resolve discrepancies
- Transfer: The goal of transfer medication the patient was receiving on the reconciliation is to consider not only what transferring unit but also any medications they were taking at home that may be appropriate to continue, restart, discontinue or modify.
- Compare BPMH vs. MAR (Medication Administration Record
- identify and resolve discrepancies
- Discharge: The goal of discharge medication reconciliation is to reconcile the medications the patient is taking prior to admission and those initiated in hospital, with the medications they should be taking post-discharge to ensure all changes are intentional and that discrepancies are resolved prior to discharge.
- Compare BPMH vs. MAR (Medication Administration Record + new medications started upon discharge
- identify and resolve discrepancies
- MEDREC MODELS
- Proactive Model: Areas with planned admissions pre admission clinic (bomb done prior to physician writing orders. Used before surgery in pra admission clinics)
- when bpmh is done before admission medication orders are written
- Retro active model: High volumes of admissions - considered inefficient as it creates more work as orders are already written before the BPMH is taken
- When thw BPMH is done after the admission medication orders are written

- Hybrid Model: bit of both
- When both models coexist
- happens when
- short staffed
- complex patients with extensive med histories
- incomplete information availible to complete a BPMH prior to admission order
- Ideally BPMH should be done within 24 hours of
admission
- what is BPMH: A BEST POSSIBLE MEDICATION HISTORY IS A HISTORY CREATED USING:
- A SYSTEMATIC PROCESS OF INTERVIEWING THE PATIENT OR THEIR CAREGIVER
- **A REVIEW OF AT LEAST TWO RELIABLE SOURCES OF INFORMATION TO OBTAIN AND VERIFY ALL OF A PATIENT’S MEDICATION USE. BOTH PRESCRIBED AND OVER THE COUNTER MEDICATIONS (OTC)**
- COMPLETE DOCUMENTATION OF ALL THE MEDICATIONS INCLUDING NAME, DOSE, ROUTE AND FREQUENCY
- Why is it important to identify all patient home meds both otc and rx
- MEDICATIONS SHOULD BE ASSESSED FOR ALL CONDITIONS
- STOPPING SOME MEDICATIONS ABRUPTLY CAN CAUSE WITHDRAW L SYMPTOMS
- IDENTIFY IF A MEDICATION IS THE CAUSE OF THE ILLNESS OR WORSENING OF SYMPTOMS
- CONSIDER POTENTIAL DRUG INTERACTIONS
- SOME MEDICATIONS CANNOT BE TAKEN BEFORE OR AFTER CERTAIN PROCEDURES OR SURGERIES
- COMMUNICATE TO THE CIRCLE OF CARE A COMPLETE LIST OF ALL MEDICATIONS ON DISCHARGE FROM HOSPITAL
- Where are BPMH’s Done
- AT ADMISSION TO HOSPITAL:
- IN EMERG
- PRE-ADMISSION CLINICS
- WITHIN UNITS OF THE HOSPITAL
- LONG-TERM CARE UNIT
- AMBULATORY CLINICS
- HOME CARE
- COMMUNITY PHARMACY (MED REVIEW)
- AT POINTS OF TRANSFER, WHEN PATIENT MOVES FROM ONE CARE SETTING TO ANOTHER
- Where are BPMH’s Documented
- WHETHER IT IS PAPER-BASED OR ELECTRONIC FORMAT, THE BPMH SHOULD BE DOCUMENTED IN A HIGHLY VISIBLE DESIGNATED LOCATION FOR ALL HEALTHCARE PROFESSIONAL TO ACCESS
- USUALLY IN THE PATIENTS CHART (ELECTRONIC OR PAPER)
- When should BPMH’s be completed
- ASAP
- ideally within 24 hrs of admission
- being done before the physician writes thea admission orders
- why
- to prevent med errors
- Anyone can do a BPMH with the proper training
- How to do a BPMH
- MEDICATION INFORMATION FROM MULTIPLE SOURCES
- 6 MONTH MEDICATION HISTORY FROM PROVINCIAL DIS OR CALL COMMUNITY PHARMACY TO GET THEIR 6 MONTH MEDICATION HISTORY
- MEDICATION VIALS
- HOSPITAL DISCHARGE SUMMARY
- NURSING HOME MAR
- AND INTERVIEW PATIENT OR CAREGIVER
- IDENTIFY AND RESOLVE DIFFERENCES BETWEEN THE SOURCES OF INFORMATION
- TALK AND LISTEN TO PATIENT/FAMILY/CAREGIVER
- ASK FOR A CURRENT MEDICATION LIST (THEY MAY HAVE ONE WITH THEM)
- ASK OPEN ENDED QUESTIONS
- ASK SPECIFICALLY ABOUT SPECIAL TYPES OF MEDICATIONS (PUFFERS, EYEDROPS, CREAMS, PATCHES, ETC.)
- DEVELOP A “TEMPLATE”
- CONSIDER ALTERNATE WAYS TO CONVEY THE SAME MESSAGE (EX. BRAND VS GENERIC NAMES)
- CONSIDER CURRENT AND ACTUAL MEDICATION USE
- TRY NOT TO USE MEDICAL LANGUAGE
- CONSIDER THE UNIQUE SITUATION OF THE PATIENT (EX. LANGUAGE, BARRIERS, COGNITION LEVEL, ACUITY OF ILLNESS ETC.)
- Interview
- INTRODUCTION
- ALLERGY INFORMATION
- COMMUNITY PHARMACY INFORMATION
- CURRENT AND ACTUAL MEDICATION USE
- REGULAR MEDICATION USE (OTC’S)
- AS NEEDED MEDICATION USE
**ALL MEDICATIONS: INHALERS, OTC’S, NASAL SPRAYS, VITAMINS, HERBALS, CREAMS, CLINICAL TRIALS, PHYSICIAN SAMPLES, ETC.** * Ask “How do you take your medication?”
- sources of information
- REVIEW WITH MULTIPLE SOURCES OF INFORMATION
- PATIENT/FAMILY/CAREGIVER
- MEDICATION VIALS
- BLISTER PACKS
- DIS HISTORY OR COMMUNITY PHARMACY HISTORY
- PATIENT’S OWN MEDICATION LIST
- DISCHARGE ORDERS FROM OTHER FACILITY
- MAR – MEDICATION ADMINISTRATION RECORD
- FAMILY DOCTOR
- HOME CARE MEDICATION LIST
- NOT ALL SOURCES OF INFORMATION ARE CREATED EQUALLY
- START WITH THE MOST RECENT SOURCES OF INFORMATION
- KNOW THE LIMITATIONS OF YOUR SOURCES
- NO SOURCE OF INFORMATION WILL TELL YOU EVERYTHING THAT YOU WILL NEED TO KNOW; BE SURE TO INVOLVE AND INTERVIEW THE PATIENT AND ASK THE RIGHT QUESTIONS
- Patient/Family
- PATIENT’S RECALL OF INFORMATION HISTORY CAN BE DIMINISHED DURING ACUTE/STRESSFUL TIME
- SOLUTION: VERIFY WHEN PATIENT IS NO LONGER IN DISTRESS; CONFIRM WITH A SECONDARY SOURCE
- POOR PERCEPTION OF WHAT A MEDICATION IS
- SOLUTION: EFFECTIVE PROMPTING OR PROBING QUESTIONS
- PATIENT MAY NOT KNOW THE NAME OR NUMBER OF THEIR COMMUNITY PHARMACY
- SOLUTION: DIS SYSTEM
- MEDICATION USE VS HOW THE MEDICATION WAS PRESCRIBED
- SOLUTION: FOCUS ON “MEDICATION USE”; SEEK CLARIFICATION (FROM OTHER COMMUNITY PHARMACIES, PRIMARY CARE PHYSICIANS, FAMILY MEMBERS, CAREGIVERS)
- COMMUNICATION BARRIERS
- LANGUAGE: NON-ENGLISH SPEAKING CLIENTS
- PATIENT’S LEVEL OF CONSCIOUSNESS/COGNITIVE ABILITY
- SOLUTION: FAMILY MEMBERS/CAREGIVERS, INTERPRETERS, OTHER SOURCES OF INFORMATION
- Medication Vials
- USE THE “SHOW AND TELL” METHOD
- CHECK THE PATIENT’S NAME ON THE VIAL
- CHECK THE DATE ON THE VIAL
- OPEN THE VIALS AND MAKE SURE WHAT IS IN THE VIAL MATCHES THE LABEL
- ASK THE PATIENT HOW THEY ARE TAKING THE MEDICATION AND COMPARE IT TO THE INSTRUCTIONS ON THE VIAL
- “TELL ME HOW YOU TAKE/USE THESE”
- Patients own medication list
- CONFIRM THE DATE IT WAS LAST UPDATED
- DETERMINE WHO WROTE THE LIST
- CONFIRM IF THE DIRECTIONS WRITTEN ARE HOW THE MEDICATIONS WERE PRESCRIBED OR HOW THE PATIENT ACTUALLY TAKES THE MEDICATIONS
- DETERMINE IF PATIENT IS TAKING ANYTHING ELSE (RX, PRNS, OTC, HERBALS, VITAMINS, ETC)
- Blister PAcks
- CHECK THE PATIENT’S NAME ON THE BLISTER PACK
- CHECK THE DATE ON THE BLISTER PACK – DETERMINE IF ANY CHANGES HAVE BEEN MADE TO THE PATIENT’S MEDICATIONS SINCE THE BLISTER PACK HAS BEEN FILLED
- DO NOT ASSUME PATIENT IS TAKING ALL OF THE MEDICATIONS IN THE BLISTER PACK
- ASK ABOUT MEDICATIONS THAT CANNOT FIT INSIDE THE PACK, EX. PUFFERS, PATCHES, EYE/EAR DRO
- PS, FRIDGE ITEMS, ETC.
- ASK ABOUT PRN MEDICATIONS
- Discharge medication list
- CHECK THE DATE ON THE LIST
- DETERMINE IF IT IS AN ACTUAL LIST OF ALL MEDICATIONS THE PATIENT IS TO BE TAKING OR IF IT IS ONLY A “PRESCRIPTION”
- DISCHARGE PRESCRIPTIONS – MAY ONLY INCLUDE “NEW” OR “CHANGED” MEDS
- THE ATTENDING PHYSICIAN MAY ASSUME THAT THE PATIENT SHOULD CONTINUE EVERYTHING THE PATIENT WAS TAKING PRIOR TO ADMISSION WITHOUT DOCUMENTING AT DISCHARGE
- BE CAREGUL OF “AUTO-SUB” MEDICATIONS (DUPLICATIONS OF MEDS)
- CONFIRM WITH THE PATIENT IF THEY ARE TAKING ANY OTHER MEDICATIONS
- CONFIRM IF THEY ARE TAKING THE MEDICATIONS DIFFERENTLY THAN PRESCRIBED
- CONFIRM IF ANY CHANGES HAVE OCCURRED SINCE DISCHARGE
- CALL COMMUNITY PHARMACY TO CONFIRM IF ANY OTHER ADDITIONAL MEDICATIONS
- MAR-Medication Administration Record
- LOOK CAN VARY BETWEEN INSTITUTIONS
- CHECK THE LAST DOSE ADMINISTERED
- BE AWARE
- HELD/HOLD MEDICATIONS
- CHANGES IN DOSE
- DISCONTINUED MEDICATIONS
- family physician
- IF NO OTHER SOURCE AVAILABLE – CALL FAMILY PHYSICIAN
- LIST MAY BE OUT OF DATE DEPENDING ON LAST VISIT
- LIST MAY NOT INCLUDE
- PRESCRIPTION MEDICATIONS ORDERED BY OTHER PHYSICIANS (SPECIALISTS, DENTISTS, ETC.)
- OTC’S, VITAMINS, HERBALS, ETC.
- What if sources do not match
- IDENTIFY THE DISCREPANCIES
- ONLY ONE OF THEM IS ACTUALLY HAPPENING
- CLARIFY WITH THE PATIENT DURING THE BPMH INTERVIEW WHAT IS BEING TAKEN
- FIND OUT AS MUCH AS YOU CAN FROM THE SOURCES OF INFORMATION, CALL PHARMACY, START-STOP DATES – INVESTIGATE FURTHER.
- DOCUMENT DISCREPANCIES
- CLEARLY RELAY THE INFO TO THE PHARMACIST, WHO CAN THEN RELAY TO PRESCRIBER SO THAT AN INFORMED DECISION CAN BE MADE
- Considerations
- IF ACTUAL MEDICATION USE VS HOW THE MEDICATION WAS PRESCRIBED
- NOTE ACTUAL MEDICATION USE ON THE BPMH
- DOCUMENT OR RELAY THE DISCREPANCY(IES) TO THE PHARMACIST
- CLINICAL DECISIONS WILL BE MADE BASED ON THE BPMH, WHICH CAN LEAD DIRECTLY TO MEDICATION ORDERS
- Helpful Tips
- Dose Concideations
- ALWAYS CONFIRM/VERIFY MOST RECENT INSULIN DOSE AS IT CAN CHANGE FREQUENTLY
- FOR PARTIAL TABLETS, THE EXACT DOSE NEEDS TO BE CLEAR
- FOR PARTIAL TABLETS RECORD THE AMOUNT TAKEN (IN MG) PER DOSE
- BEWARE OF ATYPICAL DOSING FOR CERTAIN MEDICATIONS SUCH AS WARFARIN, FENTANYL PATCHES, AND DEPOT – INJECTIONS, ETC
- EX. WARFARIN 2 MG ON SUN/TUES/THURS/ SAT; AND WARFARIN 4 MG ON MON/WED/FRI
- DOCUMENT WHICH DOSE THEY TOOK YESTERDAY OR THE DAY OF ADMISSION (IF POSSIBLE)
- BEWARE OF MEDICATIONS THAT ARE IN MCG VS MG
- FOR LIQUID SUSPENSIONS – RECORD THE CONCENTRATION OF THE LIQUID AND THE TOTAL NUMBER OF MG TAKEN
- CERTAIN MEDICATIONS (E.G. SINEMET) HAVE TO BE DOSE/TAKEN AT EXACT TIMES – TAKE NOTE OF THE EXACT TIME(S) THAT THE PATIENT TAKES EACH DOSE
- DO NOT USE DANGEROUS ABBREVIATIONS
- PAY PARTICULAR ATTENTION TO “HIGH ALERT” MEDICATIONS (E.G., ANTICOAGULANTS, INSULINS, OPIOIDS, METHOTREXATE)
- ENSURE THE PROPER FORMULATION OF THE MEDICATION IS DOCUMENTED, ESPECIALLY LONG ACTING VS. SHORT ACTING. (E.G., CR, XR, ER, LA)
- BE AWARE OF COMBINATION PRODUCTS (E.G. DIOVAN-HCT, COVERSYL PLUS, VIMOVO, ETC.) – RECORD BOTH GENERIC MEDICATION NAMES AND DOSES – ADD BRAND NAME IF ITS GOING TO GIVE CLARITY BUT MUST HAVE THE GENERIC AS WELL
- DON’T FORGET ABOUT INJECTABLES (COMMONLY MISSED DRUGS: VITAMIN B12 INJECTION, METHOTREXATE, PSYCHOTORPICS)
- FOR BISPHOSPHONATES (E.G. ALENDRONATE, RISEDRONATE) DOCUMENT THE SPECIFIC DAY OF THE WEEK THEY ARE TAKEN
- Scope of Practice
- ALWAYS BE MINDFUL OF WORKING WITHIN YOUR SCOPE OF PRACTICE
- UNDERSTAND WHEN TO REFER TO A PHARMACIST, NURSE OR PHYSICIAN:
- IF A PATIENT ASKS QUESTIONS ABOUT:
- WHY THEY ARE TAKING CERTAIN MEDICATIONS
- DRUG INTERACTIONS
- THERAPEUTIC/CLINICAL-RELATED QUESTIONS
- THEIR HEALTH STATUS
- WHAT THE PLAN IS FOR THEM WHILE THEY ARE IN HOSPITAL
- Refer to a Pharmacist
- IF A MEDICATION IS COMPLETELY UNFAMILIAR TO YOU AND YOU CAN’T FIND ANY INFORMATION ON IT
- IF YOU CANNOT RESOLVE THE DIFFERENCES BETWEEN TWO DIFFERENT SOURCES OF THE PATIENT’S MEDICATION INFORMATION
- OR AT ANY TIME WHEN YOU ARE UNSURE OF HOW TO HANDLE A PARTICULAR QUESTION OR SITUATION