W3 L3: The microbiology of milk and honey
What is milk?
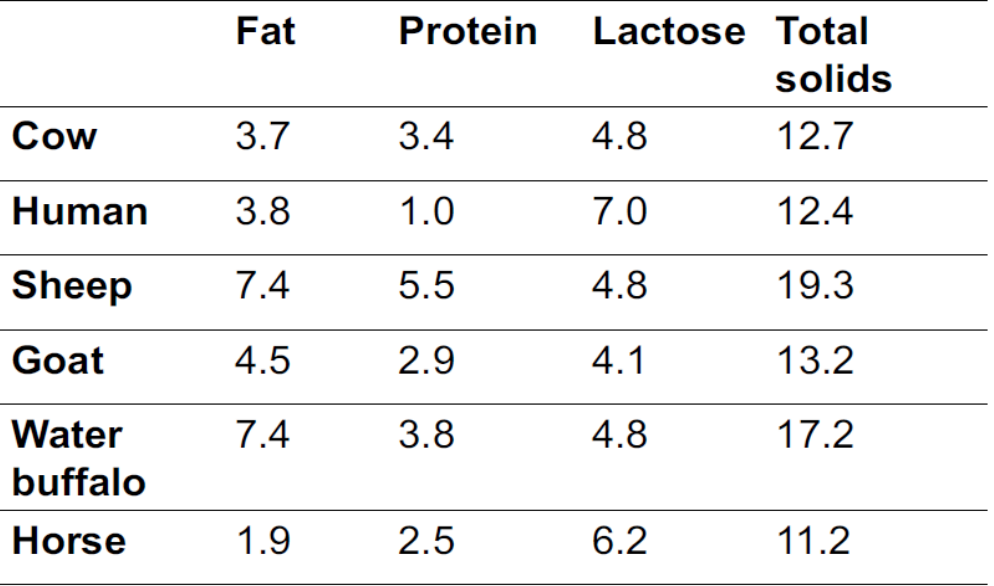
- Emulsion of fat & water containing dissolved carbohydrates, proteins, vits & minerals - that are produced in/ transported to mammary gland to provide complete nutrition & immunological protection to newborns
Components of milk:
- Water ~ 87%
- Protein ~ 3.5 %
- Fat ~ 4%
- Lactose ~ 4.7%
- Minerals ~ 0.8%
Water activity (aw) → 0.99
pH → 6.4-6.6
How is milk produced? lactation
- Following digestion necessary nutrients are absorbed from intestines into blood stream
- Nutrients are delivered to udder (high supply of blood) → allows large vol. of milk to be produced
- Nutrients used to produce accumulated milk, then secreted
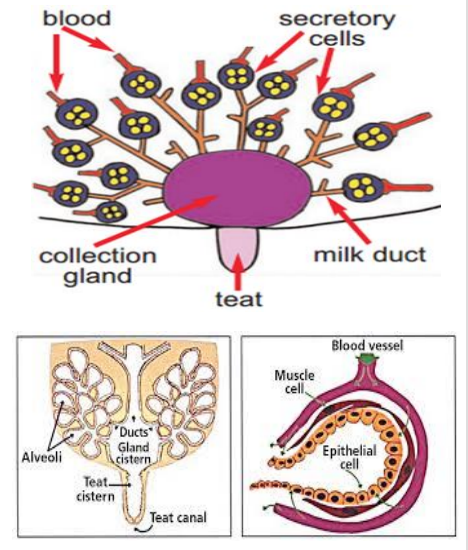
- Udder is highly developed & modified sweat gland - in cattle is composed of 4 individual glands → quarters
- Interior of each quarter comprises → teat cistern, gland cistern, milk ducts & glandular tissue
- Glandular tissue→ contains millions of microscopic sacs - alveoli
- Each alveolus is lined w/ milk-producing epithelial cells & surrounded by muscle cells that contract to squeeze milk into milk ducts when stimulated during milking (calf sucking)
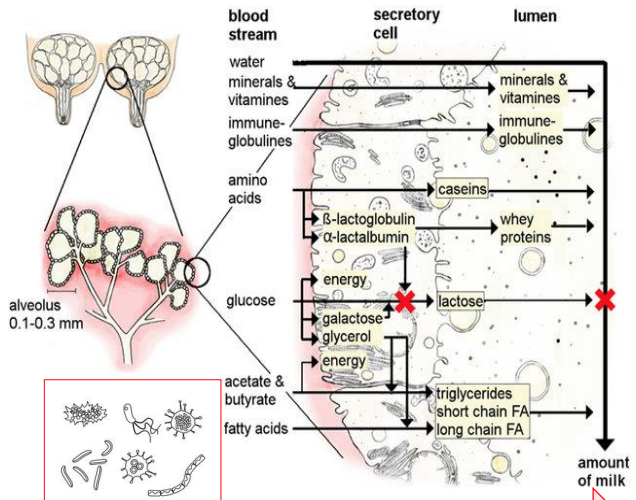
Milk formation
- Milk secreted from epithelial cells into lumen of alveoli
- Substances e.g. water, minerals, vits & immunoglobulins can pass cell membrane from blood stream
- Substance inc. proteins, lactose & fat are produced in secretory cells - then transported into lumen
- Amt. of milk regulated by lactose by influencing osmotic pressure b/w blood & alveoli
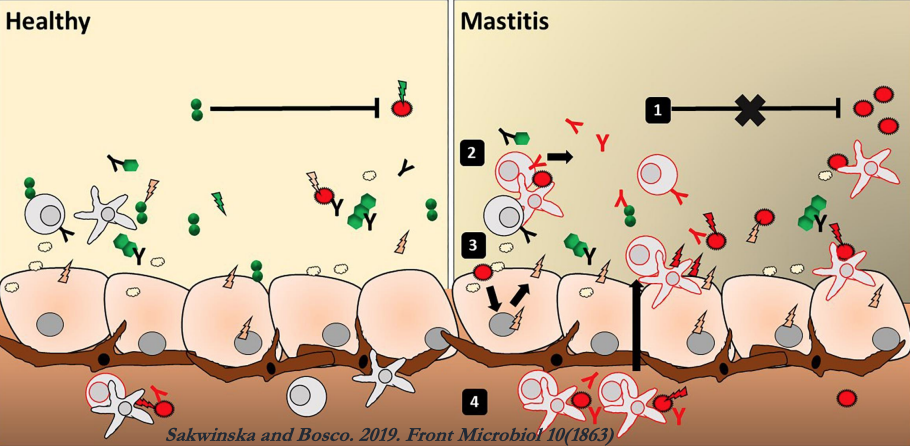
Bacteria in mammary gland
- Cross-talk b/w milk microbiota, epithelial cells & immune cells maintain a balanced, healthy environment
- Microbial imbalance that leads to infection→ commensal bacteria barely inhibit the pathogen (1); immune & epithelial cells only respond to the pathogen (2-3)
- results in massive production of pro-inflammatory mediators (cytokines, chemokines, AMPs)- causes the attraction of additional activated immune cells (4)→ leads to mastitis
![]()
Origin of human milk bacteria
- Dendritic cells go across gut epithelium to directly take up bacteria from gut lumen
- Once associated w/ dendritic cells, live bacteria spread to other locations through bloodstream
- Dendritic cells migrate using enteromammary pathway via mesenteric lymph node, so bacteria arrive at mammary gland
- mechanism explains presence & abundance of maternal gut bacteria in colostrum & breast milk
- Milk microbiota, breast milk microbiota & infant oral microbiota all continue travelling until infant gut is reached
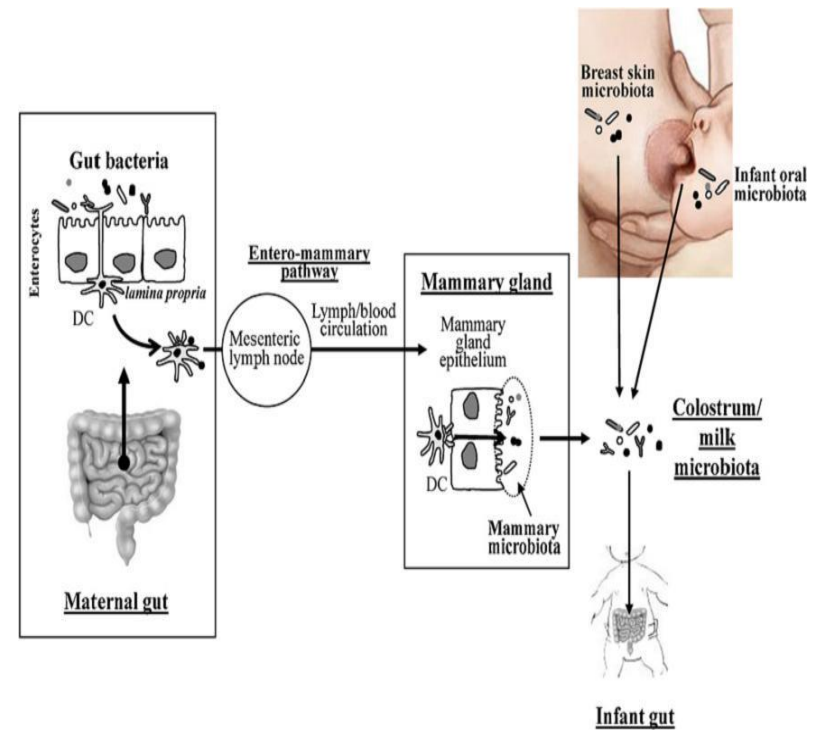
Enteromammary pathway
- When pathogen enters maternal gut, antigens are presented to immune cells that travel via blood
- IgA production induced at mammary cells & secreted as component of milk to protect infant
Maternal gut microbiome regulates neonatal gut microbiome via IgGs
- Maternal antibodies transferred placentally before birth to fetus & via breast milk to neonate after birth
- After birth, maternal milk provides 1st source of antibody-mediated protection in intestinal tract of infants against infection
- Gut microbiome can induce antigen-specific immunoglobulin G (IgG) → cross-reacts w/ pathogen antigens to promote systemic pathogen eradication in humans & animals
- Gut microbiome-induced IgG antibodies exhibit bias against Gram -ve Enterobacteriaceae e.g. E.coli - common causative bacterium in neonatal infections
- Maternal IgG antibodies cooperate w/ IgAs in neonatal gut
- Recent studies → gut microbiome-induced IgG antibodies transferred from serum to maternal milk in process facilitated by neonatal Fc receptor (FcRn)→ ↑ levels of IgG & IgA in neonatal intestine than in adult intestine & robust IgG & IgA coating of gut commensal bacteria
- FcRn expressed at high levels in epithelial cells in human mammary glands → facilitates transfer of serum IgG to maternal milk & in neonatal intestinal enterocytes to facilitate uptake of maternal milk & transcytosis to circulation
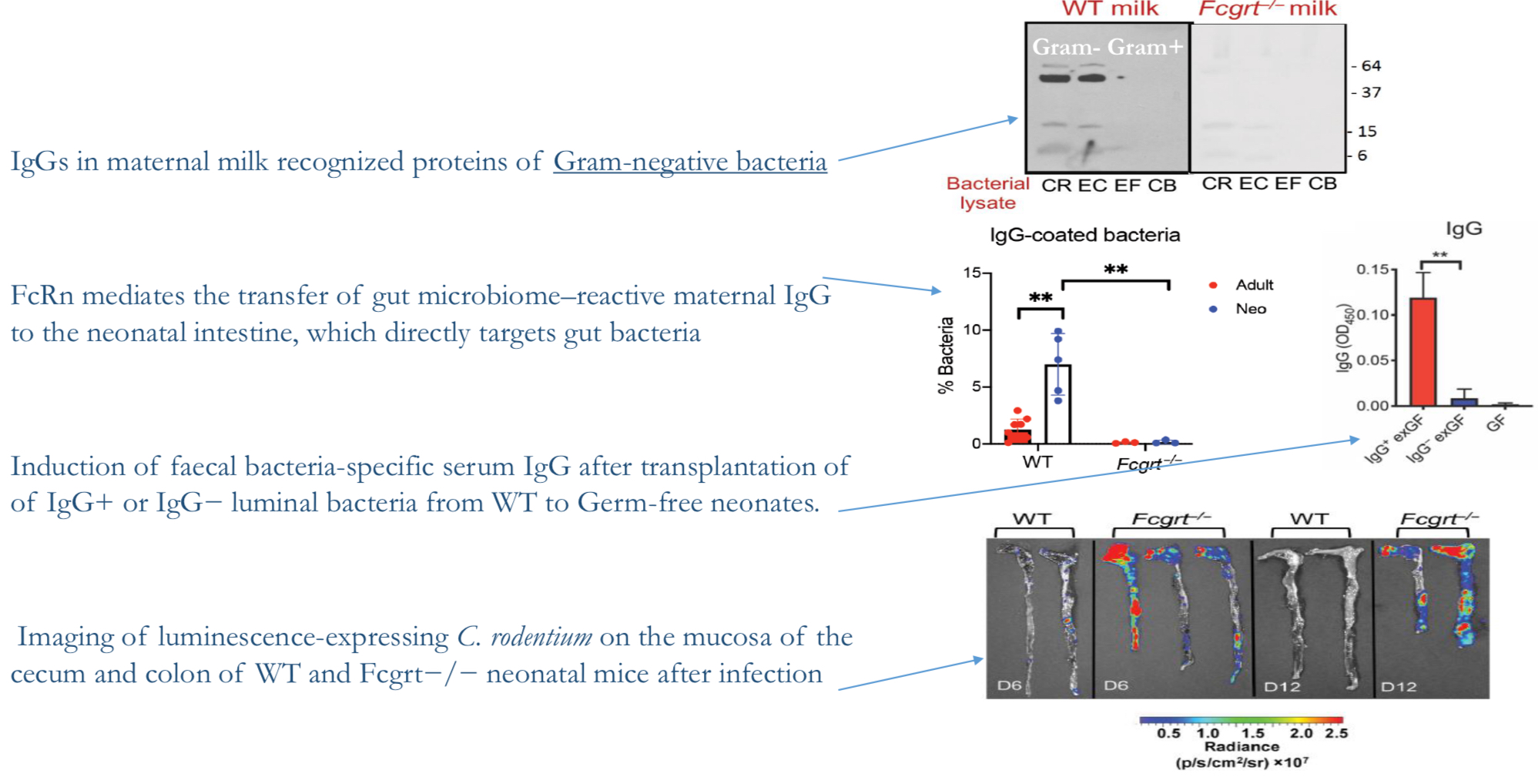
- IgGs in maternal milk recognise proteins of Gram -ve bacteria
- FcRn mediates transfer of gut microbiome-reactive maternal IgG to neonatal intestine- directly targets gut bacteria
- Induction of faecal bacteria-specific serum IgG after transplantation of IgG+ or IgG- luminal bacteria from WT to germ-free neonates
- Imaging of luminescence-expressing C rodentium on mucosa of cecum & colon of WT & Fcgrt -/- neonatal mice after infection
Milk natural antimicrobial systems
- Antibodies→ IgA, IgG

- Lactoperoxidase→ generates short lived [O] intermediates e.g. hypothiocyanite - effective in killing aerobic & anaerobic bacteria
- Xanthine oxidase→ produces antimicrobial radicals such as superoxide, nitric oxide and peroxynitrite
- Lysozyme→ degrades bacterial cell wall of Gram-positives
- Lactoferrin→ binds iron and withholds
- Phagocytes
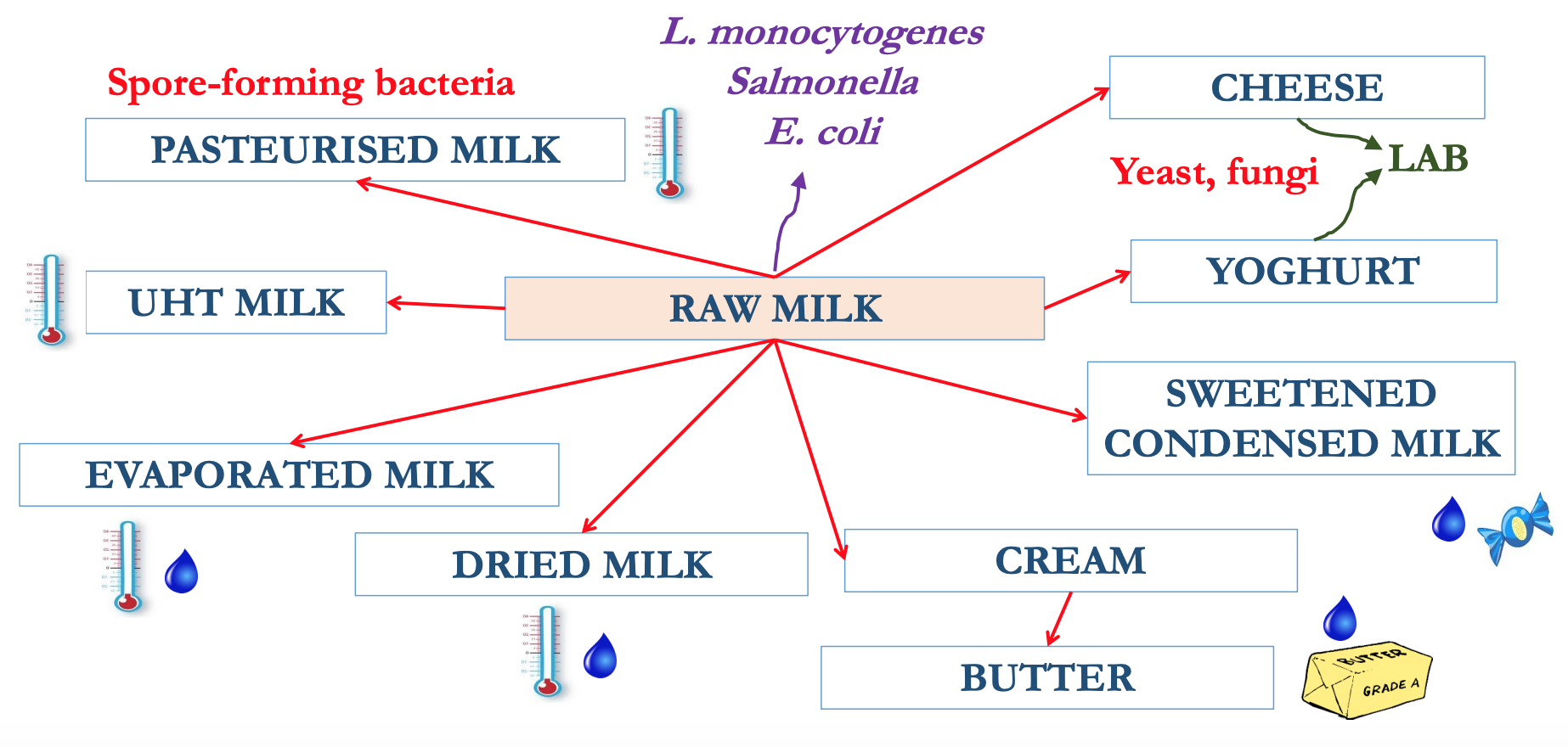
Milk Distribution
==Historically==
- ==No temperature control== →
- ==Short distribution chains== →
- ==Preservation not that important==→
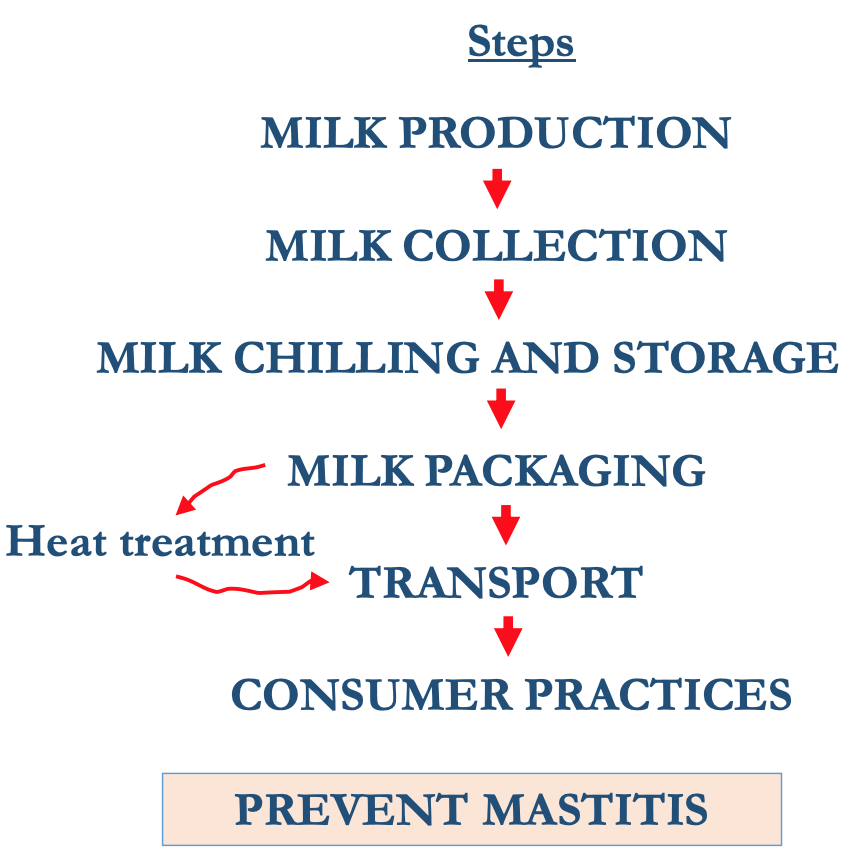
Milk distribution: factors affecting milk quality
MILK PRODUCTION→ MILK COLLECTION→ MILK CHILLING & STORAGE→ MILK PACKAGING→heat treatment→ TRANSPORT→ CONSUMER PRACTICES→ Prevent Mastitis
Important Risk Factors
- Health status, housing & herd size, silage, water source & waste management
- Milk practices, mastitis control measures, Equipment cleaning and maintenance
- Efficiency of chilling practices, equipment, personnel hygiene & sanitation
- Maintenance of chill temperatures equipment, personnel hygiene & sanitation
- Efficiency of pasteurisation
- Maintenance of chill temp- adherence to use-by-dates
→PREVENT MICROBIAL HAZARDS
Quality in distribution chain
- Mastitis prevention
- temp control
- heating
Mastitis
- Inflammation of mammary glands due to ↑ level of bacteria & somatic cells, w/ the subsequent ↓ in milk quality
- Causes major losses in milk production → clinical (25 cases per 100 cows/year) or subclinical (15-20% cows)
- Caused by 137 different organisms but 5 cause over 80% of infections:
- Staphylococcus aureus
- Streptococcus agalactiae
- Streptococcus dysgalactiae
- Streptococcus uberis
- E. coli
Methods to prevent mastitis
- Provision of clean litter
- Rapid removal of slurry
- Prevention of muddy areas
- Shave udders
- trim tails Wash teats with disinfectant
- Dry teats
- Keep parlour floor clean
- Clean teat cups
- Discard foremilk
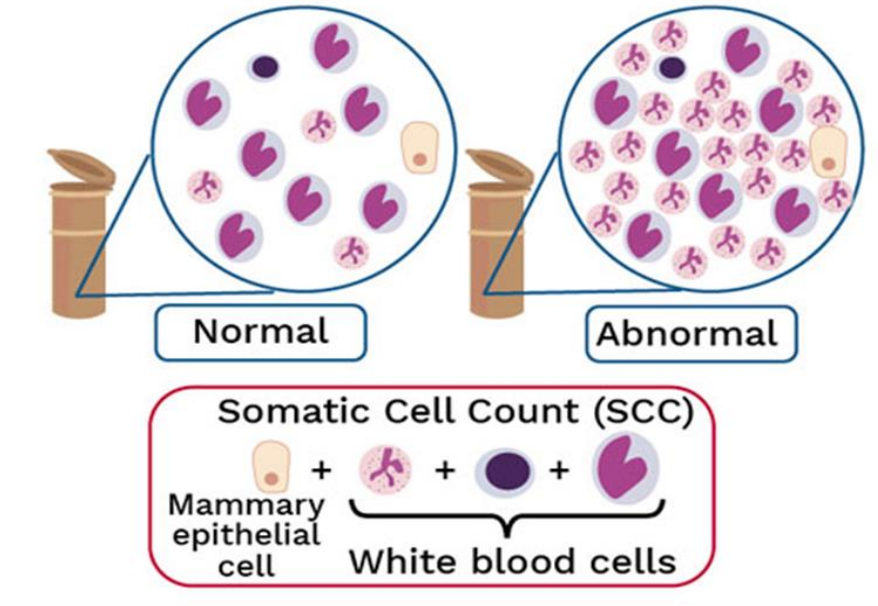
Detection
- Main indicators of milk quality
- Somatic cell count (SCC) → Plate count (PC)
- Somatic cells are a mixture of milk-producing cells (1-2%) & immune cells (98-99%)
- SCC < 100,000 cells/mL = no infection
- 200,000 cells/mL = mastitis
- EU regulations:
- PC < 100,000 mesophiles per mL
- SCC < 400,000 cells per mL
- Milk buyers pay a premium of 3-5% of milk price below threshold of 200,000 and apply reductions of 5-10% if above
The influence of farm hygiene practice
- Bacterial counts (CFU/ml)

Temp control
- Farm bulk tank→ refrigerated (< 4ºC for < 48h) = 103 CFU/mL
- Road tanker→ insulated (< 6ºC for 1-8h) = 103 -104 CFU/mL
- Rejected if > 7ºC
- Silo at dairy→ insulated (6-8ºC) or refrigerated (2-4ºC)
- < 104 CFU/mL in the silo
- < 105 CFU/mL before pasteurisation
Heating: pasteurisation/UHT
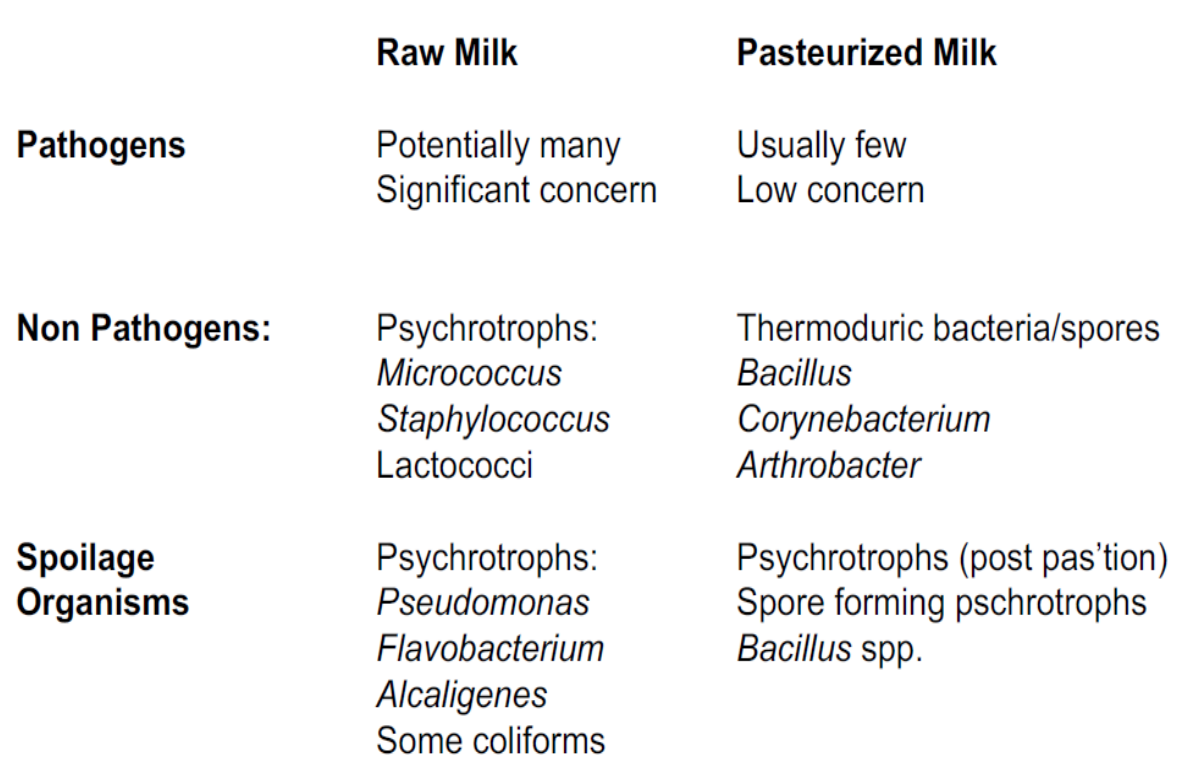
Milk spoilage → Psychrotrophic bacteria
- Refrigerated raw milk may contain psychrotrophic bacteria that produce thermoresistant exo-proteases and lipases → compromise the quality of dairy products during storage
- Carbohydrates
- 𝘓𝘢𝘤𝘵𝘰𝘤𝘰𝘤𝘤𝘶𝘴 𝘭𝘢𝘤𝘵𝘪𝘴 converts: lactose→ Lactic acid (produces sour taste/smell?)
- Proteins
- 𝘓𝘢𝘤𝘵𝘰𝘤𝘰𝘤𝘤𝘶𝘴, 𝘌𝘯𝘵𝘦𝘳𝘰𝘣𝘢𝘤𝘵𝘦𝘳, 𝘚𝘦𝘳𝘳𝘢𝘵𝘪𝘢, 𝘈𝘦𝘳𝘰𝘤𝘰𝘤𝘤𝘶𝘴 𝘢𝘯𝘥 𝘉𝘢𝘤𝘪𝘭𝘭𝘶𝘴 converts: Caseins & whey proteins → Short peptides, amino acids, amines (produces bitter, putrid smell/ taste?)
- Lipids
- 𝘓𝘢𝘤𝘵𝘰𝘤𝘰𝘤𝘤𝘶𝘴, 𝘈𝘦𝘳𝘰𝘤𝘰𝘤𝘤𝘶𝘴 𝘢𝘯𝘥 𝘈𝘤𝘪𝘯𝘦𝘵𝘰𝘣𝘢𝘤𝘵𝘦𝘳 converts: Short-chain fatty acids (produces rancid flavour)
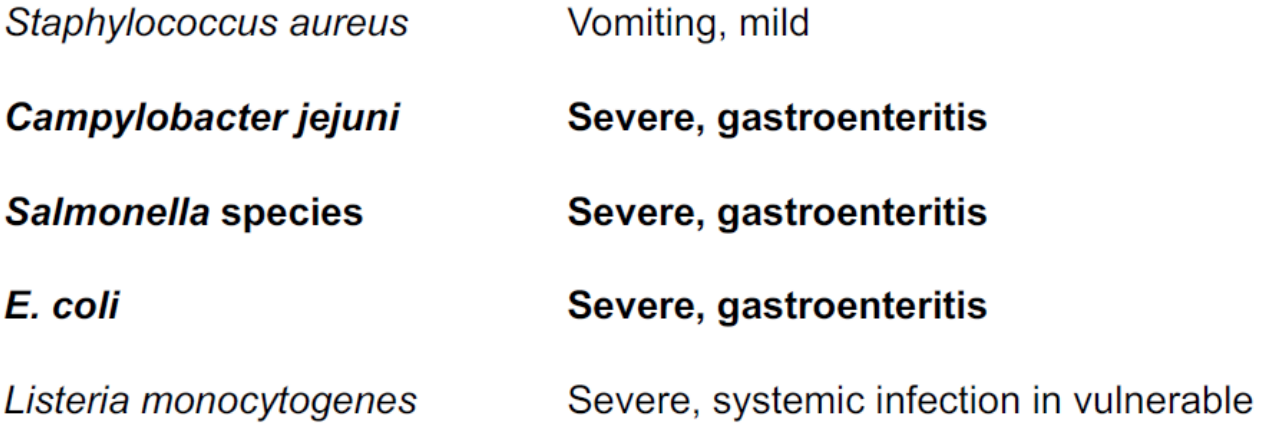
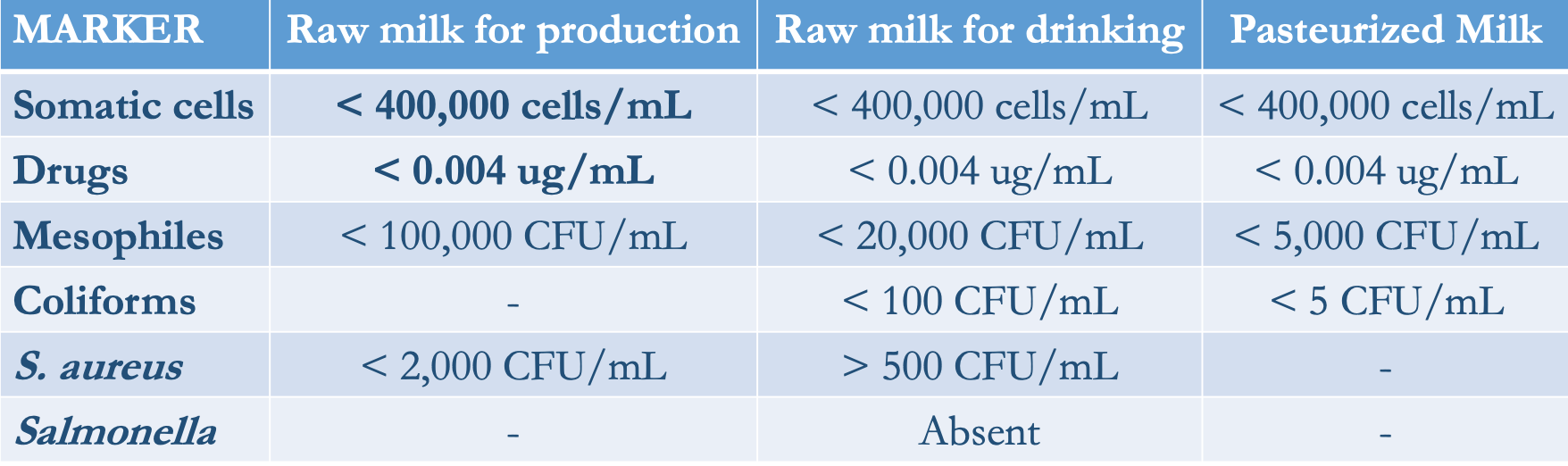
Microbial hazards in milk today
 \n
\n 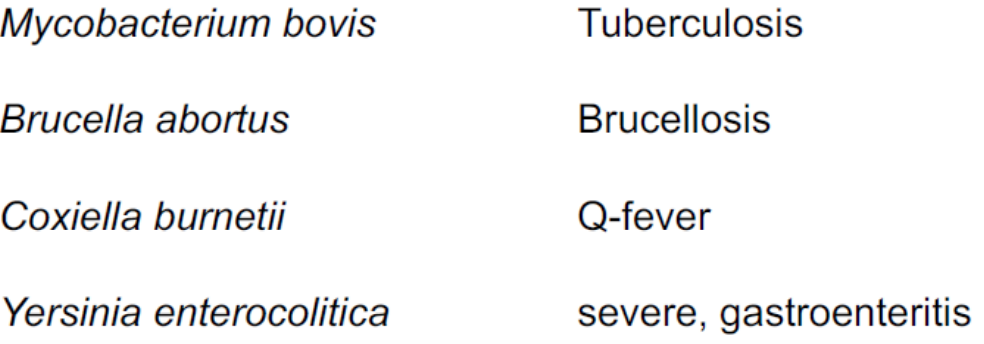
Milk legislations & testing
- EU Council Directive 92/46/ECC lays down the health rules for the production and distribution of milk and dairy product on the market
- Milk can only come from herds that are officially TB-free (and Brucellosis-free)
- Pasteurised milk must pass the phosphatase test to assure the effectiveness of the process
Honey
Sweet, viscous substance made from floral nectar by bees & some related insects
Produced after ingestion, enzymatic activity, regurgitation & H2O evaporation
- Water~18%
- Fructose~40%
- Glucose~ 30%
- Other sugars~ 10%
- Minerals~ 2%
- water activity (aw) → 0.60
- pH → 3.4 - 5
History
- Earliest evidence of humans collecting honey is a cave-painting in Valencia, on Spain's eastern coast, thought to date from around 8000 BC
- Since about 4000 BC, the ancient Hindi medical theory of Ayurveda outlined honey's medicinal qualities in treating burns, allergies & infections
- Western cultures have eventually caught up by devising honey-based wound dressings & oral medicines.
- Composition of honey varies greatly - depends on the local flora in the bees' immediate environment
- Bees visit various flowers making honey w/ diff. healing properties - scope for finding new uses for honey is vast.
How is it produced?
- Bees collect nectar using their tongue
- It goes to their honey stomach (40 mg of nectar)
- Enzymes break down sucrose into glucose & fructose
- Digested nectar is regurgitated, placed in honeycomb cells & left unsealed
- Fermentation → LAB & yeasts (acidity)
- Bees flutter their wings to circulate air & evaporate H2O (sugar conc. ↑ & then sealed with wax)
- Food supply (E) or removed by beekeepers