Neuroanatomy & Psychiatric Disorders - prereading
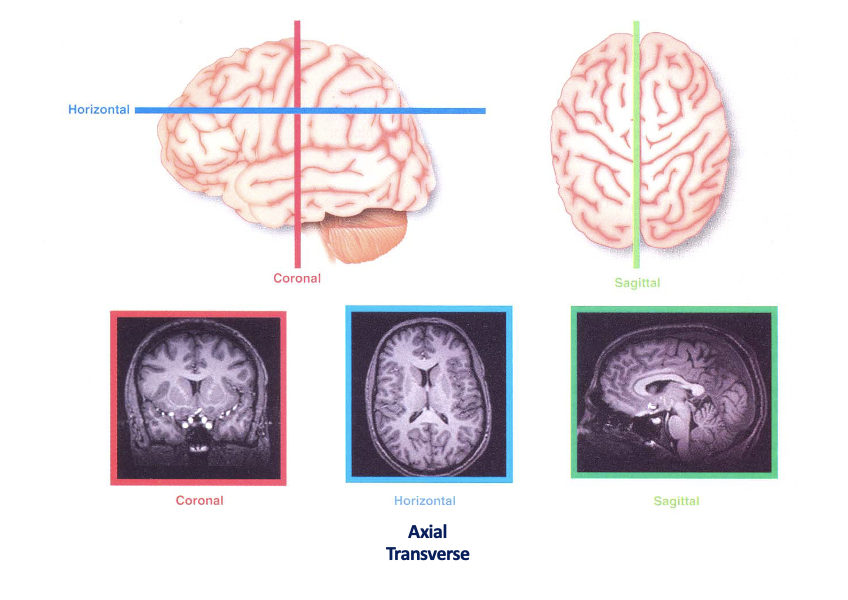
<<Planes of the brain<<
- White matter": Mainly axons due to myelination (lipid/ fatty sheath)
- Grey matter: neuronal cell bodies
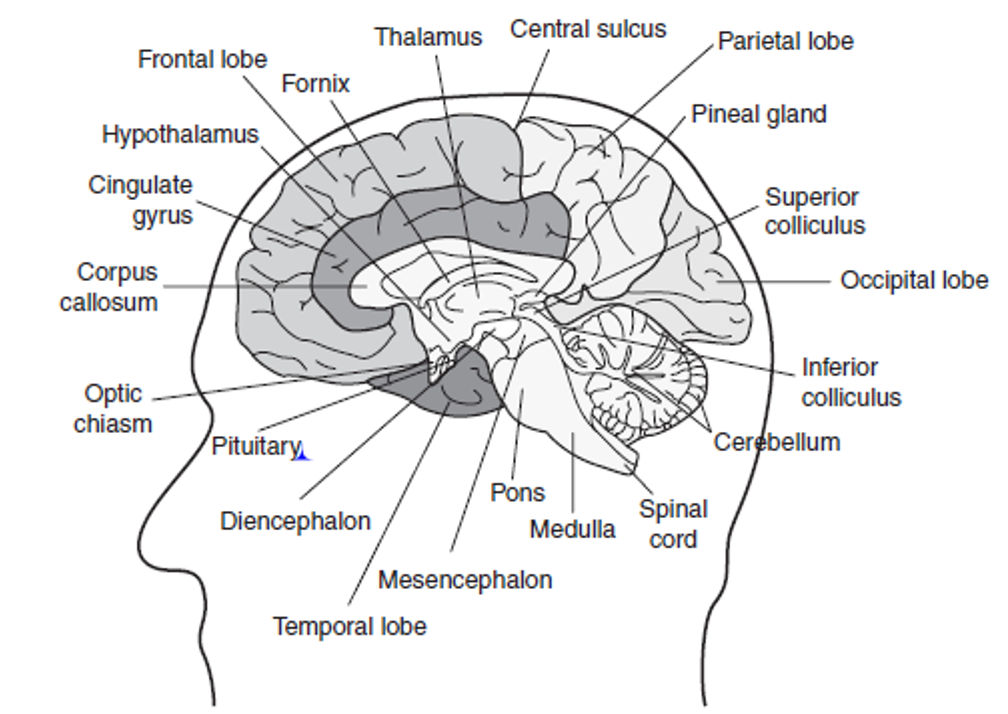
}}Main regions of the brian}}
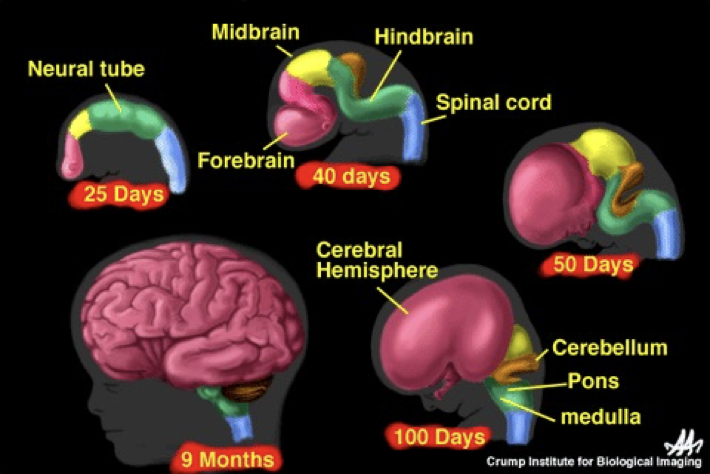
]]Embryology]]
- Refer back to case 7 embryology on the formation of the spinal cord
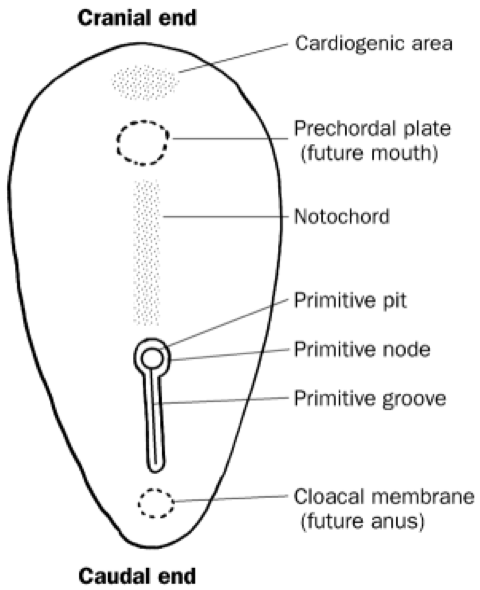
- The neural tube then splits into the main parts of the brain
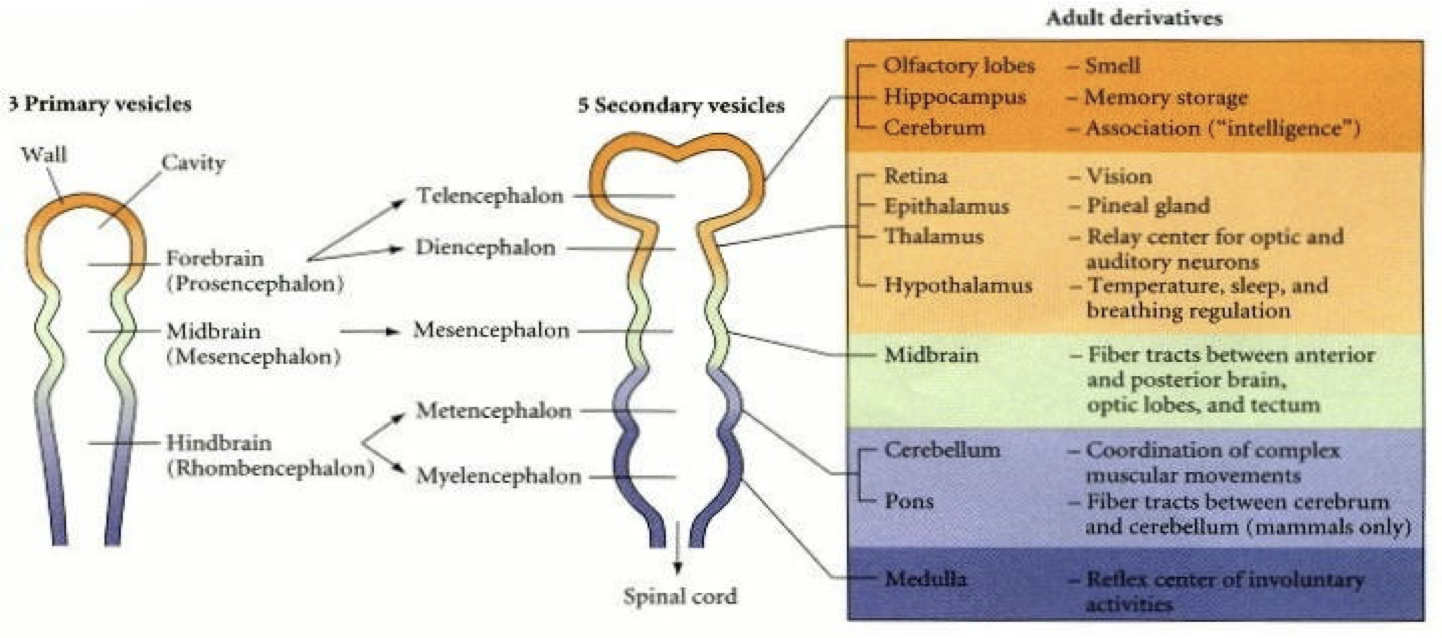
]]Rhombencephalon]]
- Brain stem
- Cranial nerves + normal nerves run from the medulla
- The cerebellum + pons are important in co-ordinating movements + responding to external stimuli
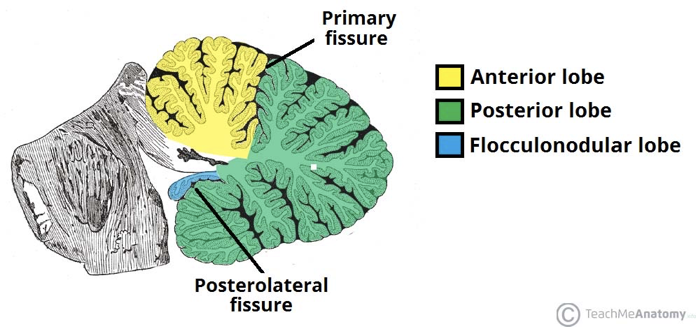
{{Cerebellum - divided i nto 3 lobes:{{
- Flocculonodular lobe
- Vestibulocerebellum/ archicerebellum
- Regulates balance + co-ordination (oldest)
- Posterior lobe
- Anterior lobe
- Contains Purkinjie + granule cells
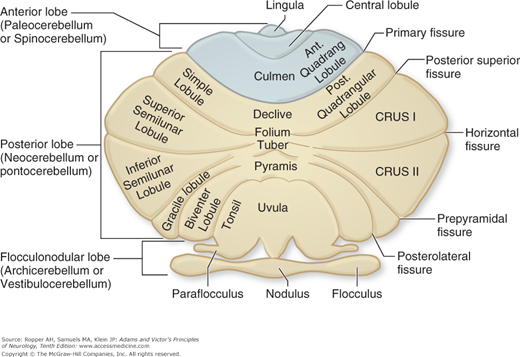
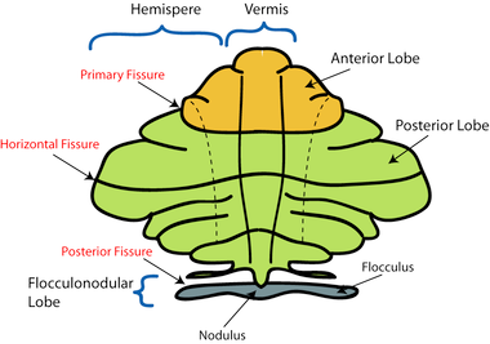
- Areas closest to the vermis- spinocerebellum/ paleocerebellum
- Spinocerebellum: regulates body temperature + limb movement
- Laterally- neocerebellum
- Neocerebellum:
regulates planning,
sensory movement for action
]]Cerebellar Disorders]]
- Damage of the neocerebellum causes ataxic gait e.g. stroke or alcohol-related
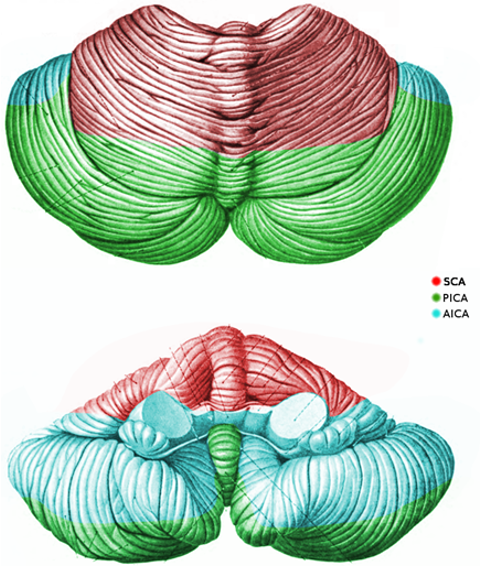
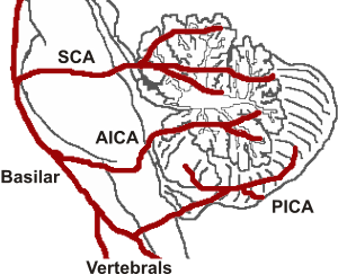
- Cerebellum has a complex arterial supply
- Therefore, it is important in cases of stroke or vertebral/ basilar artery dissection (present with cerebellar signs
]]Pontine disorders]]
- locked-in syndrome
- Central pontine myelinolysis
- Progressive Supranuclear Palsy (Steele-Richardson-Olszewski):
- Supranuclear ophthalmoplegia
- Neck dystonia
- Parkinsonism
- Pseudobulbar palsy
- Behavioural impairment
- Imbalance
- Frequently falls
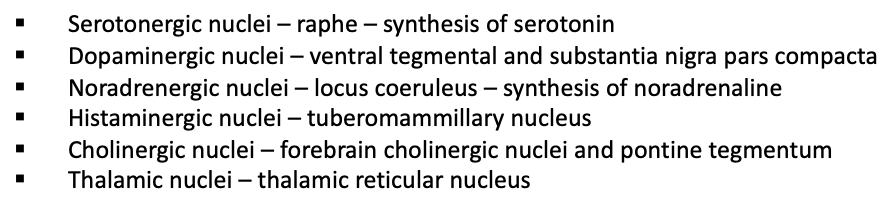
]]Reticular formation]]
- Allows for communication of the brain to the rest of the body
- A hub for the synthesis of neurotransmitters and wake/sleep state
- Ascending/ descending through the brainstem
- Includes ascending reticular activating system- role in arousal
<<Mesencephalon<<
- Midbrain
- Acts as a connector between different parts of the brain
- links everything together
- Don’t worry too much about the next info
Parts of the midbrain
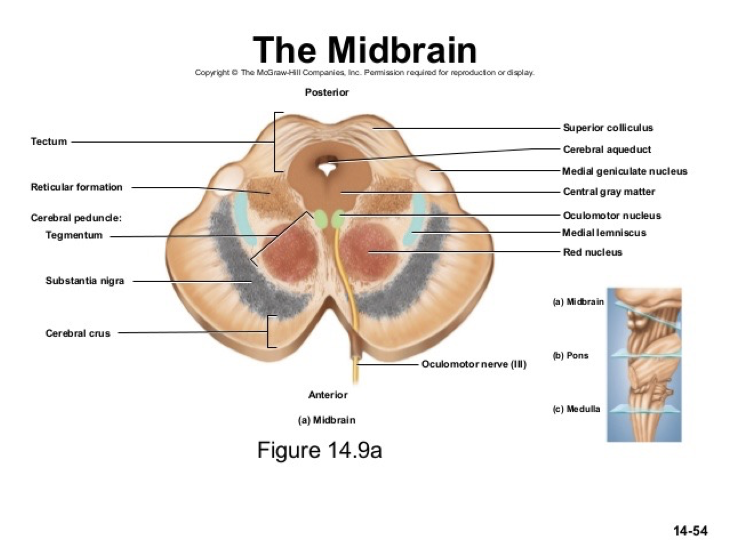
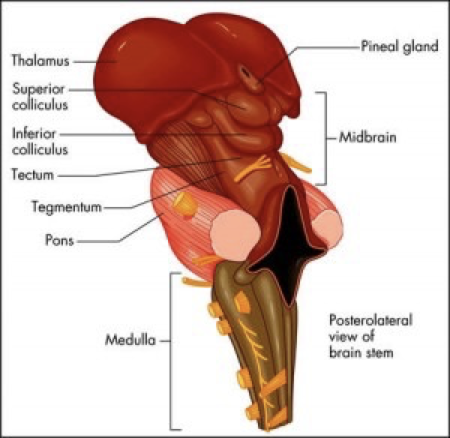
- Tectum (dorsal part) splits into:
- Superior colliculus- visual processing + eye movement control
- Inferior colliculus- auditory processing
![]()
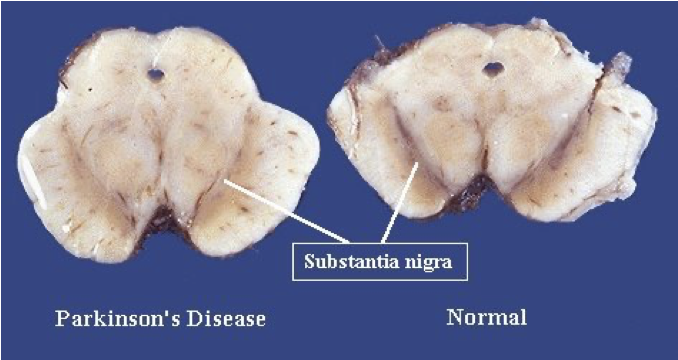
]]Disorders of the mesencephalon]]
- Parkinson’s - reduction in dopaminergic neurones in substantia nigra
- Schizophrenia- increased dopamine in substantia nigra
- Multi-system atrophy- degeneration of striatum and substantia nigra
- Ventral tegmental area- primary sites of addictive drugs (heroin, cocaine, alcohol, nicotine)
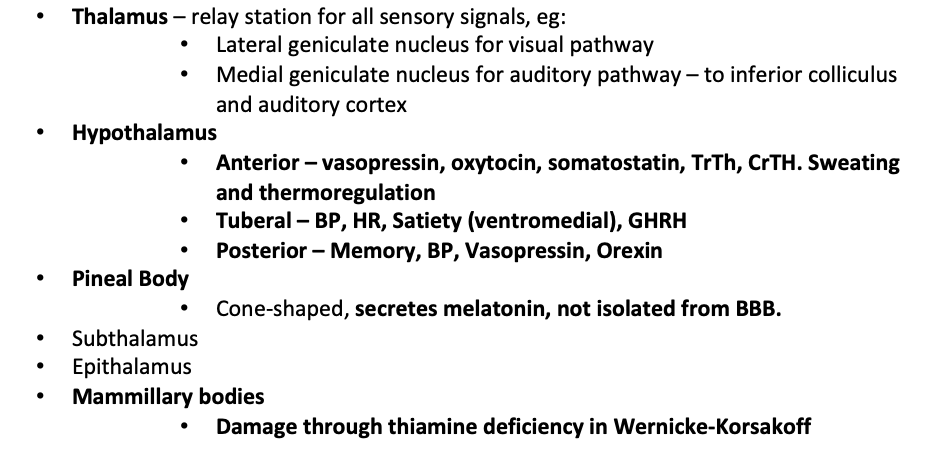
]]Diencephalon]]
Contains:
- Thalamus
- Hypothalamus
- Pineal Body
- Subthalamus
- Epithalamus
- Mammillary bodies
Limbic system:
- Connects cortical control to memory / sensory/ secretory areas
- Involved in motivation, visceral processes + rewards
- Systems of emotions
- Connects a group of structures surrounding the brainstem (cingulate gyrus, hippocampus, hypothalamus + anterior thalamic nuclei)
- Connecting these structures enables cortical control of emotion + plays a role in storing memory
]]Telencephalon]]
- higher functions such as smell, memory + Intelligence
Hippocampus
- Medial temporal lobe
- Short-term memory to long term memory
- Spatial memory
- Includes dentate gyrus + granule cells - formation of new episodic memories, site of neurogenesis, affected in depression
- Alzheimer’s + dementia → hippocampal atrophy → memory symptoms
Cortex
- Memory
- attention
- Cognition
- awareness
- thought
- language
- consciousness
- 4 lobes, gyrus (fold) + sulcus
Frontal lobe
- Superior frontal gyrus = self-awareness/ laughter
- Middle frontal gyrus
- Inferior frontal gyrus = language processing, Broca’s area
- Medial frontal gyrus = executive mechanism
- Paraolfactory area= limbic
- Orbitofrontal cortex= stimulus-reward, stimulus/outcome, addiction
- Ventromedial prefrontal cortex- decision making, emotion regulation, addiction
- frontotemporal dementia/ Pick’s disease = genetic + accumulation of tau + frontal symptoms
Prefrontal cortex
- Planning + executing actions
- One of the last to develop
- lesions:
- Dramatic changes in personality
- Loss of spontaneity/ problems with initiating speech/ movements
- inability to make + carry out sequences of actions/plans
Parietal lobe
Integrates sensory information
Dominant hemisphere lesions:
- Dysphasia, aphasia
- Dyscalculia- difficulty learning, doing calculations
- Dyslexia
- Apraxia- ability to execute or carry out skilled movements and gestures, despite having the desire and the physical ability to perform them.
- Agnosia- inability to recognize and identify objects or persons.
- Gerstmann syndrome- Dyscalculia, Dysphasia, finger agnosia, LR disorientation
Non- dominant hemisphere lesions:
- Spatial disorientation
- Constructional apraxia
- Dressing apraxia
- anosognosia- unaware of their own health problems
Temporal lobe
- Transeverse temporal gyri - Heschl’s gyri
- Superior temporal gyrus= auditory context with TTG. Pricess perception of sound + apply comprehension.
- Posterior STG = wernicke’s area
- Middle temporal gyrus
- Fusiform gyrus = FACIAL RECOGNITION, synaesthesia, dyslexia, prosopagnosia
- Inferior temporal gyrus= visual object recognition
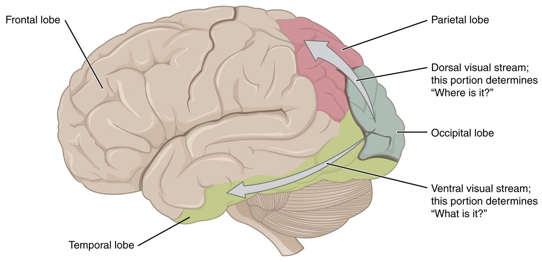
Occipital lobe
- Lingual gyrus
- role in vision + dreaming
- Visuo-limbic integration
- encoding complex images
- word processing
- Cuneus - basic visual processing
- Calcarine sulcus/fissure
- primary visual cortex
- takes signals from geniculate nucleus via thalamus
Tracts- only for reference
- Arcuate fasciculus- links Broca’s + Wernicks area
- Uncinate fasciculus
- Links temporal inferior frontal gyrus + frontal lobe
- Hippocampus + amygdala with orbitofrontal cortex
- implicated in several psych conditions
- 2 visual streams hypothesis:
- dorsal - where?
- ventral- what?
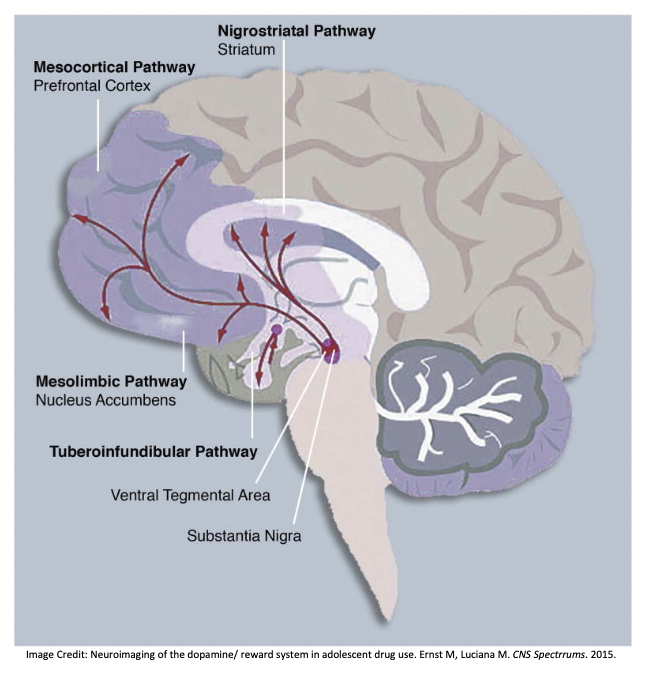
Central dopamine hypothesis
- Meso-cortical pathway
- Meso-limbic pathway
- Nigrostriatal pathway
- Affected in schizophrenia + other psych disorders
- Medications for scz work on this pathway
- Side effects of these meds are linked to these pathways (e.g. cog-wheel rigidity like that seen in parkinson’s/ galactorrhea due to pituitary stimulation)
]]Alzheimer’s Dementia]]
- Microscopic accumulations of peptide amyloid-β – plaques → cause loss of synapses, then neurons.
- Progressive degeneration
- Early changes in the hippocampus (first to be damaged)
Generalised shrinking and enlarged ventricles follow
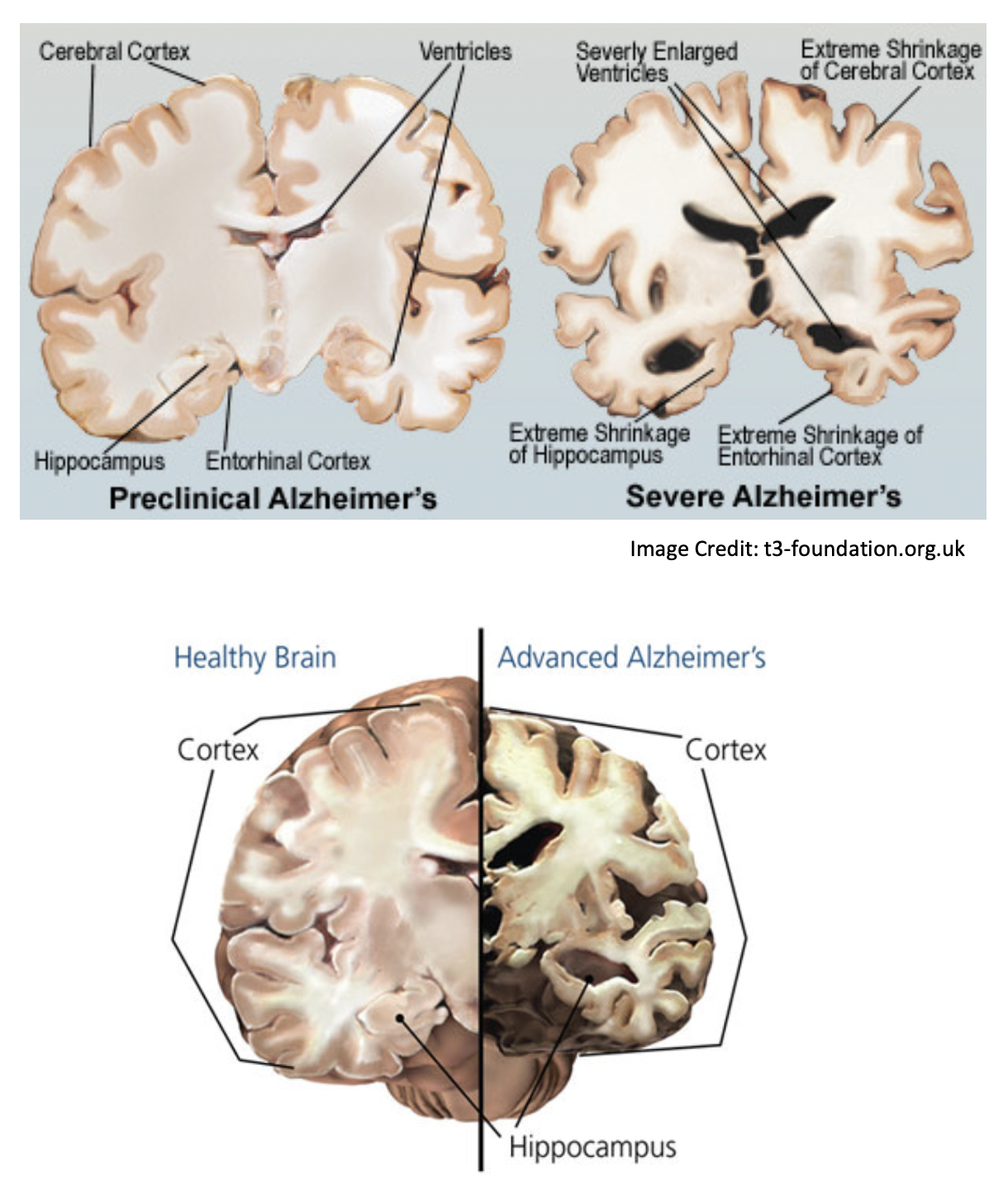
- In severe depression, the dentate gyrus don’t light up in the scans which means they don’t form many memories.
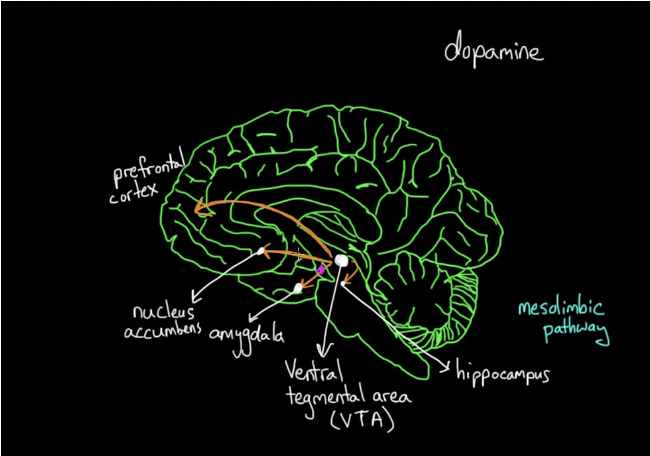
]]Drug misuse]]
- The reward system is based on dopamine.
- It activates all dopamine pathways, particularly the mesolimbic pathway.
- Dopamine is produced in the Vental Tegmental Area (VTA).
- The mesolimbic pathway links this to the Nucleus Accumbens (motivation/ reward).
- If we do something good, or use an addictive drug, this pathway is stimulated.
- The mesocortical pathway is also activated.
- This links to the Prefrontal Cortex (PFC).
- This changes how you prioritise and plan.
]]Disorders]]
Case 1- depression after frontal tumour
- 56 year old female
- Progressive apathy
- Social withdrawal
- Poor self-care for part 3 years
- Admitted to a psychiatric facility for depression
- unresponsive to antidepressants so CT was conducted
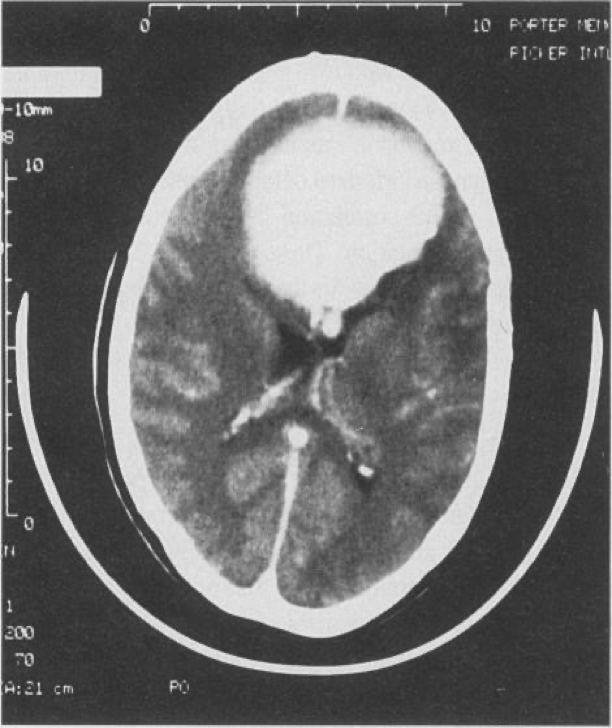
- 8cm medial bifrontal mass
- Total excision benign transitional-type meningioma → rapid improvement
- 4 months after the operation was cheerful + motivated
Case 2- Psychosis after temporal tumour
- 18-year-old female
- Referred form school to a psychosis clinic (high risk)
- 2 years of withdrawal from social activities + resent from work groups or talking in public
- 1 year later became concerned about unknown people stating + laughing at her for no reason
- Feeling the world around her has changed
- She is concerned that people are intimidating her + that there are special messages in TV for her
- She is neurologically normal + an average IQ
- Initial diagnosis: prodromal syndrome of schizophrenia but symptoms became more rapidly severe
- Routine MRI conducted
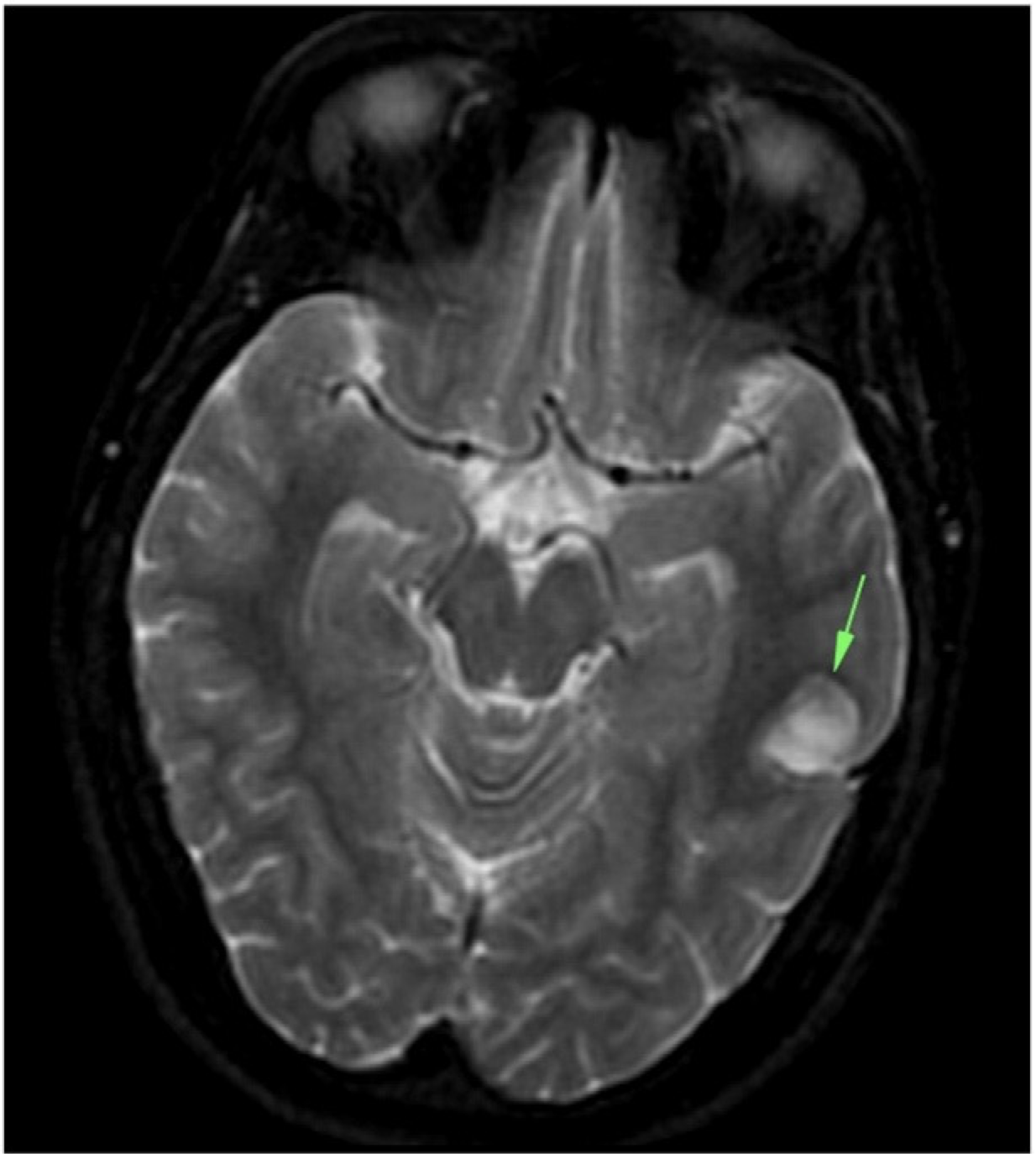
- Tumour in the left temporal lobe - dysembryoplastic neuroepithelial tumour (DNET)- usually benign glial neural neoplasm
- Surgically remove
- Psychotic symptoms improved with the help of other treatments- risperidone + CBT
- However, remained socially withdrawn
Case 3- bipolar effective disorder due to Wilsons disease
- Middle aged female
- Detained + admitted under section 2 of the Mental Health Act (MHA) 2007- decline in her mental state
- Initially aggressive behaviour + required restrain by the Emergency Department security + police
- Quietly spoken
- voicing paranoid persecutory delusions
- euthymic with labile affect
- alternating between anger
- tearfulness
- displaying disinhibited affection
- Doesn’t know why she was presented
- CT

- Hypodensity in the putamen, worse on the left
- No mass, infarct or infectious process to explain the lesions
- Consistent with the MRI from a couple of months ago which demonstrates hyperintensity of both putamina
- Associated with Wilson’s disease
- final diagnosis: psychosis secondary to neurological Wilson’s Disease
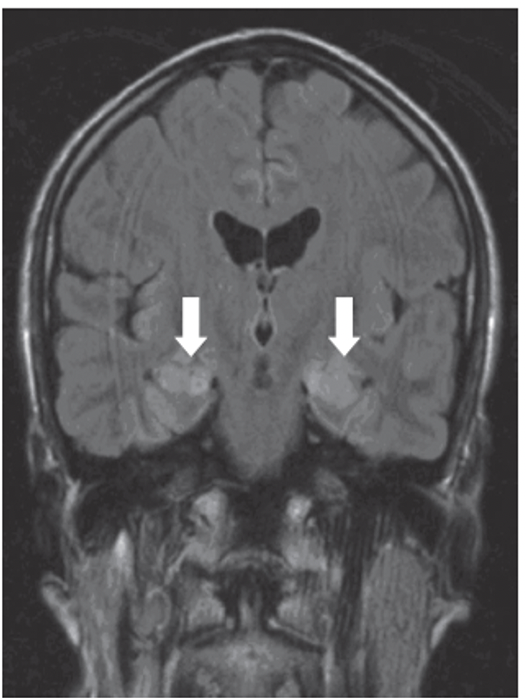
Case 4- Psychiatric syndromes associated with neurological disease
- 63-year-old male
- paranoia
- impaired anterograde memory + fatigue
- FLAIR scan shows bilateral hyperintensities in the hippocampus (arrows) → shows inflammatory process
- Blood tests revealed anti-voltage gated potassium channel antibodies