Respiration Exam
- Anatomical Position: Subject is always facing forward and you are looking at the subject that way
- Medial: Toward the midline of the body, which splits the body, head-to-toe, into two halves, the left and the right
- Lateral: Relating to the side, lying away from the median axis of the body. The lungs are lateral to the heart.
- Anatomy: The study of the structure of organisms and the relations of their parts
- Physiology: Science dealing with the function of living organisms
- Anterior (ventral): in the front of the sternum is on the anterior surface of the body
- Posterior (dorsal): in the back of the vertebrae are on the posterior surface of the body
- Superior (cranial): toward the head – high. The eyebrows are cranial to the eye
- Inferior (caudal): away from the head – low. The mouth is caudal to the nose
- Superior and inferior is used together
- Cranial and caudal is used together
- Superior/inferior is not used together with cranial/caudal
- Medial: toward the midline of the body.
- Medial Example. The sternum is medial to the arm
- Lateral: away from the midline of the body
- Lateral Example. The hip is on the lateral surface of the body
- Proximal: closer to any point of reference
- Proximal Example. The knee is proximal to the foot
- Distal: farther from any point of reference
- Distal Example. The foot is distal to the knee
- Superficial (external): located close or on the body surface
- Superficial Example: The skin is superficial to the muscles
- Deep: (internal)
- Coronal (frontal): divides the body into anterior and posterior portions
- Sagittal: divides the body into right and left sides
- Transverse: horizontal cut (divides the body into superior and inferior portions)
- Adduct: close
- Abduct: open
- Supine: laying face up
- Prone: laying face down
- Suture Line
- Coronal Suture: Divides anterior and posterior
-|-
The Cell: The basic structural and functional unit of all living things
Cells are: Highly organized masses of protoplasm (semifluid gel that consists of protein, CHO, Lipids, Nucleic acids and inorganic materials dispersed in water)
How many cells are in the human body? 100 trillion cells in the human body
Cell Function: Metabolism (use of food and oxygen to build or repair tissue), Excretion, Response to stimuli, Mobility
Cell Structure: Golgi Complex (apparatus), Organelles
Tissue: Colonies of cells combined together in such a manner as to exhibit functional unity
Cell to system order: Cell > Tissue > Organ > System
Types of Tissue: Epithelial, Muscular, Connective, Nervous, Vascular, Epithelial Tissue
The cells of epithelium form: sheets that cover the external surfaces of the body
Connective Tissue: Connects and binds the structures together, Supports the body systems
Loose connective tissue found: beneath the skin
Two types of connective tissue Dense connective tissue and Loose Connective Tissue
Areolar: forms the “bed” for skin and mucous membranes, found almost everywhere in the body
Adipose: Similar to areolar but has high fat content. Fatty tissue
Dense Connective Tissue: Collagenous + elastic fibers
Tendons: nonelastic fibers that connect muscle to bone
Ligaments: somewhat elastic fibers that connect bone to bone, bone to cartilage, or cartilage to cartilage
Aponeurosis: Covering muscles, connects muscle to muscle
-|-
- Special Connective ____: Tissue
- Cartilage: Softer than bone, Flexible, Capable of growth, Covered by a tough fibrous membrane called perichondrium
- Cartilage is dound in three forms: hyaline, elastic, fibrocartilage
- Hyaline Cartilage: Extremely strong and somewhat unmovable, Poor blood supply, Susceptible to ossification (calcification),
- Hyaline Cartilage is very important in: studying the speech mechanism
- Hyaline Cartilage is found in: nose, flexible ends of ribs, surfaces of bones at joints, cartilages in the larynx (thyroid and cricoid)
- Fibrocartilage: Very strong and dense
- Elastic cartilage: Highly flexible, Rubbery in consistency, Ossification rarely occurs
- Elastic Cartilage is found in: Epiglottis, External part of the ear (pinna), Corniculate cartilages of the arytenoids (larynx)
- Bone: The most important supporting structure of the body, hard (not flexible like cartilages)
- Bone Classification: Classified by shape
- Long bones: found in arms and legs
- Short bones: found in the fingers
- Flat bones: found in the skull, shoulder blades and pelvic girdle
- Joints: The meeting of two or more bones whether there is movement or not
- Fibrous Joints: Do not have articulatory space
- Bones are connected by: fibers
- Cartilaginous Joints: Do not have articulatory space
- Bones are connected by a cartilaginous disc: cartilaginous
- Spinous process: The spinous process is a piece of bone that comes off the back of the lamina at every level. It provides an attachment for muscles. When you feel down someone's back, the spinous processes are the bony bits that you can feel in the middle of their spine.
- Intervertebral disk
- Symphysis: a place where two bones are closely joined, either forming an immovable joint (as between the pubic bones in the center of the pelvis) or completely fused (as at the midline of the lower jaw). (oxford dictionary)
- Synovial Joints: also known as diarthrosis, joins bones or cartilage with a fibrous joint capsule that is continuous with the periosteum of the joined bones, constitutes the outer boundary of a synovial cavity, and surrounds the bones' articulating surfaces. (Wikipedia)
- Ball and socket: Consists of a rounded ball-like end of bone that fits into a cup-like cavity in another bone, Movable around a great number of axes
- Ball and socket joint examples: hip joint, shoulder joint
- Finger Joint: Simple Synovial Joint. Has a fibrous membrane and synovial cavity
- Hinge Joint: Permits movement in one plane (flexion and extension)
- Hinge Joint Examples: elbow joint
- Ellipsoid-condyloid Joint: An oval-shaped articular facet fits into an elliptical-shaped cavity
- Ellipsoid-condyloid joint: Permits movement in all directions except rotation
- Ellipsoid-condyloid joint Examples: temporo-mandibular joint (T-M)
- Muscle-Tissue: Striated (skeletal): often called voluntary muscle, attachments mainly to the skeletal system (supplied by Peripheral Nervous System- PNS)
- Smooth (visceral): involuntary organs such as stomach and intestines, blood vessels, and bronchial tubes (autonomic nervous system)
- ardiac: found only in the heart
- Muscle Cell: The smallest functional unit of the muscle tissue
- Muscle Activity: A muscle does only 2 things. it contracts (shortens) and relaxes (returns to the original position
- Contracts- shortens
- Relaxes- returns to the original position
- Action Potential: Every cell has its equilibrium potential
- Action Potential: a sudden large change in the cell polarity that causes a wave of depolarization
- Myosin and actin: molecules inside muscle fiber that control contractions
- ATP (produced by mitochondria) is an energy source that is added during muscle contraction so myosin and actin can react. Adenosine Triphosphate
- All or None Law: Each fiber contracts maximally or not at all
- Constant muscular contraction: always on
- Isometric: contracts a muscle, tension changes but length does not
- Isotonic: muscle shortens upon contraction but tension does not change
- What causes isotonic contractions: Sliding activity of myosin and actin
- Origin: place of attachment of a muscle which remains fixed during contraction
- Insertion: area of attachment of muscle to bone. It moves, more flexible
- Contraction- decreases the distance between origin and insertion
- Agonists: muscles work together
- Antagonists- muscles that produce opposite movement
- Synergist: act around a moveable joint to produce motion similar to or in concert with agonist muscles. They often act to reduce excessive force generated by the agonist muscle and are referred to as neutralizers. (Med Libre Texts)
- Nervous Tissue: monitors and regulates the functions of the body. consists of two cells- nerve cells or neurons and glial cells, which helps transmit nerve impulses and also provides nutrients to neurons. (Byjus)
- Organs: When two or more tissues combine in such a manner as to exhibit functional unity, Performs a special function
- Systems: 11 systems 5 of which are of importance to our class. Nervous, skeletal, articular, muscular-movement, urinary, reproductive, endocrine, integumentary, respiration
- Nervous system: brain and spinal cord
- Respiratory: breathing system
- Skeletal: structural support system
- Articular: articulation system
- Muscular- movement: muscle movement system
- Urinary: urinary system
- Reproductive: reproductive system
- Endocrine: hormones
- Interaugmentary: Outer layer of the body
- Respiration: Breathing
- Biological function example: Exchanging gas in the body
- Speech function example : Power supply to stimulate/vibrate the vocal folds. The power supply for stimulating vocal folds and producing voice
- Inhalation: air is taken through respiratory tract to lungs and held there until oxygen replaces carbon dioxide
- Expiration: expulsion of carbon dioxide through tract out into atmosphere
- Boyle’s law: inverse relationship between pressure and volume given a constant temperature
- Speech: breathe in, increase volume, decrease pressur of air which is related to how long we can talk. We want to speak on exhalation so we have to increase pressure to expel air
- Respiratory Tract in descending order: nasal and oral cavity, pharynx, larynx, trachea, bronchi, lungs
- Larynx: Divides the airway into upper and low respiratory tracts
- Trachea: 16-20 horse shoe shaped rings (hyaline cartilage); incomplete in the back; lies directly next to the esophagus
- The trachea has these many membranes: three membranes
- Fibrous membrane: outer cover of the t-rings
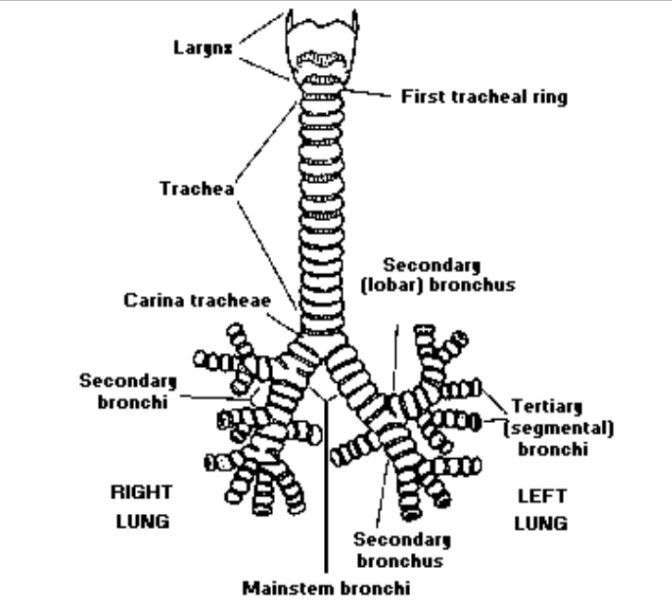
- Trachea artilage: First cartilage attaches to the larynx and the last cartilage bifurcates; separates
- Bifurcates: separates
- Mucous membrane: an (oxford)epithelial tissue which secretes mucus, and lines many body cavities and tubular organs including the gut and respiratory passages.
- Pseudostratified ciliated columnar epithelium
- Cilia: protective
- Mucous: soft tissue that lines the body's canals and organs in the digestive, respiratory and reproductive systems. It's also called the mucous membrane. Mucosa has three layers: epithelium, lamina propria and muscularis mucosae. It plays an important part in immunity. (Cleveland Clinic)
- What is the function of mucous?: ubricates and protects these organs and cavities from abrasive particles and bodily fluids, as well as invasive pathogens. (Cleveland Clinic)
- Where do we have the most mucous producing cells?
- Tracheotomy: Surgical incision 1 cm below the cricoid cartilage (the first tracheal ring)
- Tracheostoma: opening in trachea
- Why is the tracheostoma procedure performed?: It provides an air passage to help you breathe when the usual route for breathing is somehow blocked or reduced. It’s often needed when health problems require long-term use of a machine (ventilator) to help you breathe. (Mayo Clinic)
- Bronchi: Tubes that go from the tracahea to the lungs
- Arborize: become the bronchial tree; bronchioles
- Right bronchi is ____: larger
- The right bronchi is larger than the left bronchi. Why is this clinically significant?: the right lung has three lobes, while the left has only two lobes
- The Lungs: 2 cone shaped structures, spongy and elastic mass
- Lungs are ____ when the vocal folds do something: airtight
- Made of highly elastic material and very little smooth muscles
- Lungs rely on: active muscle/thoracic contractions, lungs themselves are passive
- Lungs themselves are ____: passive
-|-
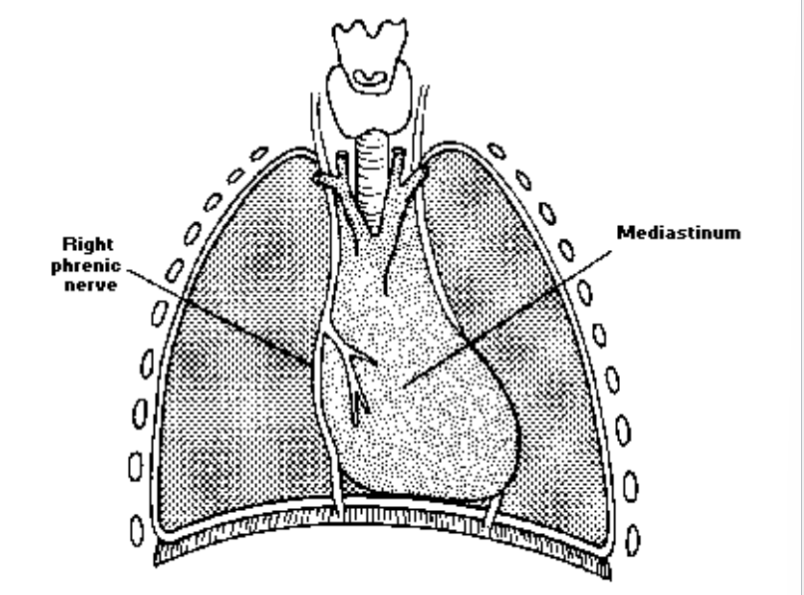
- Right phrenic nerve: Passes lateral to the right brachiocephalic vein and the superior vena cava. Runs anterior to the hilum of the right lung. Passes along the fibrous pericardium of the right atrium and pierces the diaphragm near the inferior vena cava opening. (Ken Hub)
- Mediastinum: a membranous partition between two body cavities or two parts of an organ, especially that between the lungs. (Oxford)
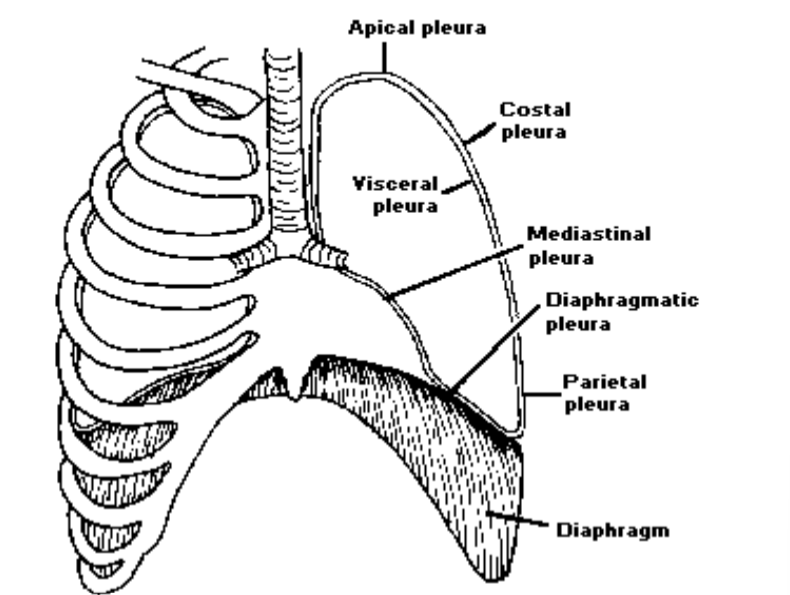
- Pleura: each of a pair of serous membranes lining the thorax and enveloping the lungs in humans and other mammals.
- serous membrane: a mesothelial tissue which lines certain internal cavities of the body, forming a smooth, transparent, two-layered membrane lubricated by a fluid derived from serum. The peritoneum, pericardium, and pleura are serous membranes. (Oxford)
- Visceral pleura: coats lungs
- Parietal (costal) pleura: coats thoracic cavity
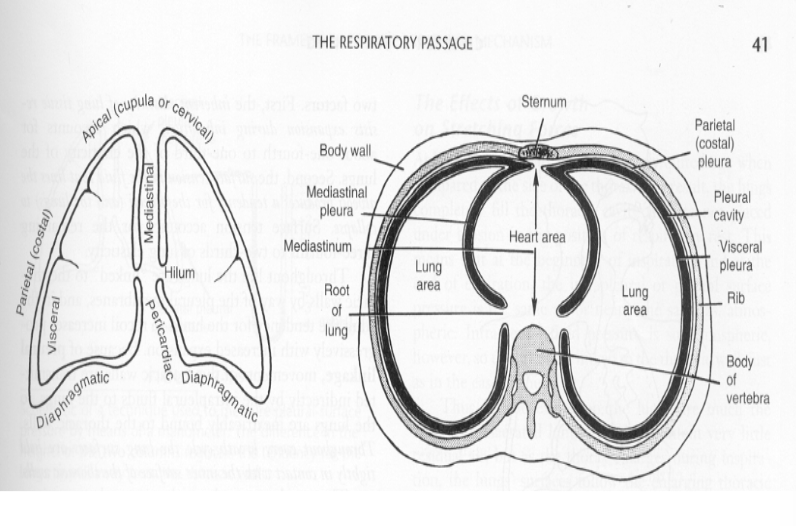
- Interpleura space: lines inner walls of thoracic cavity and lungs (Important in taking in air)
- Apical pleura: thickening in the top portion of the lung. Unilateral pleural thickening means the condition affects either the left or right lung. Bilateral affects both lungs.(mesothelioma center)
- Costal pleura: the pleural portion covering the inner surfaces of the rib cage, and is separated from the ribs/cartilages and intercostal muscles by the endothoracic fascia.
- Visceral pleura: covers the lungs and interlobar fissures
- Mediastinal pleura: The thin membrane that lines the chest cavity in the area between the lungs (NCI Dictionary)
- Diaphragmatic pleura: the portion covering the convex upper surface of the diaphragm. Its junction with the costal pleura at the diaphragmatic margin is a sharp gutter known as the costodiaphragmatic recess, which has diagnostic significance on plain radiography. (Wikipedia)
- Parietal pleura: lines the thoracic wall and superior surface of the diaphragm. It continues around the heart forming the lateral walls of the mediastinum. The pleura extends over the surface of the lungs as the visceral pleura. The surface tension of the fluid in the pleural cavity secures the pleura together. (NCBI)
- Diaphragm: located below the lungs, is the major muscle of respiration. It is a large, dome-shaped muscle that contracts rhythmically and continually, and most of the time, involuntarily. Upon inhalation, the diaphragm contracts and flattens and the chest cavity enlarges. (medline plus)
- Function of pleura: protects and cushions the lungs. This tissue secretes a small amount of fluid that acts as a lubricant, allowing the lungs to move smoothly in the chest cavity while breathing. (NCI)
- Friction free: lungs and thoracic surface
- Pleurisy: pain during inhalation, lack of moist something
- The skeleton: The framework of the body, which consists of bones and cartilage. Has joints or articulations by which the limbs are able to move.
- The right has ____ lung tissue than the left: more
- Smaller in exhalation ____ in inhalation: bigger
- ___ and ___ pleura: costal and parietal
- costal pleura: the pleural portion covering the inner surfaces of the rib cage, and is separated from the ribs/cartilages and intercostal muscles by the endothoracic fascia. (Wikipedia)
- Parietal pleura: lines the thoracic wall and superior surface of the diaphragm. It continues around the heart forming the lateral walls of the mediastinum. The pleura extends over the surface of the lungs as the visceral pleura. The surface tension of the fluid in the pleural cavity secures the pleura together. (NCBI)
-|-
- Ears are ___ to eyes: lateral
- Foot is ___ to knee: distal
- Knee is ___ to foot: proximal
- Superficial (external): located close or on the body surface
- Superficial Ex: The skin is superficial to the muscles
- Deep (internal): Further beneath the body surface.
- Deep Ex: The muscles are deep to the skin
- Coronal (frontal): divides the body into anterior and posterior portions
- Sagittal: divides the body into right and left sides
- Transverse: horizontal cut (divides the body into superior and inferior portions)
- Adduct: close
- Abduct: open
- Supine: laying face up
- Prone: laying face down
- Ventral or ____: anterior
- Dorsal or ____: posterior
- Cranial or ___: superior
- Caudal or ____: inferior
- Coronal plane: facing sideways
- Sagittal plane: frontwards facing
- Proximal: closer to any point of reference
- Proximal Ex: The knee is proximal to the foot
- Distal: Farther from any point of reference
- Distal Ex: The foot is distal to the knee
- Anterior (ventral: in front of the sternum is on the anterior surface of the body
- Posterior (dorsal): in the back of the vertebrae are on the posterior surface of the body
- Superior (cranial): toward the head - high.
- Superior (cranial) example: The eyebrows are cranial to the eye
- Inferior (caudal): away from the head - low.
- Inferior (caudal) example: the mouth is caudal to the nose
-|-
- Respiration Biological function: Exchanging gas in the body
- Respiration speech function: Power supply to stimulate/vibrate the vocal folds
- Respiration: process of exchanging gas in the body-- here red blood cells give up carbon dioxide and take on new oxygen
- Inhalation: air is taken through respiratory tract to lungs and held there until oxygen replaces carbon dioxide
- Expiration: expulsion of carbon dioxide through tract out into atmosphere
- Boyle’s law: inverse relationship between pressure and volume given a constant temperature
- Speech respiration: breathe in, increase volume, decrease pressure of air which is related to how long we can talk. We want to speak on exhalation so we have to increase pressure to expel air
- Respiratory Tract in descending order: nasal and oral cavity, pharynx, larynx, trachea, bronchi, lungs
- Larynx: Divides the airway into upper and low respiratory tracts. Is a valving mechanism with multiple functions
- The larynx divides the _ into _ upper and lower tracts: airway; respiratory
- Right bronchial tube is larger. Clinical significance?: The heart
- Trachea: 16-20 horse shoe shaped rings (hyaline cartilage); incomplete in the back; lies directly next to the esophagus. It has three membranes: fibrous membrane (outer cover of the t-rings), intratracheal fibroelastic membrane (between the rings), mucous membrane (lies inside the rings)
- Fibrous membrane: outer cover of the t-rings
- Intratracheal fibroelastic membrane: between the rings
- Mucous membrane: lies inside the rings
- Mucous membrane is comprised with: epithelial cells and contain cilia
- The three trachea membranes: fibrous, intratracheal fibroelastic membrane, mucous membrane
- Trachea has ____ shaped rings: 16-20 horse shoe shaped hyaline cartilage
- Trachea first cartilage attaches to the: larynx
- Trachea last cartilage ____: bifurcates; separates into the main stem bronchi
- Mucous membrane: pseudostratified ciliated columnar epithelium
- Cilia: Protective. Motion against gravity (bringing dust and mucous up >>throat clear)
- Smoke causes cilia to: not move and elevates mucous secretion
Mucous questions
- ==What is the function of mucous?==
- ==Where do we have the most mucous producing cells?==
- ==Where do we have the most cilia?==
Tracheotomy
- Tracheotomy: Surgical incision 1cm below the cricoid cartilage (the first tracheal ring)
- Cricoid cartilage: first tracheal ring
- Tracheostoma: opening in trachea
- ==Why is this procedure performed?==
Bronchi
- Bronchi: tubes that go from the trachea to the lungs
- Bronchi arborize: become the bronchial tree; bronchioles
- ==Right bronchi is larger - why is this clinically significant?: The left bronchi is smaller because of the heart==
Lungs
- Lungs diagram:
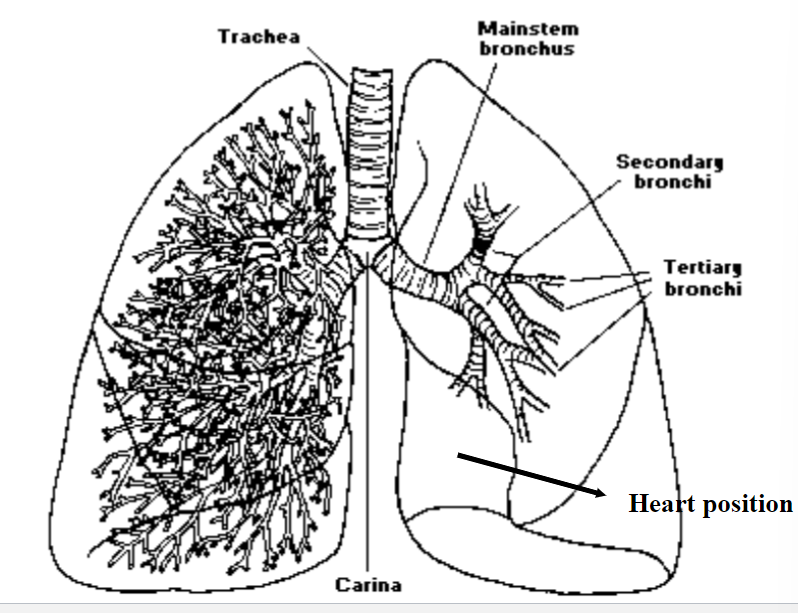
- Lung diagram
Pleura
- Visceral pleura: coats lung
- Parietal (costal) pleura: coats thoracic cavity
- Interpleura space: Lines inner walls of thoracic cavity and lungs (Important in taking in air)
- Pleura diagram:
- Respiratory Passage:
Function of Pleura
- Friction free in relation to pleura: lungs and thoracic surface. Pleurisy-- pain during inhalation, lack of moist gliding surfaces
- Pleurisy: pain during inhalation, lack of moist gliding surfaces
- Protective Pleura: traumatic puncture results in the collapse of only one lung (pnuemothorax)
- If we took the lungs out of the body they would: collapse and the thorax would expand
- The pulling forces between the interlining of the thorax and the outlining of the lungs keeps them: together (intrapleural pressure)
The Skeleton
- The Skeleton: The framework of the body, which consists of bones and cartilage. It has joints, or articulations, by which the limbs are able to move.
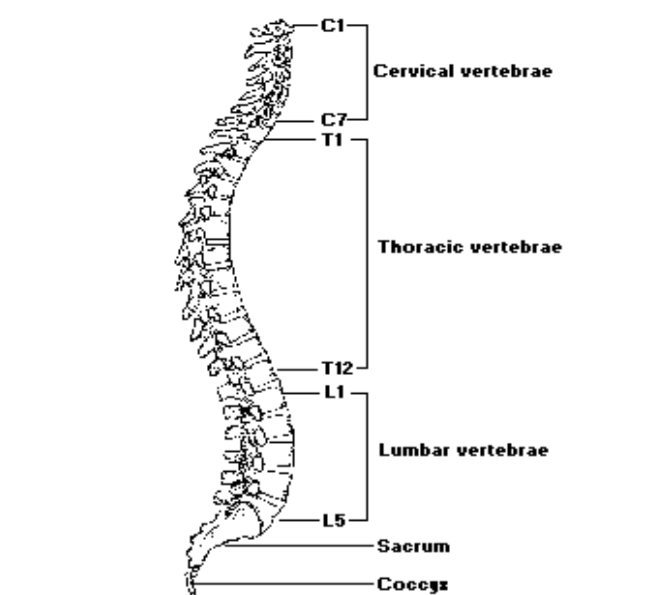
- The vertebral column: The main axis of the skeleton
- In humans, the vertebral column is: made up of 24 short segments of bone (vertebrae) and 2 larger pieces (the sacrum and coccyx)
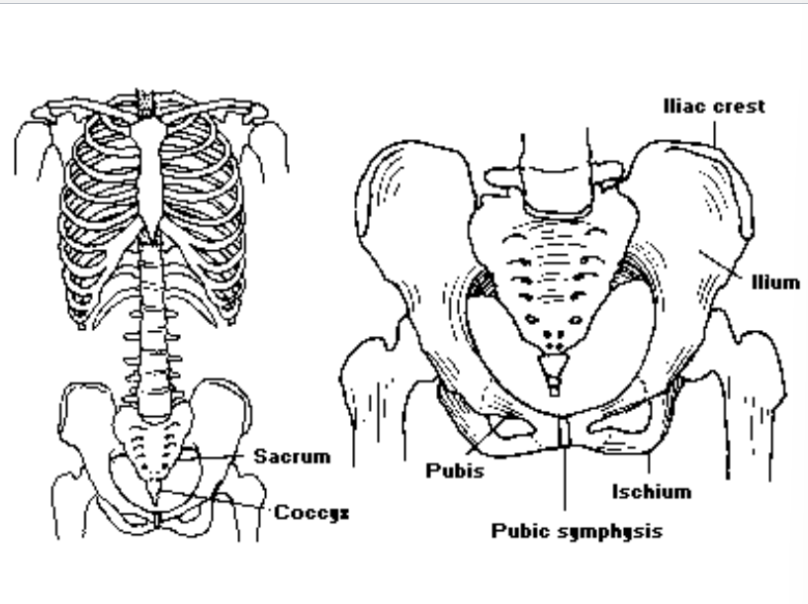
- Sacrum: the 5 lower fused vertebrae
- Coccyx: lies below the sacrum (3-4 vertebrae)
Framework of Respiratory System
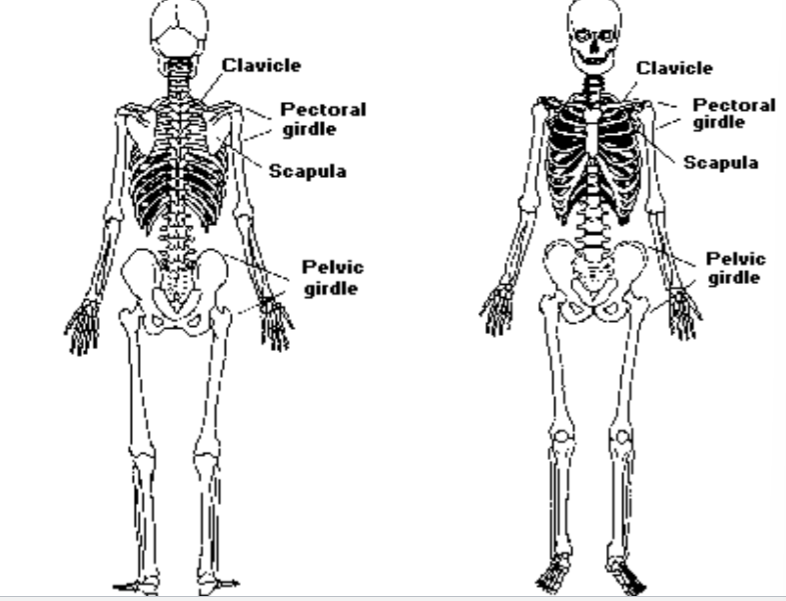
- Framework of Respiratory System: Spinal Column, Pelvic Girdle, Thoracic region, Clavicle, Scapula
- Pelvic Girdle:

- Clavicle front view:
- Clavicle back view:
- Pectoral Girdle front view:

- Pectoral Girdle Back View:
- Scapula (Pectoral Girdle)
- Scapula: Pectoral Girdle
- Framework of Respiratory System Diagram:
The Vertebral Column
- How many vertebrae?: Considering the sacrum as one, we have 26 vertebrae. 5 lumbar, 12 thoracic, 7 cervical (makes up neck)
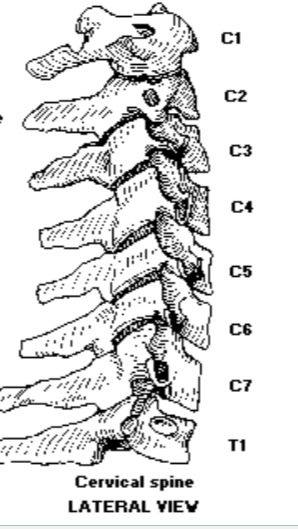
- Cervical vertebrae: makes up neck
- How many lumbar vertebrae?: 5
- How many thoracic vertebrae?: 12
- How many cervical vertebrae?: 7
- ==What does C1 rotate on?==
- ==What is C1?==
- ==What is C2?==
- Vertebral Column diagram:
- The skull rests upon the: 1st vertical vertebrae, which is known as the atlas
- Atlas: The 1st cervical vertebrae that the skull rests upon
- the 2nd cervical vertebrae: Where head rotations occurs; it is known as the axis
- Axis: The 2nd cervical vertebra where head rotations occur
Superior View of Vertebrae:

- Lateral View of Vertebrae:
- Another Vertebrae Diagram:

- ==What is the corpus?==
- ==What is the pelvic girdle?==
- ==What is the coccyx?:==
- ==What is L5?==
- ==What is the public symphysis==
- Upper skeletal diagram:

- Lower skeletal diagram:
- Attachment of upper limbs to torso diagram:

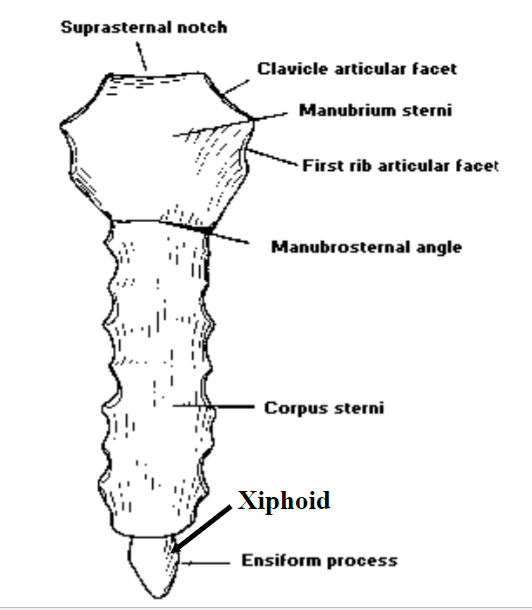
Sternum
- Suprasternal notch: lateral to this structure is the articulatory notch for the clavicle. Below this is the articulation for the 1st rib.
- Sternum Body: contains the articulatory notch for ribs 2-7
- ==Sternum Xiphoid process: What is this landmark?==
- Notch diagram:
Ribs
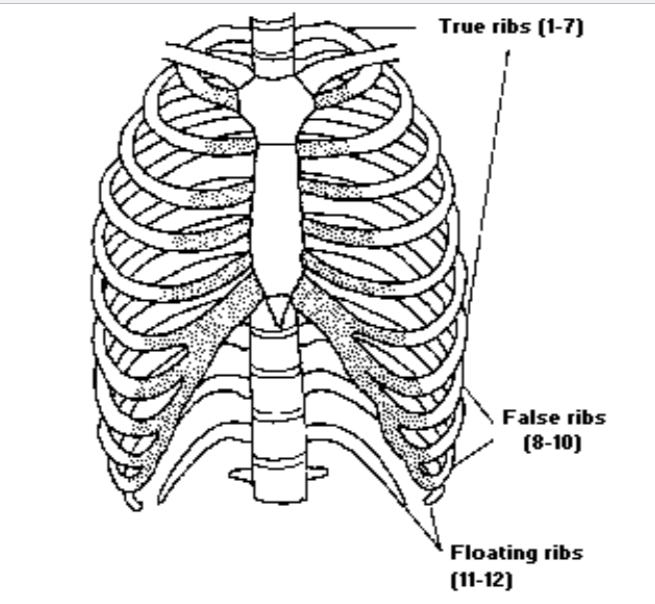
- There are ___ pairs of ribs: 12
- Ribs are ___ attached to the vertebrae: dorsally
- Which ribs are attached ventrally?: 1-7, 8-10, 11-12
- Ribs 1-7: attached to the sternum via hyaline cartilage (ossification with age)
- Ribs 8-10: attached indirectly to the sternum
- Ribs 11-12: not attached at all; embedded in abdominal muscles
- Ribs create: a barrel like shape to the thorax
- Ribs diagram:
The Rib
- The rib is a ___ bone: long curve
- The rib shaft: constitutes the bulk of the rib, and is separated from the head of the rib by the neck
- At the junction of the neck and shaft a ___ articulates with the transverse processes of the vertebra: tubercle
- The Rib diagram:

The Thoracic Cavity
- Larynx: sits on top of trachea and protects it
- Trachea: windpipe-made of cartilage
- Trachea breaks into two major stems: bronchi (which supply each side of the lung)
- Bronchioles: branches of bronchi
- Alveoli: Tiny air sacs found at the tips of bronchioles where we have the gas (air) exchange
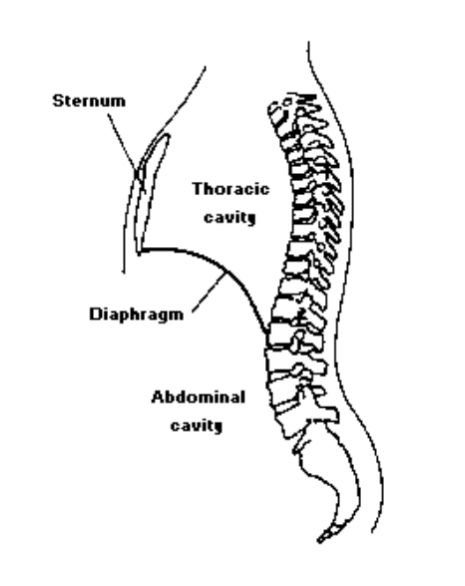
- Diaphragm: makes up floor of thoracic cavity, separates thoracic cavity from abdominal cavity, most important muscle for inspiration
- Lungs: Lie within thoracic cavity which is a protective framework
- First tracheal ring: There are 16-20 of them
- Mainstem bronchi diagram:
- Gas Exchange Diagram:

- Diaphragm Diagram:
Boyle’s Law
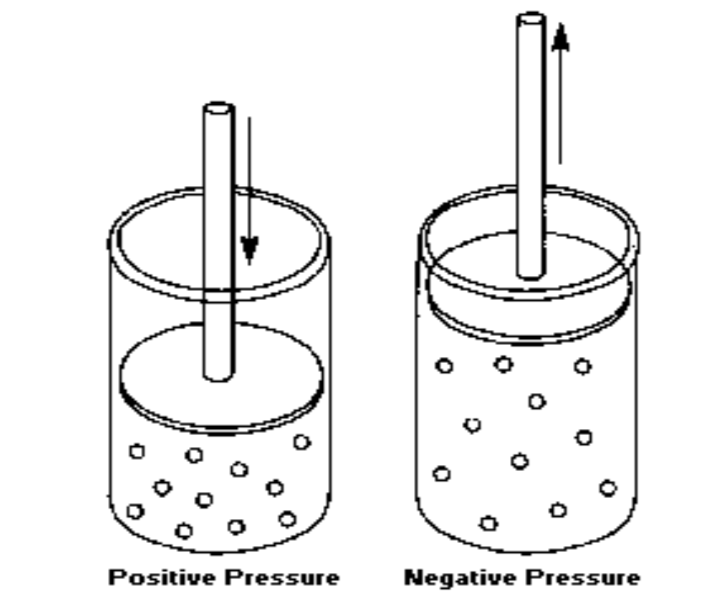
- Basic principles to remember: Air molecules always want to move from areas of high pressure to low pressure. The lungs are elastic- they are always trying to collapse
- Boyle’s Law Diagrams:
- Boyle’s Law Video Overview: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwjN9vi58t78AhWdQjABHf9LDCIQtwJ6BAgLEAI&url=https%3A%2F%2Fwww.youtube.com%2Fwatch%3Fv%3Dv8r_AU_TlPg&usg=AOvVaw0P1xwS_B2P-2A3rMk2bbco
- Inhalation: When the thoracic cavity expands (through active muscle contraction) lung volume increases (air molecules are less compressed -→ negative subglottal pressure -→ air flows into the lungs)
- Exhalation: When the thoracic cavity reduces size, lung volume decreases (air molecules are compressed -→ positive subglottal pressure -→ air flows out of the lungs)
Muscles of Inhalation
- Muscles of Quiet Inspiration: Diaphragm and intercostal muscles
- Diaphgram: lies between thoracic cavity above and abdominal region below. one of most important muscles for inhalation. Dome-shaped; flattens on inspiration. Central Tendon-location for other muscles to attach to the diaphragm.
- Central Tendon: location for other muscles to attach to the diaphragm
- Intercostal muscles: located between the ribs
- Diaphragm Origins: dorsally to the lumbar vertebrae, ventrally to the xiphoid process of the sternum, laterally to the lowest sixth rib
- Diaphragm insertion: central tendon (aponeurosis)
- Diaphragm contracts: lowers/flattens the thoracic cavity, increases lung volume
- What is the primary muscle of inspiration?: Diaphragm
- Inferior View Diagram of the Diaphragm:

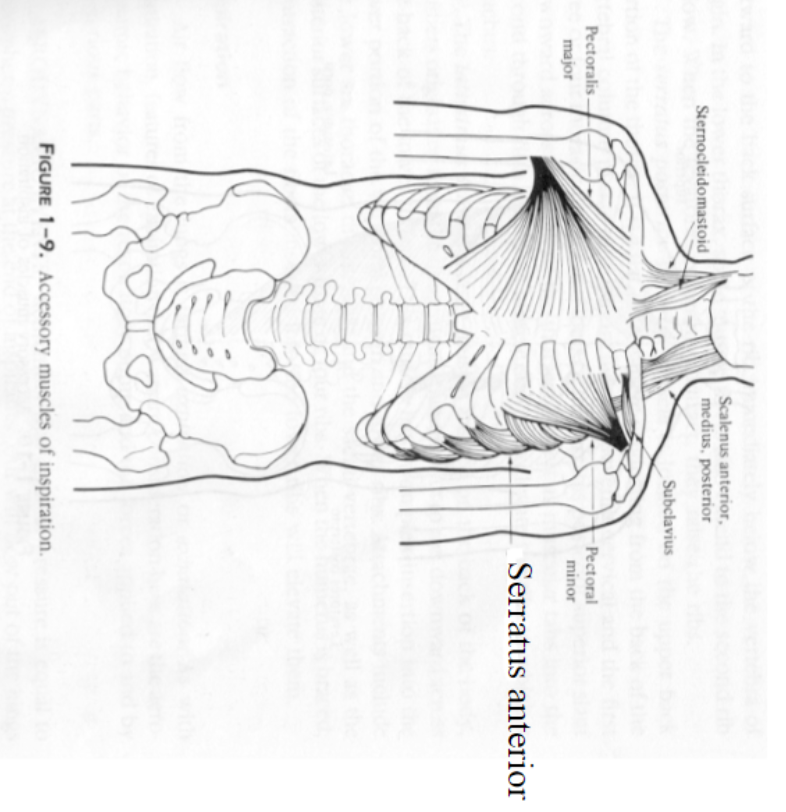
Muscles of Forced Inspiration
- Muscles of Forced Inspiration: Sternocleidomastoid muscle, Scaline Muscle Group, Subclavius, Pectoralis Major, Pectoralis Minor, Serratus Anterior, Costal Levators, Serratus Posterior Superior, Latissimus Dorsi
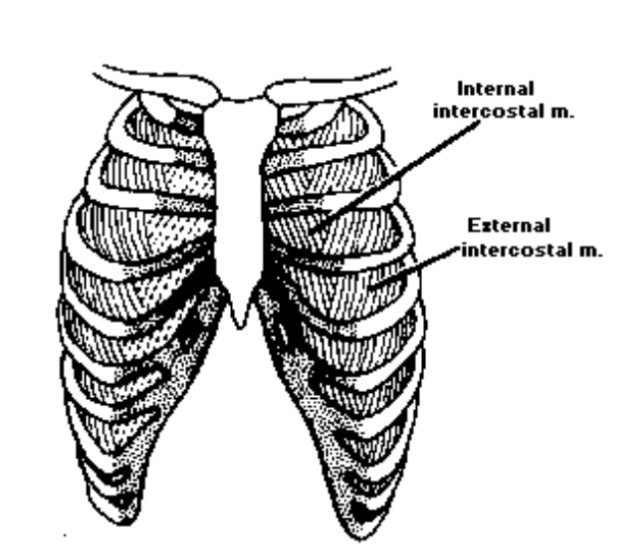
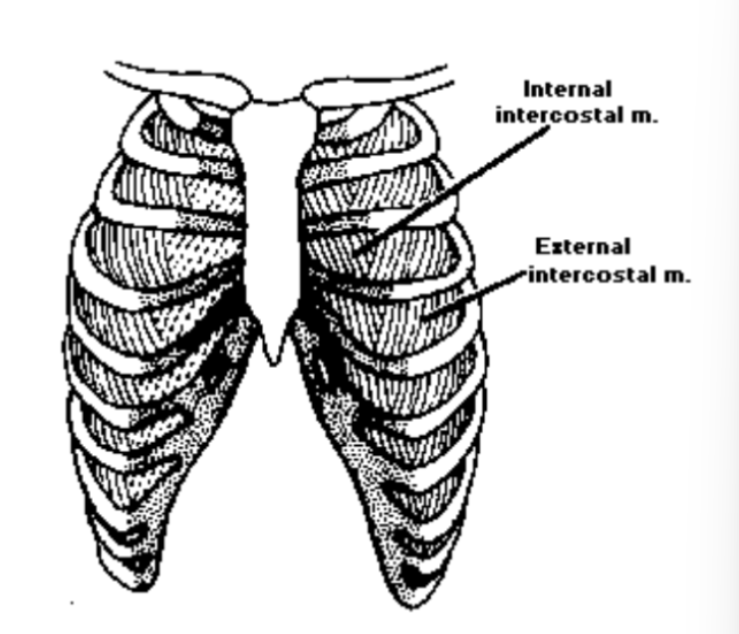
Intercostal muscles
- Intercostal muscles are situated: between the ribs
- External Intercostals: rise from lower margin of one rib, run downward and forward to be inserted at the upper margin of the rib below. When they contract they have an upward pull on the ribs they attach to
- ==Are they a muscle of inspiration or expiration?: Expiration==
- Intercostal Diagram:
Sternocleidomastiod Muscle
- Sternocleidomastiod origin: lateral surface of mastoid
- Sternocleidomastiod Insertion: sternum
- Sternocleidomastiod Contracts: raises the sternum and indirectly the ribs, increase lung volume
Scaline Muscle Group: muscles inserted deep into the neck
\n • Scalinus Anterior: origin c3-c6, insert into 1st \n rib, pulls up on 1st rib.
\n • Scalinus Medius: origin c2-c7, inserts into 1st \n rib, raises1st rib
\n • Scalinus Posterior: origin c2-c3, inserts into 2nd \n rib, raises 2nd rib
\n • Scaline Muscle Group Contraction: lifts the rib cage, increases lung volume
Subclavius
Subclavius: Origin- inferior margin of clavicle; Insertion- superior surface of the first rib; Contracts-lifts the first rib
Subclavius origin: inferior margin of the clavicle
Subclavius insertion: the superior surface of the first rib
Subclavius contraction: lifts the first rib
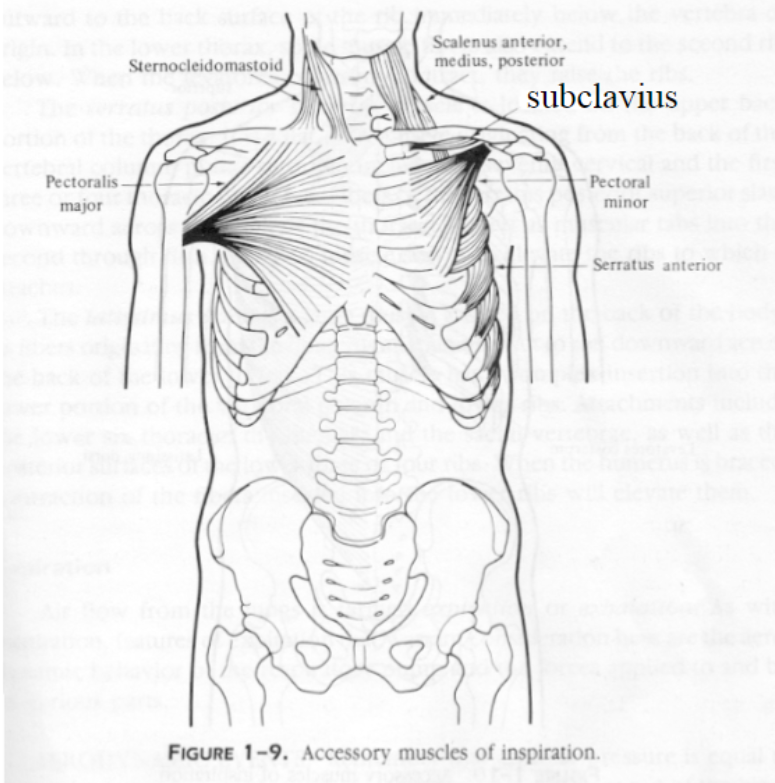
Pectoralis Major
- Pectoralis Major: Largest chest muscle. Fan-shaped on superficial surface of anterior thoracic cavity.
- Pectoralis Major Origin: humerous
- Pectoralis Major Insertion: clavicle, sternum and ribs
- Pectoralis Major Contraction: lifts the rib cage, increases lung volume
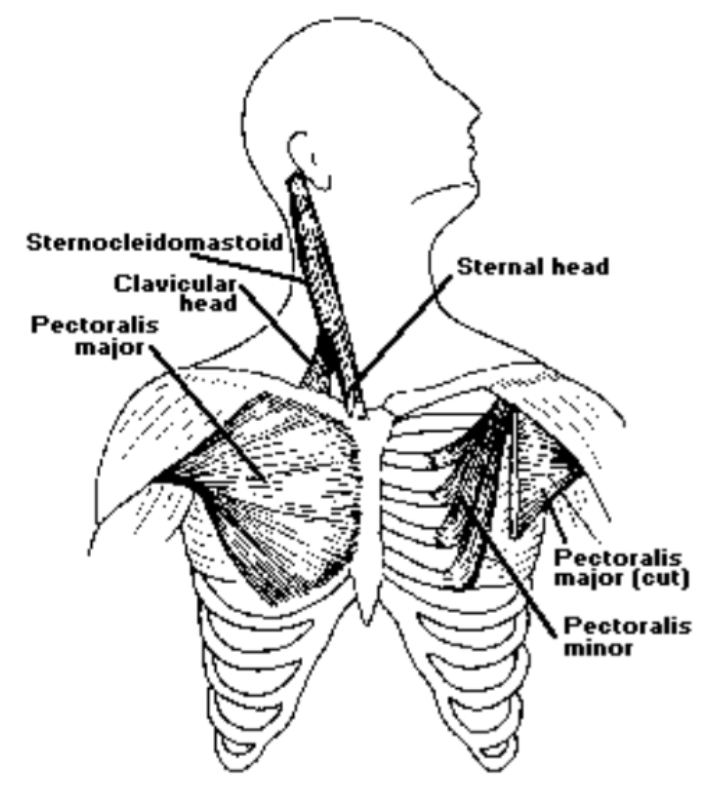
Pectoralis Minor
- Pectoralis Minor: Chest muscle, lies underneath pectoralis major, fan-shaped, paired
- Pectoralis Minor Origin: Scapula
- Pectoralis Minor Insertion: 2nd-5th ribs
- Pectoralis Minor Contraction: lifts the rib cage, increases lung volume
Serratus Anterior
- Serratus Anterior origin: outer surfaces and superior borders of the upper 9 ribs
- Serratus Anterior Insertion: fibers curve sideward and backward to insert into the vertebral border of the scapula
- Serratus Anterior Contraction: -lifts the rib cage, increases lung volume
Costal Levators
- Costal Levators help: elevate ribs during inhalation
- Costal Levators Origin: the transverse process of 7th or lowest cervical vertebrae and upper eleventh thoracic vertebrae
- Costal Levators Insertion: downward and laterally inserting into the ribs a short distance from the vertebral column
- Costal Levators Contraction: lifts the rib cage, increases lung volume
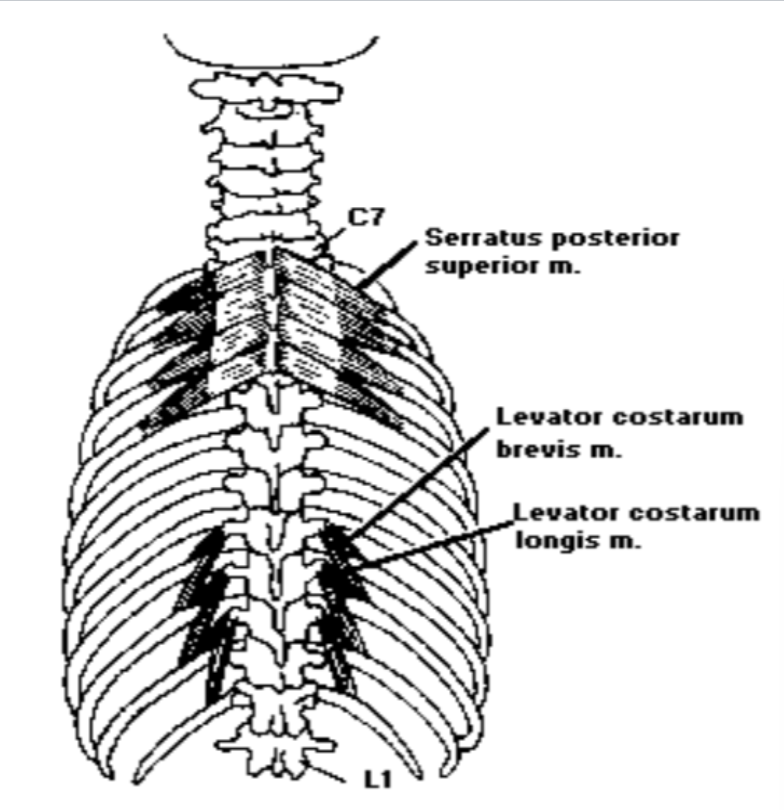
Serratus Posterior Superior
- Serratus Posterior Superior Origin: spinous process of the last two cervical vertebrae and the first two thoracic vertebrae
- Serratus Posterior Superior Insertion: 2nd and 5th ribs
- Serratus Posterior Superior Contraction: raises those ribs, thus increasing lung volume
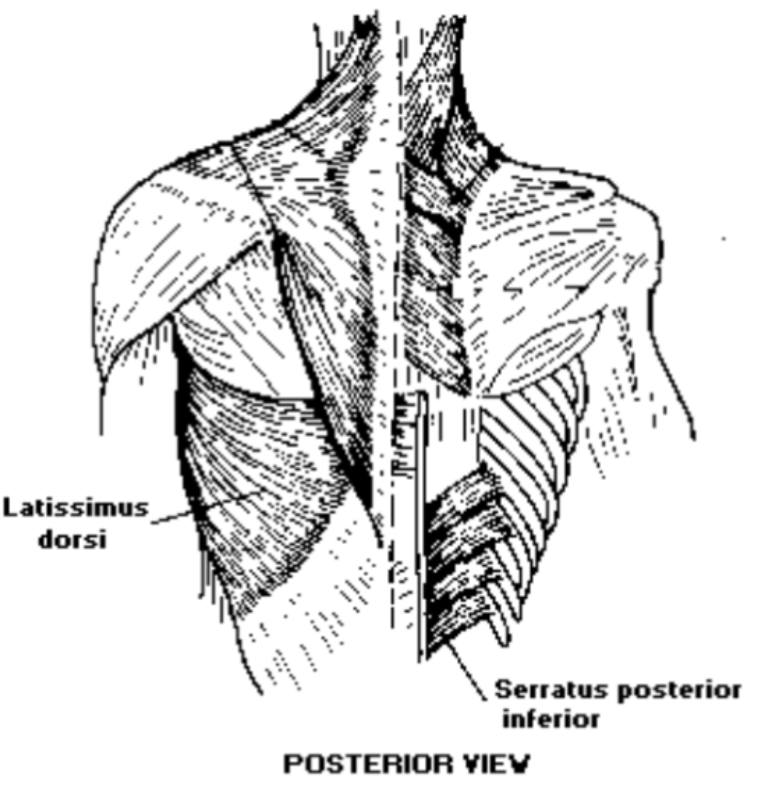
Latissimus Dorsi
- Latissimus Dorsi: superficial muscle covering lower half of back
- Latissimus Dorsi Origin: t6-t11, lumbar, sacral regions of vertebrae, and pelvis
- Latissimus Dosi Insertion: converges lateral and upward to insert into ribs, attaches into humorous bone
- Latissimus Dorsi Contraction: Can elevate and depress ribs
- Muscles of Inspiration: They help increase lung volume
Muscles of expiration:
- Muscles of expiration are responsible for: decreasing the dimensions of the thoracic cavity
- Abdominal muscles of expiration: can push up on diaphragm thus reducing vertical dimension of thorax
- Thoracic muscles of expiration: act upon the ribs, essentially depressing them to reduce thoracic dimensions
Muscles of Quiet Expiration
- Passive expiration is accomplished by: nonmuscular forces (recoil forces)
- Potential (stored) energy in the muscles of quiet expiration: resulting from stretched inspiratory muscles is released
- Think of the recoil of a: stretched spring
Abdominal Aponeurosis
- Abdominal aponeurosis: broad flat tendonous tissue in the ventral abdominal wall extending from the sternum to the pubis
- Abdominal aponeurosis: serves for muscle attachment of abdominal muscles
- A prominent strand of the aponeurosis inferiorly running from the pubic symphysis to the anterioriliac spine is the: inguinal or Pupart’s ligament
(161)
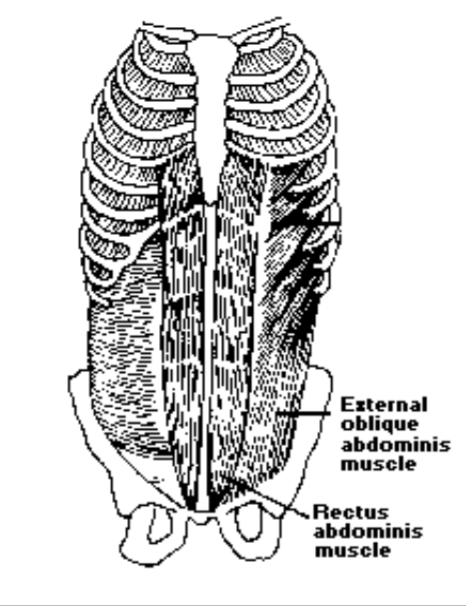
External Oblique
- External Oblique: one of the outermost abdominal muscles, extending from the lower half of the ribs around and down to the pelvis
- External Oblique is the most ____ of the abdominal muscles: strongest and most superficial
- External Oblique Origin: exterior surfaces and lower borders of ribs 5-12
- External Oblique Insertion: anterior half of the iliac crest, or abdominal aponeurosis
- External Oblique Function: pulls down the rib cage, lowers lung volume
Internal Oblique
Internal Oblique: muscle found on the lateral side of the abdomen. It is broad and thin. it forms one of the layers of the lateral abdominal wall along with external oblique on the outer side and transverse abdominis on the inner side.
Internal Oblique Origin: exterior surface and lower border of ribs 5-12
Internal Oblique Insertion: ribs 10-12 and abdominal aponeurosis
Internal Oblique Function: pulls down the rib cage, decreases lung volume
Transverse Abdominal Muscle
What is the transverse abdominal muscle?: Deepest abdominal muscles lying beneath the external and internal oblique muscles
Transverse Abdominal Muscle Origin: inner surfaces of the lower 7 ribs, from the lumbar fascia, iliac crest, and from lingual ligament
Transverse Abdominal Muscle Insertion: most fibers run horizontally into the abdominal aponeurosis
Transverse Abdominal Muscle Function: pulls down the rib cage, increases lung volume
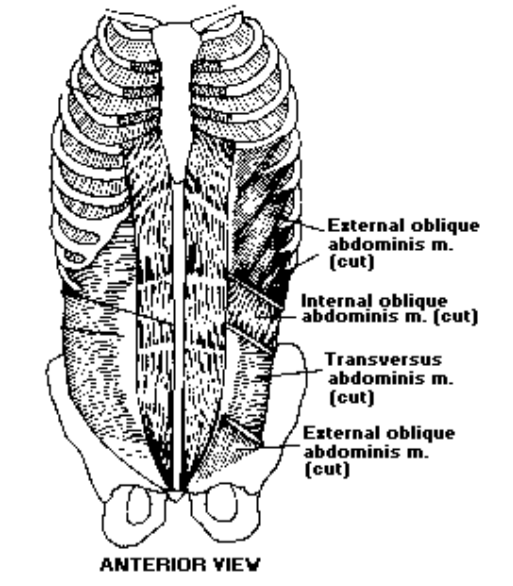
- Transverse Abdominal Muscle: located in the abdomen immediately inside of the internal oblique muscle. It is one of the innermost muscles of the abdomen and it arises from the inguinal ligament, iliac crest, the inner surfaces of the lower six ribs and the thoracolumbar fascia.
Serratus Posterior Interior
What is the serratus posterior inferior?: lies on the dorsal wall of the thoracic wall
Serratus Posterior Inferior origin: spinous processes of the 3 lowest thoracic vertebrae and 2 of the upper lumbar vertebrae
Serratus Posterior Inferior Insertion: fibers run upward and laterally to insert along inferior borders of the four lowest ribs
Serratus Posterior Inferior Function: probably draws lowest four ribs downward aiding in forced exhalation, increases lung volume
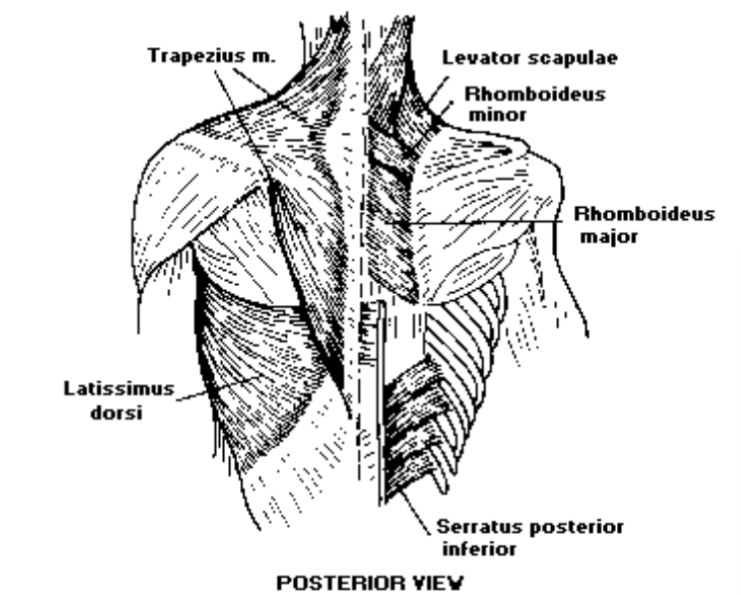
- Serratur Posterior Inferior: originates from the spinous processes of the T11 to T12 thoracic vertebrae and has its insertion on the four lower ribs. Both muscles are known to be among the secondary back muscles, meaning that they migrated to the back in the course of embryogenesis.
Quadratus Lumborum
What is the Quadratus Lumborum?: Flat sheets of muscle located in the lateral dorsal aspect of the abdominal wall
Quadratus Lumborum Origin: iliac crest and fibers run vertically upward and converge
Quadratus Lumborum Function: contraction of this muscle as a whole compresses the lower portion of thoracic cage
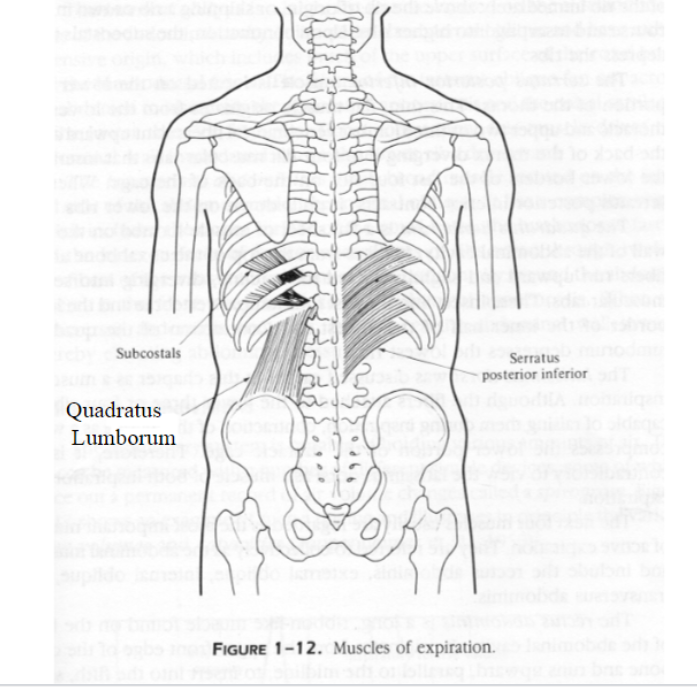
- Quadratus Lumborum: the deepest back muscle and originates from the iliac crest and inserts on the transverse process of lumbar one through five and the lower part of the twelfth rib. The QL muscle is flattened and has a quadrangular shape
Internal Intercostals
- Internal Intercostals are located here: lies deep to the external intercostals between ribs
- Internal Intercostals origin: lower borders of the upper 7 ribs
- Internal Intercostals Insertion: inner space of the ribs
- Internal Intercostals Function: controversial as to their action either inhalator or exhalatory
- Latest research shows this about Internal Intercostals: they reduce thoracic cavity for forced exhalation
- Internal Intercostals: pull down on the rib cage and push air out of the lungs. The internal intercostals are the most important respiratory muscles for normal speech and singing, for they are the muscles that propel air out through the mouth and nose
Breathing
- Passive/Quiet: inhalation is active because muscles are contracting and exhalation is passive (gravitational + elastic forces)
- Active Breathing: in speech, controlled and prolonged expiration with rapid inspiration
- Forced Breathing: forcing air out of the lungs by contracting abdominal muscles, forced exhalation
Vegetative/tidal/passive/quiet breathing
- Quiet inspiration: inspiratory muscles (namely the diaphragm and external intercostals) upon contraction expand the thoracic cavity
- Vegetative/tidal/passive/quiet breathing is a ___ function: physiological
- In vegetative/tidal/passive/quiet breathing air moves from: regions of higher pressure to regions of lower pressure
- When lung volume is increased, intrathoracic air pressure is ____: decreased (less than the atmospheric pressure)
- Air flows into the lungs until: air pressure within the lungs is equal to atmospheric pressure
- Quiet expiration: begins when gravity and elastic forces act upon the ribcage, decrease lung volume, increase intrathoracic pressure (more than the atmospheric pressure)
- Air flows out of the lungs until: air pressure within lungs is equal to atmospheric pressure
Forced Breathing
Forced inspiration: accessory inspiratory muscles are recruited to help the diaphragm and the external intercostals increase the lung volume
When lung volume is increased, intrathoracic air pressure is: more decreased (much less than the atmospheric pressure)
Forced expiration: All expiratory/abdominal muscles contract pushing against the diaphragm, which is raised
When lung volume is decreased, intrathoracic pressure is: increased (much more than the atmospheric pressure)
When we relax, the diaphragm returns to its natural position (down)
The breathing cycle is repeated: increase in lung volume----air flows into the lungs
Lung Volumes
- Resting lung volume: the amount of air in the lungs at rest position
- Tidal volume: the amount of air that one can inhale and exhale during passive breathing (20%)
- Inspiratory capacity: the amount of air that one can inhale from the reset position
- Expiratory capacity: the amount of air one can exhale from the rest position
- Total lung volume: the amount of air in the lungs after a maximum inhalation (100%)
- Vital capacity: the amount of air one can maximally exhale after a maximal inhalation (80%)
- ==Note the difference between total and vital capacity- what is residual volume?==
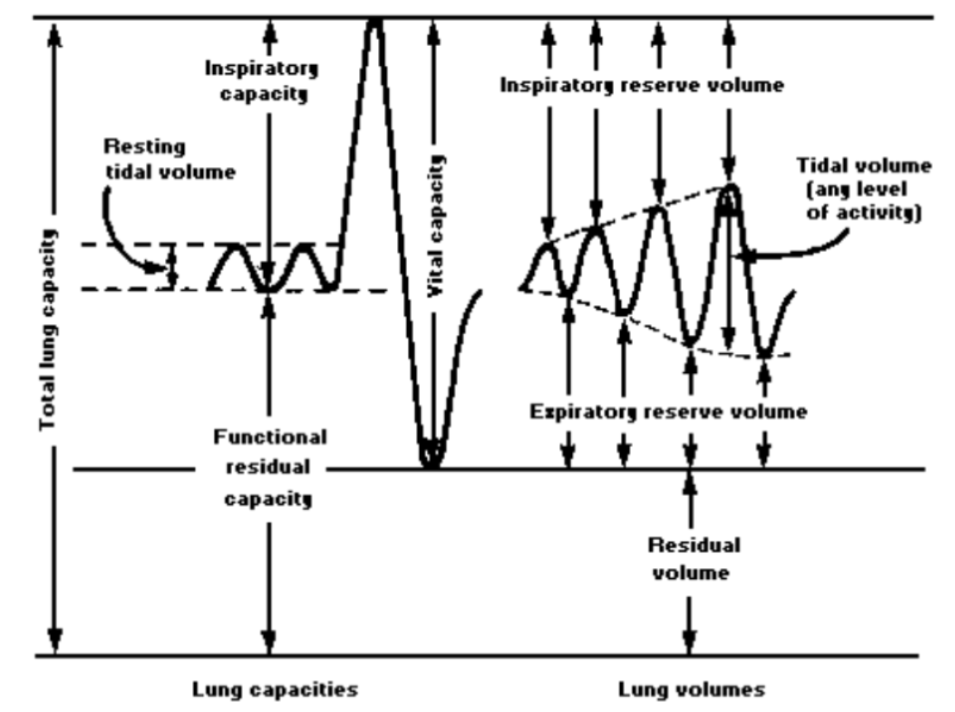
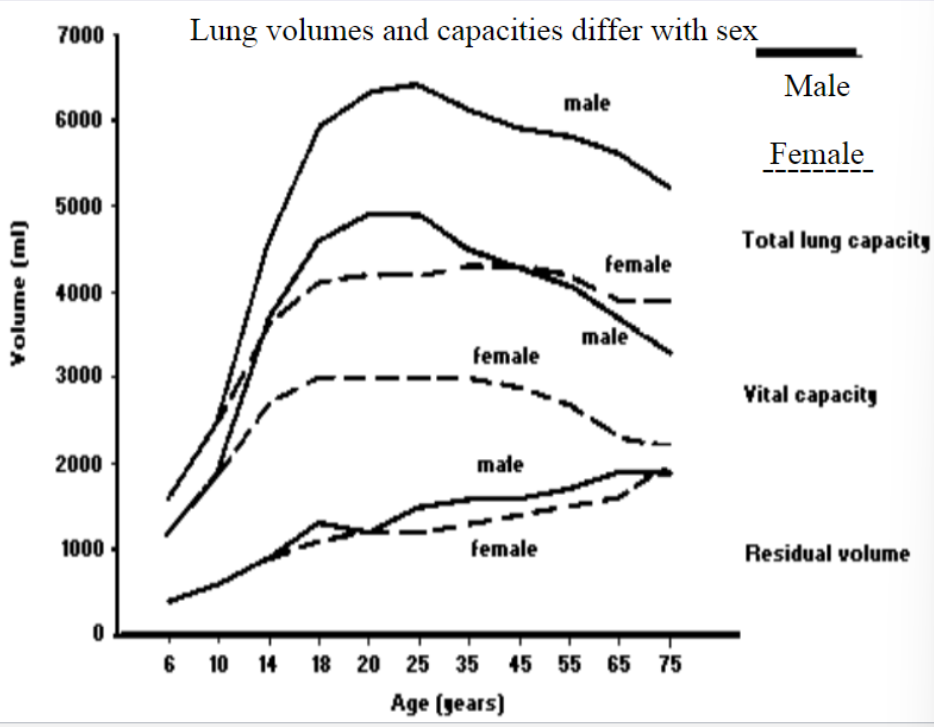
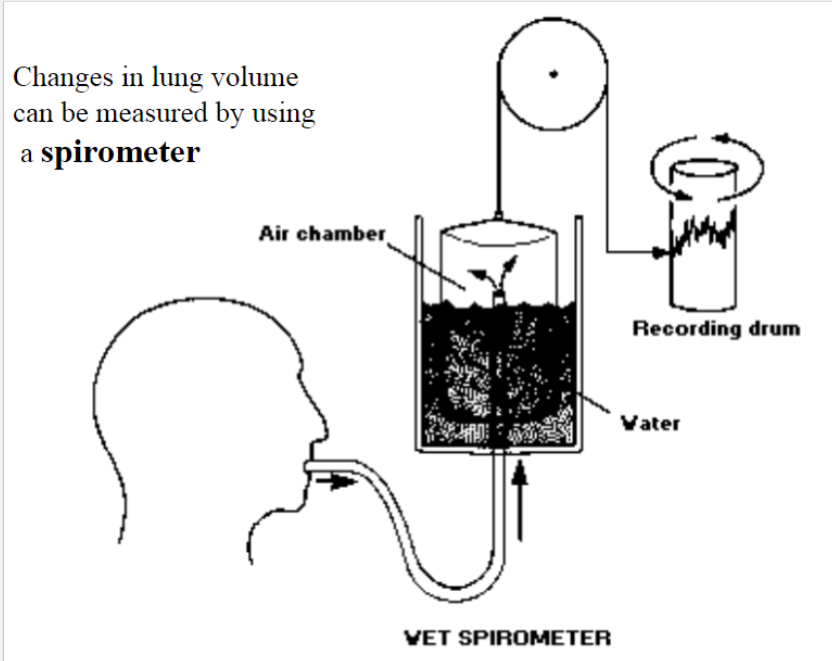
- Changes in lung volume can be measured by using: a spirometer
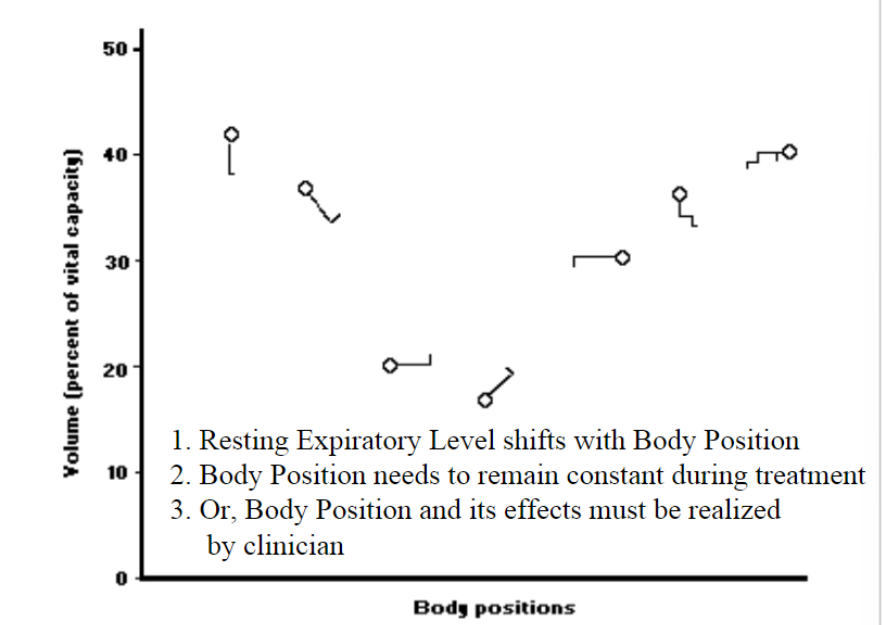
Vital Capacity and Body Position
- Extremely important for treatment purposes: the position that your place your patient in when you are working with breathing, phonation, or speech
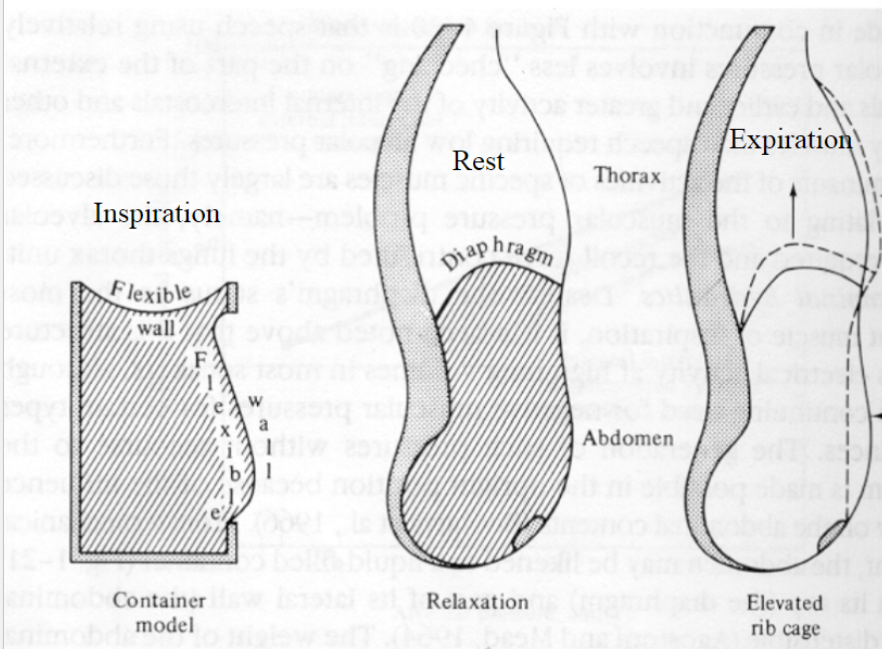
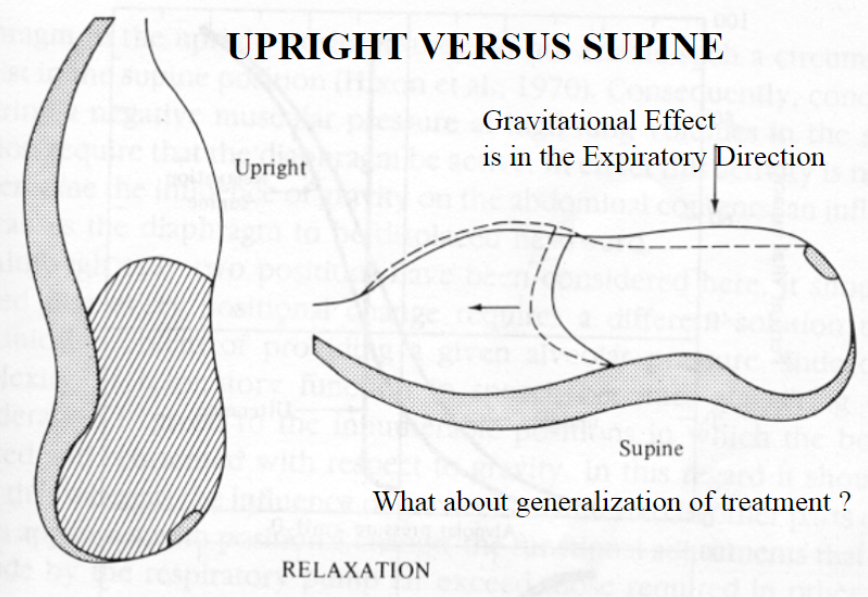
A Functional Unit Concept
Lung and thorax typically operate as: a unit via pleural linkage
Resting position in contact unit is different: when the two are separated
Separated at rest: lung = collapsed, thorax = more expanded state
Lungs: collapsed
Thorax: more expanded state
Pleural linkage at rest: lungs = somewhat expanded, thorax = somewhat compressed
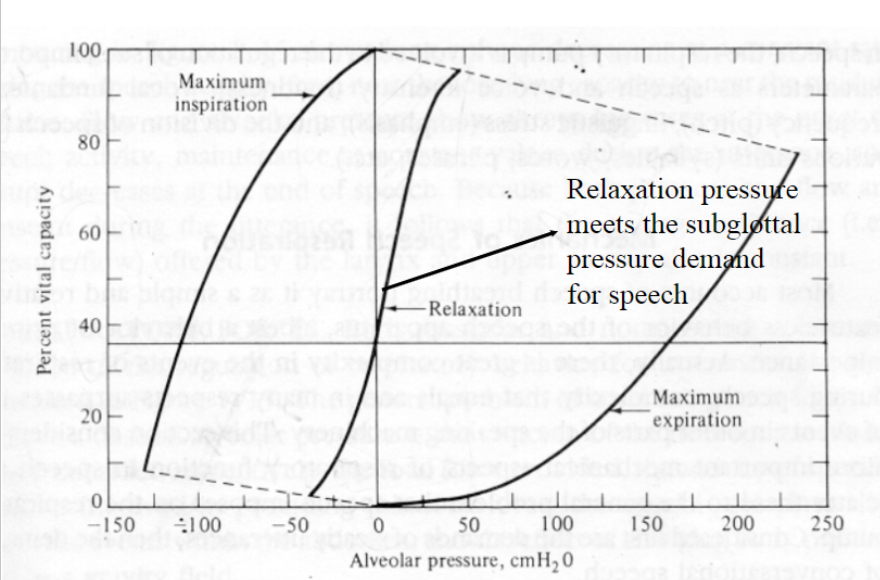
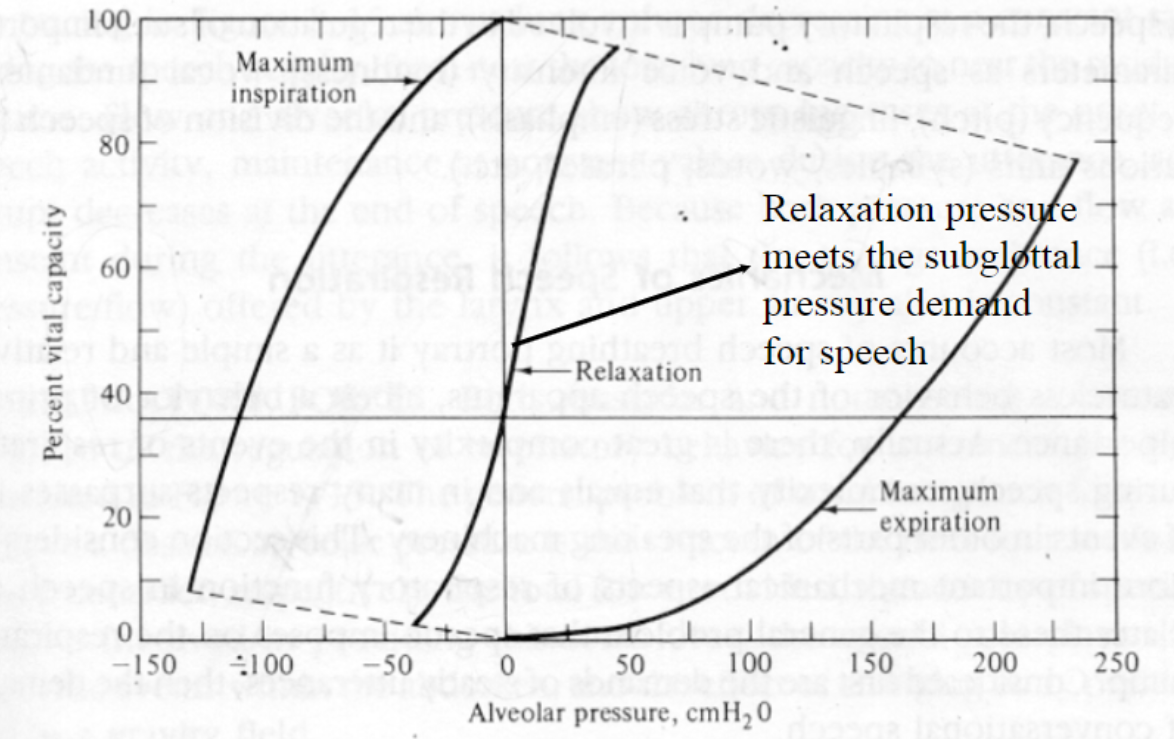
Relaxation Pressure
- Respiratory maneuver
- The pressure produced entirely by nonmuscular forces of the respiratory apparatus
- Relationship between subglottic pressure and lung volume is determined when all respiratory muscles are relaxed
- Determined for inspiratory and expiratory pressure
- Relaxation pressure varies according varies according to the quantity of air in lungs
- Departure from the relaxation pressure can be achieved through the use of muscular effort (net inspiratory or net expiratory muscle effort)
Relaxation Pressure Diagram
- in the relaxation pressure diagram, the amounts of air within the lungs are expressed as a: percentage of vital capacity (horizontal axis)
- Points to the right of zero atmospheric pressure represent pressures greater than the atmospheric pressure, those to the left of zero are subatmospheric in the: relaxation pressure diagram
- Three curves in the Relaxation Pressure Diagram: relaxation/ maximum expiration/ maximum inspiration
• Respiratory maneuver \n • Respiratory manuveur: The pressure produced entirely by \n nonmuscular forces of the respiratory \n apparatus \n • Respiratory Manuveur Relationship: relationship between subglottic pressure \n and lung volume is determined when all \n respiratory muscles are relaxed \n • Determined for inspiratory and expiratory \n pressure
Relaxation Pressure
• Relaxation pressure varies according to the \n quantity of air in the lungs \n • Departure from the relaxation pressure can \n be achieved through the use of muscular \n effort (net inspiratory or net expiratory \n muscle effort)
Relaxation Pressure \n • Respiratory maneuver \n • The pressure produced entirely by \n nonmuscular forces of the respiratory \n apparatus \n • Relationship between subglottic pressure \n and lung volume is determined when all \n respiratory muscles are relaxed \n • Determined for inspiratory and expiratory \n pressure
Relaxation Pressure• Relaxation pressure varies according to the \n quantity of air in the lungs \n • Departure from the relaxation pressure can \n be achieved through the use of muscular \n effort (net inspiratory or net expiratory \n muscle effort)
Relaxation Pressure Diagram \n • The amounts of air within the lungs are expressed \n as a percentage of vital capacity (horizontal axis) \n • Points to the right of zero atmospheric pressure \n represent pressures greater than the atmospheric \n pressure, those to the left of zero are \n subatmospheric \n • Three curves: relaxation/ maximum expiration/ \n maximum inspiration
Exhalation \n • Passive exhalation: above the resting lung \n volume (the amount of air in the lungs at \n rest position) is achieved through elastic \n /recoil forces and gravity
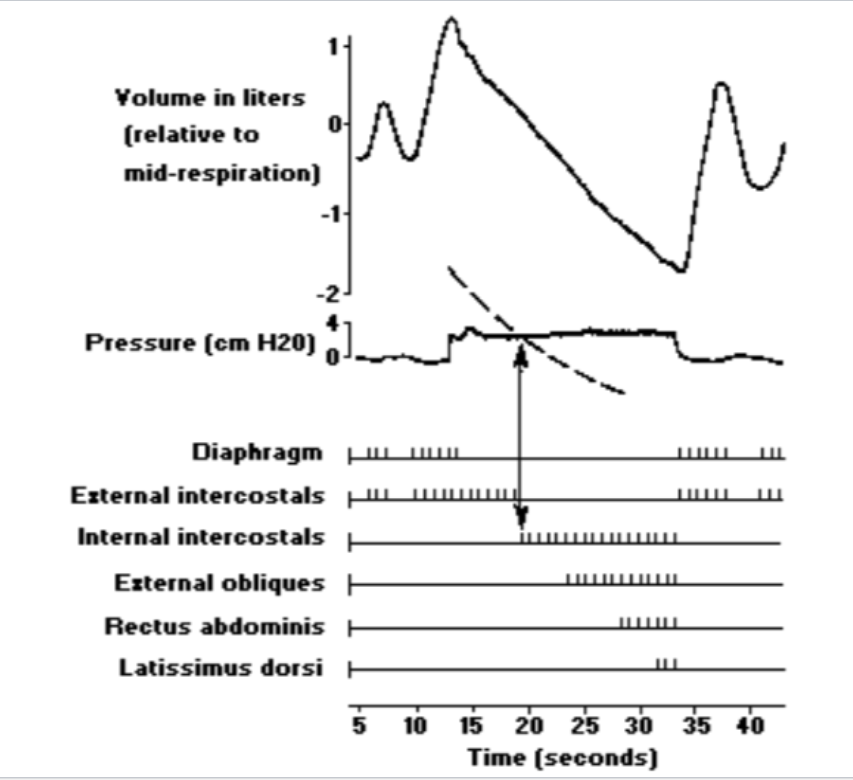
Active expiration: below the resting lung \n volume, achieved through active muscle force \n \n rectus abdominis \n external obliques \n internal obliques \n transverse abdominis \n serratus posterior \n internal intercostals \n quadratus lumborum
• Upon these muscles contraction-- decrease \n in the thoracic cavity, decrease in the lung \n volume, increase in air pressure, the air \n flows out of the Lungs \n Exhalation>>>Phonation
Expiratory Airflow \n • Maintained with precise control of the \n expiratory muscles to meet the requirements \n of phonation (VF) and articulation \n (Articulators) \n • External intercostals:( major inspiratory \n muscle) still contracting for active \n exhalation, to control exhalation (airflow \n brakes) in order to maintain just the \n necessary pressures for speech
• Internal intercostals : contracting to \n achieve exhalation, to provide \n exhalation \n • Respiration is work: generating \n pressure requires muscular activity and \n restraining that pressure for speech \n requires even more work
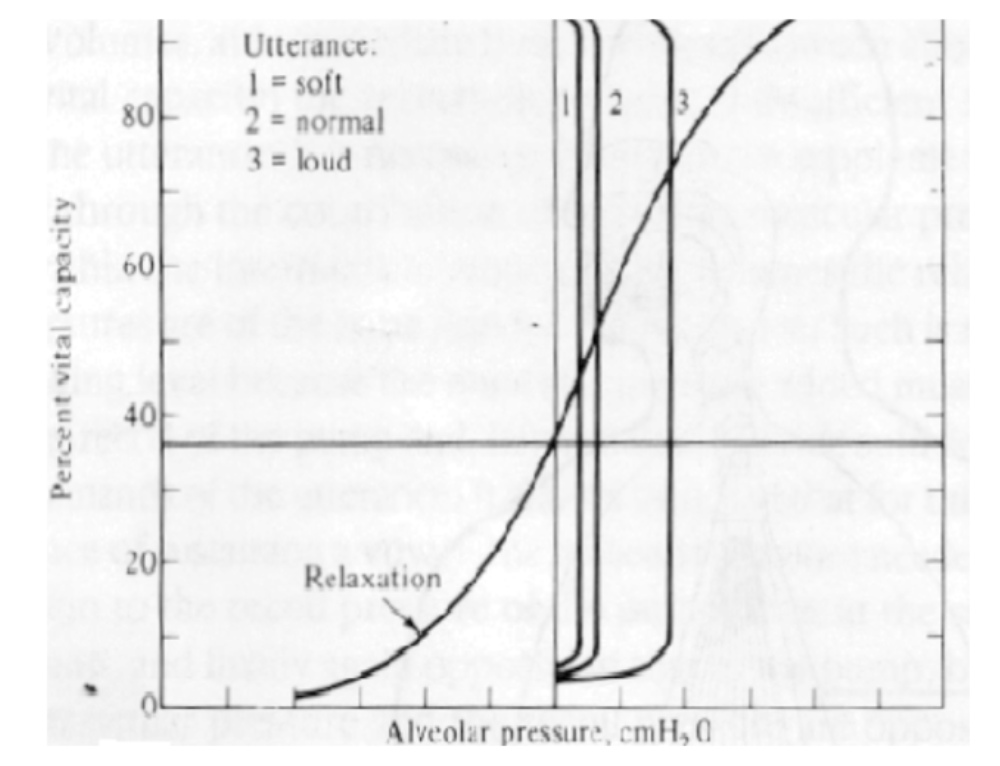
Speech/Active Breathing \n • Respiratory cycle does not begin from \n vegetative breath ( you need more volume \n that will grant you more recoil>>less work ) \n -Exhalation is active \n -Most speech occurs during exhalation \n -35-70% of vital capacity is used as power \n source of the speech mechanism
• Continuous airflow to maintain the FV vibration
- intrathoracic/subglottal air pressure has to be developed and maintained 5-20 cm H2O
- Prolonged and controlled exhalations
- Rapid inspiration
• Abdominal muscles upon contraction push against the diaphragm
- Controlling the airflow
- Vocal folds serve as resistance to increase subglottal pressure
Function of the Respiratory System in Speech
- Provide a power source: subglottal pressures build up, vocal folds act as resistance
- Increase loudness of voice: subglottal pressure and loudness are directly related-- the higher the pressure, the bigger the amplitude of VF vibration
3) Utterance/ speech duration : related with \n the rate of airflow, determined by firing of \n the muscle fibers (6-8 phonemes / sec) \n The respiratory System is always adapting \n to the speech tasks
Conditions that affect the \n respiratory system \n • Asthma \n • Chronic obstructive pulmonary disease \n • Emphysema \n • Vocal fold paralysis/paresis
Breathing
- Passive/Quiet Breathing: inhalation is active because muscles are contracting and exhalation is passive (gravitational + elastic forces)
- Active Breathing: in speech, controlled and prolonged expiration with rapid inspiration
- Forced Breathing: forcing air out of the lungs by contracting abdominal muscles, forced exhalation
Mechanisms of Breathing
- Mechanisms of breathing: vegetative/tidal/passive/quiet breathing
- Mechanisms of breathing are a ___ function: physiological
- Air moves from regions of higher pressure to regions of: lower pressure
- Lung volume is increased, intrathoracic air pressure is decreased (less than the atmospheric pressure)