AP Psychology Midyear Review
Unit 0: Research Methods
Experimentation (IV, DV, Control Group, Experimental Group, Confounding Variables, Operational Definitions)
Experimentation: attempting to establish a cause and effect relationship between the independent variable (the variable being manipulated) and the dependent variable (the variable that is affected by such manipulation)
Hypothesis: prediction of the effect of the independent variable on the dependent variable
Null hypothesis: predicts that the independent variable will have no effect on the dependent variable, which can only be rejected using data from the experiment that suggests otherwise
Confounding variables: factors the experimenter did not control for that may have affected the results
Operational definition: a clear, concise, detailed definition of a measure that we need so that we know exactly what researchers are talking about when they refer to a variable (eg measuring intelligence through SAT scores)
Replication: other researchers repeat an experiment to confirm its conclusions; the more times the experiment yields the same results, the more reliable it is said to be
Placebo group: participants are led to believe they are receiving the drug (independent variable), but they are not, which helps to determine whether the drug itself is having an effect or whether belief in the drug is having the effect
Single-blind study: participants do not know which group they belong to
Double-blind study: neither the participants or the experimenters know which group the participants belong to
Eliminates possible confirmation bias, when an experimenter looks for information to support their hypothesis
We must use random selection/sampling to get a representative sample, a subset of a population that accurately reflects the characteristics of the entire population (choosing people to participate in experiment)
Random Assignment: each subject has an equal chance of being assigned to the control or experimental group (choosing people to be in each group)
Population: all individuals who share a particular characteristic and can be considered as part of the larger group from which samples are drawn
Correlational Research (Positive and Negative Correlation)
Positive correlation: variables move in same direction; (direct relationship)
Negative correlation: variables move in opposite direction (eg temp goes, up, amount of clothing worn goes down)
Correlation coefficient: measure of the strength of the relationship between two variables
+/- 1.00 is a perfect correlation; +/- 0.5 is considered a strong correlation (does not have anything to do with +/-, but rather the value of the #); eg r=1 is a perfect + correlation, r=-1 is a perfect negative correlation, ±0.3 is a low correlation
Third variable: you cannot infer causation from correlation between two variables due to variables that affect both the dependent and independent variable (confounding variable)
Descriptive Research: Naturalistic Observation, Case Study, Survey, Longitudinal and Cross-Sectional Studies
Survey: collecting self-reported data from study participants
Advantages: usually cost-effective, fast results, large population=greater statistical power
Disadvantages:
Framing: the way you ask a question can significantly influence the responses you receive
Demand characteristic: when participants change their behavior or responses based on what they believe the research is about in an attempt to align with what the researchers are expecting
Self-report bias: when people do not accurately report or remember their behaviors
Social desirability bias: the tendency of people to answer questions in a manner that will be viewed favorably by others
Non-response bias: some people don’t respond to surveys or to particular items within a survey, even though their responses might well be useful or representative
Naturalistic observation: observing and recording behavior in naturally occurring situations w/out interference or interaction with the participants
Two key elements:
A clear, measurable operational definition of what you’re observing
Remaining unobtrusive
Case study: examining in depth an event that has already occurred with the hope that the case might reveal universal principles; an in-depth study of one person, group, or event
Advantages: gives new insight that might be applied to other situations, very in-depth analysis, less general than other research methods
Disadvantages: single case may not be generalizable to the larger population
Longitudinal study: studying the same group of people over a long period of time; involves repeated observations of the same variables (e.g., people) over long periods of time
Advantages: identify changes over time + provide insight into cause-and-effect relationships that other research methods do not allow for
Disadvantages: very expensive and time-consuming, require long-term commitment, and many participants may choose to no longer participate after a long period of time
Cross-sectional study: studying representative samples of different age groups at a single point in time
Advantages: usually inexpensive and easy to conduct, useful for establishing preliminary evidence in planning a future advanced study, able to determine similarities in a certain variable across different groups
Disadvantages: cannot establish a cause-and-effect relationship or analyze behavior over a period of time + cohort effect (the variation of characteristics over time, among groups of people marked by some shared life experience or time experience)
Statistical Significance, Generalizability, Confirmation Bias
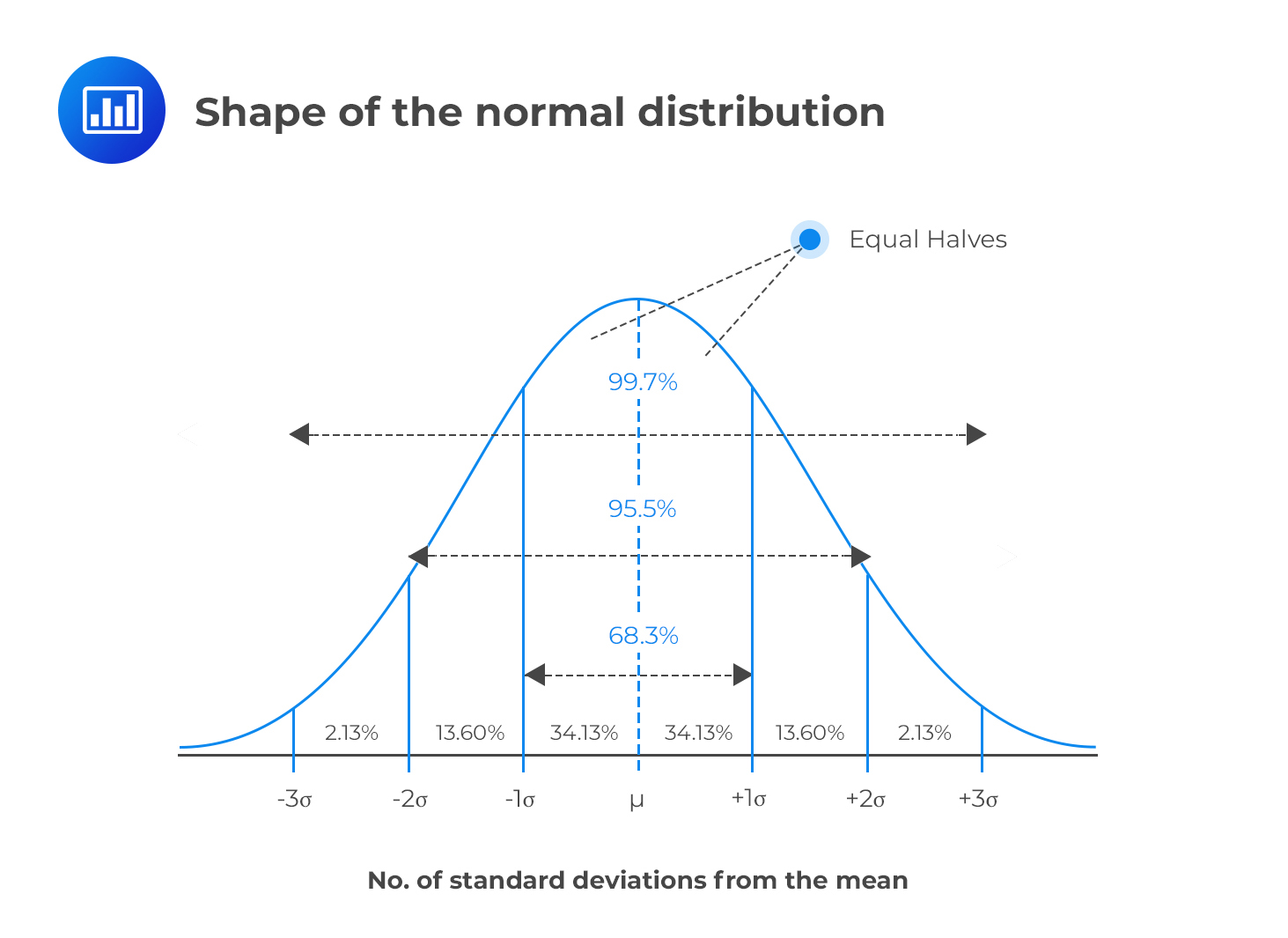
Standard Deviation: the “typical” difference between each score and the mean
Low Standard Deviation: data points clustered around the mean with few outliers
High Standard Deviation: data is dispersed over a wider range of values
Data isn’t always symmetrical:
Positive skew: a distribution of data where the majority of data points cluster towards the lower end of the spectrum, with a smaller number of outliers near the higher end
Negative skew: a distribution of data where the majority of data points cluster towards the higher end of the spectrum, with a smaller number of outliers near the lower end
Statistical significance: degree to which results cannot be attributed to chance
The generally accepted statistical cut-off is p < .05, meaning there’s a 95% likelihood the results are NOT likely due to chance (if p-value is below 0.05, it is considered significant)
Ethical Guidelines
Researchers must obtain informed consent; volunteers only
Researchers must induce a minimum of harm or stress
Volunteers have the right to discontinue at any time
Researchers must maintain the confidentiality of the volunteers
Researchers must insure a minimum amount of deception
Researchers have an obligation to debrief after the research has ended
Today, all research proposals in psychology must pass through an Institutional Review Board (I.R.B.)
Unit 1 P. 1: Biological Bases of Behavior
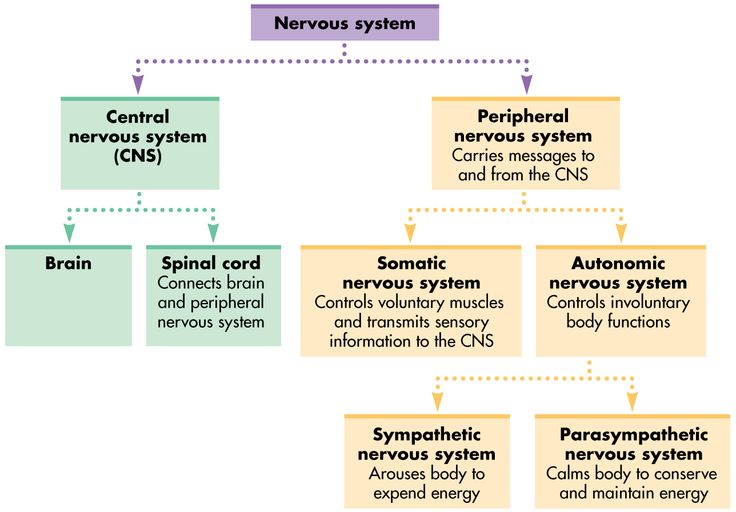
Branches of the Nervous System (Central vs Peripheral, Sympathetic vs Parasympathetic)
Central nervous system: made up of the brain and spinal cord that controls most of the functions of the body
Peripheral nervous system: connect the CNS to the limbs and organs, essentially serving as a relay between the brain and spinal cord and the rest of the body
Afferent vs Efferent Neurons
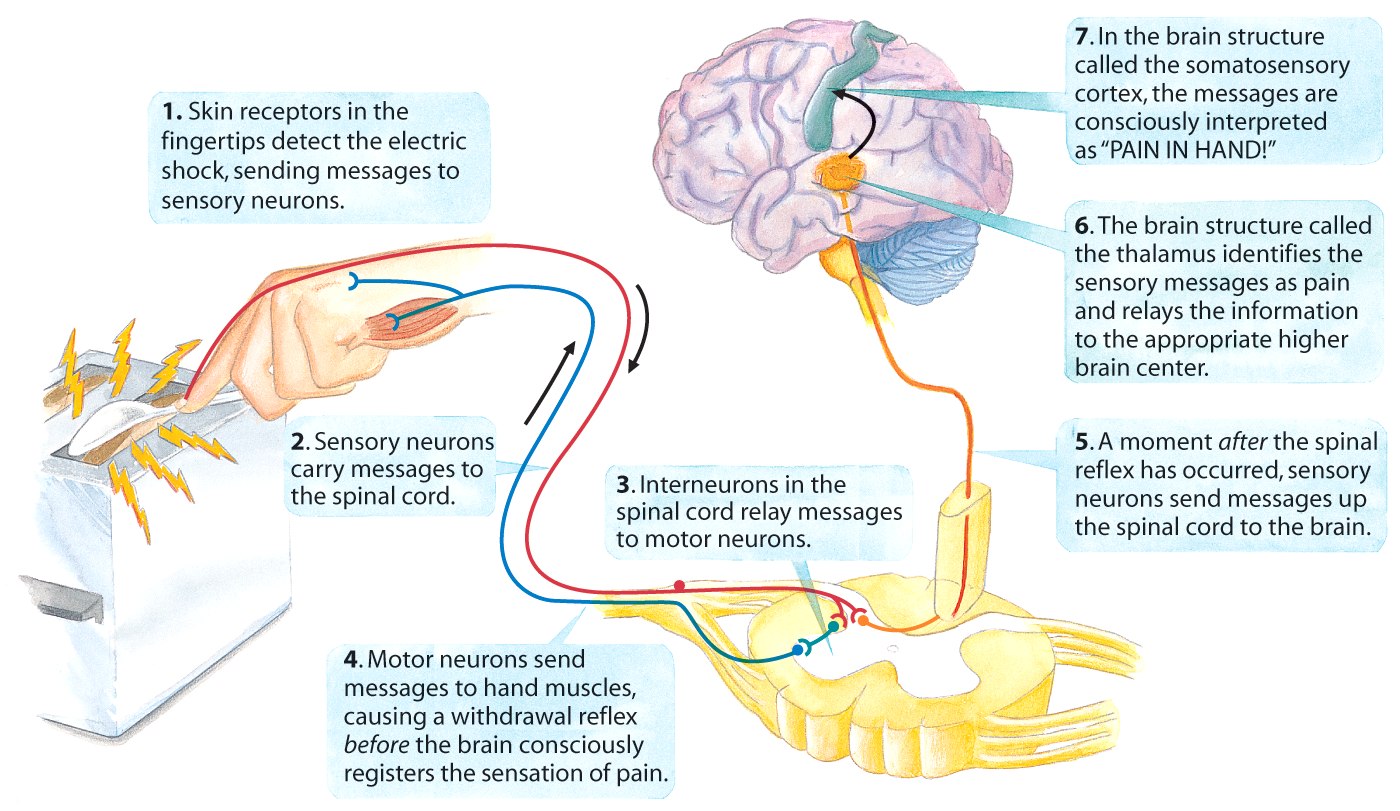
Afferent (Sensory) neurons carry messages in to the CNS
Efferent (Motor) neurons carry messages out from the CNS to the muscles + glands
Then there are interneurons, neurons in the CNS that communicate between sensory and motor neurons
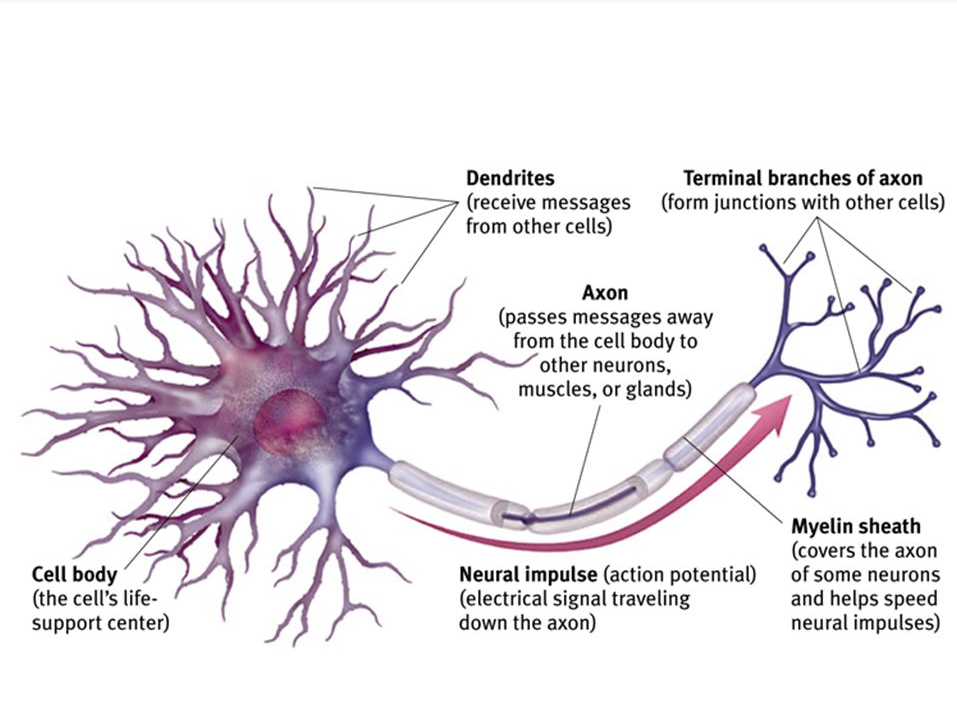
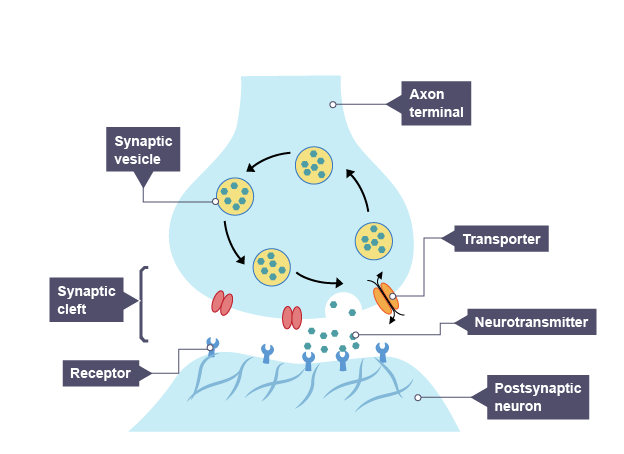
Parts of a Neuron (Dendrite, Soma, Axon, Myelin Sheath, Axon Terminals)
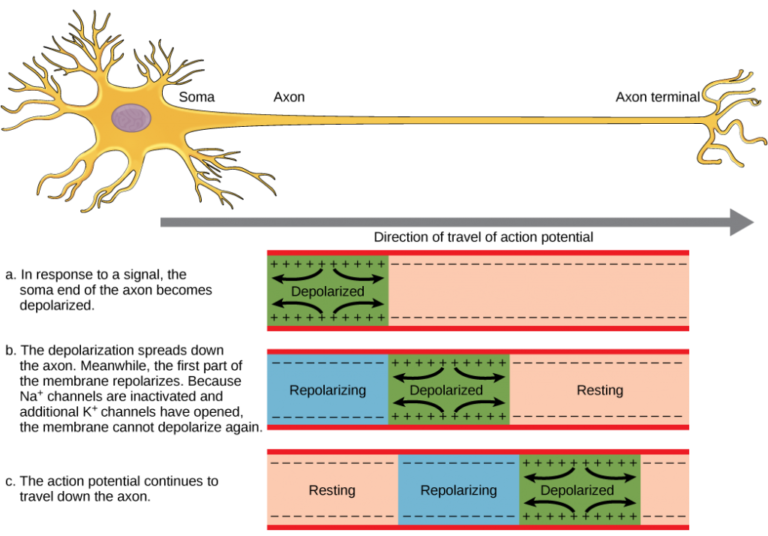
Neural Firing (Resting Potential, Firing Threshold, Action Potential, Refractory Period)
Resting Potential: The neuron is polarized - negatively charged inside the cell, positively charged outside, impermeable membrane
Firing threshold: When the neuron receives enough input, it “fires” in an all-or-none manner
Action potential: The electrical charge that skips down the axon of the neuron. The neuron is depolarized - positively charged inside the cell, permeable membrane
Refractory period: Brief period in which the neuron cannot “fire” while it “reloads.” A process of repolarization
Glial cells:
“Glue” neurons in place
Form myelin around axons
Support and provide nutrients
Cleaning up excess potassium ions
Reuptake: once the neurotransmitter is released into the synapse and completes its "work" it is reabsorbed back into the presynaptic neuron
Neurotransmitters (Excitatory vs Inhibitory, Substance P, Endorphins, Epinephrine/ Norepinephrine, Serotonin, Dopamine, Acetylcholine, GABA, Glutamate)
Excitatory: Neurotransmitters that stimulate neural activity
Inhibitory: Neurotransmitters that slow neural activity
Substance P (excitatory) : sends pain messages
Endorphins (inhibitory): block pain messages and linked to pleasure; opiates like opium, morphine and heroin are essentially artificial endorphins
Epinephrine/norepinephrine (excitatory): involved in alertness and arousal of fight or flight; makes the heart beat faster + increases blood pressure
Serotonin (inhibitory): stabilizing effect on mood, sleep, and appetite; mediates (inhibits) arousing impulses or stressful emotions + plays a role in how well and long you sleep (relaxation)
Dopamine (both excitatory and inhibitory): associated with pleasurable emotions, learning and attention, and movement; too much dopamine may lead to schizophrenia, too little may lead to Parkinson’s
Acetylcholine (excitatory): influences memory + enables muscle action; too little linked to Alzheimers
G.A.B.A. (Gamma-aminobutyric acid): primary inhibitory neurotransmitter; mood regulation
Glutamate: Primary excitatory neurotransmitter in the brain
Agonists and Antagonists:
Psychoactive drug: chemical substances that change a person’s perception, mood, and/or consciousness by affecting the way that their brain and nervous system function
Blood-brain barrier: semi-permeable membrane between the brain and the blood that only allows certain molecules to pass + blocks others from entering the brain tissue; drugs must pass this barrier in order to have an effect
Substance use vs. abuse:
Substance use: using substance, but does not yet interfere with person’s life
Substance abuse: pattern of drug use that diminishes one’s ability to fulfill their responsibilities; individual is dependent on drug if…
Tolerance: drug has a diminished effect on individual after repeated use, which means they have to consume it in increasingly larger amounts to achieve the original effect
Withdrawal: physical discomfort and distress when the substance use is discontinued
Using substance for a longer period of time/greater quantities than previously intended
Desire/repeated attempts to cut back on drug use
Spending large amount of time using/obtaining substance
Reduction/cessation of usual activities
Continued use of drug despite awareness of its dangers/negative effects
Types of dependence:
Psychological addiction: psychological need to use drug for relieving mental stress/negative emotions
Physical addiction: need drug to alleviate physical pain; severe withdrawal symptoms when drug use is discontinued
Agonists - drugs that mimic or encourage the activity of a specific neurotransmitter
Antagonists - drugs that block the effect of a particular neurotransmitter by blocking receptor sites
3 kinds of psychoactive drugs:
Depressants
Drugs that reduce neural activity + slow body function
Alcohol: dis-inhibitor that slows the brain activity responsible for making judgments and inhibitions + slows neural processing
slurred speech, lower skill performance, loss of balance and coordination, memory disruption/blackouts, loss of self-awareness
GABA agonist: mimics GABA activity (primary inhibitory neurotransmitter)
Barbituates (tranquilizer): GABA agonist that can be used to induce sleep and reduce anxiety, but can lead to memory and judgment impairment in large amounts + can be lethal when combined w/ alcohol
Opioids: endorphin agonist (mimics body’s natural painkillers) that causes euphoria followed by clouded mental functioning, reduces pain and anxiety, depresses sympathetic nervous system (pupil dilation, slowed breathing), and brain eventually stops producing its own endorphins w/ repeated use
Heroin
Opium
Morphine
Oxycodone
Stimulants: drugs that excite neural activity and speed up bodily functions
Caffeine: adenosine antagonist (inhibitory neurotransmitter that promotes sleep and supresses arousal), leading to increased alertness and wakefulness, withdrawal symptoms (headaches, fatigue, irritability, depression)
Nicotine: acetylcholine antagonist found in tobacco that boosts release of dopamine, and can have either stimulating or sedative effects depending on the amount smoked, and is highly addictive
Cocaine: dopamine agonist that leads to rush of euphoria and increased alertness/energy, may heighten aggression, and have depressive effects as it wears off
Ecstasy (MDMA): dopamine and serotonin agonist that is also a mild hallucinogen, leads to high energy, emotional elevation, and connectedness with those around them, and can damage the neurons that produce serotonin after repeated use, leading to depression
Amphetamines (Such as meth- amphetamines): dopamine and epinephrine agonist that speed up bodily functions, leading to increased energy and better mood, sometimes sense of euphoria, repeated use may reduce baseline dopamine levels, making normally pleasurable activities less enjoyable
Hallucinogens: drugs that distort visual and auditory perceptions and evoke sensory perceptions in the absence of sensory input
LSD: glutamate antagonist and serotonin agonist that causes sensory experience in the absence of stimuli, euphoria, and detachment from body, but can lead to paranoia and panic
Marijuana (THC): cannabinoid agonist that amplifies sensitivity to senses, relaxes, dis-inhibits, and produces euphoric feeling, can be used for pain relief in medicine, impairs motor coordination, perceptual skills, and reaction time, may intensify anxiety and depression, disrupts memory formation and interferes with immediate recall or new information (heavy use is associated with shrinkage of areas of the brain that process memory and emotions)
Parts of the Brain
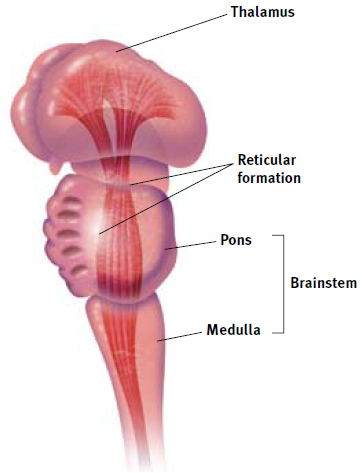
Hindbrain/Old Brain (Thalamus, Reticular Formation, Pons, Medulla, Cerebellum)
Brainstem: medulla (controls heartbeat, breathing, blood circulation, food digestion), pons (bridge between forebrain and cerebellum involved in movement, sleep, and dreaming), reticular formation (controls alertness and attention to incoming stimuli)
Thalamus: lies directly above brainstem + receives all sensory information except for smell, and directs the messages to the corresponding parts of the brain
Cerebellum: center for balance and coordination, smooth muscle movement, and storage of implicit memories related to movement
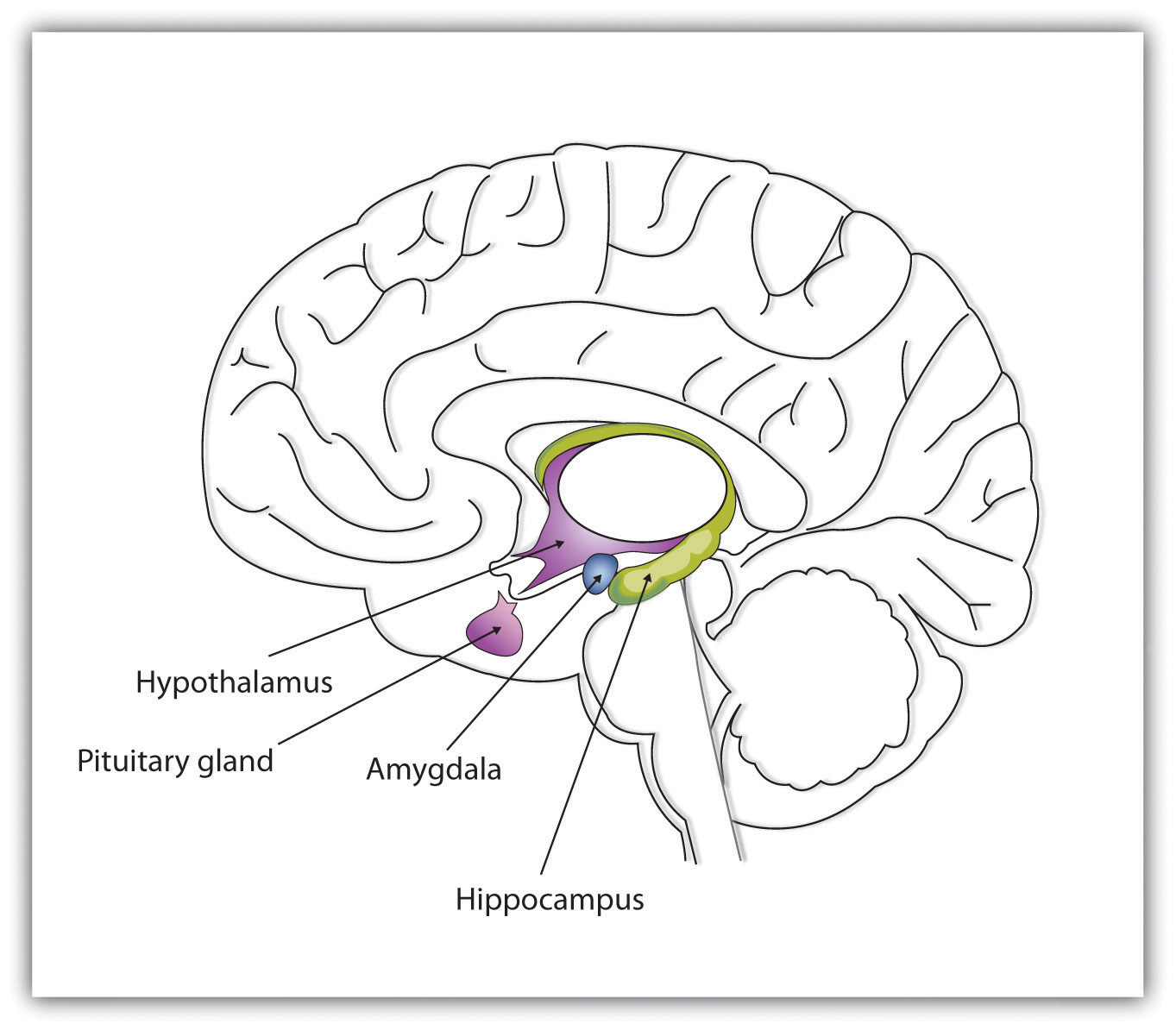
Midbrain/Limbic System (Amygdala, Hypothalamus, Hippocampus)
Hippocampus: formation of new memories
Amygdala: associated with fear, anger, and aggression
Hypothalamus: regulates appetite and thirst, sex drive, and fight or flight response; four “f’s” : feeding, fleeing, fighting, fornication
Forebrain/Cerebral Cortex (Frontal lobes, Parietal lobes, Occipital lobes, Temporal Lobes, Motor Cortex, Somatosensory Cortex, Broca’s Area, Wernicke’s Area)
Frontal lobe: judgment, planning, abstract thinking, social/emotional skills (personality), speaking
Broca’s Area: expression of language
Motor cortex: controls voluntary movement
Temporal lobe: processes sound + located above the ears
Olfactory cortex: processes smell
Parietal lobe: processes sense of touch, temperature, pain
Somatosensory cortex: processes incoming sensations
Wernicke’s area: located where the parietal lobe meets the temporal lobe that controls the comprehension of language
Occipital lobe: processes visual information, located in the back of the brain, meaning you see stars when you are hit in the back of the head
Brain Specificity vs Brain Plasticity and Long-Term Potentiation
Specificity/localization: concept that certain functions are localized in the brain
Brain plasticity: brain rewires and wires itself in response to new experiences (sometimes injury, but not always); brain modifies and adapts itself
The younger one is when injury occurs, the more functioning can be regained
Long-term potentiation: persistent strengthening of neural synapses based on frequent activity/consistent firing of certain neural pathways
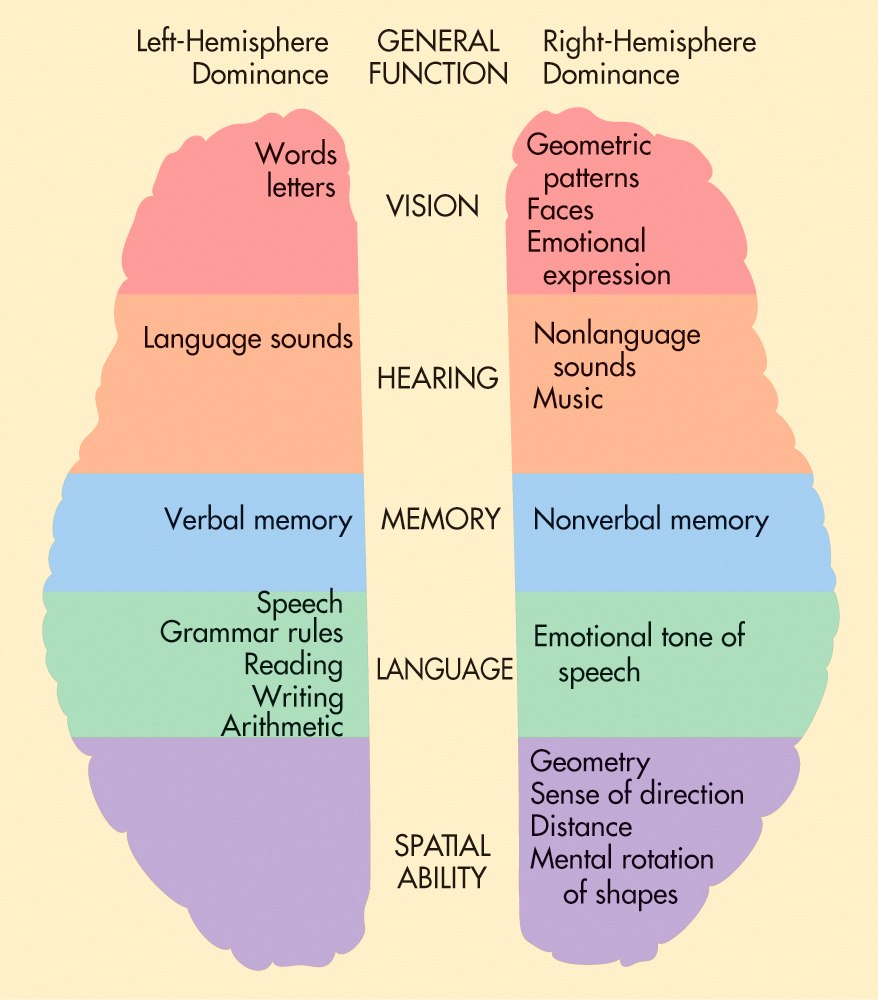
Left-brained: methodical, analytical, logical
Right-brained: artsy, creative, emotional
Right Hemisphere vs Left Hemisphere, Corpus Callosum, Split-Brain Research
Corpus Callosum: large, c-shaped, nerve fiber bundle connecting the two hemispheres (allows for communication between the left and right)
Split-brain: severing the corpus callosum, isolating the brain’s two hemispheres, which can be used to treat epileptic seizures
When split-brain patients are shown an image only in the left half of each eye's visual field, they cannot verbally name what they have seen; communication between the two hemispheres is inhibited, so the patient cannot say out loud the name of that which the right side of the brain is seeing
If a split-brain patient touches an object with only the left hand while receiving no visual cues in the right visual field; the patient will be unable to name the object
Each hemisphere controls the opposite side of the body that it is located in
Left hemisphere controls language, word processing, logic, analytical thinking, reasoning, writing, reading, listening, speaking, movement of right side of the body
Right hemisphere controls spatial ability/awareness, image processing, visualization, face recognition, body language, movement of left side of body
Sleep
Suprachiasmatic Nucleus (SCN), Pineal Gland, Melatonin
Suprachiasmatic nucleus: located in the anterior region of the hypothalamus that regulates the body’s circadian rhythm (regulates the timing and activity of the sleep-wake cycle)
Pineal gland: helps to control sleep and wake cycle by secreting melatonin when it is dark and decreases melatonin production when it begins to get light out again
Melatonin: hormone that your brain produces in response to darkness
NREM Stages (1,2,3) and REM Sleep
NREM sleep: stages 1-3 (not REM)
NREM-1 sleep: light sleep when hynogogic sensations, such as feelings of falling, occur characterized by theta waves
NREM-2 sleep: sleep characterized by theta waves interrupted by sleep spindles—bursts of rapid activity
NREM-3 sleep: deep sleep that is hard to wake from, characterized by delta waves (typically only first third of the night)
REM sleep: fourth stage (deepest stage of sleep w/ most pronounced dreams); rapid eye movement + delta waves
each cycle lasts about 90-110 mins, and as the night progresses, sleeper spends less time in deep sleep and more in lighter stages of sleep
Paradoxical sleep: while muscles are essentially paralyzed during REM because brainstem blocks messages from motor cortex, your brain is nearly as active as when you are awake, which can lead to sleepwalking and talking if messages not properly blocked
EEG (electroencephalogram): used to identify brain waves that characterize each stage of sleep; allows one to identify stage of sleep as well as how long they are in stage
Alpha Waves, Theta Waves, Delta Waves
Gamma waves occur when one is concentrating (high frequency)
Beta waves: brain waves that occur in a waking stage
Alpha waves: slower + less rapid than beta waves (relaxed, but awake)
Theta waves: characterize NREM-1 sleep, or the first official sleep stage; theta waves are slower + less frequent than alpha waves
brief transitional phrase that might cause one to feel as if they are floating or falling
hypnagogic jerks/sensations: sudden twitching movements that are involuntary
Delta waves: high amplitude brain waves that characterize deeper stages of sleep (low frequency)
Insomnia, Narcolepsy, Sleep Apnea, Night Terrors, Somnambulism, REM Sleep Behavior Disorder
Chronic sleep deprivation can lead to depression, obesity, high blood pressure, suppressed immune system function, and slowed reaction time
Insomnia: disorder characterized by inability to fall asleep/stay asleep that can lead to memory loss, irritability, and a weaker immune system
Narcolepsy: disorder characterized by sudden, involuntary change from an alert stage to a sleep stage when individual quickly enters REM sleep, which can cause loss of major muscle functioning (sleep paralysis and cataplexy) that accompanies REM
Sleep apnea: disorder in which individual frequently stops breathing during night, causing them to gasp and come to an awake state; constantly restarting REM sleep=miss out on deep sleep + lighter REM sleep, causing excessive sleepiness during day
NREM-3 sleep disorders that are more common in children :
Night terrors: waking with high physiological awareness (sweating, increased heart and respiration rates) with little to no recollection of event in morning
Somnabulism: characterized by walking in sleep that may result from images + thoughts that occur during NREM period, when ones body is generally difficult to wake, and do not recall what has happened upon waking
Sleep talking/somniloguy: talking in one’s sleep w/ no subsequent recollection of event
Sleep paralysis: temporary inability to move or speak while falling asleep or waking up
REM sleep behavior disorder: occurs when a sleeper is not “paralyzed” during REM sleep and may physically act out their dreams
Memory-Consolidation Theory, Sigmund Freud’s Wish Fulfillment Theory, Manifest Content, Latent Content, Activation-Synthesis Theory
Evolution/adaptive theory: we sleep at night because it has generally been safer/more functional for us to do
Restorative theory: we sleep simply to rejuvenate and recuperate; replenish physical energy, and to allow neurons and other cells to rest and repair themselves
Memory consolidation theory: we need to sleep + dream to sift through the day’s events, filing and processing memories that we wish to keep and disposing of those we wish to discard (strengthening some neural connections)
Growth theory: sleep is when the pituitary gland releases growth hormones
Dreams: images, sounds, thoughts, and emotions that pass through our mind while sleeping
Wish-fulfillment theory: Freud’s idea that dreaming allows us to act out the desires that we must repress during the day
Manifest content: Freud’s argument that dreams have a superficial plot/story line
Latent content: underlying, symbolic “unconscious” meaning of the dream
Activation synthesis theory: because the brain is active during REM periods, when the majority of dreaming takes place, Hobson and McCarley proposed that REM sleep triggers neural activity that our brain tries to make sense of by weaving them into a story
Problem-solving theory: dreams are opportunities to work through daily emotional and cognitive problems when not occupied by other external stimuli
Lucid dreaming: being aware that one is in a dream/being able to control aspects of dream
Sensation
Transduction
Structures of the Eye (Cornea, Pupil, Iris, Lens, Retina, Rods, Cons, Fovea, Optic Nerve/Blind Spot)
Transduction: converts physical energy into forms of neural messages (sound and light waves)
Cornea: eye’s clear, protective outer layer of tissue that covers the pupil and the iris; light enters the eye through the cornea first, and it helps focus light
Pupil: the opening in the center of the iris through which light passes
Iris: a ring of muscle tissue that forms the colored portion of the eye and controls the size of the pupil
Lens: the transparent structure behind the pupil that changes shape to focus images on the retina
Accommodation: the curvature of the lens of your eyes changes in response to changes in distance
To focus on a distant object – the lens is pulled thin, this allows the light rays to refract slightly + flatten
To focus on a nearby object, the lens thickens and curves
Retina: back wall of eye that contains rods and cones + layers of neurons that begin processing of visual information
Rods: photoreceptors that detect black, white, and gray, and are necessary for peripheral and twilight vision when cones don’t respond
Cones: photoreceptors that are concentrated near the center of the retina (fovea!!) and function in daylight or in well-lit conditions; cones detect fine detail and create color sensations
Light waves are transduced into neural impulses by the rods and cones, then passed to the bipolar cells and the ganglion cells, and then the optic nerve
Fovea: central focal point of the retina where the highest concentration of cones is located; area of greatest visual acuity/sharpness
Optic nerve: leaves through the back of the eye and carries neural impulses from the eye to the brain
Blind spot: the head of the optic nerve creates a “blind” spot because no receptor cells (rods or cones) are located there
Accommodation, Trichromatic vs Opponent Process Theory, Color Blindness
Trichromatic theory: theory that there are three kinds of cones: red, blue, green; these combine to form 7.5 million different hues
Opponent process theory: humans are equipped with red/green cells and blue/yellow cells
When one is excited the other is inhibited
Color blindness: more like color deficiency, can see some colors, just can’t differentiate between some hues (red-green color blindness most common in males)
Structures of the Ear (Auditory canal, Tympanic membrane, Hammer/Anvil/Stirrup, Semicircular canals, Cochlea, Basilar membrane/Hair cells, Auditory Nerve)
Hair cells (fibers on tip of cilia) that are located in the cochlea on the basilar membrane, and are bent by the fluid in the cochlea
hair cells transduce sounds waves into auditory impulses, which then travel to the thalamus, and then to the auditory cortex in the temporal lobe
Semicircular canals: 3 tubes that are filled with fluid and allow us to balance
Cochlea: snail shape, fluid filled tube that contain hair cells on the basilar membrane
Auditory canal: sound waves travel through the canal to the middle ear
Tympanic membrane: eardrum, passes vibrations to the ossicles + tightly stretched and very fragile
Hammer/Anvil/Stirrup (ossicles): 3 tiny bones that pass vibrations to the oval window (cochlea)
Auditory nerve: carries auditory info (neural messages) to the thalamus to the auditory cortex to the temporal lobe
Frequency is the number of waves that arrive per second; the higher the frequency, the higher the pitch, and the lower the frequency, the lower the pitch
Sound localization: is the ability to determine the location and the distance of a sound
Sensorineural vs Conductive Deafness
Conductive deafness: problems with carrying sounds into inner ear, which can be caused by damage to middle ear/tympanic membrane/ eardrum
Sensorineural deafness: hearing impairment associated with damage to hair cells on the basilar membrane of the cochlea or the auditory nerve
Place Theory vs Frequency Theory
Place theory: the pitch of a sound is determined by the location on the basilar membrane where the sound vibrates hair cells
Frequency theory: hair cells fire at the same frequency as the incoming sound wave
Volley principle: at very high frequencies, hair cells fire in rapid succcession one after another to achieve the frequency of the sound wave
Olfaction, Olfactory Cells
Olfactory receptor cells in the nasal cavity respond to airborne molecules; lock and key, as certain molecules only bind to certain receptors
Olfactory bulb sends neural messages to the olfactory cortex in the temporal lobe
Touch Receptors (Pressure, Pain, Cold, Warmth)
Touch receptors: nerve endings under the skin that respond to cold, pain, warmth, and pressure
wetness=cold and pressure receptors repeatedly stimulated
tickle: caused by stimulation of neighboring pressure receptors
itching: repeated stimulation of pain receptors
Gate Control Theory of Pain: pain is determined by the operation of small and large nerve fibers in the spinal cord
small nerve fibers: carries pain from the body to the brain
large nerve fibers: conduct most other sensory signals
spinal cord contains a neurological gate; when small nerve fibers open the gate, we experience pain, and when large nerve fibers close the gate, it blocks small nerve fiber pain messages
Vestibular Sense, Kinesthetic Sense, Proprioceptors
Vestibular sense: body’s sense of whole body balance and posture due to fluid and hair cell receptors in the semicircular canal responding to gravity and changes in body position
Kinesthetic sense: body’s sense of body part position and posture due to prioreceptors in the body’s muscles and joints/tendons
Synesthesia
Perceptual phenonemon in which stimulation of one sense causes automatic experience of another sense
Habituation, Selective Attention, and Sensory Adaptation
Sensory Adaptation: when our sensory receptors become less responsive to stimulus over time, but our attention can be brought back to it if there is a change in the stimulus (sensory/neural level)
Habituation: when we stop responding to stimulus after repeated exposure (learned behavior)