Endocrine System and Blood
Section 1.1: Endocrine System Anatomy & Physiology
Materials
Endocrine system models
This section introduces you to the anatomy, histology, and physiology of the endocrine organs and hormones. The endocrine system:
Is a diverse group of ductless glands that plays a major role in maintaining homeostasis of multiple physiological variables.
Note: Endocrine glands are different from exocrine glands, which are glands that rely on ducts to release their substance, such as enzymes, tears, sweat, and milk.
Examples of exocrine glands are sweat, salivary, lacrimal, digestive, & mammary glands.
The endocrine system works closely with the other system that maintains homeostasis of multiple physiological variables—the nervous system.
The endocrine system, along with the nervous system, provides means for regulating other organ systems and tissues and maintaining homeostasis.
Although these 2 systems both work toward the same goal of internal communication and coordination, you will notice that the methods by which they do so differ:
The nervous system functions via action potentials (nerve impulses) and releases neurotransmitters that directly affect target cells. The effects are nearly immediate, but they are very short in duration.
In contrast, the endocrine system brings about its effects via the secretion of hormones—chemicals released into the bloodstream that typically act on distant targets. The effects of hormones are not immediate, but they are longer-lasting than those of the nervous system.
In general, hormones regulate the processes of other cells, including inducing the production of enzymes or other hormones, changing the metabolic rate of a cell, and altering permeability of the plasma membrane.
You might think of hormones as the “middle managers” of the body, because they communicate the messages from their “bosses” (the endocrine glands) and tell the “workers” (other cells) what to do.
Some endocrine glands (e.g., the thyroid and anterior pituitary glands) secrete hormones as their primary function. Others, however, secrete hormones as a secondary function, examples of which are the heart (atrial natriuretic peptide), adipose tissue (leptin), the kidneys (erythropoietin), and the stomach (gastrin).
The nervous system is often referred to as our fast response system and tends to have very specific and localized targets of its action.
In contrast, the endocrine system is our slow response system, often taking hours, days, weeks, or longer to produce noticeable physiological changes in the body. Although typically much slower, the endocrine system nevertheless can elicit powerful physiological effects throughout the body and on many organs and tissues simultaneously, as long as the target cells of specific hormones have the necessary receptors.
Endocrine Organs, Hormones, & Functions
Here are the 10 endocrine organs that have hormone secretion as a primary function:
Note: from here on out, students are required to spell out any abbreviated terminologies listed in the lab manual. Abbreviated answered will be considered incorrect. We will inform all of you for any exceptions to this rule.
Hypothalamus
Pituitary gland
Pineal gland
Thyroid gland
Parathyroid glands
Thymus gland
Adrenal glands
Pancreas
Ovaries
Testes.
Let’s take a closer look at each of these organs (note that we discuss the ovaries and testes only briefly here; they are discussed further in Exercises 10 and 11).
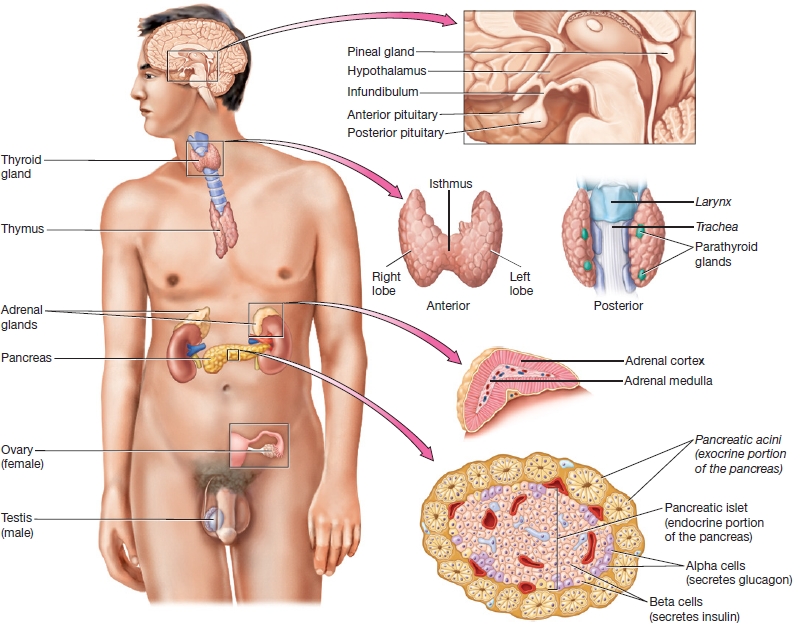
Figure 1.1 Organs and tissues of the endocrine system.
1. Hypothalamus: is the inferior part of the diencephalon and is known as a neuroendocrine organ.
It can be likened as the endocrine system’s chief executive officer (CEO).
It has a close working relationship with the pituitary gland, to which it is attached by a stalk called the infundibulum (in-fun-di-bu-lum).
The hypothalamus produces the following hormones, which will be dependent on whether these hormones interact with the anterior or posterior pituitary glands. Again, these hormones are still produced by the hypothalamus, not by the pituitary gland:
A. Interacts with the Anterior Pituitary:
Inhibiting and Releasing Hormones: are hormones that inhibit and stimulate secretion from the anterior pituitary gland.
In Figure 1.2A, you can see how the hypothalamus communicates with the anterior pituitary gland via a specialized set of blood vessels, called hypothalamic-hypophyseal portal system (HHPS). As shown in the pathway below:
The inhibiting and releasing hormones are synthesized by hypothalamic neurons⇒ then, they enter capillaries in the hypothalamus ⇒ after which they travel through small veins in the infundibulum ⇒ finally, they enter a second capillary bed in the anterior pituitary, where they exit the blood and interact with anterior pituitary cells to influence their functions.
B. Interacts with the Posterior Pituitary:
Oxytocin and Antidiuretic Hormone: These hormones are produced by hypothalamic neurons that extend the length of the infundibulum down into the posterior pituitary gland, where they are stored (Fig. 1.2B).
Oxytocin: Triggers uterine contraction and milk ejection from the mammary glands. Do not confuse its function with prolactin. Oxy- means sharp and -tocin refers to childbirth.
Milk ejection makes sense for this hormone since the birth of the child already happened, therefore it needs the milk ejected from the mother's mammary glands for sustenance.
Antidiuretic Hormone(ADH): Causes water retention from the kidneys. It also assists with blood pressure control. Anti- means against, while diuretic pertains to production of urine.
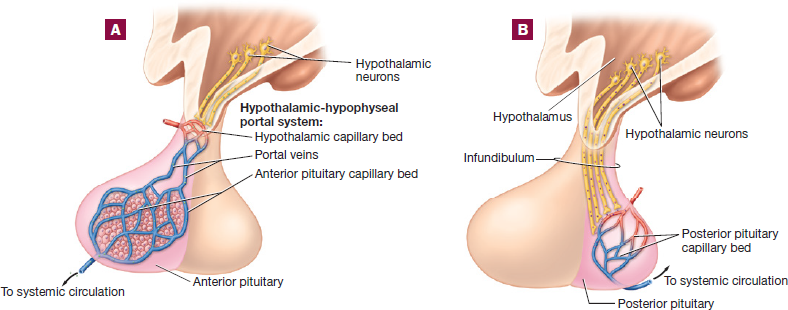
Figure 1.2 Hypothalamus and pituitary gland: (A) hypothalamus and anterior pituitary;
(B) hypothalamus and posterior pituitary.
2. Pituitary Gland: Notice in Figure 1.2 that the pituitary gland is actually made of 2 separate regions:
The anterior pituitary gland or adenohypophysis, is composed of glandular epithelium and secretes a variety of hormones that affect other tissues in the body.
The posterior pituitary or neurohypophysis, is actually composed of nervous tissue rather than glandular tissue.
In response to hypothalamic-releasing hormones, the anterior pituitary gland secretes hormones that stimulate other endocrine and exocrine glands in the body.
Anterior Pituitary Gland: mostly produces hormones known as tropic hormones.
Tropic hormones influence the functions of other endocrine or exocrine glands.
Mnemonic: FLAT-PG
2 reproductive hormones which affects both the testes and ovaries:
Follicle-Stimulating Hormone (FSH), a hormone that will influences and stimulates follicles in the ovary and sustentacular cells in the testes.
Luteinizing Hormone (LH), a hormone that influences and stimulates the oocyte in the ovary and interstitial cells in the testes.
Adrenocorticotropic Hormone (ACTH), which stimulates secretion from the adrenal cortex (a-dre-no-cor-ti-co-tro-pic).
Thyroid-Stimulating Hormone (TSH), which stimulates growth of and secretion from the thyroid gland.
Prolactin, which stimulates milk production from mammary glands. Do not confuse its function with oxytocin's function.
An exception is Growth Hormone (GH), which increases the rate of cell division and protein synthesis in all tissues and has both tropic and non-tropic effects.
Posterior Pituitary Gland: Does not produce any hormones at all and functions merely as a place to store the oxytocin and antidiuretic hormone produced by the hypothalamus.
3. Pineal Gland: Located in the posterior and superior diencephalon.
This neuroendocrine organ secretes the hormone melatonin.
It secretes it in response to decreased light levels.
The hormone acts on the "reticular formation" part of the brainstem to trigger sleep.
4. Thyroid Gland: Located in the anterior-inferior neck superficial to the larynx (not larnyx) or voicebox.
It consists of right and left lobes connected by a thin band of tissue called isthmus.
Microscopically, it is composed of hollow spheres called thyroid follicles (Fig. 1.3).
The cells that line the thyroid follicles are simple cuboidal cells called follicle cells.
The spheres encapsulates a gelatinous, iodine-rich substance called colloid.
The follicle cells respond to TSH from the anterior pituitary by secreting a chemical into the colloid that reacts with iodine to produce 2 different hormones:
Thyroxine (T4): has 4 iodine molecules. Do not confuse with thymosin.
Triiodothyronine (T3): has 3 iodine molecules (tri-i-o-do-thy-ro-nine).
T3 is the most active of the two hormones.
Acts on essentially all cells in the body to increase the metabolic rate, increase protein synthesis, and regulate the heart rate and blood pressure, among other things.
About 10 times as much T4 is produced as T3, and the body converts T4 to T3 when the T3 level in the blood drops.
Between the follicle cells we find another cell type called the parafollicular cells.
These cells produce the hormone calcitonin.
1 of the 2 hormones that play a role in calcium ion homeostasis.
Calcitonin is secreted when calcium ion levels in the blood rise.
It triggers osteoblast activity and bone deposition, thus lowering the blood calcium levels.
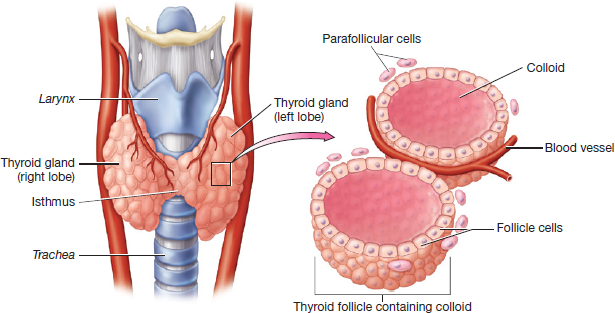
Figure 1.3 Thyroid gland and thyroid follicles.
5. Parathyroid Glands: Refer back to Figure 1.1 where you can see these 4 small glands on the posterior side of the thyroid gland.
They secrete the hormone Parathyroid Hormone (PTH):
Which is the main hormone in the body that maintains calcium ion homeostasis.
PTH is secreted in response to a decreased level of calcium ions in the blood. It triggers:
Osteoclast activity and resorption (losing) of bone tissue.
Increased calcium ion absorption from the intestines.
Increased calcium ion reabsorption (absorbing again) from the kidneys.
They all result in increasing blood calcium levels.
Note: Hormones such as PTH and calcitonin that have opposite actions are called antagonists.
6. Thymus Gland: Sits in the superior mediastinum.
It is large and active in infancy and early childhood, during which time it secretes the hormones thymosin and thymopoietin.
Both of these hormones stimulate the development of T lymphocytes within the thymus gland.
In adults most of the thymic tissue is gradually replaced by fat and other connective tissue.
7. Adrenal Gland: As the name implies, the adrenal glands sit atop the superior pole of each kidney (ad- means next to, while renal refers to kidney).
Like the pituitary gland, the adrenal gland is actually composed of 2 separate structures:
Outer adrenal cortex
Inner adrenal medulla
The glands are surrounded by a thin layer of connective tissue - adrenal capsule (Fig. 1.4).
Adrenal Cortex: The superficial region of the adrenal gland consists of glandular tissue.
It secretes steroid hormones (derived from cholesterol), in response to stimulation by the adrenocorticotropic hormone produced by the anterior pituitary gland and other factors.
It is made up of 3 sections/zones:
Mnemonic: Zona GFR
Note: pay attention to the words "type" of steroid hormone vs "examples" of these types of steroid hormones.
Zona Glomerulosa: The outermost zone of the adrenal cortex, it secretes a type of steroid hormone called mineralocorticoids.
A specific example of mineralocorticoid is aldosterone, which regulates fluid, electrolyte, and acid-base homeostasis.
Mnemonic:GMA (Glomerulosa, Mineralocorticoid, Aldosterone)
Zona Fasciculata: The middle zone of the adrenal cortex, it secretes a type of steroid hormone called glucocorticoids.
A specific example of glucocorticoid is cortisol, which regulates the stress response, blood glucose, fluid homeostasis, and inflammation.
Mnemonic: FGC (Fasciculata, Glucocorticoid, Cortisol)
Zona Reticularis: The innermost zone of the adrenal cortex, it secretes a type of steroid hormone called gonadocorticoids and also glucocorticoids.
Examples of gonadocorticoid are androgens and estrogen, which affect the gonads and other tissues.
Androgens control many aspects of male development and reproductive physiology.
Adrenal Medulla: The deep region or core of the adrenal gland.
It consists of modified postsynaptic sympathetic neurons that secrete the hormone adrenal catecholamines which are derived from amino acids, examples are:
Epinephrine and norepinephrine which are secreted into the blood in response to sympathetic stimulation (fight or flight).
The adrenal catecholamines have the same effects on target cells as the neuronal catecholamines released by sympathetic neurons, such as:
Dilation of bronchioles; increase in the rate and force of contraction of the heart; constriction of blood vessels serving the skin and abdominal viscera; dilation of the pupil; and more (these all makes sense since it is preparing the body for fight or flight).
Adrenal catecholamines also:
Prolongs the sympathetic response, as the effects of neuronal catecholamines are terminated after only a few seconds.
Are able act on target cells that are not innervated by sympathetic neurons.
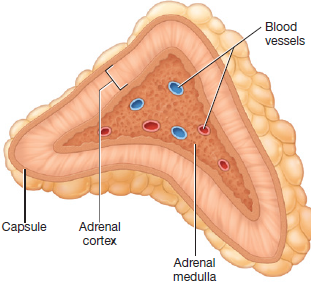
Figure 1.4 Adrenal gland.
8. Pancreas: An elongated and spongy gland located below and behind the stomach. It has both endocrine and exocrine functions.
Exocrine Functions: Are carried out by a group of cells called pancreatic acini or acinar cells, which occupies about 99% of the gland and release pancreatic juices into pancreatic ducts.
These pancreatic juices contribute to neutralizing hydrochloric acid, digesting protein, fat, and starches.
Endocrine Functions: Are carried out by these small round islands called pancreatic islets, which are embedded within the pancreatic acini (Fig. 1.5).
The cells within the pancreatic islets secrete the hormones insulin and glucagon, which play a major role in regulating blood glucose levels.
Insulin: produced by cells called beta (β) cells.
It triggers the uptake of glucose by cells, which decreases the concentration of glucose in the blood.
Glucagon: produced by alpha (α) cells, is insulin’s antagonist.
It triggers the release of stored glucose from the liver and the production of new glucose, which increases the concentration of glucose in the blood.
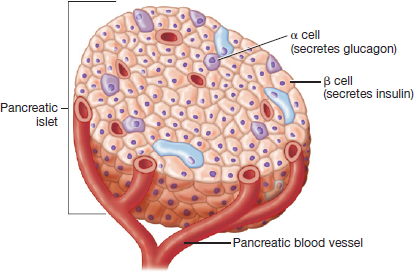
Figure 1.5 Pancreatic islet.
9. Testes: Anatomically speaking, these are the male reproductive organs located in the scrotum that produce sperm cells (male gametes).
Cells within the testes called interstitial cells produce a steroid hormone called testosterone.
This hormone promotes the production of sperm cells and the development of male secondary sex characteristics such as a deeper voice, greater bone and muscle mass, and facial hair.
10. Ovaries: Anatomically speaking, these are the female reproductive organs, located in the pelvic cavity that produce oocytes (female gametes).
The ovaries produce steroid hormones called estrogen and progesterone.
Estrogen play a role in the development of oocytes, female secondary sex characteristics such as breasts and subcutaneous fat stores, and a variety of other processes.
Progesterone has a number of effects that prepare the body for pregnancy.
1. Erythrocytes: commonly known as red blood cells, carry oxygen around the body on an iron-containing protein called hemoglobin (Fig. 1.9). They are the most numerous blood cells, averaging about 44 percent of the total blood volume. This value, known as the hematocrit, which is typically higher in males (40 to 50 percent) than in females (36 to 44 percent). Erythrocytes are easily distinguished from the other formed elements by their reddish-pink color and the fact that mature erythrocytes lack nuclei and most organelles.

Figure 1.9 Photomicrograph of erythrocytes and platelets.
2. Thrombocytes: commonly known as platelets. Note in Figure 1.9 that they aren’t actually cells at all but are instead just small cellular fragments. As such, they lack nuclei and most organelles and are much smaller than the other formed elements. They are involved in blood clotting and make up less than 1 percent of the total blood volume.
3. Leukocytes: commonly known as white blood cells, play a role in the immune system and make up less than 1 percent of the total blood volume. The two subclasses of leukocytes (granulocytes and agranulocytes) are based upon the presence or absence of visible granules in their cytoplasm.
A. Granulocytes: As implied by their name, they are cells containing cytoplasmic granules that are visible when stained. The 3 types of granulocytes stain differently when treated with the dyes hematoxylin (dark purple) and eosin (red) and are named for the type of stain with which they interact.
Neutrophils: does not interact strongly with either type of dye, and their granules stain a light violet-pink color. They are the most numerous type of leukocyte, making up about 60 to 70 percent of the total leukocytes in the blood. They typically have multilobed nuclei, although their nuclei often vary in appearance, which gives rise to their other name: polymorphonucleocytes. One common variation in nucleus shape, shown in Figure 1.10, is seen in immature neutrophils called band cells. As you can see, the nucleus of a band cell has a single lobe that is stretched into a U-shape (or a single “band”).
Neutrophils are attracted to the site of any cellular injury, and are particularly active in ingesting and destroying bacteria.
Eosinophils: interact strongly with the red dye: eosin, and their granules stain bright red. They are far less numerous than neutrophils, accounting for only about 4 percent of the total leukocytes in the blood. As with neutrophils, their nuclei are segmented into lobes, although eosinophils’ nuclei tend to be bilobed.
Eosinophils play a role in the immune response to infection with parasitic worms and the allergic response.
Basophils: take up the dark purple stain: hematoxylin (it is a basic dye, hence their name basophil), and their granules appear dark blue-purple. Like eosinophils, they tend to have bilobed nuclei, but their nuclei are often obscured by their dark granules. They are the least numerous of the leukocytes, making up fewer than 1 percent of the total leukocyte count, and will likely be the most difficult to find on your slide.
Basophils are primarily involved in the allergic response.

Figure 1.10 Formed elements of blood.
B. Agranulocytes: They lack visible cytoplasmic granules. The 2 types of agranulocytes are:
Lymphocytes: tend to be smaller than granulocytes and have large, spherical nuclei that are surrounded by a rim of light blue-purple cytoplasm. They are the second most numerous type of leukocyte, making up 20 to 25 percent of the total leukocyte count. There are two populations of lymphocytes:
B lymphocytes produce proteins called antibodies that bind foreign glycoproteins called antigens.
T lymphocytes play numerous roles, including enhancing other aspects of the immune response, destroying cancer cells, and destroying cells infected with viruses.
Monocytes: are the largest of the leukocytes and have U-shaped or horseshoe-shaped nuclei with light blue or light purple cytoplasm. They are the third most numerous type of leukocyte, accounting for 3 to 8 percent of the total.
Monocytes exit the blood to mature into cells called macrophages, which are very active phagocytes. Phagocytes engulf or eat bacteria or other foreign cells.
Blood transfusion, the infusion of a recipient with a donor’s blood cells, is a commonly performed medical procedure. Before a recipient is given a blood transfusion, the medical team must first learn the patient’s blood type and then find a suitable, or “matching,” donor. This is necessary because of the A, B, and Rh antigens on the surface of the donor erythrocytes and the presence of preformed antibodies in the recipient’s blood plasma. If a donor’s erythrocytes have antigens the recipient’s immune system recognizes as foreign, the recipient’s antibodies will agglutinate the foreign erythrocytes. The agglutinated erythrocytes are then destroyed by the immune system, a process known as hemolysis. This is called a transfusion reaction, and it is a medical emergency that can lead to kidney failure and death.
To ensure that a transfusion reaction does not occur, we must make sure the donor blood does not have antigens the recipient’s immune system will recognize as foreign. For the ABO blood group, our immune systems produce antibodies to any antigen not present on the surface of our own cells.
People with type A blood have A antigens and so produce anti-B antibodies.
People with type B blood have B antigens and so produce anti-A antibodies.
People with type O blood have neither A nor B antigens and so produce anti-A and anti-B antibodies.
People with type AB blood have both A and B antigens and so produce neither anti-A nor anti-B antibodies.
If you’re wondering about the Rh factor, wait just a moment—we’re getting there. Let’s do an example with the ABO blood group first:
Felix has type B blood, which means that he has anti-A antibodies. What will happen if we give him blood from a donor with:
Type A blood? There are A antigens on these donor erythrocytes, and Felix’s anti-A antibodies would agglutinate them. ✗
Type B blood? Felix’s anti-A antibodies would have no effect on the B antigens on these donor erythrocytes, so this blood is safe. ✓
Type O blood? There are no antigens on these donor erythrocytes, so Felix’s anti-A antibodies would have no effect on them, and this blood is safe. ✓
Type AB blood? There are both A and B antigens on these donor erythrocytes, and Felix’s anti-A antibodies would bind and agglutinate the A antigens. ✗
Now that’s easy, isn’t it?
Next let’s address the Rh factor. The blood of an Rh-negative person does not contain preformed antibodies to the Rh antigen. However, anti-Rh antibodies are made if an Rh-negative person is exposed to the Rh antigen. In an emergency setting, it is generally not possible to determine if an Rh-negative person has been exposed to the Rh antigen, so healthcare professionals err on the side of caution and assume that the person has anti-Rh antibodies. For the sake of simplicity, we will assume the same thing in this exercise. So, for our purposes:
People with Rh-positive blood do not produce anti-Rh antibodies.
People with Rh-negative blood do produce anti-Rh antibodies.
Let’s do one more example, taking into account the Rh factor this time:
Lourdes has A- blood, which means that she has anti-B and anti-Rh antibodies. What will happen if we give her blood from a donor with:
Type A + blood? There are A and Rh antigens on these donor erythrocytes, and Lourdes’ anti-Rh antibodies would agglutinate the Rh antigens. ✗
Type B− blood? There are B antigens on these donor erythrocytes, and Lourdes’ anti-B antibodies would agglutinate them. ✗
Type O− blood? There are no antigens on these donor erythrocytes, so Lourdes’ anti-B and anti-Rh antibodies would have no effect on them, and this blood is safe. ✓
Type AB + blood? There are A, B, and Rh antigens on these donor erythrocytes, and Lourdes’ anti-B and anti-Rh antibodies would agglutinate the B and Rh antigens. ✗
Rule of Thumb, that you may or may not find helpful:
If the blood type has a positive sign, it can donate/give to positive blood types only. But it can receive from both positive and negative blood types. It will just depend whether it is A, B, AB, or O.
Think of a person with a positive attitude still giving out positivity to the world, even though they are receiving both positive and negative energy from everyone else.
If the blood type has a negative sign, it can donate/give to both positive and negative blood types. But it can only receive from negative blood types. It will just depend whether it is A, B, AB, or O.
Think of a negative person's negativity affecting (giving) both people with positive and negative energies. They are only receiving more negative energy from other negative people.
You should notice something from Table 1.2: People with AB+ blood can receive from any donor blood type, and people with O− blood can donate to any recipient blood type. This is because people with AB+ erythrocytes have all three antigens and so their blood contains no antibodies to bind to donor blood. Conversely, people with type O− erythrocytes have none of the three antigens and so there is nothing for any recipient’s antibodies to bind. For these reasons, type AB+ blood is often called the universal recipient and type O− blood is often called the universal donor.