Mitral and Tricuspid Valve Regurgitation
Introduction
The purpose of echocardiography in the context of surgery and intervention for valve diseases.
Need to inform surgeons and interventionists about key valve characteristics: etiology of regurgitation, mechanism, severity, and consequences on heart chambers.
Key Concepts in Valve Assessment
Understanding the etiology of valve regurgitation is crucial.
Mechanism of Regurgitation
Primary Mitral Valve Regurgitation: Issues with leaflets, cords, or papillary muscles.
Secondary/Functional Mitral Regurgitation: Mitral valve itself is normal; problems arise from the left atrium (left atrial dilation —> annulus dilitation —> regurgitation) or left ventricle issues (ventricular remodeling, papillary muscle displacement). MV due to ischemia example: LCx/LAD CAD resulting in apical hypokinesis and apical/posterior displacement of papillary muscles (known as seagull sign). Chest XRT can also cause IIIa regurgitation and necessitate replacement.
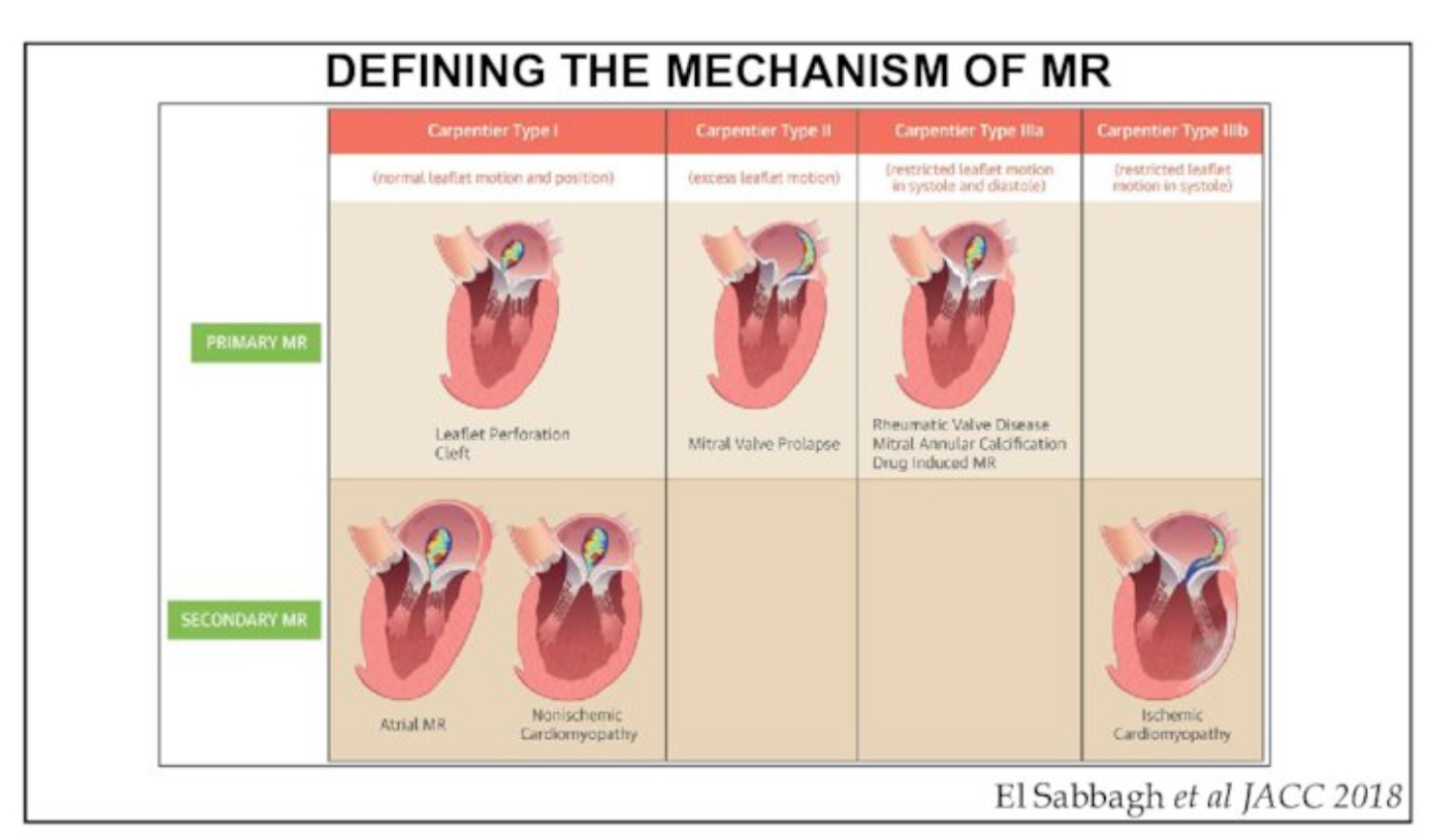
Carpentier Classification: Leaflet motion categorization to assess severity and mechanism.
Type I: Normal motion- potentially repairable
Type II: Excessive leaflet motion- highly repairable
Type III: Restricted leaflet motion (subdivided into IIIa and IIIb).
IIIa: systolic and diastolic - not repairable, requires replacement
IIIb: systolic only- medical therapy first, repair/replacement second line therapy
Detailed Echocardiographic Assessment
Three-Dimensional Imaging: Important for defining anatomical landmarks and identifying clefts associated with valve conditions.
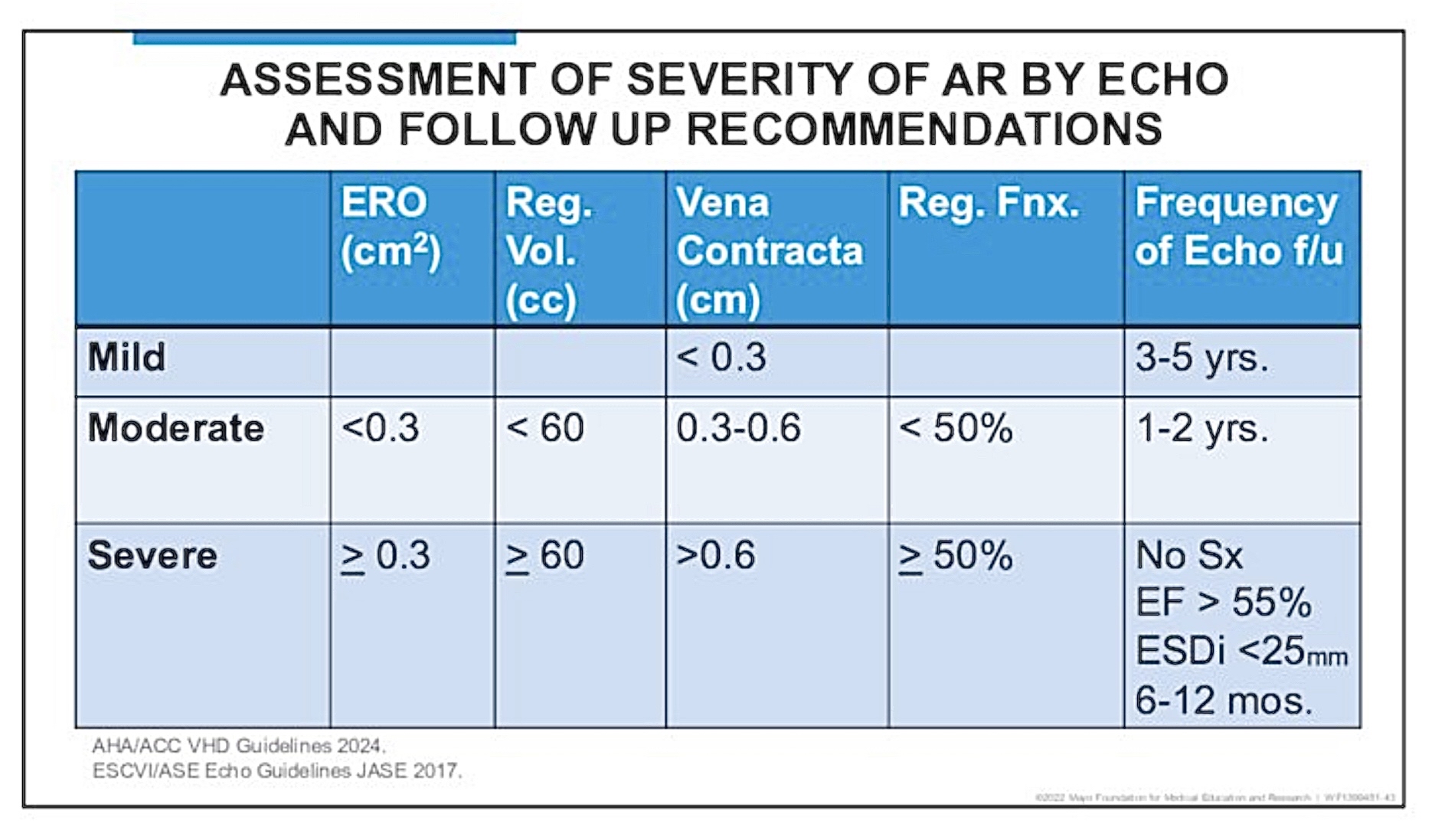
Assessing Severity of Mitral Regurgitation (MR)
Identifying severe MR using echocardiographic methods: left atrial size, left ventricle size, the presence of systolic flow reversals, and other echocardiographic indicators.
Quantitative Measurement: Proximal Isovelocity Surface Area (PISA) method recommended for accurate assessment of regurgitant orifice size.
Importance of careful imaging: zoom and adjust settings to enhance visualization of the regurgitation jets.
Tricuspid Regurgitation Assessment
Similar assessment method as MR, but tricuspid anatomy is more complex due to three leaflets.
Common Causes:
Primary (occurs in about 10% of cases)
Endocarditis
Trauma
Ruptured chordae
Inflammatory
Drugs/toxins
PPM lead
Congenital
Functional (about 90% of cases- no intrinsic abnormalities of the leaflets)
Left-sided heart disease
Pulmonary HTN
Right ventricular dysfunction
Atriopathy
Mechanisms:
RV remodeling
Papillary muscle displacement
Leaflet tenting or tethering
Annulus dilation
Evaluation: Consider evaluation of volumetric measurement of of RV. With disease processes like idiopathic FTR and pHTN FTR, the RV may elongate but width will be essentially the same.
Surgical vs. Percutaneous Options
Repairability of Valves: Different strategies based on leaflet motion type:
Type I: Potential for repair.
Type II: High likelihood of repair, especially if flail vestiges are present.
Type III: Often requires valve replacement.
Percutaneous Repair Devices:
MitraClip: For mitral valve.
TriClip: For tricuspid valve.
Recent developments in transcatheter valve replacements for patients unfit for open heart surgery.
Operational Considerations
Importance of pre-operative imaging to guide surgical or interventional approaches, ensuring adequate visualization of anatomy.
Necessity of communication between imaging specialists and interventionists to optimize procedures.
Conclusion
Summarized the essential elements of echocardiography for valve disease management to ensure informed decisions for interventions or surgeries.