DHY 207 Diagnostic Process
DHY 207
Diagnostic Process
Definition of the Diagnostic Process
- The process of diagnosis requires gathering information that is relevant to the patient and the lesion being evaluated
- This information comes from various sources
The Diagnostic Process
- Clinical diagnosis
- Radiographic diagnosis
- Historial diagnosis
- Laboratory diagnosis
- Microscopic diagnosis
- Surgical diagnosis
- Therapeutic diagnosis
- Differential diagnosis
Clinical Diagnosis
The strength of the diagnosis comes from the clinical appearance of the lesions
Observe, palpate, and document
Sometimes clinical diagnosis is all you need
T or F: Clinical diagnosis may be enough to diagnosis
True; Fordyce’s granules, torus palatinus, mandibular tori, melanin pigmentation, retrocuspid papillae
How does the lesion present?
Color
Shape
Location
History of lesion
Fordyce granules
Torus palatinus
Mandibular tori
Melanin pigmentation
Retrocuspid papillae
Fissured tongue
Geographic tongue
Median rhomboid glossitis
White hair tongue
Circumvallate papillae
Black hairy tongue











Clinical Diagnosis + Historical Information
Amalgam tattoo
Caused by fragment of amalgam that entered the oral mucosa

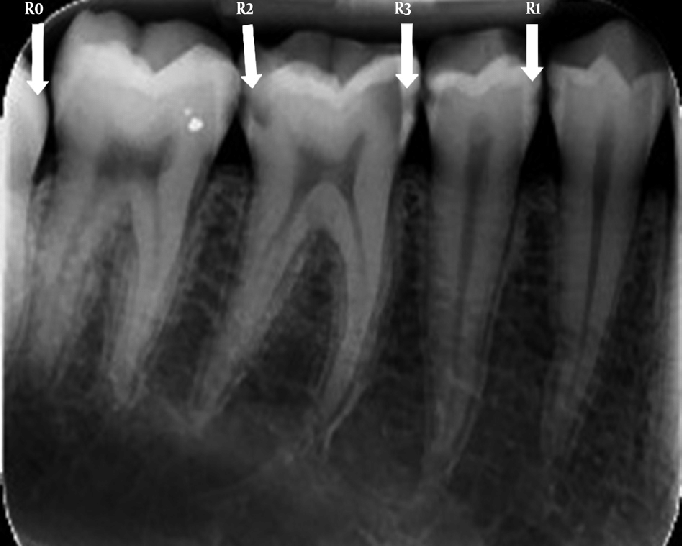
Radiographic Diagnosis
In a radiographic diagnosis, the radiograph provides sufficient information to establish the diagnosis
The presence of a fistula warrants a radiographic image
Fistula: Pus-filled pimple
Fistula is an infection and much be radiographed because the infection may reach the brain
Periapical pathosis: Acute or chronic inflammatory lesion around the apex of a tooth root, most commonly caused by bacterial invasion of the pulp of the tooth
External resorption
External PDL wants to meet pulp
Internal pulp wants to meet PDL
Caries
Compound odontoma
Looks like little teeth
“Odontoma” means benign tumor
Complex odontoma
Looks like a star explosion





Radiographic Diagnosis: Abnormalities
Supernumerary teeth
Medioden #8-9
Mesial molar
Impacted teeth
Calcified pulp



Radiographic Diagnosis: Normal Anatomic Landmarks
Nutrient canals
Permanent dentition coming in
Amalgam fragments and overhangs
Eyeglasses frames
Piercings
Retained metals such as shotgun pellets or shrapnel

Historial Diagnosis
Historial date constitute an important component in every diagnosis
Occasionally when historical data are combined with observation of the clinical appearance of the lesion, the historical information constitutes the most important contribution to the diagnostic process
Personal history
Family history
Amelogenesis imperfecta
Dentinogenesis imperfecta
Past and present medical and dental histories
Medical conditions such as ulcerative colitis
Drug history such as calcium channel blockers
Gingival overgrowth
Allergic reactions
History of surgical procedures
History of drug ingestion
History of the presenting disease or lesion


Laboratory Diagnosis: Blood Chemistries, Urinalysis, and Cultures
Radiographic appearance is a “cotton-wool effect” + elevated serum alkaline phosphatase level = Paget disease

Microscopic Diagnosis
Often the main component of the definitive diagnosis
Microscopic examination is of particular importance in the diagnostic process and therefore, although it is a form of laboratory diagnosis, it is discussed separately from laboratory diagnosis
Adequate tissue sample is necessary
Brush test can be used to obtain information from oral mucosal epithelium
A circular brush is used to obtain cells from the full thickness of epithelium
The results of this test may help determine whether a scalpel biopsy is needed to establish a definitive diagnosis
A white lesion cannot be diagnosed on the basis of clinical appearance alone
The microscopic appearance can vary from a thickening of epithelium to epithelial dysplasia, which can be premalignant
Oral cancer is most likely found on the lateral border of the tongue and the floor of the mouth
Red lesion is more likely to be cancer, not white
Surgical Diagnosis
Diagnosis is made using the information gained during the surgical procedure
Traumatic bone cyst
May appear as a radiolucency that scallops around the roots
When the lesion is opened surgically, an empty void is found
Lingual mandibular bone cavity (static bone cyst or Stafne bone cyst)
Surgical examination of the well-circumscribed, radiolucent area reveals salivary gland tissue entrapped during development
Cysts are always lined with epithelium cells
Stafne bone is a pseudocyst
Therapeutic Diagnosis
Nutritional deficiencies are common conditions to be diagnosed by therapeutic means
Angular cheilitis
May be associated with a deficiency of B-complex vitamins
Most commonly a fungal condition and responds to topical application of an antifungal cream or ointment such as Nystatin
Necrotizing ulcerative gingivitis (NUG)
Responds to hydrogen peroxide
Why? NUG is caused by anaerobic bacteria. Hydrogen peroxide brings oxygen to the anaerobic environment
Differential Diagnosis
That point in the diagnostic process when the practitioner decides which test or procedure is required to rule out the conditions originally suspected and to establish the definitive or final diagnosis
A differential diagnosis is a listing of the probable cause of a particular disease manifestation or group of manifestations
1.) Describe the abnormality in clinical terms
2.) Determine a list of diseases/conditions that present with similar manifestations
3.) Eliminate some of the possible causes already listed by adding other factors that could be involved with the abnormality (chronic health condition, medications, patient age, and whether the patient has an other manifestations that are inconsistent with any of the listed possibilities)
4.) Rank the remaining possible causes according to the probability they are the causative agent
5.) Decide what additional information might be necessary to eliminate more of the possibilities, such as blood tests, biopsy, diagnostic radiographs, cultures of oral microbes, and medical consultations
White lesions on tongue
1.) Measure & document location and appearance of lesion
2.) Ask how long it has been there
3.) Ask if they are biting their tongue
4.) Check if patient has malocclusion, broken restorations, or if they are clenching
5.) If none, come back in 2 weeks. If it’s still there then send out referral for surgical biopsy
Definitive Diagnosis
All elements of the differential diagnosis have been eliminated except one
Clinical appearance
Radiographic appearance
Response to therapy
Biopsy or laboratory test/cultures
Hygienists’ Role in DIfferential Diagnosis
Be observant
Collect data
Patient’s medical and dental health histories
History of lesion
Clinical description and evaluation
Biopsy and microscopy reports
Extra and Intraoral Examinations
Systematic sequence
Observe then palpate
Findings
Atypical
Pathologic
Traumatic
Infectious
Benign
Malignant
Others
Final Words
- Don’t assume something is atypical or a variation of normal unless you are 100% sure
- Explain your concerns to your patient, include them in a decision to refer for further diagnostic measures
- Follow-up on patients asked to return for a reevaluation of a lesion
- Must document everything
- Once in doubt, refer it out