homeostasis/thermoregulation/osmoregulation
Santa Maria College Year 12 Human Biology 2024
OBJECTIVE SHEET 3 – HOMEOSTASIS
HOMEOSTASIS OF BODY TEMPERATURE AND BLOOD GLUCOSE – Negative Feedback, Thermoregulation and Regulation of Blood Glucose Level
HOMEOSTASIS OF BODY FLUIDS AND GAS CONCENTRATIONS – Osmoregulation and Gas Concentration Regulation.
DISRUPTION TO HOMEOSTASIS – Diabetes, Dehydration and Excessive Water Intake
Human Perspectives ATAR Units 3 & 4 Chapter 5, 6 and 8
Creelman Exam Questions 2024 TBA
Course Objective & Description | Tick when done | ||||||||||||||||||||||
Homeostasis: procees of keeping the environment inside the body constant. | |||||||||||||||||||||||
1 | Describe the components of a feedback system – stimulus, receptor, modulator (control centre), effector, response, feedback (negative). Stimulus: a change in the environment. Receptor: the stimulus is detected by sensory cells. Message: sensory cells generates a message in the form of a nerve impulse of hormone. Modulator: a control centre processes the message receives from the receptor. Message: a new message is sent out by modulator. Effector: muscles or glands receives the message from the modulator. Response: the effector organ bring about an appropriate reaction. Feedback: response changes the orginal stimulus.
Aspects of internal environment: ▹ Core body temperature ▹ pH and concentration of dissolved substances in body fluids ▹ Concentration of glucose in the blood. ▹ Concentration of oxygen and carbon dioxide in the blood and other body fluids ▹ Blood pressure ▹ Concentration of metabolic wastes
Homeostasis Mechanism: work to maintain homeostasis: main sensory and controlling body systems: - Nervouse system: fast process - Hormonal system: slower *both operate through feedback systems.
Feedback loops: are cicurlar in which the body respond to a stimulus, with the response altering original stimulus. Can be negative or positive depending on whether the response decreases or increases original stimulus.
|
| |||||||||||||||||||||
Thermoregulation | |||||||||||||||||||||||
2 | Describe how heat is generated in the body. Gained from surrounding by conduction and radiation Heat from body processes (metabolism), especially respiration of liver and muscle cells. Radiation: transfer of heat from one object to another without direct contact: e.g. gain of heat when sitting in the sun or loss of heat from the body in a cold room. Conduction: heat transfers to another object through physical contact(energy passes fro molecule to molecule when in contact). E.g. placing hands in warm water to heat them up. - Body processes – metabolism (cell respiration and excerise. - Heat gained from the environment/ conduction/radiation. - Illness. - Increase in secretion of adrenaline from the adrenal medulla. - Stress or emotions. - Increased thyroxine levels. - Medications.
|
| |||||||||||||||||||||
3 | Describe how heat can be lost from the body. Radiation, conduction and convection to surroundings. Evaportation of water from skin and lungs; warm air breathed out; warm unrine and faeces. - Evaporation- water from the skin and lungs. - Warm air breathed out. - Voiding of warm urine and faeces. - Radiation of body heat to the cooler surroundings. - Heat loss to the environment- conduction and convection.
|
| |||||||||||||||||||||
4 | State that the normal body temperature of humans is approximately 36.70C. = homeothermic
cells function optimally at this temperature- increased body tmep acan cause nerve malfunction and change the structural integrity of protein and enzymes. - A constant body temperature is achieved by a balance between heat gain and heat loss. |
| |||||||||||||||||||||
5 | Describe the location of the thermoreceptors in the body (both peripheral and central).
Central: located in the hypothalamus – detects the temperature of the internal environment. Peripheral: located in the skin and in some mucous membranes – detects temperature changes in the external environment and sends this information to the hypothalamus. |
| |||||||||||||||||||||
6 | Describe how heat can be transferred by radiation, conduction and convection. Radiation: transfer of heat from one object to another without direct contact: e.g. gain of heat when sitting in the sun or loss of heat from the body in a cold room. Conduction: heat transfers to another object through physical contact(energy passes fro molecule to molecule when in contact). E.g. placing hands in warm water to heat them up.
Convection: flow of warm, less dense air upwards, which is replaced by cooler, more dense air. The faster the flow, the faster the cooling. E.g. electric fans help to move warm air away from our skin to be replaced with cool air. |
| |||||||||||||||||||||
7 | Explain how evaporation of sweat can lead to cooling the body. Heat is removed from the body when liquid is converted to a vapour.
It absorbs heat from the body, causing a cooling effect because of the process of changing from a liquid to a gas requires energy. |
| |||||||||||||||||||||
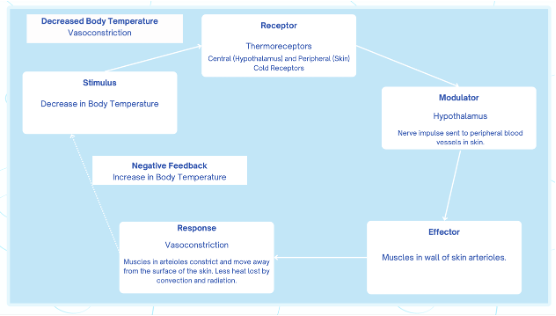
8 | Describe how the body responds to a fall in body temperature. (Include both physiological* and behavioural responses.) Physiological: The body starts to shiver and any blood vessels near the skin vasoconstrict. Increase in metabolic rate.
Behavioural: We wear thicker warmer clothes, take warm showers, decrease body surface area(by hudling in a ball), sit in front of a heater/fire. Increase activity.
|
| |||||||||||||||||||||
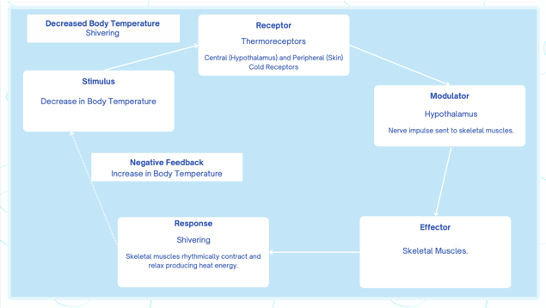
9 | Describe how the body responds to a rise in body temperature. (Include both physiological* and behavioural responses.) Physiological: The body starts sweatin increase heat loss by evaporative cooling, the blood vessels in the skins surface vasodilate- increasing heat loss vie radiation.
Behavioural: Wear less/lighter clothes, take cool shower, sit in shade, fan and reduce voluntary activity. Spreading out limbs(increasing body surface area.
|
| |||||||||||||||||||||
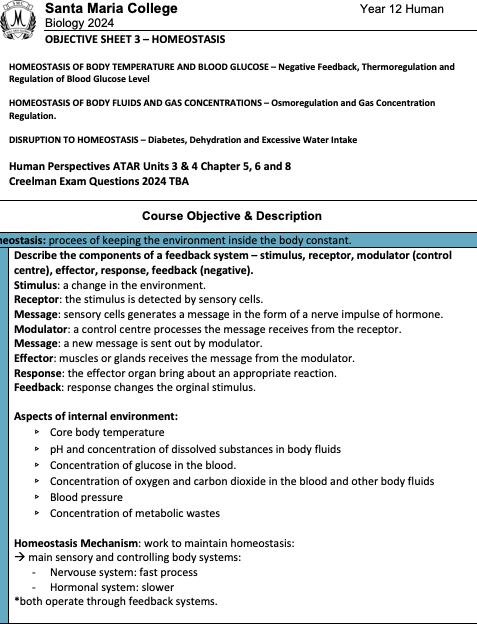
10 | Explain the terms vasodilation and vasoconstriction. Vasodilation: is the widening of blood vessels, allowing for increase blood flow .
Vasoconstriction: is the narrowing of blodd vessels, allowing for reduction of blood flow through the blood vessels.
|
| |||||||||||||||||||||
11 | Describe the relationship between the level of thyroxine and body temperature. ****** Thyroid hormone plays an important role in keeping bodily temperature stable when the outside temperature changes. In the cold, an increase in thyroid hormone leads to an increase in basal metabolic rate and heat generation. This is reversed in the heat |
| |||||||||||||||||||||
12 | Explain why piloerection is ineffective in humans as a means of preventing body temperature from falling:
As humans have relativel sparse body hair, especially in comparison to our early human ancestors or other mammals adapted to cold climates. The amount and thickness of body hair in huams are not sufficient to provide significant insulations against cold temperatures. The thin layer of body hair we possess does not provide enough insulation to significantly affect body temperature.
|
| |||||||||||||||||||||
Glucose (Blood Sugar) Regulation (Chapter 5 and Chapter 8) | |||||||||||||||||||||||
13 | Explain the relationship between glucose and glycogen. - Glycogen is storen in the liver and skeletal muscles. - Glucose is a simple monosaccharide. - Glycogen is broken down into glucose and glucose is created into glycogen. |
| |||||||||||||||||||||
14 | Explain the role of the liver in the regulation of blood sugar - Liver converts glucose into glycogen for storage. - Converts glycogen into glucose for release into the blood. - * most of the livers blood supply comes through the heptic portal, (brings blood directly from stomach, spleen, pancrease, and small and large instestines.
- The heptic portal vein carries the glucose to the liver.
Glucose may be: - Be removed from the blood by the liver to provide energy for liver functioning Be removed by the liver and/or muscles and converted into glycogen for storage - Continue to circulate in the blood, available for body cells to absorb and use as a source of energy (cellular respiration) - Be converted into fat for long-term storage it it is in excess of that required to maintain both normal blood sugar and tissue glycogen levels
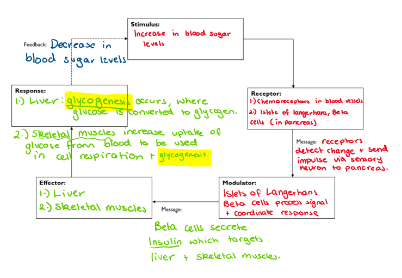
Glycogensis(lowers blood glucose levels(insulin)). Glucose into glycogen – storage in liver and skeletal muscle cells.
Glycogenolysis: rasies blood glucose levels (glucagon): glycogen into glucose – into the bloodstream.
Gluconeogenesis: raises blood glucose levels (glucagon): fats and amino acids into glucose – into the bloodstream. |
| |||||||||||||||||||||
15 | Describe the possible fate of glucose absorbed in the small intestine. Digestion (Breaking Down Carbohydrates into Glucose)
Absorption into the Bloodstream
Transport to the Liver via the Hepatic Portal Vein
Regulation by Insulin and Glucagon
Summary
|
| |||||||||||||||||||||
16 | Describe the regulation of blood sugar levels by the hormones insulin and glucagon*. Glucagon: raises blood glucose level: - Achieved though glycogenolysis and gluconeogensesis. - Insulin: lowers blood glucose level. - Achieved through glycogenesis, - Lipogenesis: promotes protein synthesis- requiring energy = blood glucose utilized. - Accelerating the transport of glucose from the bood into the body cells, especially those of the skeletal muscles. |
| |||||||||||||||||||||
17 | Define the following terms: glycogenesis, glycogenolysis and gluconeogenesis. - ‘genesis’ = to make/to begin - ‘lysis’ = to split apart/breakdown - Glycogenesis – to make glycogen (glucose --> glycogen) INSULIN - Gluconeogenesis – to make glucose from non- carbohydrate sources (amino acids --> glucose or fats --> glucose) GLUCAGON - Glycogenolysis – to breakdown glycogen (glycogen --> glucose) GLUCAGON
|
| |||||||||||||||||||||
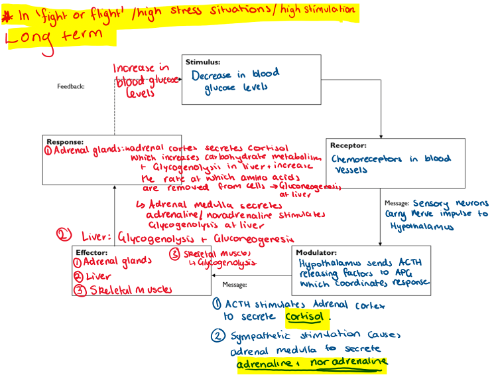
18 | Describe the effects of adrenalin and cortisol (a glucocorticoid) on blood sugar concentration. - The adrenal cortex, under the influence of ACTH produced by the anterior pituitary gland, secretes glucocorticoids- cortisol. - The adrenal medulla, under the control of the autonomic nervous system secretes adrenaline/noradrenalines.
Cortisol: is a glucocortiod. - Increases blood sugar levels. o Stimulates the conversion of glycogen into glucose(glycogenolysis) o Increases the rate at which amino acids are converted into glucose, in the liver (gluconenogenesis). o Proteins are broken down in the muscle cells and the amino acidsa are transported to the liver and converted into glucose. - Adrenalin increases blood sugar levels. o Stimulates the conversion of glycogen into glucose (gluconenogenesis). o Lactic acid is converted to the cells surface become more sensitive. |
| |||||||||||||||||||||
19 | Explain the term hyperglycaemia and the possible causes:
Hyperglycemia: abnormally high blood glucose level Symptoms: - Being excessively thirsty - Passing more urine - Feeling tired and lethargic - Always feeling hungry - Having cuts that heal slowly - Itching, skin infections - Blurred vision - Weight change (Type 1 – weight loss) |
| |||||||||||||||||||||
20 | Distinguish between diabetes type 1 and type 2 (Chapter 8 pages 207 - 209.)
|
| |||||||||||||||||||||
21 | Explain how gene therapy and synthetic hormones can be used to treat diabetes mellitus
TYPE 1 DIABETES
TYPE 2 DIABETES
|
| |||||||||||||||||||||
Osmoregulation (Chapter 6) | |||||||||||||||||||||||
22 | Distinguish between intracellular fluid, blood plasma and intercellular fluid (tissue fluid/interstitial fluid).
Intracellular Fluid (Cytosol)
Extracellular Fluid
Plasma
Intercellular Fluid (Tissue Fluid/Interstitial Fluid)
|
| |||||||||||||||||||||
23 | Explain how nutrients, wastes and water move between cytoplasm and vascular fluids. (Hint: explain the role of tissue fluid and the process of diffusion.)
Role of tissue fluid: - Tissue fluid surrounds body cells and acts as a medium for exchanging substances between capillaries (vascular fluids) and the cytoplasm of cells. - It forms when plasma leaks out of capillaries due to hydrostatic pressure and provides nutrients to cells. Nutrient movement (oxygen, glucose, amino acids, etc). - Oxygen and nutrients diffuse from capillaries into tissue fluid and then into cells following a concentration gradient. - Glucose and amino acids may also be transported by facilitated diffusion or active diffusion. Waste removal ( carbon dioxide, urea, etc): - Metabolic wastes like carbon dioxide and yurea move from cells into tissue fluids and then diffuse into capillaries, where they are transported for excretion. - Carbon dioxide diffuse into the blood, where it dissolves in plasma or binds to hemoglobin before being transported to the lungs. Water movement (osmosis): - Water moves by osmosis from areas of low solute concentration (tissue fluid) to areas of hugh solute concetration (inside cels or blood plasma). - The lumphatic systems help return excess tissue fluid to the bloodstream, preventing swelling (edema).
|
| |||||||||||||||||||||
24 | Define excretion and list the excretory structures and their products: Excretion:
|
| |||||||||||||||||||||
25 | Describe the structure of the nephron. |
| |||||||||||||||||||||
26 | Outline very briefly the processes involved in the formation of urine – filtration, selective reabsorption and tubular secretion.
Filtration
Selective Reabsorption
Tubular Secretion
|
| |||||||||||||||||||||
27 | Describe where in the nephron water reabsorption occurs |
| |||||||||||||||||||||
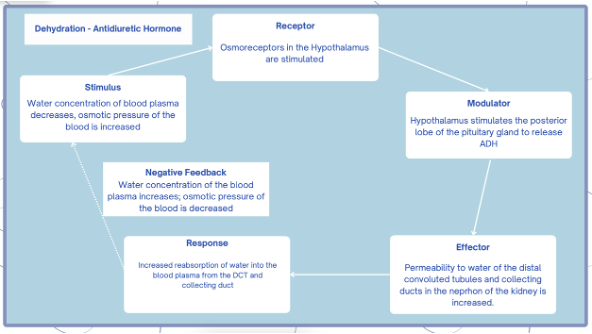
28 | Describe the role of ADH (antidiuretic hormone) in maintaining the water balance*.
|
| |||||||||||||||||||||
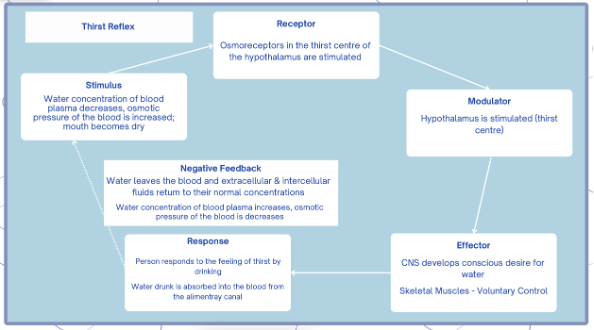
29 | Describe the role of the thirst reflex in maintaining the water balance: - Water concentration of blood plasma decreases; osmotic pressure of the blood is increased; mouth becomes dry - Osmoreceptors in the thirst center of the hypothalamus are stimulated - Person feels thirsty - Person responds to the feeling of thirst by drinking - Water drunk is absorbed into the blood from the alimentary canal - Water leaves the blood and the extracellular and intercellular fluids return to their normal concentrations |
| |||||||||||||||||||||
30 | Explain the causes and consequence of dehydration:
|
| |||||||||||||||||||||
31 | Explain the consequences of water intoxication.
|
| |||||||||||||||||||||
Gas Regulation (Chapter 6) | |||||||||||||||||||||||
32 | Write a word equation for cellular respiration. |
| |||||||||||||||||||||
33 | Name the muscles that are responsible for ventilation and name the nerves that stimulate them. |
| |||||||||||||||||||||
34 | Describe the relationship that exists between the concentration of CO2 in the plasma and the concentration of hydrogen ions (pH) - see equation page 140. |
| |||||||||||||||||||||
35 | Name the chemoreceptors that are stimulated when the oxygen concentration decrease dramatically. |
| |||||||||||||||||||||
36 | Describe how a very low concentration of oxygen in the blood can affect the breathing rate. |
| |||||||||||||||||||||
37 | Describe the regulation of carbon dioxide in the blood (and pH of blood plasma)*. |
| |||||||||||||||||||||
38 | Describe the difference between quiet and active breathing. |
| |||||||||||||||||||||
39 | Explain why it is dangerous to hyperventilate before swimming under water. |
| |||||||||||||||||||||
* Draw the appropriate feedback loop:
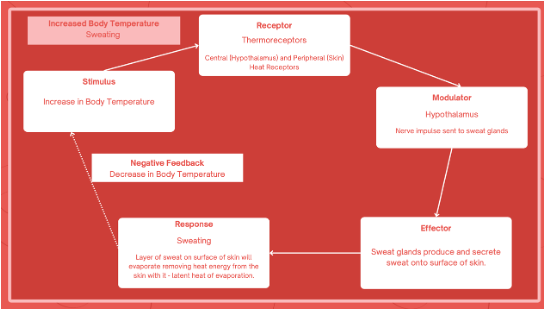
Thermoregulation - via vasoconstriction and vasodilation of surface arterioles, shivering, sweat production and adjustments to metabolic rate
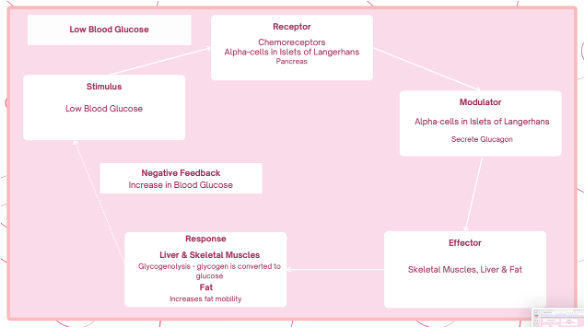
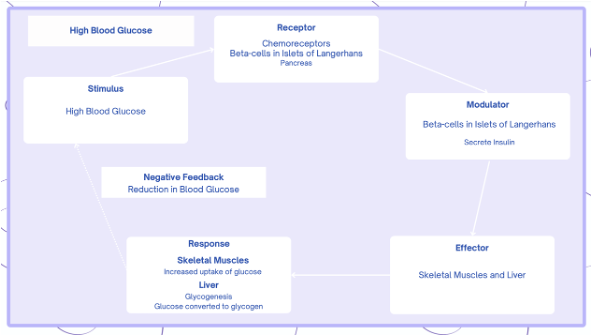
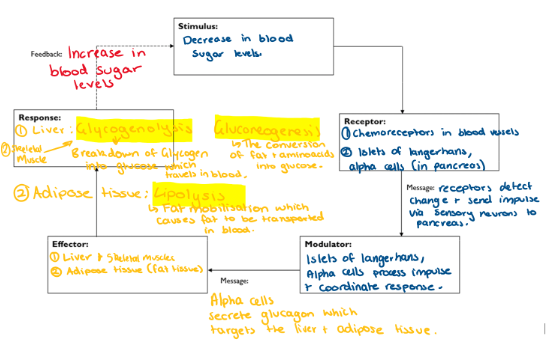
Blood glucose regulation – via insulin and glucagon
Osmoregulation – via ADH secretion and its influence on the volume and concentration of urine/ thirst reflex
CO2 regulation – via alterations to rate and depth of breathing
THERMOREGULATION:
BLOOD GLUCOSE REGULATION
OSMOREGULATION:
Extended response questions:
Explain how the nervous system and endocrine system work together to prevent body temoerature from falling below optimum levels in the short term (10 marks)
- Thermorecptors in the hypothalamus detect change of decrease in blood temperature.
- Peripheral thermoreceptors/ cold receptors in the skin send a nerve impulse to hypothalamus.
- Hypothalamus send nerve impulse through the autonomic division of the nervous system.
- To the skin which stimulate arterioles to constrict/vasoconstrict.
- To skeletal muscles that contract and relax rapid/shiver.
- To sweat glands to reduce production of sweat.
- Hypothalamus also stimulate the adrenal medulla
- via sympathetic nerves.
- Adrenal medulla secretes adrenalin and noradrenaline into blood.
- These hormone increase cell respiration/metabolism/heat production.
Describe the negative feedback loop for when the body is too cold:
- 1. Vasoconstriction (physiological response)
- 2. Hypothalamus (HT) receives messages from the cold receptors in the skin which then is sensed by the central receptors and the central receptors in the HT.
- Vasoconstriction causes less prevents heat loss by convection and radiation (P)
- 3. Sympathetic nerves (AUTONOMIC NS) cause the blood vessels to constrict / less blood flow to skin surface due to reduced blood vessel diameter.
- 4. Hypothalamus stimulates adrenal medulla to secrete adrenaline and noradrenaline into blood (again triggered by the sympathetic nerves)
- In turn causes increases cell metabolism – generate heat energy.
- 5. Shivering: hypothalamus targets skeletal muscles to contract / relax (muscle tone). Generate heat energy.
- 6. Over a longer period of time (several months in the cold) there is an Increase in production of thyroxine. HT causes the anterior lobe of the PG to secrete TSH which cause the thyroid to secrete more thyroxine to increase metabolic rate. This does not happen in the short term.
- Behavioural responses. Include: wearing thicker clothes, having a warm shower, sitting infront of a heater, by increasing voluntary activity, and decreasing surface area.
Describe the negative feedback loop for when the body is too hot:
- 1. Hypothalamus (HT) receives messages from the hot receptors in the skin which then is sensed by the central receptors and the central receptors in the HT.
- 2. Vasodilation: increase heat loss by radiation and convection triggered by the hot receptors (peripheral followed by central). Blood vessel muscles relax and diameter of blood vessel widen: increased blood flow and loss of heat by radiation and convection.
- 3. Sympathetic nerves (Autonomic NS) cause sweating and active periodic contraction of cells surrounding sweat ducts: latent heat of evaporation: describe.
- 4. In the long term there will be a decrease in metabolic rate, reduction in the secretion of thyroxine.
- Behavioural responses: body starts sweating, arterioles vasodilate, decrease in metablic rate, wear less clothes, have a cool shower, increase body surface area: spreading out limbs.
- 13 A person lost in the desert would suffer extreme dehydration. Although the thirst receptors would try to initiate drinking behaviour, the lack of available water would not allow this requirement to be met. Describe the mechanisms the body would employ to conserve water while getting rid of metabolic wastes.
- Answer: The person would be losing water through sweating but would be unable to replace that water. This means that the osmotic pressure of the blood would be raised. Osmoreceptors in the hypothalamus detect the increased osmotic pressure of the blood. The hypothalamus stimulates the posterior lobe of the pituitary gland to release ADH into the bloodstream. ADH affects its target organs, which are the nephron tubules in the kidney. The permeability to water of the distal convoluted tubules and the collecting ducts is increased. More water is then reabsorbed into the blood plasma from the tubules and ducts. This response will cause a dramatic decrease in the volume of urine produced and an increase in the concentration as less water is available to dilute the salts/wastes being excreted. Small quantities of highly concentrated urine will be produced.
-
- 14 A student made the following observations. On a very hot day, the volume of urine produced was small and it was dark in colour. On a cold day, urination occurred more frequently, and the urine was pale in colour. Explain these observations.
- Answer: On a very hot day, the student will sweat in order to cool the body and maintain homeostasis. This results in an increase in water loss from the body, which raises the osmotic pressure of the blood. More ADH will be released from the posterior pituitary. This causes the nephron to become more permeable to water, so water is retained in the blood and only small quantities of urine are produced. The urine would be dark in colour because the metabolic wastes are concentrated due to the excretion of less water.
- On a cold day, the opposite occurs. The student will not lose as much fluid through sweat. Less ADH will be released from the posterior pituitary. This causes the nephron to become less permeable to water, so water is retained in the collecting tubule and is lost as urine. It is light or pale in colour because the metabolic wastes are diluted by the larger volume of water being lost.