Chapter 17: Regional Injuries
Regional injuries — comprise injuries to various anatomical regions of the body having medicolegal significance and include injuries to the — head, neck, spine and spinal cord, chest, abdomen, limb bones, and joints.
17.1: Head Injury
- Head injury — a morbid state, resulting from gross or subtle structural changes in the scalp, skull, and/ or the contents of the skull, %%produced by mechanical forces%%.
Classification of Head Injuries
- Head injuries are basically classified into two types depending on the involvement of dura mater:
- Closed head injury — wherein dura mater is intact.
- Open head injury — wherein dura mater is torn.
Causes of Head Injuries
- They often result due to road traffic accidents (RTA), assaults, falls, etc.
- Blunt force trauma to the head with a non-penetrating object or from a fall, or the head striking a flat surface or a firm object can produce a closed head injury.
- The mechanical force, which produces a brain injury, usually produces injury of the scalp, and fractures of the skull.
- A fatal brain injury may be caused without any damage to the scalp or skull.
17.2: Scalp Injuries
- Scalp — the outermost covering of the head and is continuous with the skin of the face and has five layers from outside to inwards: %%skin, connective tissue, galea aponeurotica, loose areolar tissue, and pericranium.%%
- Brush abrasions are less common than in other sites because of the protective effect of the hairs, which also tends to prevent or blur the patterned effect of less severe impacts.
- Contusions:
- Black eye: This is a condition %%due to the bleeding in the soft tissue around the eye%% owing to blunt trauma of the forehead rupturing the blood vessels and the blood tracks along the facial attachments around the lower margin of the orbits.
- Spectacle hematoma: This is a condition in which the %%blood is collected in the soft tissue around the eyes%%, due to the fracture of the base of the skull – anterior cranial fossa fractures.
- Lacerocontused wound: A laceration of the scalp is usually a split laceration
Medicolegal Importance
- A scalp injury may be the only clue about a deep-seated fatal trauma, and it can also be of help in establishing the time since injury.
- Scalp lacerations bleed extensively, particularly in persons who are intoxicated, and in the appropriate situation may even result in death from exsanguinations.
- The possibility of tetanus however should always be considered.
- The scars they produce on healing will be designated and contain no hair.
- In the rare instances when they become infected, they may lead to the transfer of the infection through emissary veins into the superior sagittal (capital) sinus and more rarely into the cavernous sinuses.
17.3: Facial Injuries
- Facial injuries — comprise injury to the eyes, nose, ears, lips, and teeth.
- Facial injuries are usually prone to heavy bleeding as face is a highly vascular part of the body.
- Wounds of the face, which are more than skin-deep can cause disfiguration
- Penetrating injuries of the face are mostly fatal, particularly of the area where sense organs are present.
- Blindness is a common sequel of blows to face as retina is usually affected resulting in detachment of retina.
Injuries to the Eyes
- Lacerated wounds of the eye/s.
- Permanent injury to cornea, iris or lens.
- Vitreous hemorrhage
- Detachment of retina
- Rupture of retina
- Traumatic cataract
- Penetrating injuries to eyes or gouging out of the eyes by finger may prove fatal as this may set up meningitis.
- Black eye
Injuries to the Nose
- Commonest injury is biting or cutting off of the nose, out of enmity, vengeance, sexual jealousy or suspicion of infidelity of a woman.
- Left nostril may be injured in Indian female if the nose ring or stud is snatched.
- Left nostril may be injured in Indian female if the nose ring or stud is snatched.
- A blow on the head may cause nose bleeding (epistaxis) due to partial detachment of mucous membrane without any injury to the nose.
Injuries to the Ears
- Ears may be cut off or beaten off.
- A blow can cause rupture of the tympanum, resulting in permanent deafness.
- Severe blow can cause injury to labyrinth.
Injuries to the Lips
- A blunt force trauma such as a blow with a fist or any blunt weapon can result into contusions or lacerations.
- Sometimes lips are also cut in sexual jealousy.
Injuries to the Teeth
- With violence, there may be fracture or dislocation of teeth, with bleeding from sockets and contusion or laceration of the gums.
- A radiograph of the jaw may exhibit the fracture of the alveolar margin at the site of dental injury.
Injuries to the Facial Bones
- Blunt force trauma includes blow with blunt weapons such as stick, fist or by fall from height over the face which can bring about fracture of the facial bones such as:
- Nasal bones
- Ethmoidal bones
- Maxilla
- Malar bones
- A heavy blow on the jaw can drive the condyles against the base of the skull, producing a fissured fracture.
Medicolegal Importance of Facial Trauma
- Commonly facial injuries include-cutting nose, cutting of lips, cutting of ears, etc.
- Any injury resulting in permanent privation of eye sight of either eye, or hearing of either ear or/and fracture dislocation of tooth are considered as grievous hurt.
17.4: Skull Injuries
- Skull is a diploic bone having an outer table and inner table.
- The outer table is thicker and stronger, while the inner table is thinner and weaker.
- Diploe — the spongy bone in between the tables and gives greater elasticity to the bone.
- In children and babies the sutures have not united and thus there is even much larger lendency to give way between bones.
- Skull injuries — may involve the cranial vault, the base of the skull and the facial skeleton.
Factors of Skull Injury
- Violence Acting:
- Direct violence: Here the %%forces acting directly on the bone%% produce a fracture.
- Compression of head of the fetus
- Head getting crushed under the wheel of a moving vehicle in a road traffic accident.
- A moving object such as a stone or bullet strikes the head.
- Falls from a height onto the head.
- Kicking and stamping injuries.
- Repeated mutual punches.
- Indirect violence: Here the %%force is acting on the skull indirectly%%, through some other structures, which receive the primary impact.
- Fall on the buttocks or feet from a height, transmits the force through the vertebral column onto occipital bone and produces a Ring fracture around foramen magnum.
- Blast explosions of the face with the direction of the force coming from below.
- Heavy blows on the chin wherein the force is transmitted to the skull, leading to fracture of base of the skull.
- Site of Injury on the Skull:
- As the skull is a diploic bone with limited elasticity; the actual mechanism of skull undergoing fracture may be explained as follows:
- Initially due to the bone elasticity, only the outer table undergoes bending.
- Further increase in force results in fracture of the inner table first, which is weaker, followed by outer table ultimately.
- Age of the Victim:
- In infants and children: The skull is more elastic in infants and children. Hence it is less prone to fractures.
- In adults Skull: Bones are less elastic and compliant in adults. Hence, they are more prone to fractures.
- Sequence of Skull Injuries:
- Puppe’s rule: A later fracture does not cross a pre-existing fracture line but terminates on reaching the fracture line of the earlier fracture.
Classification of Skull Fracture
Fractures of the Vault of the Skull
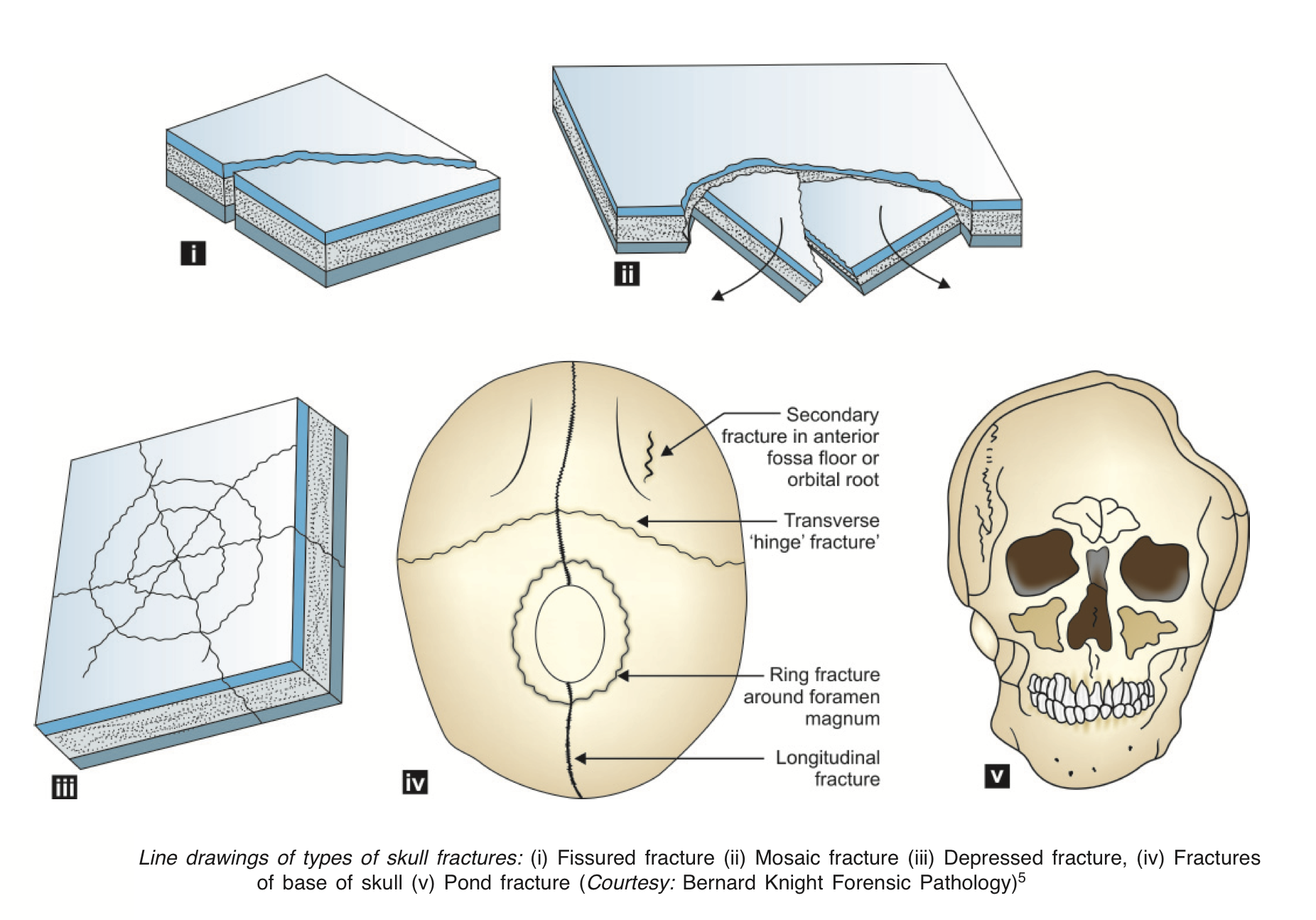
- Fissured Fracture — a linear fracture %%involving only outer or inner table or both tables simultaneously%%. Also called as crack fracture.
- Coup-fissured fracture – occurs when head is stationary.
- Contra coup-fissured fracture – occurs when the moving head strikes a stationary object.
- Bursting-fissured fracture – occurs on the vertex and may extend up to the base of the skull or vice versa, when the head is compressed between mechanical force on one side and a hard surface on other side.
- Depressed Fracture — a fracture wherein the fractured bone fragment is %%driven inwards%% for some distance below the rest of the adjacent skull's contour.
- Comminuted Fracture — a fracture, wherein the bone is %%broken into several pieces of different sizes%%, also known as crushed fracture.
- Stellate Fracture — a comminuted fracture with fissured fractured %%fragments radiating from it and held intact%%.
- Mosaic Fracture — a non-depressed comminuted fracture where fractured site appears in the form of several fissures %%forming a spider's web or cobweb or mosaic pattern%%.
- Elevated Fracture — a fracture, wherein %%one end of the fractured fragment is elevated above the surface of skull%%, while the other end may dip down into the cranial cavity and injure the dura mater of the brain directly.
- Diastatic Fracture — a fracture %%occurring along skull sutures%%, and occurs in children and young persons.
- Gutter Fracture — a fracture wherein the %%thickness of the skull bone is affected leading to an irregular depressed fracture%% of the inner table.
- Pond Fracture — a simple dent in the skull, which results from an %%obstetric forceps blade%%, or a blow from a blunt object or forcible impact against some protruding object.
- Perforating Fracture — an open fracture %%caused by a projectile%% (bullet) passing through the affected bone.
- Cut Fracture: A heavy cutting weapon can cause %%straight chops of the skull%%, involving either the outer table alone, or sometimes affecting both tables.
- Combined Fracture — fracture, wherein there is a %%combination of more than one%%.
Fracture of Base of the Skull
- Fracture of the Anterior Cranial Fossa — due to direct impact or as a result of contrecoup injuries, resulting in a black eye or escape of CSF and blood from the nose and damage to the roof of the orbit.
- Fracture of the Middle Cranial Fossa — due to direct impact behind the ears or crush injuries of the head resulting in escape of CSF and blood from the ear when the petrous part of the temporal bone is fractured.
- Fracture of the Posterior Cranial Fossa — due to the impact on the back of the head, resulting in escape of CSF and blood into the tissues of the back of the neck.
- Fracture around Foramen Magnum — fissured fracture occurring around the foramen magnum, situated 3 to 5 cm outside the foramen magnum at the back, the middle ear on either side and the roof of the nose anteriorly.
- Hinge Fracture — a fracture of the base of the skull where the fracture line runs from side to side across the floor of the middle cranial fossa, passing through the pituitary fossa in the midline following the course of least structural resistance.
Clinical Features of Fracture Skull
- Fracture of Anterior Cranial Fossa
- Bleeding – may be seen into the orbit, with swelling and purple discoloration around the eye (black eye/spectacle hematoma).
- CSF leaking – may be seen from the nose.
- Cranial nerve trauma – Injuries to any of the first six cranial nerves.
- Fracture of Middle Cranial Fossa
- Bleeding – may be seen through the ears.
- CSF leaking – may be seen through the ears.
- Cranial nerve trauma – Injuries to VII and VIII cranial nerves.
- Fracture of Posterior Cranial Fossa
- Bleeding or CSF leakage may/ may not be seen into the tissues of the back of the neck.
- Cranial nerve trauma – Optic nerve may be affected.
Complications of Fracture Skull
- Time since Injury of Skull Fracture: Also known as age of the skull injury is assessed by the changes during the healing stages of the fracture.
- Healing in Fissured Fracture: The edges are adjacent in this type of fracture and these edges begin to stick to each other within one week, calcification of inner table and rounding of the sharp fractured ends takes place by two weeks.
- Healing of Comminuted Fracture: The gap is filled up by fibrous tissue within 1 to 3 months' time depending on the size of the gap.
Injury to Meninges
- The meningeal membranes covering the brain inside the cranial cavity consist of the following:
- Dura mater — the strong and gray/bluish connective tissue membrane that is firmly attached to the skull, penetrated by bridging veins (emissary's veins) along the vertex.
- Arachnoid mater — a thin, vascular meshwork-like membrane beneath the dura.
- Pia mater — a surface network of glial fibers that are inseparable from underlying brain.
17.5: Traumatic Brain Injury
- Traumatic Brain Injury — brain injuries of traumatic origin, which happens to be the major cause of death among the population less than 45 years age.
- Severe TBI may be caused without any actual mechanical force or blow or fall on head.
Causes of Brain Injury
- Relative movements of the brain with skull: The falx cerebri, and the tentorium cerebelli, divide the cranial cavity into three compartments, which are relatively rigid structures and act in the same way as skull in resisting the movements of the brain and can result in brain injury.
- Penetrating wounds of the skull: Knife, bullet, etc. or fragments of skull in a depressed fracture can produce penetrating injury to brain.
- Fracture and distortion of the skull: When a localized segment of the skull undergoes deformation or indentation, shear strains may develop in the underlying, brain tissue resulting in a contusion in the surface layers of the brain tissue.
Mechanisms of Brain Injury
- Accelerating Injury: When a moving object hits the head, which is static, the skull picks up the momentum first and hits the brain, which is still at rest, yet to pick up the momentum a fraction of a second later.
- Decelerating Injury: When a non-moving object suddenly arrests the head in motion, the skull loses its momentum much prior to brain, which hits the inner aspects of the skull before becoming static.
- Shear Strain/Rotational Injury: This is due to side-to-side or rotational movement of the head, which makes the brain to get jolted on the sharp edges of the tentorial attachments in the interior of the skull and on the bony buttresses produced by the bones of the base of the skull and get injured.
- Coup Injury: Here the injury to skull and brain %%both occurs at the site of impact%%.
- Contrecoup Injury: Here the injury to skull and brain occurs on the opposite side of the site of impact.
Cerebral Concussion
- Cerebral concussion is a condition wherein there is %%a reversible or irreversible derangement of the neuronal activity without any demonstrable organic lesion in the brain.%%
- Reversible Cerebral Concussion: Here clinically the patient will %%present with loss of consciousness and flaccidity of muscles, followed by recovery of the consciousness, leading to a second loss of consciousness later%%.
- Lucid interval — the %%period of recovered consciousness between two bouts of unconsciousness%%.
- Irreversible Concussion — severe trauma can %%bring about brainstem damage%% resulting in fatality.
Medicolegal Importance of Cerebral Concussion
- Post-concussion syndrome – It is characterized by headache, dizziness, agitation, emotional problems and nervousness.
- Epilepsy: Severe head injury cases may develop post traumatic grand mal or focal epilepsy.
- Retrograde amnesia: Victim is %%unable to recollect the exact manner%% in which the injury occurred and even the events occurring before and after the accident.
- Punch-drunk syndrome — a %%syndrome of confusion in a setting of impaired physical function%% resembling Parkinson's disease. Usually caused by repeated blows to the head. It also resembles the condition found in chronic alcoholics.
- Drunkenness: A head injury victim may present with clinical manifestations, which resemble drunkenness (intoxication with ethanol).
- Alcohol and head injuries: A head injury sustained by a person, who has already consumed alcohol, usually creates great difficulty in assessing the relative importance.
Diffuse Neuronal Injury
- %%Neurons and nerve fibers sustain injury in a diffuse manner when the force of impact is transmitted through the brain.%% This may be wholly or partly reversible.
- Shear strains due to rotational movements are the probable cause for this.
Diffuse Axonal Injury (DAI)
- Diffuse axonal injury (DAI) — a clinical condition, which is one of the most common and devastating types of brain injuries occurring in almost half of all cases of severe head trauma.
- It is one of the major causes of unconsciousness and persistent vegetative state after head trauma.
- Severe sudden twisting or torqueing of the brain, as occurs in a sudden acceleration/deceleration – whiplash – accident, can stretch, twist, and damage these delicate axonal fibers — which causes DAI.
- In mild DAI, there is coma for 6 to 25 hours.
- In moderate DAI, there is coma for more than 24 hours, but there are no clinical signs of brain stem dysfunction.
- In severe DAI, there is coma of more than 24 hours with signs of brain stem dysfunction.
Cerebral Contusions
- Cerebral contusion — it is the %%bruising of the cerebral tissue%%. There may not be any apparent injury of the scalp or skull outside.
- Common injuries that can result in cerebral contusion are:
- Coup and contrecoup injuries
- Shear strain injuries
- Absorption shock waves
- Penetrating injuries
- Skull fractures
- Most commonly observed sites are:
- Frontal lobe contusions — commonly.
- Cerebellar and medullar contusion — observed often with coning or herniation of brain into foramen magnum.
Cerebral Laceration
- Cerebral laceration is %%tearing of the cerebral tissue%% and is usually found with cerebral contusion of several degrees.
- It could be of three types, wherein the lesion is:
- Superficial (gray matter alone is involved).
- Deep (white matter alone is involved).
- In the vital centers or ventricles.
- Clinical Features:
- Loss of consciousness predominantly.
- Bleeding from torn pial blood vessels
- Edema of the brain tissue
- Increased intracranial pressure
- Death when not properly treated
- Healing of cerebral lacerations is by gliosis.
Cerebral Irritation
- Cerebral irritation — includes a peculiar set of symptoms that may follow cerebral concussion, victim lies curled up in the bed, with face hidden beneath the clothes, resents all forms of interference and exposure to light.
- %%Patient is conscious and may become violent and abusive if disturbed.%%
- These symptoms disappear after a varying period with total recovery or may be followed by post-concussion syndrome symptoms.
Cerebral Compression
- Cerebral Compression — a clinical condition due to %%increased intracranial pressure%%, which disturbs the function of the brain.
- Formation of pressure over and around the brain stem, due to increase in intracranial pressure as a result of depressed fracture of the skull, foreign body, edema and hemorrhage are the common causes of cerebral compression.
17.6: Intracranial Hemorrhage
- Intracranial hemorrhage includes hemorrhage occurring within the cranial cavity.
- Fracture of the skull bones, though the common cause of intracranial hemorrhage, the hemorrhage can occur even without fracture of any of the skull bones, or in absence of any injury to the brain, but due to disease process or effects of trauma on the existing diseased area of the brain.
- Hemorrhage resulting directly from trauma usually occurs over the surface of the brain, but deep-seated hemorrhage can also occur in the cerebrum, cerebellum, or brain stem, due to trauma.
- The intracranial hemorrhage is usually accompanied by contusions or lacerations of the brain as a coup or contra-coup injuries.
- A single area of deep-seated intracerebral hemorrhage is usually due to some disease process other than trauma.
Brain Membranes
- Common causes of intracranial hemorrhages (ICHs) are as follows:
- Diseases like aneurysms, arteritis, blood disorders, neoplasm, etc.
- Trauma to the skull, brain or its membranes.
- Effects of injury upon already existing disease.
Classification of Intracranial Hemorrhage
- Intra-axial Hemorrhage — %%bleeding within the brain itself%%.
- Intraparenchymal hemorrhage: Bleeding %%within the brain tissue%%.
- Intraventricular hemorrhage: Bleeding %%within the brain's ventricles%%.
- Extra-axial Hemorrhage — bleeding that occurs %%within the skull but outside of the brain tissue.%%
- Extradural hemorrhage — %%caused by trauma, and results from laceration of an artery,%% most commonly the middle meningeal artery.
- Subdural hemorrhage — %%results from tearing of the bridging veins in the subdural space%% between the dura and arachnoid mater.
- Subarachnoid hemorrhage — %%result either from trauma or from rupture of aneurysms%% or arteriovenous malformations.
17.7: Extradural Hemorrhage
- Extradural hemorrhage — a type of intracranial hemorrhage, wherein the %%bleeding is outside the dura mater.%%
- It is common in adults. Normally in young adults, meningeal arteries are in close proximity to the skull bone.
Common Causes Encountered in Routine Medicolegal Practice
- Fracture of the temporal bone — especially the squamous portion can result in rupture of the middle meningeal artery or vein, leading to heavy bleeding into the temporal fossa.
- Fracture of the frontal bone — can result in rupture of the anterior meningeal artery or vein, leading to anterior cranial fossa hemorrhage, which in turn can press upon the frontal lobe.
- Fracture of the occipital bone — can result in rupture of the posterior meningeal artery or vein, leading to posterior cranial fossa hemorrhage, which can develop a large hematoma, which in turn can press upon the cerebellum and the occipital lobes.
- Fracture of the vault — can result in rupture of superior sagittal sinus or diploic veins and lead to hematoma formation.
Medicolegal Importance
- Victim may present with volitional activities immediately after the injury or prior to death.
- Victim may also present with Lucid interval.
- Victim may be confused for alcoholic intoxication and may be held in custody under drunkenness charge.
17.8: Subdural Hemorrhage
- Subdural hemorrhage — a type of intracranial hemorrhage wherein the %%bleeding is under the dura mater.%%
- It is common in children and old people. It is rarely found in a pure form. Usually, it is associated with subarachnoid hemorrhage.
Mechanisms
- Gliding movement between dura and arachnoid mater leading to overstretching and tearing of communicating veins traversing in the subdural space.
- Injury to the brain such in form to bruises/lacerations.
- In old age, any minor trauma due to sudden jerky movements of the head can lead to bilateral subdural hemorrhages.
- Spontaneous causes.
Classification
- Acute type — diagnosed only at autopsy.
- Subacute type — here the symptoms manifest after 2 to 14 days.
- Chronic type — here the symptoms are further delayed (after a few weeks or more).
Clinical Findings
- Unconsciousness (acute type)
- Ipsilateral pupillary disturbances
- Hemianopia (blindness on any one side)
- Mild headache (subacute type)
- Speech defect (subacute/chronic type)
- Urinary disturbance (subacute/chronic type)
Medicolegal Importance
- Chronic type can result in sudden natural death.
- Clinical symptoms may be mistaken for:
- Schizophrenia in young victims
- Presenile or senile dementia in elderly victims.
- Lucid intervals.
17.9: Subarachnoid Hemorrhage
- Subarachnoid hemorrhage — a type of intracranial hemorrhage wherein the %%bleeding occurs in the subarachnoid space.%%
Specific Causes and Mechanisms
- SAH of Traumatic Origin:
- All traumatic causes such as contusion or laceration of the brain, explosive blasts, strangulation, traumatic asphyxia, and damage to the vertebral arteries due to fracture of the upper cervical vertebrae as a result of blows across the neck from behind.
- Prolonged hyperextension of the neck as with special investigation such as bronchoscopy may result in rents in basal vertebral arteries.
- SAH of Spontaneous Origin
- Diseases like atherosclerosis and hypertension, leukemia, etc.
- Congenital defects like miliary aneurysms, and Berry aneurysms of basilar arteries, which rupture with mild trauma.
17.10: Intracerebral Hemorrhage
- Intracerebral Hemorrhage — a type of intracranial hemorrhage wherein the %%bleeding occurs in the cerebral tissue%%.
- It can occur due to violence alone or due to disease of the cerebral vessels. However, the various causes that can be enumerated are as follows:
- Rupture of berry aneurysms
- Intracerebral stress or impact (vascular tear)
- Coup injury
- Frontal impact resulting in expansion of the skull, which in turn can lead to separation of the brain ventricles.
- With cerebral contusion
- Movements of falx cerebri
- Skull fracture
- It is very essential to decide at autopsy whether the hemorrhage is post-traumatic or spontaneous (apoplexy).
17.11: Intraventricular Hemorrhage
- Intraventricular hemorrhage — a type of intracranial hemorrhage wherein %%bleeding occurs in the brain ventricles.%%
- An isolated form is very rare. It usually occurs with an extensive type of intracranial bleeding due to vascular malformation of the choroid plexus.
17.12: Pontine Hemorrhage
- Pontine hemorrhage — a type of intracranial hemorrhage wherein %%bleeding occurs in the pons or brain stem.%%
- It usually occurs in a person with high BP.
- Sometimes a natural intracranial hemorrhage in pons may precipitate on an accidental fall or traffic accident, and the resulting head injury makes it difficult to identify the nature of brain hemorrhage.
- Pontine hemorrhage could be spontaneous, severe pontine hemorrhage of single type, occupying one-third to half of the substance of the pons, or traumatic hemorrhage occurring in multiple separate foci which may unite to form a large area when the victim survives for a sufficient time.
- Primary hemorrhages in the brain stem are usually small and are seen in relation to the walls of the third and fourth ventricles and of the aqueduct.
- Hemorrhages in the rostra brain stem are usually more numerous and severe than those in the medulla resulting in rapidly fatal injuries.
17.13: Cerebral Edema
- Cerebral edema — occurs due to a localized or diffuse %%abnormal accumulation of water and sodium, which increases the volume of the brain.%%
- It is caused due to:
- Increase in the intravascular pressure
- Increased permeability of the cerebral vessels, and
- Decrease in plasma colloid osmotic pressure.
- Focal edema is almost invariably associated with and secondary to contusions and lacerations of the brain.
- Focal edema in the brainstem is usually fatal.
- Generalized cerebral edema occurs with diffuse brain injury.
Cause of Death in Head Injuries
- Most deaths are due to damage to vital cerebral areas, located around the posterior hypothalamus, midbrain, and medulla. Usually, respiratory failure or paralysis is followed by permanent cardiac arrest.
- Vital centers may be compressed or concussed directly or they may be injured by secondary changes.
- Another mechanism is markedly raised intracranial pressure.
- Other causes of death are infections, hypostatic pneumonia, pulmonary embolism and renal infection.
17.14: Spine and Spinal Cord Injuries
- Concussion of spinal cord:
- Railway spine — is a condition wherein the victim develops %%transient paralysis without loss of sexual power.%%
- Whiplash injury: Occurs with a severe blow to the chin from below with a hand or blow on the brow by dashing the windscreen of a car resulting in hyperextension of the head, producing dislocation at C4-C6 levels.
- Shaken Baby Syndrome — a trauma %%suffered by small children as the result of deliberate abuse%%.
- Compression of the spinal cord: It is usually due to fracture dislocation, usually at levels such as C4-C6, T3-T6, T10-L3, etc.
- The victim may die in 24 hours or survive with permanent paralysis.
- Pithing — It is killing by pushing a fine needle into the nape of the neck between the base of the skull and the first cervical vertebra and is a concealed punctured wound.
- Laceration of Spinal Cord: Twisting the neck can lead to laceration of spinal cord, which in turn can lead to death without evident external injury.
- Common in killing unwanted children.
- This can happen in wrestling.
- Firearm injury may also cause spinal laceration even when the missile has not entered the cord, but just has brushed the neck.
17.15: Injuries to Neck and Neck Sutures
- Scratches and bruises — as occurring with asphyxial death namely, the ligature mark of hanging, strangulation, etc., and the nail markings of throttling.
- Injury to the hyoid bone — this is usually a fracture of the greater cornu at the junction of the outer with the inner two-thirds.
- Lacerations of the neck and its structures: In contrast to an abrasion, none of the skin is missing. A cut is commonly conceived of as a wound caused by a sharp object, such as a shard of glass. Lacerations are commonly caused by blunt trauma.
- Incised wounds of the neck or throat — Cutthroat wounds are common in the neck with sharp weapons. They could be homicidal or suicidal.
17.16: Injury to Chest and Thorax
- Motor vehicle collisions (MVC) represent the most common cause of major thoracic injury among emergency department (ED) patients.
- Increased mortality and morbidity are associated with multiple rib fractures, increased age, and higher injury severity scores.
Various types of chest injuries encountered in routine medicolegal practice:
- Concussion of the chest can lead to death.
- Contusion of the chest resulting in pleurisy or pneumonia or tuberculosis.
- Fracture ribs commonly 4th to 8th ribs are involved and called knobbing fractured ribs.
- Flail chest injury wherein multiple bilateral rib fractures are seen.
- Injury to lungs such as bruising, laceration, stab wounds, etc.
- Injury to the heart due to blunt/and sharp force trauma, namely:
- Buckled sternum
- Bruising/crush injury/rupture/avulsion of heart.
- Cardiac tamponade/hemopericardium
- Injury to major blood vessels like the aorta/pulmonary artery/inferior vena cava (IVC), etc.
- Injury to trachea and esophagus.
17.17: Abdominal Injuries
- Various types of abdominal injuries encountered in routine medicolegal practice are:
- Incised wounds, which could be non-penetrating or penetrating, lead to death due to shock, hemorrhage, sepsis, or injury to vital organs such as the liver, spleen, pancreas, kidneys, etc.
- Blunt injuries such as contusions or lacerations of viscera such as the stomach, intestines, pancreas, liver, spleen, etc.
- Probable causes could be:
- Blows/ kicks over the abdomen
- Fall on a pointed object
- Stab injuries,
- Road traffic accident injuries,
- Crush injuries, and more.
- Complications could be immediate or remote, which could be any one of the following:
- Hemorrhage
- Peritonitis
- Sepsis
- Vagal inhibition, etc.
- Death due to any of these complications when not treated properly.
17.18: Limb Skeletal Bone Injuries
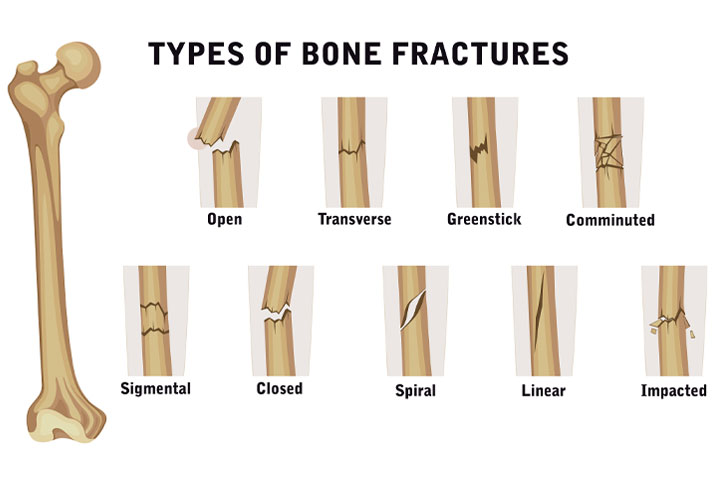
Types of Bone Fractures
- Closed or open (compound):
- Closed fractures are those in which the skin is intact;
- Open (compound) fractures involve wounds that communicate with the fracture and may expose the bone to contamination.
- Simple or multi-fragmentary (formerly comminuted)
- Simple fractures are fractures that %%occur along one line%%, splitting the bone into two pieces;
- Multi-fragmentary fractures involve the %%bone splitting into multiple pieces%%.
- Compression fracture: An example of a compression fracture is when the front portion of a vertebra in the spine collapses due to osteoporosis, a medical condition that causes bones to become brittle and susceptible to fracture.
- Other types of fracture:
- Complete fracture: A fracture in which bone fragments %%separate completely%%.
- Incomplete fracture: A fracture in which the bone fragments are still %%partially joined%%.
- Linear fracture: A fracture that is %%parallel to the bone's long axis%%.
- Transverse fracture: A fracture that is at a %%right angle to the bone's long axis.%%
- Oblique fracture: A fracture that is %%diagonal to a bone's long axis%%.
- Compression fracture: A fracture that usually %%occurs in the vertebrae%%.
- Spiral fracture: A fracture where at %%least one part of the bone has been twisted%%.
- Comminuted fracture: A fracture causing %%many fragments%%.
- Compacted fracture: A fracture caused when %%bone fragments are driven into each other%%.
- Open fracture: A fracture when the %%bone reaches the skin%%.
- Bug fracture: A fracture when the %%bone is in place, but the fracture has the appearance of a crushed insect%%.
- Special Considerations for Children
- Greenstick fracture: Occurs because the bone is not as brittle as it would be in an adult, and thus does not completely fracture, but rather %%exhibits bowing without complete disruption of the bone's cortex%%.
- Salter-Harris fractures — growth plate injuries that require careful treatment and accurate reduction to make sure that the bone continues to grow normally.
- Plastic deformation of the bone, in which the bone permanently bends but does not break, is also possible in children.
- Joint injuries — include dislocation, sprain, punctured/incised/ lacerated wounds.
- Fractures of bones or dislocations of joints are grievous hurt.