Cardiovascular Anatomy and Physiology
19.1-Heart Anatomy
Where is the human heart located? Describe the structure surrounding the heart in the mediastinum. | 1) Within the thoracic cavity between the lungs in the space known as the mediastinum. 2) The pericardium/pericardial sac surrounds the heart to separate it from other mediastinal structure. It has it’s own space known as the pericardial cavity. |
Where is the dorsal surface of the heart located? The anterior surface? The base? The inferior tip? | 1) Near the bodies of the vertebrae. 2) Sits deep to the sternum and costal cartilages. 3) At the level of the third costal cartilage. 4) Left of the sternum between the junction of the fourth and fifth ribs near their articulation with the costal cartilages. It is also known as the apex. |
What is the cardiac notch? | A depression in the medial surface of the superior lobe of the left lung that exists because the heart is there. |
What are the dimensions of the heart? What can its size be compared to? What is its mass for both males and females? | 1) 12 cm in length, 8cm in width, and 6 cm in thickness. 2) A pinecone. 3) F:250-300 grams; M:300-350 grams. |
What is hypertrophic cardiomyopathy? | An abnormally enlarged heart muscle for no apparent reason. Can cause unexplained death in otherwise healthy people. |
How is cardiac muscle affected by exercise? | Like the skeletal muscle, it grows larger and stronger with exercise (CELLS NOT NUMBER OF CELLS), this is normal and healthy unlike cardiacmyopathy. This is known as hypertrophy. |
What are the atria? The ventricles? | 1) The chambers that receive blood from either the systemic circuit or the pulmonary circuit. 2) The ventricles are the chambers that pump the blood into the systemic or pulmonary circuit. |
What are the systemic and pulmonary circuits? | 1) Transports oxygenated blood to the tissues of the body, returns deoxygenated blood to the right atrium. 2) Transports blood from the right ventricle to the lungs and from the lungs to the left atrium. |
What is the pulmonary trunk? What are the pulmonary arteries? What are the pulmonary capillaries? | 1) The blood vessel that takes blood from the right ventricle to the lungs. It bifercates into the pulmonary arteries. 2) Branches of the pulmonary trunk that carry the blood to the lungs, left goes to left lung, right goes to right lung. 3) The capillaries in which gas exchange in the lungs occurs. |
What are the superior and inferior venae cavae? | The two major veins of the systemic circuit. The superior drains deoxygenated blood from above the diaphram and the inferior drains deoxygenated blood from below the diaphram. |
What are the septa of the heart? | A wall of partition that divides the heart into chambers. |
What is the interatrial septum? What is the interventricular septum? How are they different? | 1) A septum located between the two atria. 2) A septum found between the two ventricles. 3) Location, the interventricular septum is thicker due to the greater pressure excerted by the ventricles. |
What is the fossa ovalis? What is the foramen ovale? | 1) An oval shaped depression that is a remnent of the foramen ovale. 2) An opening in the fetal heart that allowed blood to pass directly between the right and left atria. |
What is the septum primum? | 1) A flap that previously acted as a valve that closes the foramen ovale after birth. |
What is the atrioventricular septum? What valves are found in it? | 1) The septum between the atria and the ventricles. 2) The atrioventricular and semilunar valves. |
What do valves do? | Valves are specialized structures that ensure the one way flow of blood. |
What are the atrioventricular valves? What are the semiluanr valves? | 1) The valves between the atria and the ventricles. 2) The vales that lead to the aorta or the pulmonary arteries. |
What is the cardiac skeleton? | Dense conective tissue that reinforces the heart due to weakness cause by valves. It also serves as a barrier in the heart electrical conduction system. |
What does the right atrium do? | Serves as a receiving chamber for blood returning from the systemic circuit, and sends said deoxygenated blood to the right ventricle. |
What blood vessels send blood to the right atrium? | The superior and inferior vena cavae, and the coronary sinus (which brings blood from the myocardium). |
Where do the superior and inferior vena cavae drain blood from? | 1) Regions above the diaphragm. 2) Regions below the diaphragm. |
What are pectinate muscles? | Ridges of muscle found on the anterior surface of the right atrium and the auricles. |
What is the tricuspid valve? | The valve that allows blood to flow from the right atrium to the right ventricle. |
What are the cordae tendineae? | The strong strands of connective tissue found in the heart, also known as heart strings. |
What do the chordae tendineae connect the flaps of the tricuspid valve to? | To one of the three pappilary muscles found in the right ventricle (the anterior, posterior, and septal muscles). |
How do valves stop blood from flowing from one chamber to another unintentionally? | The contraction of the myocardium causes tension to be applied ot the chordae tendineae which stops the flaps from being forced into the other chamber. |
What are the trabeculae carneae? | Ridges of the cardiac muscle covered by endocardium. |
What is the moderator band? | A cardiac muscle that reinforces the thin walls of the right ventricle and plays a crucial role in cardiac conduction. |
Where does the right ventricle send blood? | Into the pulmonary trunk, which then follows the various vessels of the pulmonary circuit to the lungs. |
Where does the left atrium receive blood from? | It recieves oxygenated blood from the lungs that returns to it via one of the four pulmonary veins. |
Does the left atrium have pectinate muscles? Pectinate ridges? | 1) No. 2) Left auricle. |
How many papillary muscles does the left ventricle have? The right? | 1) 2. 2) 3. |
Does the left ventricle have a moderator band? | No, but the right ventricle does. |
How are the left atrium and ventricle separated? Is this valve bicuspid or tricupsid? | 1) By the miatrial valve. 2) Bicuspid. |
Where does the left ventricle send blood? | To the systemic circuit, through the aorta via the aortic semilunar valve. |
How many flaps do bicuspid valves have? Tricuspid? | 1) 2 flaps. 2) 3 flaps. |
What type of valve is tricuspid? What chambers does it separate? | 1) Right atrioventricular valve. 2) The right atrium and the right ventricle. |
Why is the right atrioventrilar valve tricuspid while the miatrial vale is bicuspid? | The main reason for this lies in the embryonic development. During the embryonic development blood flows from the right atrium to left atrium through foramen ovale and from atrium to ventricle via atrioventricular channel. |
What is the pulmonary semilunar valve? What is it also known as? Is it bicuspid or tricuspid? Does it make an audible sound? | 1) The valve that separates the right ventricle from the pulmonary trunk. 2) Pulmonary valve. 3) Tricuspid. 4) Yes, it is S2. |
What is the aortic semilunar valve? What is it known as? Is it bicuspid or tricuspid? Does it make an audible sound? | 1) The valve that separates the left ventricle and the aorta, prevents aortic backflow. 2) Aortic semilunar valve. 3) Tricuspid. 4) Yes, it is S2 in addition to the pulmonary seimilunar valve. |
What causes the right atrioventricular and mitral valves to close? | During ventricular systole, pressure in the ventricles rises, which send a little bit of blood back into the atria which closes the valves. Then, the chordae tendineae hold the valves closed. |
How do the aortic and pulmonary semilunar valves close? | A little bit of bloood flows into the blood vessels to close the valves, but they don’t have chordae tendoneae. They are kept closed by connective tissue in the walls of the endocardium. |
What do the coronary arteries do? | They supply blood to the heart, specifically the myocardium. |
What are epicardial coronary arteries? | Coronary vessel branches that remain on th e surface of the artery and follow the sulci. |
What are the sinuses? Where are they located? Do they give rise to blood vessels? | 1) Dilations in the wall of the aorta just above the aortic semilunar valves. 2) The first and second give rise to the left and right coronary arteries. |
What is the circumflex artery? | A coronary artery that arises from the left coronary artery and follows the coronary sulculus to the left. It eventually fuses with the small branches of the right coronary artery. |
What does LAD stand for? What is it? What is it also known as? | 1) Left Anterior Descending artery. 2) The second branch arising from the left coronary artery that follows the anterior interventricular sulcus around the pulmonary trunk. 3) Interventricular artery. |
What is an anastomosis? Are there a lot in the heart? What are the consequences of this? | 1) An area where blood vessels form an alternate path to certain tissues in case a blood vessel is blocked. 2) The anatomosis in the heart are very small. 3) This makes it so that a coronary artery blockage results in a myocardial infarction. |
What does the right coronary artery distribute blood to? | The right atrium, portions of both ventricles, and heart conduction system. |
What do the marginal arteries supply blood to? | The superficial portions of the right ventricle. |
What does the posterior interventricular artery do? What gives it rise? What is it also known as? | 1) It runs along the posterior portion of the interventricular sulcus toward the apex of the heart, giving rise to branches that supply the interventricular septum and portions of both ventricles. 2) The right coronary artery. 3) The posterior descending artery. |
What are coronary veins? Where is the great cardiac vein located? What artery does the great cardiac vein parallel? | 1) Blood vessels that drain the heart. They are generally parallel to the larger surface arteries. 2) It follows the interventricular sinus, and eventually flows along the coronary sulculus to the coronary sinus on the posterior surface. 3) The anterior interventricular artery. |
What are the branches of the great cardiac vein? What arteries do they parallel? | 1) Posterior cardiac vein-marginal artery branch of the circumflex artery. 2) Middle cardiac vein-posterior interventricular artery. 3) Small cardiac vein-right coronary artery, drains the posterior surfaces of the right atrium and ventricle. 4) Anterior cardiac veins-small cardiac arteries. |
Why is the anterior cardiac vein different from the other cardiac veins? | It bypasses the coronary sinus and drains directly into the right atrium. |
What is the coronary sinus? | A large thin-walled vein on the posterior surface of the heart lying within the atrioventricular sulcus. It empties directly into the right atrium. |
19.2-Cardiac Muscle and Electrical Activity
Question | Answer |
What is autorhythmicity? | The ability of cardiac muscle tissue to initiate an electric potential that causes the myocardium to contract at a regular rate. |
In addition to autorhythmicity, what regulates the heart rate? | The endocrine and nervous systems. |
What are the two main types of cardiac muscle cells? | Myocardial contractile cells and myocardial conducting cells. |
What do myocardial contractive cells do? | Make up 99% of the cells in the atria and ventricles. They conduct impulses and are responsible for the contractions that pump blood through the body. |
What do myocardial conduction cells do? | Initiate and propagate the action potential/electrical impulse that triggers contractions of the myocardial contractile cells. |
What are Purkinje cells? | A type of myocardial conduction cell that are larger than myocardial contractile cells. |
How are cardiac and skeletal muscles similar? | The contractile elements are essentially the same. |
How are cardiac and skeletal muscles different? | Cardiomyocytes are smaller, and there are half as any T Tubules. |
What are T Tubules? | Also known as transverse tubules, they allow electrical impulses to reach the interior of cardiomyocytes. |
What are cardiomyocytes? | Cardiac muscle cells. |
What is the junction between two cardiomyocytes? What does it do? | An intercalated disc, which supports syncronized contraction. |
Why is it important intercalated discs are strong? | Due to the forces applied during contraction. |
Describe the contractions of the heart. | Cardiomyocytes undergo twitch-type contractions with long refractoroy periods, followed by a brief pause. |
Why is it important for the contraction of cardiomyocytes to have a long refractory period? | In order to prevent the possiblity of tetany (a condition in which the muscle remains involuntarily contracted-not compatible w/life in the heart). |
How do myocardial conduction cells set the heart rate? | The cell with the fastest electrical impulses sets the pace. |
What are the components of the cardiac conduction system? | Sinoatrial node, atrioventricular node, atrioventrivular bundle, the atrioventricular bundle branches, and the Purkinje cells. |
What is the sinoatrial (SA) node? What does it do? | 1) A specialized clump of myocardial conducting cells located in the superior and posterior walls of the right atrium near the opening of the superior vena cava. 2) Establishes normal cardiac rhythm. |
What is the sinus rhythm? | The normal electrical pattern followed by the contraction of the heart. |
What does polarization and depolarization mean in the context of the heart? | Polarization-cardiomyocytes relax after contraction. Depolarization-cardiomyocytes contract. |
How do electrical impulses spread from the sinoatrial node throughout the atria? Which node do the impulse reach next? | 1) Via specialized internodal pathways. 2) Atrioventricular node. |
What is Bachmann’s bundle? What is it also known as? | 1) A specialized pathway that carries electrical impulses from the right atrium to the left atrium. 2) Interatrial band. |
What prevents electrical impulses from reaching the ventricles in a way that’s not the atrioventricular node? | The connective tissues of the cardiac skeleton. |
What is the atrioventricular node? | A second clump of specialized myocardial conductive cells, located in the inferior portion of the right atrium within the atrioventricular septum. |
What does the atrioventricular node do? | Transmits the impulse to the ventricles. |
What causes the pause as the atrioventricular node transmits the impulse to the ventricles and why is it important? | 1) The small diameter of the nodal cells, and the fact that conduction between nodal cells is less efficient than conduction between conduction cells. 2) Allowst he atria to pump the blood into the ventricles before they contract and send the blood elsewhere. |
Where does the atrioventricular bundle arise and what is it also known as? | 1) The atrioventricular node. 2) bundle of His. |
What do the left atrioventricular bundle branches do? Why is it larger than the right? | 1) Transmits the impulse to the left ventricle. 2) The left ventrical is larger than the right ventricle. |
What does the right atrioventricular bundle branch do? | Supplies the right ventricle with the impulse. |
Why do the right papillary muscles contract just before the remaining myocardial contractile cells? | Portions of the right atrioventricular branch are found in the moderator band (which supplies the right papillary muscles). |
What are Purkinje fibers? What do they do? | Additional conductive fibers that spread the electrical impulse to the myocardial contractile cells in the ventricles. |
Where does Purkinje fiber driven contraction start? Why is this important? | 1) The apex of the heart. 2) Allows blood to be pumped out of the ventricles into the aorta and pulmonary artery. |
How do electrolytes affect the contraction of the heart? | They form a electrical gradient across the heart which then causes spontaneous/prepotencial depolarization and then depolarization. |
What does Na+ do to the heart in terms of contractions? | Causes prepotencial/sponatneous depolarization. |
What does Ca2+ do to myocardial conductive tissues of the heart? | Causes depolarization (contraction). |
What does K+ do to the myocardial conductive tissues of the heart? | Causes repolarization (relaxation). |
What is the electrical pattern concerning the contractile cells? | Rapid depolarization followed by a plateau phase, and lastly repolarization. |
What does Na+ do to the contractile cells? | Causes rapid depolarization. |
What does Ca2+ do to the contractile cells? | Allows the plateau to occur. |
What does K+ do to the contractile cells? | Causes repolarization. |
What is the order of the nodes from fastest to slower? | Sinoatrial node, atrioventricular node, and finally the Purkinje fibers. |
How do electrocardiograms work? | Electrodes that measure cardiac electric impulses are placed on the body of the patient. Said electrodes then amplify the impulses so they can be better measured. |
What does normal metabolism in the heart entail? | Typical gas exchange, which typically gives the heart enough oxygen. |
19.3-The cardiac cycle
Question: | Answer: |
What is the cardiac cycle? | The period of time that cbeings with the contraction of the atria and ends with ventricular relaxation. |
What is the diastole? | The period of relaxation as the chambers fill with blood. |
What is the systole? | The period of time in which the heart contracts in order to pump blood into circulation. |
Why does blood flow from the atria into the ventricles during the atrial systole? | Because pressure is lower in the ventricles, and fluids move according to pressure gradients. This is the same reason why blood flows from the ventricles to the pulmonary trunk or aorta during the ventricular systole. |
How does blood enter the right atrium? The left? | 1) Via the superior and inferior vena cavae and the coronary sinus. 2) Via the four pulmonary veins. |
In addition to during the atrial systole, when else does blood flow to the ventricles? What portion of the blood moves this way? | 1) During the first stage in the cardiac cycle (everything is dyastole), b/c the tricuspid and miatrial valves are open. 2) 70-80% of the blood. |
What changes between the atrial systole and diastole for blood being transfered between the atria and the ventricles? | Pressure increases in the atrium, which increases the pressure gradient, “kicking” the remaining 20-30% of the blood into the ventricles. |
What is EDV? | End diastolic volume-volume of the ventricles before they begin the systole. |
What are the two phases of ventricular systole? | Isovolumic contraction and ventricular ejection phase. |
What happens during the isovolumic contraction phase? | The pressure in the ventricles rises to the point that some blood flows back into the atria closes the tricuspid and miatrial valves. Blood doesn’t go to the lung or the systemic circuit yet. |
What happens during the ventricular ejection phase? | The contraction of the ventricular muscles has raised the pressure higher than the pulmonary trunk and aorta so most of the blood leaves the ventricles. |
What is ESV? | End systolic volume-blood remaining in the ventricles after contraction. |
What are the two stages of ventricular diastole? | Isovolumic ventricular relaxation phase and the late ventricular diastole. |
What happens in the isovolumic ventricular relaxation phase? | Pressure drops and some blood flows back into the ventricles from the pulmonary trunk and the aorta, the semilunar valves close to present further backflow. |
What happens in the late ventricular diastole? | Pressure continues to drop until it drops below the atrial pressure and the mitral and tricuspid valves open and blood flows into the ventricles. |
What are the two sounds emitted by a normal healthy heart? | S1 (lub) and S2 (dub). |
What makes S1 and what makes S2? | 1) Closing of the atrioventricular valves during ventricular contraction. 2) Closing of semilunar valves during ventricular diastole. |
What does S3 indicate? | It can mean nothing when heard in youth, some athletes, and pregnant people, but when heard in older people it can indicate congestive heart failure. |
What is S3 made by? | Blood sloshing around in the atria or ventricles. |
What does S4 mean and what is it made by? | 1) Failure of the left ventricle. 2) The atria pushing blood into a stiff/hypertrophic ventricle. |
Which sounds make up the “Kentucky Gallop” and which sounds make up the “Tennesse Gallop?” | 1) S1, S2, and S3. 2) S1, S2, and S4. |
What is S7? | A combination of S3 and S4. |
What is a heart murmur? | A sound coming from the heart causes by turbulent flow of blood. |
Explain the scale that murmurs are graded on. | A 1-6 scale, w/1 being the most common and most difficult to detective, and 6 being the exact opposite. |
Why are patients asked to breathe deeply when listening for murmurs? | Because different parts of the breathing process restricts bloodflow to certain parts of the heart and thus amplifies the murmur. |
19.4-Cardiac Physiology
What is cardiac output? | A measurement of the amount of blood pumped by each ventricle in one minute. CO = SV x HR |
What is stroke volume? | The amount of blood pumped by one ventricle. SV = EDV - ESV |
What factors affect heart rate? | Autonomic innervation, hormones, fitness levels, age. |
What factors affect stroke volume? | Heart size, fitness levels, gender, contracablity, duration of contraction, preload (EDV), afterload (resistance). |
What are cardiac reserves? | The difference between maximum and resting CO. |
How is resting heart rate related to age? | The younger you are, the higher the resting heart rate. |
What is bradycardia? | A condition in which resting heart rate drops below 60 BPM IN ADULTS. |
What is tachycardia? | A condition in which restign heart rate is above 100 BPM IN ADULTS. |
How does excercise impact the heart? | Initially, heart rate and stroke volume both increase, but as heart rate continues to increase stroke volume decreases because the ventricles have less time to fill with blood. Cardiac output follows the same pattern of being stable at the beginning and later decreasing. |
What role does the vague nerve play in heart rate? | It causes the heart rate to decrease. NOT A FLASHCARD |
What role do the sympathetic cardiac nerves play in heart rate? | They increase heart rate and force of contraction. NOT A FLASHCARD |
What is the cardiac plexus? | A complex network of nerve fibers near the base of the heart. |
What are the two paired cardiovascular centers of medulla oblongata? | The cardioaccelerator centers and the cardioinhibitory centers. |
What do the cardioaccelerator centers do? | Stimulate activity via sympathetic stimulation of the cardioaccerelator nerves. |
What do the cardioinhibitory centers do? | Decrease heart activity by parasymethetic stimulation of the vagus nerve. |
What does sympathetic stimulation cause? | Norepinephrine release, which shortens the repolarization period. |
What does parasympathetic stimulation cause? | Releases acetylcholine, which slows the rate of spontaneous depolarization. |
What are the cardiac reflexes? | The baroreceptor reflex, the atrial/bainbridge reflex, several others. |
What is the baroceptor reflex? | Monitors barocepter firing in order to maintain cardiac homeostasis. Baroceptorsare stretch receptors, and they sense how much blood stretches out the heart (if there’s not enough blood changes are made). |
What is the atrial reflex and what is it also known as? | 1) Uses specialized atrial baroreceptors to make sure there’s enough blood in the atria. 2) Bainbridge reflex. |
What does the heart do when it realizes that there’s not enough blood? | Increases sympathetic stimulations (increases heartrate). |
What are the catecholamines? | Epinephrine and Norepinephrine-increase the rate of depolarization. |
What does thyroxin do and how does it do it? | 1) Increases cardiac rate and contractability. 2) Enters the cardiomyocytes and works at the genome level. |
How does calcium ion levels impact heart rate and contractability? | As calcium ion levels increase so do heart rate and contractibility. |
What do caffeine and nicotine do to the heart and how is their affect different? | 1) Increase heart rate. 2) Caffeine affects the sinoatrial node and nicotine stimulates the sympathetic neurons. |
What are factors that can slow heart rate? | Altered sodium and potassium levels, hypoxia, acidosis, alkalosis, and hypothermia |
What are hyponatremia and hypernatremia and what do they do the heart? | 1) Low sodium levels-initially leads to tachycardia, later on bradycardia and other arrhythmias. 2) High sodium levels-initially leads to tachycardia, later on leads to fibrillation. |
What is fibrillation? | A quivering or irregular heart rate. |
What are hypokalemia and hyperkalemia and what do they do to the heart? | 1) Low potassium levels-leads to arrhythmias. 2) High potassium levels-cause the heart to become weak and flacid and eventually fail. |
What are acidosis and alkalosis and what do they do to the heart? | 1) Blood is too acidic. 2) Blood is too alkaline. 3) Enyzmes are sensitive to PH, so it would mess up the enzymes having a complex affect on heart rate. |
What are hyperthermia and hypothermia and what do they do to the heart? | 1) Elevated body temp-increases heart rate and strength of contraction. 2) Lowered body temp-slows heart rate and strength of contractions. |
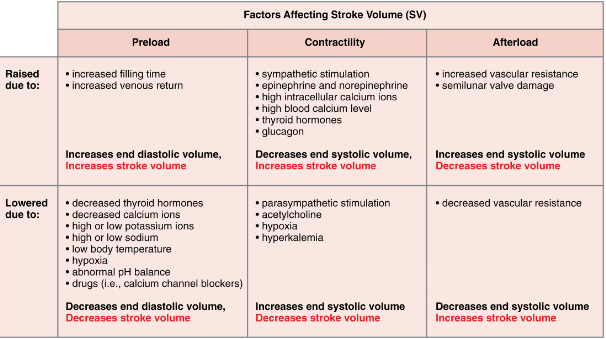
What are the three primary factors to consider when finding stroke volume? | Preload, contactabiloty, and afterload. |
What is preload? | The stretch on the ventricles prior to contraction. |
What can preload tell us about the heart? | The higher the preload, the longer the ventricular diastole or filling time. |
What are sarcomeres? | The basic contractile unit of a myocyte. |
What is the Frank-Starling mechanism and what is it also known as? | 1) States that within physiological limits, the force of heart contraction is directly proportional to the initial length of the muscle fiber. 2) Starling’s Law of Heart. |
Why do sarcomeres grow stronger as they become more stretched until their optimal lengths? | Because more myosin heads can bind to the actin on the thin filaments, which forms cross bridges. |
Who developed the Frank-Starling Mechanism and when did they publish their respective theories? | 1) Otto Frank and Ernest Starling. 2) 1912. |
What is venous return? | Venous return refers to the flow of blood from the periphery back to the right atrium, and except for periods of a few seconds, it is equal to cardiac output. |
What is contractibility? | The force of contraction of the heart muscle. |
How does it impact stroke volume? | The greater the contractibiloty, the greater the stroke volume. |
What are positive and negative inotropic factors? | 1) Factors that increase contractibility (e.g. sympathetic stimulation and norepinephrine and epinephrine. 2) Factors that decrease contractibility (e.g. parasympathetic stimulation and acetylcholine). |
What is afterload? | The tension that the ventricles develop to pump blood effectively against the resistance in the vascular system. |
How do the semilunar valves impact afterload? | Many conditions that increase afterload involve the valves being damaged and thus needing more force to open them. |
Table showing the main factors that impact stroke volume: | |
Table showing the main factors that impact cardiac output: | c |
19.5 Developement of the Heart
Question: | Answer: |
What is the first functional organ to develop and when does it begin working? | The heart around day 21 (a mere three weeks after fertilization). |
What does the heart develop from and where does it form? | 1) The mesoderm (an embryonic tissue). 2) The cardiogenic area (a region near the head of the embryo). |
What happens at 20 days? | Bloodflow through the endocardial tubes. |
What happens at 21 days? | The endocardial tubes fuse into the the primitive heart tube. |
What are the five regions of the primitive heart tube from head to tail as of 22 days? | Truncus arteriosus, bulbus cordis, primitive ventricle, primitive atrium, and the sinus venosus. |
What will the truncus arteriosus, bulbus cordis, primitive ventricle, primitive atrium, and the sinus venosus become? | 1) It will divide and give rise to the ascending aorta and the pulmonary trunk. 2) The right ventricle. 3) The left ventricle. 4) The anterior portion of the atria and the auricles. 5) Posterior portion of the right atrium, the sinoatrial node, and the coronary sinus. |
When does the heart take on a shape resembling an adult heart? | Between days 23 and 28. |
When does the heart partition itself into four chambers? | By the end of the fifth week. |
When do the atrioventricular and semilunar valves form? | 1) Weeks 5-8. 2) Weeks 5-9. |
20.1-Structure and Function of Blood Vessels
Question: | Answer: |
What is an artery? What is a vein? | 1) A blood vessel that carries blood away from the heart. 2) A blood vessel that returns blood to the heart. |
What do the pulmonary and systemic circuits do? | 1) Pulmonary arteries take deoxygenated blood from the right ventricles to the lungs and Pulmonary veins return freshly oxygenated blood to the left atrium. 2) Systemic arteries take freshly oxygenated blood from the left ventricle through the aorta to the rest of the body. Systemic veins take deoxygenated blood back to the right atrium via either the superior or inferior vena cavae. |
What is the difference between arteries and arterioles and veins and venules? | Arteries/arterioles have thicker walls due to the greater blood pressure of the blood flowing within them, and they have thinner lumens than veins/venules. |
What is a lumen in the context of the circulatory system? | The hollow passageway in which blood flows in the veins/venules and arteries/arterioles. |
How do you identify an artery vs a vein in an image? | Arteries appear rounder due to their thicker tunic. |
Why do veins have valves and why are they more important in the extremities? | 1) Ensure unidirectional bloodflow. 2) Bloodflow is sluggish in the extremities due to lower blood presure and gravity. |
What are vasa vasorum and what do they do? | 1) Blood vessels within the larger blood vessels. 2) Distribute oxygen and nutrients withing larger blood vessels. |
What is the difference in location between the vasa vasorum in veins and arteries and why does this occur? | They are located in the outer regions of the arteries and closer to the lumen of the veins due to differences in blood pressure. |
Why are arterial diseases more common than venous diseases? | The location of the vasa vasorum makes it more difficult for them to distribute nutrients and oxygen in arteries than veins. |
What are nervi vasorum? | Small nerves located in the veins and arteries than control the contraction and dilation of smooth muscle. |
What are tunics of the veins and arteries, from innermost to outermost? | Tunica intima, tunica media, tunica externa. |
What is the tunica intima and why is it important? | 1) The innermost layer of the veins/arteries, which in continuous through the entire cardiovascular system. 2) Separates the lumens from the walls of the veins/arteries, regulates capillary exchange, alters bloodflow, regulates blood pressure. |
What does the uncompensated overproduction of endthelins do and what emits them? | 1) Causes high blood pressure and heart disease. 2) Tunica intima. |
What is the internal elastic membrane and what is it also known as? | 1) A thick layer of elastic fibres located between the tunica intima and the tunica media that provides structure while also allowing the structure to stretch. It is not apparent in veins. 2) Internal elastic lamina. |
How can you tell the lumen and tunica intima in the veins from the lumen and tunica intima in the arteries? | The lumen and tunica intima of a vein will appear smooth while the lumen and tunica intima of an artery will appear wavy due to partial constriction of the smooth muscle in the tunica media. |
What is the tunica media? | The middle layer of veins/arteries, which is the thickest layer in arteries and is much thicker in arteries than veins. |
What does the tunica media consist of? | Smooth muscle that is supported by connective tissue made up of elastic fibres. Toward the outer regions of this tunic there are longitudinal muscles. |
What is vasoconstriction and vasodilation? | 1) Constriction of the smooth muscles, decreases blood flow. Narrows the lumen. 2) Relaxation of the smooth muscle, increases blood flow and widens lumen. |
What is the external elastic membrane and what vascular structures is it found in? | A membrane that separates the tunica media from the tunica externa, which is only found in larger arteries. |
What is the tunica externa? | A sheath of connective tissue that makes up the outermost layer of a vein/artery. |
What is the tunica externa composed of? What does it do? | 1) Primary collagenous and elastic fibres. 2) It prevents veins/arteries from moving. |
In what situation will the tunica externa be thicker than the tunica media? | In veins and larger arteries. |
What kinds of arteries have the thickest walls and why? | 1) Arteries closest to the heart -> AKA elastic arteries. 2) Due to the higher blood pressure closer to the heart. |
What are elastic arteries and what are they also known as? | 1) Arteries close to the heart that have thicker walls and a higher percentage of elastic fibres in all three tunics. 2) Conducting artery-called this because their lumens can expand and conduct a lot of blood. |
What are muscular arteries and what are they also known as? | 1) Arteries found further away from the heart that have a higher percentage of smooth muscle in them. 2) Distributing aries because they distribute the blood to a network of arterioles. |
What is an arteriole? What are they also known as and why? | 1) A very small artery that leads to a capillary. 2) Resistance arteries because they slow blood down and lower blood pressure. |
How are the tunics different in arterioles? | They have the same three tunics but the thickness of them is greatly decreased. |
What is vascular tone and why is it especially important in arterioles? | 1) The muscle tone of the arteries that occurs due to partial contraction of the smooth muscle. 2) They are the main reason why blood is slowed in arterioles. |
What is the diameter of lumens dependant on? | Neural and chemical controls. |
What are capillaries? What is perfusion? | 1) Microscopic channels that supplies blood to tissues. 2) The process of supplying blood to tissues, what capillaries do. |
What is microcirculation? | Circulation through the capillaries. |
What are the layers in capillary walls? | The endothelial layer, the basement membrane, and occasional smooth muscle fibres. |
What are the types of capillaries, what determines the type, and why must they be this way? | 1) Continuous, fenestrated, and sinusoid. 2) How leaky they are. 3) Blood must be able to leave the capillaries to go to the tissues. |
What are continuous capillaries and where are they found? | 1) Capilaries that have a complete endothelial lining withe tight junctions between endothelial cells, which onlys for the passage of water and ions. 2) All vascularized tissues. |
How do materials other than water and ions pass from continuous capillaries to tissues? | Through intercellular clefts. |
Where do continuous capillaries not have intercellular clefts? Why? | 1) The brain. 2) To maintain the brain blood barrier and protect the brain from toxins. |
What are fenestrated capillaries and where are they found? | 1) A capillary that has pores in addition to tight junctions in the endothelial lining. 2) The small intestines, the kidneys, the choroid plexus of the brain, and many endocrine structures. |
What causes the number of fenestrations and the degree of permiability to vary? | The location in which the fenestrated capillaries are found. |
What is a sinusoid capillary? | Cappilares that are flattened with extensive intercellular gaps and incomplete basement membranes, in addition ot intercellular clefts and fenestrations. |
What are the capillary types from most common to least common? | Continous, fenestrated, and sinusoid. |
What are sinusoid capillaries used for? | Allowing the largest molecules to pass between the capillary and tissue, and allowing newly formed red blood cells to join the bloodstream. |
Which type of capillary does blood flow most slowly through? What does this allow? | 1) Sinusoid capillaries. 2) In order to allow more time to exchange gasses, nutrients, and waste. |
Where are sinusoid capillaries found? | Liver, spleen, bone marrow, lymph nodes (in this setting they carry lymph not blood), and in some endocrine glands. |
What are metarterioles? | A type of blood vessel that has the structural charecteristics of an ateriole and a capillary. |
What are capillary beds? | An interwoven network of capillaries that supplies an organ. |
What are precapillary sphincters? Why are they important? | 1) Smooth muscle cells that surround the junction between metarterioles and capillaries that regulate the flow of blood into capillary beds. 2) If they were always opened, all the blood iin thebody would be in the capillary beds and not in the ateries, vein, arterioles, venules, or the heart. |
What happens to blood when precapillary sphincters are closed? In what other situation might blood bypass a capillary bed? | 1) It travels from the metarterioles through a thoroughfare channel into the venous circulation. 2) Arteriovenous anatomosis. |
What is an arteriovenous anastomosis? | Direct connections between small arteries and small veins. |
What is vasomotion and what is it regulated by? | 1) The irregular pulsating way that blood moves through capillary beds. 2) Chemical signals that are triggered in response to changes in internal conditions. |
What are venules? | Extremely small veins, which join to form large veins and join veins to the capillary beds. |
What are venules the primary site of? Define it. | 1) Emigration/diapedesis. 2) The movement of leukocytes out of the circulatory system and towards the site of tissue damage or infection. |
How is the interior of veins and arteries different? | Veins have thinner walls and large and irregular lumens. They also have valves that promote unidirectional bloodflow. |
What is the secondary function of veins and why are they able to do this? | 1) Holding blood, in addition to returning it to the heart. 2) High capacitance (ability to expand and hold blood). |
What are veins sometimes referred to as? | Capacitance vessels. |
What happens when blood needs to be redistributed to other parts of the body? | The smooth muscles on veins contract, speeding the blood’s return to the heart and displacing any blood that is being held in the veins. |
What is venous reserve? | The blood that resides in the veins that is used when the body needs to redistribute the blood that stays in the veins. |
20.2-Blood Flow, Blood Pressure, and Resistance
Question: | Answer: |
What is blood flow? | The movement of blood through a vessel, tissue, or organ, that is expressed in terms of volume per unit of time. |
What is blood pressure? | The force exerted on the walls of the blood vessels or the chambers of the heart. |
How is blood pressure measured and in what units? | 1) Using te brachial artery of the arm and a blood pressure cuff. 2) mm/Hg. |
What are the components of arterial blood pressure? | Systolic, diastolic, pulse, and mean arterial pressure. |
How is systemic arterial blood pressure recorded and what does each number represent? | 1) A ratio of two numbers (e.g. 120/80). 2) The higher number is the systolic pressure, the denominator is the diastolic pressure. |
What is systolic pressure? | Reflects arterial pressure resulting from the ejection of blood during ventricular contraction (ventricular systole). |
What is diastolic pressure? | Represents the arterial pressure of blood during ventricular relaxation (ventricular diastole). |
What is pulse pressure? | The difference between systolic pressure and diastolic pressure. In health individuals, it should be at least 25% of the systolic pressure. |
What does a low/narrow pulse pressure indicate? | Low stroke volume, congestive heart failure, stenosis of the aortic valve, or significant blood loss. |
What does a high/wide pulse pressure indicate? | Normal after exercise, excessive resistance in the arteries. This harms the heart, brain, and kidneys. |
What is MAP and what does it stand for? | 1) The average blood pressure of the arteries. Can be approxiamted with MAP = diastolic BP + (systolic BP-diastolic BP)/3. 2) Mean Arterial Pressure. |
What are ischemia and hypoxia? | 1) Insufficient blood flow. 2) Inadequite oxygenation of tissues. |
What is pulse? | The expanse and recoil of elastic fibres in arteries due to the contraction of the heart. |
How evident is the systolic and diastolic components of pulse? | It is evident until the level of arterioles, but the effect diminishes with distance from the heart. |
Why is it important to measure pulse? | It can indicate the strength of ventricular systole and cardiac output. It can also indicate the presence of a heart condition. |
What arteries are used to measure pulse? | Temporal, facial, brachial, femoral, popliteal, posterior tibal, and dorsalis pedis arteries in the feet. |
What happens when pressure in the arteries is increased? In the veins? | 1) Blood flow will decrease. 2) Blood flow will increase. |
What happens to blood flow when cardiac output is increased? | Blood pressure (NOT arterial pressure) will increase, and so will blood flow. |
What is compliance? Are veins or arteries more compliant? | 1) The ability of any compartment to expand to accommodate increased content. 2) Veins. |
What happens when vascular disease stiffens the arteries? | Compliance is reduced and resistance to blood flow increase -> more turbulence, more pressure within the vessel, reduced blood flow -> the heart has to work harder. |
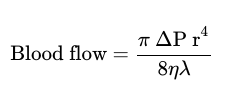
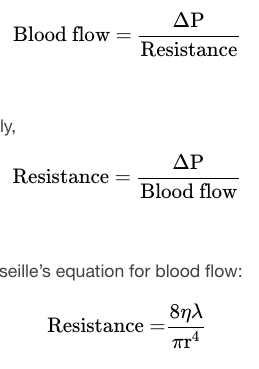
Who was Jean Louis Marie Poiseuille? | A french physician and physiologist, created a mathematical equation that describes blood flow and its relationship to known parameters. |
-π is the Greek letter pi, used to represent the mathematical constant that is the ratio of a circle’s circumference to its diameter. It may commonly be represented as 3.14, although the actual number extends to infinity. -ΔP represents the difference in pressure. -r4 is the radius (one-half of the diameter) of the vessel to the fourth power. -η is the Greek letter eta and represents the viscosity of the blood. -λ is the Greek letter lambda and represents the length of a blood vessel. | |
How is blood volume related to pressure and flow? | As blood volume increase, so does blood pressure and blood flow. |
What is hypovolemia, what causes it, and how is it treated? | 1) Low blood volume. 2) Bleeding, dehydration, vomiting, severe burns, some medications uses to treat hypertension. 3) Intravenous fluid replacement (blood transfusion). |
What is hypervolemia, what causes it, and how is it treated? | 1) Excessive fluid volume. 2) Heart failure, livercirrhosis, kidney disease, hyperaldosteronism, and glucocorticoid steroid treatments. 3) Treating the underlying condition that caused it. |
What are the two primary determinants of blood viscosity? | Formed elements (specifically erthrocytes) and plasma proteins (from the liver). |
How is the length of a vessel related to its resistance? | They are directly proportional, so as the length increases so does the resistance. |
How does the weight of the body impact the heart? | The larger the body, the more length of blood vessels, and thus the more resistance the heart has to push against. |
What are the main things that determine the diameter of blood vessels? | The type of vessel, and neural and chemical signals (they trigger vasodilationa nd vasoconstriction). The most important determinant is vascular tone. |
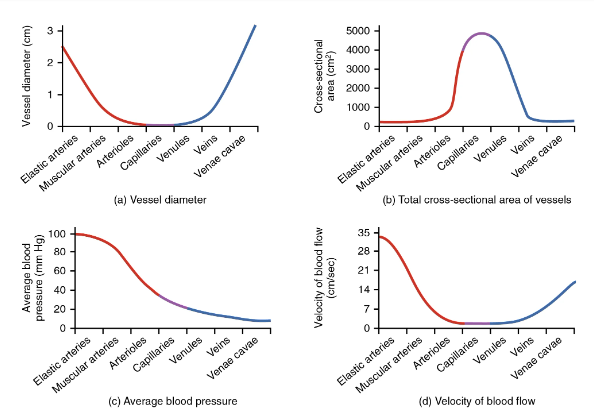
How does the diameter of the vessel impact blood flow? | The greater the diameter, the less resistance (less blood contacts the edge of the vessel), and thus the greater blood flow. |
How is resistance mathematically related to the radius of the vessel? | R = 1/r4 |
Why do capillaries have less resistance than arterioles even though they have a smaller lumen? | The total cross sectional area of capillary beds are much greater than the diameter of arterioles. |
What vessels’s vasoconstriction and vasodilation impact blood pressure the most? | The arterioles. |
What is the skeletal muscle pump? Why is it important? | 1) A mechanism that causes the pressure in the veins to be increased with the contraction of the skeletal muscle. 2) It helps lower pressure veins counteract the force of gravity. |
If we didn’t have the skeletal muscle pump, what would happen? | Blood would pool in the lower limbs, and not return to the heart, which would prevent the brain from getting enough blood, which would cause the patient to lose conciousness. |
What is the respiratory pump? | The respiratory pump is a mechanism to pump the blood back to the heart using inspiration (breathing in). |
What does the respiratory pump cause the blood to do? | It helps blood from the thorax return to the right atrium. |
Does blood travel faster in veins or venules and why? | Veins, due to the skeletal muscle pump and a greater pressure gradient between veins and the right atrium/the venae cavae. |
20.3-Capillary Exchange
Question: | Answer: |
What is the primary purpose of the cardiovascular system? | To circulate gases, nutrients, wastes, and other substances to and from the cells of the body. |
What is bulk flow? | The movement of blood from a region of high pressure to a region of low pressure. |
What is filtration? | The movement of material from a capillary into the interstitial fluid, moving from an area of higher pressure to lower pressure. |
What is reabsorption? | The movement of fluid from an area of higher pressure in the tissues into an area of lower pressure in the capillaries. |
What is hydrostatic pressure? | The pressure of any fluid enclosed in a space, and the primary force driving fluid transport between capillaries and tissues. |
What is blood hydrostatic pressure? | The force exerted by the blood confined within blood vessels or heart chambers. |
What does CHP stand for and what does it mean? | 1) Capillary hydrostatic pressure. 2) The pressure exerted by blood against the wall of a capillary. |
How is IFHP impacted by fluid from the capillaries entering the tissues? | It rises, because there is more fluid in the same amount of space. |
What does IFHP stand for? | Interstitial fluid hydrostatic pressure. |
Why is the CHP (originating from arterial pathways) higher that IFHP? | The lymphatic vessels are continuously absorbing extra fluid from the tissues. |
What is osmotic pressure and what is it also referred to as? | 1) The minimum pressure that must be applied to a solution to halt the flow of solvent molecules through a semipermeable membrane (osmosis). 2) Oncotic pressure. |
What is the difference between hydrostatic pressure and osmotic pressure? | Hydrostatic pressure sends fluids out of the capillaries while osmotic pressure pulls fluid back in. |
What is osmotic pressure determined by and why? | 1) Osmotic concentration gradients (the solute to water concentrations in the blood vs the tissue). 2) A region higher in solutes draws water across a semipermiable membrane (wall of capillary) from a region lower in solute concentration. |
What is the difference in the solute-to-water ratio in tissue vs blood? | Blood has more solutes and less water than tissues, so they draw water from the tissues. |
What does BCOP stand for and what is it? | 1) Blood colloidal osmotic pressure. 2) The pressure created by the concentration of colloidal proteins in the blood. |
What is IFCOP and what does it stand for? Why is it always lower than BCOP? | 1) The pressure created by the concentration of colloidal proteins in the blood. 2) Interstitial fluid colloidal osmotic pressure. 3) Interstitial fluid contains very few proteins. |
What unit is used to express pressures in the cardio vascular system? | Millmeters of mercury (mm Hg). |
How does CHP change as blood moves through the capillary beds? | When blood has only just left the arterioles, the CHP is higher, and it decreases as blood travels through the capillary bed towards the venous end. |
Why does BCOP remain constant throughout the blood’s journey through the capillary beds? | Because plasma proteins stay in the blood and don’t get filtrated into the interstitial fluid. |
What is NFP and what does it stand for? | 1) The net pressure of the hydrostatic and osmotic pressure. CHP - BCOP. 2) Net Filtration Pressure. |
Based on the NFP, how do you know if filtration or reabsorption is occurring? Where is the value positive or negative? | 1) It will be positive during filtration and negative during reabsorption. 2) Positive in the arterial end, negative in the venous end. |
Is more fluid filtered or reabsorped? What happens to the extra fluid? | 1) More fluid is filtered. 2) The extra fluid is taken by the lymphatic vessels. |
20.4-Homeostatic Regulation of the Vascular System
Question: | Answer: |
What must the cardiovascular system do to maintain homeostasis? | Blood flow must be redirected continually to the tissues as they become more active. |
What is the only organ that has the same amount of blood allocated to it all the time? | The brain. |
During autoregulation, what is done to maintain homeostasis? | Changes to blood flow are made is response to changes by local receptors (vasodilators and vasoconstrictors, which either increase or decrease blood). |
What are the primary neural regulation sites? | Cardiovascular centers in the brain, generalized neural responses from the limbis system and the autonomic nervous system. |
Where is the cardiovascular center of the brain located and what are its three main components? | 1) Medulla oblongata. 2) Cardioaccelerator centers, cardioinhibitor centers, and the vasomotor centers. |
What does the cardiovascular center respond to? | Changes in blood pressure, blood concentrations of oxygen, carbon dioxide, hydrogen ions. |
What does the cardioaccelerator regions do? | Stimulate cardiac function by regulating heart rate and stroke volume by using sympathetic stimulation from the cardiac accelerator nerve. |
What do the cardioihibitor centers do? | They slow cardiac function by decreasing heart rate and stroke volume via parasympathetic stimulation from the vagus nerve. |
What do the vasomotor centers do? What does this impact? | 1) Control contraction of the smooth muscle in the tunica media. 2) This causes changes in the diameter of the lumen, which impact resistance, pressure, and flow. |
What are baroreceptors? Where are they located? | 1) Specialized stretch receptors in the heart that measure the stretch caused by blood. 2) Thin areas of blood vessels, and in the heart (specifically the sinuses). |
What do barorecptors do when blood pressure is too high? | They fire at a higher rate which triggers parasympathetic stimulation (heart beats slower, cardiac output decreases). Peripheral arterioles are caused to dilate. These activities cause blood pressure to fall. |
What do baroreceptors do when blood pressure is too low? | Baroreceptors fire too slowly, which increases sympathetic stimulation (heart rate increases, cardiac output increases). Peripheral vessels will constrict. These cause blood pressure to rise. |
What is the atrial reflex? | If blood returns to the right atrium faster than it leaves the aorta, atrial receptors will trigger sympathetic stimulation which in turn increases cardiac output (amount of blood pumped by the left ventricle in a unit of time). |
What do chemoreceptors do in the circulatory system? Where are they located? | 1) Monitor levels of oxygen carbon dioxide, and hydrogen ions (pH) in the blood. 2) They are located near baroreceptors in the aortic and carotid sinuses. |
How are hydrogen ions produced in the body? | It is produced in cellular respiration, which increases when the body is active. Lower pH -> active body, higher pH -> resting body. |
How do chemoreceptors respond to increasing carbon dioxide and hydrogen ions (falling pH)? What are oxygen levels in this scenario? | 1) They stimulate the cardio accelerator and vasomotor centers which increases cardiac output and constricts peripheral vessels. They also suppress the cardioinhibitor centers. 2) They are lower. |
How do the chemoreceptors respond to falling carbon dioxide and hydrogen ions (increasing pH)? What are oxygen levels in this scenario? | 1) Cardioinhibitor centers are stimulated, which decreases cardiac output and causes peripheral vasodilation. The cardioaccelerator and vasomotor centers are suppressed. 2) They are higher. |
What does endocrine regulation entail? | Catecholamines, epinephrine and norepinephire, and several hormones that interact with the kidneys in order to regulate blood volume. |
What do epineprine and norepinephrine do to the heart? What releases these hormones? | 1) They increase heart rate and force of contraction. 2) The adrenal medulla. |
What does ADH stand for and what does it do to the heart? | 1) Antidiuretic hormone. 2) It signals the kidneys to reabsorb more water, which increase fluid levels and helps restore blood volume and pressure. |
What releases ADH and what triggers its release? | 1) The hypothalamus. 2) Increasing osmolarity of tissue fluid which signals significant blood loss. |
What is the renin-angiotensisn-aldosterone mechanism? | A mechanism that uses the hormones/enzymes renin and erythropoietin in order to form a long term solution to decreases blood pressure and volume. |
What is renin, what releases it, what triggers the release, and what does it do to the heart and circulatory system? | 1) An enzyme. 2) Specialized kidney cells, known as juxtaglomerular (JG) cells. 3) Decreasing blood pressure. 4) Activates a plasma protein known as angiotensinogen, turning it into angiotensin 1. |
How does angiotensin 1 turn into angiotensin 2, and where does this occur? | It is carried by the circulatory system from the kidneys to the lungs where ACE turns it into angiotensin 2. |
What does angiotensin 2 do to the circulatory system? | It is a powerful vasocinstrictor, and its presence increases blood pressure. |
What is aldosterone and what does it do to the circulatory system? | 1) A hormone produced by the adrenal cortex. 2) Increases the reabsorption of sodium into the blood, which in turn increases the reabsorption of water because water follows sodium. It additionally stimulates the thirst center in the hypothalamus. These efforts increase blood volume and pressure. |
What does EPO stand for, what is it released by, and when is it released? What does it do to the circulatory system? | 1) Erythropoietin. 2) The kidneys. 3) When blood flow or oxygen levels decrease. 4) Stimulates the production of erythrocytes in bone marrow (red blood cells). It is also a vasoconstrictor. This causes blood volume and pressure to increase. |
What does ANH stand for, what secretes it, what triggers its secretion, and what does it do to the circulatory system? | 1) Atrial Natriuretic hormone. 2) Cells in the atria of the heart. 3) When blood volume is high enough to cause extreme stretching of the cardiac cells. 4) They promote loss of sodium and water in the kidneys, suppress renin, aldosterone, ADH, production. This causes blood pressure and volume to drop. |
What signals does autoregulation of perfusion rely on? | Local self-regulatory mechanisms such as chemical signals and myogenic controls. This does not include nervous stimulation or endocrine control. |
What do chemical signals do in the cardiovascular system? How does this affect the cardiovascular system? What chemicals do opening and closing use? | 1) Regulate opening and closing of the precapillary sphincters. 2) Determines if blood flows to the capillaries. 3) Opening-NO (vasodilator, released from endothelial cells), Closing-Endothelins (vasoconstricting peptides, released from endothelial cells). |
What triggers the opening of precapillary sphincters? The closing? | 1) Decreased oxygen concentrations; increased carbon dioxide concentrations; increasing levels of lactic acid or other byproducts of cellular metabolism; increasing concentrations of potassium ions or hydrogen ions (falling pH); inflammatory chemicals such as histamines; and increased body temperature. 2) Opposite levels of the regulators, which prompt the release of endothelins, powerful vasoconstricting peptides secreted by endothelial cells. Platelet secretions and certain prostaglandins may also trigger constriction. |
What is the myogenic response? Why does it occur? | 1) A reaction to the stretching of the smooth muscle in the walls of arterioles as changes in blood flow occur in the vessel. 2) To prevent dramatic fluctuations in blood pressure and blood flow which maintains homeostasis. It also stabalizes blood flow in nearby capillary beds. |
What will the myogenic response be when bood flow is too high? Too low? | 1) Smooth muscle will contract (vasoconstriction), which reduces blood flow. 2) Vessel will dialate, which increases blood flow. |
How does tissue prefusion change during exercise? | Selective vasodilation in the skeletal muscles, heart, lungs, liver, and integument. Vasoconstriction occurs in the vessels leading to the kidneys, and digestive and reproductive organs. |
How is venous return enhanced during exercise? | The skeletal muscle and respiratory pumps are more efficient due to the increased stimulation in the skeletal muscles and lungs. |
What are hypertension and hypotension? What are the effects that they have? | 1) Chronically elevated blood pressure-heart attack, stroke, aneurysm, peripheral arterial disease, chronic kidney disease, heart failure. 2) Chronically low blood pressure. |
What is hemorrhage? | A loss of blood that cannot be controlled by hemostatic mechanisms. |
What is circulatory shock? What are the symptoms? What are the types of circulatory shock? | 1) A condition in which the circulatory system is unable to maintain blood flow to adequately supply sufficient oxygen and other nutrients to the tissues to maintain cellular metabolism. 2) Increased heart rate but lowered blood pressure, urine output falls dramatically, patient will be confused or lose conciousness. 3) Hypovolemic, cardiogenic, vascular, and obstructive. |
20.5
Question: | Answer: |
What is the role of the circulatory system in the digestive system? | Absorbs nutrients and water; delivers nutrients (except most lipid) to liver for processing by hepatic portal vein; provides nutrients essential for hematopoiesis and building hemoglobin. |
What is the role of the circulatory system in the endocrin system? | Delievers hormones, hormones are use to maintain homeostasis in the circulatory system. |
What is the role of the circulatory system in the intergumentary system? | Carries clotting factors, platelets, and white blood cells for hemostasis, fighting infection, and repairing damage. Regulates temperature by controlling blood flow to the surface, provides some coloration of the skin, and acts as a blood resovoir. |
What is the role of the circulatory system in the lymphatic system? | Transports various white blood cells and immunoglobins (antibodies), carries excess tissue fluid not able to be reabsorbed by the vascular capillaries back to the lymphatic system for processing. |
What is the role of the circulatory system in the muscular system? | Provides nutrients and oxygen for contraction, removes lactic acid and distributes heat generated by contraction, muscular pumps aid in venous return, exercise contributes to cardiovascular health. |
What is the role of the circulatory system in the nervous system? | Produces cerebrospinal fluid (CFC) within choroid plexuses, contributes to blood-brain barrier, cardiac and vasomotor centers regulate cardiac output and blood flow. |
What is the role of the circulatory system in the respiratory system? | Provides blood for critical exchange of gases to carry oxygen needed for metabolic reactions and carbon dioxide generated a byproducts of these processes. |
What is the role of the cicrculatory system in the skeletal system? | Provides calcium, phosphate, and other minerals critical for bone matrix, transports hormones regulating buildup and absoption of matrix including growth hormone, thyroid hormone, and calcitonins, and parathyroid hormone, erythropietin stimulates myeloid cell hemtopoiesis, some level or protection for some vessels by bony structures. Add this table from the text |
20.6-Development of Blood Vessels and Fetal Circulation
Question: | Answer: |
By what time are fetal circulation patterns established? | Within the fourth week of embryonic life. |
Where do blood vessels begin to form? What are these initial cells known as? | 1) The embryonic mesoderm. 2) Hemangioblasts. |
What are angioblasts? | Cells that give rise to blood vessels and pluripotent stem cells. |
What are blood islands? What are the spaces on the blood islands? | 1) Masses of cells that will become blood vessels that are scattered throughout the embryonic disk. 2) Spaces that will one day become blood vessel lumens. |
Where does the endothelial lining come from? The smooth muscle and connective tissues? The actual blood? | 1) The angionblasts. 2) Mesenchymal cells. 3) Pluriponent stem cells start to form blood. |
What are vascular tubes? | Tubes that will eventually become veins, arteries, and capillaries. They eventually connect to each other and the tubular heart. |
What is angiogenesis? | The creation of new blood vessels from existing ones, which continues throughout life not just as a fetus. |
How is blood vessel and nerve development related? | They often travel to the same tissues and organs at the same time (e.g forming blood vessels and forming nerves will form in the liver at the same time). |
How do vessels know whether to develop into a vein or an artery? | This is based on local concentrations of signaling proteins. |
What does the umbilical vein do? | It caries oxygen rich blood from the placenta from the pregnant person to the fetal inferior vena cava via the ductus venosus. |
What do the umbilical arteries do? | They carry oxygen depleted fetal blood, which includes wastes are carbond dioxide. Remnants of these arteries remain in the adult. |
What are shunts? What are the three main shunts in the fetal circulatory system? | 1) Alternate pathes from blood flow. 2) The foramen ovale, the ductus arteriosus,a and the ductus venosus. |
Which shunts are the most critical and why? | 1) The foramen ovale and the ductus arteriosus. 2) Because the lungs are filled with amniotic fluid and are compressed. |
What is the ductus arteriosus? How does it close? | 1) A short muscular vessel that connects the pulmonary trunk to the aorta. This is there because blood is only circulated to the lungs in order to maintain the developing lung tissues. 2) Pressure in the lungs drops as the newborn takes its first breath, and as the amount of oxygen rises, smooth muscles in the wall of the ductus arteriosus constrict which seals them off. |
What is the ductus venosus? How does it close? | 1) A temporary blood vessel that branches from the unbilical vein to the placenta that allows blood to bypas the fetal liver and go directly to the fetal heart. 2) It closes slowly during the first weeks of infancy, and then degrades into the ligamentum venosum. |
18.1-An Overview of Blood
Question: | Answer: |
Why is blood a connective tissue? | It is made up of cellular elements and an extracellular matrix. |
What are the cellular elements? | The formed elements, which includes red blood cells (RBCs), white blood cells (WBCs), and platelets. |
What are platelets? | Cell fragments. |
What is the extracellular matrix? | Plasma. |
What is the primary function of blood? | To deliver oxygen and nutrients, and to remove wastes from body cells. |
How does the blood help with defense? | The WBCs protect the body from both external threats (disease) and internal threats (cancer). |
How does blood help maintain homeostasis? | It regulates temperature, chemical balance, and water content of the body. |
What is a hematocrit? | A test that measures the percentage of RBCs. |
What are RBCs clinically known as? What does RBC stand for? Where do RBCs settle in a hematocrit? | 1) Erythrocytes. 2) Red blood cells. 3) The bottom of the hemotocrit tube. |
What is the buffy coat? | The layer in which WBCs and platelets settle in a blood test (specifically a hemocrit test). |
What are WBCs clinically known as? What does WBC stand for? What are platelets clinically known as? | 1) Leukocyctes. 2) White Blood Cells 3) Thrombocyctes. |
What does PCV stand for? What is it? | 1) Packed cell volume. 2) The volume of erythrocytes after centrifugation. |
Is there more plasma or erythrocytes in the blood? List the components of blood from most to least numerous. | 1) Plasma. 2) Plasma, erythrocytes, buffy coat. |
What is anemia? Polycythemia? | 1) Low erythrocyte volume. 2) Too many erthrocytes. |
How does the color of the blood varie with oxygen content? Why does this occur? | 1) Blood that has just gotten oxygen from the lungs is bright red, and blood that has already transported its oxygen to the blood is a more dusky red. 2) This occurs due to hemoglobin, which is a pigment that changes color depending on the degree of oxygen saturation. |
How does the viscosity of blood compare to water? | It is five times more viscous than water. |
What is the temperature of blood? Why is it this way? | 1) Slightly above body temperature. 2) Friction between the blood and blood vessels. |
What is the average pH of blood? How it compare to the pH of water? | 1) 7.4 2) It is slightly more basic than water. |
What is blood plasma composed of? | 92% is water, 7% is proteins that are dissolved in the water, 1% is other substances. |
What are the three major groups of plasma proteins? | Albumin, globulins, and fibrinogen. |
What is albumin? What percent of the plasma does this make up? | 1) The most abundant of the plasma proteins, that is manufactured by the liver. It serves as a binding protein that transports fatty acids and steroid hormones. It is also the most significant contributor to osmotic pressure. 2) 54% |
What are the types of globulins? What does each do? What percent of the plasma do globulins make up? | 1) Alpha and beta globulins transport iron, lipids, and fat soluble vitamins A, D, E, and K. 2) Gamma globulins are proteins involved in immunity or antibodies. 3) 38% |
What is the difference between alpha and beta globulins? | Alpha globulins encompass proteins involved in various roles, including enzyme inhibition, acute phase response, and the binding of free hemoglobin. Beta globulins include proteins related to iron transport, immune system support, and complement system activation. |
Where are gamma globulins produced and what are they also known as? | 1) They are produced by specalized leukocytes known as plasma cells. 2) Immunoglobulins or antibodies. |
What is fibrinogen? What percentage of the plasma does it make up? | 1) A plasma protein that is important to the blood-clotting process. It is produced by the liver. 2) 7% |
In addition to plasma proteins, what are the other solutes in plasma? | Various electrolytes, such as sodium, potassium, and calcium ions; dissolved gases, such as oxygen, carbon dioxide, and nitrogen; various organic nutrients, such as vitamins, lipids, glucose, and amino acids; and metabolic wastes. |
18.2-Production of the Formed Elements.
Question: | Answer: |
What is are the average lifespans of bloodcells and platelets? What is the exception of this? | 1) A few weeks to a few days. 2) Special leukocytes known as memory cells that live for years. |
What is hemopoiesis? What is it also known as? | 1) The process by which blood replacement occurs. 2) Hematopoiesis. |
Where does hemopoiesis occur in fetuses? Neonats? Children? Adults? | 1) Yolk sac, fetal liver, spleen, and lymphatic tissue, eventually red bone marrow. 2) Red marrow. 3) medullary cavity of long bones. 4) Cranial and pelvic bones, vertebrae, the sternum, and the proximal epiphyses of the femur and humerus. |
What is extramedullary hemopoiesis? | Hemopoiesis that occurs outside the medullary cavity of adult bones, within the liver and spleen. This is triggered when regular hemopoiesis is prevent by disease. |
How do stem cells turn into a specific cell of the human body? | A stem cell divides in two, and one cell differentiates into a specific cell type. |
What is a totipotent stem cell? | A stem cell that can give rise to any type of cell in the human body. |
What is a pluripotent stem cell? | A stem cell that gives rise to multiple types of cells and some supporting fetal membranes. |
What are mesenchymal stem cells? | Stem cells that only developes into types of connective tissue: fibrous connective tissue, bone, cartilage, and blood. |
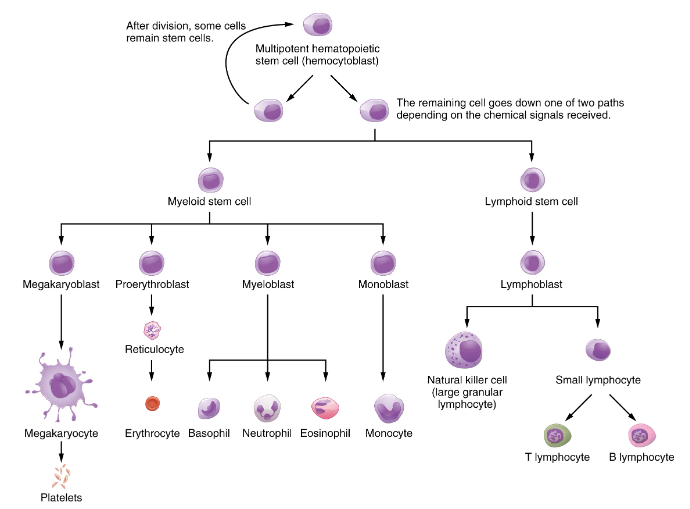
What are hematopoietic stem cells? What are they also known as? | 1) A type of stem cell that can give rise to all the formed elements of blood. 2) Hemocytoblast. |
What are hemopoietic growth factors? | Chemical stimuli that prompt a hematopoietic stem cell to divide. |
What are the two types of stem cell that a hematopoietic stem cell can become? | Lymphoid stem cells and myeloid stem cells. |
What are lymphoid cells? | Stem cells that give rise to a class of leukocytes known as lymphocytes (this includes T cells, B cells, and natural killer cells). |
What are myeloid stem cells? | Stem cells that give rise to all formed elements other than lymphoid cells. |
What kinds of cells will a myeloid stem cell differentiate into? | Megakaryoblasts, proerythroblasts, monoblasts and myeloblasts. |
Diagram for cheat sheet: | |
What does EPO stand for and what is it? | 1) Erthyropoietin. 2) A glycoprotein hormone secreted by the interstitial fibroblast cels of the kidneys in response to low oxygen levels. |
What is thrombopoietin? | A glycoprotein hormone produced by the liver and kidneys that triggers the development of megakaryocytes into platelets. |
What are cytokines? | Small proteins that are crucial in controlling the growth and activity of other immune system cells and blood cells. |
What are the main types of cytokines? | Colony stimulating factors and interleukins. |
What does CSF stand for and what are they? | 1) Colony-stimulating factors. 2) Glycoproteins that activate intracellular signaling pathways that can cause the cells to proliferate and differentiate into a specific kind of blood cell, usually white blood cells. |
What are the types of CSFs? What does each do? | 1) Granulocyte CSFs-Trigger the differentiation of myeloblasts into granular leukocytes. 2) Monocyte CSF-Triggers the production of monocytes. |
What are interleukins? | A type of cytokine singaling molecule that is produced by leukocytes, bone marrow, and endothelium. They communicate with leukocytes and play roles in differentiation and maturation of cells, producing immunity and inflammation. |
18.3-Erythrocytes
Question: | Answer: |
What is the most common formed element? How many is found in a milliliter of blood for female and male? | 1) Erythrocytes. 2) M-5.4 million; F-4.8 million. |
What is the primary function of erthrocytes? | They pick up inhaled oxygen and transport it to the body’s tissues, and they take 24% carbon dioxide waste from the tissues and transport it to the lungs for exhalation. |
Do erythrocytes stay in the blood vessels all the time? Is there a type of formed element that doesn’t? | 1) Yes. 2) Leukocytes. |
How do erythrocytes appear in a standard blood smear? What is their lifespan? | 1) They appear as a flattened biconcave disk with no nucleus that appears a pale red color. 2) 120 days. |
What is a reticulocyte? When are erthrocytes reticulocytes? Why? | 1) An immature erythrocyte that still contains remnants of organelles. 2) During their first day or two of circulation. 3) Erythrocytes don’t have organelles, and they extrude most of their organelles when they mature in the red bone marrow although this process is not complete by the time they enter the blood stream. |
What proteins do erthrocytes keep? Why? | 1) Some structural proteins. 2) To help them change their shape to squeeze through capillaries. |
What shape are erythrocytes? Describe it. | 1) Biconcave disks. 2) They are plump at the periphery and thin in the center. |
What do erythrocytes lack organelles? What are they biconcave in shape? | 1) So there will be more room for meoglobin molecules inside. 2) So that they have a greater surface area for gas exchange. |
What does hemoglobin do? What is hemoglobin? | 1) Transport gases. 2) A large molecule made up of proteins and iron. |
How does gas exchange happen in erythrocytes? | Oxygen diffuses into the plasma where it gets into the tissues from the capillaries via osmosis, and the carbon dioxide diffuses into the plasma in the capillary to be picked up by erythrocytes. |
What is a rouleaux? | A stack of erythrocytes that forms in a wider blood vessel. It looks like a roll of coins. |
What are the parts of hemoglobin? | Four folded chains made up of a protein called globin, that are bound to a red pigment molecule called heme (which contains the one iron ion). |
How many oxygen molecules can one hemoglobin molecule transport and why? How many molecules of oxygen can be transported by a erythrocyte? | 1) Four, each iron ion in the heme can bind to one oxygen molecule. 2) 1.2 billion. |
What is oxyhemoglobin? Deoxyhemoglobin? | 1) Hemoglobin in which oxygen is bound to the iron ions. 2) Hemoglobin that has already dropped off its oxygen and has no oxygen attached to the iron ions. |
What happens to the CO2 that has diffused into the plasma of the capillaries? | 76% dissolves into the plasma, and 24% binds to the amino acids in hemoglobin. |
What is carbaminohemoglobin? | Hemoglobin that has carbon dioxide bonded to its amino acids. |
What happens to patients that have insufficient hemoglobin? What happens to patients with polycythemia? | 1) Tissues don’t receive sufficient oxygen -> this is a form of anemia. 2) Blood viscosity is too high. |
How do medical professionals determine the oxygenation of tissues? | By measuring the percent saturation (percent sat), which is the percentage of hemoglobin sites that is occupied by oxygen. |
What is percent sat measured with? How does it work? What is a normal percent sat? | 1) A pulse oximeter. 2) It sends two wavelengths of light into a thin part of the body (usually the finger) and detects the light that exits. The way that hemoglobin absorbs light depends on oxygen saturation. 3) 95-100. |
What do the kidneys do when oxygen saturation is low? Why are they the ideal sites for receptors that determine the oxygen saturation of blood? | 1) EPO is released, which increases erythrocyte production. 2) They filter 20% of blood volume every day, and if there is less oxygen in the blood, less oxygen will pass through the kidneys. The kidneys know what is it the blood. |
Why do people have symptoms of hypoxia when they travel to high altitudes? | There is less oxygen in the air, and they don’t have enough erythrocytes to handle it. Eventually, they produce more erythrocytes and the symptoms vanish. |
What is the difference between hypoxia and hypoxemia? | Hypoxia refers to low oxygen levels in the tissues and hypoxemia refers to low oxygen levels in the blood. |
How many erythrocytes are produced per second? | 2 million cells per second. |
What trace elements are required for erythrocyte production? Why? | 1) Iron-iron is needed for hemoglobin. 2) Copper-it is a component of the plasma proteins hephaestin and ceruoloplasmin that are essential for hemoglobin production. 3) Zinc-it facilitates the synthesis of the heme production portion of hemoglobin. 4) B vitamins-folate and B12 facilitate DNA synthesis which is needed for all cell production not just erythrocyte production. |
How does bone marrow, the liver, and the spleen store iron for hemotopoises? | In ferritin and hemosiderin. |
How are worn out erythrocytes removed? What are they? | 1) By macrophages. 2) Myeloid phagocytic cells that remove worn out erythrocytes. |
What happens to hemoglobin after the erythrocyte is destroyed? | Globin is broken down into amino acids which are then sent back to the bone marrow to be recycled. Iron contained in heme is stored in the liver/spleen, or sent back to the bone marrow to be recycled. The non-iron portion of heme is turned into bilierdin (green pigment waste product) and then bilirubin (yellow pigment waste product). |
Why do bruises have color? Why does jaundice happen? | 1) Pigment breakdown from the non-iron portion of heme 2) Liver can’t filter out bilirubin so the yellow pigment waste product builds up in the blood. |
What are the three categories of anemia? | Faulty/decreased RBC production, blood loss, excessive destruction of RBCs. |
What are the two groupings of anemia that clinicians use in diagnosis? | The kinetic approach focuses on evaluating the production, destruction, and removal of RBCs, whereas the morphological approach examines the RBCs themselves, paying particular emphasis to their size. |
What does MCV stand for and what is it? | 1) Mean corpuscle volume. 2) A test that measures blood cell size. |
What are normal sized RBCs called? Small RBCs? Large RBCS? | 1) Normocytic. 2) Microcytic. 3) Macrocytic. |
What can reticulocyte counts tell us about anemia? | If the reticulocyte is down, it means that there is less RBC production. |
How does anemia affect the body? | If there isn’t enough RBCs or oddly shaped RBCs there are issues with enough oxygen getting to the tissues and organs of the body. |
What are blood loss anemias caused by? | Bleeding from wounds/lesions, ulcers, hemorrhoids, gastritis, cancers of the gastrointestinal tract, excessive menstruation, loss of blood during childbirth. |
What are the types of anemia caused by faulty/decreased RBC production? | Sickle cell anemia, iron deficiency anemia, vitamin deficiency anemia, and various diseases of the bone marrow/stem cells. |
What is sickle cell anemia? What groups is it common among? | 1) A genetic condition in which RBCs have a crescent shape caused by Hemoglobin S, which also delivers less oxygen to tissues. This odd shape causes the RBCs to get stuck in capillaries because they can’t deform, which blocks blood flow to tissues which in turn causes a who other host of issues. 2) People of african decent. |
What is iron deficiency anemia? What groups is it common among? | 1) The most common type of anemia, in which the amount of iron is too low to make sufficient heme. 2) Teens, children, vegans, vegetarians. |
What is vitamin deficient anemia? What are the subtypes? What groups is this common among? | 1) Anemia caused by insufficient vitamin B12 and folate. 2) Megaloblastic-deficient of B12 and folate, pernicious-poor B12 absorption. 3) Pregnant people, alcoholics, people with celiac disease. |
What are the consiquences vitamin deficiency anemia in pregnacy? How can this be prevented? | 1) Neurological defects, including spin abifida. 2) Supplementing with Folic Acid. |
What is aplastic anemia? What is thalassemia? | 1) A condition where there are deficient numbers of RBC stem cells, which are often caused by radiation, medication, chemotherapy, and infection. 2) An inherited condition typically occurring in individuals from the middle east/the mediterranean/africa/southeast asia, where RBCs don’t mature properly. Most severe form is Cooley’s Anemia. |
What does lead exposure do to bone marrow? | It causes the destruction of the red bone marrow. |
What diseases can lead to anemia? | Chronic kidney disease, hypothyroidism, some cancers, lupus, rheumatoid arthritis. |
What is the main consequence of polycythemia? What is it caused by? | 1) The blood viscosity becomes too high. 2) Dehydration, bone marrow disease (polycythemia vera). |
18.4-Leukocytes and Platelets.
Question: | Answer: |
What do leukocytes do? What do platelets do? | 1) Protect the body against invading microorganisms and cancer cells, clean up debris. 2) Repair blood vessels. |
How are leukocytes different from erythrocytes? | They are far less numerous, they have organelles (only formed element with them), have shorter lifespans, more types. |
Why do leukocytes have shorter lifespans than erythrocytes? | Their usage often causes them to die. |
Do leukocytes stay in the blood vessels? How would they leave? | 1) No. 2) They exit through the capillaries in a procces known as either emigration or diapedesis in which they squeeze through the vessel wall. |
What are emigration and diapedesis? | 1) Leukocytes leaving via the capillaries. 2) Leukocytes returning to the capillaries. |
What is positive chemotaxis? | Movement in response to chemical signals. |
What happens to leukocytes after they leave the capillaries? | They might take up fixed position in the lymphatic tissue, or they will move through tissue spaces waiting for a “911 call” from an injured or infected cells. |
What are the two types of leukocytes? What are these types determined by? | 1) Granular and agranular. 2) If their cytoplasm contains visible granules. |
What are granular leukocytes? What are the types that they include? | 1) A leukocyte with visible granules in their cytoplasm. 2) Neutrophils, eosinophils, and basophils. |
What are neutrophils? What percentage of leukocytes do they make up? How do they appear in blood smears? | 1) Leukocytes that are rapid responders to the site of infections, that are efficient phagocytes with a preference for bacteria. 2) 50-70%. 3)They have many fine granules that appear light lilac. They have chemically neutral stains. They will also have 2 to 5 lobes. |
How do the lobes of neutrophils change with age (of cell not person)? What does polymorphonuclear mean? | 1) Young/immature neutrophils are only begining to develope lobes, and the number of lobes increaces with time. 2) It is a word that refers to an old neutrophil that has many lobes. It means ‘a nucleas with many forms.’ |
What do the granules of neutrophils do? | They include an enzyme known as lysozyme which breaks down bacterial walls, and oxidents such as H202, as well as defensins (proteins that bind to and punctire bacterial and fungal plasma membranes. |
What does a high level of neutrophils indicated/what is it caused by? What does a low level of neurtophils indicate/what is it caused by? | 1) It indicates infection/inflamation caused particullary by bacteria, but it can also occur in burn patients or those under unsual stress. 2) It may be caused by drug toxicity and other disorders. |
What are eosinophils? What percentage of the total leukocyte count do they make up? How do they appear in stains? | 1) A type of granular leukocyte that targets paracites. 2) 2-4%. 3) They will have two to three lobes, and a red/orange color. They stain best with an acidic stain known as eosn. |
How do the sizes of eosinophils and neutrophils compare to the size of an erythrocyte? | They are both 10-12 millimeters in diameter, which is slightly larger than an erythrocyte. |
What do the granules of a eosinophil do? | They contain antihistamine molecules, as well as molecules that are toxic to paracitic worms. |
What is phagocytosis? ******** | the ingestion of bacteria or other material by phagocytes |
What are basophils? What percentage of the total leukocyte volume do they form? How do they appear on stains? | 1) A type of granular leukocytethat intensifies the inflammatory response. 2) <1%. 3) They have large granulars, and their nucleai have two lobes. They stain best with basic/alkaline stains. |
What do the granules of basophils do? | They release histamines (contribute to inflammation) and heparin (reduces clotting). |
What are high levels of basophils associated with? Low levels? | 1) Allergies, parasitic infections, and hypothyroidism. 2) Pregnancy, stress, and hyperthyroidism. |
What are high levels of eosinophils associated with? Low levels? | 1) Allergies, parasitic worm infections, and some autoimmune diseases. 2) Drug toxicity and stress. |
Do agranular leukocytes have granules? How do they differ from granular leukocytes? | 1) Yes, but they are not visible. 2) In addition to the invisible granules, they also have simple nucleauses with no lobes. |
What are the two main types of agranular leukocytes? | Lymphocytes and monocytes. |
What are lymphocytes? What is unique about their development? | 1) A type of agranular leukocyte that are essenstial for most of the immune response. 2) The only formed element of blood hat arises from lymphoid stem cells. They initially form in bone marrow and then mature in the lymphatic tissues. |
What percentage of leukocytes do lymphocytes make up? What are the three size ranges of lymphocytes? What type of lymphocyte is typically found in each category? | 1) 20-30%. 2) 6-9 mm-b or t cells. 10-14-no specific type, most lymphocytes fall here. 14-17-Natural Killer cells. |
What are the three major groups of lymphocytes? | Natural killer cells, B cells, and T cells. |
What are NK cells? What does NK stand for? | 1) Cells that kill all foreign cells (cancer cells, infected cells). They provide a non-specific immunity. 2) Natural Killer cells. |
What are B cells and T cells? | 1) A lymphocyte that produces antibodies and immunoglobins. They provide humoral immunity. 2) A lymphocyte that attacks diseased and foreign cells. They provide cellular level immunity. |
Can B cells and T cells be differentiated on a blood smear? | Not on a normal one. |
What do abnormally high lymphocyte counts mean? Abnormally low? | 1) Viral infections, some cancers. 2) Prolonged (chronic) illness or immunosuppression, including that caused by HIV infection and drug therapies that often involve steroids. |
What are monocytes? What percentage of leukocytes do they make up? What is their size? | 1) Leukocytes that originate from myeloid stem sells that are phagocytic cells. This means they break down infections by “eating” them. 2) 2-8%. 3) 12-20 mm. |
What do monocytes look like? | They have a horseshoe-shaped nuclei. |
What are macrophages? | Worn out monocytes that leave circulation and ohagocytize (read: eat). They eat debris, foreign pathogens, worn-out erythrocytes, and many other dead, worn out, or damaged cells. Macrophages also release antimicrobial defensins and chemotactic chemicals that attract other leukocytes to the site of an infection. |
What do high counts of monocytes are associated with? Low counts? | 1) Viral or fungal infections, TB, some forms of leukemia, and other chronic diseases. 2) Supression of bone marrow. |
What is leukemia? | A cancer involing an abundance of nonfunctional leukocytes. |
What is leukopenia? What is leukocytosis? | 1) A condition in which few leukocytes are produced. 2) A condition in which too many leukocytes are produced. |
What is lymphoma? | A form of cancer in which masses of malignant T and/or B lymphocytes collect in lymph nodes, the spleen, the liver, and other tissues. As in leukemia, the malignant leukocytes do not function properly, and the patient is vulnerable to infection. |
Are platelets cells? What are they? | 1) No, even though their official name ends in cyte. 2) A fragment of the cytoplasm of a cell called a megakaryoctye that is surrounded by a plasma membrane. |
What do megakaryocytes look like? What is their size? How do they contribute to platelet/thrombocyte production? | 1) They have an enlarged lobed nucleus. 2) They are 50-100 mm large. 3) Every megakaryocyte emits 2000-3000 platelets in its lifetime. |
How are platelets formed? | Thrombopoietin is secreted by the kidneys and liver, which stimulates the production of megakaryoblasts, which mature into megakeryocytes. They then splinter into cytoplasm fragments surrounded by a plasma membrane. |
What is the size and distribution of platelets? | 1) 2-4 mm in diameter. 2) 150,000-160,000 per mL of blood. |
What do platelets do? | Promote clotting, which stops us from bleeding out. They also secrete a variety of growth factors essential for growth and repair of tissue, particularly connective tissue. |
What is thrombocytosis? What is thrombocytopenia? | 1) Too many platelets -> unnecessary clots. 2) Too few platelets -> can cause excessive bleeding. |
18.5-Hemostasis
Question: | Answer: |
What is hemostasis? | The process by which the body seals a ruptured blood vessel and prevents further loss of blood. |
What are the three stages to hemostasis? What will happen if hemostasis fails? | 1) Vascular spasm, the formation of a platelet plug, and coagulation. 2) Hemorrhage. |
What is vascular spasm? When does it occur? | 1) The smooth muscle layers of the vessel contract dramatically, limiting blood flow (circular layers) and the vessel is drawn back into the surrounding tissue (longitudinal muscle). 2) When a vessel is punctured or severed. |
What is the platelet plug? How does it form? | 1) A temporary blockage in an artery or vein that prevents bleeding when it is severed or puncture. 2) Platelets encounter the area of rupture and begin to pile up, all while releasing chemicals that call more platelets. |
What chemicals do platelets release during the formation of the platelet plug and what are they used for? | 1) Adenosine diphosphate (ADP), which helps additional platelets to adhere to the injury site, reinforcing and expanding the platelet plug 2) Serotonin, which maintains vasoconstriction 3) Prostaglandins and phospholipids, which also maintain vasoconstriction and help to activate further clotting chemicals, as discussed next. |
What is coagulation? Why is it classified as a cascade? | 1) The formation of a blood clot. 2) One event prompts the next. |
What is the result of coagulation? | A gelatinous but robust clot made of a mesh of fibrin that catches blood cells and platelets. |
What are the two pathways that coagulation is initiated by? Define them. How do they merge? | 1) Extrinsic pathway-triggered by trauma. 2) Intrinsic pathway-begins in the bloodstream, is triggered by internal damage to the wall of the vessel. 3) In the common pathway. |
What are clotting factors? What are they released by? | 1) Chemicals that trigger and aid in coagulation. 2) The liver and the platelets/ |
What are the 12 clotting factors and why are 13 listed? | 1) Fibrinogen, prothrombin, tissue thromboplastin, calcium ions, proaccerlarin, proconvertin, antihemolytic factor A, Antihemolytic factor B (plasma thromboplastin component), Stuart–Prower factor (thrombokinase), Antihemolytic factor C (plasma thromboplastin antecedent), Hageman factor, Fibrin-stabilizing factor. 2) Factors 5 and 6 were thought to be different but it was later discovered that theyre the same. 6 is kept as a placeholder. |
What happens in the extrinsic pathway? | Upon contact with blood plasma, the damaged extravascular cells, which are extrinsic to the bloodstream, release factor III (thromboplastin). Sequentially, Ca2+ then factor VII (proconvertin), which is activated by factor III, are added, forming an enzyme complex. This enzyme complex leads to activation of factor X (Stuart–Prower factor), which activates the common pathway discussed below. |
What happens in the intrinsic pathway? How long does it take to complete? | 1) Initiated when factor XII (Hageman factor) comes into contact with foreign materials. Within the body, factor XII is typically activated when it encounters negatively charged molecules, such as inorganic polymers and phosphate produced earlier in the series of intrinsic pathway reactions. Factor XII sets off a series of reactions that in turn activates factor XI (antihemolytic factor C or plasma thromboplastin antecedent) then factor IX (antihemolytic factor B or plasma thromboplasmin). In the meantime, chemicals released by the platelets increase the rate of these activation reactions. Finally, factor VIII (antihemolytic factor A) from the platelets and endothelial cells combines with factor IX (antihemolytic factor B or plasma thromboplasmin) to form an enzyme complex that activates factor X (Stuart–Prower factor or thrombokinase), leading to the common pathway. 2) The events in the intrinsic pathway are completed in a few minutes. |
What happens in the common pathway? | vessel. Once factor X has been activated by either the intrinsic or extrinsic pathway, the enzyme prothrombinase converts factor II, the inactive enzyme prothrombin, into the active enzyme thrombin. Then, thrombin converts factor I, the soluble fibrinogen, into the insoluble fibrin protein strands. Factor XIII then stabilizes the fibrin clot. |
What is fibrinolysis? | Graduale degradation of the clot. |
What is the process by which a clot fully blocks a blood vessel? | Contractile proteins within the platelets, which pull the edges of the clot closer to the edge of the vessel. |
What happens to plasminogen in fibrinolysis? How does it impact the clot? | 1) It is changed from its inactive form to plasmin. 2) It breaks down the fibrin of the clot. |
What is an anticoagulant? What do they do? | 1) A subject that opposes coagulation (blood clotting). 2) They will inactivate coagulants. |
What does the protein C system do? What does TFPI stand for and what does it do? | 1) It inactivates the clotting factors in the intrinsic pathway. 2) Tissue factor pathway inhibitor-inhibits the conversion of the inactive factor VII to the active form in the extrinsic pathway. |
What does anthrombin do? What does heparin do? | 1) Inactivates factor X, opposes the conversion of prothrombin (factor II) to thrombin in the common pathway. 2) opposes prothrombin. |
What is hemophilia? What does it do to your body? | 1) Either factors VIII, IX, or XI are deficient. There are three types (A, B, and C), and they are each a different coagulent deficiency. 2) Prevents the body from forming clots, and so they bleed from even the most minor of injuries. |
What is thrombosis? | Excessive clot formation, clots form in undamaged or only slightly damaged blood vessels. |
Whar is a mural thrombus? An occlusive thrombus? | 1) A clot found in larger arteries or veins that only partially blocks flow. 2) A clot that completely blocks smaller artery or vein. |
What usually causes thrombi to form? | Vessel damage to the endothelial lining, which includes venous stasis (blood in the veins of the lower body staying still for a long time). |
What is thrombophilia? What is it also known as? | 1) A condition where there is a tendency to form thrombosis. 2) Hypercoagulation. |
What is an embolus? When does it turn into an embolism? Why is it dangerous? | 1) A piece of a thrombus that breaks free from the vessel wall and it carried along with the bloodstream. 2) When it gets stuck again. 3) It could block a major artery to the brain, heart, or lungs, which causes a heart attack, stroke, or pullmonary embolism. |
Why does one take asprin if they believe they are having a heart attack? | It is an anticoagulant, which might break down the thrombus which could cause a heart attack. |
What class of drugs helps speed up the degradation of an abnormal clot? Why is it important to determine the cause of a stroke before it is administrated in this cause? | 1) Thrombolytic agents. 2) Some strokes are caused by hemorrhage, so thrombolytic agents would make it much worse. |
18.6-Blood Typing
Question: | Answer: |
What is blood type determined by? | The presence or absence of specific marker molecules (antigens) on the plasma membranes of erythrocytes. |
Why is it an issue if someone gets blood thats not the right type? | The antigens on foreign blood cells aren’t the same as cells that actually belong to the body, and antibodies destroy the erythrocytes which releases hemoglobin which the kidneys need to process and if theres too much for the kidneys to process they could fail. |
What is aggultination? Why is it bad? | 1) The process in which Y shaped antibodies latch onto foreign erythrocytes and cause them to clump together. 2) This blocks arteries and veins, which deproves tissues of oxygen and nutrients. |
What is hemolysis? | The process by which hemoglobin from RBCs that have been destroyed is returned to the bloodstream. |
What are the two blood groups? | ABO and Rh. |
What are the types of ABO blood? What antigens does this concern? How is ABO blood type determined? | 1) A, B, AB, and O. 2) Antigens A and B-A has A, B has B, AB has both, and O has none. 3) Genetically. |
Why does the human body have antibodies for A and B antigens? | Because they are found in nature, and in food, so the body has been exposed to them and has developed an antibody. |
What are the types of Rh blood? What determines Rh blood type? | 1) Rh+ and Rh- 2) If there is the Rh D antigen on the erythrocytes. |
In what individuals are anti-Rh D antibodies produced? | People negative for Rh D. |
What does HDN stand for? What is it? | 1) Hemolytic disease of the newborn. 2) When a Rh- mother has a Rh+ baby and the antibodies from the mother attack the baby’s erythrocytes. |
What is RhoGAM? What does it stand for? | 1) A medication given to a Rh- mother having a Rh+ baby in order to suppress the antibodies that attack Rh-D. 2) Rh immune globulin. |
How do clinicians determine blood type? | By taking a blood sample and adding commercially produced antibodies. If the wrong one gets added, there will be visible aggulination of the cells. |
What is the ideal blood type transfussion scenario? What happens in emergencies? | 1) Some gets blood type that matches them exactly. B+ gets B+ 2) O- is used, because it has no antigens to let it be attacked. Known as the universal doner. |
What is the one issue with using O- blood? | It contains antibodies for everything, so there is some introduction of antibodies but in a very small amount. |
What is the universal recipient? | AB+ |