M3 - Physio Psych [REVIEWER]
LESSON 1 - THE CONTROL AND MECHANISM OF MOVEMENT
MUSCLES AND THEIR MOVEMENTS
Three vertebrate muscles:
Smooth muscles - control the digestive system and other organs
Skeletal or striated muscles - control movement of the body in relation to the environment
cardiac muscles - control the heart
♣ Smooth muscles - control internal organs
long thin cells
♣ Skeletal or striated muscles control movement of body in relation to the environment
long cylindrical with stripes
neuromuscular junction: synapse of motor neuron with muscle fiber
axons release acetylcholine at synapse
♣ each muscle moves in one direction and in absence of acetylcholine, it relaxes
♣ movement in two directions requires antagonistic muscles: flexor to raise arm and extensor to lower arm
Neuromuscular junction
- synapse between a motor neuron axon and a muscle fiber.
In skeletal muscles, every axon releases acetylcholine at the neuromuscular junction, and acetylcholine always excites the muscle to contract.
A deficit of acetylcholine or its receptors impairs movement. Each muscle makes just one movement, a contraction. There is no message to cause relaxation; the muscle relaxes when it receives no message to contract.
Moving a leg or arm back and forth requires opposing sets of muscles, called antagonistic muscles.
At your elbow, for example, your flexor muscle brings your hand toward your shoulder and your extensor muscle straightens the arm.
♣ Cardiac or heart muscles
fibers that fuse together at points
somewhat between smooth and skeletal muscles
♣ Myasthenia Gravis is autoimmune disease
immune system antibodies attack acetylcholine receptors;
weakness and rapid fatigue of muscles because motor neurons can’t constantly produce maximum acetylcholine
treated by drugs that inhibit acetylcholinesterase to prolong acetylcholine
Vertebrate muscles
(a) Smooth muscle, found in the intestines and other organs, consists of long, thin cells.
(b) Skeletal, or striated, muscle consists of long cylindrical fibers with stripes.
(c) Cardiac muscle, found in the heart, consists of fibers that fuse together at various points. Because of these fusions, cardiac muscles contract together, not independently.
NOTES:
The biceps of the arm is a flexor. The triceps is an extensor
Movements can be more precise where each axon innervates only a few fibers, as with eye muscles, than where it innervates many fibers, as with biceps muscles.
Slow-twitch fibers do not fatigue because they are aerobic—they use oxygen during their movements. You can think of them as “pay as you go.”
Prolonged use of fast-twitch fibers results in fatigue because the process is anaerobic— using reactions that do not require oxygen at the time but need oxygen for recovery. Using them builds up an oxygen debt. Imagine yourself bicycling. At first your activity is aerobic, using your slow-twitch fibers. However, your muscles use glucose, and after a while your glucose supplies begin to dwindle. Low glucose activates a gene that inhibits the muscles from using glucose, thereby saving glucose for the brain’s use. You start relying more on the fast-twitch muscles that depend on anaerobic use of fatty acids.
Muscle types:
fast-twitch fibers with fast contractions and rapid fatigue to slow-twitch fibers with less vigorous contractions and no fatigue.
♣ Proprioceptors control the movement.
(from the Latin proprius,
meaning “one’s own”) is a receptor that detects the position or movement of a part of the body—in these cases, a muscle.
Muscle proprioceptors
detect the stretch and tension of a muscle and send messages that enable the spinal cord to adjust its signals. When a muscle is stretched, the spinal cord sends
a signal to contract it reflexively. This stretch reflex is caused by a stretch; it does not produce one.
One kind of proprioceptor is the muscle spindle, a receptor parallel to the muscle that responds to a stretch. Whenever
the muscle is stretched more than the antagonistic muscle, the muscle spindle sends a message to a motor neuron in the spinal cord, which in turn sends a message back to the muscle, causing a contraction). Note that this reflex provides for negative feedback: When a muscle and its spindle are stretched, the spindle sends a message that results in a muscle contraction that opposes the stretch.
The sensory nerves of the spindles send action potentials to the motor neuron in the spinal cord, and the motor neuron sends action potentials to the extensor muscle.
Golgi tendon organs (another kind of proprioceptors)
respond to increases in muscle tension. Located in the tendons at opposite ends of a muscle, they act as a brake against an excessively vigorous contraction.
Golgi tendon organs detect the tension that
results during a muscle contraction. Their impulses travel to the spinal cord, where they excite interneurons that inhibit the motor neurons. In short, a vigorous muscle contraction inhibits further contraction by activating the Golgi tendon organs.
VOLUNTARY AND INVOLUNTARY MOVEMENTS
♣ Reflexes such as the stretch reflex or constriction of pupil to light are involuntary
infant reflexes include rooting, grasp, and Babinski
allied reflexes are strong in infants and still in adults, e.g., sneezing, closing eyes in strong sunlight
♣ Reflexes are consistent automatic responses to stimuli.
♣ Most movements, e.g., walking, are a combination of voluntary and involuntary muscle control
involuntarily adjust to irregularities in road and automatically swing your arms
SENSITIVITY TO FEEDBACK
♣ Ballistic movements, e.g., reflexes, cannot be altered once started
♣ Central pattern generators
neural mechanisms in spinal cord and elsewhere that generate rhythmic patterns, e.g., wing flapping in birds and fin movements in fish
started by stimulus but motor program sets frequency of movement, e.g., cats scratch themselves 3-4 times/sec
♣ Motor program is a fixed sequence of movements
Ex: cat washing face, gymnast with complex movements, yawn
automatic patterns may be disrupted when thinking about them, e.g., typing or playing piano
evolutionary holdover: chicken still flaps wings when dropped even though can’t fly
ROLE OF CEREBRAL CORTEX
♣ Cerebral cortex important for complex actions such as writing
less voluntary movements e.g., coughing, laughing, crying are controlled by subcortical areas
♣ Stimulation of primary motor cortex elicits certain outcome movements in corresponding body area
500 msec stimulation of arm region of monkey results in grasping movement and moving hand toward head
also, finger area of cortex active when pianist hears music
Since the pioneering work of Gustav Fritsch and Eduard Hitzig (1870), neuroscientists have known that direct electrical stimulation of the primary motor cortex—the precentral gyrus of the frontal cortex, just anterior to the central sulcus —elicits movements. The motor cortex does not send messages directly to the muscles. Its axons extend to the brainstem and spinal cord, which generate the impulses that control the muscles.
♣ Prefrontal cortex active when planning and calculating possible outcomes of a
movement
damage results in badly planned movements, showering with clothes on, salting tea instead of food, etc.
inactive during dreaming and dreams are usually haphazard
♣ Premotor cortex is active during preparations for a movement
receives information about target and body location
♣ Supplementary motor cortex active during preparations for a rapid series of movements; typing, dancing, speaking, playing musical instrument
♣ Posterior parietal cortex keeps track of position of body relative to
environment
if damaged we can describe what we see but can’t walk toward it, pick it up, or step over object
♣ Primary somatosensory cortex is main receiving area for touch and other
body information
responds to shape of object and grasping, lifting or lowering
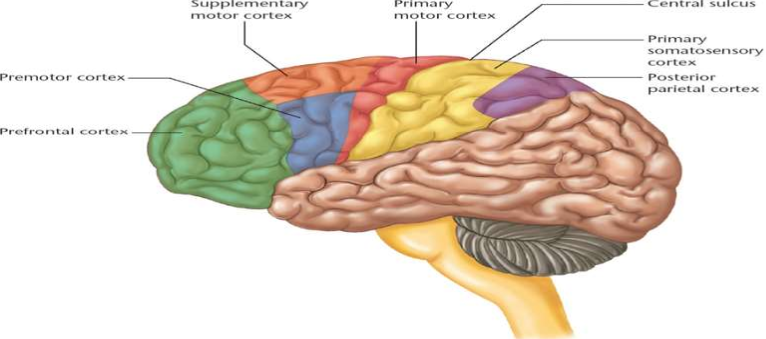
Figure 8.8 Principal areas of the motor cortex in the human brain. Cells in the premotor cortex and supplementary motor cortex are active during the planning of movements, even if the movements are never actually executed. (Kalat,2018)
CONNECTIONS FROM BRAIN TO SPINAL CORD
♣ Messages from brain reach the medulla and spinal cord through dorsolateral or ventromedial tracts
♣ Dorsolateral (pyramidal tract)
originate from primary motor cortex, surrounding areas and red nucleus
in pyramids of medulla, axons cross over to opposite side of spinal cord but contralateral
control develops gradually
clumsiness in children with cerebral palsy comes from competition between contralateral and ipsilateral paths
♣ controls movement in hands, fingers, toes
♣ damage here means loss of fine movements
♣ Ventromedial tract
includes axons from the primary and supplementary motor cortex, midbrain tectum, reticular formation and vestibular nucleus
do not cross to contralateral side because axons control bilateral movement of the neck, shoulders, and trunk
damage here impairs walking, turning, bending, standing up and sitting down
Paths from the cerebral cortex to the spinal cord are called the corticospinal tracts. We have two such tracts, the lateral and medial corticospinal tracts. Both tracts contribute in some way to nearly all movements, but certain movements
rely on one tract more than the other.
The lateral corticospinal tract is a pathway of axons from the primary motor cortex, surrounding areas of the cortex, and from the red nucleus, a midbrain area that controls certain aspects of movement.
Axons of the lateral tract extend directly from the motor cortex to their target neurons in the spinal cord. In bulges of the medulla
called pyramids, the lateral tract crosses to the contralateral opposite) side of the spinal cord. (For that reason, the lateral tract is also called the pyramidal tract.) It controls movements in peripheral areas, especially the hands and feet.
The medial corticospinal tract includes axons from many parts of the cerebral cortex, not just the primary motor cortex and its surrounding areas. The medial path also
includes axons from the midbrain tectum, the reticular formation, and the vestibular nucleus, a brain area that receives
input from the vestibular system.
Functions of the lateral and medial tracts:
The lateral tract controls muscles in the
lateral parts of the body, such as hands and feet.
The medial tract controls muscles in the medial parts of the body, including trunk and neck.
ROLE OF CEREBELLUM
♣ Important for motor control and has more neurons than rest of brain
♣ Enhances new motor programs and skills
♣ Processes information about guiding movement, not the movement itself
active when weighing objects with hands or when objects rub hands
♣ Damage causes difficulty with:
rapid, ballistic movements, sequences that require accurate aiming and timing, e.g., tapping rhythm, speaking, writing, playing musical instrument
finger-to-nose task: initial rapid movement may strike face or hold segment of task may
waver, as when intoxicated
judging differences in delay in pairs of tones
normal shifting of attention within 100 msec: may take up to a second
♣ Damage does not affect controlling force of movement or judging loudness of tones
CELLULAR ORGANIZATION IN CEREBELLUM
♣ Receives input from the spinal cord, sensory systems through the cranial nerve nuclei, and from the cerebral cortex
♣ Cells are arranged in precise, repeating geometric patterns
♣ Purkinje cells are very flat and exist in sequential planes
• parallel fibers are perpendicular to the planes of the Purkinje cells
• parallel fibers excite Purkinje cell
the more excited, the longer the duration of the Purkinje output which may control either a movement or a cognitive process
NOTE: Parallel fibers (yellow) activate one Purkinje cell after another. Purkinje cells (red) inhibit a target cell in one of the nuclei of the cerebellum. The more Purkinje cells that respond, the longer the target cell is inhibited. In this way, the cerebellum controls the duration of a movement.
ROLE OF BASAL GANGLIA
♣ Basal ganglia: group of large subcortical structures in the forebrain
♣ caudate nucleus and putamen receive input from thalamus and cortex
♣ globus pallidus sends information to the thalamus where it goes on to the motor and
premotor cortices
♣ stores sensory information to guide movements, learn rules and organize sequences of movements into a smooth, automatic whole
Organize action sequence into chunks or units like learning to drive a car (habit learning)
♣ Active in selection or inhibition of movements, e.g.:
surgery patients had activity when they made a movement with finger in response to signal
drawing a new line on computer
♣ Linked to obsessive-compulsive disorder
OCD is marked by repetitive thoughts and actions that person knows is pointless or nonsensical
OCD increases activity in caudate nucleus and this may be linked to strong habits
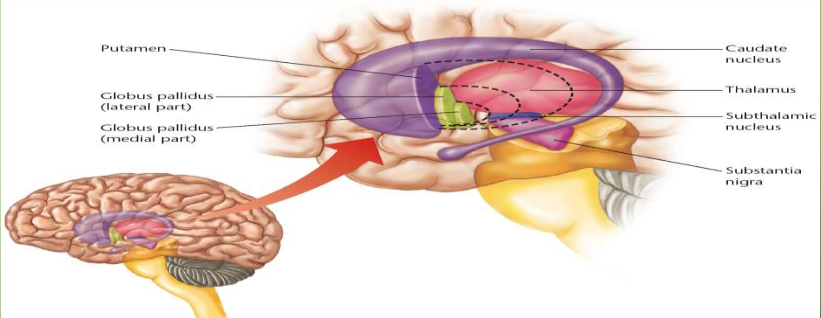
Figure 8.15 Location of the basal ganglia. The basal ganglia surround the thalamus and are surrounded by the cerebral cortex (Kalat, 2018).
LESSON 2 - THE MECHANISM OF WATER REGULATION,
DIGESTION AND FOOD SELECTION
THIRST
♣ Water constitutes 70% of the mammalian body.
♣ Water in the body must be regulated within narrow limits.
♣ The concentration of chemicals in water determines the rate of all chemical reactions in the body.
♣ Mechanisms of water regulation vary for
humans.
♣ Water can be conserved by:
Excreting concentrated urine.
Decreasing sweat and other autonomic responses.
♣ Most often water regulation is accomplished via drinking more water than we need and excreting the rest.
♣ Vasopressin is a hormone released by the posterior pituitary which raises blood pressure by constricting blood vessels.
helps to compensate for the decreased water volume.
♣ Vasopressin is also known as an antidiuretic hormone because it enables the kidneys to reabsorb water and excrete highly concentrated urine.
♣ Two different kinds of thirst include:
Osmotic thirst – a thirst resulting from eating salty foods.
Hypovolemic thirst – a thirst resulting from loss of fluids due to bleeding or sweating.
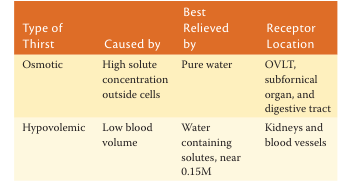
Each kind of thirst motivates different kinds of behaviors.
♣ Eating salty food causes sodium ions to spread through the blood and extracellular fluid of the cell.
♣ The higher concentration of solutes outside the cell results in osmotic pressure, drawing water from the cell to the extracellular fluid.
♣ Certain neurons detect the loss of water and trigger osmotic thirst to help restore the body to the normal state.
When osmotic thirst is triggered, water that you drink has to be absorbed through the digestive system.
To inhibit thirst, the body monitors swallowing and detects the water contents of the stomach and intestines.
♣ Hypovolemic thirst is thirst associated with low volume of body fluids.
Triggered by the release of the hormones vasopressin and angiotensin II, which constrict blood vessels to compensate for a drop in blood pressure.
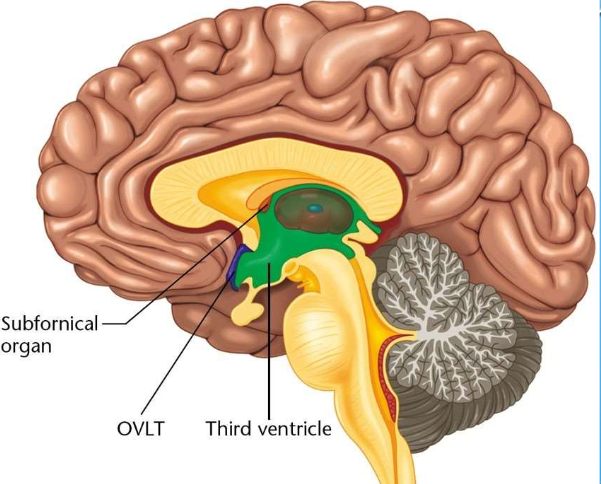
♣ Angiotensin II stimulates neurons in areas
adjoining the third ventricle.
♣ Neurons in the third ventricle send axons to the hypothalamus where angiotensin II is also released as a neurotransmitter.

HUNGER
The brain regulates eating through messages from the mouth, stomach, intestines, fat cells and elsewhere.
The desire to taste and other mouth sensations, such as chewing, are also motivating factors in hunger and satiety.
Sham feeding experiments, in which everything an animal eats leaks out of a tube connected to the stomach or esophagus, do not produce satiety.
The duodenum is the part of the small intestine where the initial absorption of significant amounts of nutrients occurs.
Distention of the duodenum can also produce feelings of satiety.
The duodenum also releases the hormone cholecystokinin (CCK), which helps to regulate hunger.
Cholecystokinin (CCK) released by the duodenum regulates hunger by:
– Closing the sphincter muscle between the stomach and duodenum and causing the stomach to hold its contents and fill faster.
– Stimulating the vagus nerve to send a message to the hypothalamus that releases a chemical similar to CCK.
Glucose, insulin, and glucagon levels also influence feelings of hunger.
• Most digested food enters the bloodstream as glucose, an important source of energy for the body and nearly the only fuel used by the brain.
• When glucose levels are high, liver cells convert some of the excess into glycogen and fat cells convert it into fat.
• When low, the liver converts glycogen back into glucose.
♣ Insulin is a pancreatic hormone that enables glucose to enter the cell.
Insulin levels rise as someone is getting ready for a meal and after a meal.
In preparation for the rush of additional glucose about to enter the blood, high insulin levels let some of the existing glucose in the blood to enter the cells.
Consequently, high levels of insulin generally decrease appetite.
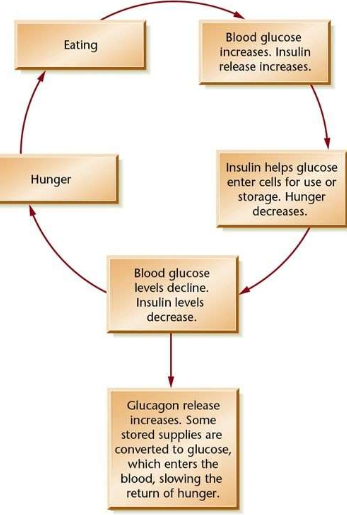
Glucagon is also a hormone released by the pancreas when glucose levels fall.
Glucagon stimulates the liver to convert some of its stored glycogen to glucose to replenish low supplies in the blood.
As insulin levels drop, glucose enters the cell more slowly and hunger increases.
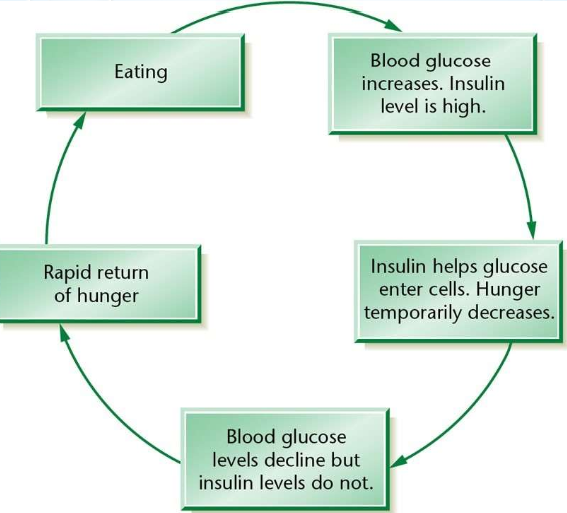
If insulin levels constantly stay high, the body continues rapidly moving blood glucose into the cells long after a meal.
Blood glucose drops and hunger increases in spite of the high insulin levels.
Food is rapidly deposited as fat and glycogen.
The organism gains weight.
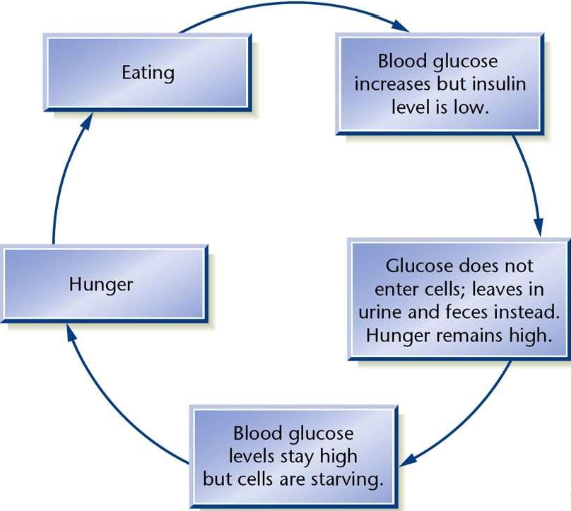
In people with diabetes, insulin levels remain constantly low, but blood glucose levels are high.
People eat more food than normal, but excrete the glucose unused and lose weight.
Long-term hunger regulation is accomplished via the monitoring of fat supplies by the body.
The body’s fat cells produce the peptide leptin, which signals the brain to increase or decrease eating.
Low levels of leptin increase hunger
High levels of leptin do not necessarily decrease hunger.
Most people are obese because they are less sensitive to leptin.
Some people are obese because of a genetic inability to produce leptin.
At the age of weaning, most mammals lose the intestinal enzyme lactase, which is necessary for metabolizing lactose.
Lactose is the sugar found in milk.
Milk consumption after weaning can cause gas and stomach cramps.
Declining levels of lactase may be an evolutionary mechanism to encourage weaning.
A carnivore eats meat and necessary vitamins are found in the meat consumed.
• Herbivores exclusively eat plants.
• Omnivores eat both meat and plants.
Herbivores and omnivores must distinguish between edible and inedible substances to find sufficient vitamins and minerals.
Selecting foods to eat is usually accomplished via imitation of others.
Other strategies of selecting food include:
– Selecting sweet foods and avoiding bitter
foods.
– Preferring things that taste familiar.
– Learning from consequences that happen
after a food is consumed.
♣ A conditioned taste aversion is a distaste for food that develops if the food makes one ill.
Lesson 3 - The Movement Disorders and Eating Disorders
Movement Disorders
Parkinson’s Disease:
Gradual progressive death of neurons especially in substantia nigra
decrease in dopamine results in decreased excitation of cerebral cortex
Symptoms begin when neurons decrease 20%-30%
slow on cognitive tasks
some depression and cognitive deficits but no emotional outbursts
rigidity, muscle tremors, slow movements and difficulty initiating physical and mental activity
- but patients function well with visual cues, e.g., follow parade, climb stairs and step on lines at fixed intervals
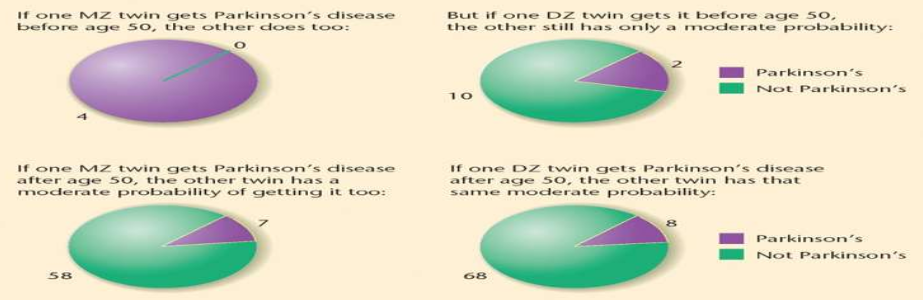
Figure 8.18 Probability of developing Parkinson’s disease if you have a twin who developed the disease before or after age 50. Having a monozygotic (MZ) twin develop Parkinson’s disease before age 50 means that you are very likely to get it too. A dizygotic (DZ) twin who gets it before age 50 does not pose the same risk. Therefore early-onset Parkinson’s disease shows a strong genetic component. However, if your twin develops Parkinson’s disease later (as is more common), your risk is the same regardless of whether you are a monozygotic or dizygotic twin. Therefore late-onset Parkinson’s disease has little or no heritability. (Source: Based on data of Tanner et al., 1999.)
L-Dopa Treatment
Most common treatment precursor for dopamine that crosses blood-brain barrier effective in early to intermediate stages but some patients do not benefit at all does not stop progression of the disease, may do harm side effects: nausea, restlessness, sleep problems, low blood pressure, hallucinations, and delusions
Huntington’s Disease:
♣ Severe neurological disorder striking 1 in 10,000
♣ Extensive damage to caudate nucleus, putamen, and globus pallidus, and some in the cerebral cortex
♣ Symptoms most often appear between 30-50 years
♣ begin with jerky arm movements, then facial twitch, later tremors spread and develop into writhing
♣ cannot learn new or improve movements
includes depression, memory impairment, anxiety, hallucination may be misdiagnosed as schizophrenic
Eating Disorders
♣ include extreme emotions, attitudes, and behaviors surrounding weight and food issues.
♣ Anorexia nervosa:
is an eating disorder associated with an unwillingness to eat as much as needed.
Genetic predisposition is likely, but no clear link has been established.
Associated with a fear of becoming fat and not a disinterest in food.
Biochemical abnormalities in the brain and blood are probably not the cause, but a result of the weight loss.
♣ Bulimia nervosa:
is an eating disorder in which people alternate between extreme dieting and binges of overeating.
Some force vomiting after eating.
Associated with decreased release of CCK, increased release of
ghrelin, and alterations of several other hormones and transmitters.
Reinforcement areas of the brain are also implicated.
♣ BINGE EATING DISORDER (also known as COMPULSIVE OVEREATING):
Characterized primarily by periods of uncontrolled eating beyond the point of feeling comfortably full.
While there is no purging, there may be sporadic fasts or repetitive diets and often feelings of shame or self-hatred after a binge.
People who overeat compulsively may struggle with anxiety, depression, and loneliness, which can contribute to their unhealthy episodes of binge eating.
SUMMARY AND NOTES TO REMEMBER:
LESSON 1
Vertebrates have smooth, skeletal, and cardiac muscles.
2. All nerve–muscle junctions rely on acetylcholine as their neurotransmitter.
3. Skeletal muscles range from slow muscles that do not fatigue to fast muscles that fatigue quickly. We rely on the slow muscles most of the time, but we recruit the fast muscles for brief periods of strenuous activity.
4. Proprioceptors are receptors sensitive to the position and movement of a part of the body. Two kinds of proprioceptors, muscle spindles and Golgi tendon organs, help regulate muscle movements.
5. Some movements, especially reflexes, proceed as a unit,
with little if any guidance from sensory feedback. Other
movements, such as threading a needle, are guided and redirected by sensory feedback.
Central pattern generators produce fixed sequences of behaviors with a fixed rhythm.
The primary motor cortex provides most of the output to the medulla and spinal cord.
Motor neurons in the medulla and spinal cord control muscle contractions. Pathways from the primary motor cortex, other cortical areas, midbrain, and medulla control those motor neurons.
prefrontal cortex and the supplementary motor cortex are also important for planning and organizing a rapid sequence of movements
mirror neurons, which are active both during preparation for a movement and while watching someone else perform the same or a similar movement.
The basal ganglia surround the thalamus and are surrounded by the cerebral cortex.
The indirect pathway has extra connections within the globus pallidus and back and forth to the subthalamus.
On average, the brain’s readiness potential began at least 300 ms before the reported decision, which occurred 200 ms before the movement
The primary motor cortex is the main source of brain input to the spinal cord. The spinal cord contains central pattern generators that actually control the muscles.
Each area of the motor cortex is closely aligned with a portion of the somatosensory cortex that pertains to the same body part.
The primary motor cortex produces patterns representing the intended outcome, not just the muscle contractions.
Areas near the primary motor cortex—including the prefrontal, premotor, and supplementary motor cortices—are active in detecting stimuli for movement and preparing for a movement.
The ability to inhibit inappropriate behavior develops gradually in children and adolescents, depending on maturation of the prefrontal cortex and basal ganglia.
Mirror neurons in various brain areas respond to both a self-produced movement and an observation of a similar movement by another individual. Their role in imitation and social behavior is uncertain. In many, possibly all, cases they develop their properties by learning, and they may be a result of imitation more than a cause of it.
The lateral tract, which controls movements in the periphery of the body, has axons that cross from one side of the brain to the opposite side of the spinal cord. The medial tract controls bilateral movements near the midline of the body
The cerebellum is critical for movements that require accurate aim and timing.
The cerebellum has multiple roles in behavior, including sensory functions related to perception of the timing or rhythm of stimuli.
The cells of the cerebellum are arranged in a regular pattern that enables them to produce outputs of precisely controlled duration.
The basal ganglia are a group of large subcortical structures that are important for self-initiated behaviors. The basal ganglia process information about probable rewards and thereby regulate the vigor of responses.
The learning of a motor skill depends on changes occurring in both the cerebral cortex and the basal ganglia.
When people identify the instant when they formed a conscious intention to move, their time precedes the actual movement by about 200 ms but follows the start of motor cortex activity by about 300 ms. However, it is not clear how accurately people can report the time of a conscious decision. A voluntary decision to move develops gradually, not suddenly
Parkinson’s disease and Huntington’s disease both result from brain deterioration that includes the basal ganglia.
Parkinson’s disease is characterized by impaired initiation of activity, slow and inaccurate movements, tremor, rigidity, depression, and cognitive deficits.
Parkinson’s disease is associated with the degeneration of dopamine-containing axons from the substantia nigra to the caudate nucleus and putamen.
Researchers have identified many gene variants that increase the risk of Parkinson’s disease, although none of them by itself has a major effect.
The chemical MPTP selectively damages neurons in the substantia nigra and leads to the symptoms of Parkinson’s disease. Some cases of Parkinson’s disease may result in part from exposure to toxins.
The most common treatment for Parkinson’s disease is L-dopa, which crosses the blood–brain barrier and enters neurons that convert it into dopamine. However, the effectiveness of L-dopa varies, and it produces unwelcome side effects.
Huntington’s disease is a hereditary condition marked by deterioration of motor control as well as apathy, depression, memory impairment, and other cognitive disorders.
By examining a gene on chromosome 4, physicians can determine whether someone is likely to develop Huntington’s disease later in life. The more C-A-G repeats in the gene, the earlier the likely onset of symptoms.
The gene responsible for Huntington’s disease alters the structure of a protein, known as huntingtin. Inhibiting the production of that protein is a theoretically possible treatment.
LESSON 2 & LESSON 3
Mammalian species have evolved ways of maintaining body water, ranging from frequent drinking (beavers) to extreme conservation of fluids (gerbils). Humans alter their strategy depending on the availability of acceptable fluids.
An increase in the osmotic pressure of the blood draws water out of cells, causing osmotic thirst. Neurons in the OVLT and subfornical organ detect changes in osmotic pressure and send information to hypothalamic areas responsible for vasopressin secretion and for drinking.
The subfornical organ initiates thirst in anticipation of future need, such as during a meal and shortly before
bedtime. It decreases thirst after drinking, long before the ingested water reaches the cells that need it.
Loss of blood volume causes hypovolemic thirst. To satisfy hypovolemic thirst it is necessary to drink water containing solutes.
Loss of blood volume causes hypovolemic thirst. To satisfy hypovolemic thirst it is necessary to drink water containing solutes.
Loss of sodium salts from the body triggers a craving for salty tastes.
Appetite depends partly on the availability of glucose and other nutrients to the cells. The hormone insulin increases the entry of glucose to the cells, including cells that store nutrients for future use. Glucagon mobilizes stored fuel and converts it to glucose in the blood. Thus, the combined influence of insulin and glucagon determines how much glucose is available at any time.
Fat cells produce a peptide called leptin, which provides the brain with a signal about weight loss or gain and therefore corrects day-to-day errors in the amount of feeding. Low levels of leptin increase hunger more effectively than high levels decrease it.
The arcuate nucleus of the hypothalamus receives signals of both hunger and satiety. Good-tasting foods and the transmitter ghrelin stimulate neurons that promote hunger. Glucose, insulin, leptin, and CCK stimulate neurons that promote satiety.
Axons from the two kinds of neurons in the arcuate nucleus send competing messages to the paraventricular nucleus, releasing neuropeptides that are specific to the feeding system. Cells in the paraventricular nucleus inhibit the lateral nucleus of the hypothalamus. Hunger signals increase feeding by decreasing the inhibition from the paraventricular nucleus.
The lateral nucleus of the hypothalamus facilitates feeding by axons that enhance taste responses elsewhere in the brain and increase the release of insulin and digestive juices.
The ventromedial nucleus of the hypothalamus and the axons passing by it influence eating by regulating stomach emptying time and insulin secretion. Animals with damage in this area eat more frequently than normal because they store much of each meal as fat and then fail to mobilize their stored fats for current use.
Obesity is partly under genetic control. Syndromal obesity occurs if a gene leads to both obesity and other medical problems. Monogenic obesity results from a single gene that does not impair other body functions. Common obesity is influenced by many genes, as well as environmental factors.
Dieting is seldom an effective means of long-term weight loss. Reducing consumption of soft drinks is highly recommended. Stomach bypass surgery is an option for relatively severe cases of obesity.
Bulimia nervosa is characterized by alternation between undereating and overeating. It has been compared to addictive behaviors.
Anorexia nervosa is characterized by refusal to eat enough to maintain a healthy weight. Antidepressant treatments are seldom effective. The increased physical activity associated with anorexia may be motivated by temperature regulation.