Untitled Flashcards Set
First Aid
The initial assistance or treatment given to a victim for any injury or sudden illness before the arrival of an ambulance, doctor, or any qualified personnel.
Aims:
Preserve life
Prevent the victim’s condition from becoming worse
Promote recovery
Responsibilities as a First Aider
Quickly assess the situation and call for appropriate help.
Protect the victim and others from potential danger.
Identify the illness (medical) or mechanism of injury (trauma) affecting the victim.
Provide early, appropriate treatment, prioritizing serious conditions.
Arrange for the victim's transfer to a hospital or doctor’s care.
Stay with the victim until proper care is available.
Report observations to caregivers and assist further if needed.
Priority of Victims
Prioritize conscious victims over unconscious ones as they have higher recovery chances.
Save the young before the old.
Do not risk your own life while giving First Aid; leave immediately if in danger.
Preserve life without endangering your own while providing aid.
Victims should be treated in the order of priority, usually given by the
“3 Bs”:Breathing
Bleeding
Bones
Vital Signs Taking
Vital Signs:
T - Temperature
P – Pulse
R - Respiration
BP - Blood Pressure
P - Pain
P - Pupils
O2 Sat - Oxygen Saturation
Temperature Scale
Hyperthermia
38 degrees & above
Normal
37 degrees centigrade
Hypothermia
35 degrees centigrade & below
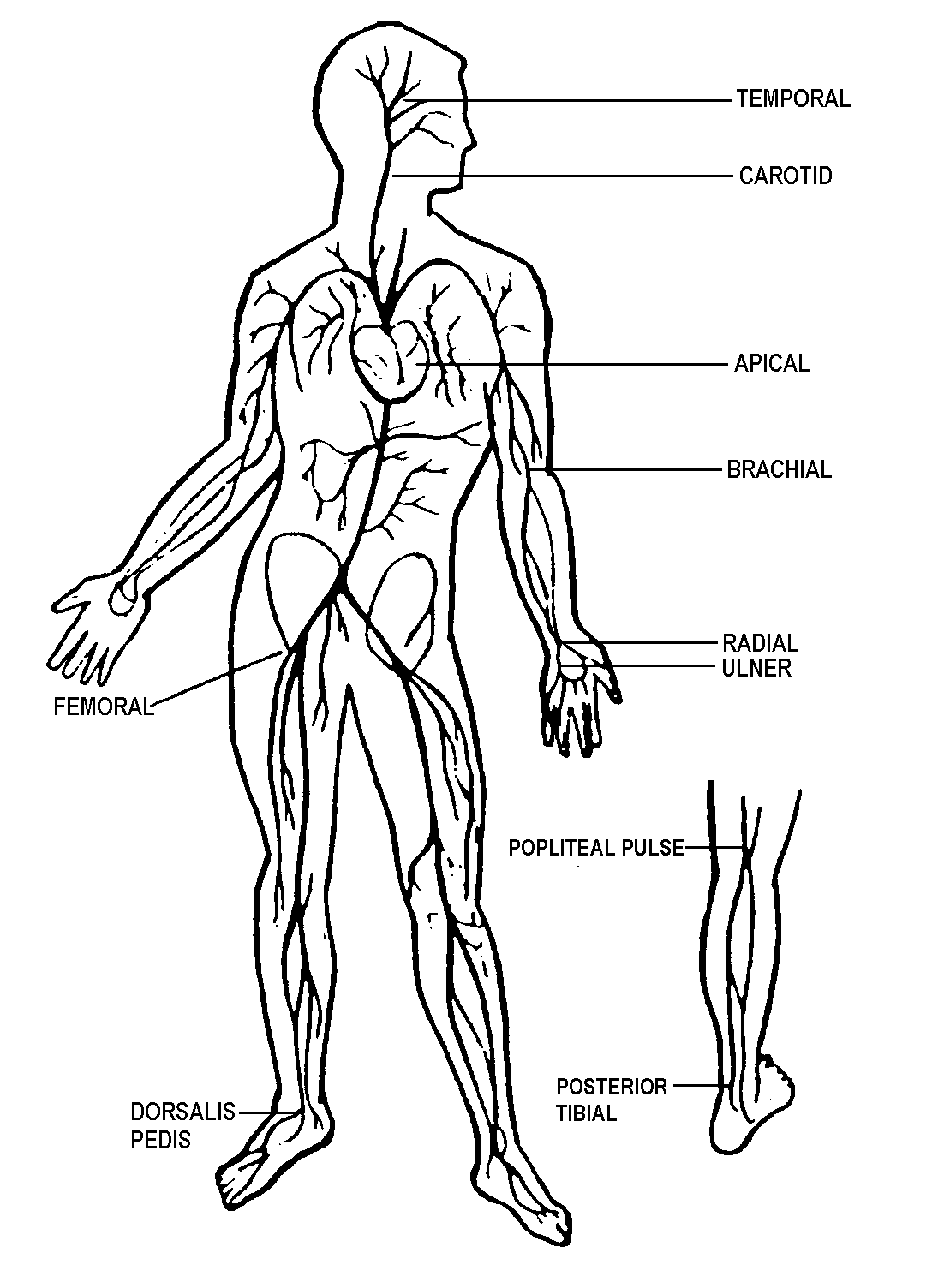
Pulse Sites
Normal Pulse Rates
Infant 100 - 160
Child 70 - 150
Adult 60 - 100
Normal Respiratory Rates
Infant 25-50 rpm
Child 15-30 rpm
Adult 12-20 rpm
Blood Pressure
Systolic (first beat)
Diastolic (last beat)
Pain Scale (0 - 10 Scale)
0 - No pain
10 - Most Painful
Pupils
Normal response
Pupils constrict with light exposure and dilate when light is reduced.
Both pupils should be the same size unless a prior injury or condition changes.
To assess, shine a penlight to the eyes.
If outdoors, cover the eyes and assess for dilation.
Abnormal findings:
No reaction to light:
Pupils remain constricted (possible drug overdose)
Unequal pupils (head injury or stroke)
Oxygen Saturation
Normal Oxygen Saturation (PulseOxi Reading): 95%-100%
Common Emergencies
Hyperventilation (Excessive Breathing)
causes a reduction of carbon dioxide concentration (below normal) in the blood.
Symptoms:
Unnaturally fast, deep breathing
Attention-seeking behaviors
Dizziness, faintness, trembling, or marked tingling in hands, feet, and lips
Headache
Chest pain
Slurred speech
Cramps in the hands and feet
Causes:
Stress, anxiety, panic
Consequence of lung diseases, head injuries, or stroke
Treatment:
Be firm but kind when speaking to the victim.
Lead the victim to a quiet place to help regain control of breathing.
Allow the victim to re-breathe their exhaled air from a paper bag.
Fainting
A brief loss of consciousness caused by a temporal reduction of blood flow to the brain
Symptoms:
A brief loss of consciousness causing the victim to fall to the floor
A slow pulse
Pale, cold skin and sweating
Causes:
Too little food and fluid consumption (dehydration)
Low blood pressure
Lack of sleep
Over exhaustion
Treatment:
Lay the victim down and elevate legs slightly.
Ensure fresh air.
Reassure them and help them sit up gradually.
Check for and treat any injuries from falling.
Hemorrhage/Bleeding
The loss of blood from the body.
It can be external and internal.
External Hemorrhage
The wound and loss of blood are visible.
Types:
Arterial: Bright red, spurting blood, pulsating flow (hardest to control)
Venous: Dark red, steady flow of blood.
Capillary: Slow, even flow.
The body contains about 4.5 to 5.5 liters of blood.
Losing up to half a liter usually has no negative effects (equivalent to blood donation).
Loss of 1 liter may lead to shock.
Loss of 3 liters often results in death.
Children and the elderly may go into shock sooner.
Pre-hospital Treatment for External Hemorrhage
Apply direct pressure
Elevate injured extremity
Use pressure points
Use a tourniquet
Direct Pressure Method
Apply and maintain direct pressure on the wound with a sterile cloth or your hand until bleeding stops.
Elevation Method
Elevate the injured limb above the heart to help reduce blood flow.
Pressure Points Method
Apply pressure to specific points near the wound to control bleeding.
Using Tourniquet
Use only in severe emergencies when other methods fail to stop bleeding from an extremity.
Apply as distal (far from the body) as possible.
Danger: Can damage nerves and blood vessels, potentially leading to loss of the extremity.
Stops blood flow by compressing blood vessels in the arm or leg.
Can result in serious issues, including loss of the limb.
Use Only If
Uncontrolled bleeding from the arm or leg is life-threatening.
Commercial tourniquets are preferable over homemade ones.
Internal Hemorrhage
May not be obvious, can be life-threatening.
Common Mechanisms:
Car accidents
Falls
Knife and gunshot wounds
Trauma causing internal organ injury or fractures
Medical conditions
For a hematoma:
Transport the patient ASAP.
Report the possibility of internal bleeding to EMS personnel upon arrival.
TYPES OF WOUNDS
Laceration
Cut or torn wound
Often has jagged edges
Puncture
Greatest chance of infection
May cause internal bleeding
Abrasion
Painful scraping away of skin
Avulsion
Skin or tissue completely/partially torn from body
Causes severe bleeding
Fold/replace torn skin if possible
Wrap wound as laceration
Nosebleeds (Epitaxis)
Do not tilt nose up or put head between knees
Treatment:
Sit in a chair and tilt the head slightly forward.
Pinch nostrils together for about 10 minutes.
Apply an ice pack wrapped in a moist cloth to the nose.
Breathe through the mouth.
Get medical help if:
Bleeding lasts for more than 20 minutes.
Difficulty breathing occurs.
Bleeding is very fast or heavy.
Person feels dizzy or weak.
Occurs after a head injury.
Associated with hypertension.
Animal Bites (DOG, CAT, RAT)
Wash the wound thoroughly with soap and warm water to reduce infection risk.
Raise and support the wound, pat it dry with clean gauze, and cover with a sterile dressing.
If the wound is large or deep, treat for bleeding.
Bring to hospital or RHU for anti-tetanus and anti-rabies shots.
Snake Bites
Note the snake’s appearance
Protect the victim
Move the person away from the snake.
Have the person lie down with the wound below the heart.
Keep the person calm and still to prevent venom spread.
Cover the wound with a loose, sterile bandage.
Remove jewelry or shoes from the bitten area.
Cramps
Painful sensations caused by contraction or over shortening, usually of muscles.
Causes:
Cold or overexhaustion
Treatment:
Stretch the muscle and apply heat or cold (preferably heat)
Cramps from lack of salt and water. Stretch the muscle, drink water and increase salt intake.
Types of Burns
Dry burn
Caused by flame, contact with hot object, friction etc.
Scalds
Contact with steam and hot fluids
Electrical burn
Low-voltage current, lightning strike
Cold injury
Contact and freezing metals, dry ice, freezing vapors (Liquid oxygen and liquid nitrogen)
Chemical burn
Industrial chemicals, inhaled fumes, corrosive gases
Household chemicals (e.g., paint remover, strong acids/alkalis, bleach, weed killer).
Radiation burn
Sunburn over-exposure to ultra-violet (UV) lamp and exposure to radioactive source.
Degree of Burn
First Degree Burn
Affects the outer skin layer, causing redness, swelling, and tenderness.
Second Degree Burn
Affects epidermis, causing rawness, blisters, and clear fluid. Can be fatal if over 60% of the body is affected.
Third Degree Burn
Burns all skin layers, possibly damaging nerves and muscles. Skin appears waxy, pale, or charred. No pain felt. Urgent medical care needed.
Heart Attack
Occurs when coronary arteries that supply blood to the heart muscle become narrowed due to plaque buildup (fat, cholesterol, and other substances). This process is known as atherosclerosis.
If plaque breaks, a blood clot forms around it, blocking blood flow through the artery to the heart muscle.
Ischemia is when blood flow and oxygen are restricted in a part of the body.
Cardiac ischemia is decreased blood flow to the heart muscle.
When this leads to damage or death of part of the heart muscle, it is called a heart attack or myocardial infarction (MI).
Heart Attack Signs & Symptoms
Chest discomfort (pain, pressure, tightness, squeezing, fullness)
Discomfort may radiate to the arms, neck, back, jaw, or abdomen
Often mistaken for heartburn or indigestion
Pale, cool, sweaty skin
Shortness of breath
Dizziness, fainting, or unresponsiveness
Nausea and vomiting
Unexplained fatigue
Emergency Care for Heart Attack
Call rescue
Position of comfort, usually sitting
Calm, reassure person
Check breathing if victim becomes unresponsive
If no breathing or only gasping, begin compressions
Stroke
Like a heart attack but in the brain.
Caused by a clot or bleed in the brain.
Symptoms may be minor or severe; many survivors face permanent impairment.
Stroke Signs & Symptoms
Sudden onset
Weakness or numbness in one arm or leg (usually on one side)
Facial droop or paralysis
Difficulty speaking, eating, swallowing, or managing secretions
Loss of balance, uncoordination, or difficulty walking
Confusion, anxiety, or unresponsiveness
Changes in sensation, severe headache, dizziness, or vision changes
Temporary symptoms may indicate a mini-stroke (TIA).
STR: Smile, Talk, Reach Assessment
Smile: Ask the person to smile. Look for uneven smile or facial droop.
Talk: Ask the person to repeat a common phrase. Listen for slurred or incorrect words.
Reach: Ask the person to close their eyes and raise both arms. Look for arm drift or weakness on one side.
FAST:
Face drooping
Arm weakness
Speech difficulties
Time to call
Trauma
A wound or injury caused by sudden external force or violence.
Major trauma can lead to shock, respiratory failure, and death.
Motor vehicle accidents are the most common cause of injury-related death.
Gunshot wounds are the 3rd leading cause.
Traumatic Injuries
Amputation
Partial or complete loss of a body part.
Treatment:
Stop bleeding and salvage the amputated part.
Apply direct pressure.
Wrap amputated part in dry sterile gauze, place in a plastic bag, then into a second bag filled with ice.
Do not let ice touch the part or immerse in water.
Impaled Object
Object remains embedded in the skin.
Treatment:
Stop bleeding and stabilize the object in place.
Call rescue.
Expose the wound and apply direct pressure at wound edges to control bleeding.
Stabilize the object with bulky dressings or clean cloths and tape, securing at least ¾ of the object.
If in extremity and EMS is delayed, apply a splint.
Calm and reassure the victim.
Do not apply pressure on the object or remove/shorten it, as it may cause severe bleeding.
Impaled Object on the Cheek
Consider removing object if massive bleeding obstructs airway.
If difficult to remove, leave in place.
Pack sterile gauze between teeth & cheek and position victim so blood drains from mouth.
Penetrating wounds
Gunshot Wound
Causes damage to bones, vital organs, and major blood vessels
May have exit wound larger than entrance wound
Treatment:
Ensure scene safety
Call rescue and PNP
Check for entrance and exit wound
Control bleeding
Treat for shock
Keep the victim still
Spinal immobilization if needed
Do not disturb potential crime scene evidence.
Chest Injuries
Penetrating Chest Injuries
Open chest wounds, often caused by a foreign object, with a possible exit wound (perforating injury).
Can impair breathing, called a "sucking chest wound," producing a sucking sound during breathing.
Treatment
Apply an occlusive dressing with one open side as a relief valve to create an airtight seal.
Head-To-Toe Assessment
First Responder Actions
Ensure Personal Safety: Use Body Surface Isolation (BSI)/PPE and secure the scene.
Scene Size-Up: Ensure patient and bystander safety, identify injury type (trauma/medical), and assess need for additional resources.
Identify Yourself: State your name, organization, and identify as a first responder. Ask for patient consent to help.
Identify and Treat Life-Threatening Injuries: Perform initial assessment (see next slide).
Stabilize and Monitor the Patient.
Initial Assessment:
General Impression: Form an impression and gather a chief complaint and brief environmental assessment.
Check for Responsiveness & Breathing: Gently shake and shout "Are you okay?" (3 times). Classify responsiveness:
A = Alert
V = Verbal
P = Painful
U = Unresponsive
Determine if Trauma or Medical: Apply cervical collar for trauma cases with suspected cervical spine injury.
Ensure Adequate Airway:
Responsive: Check for clear speech; gurgling may indicate obstruction.
Unresponsive: Ensure the airway is open and the patient is breathing.
Verify Breathing: Look, listen, and feel for air exchange (3-5 seconds).
Adequate Breathing: Full chest rise/fall, easy breathing, normal rate.
Inadequate Breathing: Insufficient rise/fall, increased effort, cyanosis, mental status changes, or abnormal rate.
Assess Circulation: Take 5-10 seconds to check if adequate pulse is present.
Responsive Patient: Check radial pulse for adults, brachial pulse for infants.
Unresponsive Patient: Check carotid pulse for adults, carotid/femoral for children, brachial for infants.
Methods to Open Airway
Head-tilt/chin-lift maneuver
(for non-trauma)
Jaw thrust maneuver
(for trauma)
Methods of Patient Assessment
Inspection (Looking): Observe the patient and body for signs of injury or illness.
Auscultation (Listening): Listen for signs of illness, particularly air entering and leaving the lungs to assess respiratory status.
Palpation (Feeling): Feel for signs of injury or illness, typically done last to avoid causing pain.
Patient Status Update
Inform EMS of your findings and request additional resources if needed.
Notify EMS if the patient has life-threatening injuries or illness, or if the patient is stable with minor injuries.
Complete the initial assessment and treat life threats before proceeding with the physical exam.
Conducting an Exam
Medical vs. Trauma Patients
Medical: Problems are felt by the patient.
Trauma: Physical signs are obtained and palpated.
Check for Signs of Injury (D.O.T.S)
D = Deformities
O = Open injuries
T = Tenderness
S = Swelling
Blood
Physical Exam (Head-to-Toe)
Examination of the Head:
Scalp and skull: Check for deformities, open injuries, tenderness, swelling.
Ears and nose: Look for blood or cerebrospinal fluid (CSF) around openings.
Pupils: Check reactivity to light and symmetry.
Mouth: Check for deformities, injuries, and airway obstructions.
Examination of the Neck:
Check for deformities, injuries, tenderness, swelling.
Check trachea for mid-line position
Palpate vertebrae.
Check for open injuries (bandage immediately with occlusive dressing).
Check for medic alert necklace
Examination of the Chest
Feel for deformities, tenderness, and swelling, which may indicate fractures or internal injuries.
Check ribs for tenderness, including near the spine and sternum.
Gently palpate the sternum for pain or fractures.
If trained, use a stethoscope to listen for equal breath sounds in both lungs, which helps assess lung function.
Examination of the Abdomen:
Palpate quadrants with pain last. Check for swelling or discoloration.
Examination of the Back:
Check for chest wall deformities (possible broken ribs).
Check spine for tenderness or deformities (possible spinal injury).
As with chest injuries, check for sucking wounds or penetrating injuries.
Examination of the Pelvis:
The pelvis includes the ileum, ischium, and pubic bone.
Pelvic/hip fractures can cause significant blood loss (up to 2 liters).
Internal organs, blood vessels, and nerves pass through, and spinal injury is possible.
Check for priapism in males.
Deformities may not be visible; palpate iliac crests and pubic bones for tenderness.
Open or penetrating injuries are rare but possible. Always assess for tenderness.
Examination of Lower Extremities:
Check for deformities, injuries, tenderness, and swelling.
Check pulse (dorsalis pedis or posterior tibial).
Check for motion and sensation (PMS – Pulse, Motor, Sensation).
Examination of Upper Extremities:
Check for deformities, injuries, tenderness, and swelling.
Check radial pulse, motion (wiggle fingers), and sensation (PMS).
Capillary Refill
Used for infants and children under 6 years old, not always accurate in adults.
Press on the nail bed and observe how long it takes for normal pink color to return after release.
Recheck in the same place; delayed refill may occur in cold extremities.
Used in adult triage situations.
Skin Color:
Paleness (ashen): Indicates shock, heart attack, or emotional stress.
Redness (flushing): Caused by high BP, sunburn, alcohol abuse, heat stroke, or infection.
Blueness (cyanosis): Indicates reduced oxygen levels, seen around fingertips and mouth.
Yellowness (jaundice): Indicates liver disease, including in the sclera (eyes).
Black and Blue Mottling: Caused by blood under the skin, often due to injury or infection.
In darker skin, check lips, nailbeds, palms, lower eyelids, gums, and tongue for color changes.
Skin Condition:
Reported as dry, moist, or wet based on the environment.
S.A.M.P.L.E. Mnemonic:
Signs & Symptoms: Ask open-ended questions; do not diagnose.
Allergies: Identify allergies to medications, food, or the environment.
Medications: Identify medications currently being taken.
Pertinent History: Focus on history relevant to the emergency.
Last Oral Intake: Ask when the patient last ate or drank.
Events: Identify events or activities before the incident.
Ongoing Assessment:
Reassess the patient every 5 minutes for unstable patients, and every 15 minutes for stable patients.
Check Level of Consciousness (LOC), airway, breathing, pulse, skin condition, and reassess interventions.
Continue comforting the patient and do not leave them unattended.
Hand-Off-Report/Patient Care Report (PCR)
The hand-off report, either verbal or written, transfers patient information to a higher-level care provider. It should include:
Patient age and sex
Circulation status
Chief complaint
Patient history
Level of consciousness
Treatment given
Airway status
Breathing status
The report provides up-to-date details on the patient's condition and treatment.
Musculoskeletal Injuries:
Ligaments and Tendons:
Ligaments: Connect and hold bones together at the joints.
Tendons: Attach skeletal muscles to bones, controlling joint movement.
Fracture
A break or crack in the bone.
Symptoms:
Pain at or near the fractured site
Tenderness on gentle pressure
Swelling
Deformity (e.g., angulation, irregularity, or depression)
Loss of power
Signs of shock
Treatment:
Support and immobilize the injured limb.
Use a splint to prevent movement.
Call emergency services.
Do not attempt to replace the bones.
Dislocation
The displacement of one or more bones at a joint.
Common sites: Shoulders, elbows, thumbs, fingers, lower jaw.
Symptoms:
Pain at the injury site
Limited movement
Deformity
Swelling
Tenderness
Treatment:
Support and immobilize the limb.
Use a splint if possible.
Call emergency services.
Strain
An injury to a muscle caused by overstretching.
Symptoms:
Localized pain
Stiffness
Inflammation
Bruising
Treatment:
Support the joint in a comfortable position.
Apply P.R.I.C.E. (Protect, Rest, Ice, Compression, Elevation).
Sprains
An injury to a ligament.
Treatment: Follow the same as for strains (P.R.I.C.E.).
Bandages
Any clean cloth material used to hold dressings in place, control bleeding, or immobilize body parts.
Triangular
Muslin binder
Four-tail
Roller
Cravat
Elastic
Open Bandages: Head/Scalp, Face/Cheek, Chest/Back, Palm/Foot
Closed Bandages: Forehead, Eye/Eyes, Cheek/Jaw, Limb, Elbow, Palm V/H, Ankle w/ heel, Ankle w/o heel
Splinting
Applying a device to stabilize a painful, swollen, or deformed body part, preventing further movement of joints and bone ends.
Sling and Swathe
Two triangular bandages used to hold an injured arm in place against the body.
Improvised Splints
Can include materials like books, cardboard, pillows, blankets, etc.
Types of Splints
Rigid Splints
Conforming Splint
Traction Splint
Improvised Splint
Splinting the Upper Extremities
Always check pulse, motor function, and sensation before and after splinting.
Humerus (Shoulder) Injury
Signs and Symptoms: Pain, swelling, deformity.
Treatment: Apply a rigid splint to the outside of the arm, pad voids, then apply sling and swathe.
Shoulder and Clavicle Injury
Signs and Symptoms: "Dropped" shoulder, deformity, pain.
Treatment: Apply sling and swathe with padding as needed.
Elbow Injury
Important: Splint in the position found—do not attempt to straighten.
Signs and Symptoms: Pain, swelling, deformity.
Treatment: If bent, splint with sling and swathe or a pillow/blanket. If straight, splint the entire arm from armpit to fingertips.
Forearm and Wrist Injury:
Signs and Symptoms: Pain, swelling, deformity.
Treatment: Splint with an arm board, then apply sling and swathe.
Hand and Fingers Injury:
Important: Check pulse via capillary refill.
Signs and Symptoms: Pain, swelling, deformity.
Treatment: If one finger is fractured, tape it to the adjacent finger. If multiple fingers are fractured, splint the entire hand in its functional position.
Splinting the Lower Extremities
Pelvic Injuries
Can be life-threatening due to massive blood loss and possible spinal injury.
Signs and Symptoms: Pain when pressure is applied to the iliac crests, inability to lift legs while on the back.
Hip Injuries
Difficult to distinguish from femoral or pelvic fractures.
Signs and Symptoms: Pain, discoloration, possible foot rotation, swelling, inability to move legs.
Femoral Fractures
Can lead to significant internal bleeding.
Signs and Symptoms: Intense pain, deformity, rigidity, shortened limb.
Treatment: Use two padded boards to splint the leg in a straight position, securing with cravats.
Knee Injury (Bent)
Stabilize the knee in its bent position using splints.
Knee Injury (Straight)
Stabilize with splints that keep the knee in its straight position.
Tibia or Fibula Injury
Signs and Symptoms: Pain, swelling, deformity.
Pre-hospital Treatment: Use pneumatic splint or two padded long boards, secured with cravats. Alternatively, use a circumferential splint for closed injuries.
Ankle and Foot Injuries
Signs and Symptoms: Pain, swelling, deformity.
Pre-hospital Treatment: Stabilize, remove shoes and socks if possible, and apply a circumferential splint. Alternatively, use padded boards to the mid-thigh for stabilization.
Skull Fractures
Do not attempt to remove an object impaled in the skull; stabilize it with bulky dressings.
Do not stop the flow of cerebrospinal fluid (CSF) from the ears or head wound; cover the opening with sterile gauze.
Signs and Symptoms:
Altered mental status (confusion to unresponsiveness)
Pain, inflammation, deep scalp lacerations, or hematoma
Softness or depression of the skull
Facial bruising (Battle's sign, raccoon eyes)
Sunken eyes, unequal pupil size
Sudden or severe headache, nausea, vomiting
Blood or CSF leaking from ears/nose
Deteriorating vital signs, abnormal posturing, seizures
Pre-Hospital Treatment:
Use universal precautions, secure the scene.
Perform initial assessment, treat life-threatening conditions. Hyperventilate at 25 rpm if brain injury suspected.
Control bleeding, do not stop CSF drainage.
Suspect cervical spine injury, manually immobilize head/neck in neutral position.
Administer oxygen per protocol.
Cover and bandage open wounds.
Brain Injuries
Open/Penetrating Brain Injury: Involves skull break or impaled object, exposing cranial cavity.
Closed Brain Injury: No skull break, although skin may be broken but serious brain injury is possible.
Signs and Symptoms
Vomiting, headache, weakness, unconsciousness
Posture changes (decorticate, decerebrate), altered breathing
Treatment: Same as for skull fracture.
Facial Fractures
The main danger is airway obstruction due to bone fragments or blood.
Signs and Symptoms
Blood in airway, facial deformities
Color change below eyes, limited jaw motion, misaligned teeth
Loose or broken teeth, pain/numbness, swelling
Signs of severe blow (contusions, bruising)
Pre-Hospital Treatment
Ensure open airway.
Control bleeding
Bandage open wounds.
Monitor vital signs
Treat for shock.
Spinal Injuries
Signs and Symptoms
Numbness or tingling in arms or legs
Paralysis of limbs
Pain during movement of arms/legs
Sensitivity or pain along the neck or back
Deformity of head or neck
Head injury or hematomas in shoulders, back, or sides
Loss of bowel or bladder control
Difficulty breathing with minimal chest movement
Posturing (arms extended above head) indicating cervical damage
Priapism (persistent erection)
Determining Possible Spinal Injury
Conscious Patient
Ask about the incident, how they feel, and if they can move their hands/feet.
Check for hematomas, lacerations, deformities.
Palpate for sensitive or injured areas.
Spinal injury may not be apparent immediately.
Unconscious Patient
Look for cuts, hematomas, deformities.
Palpate for deformities and injuries.
Inquire about the incident from others.
Complications
Respiratory Arrest Paralysis of thoracic muscles affects breathing, as breathing relies solely on the diaphragm.
Neurogenic Shock Neurological injury affects blood vessels, leading to shock.
General Paralysis Can occur due to spinal cord injury.
Pre-Hospital Treatment
Use universal precautions and secure the scene.
Determine the mechanism of injury.
Provide manual in-line neutral stabilization of head and neck.
Conduct initial assessment and assume spinal injury for unconscious patients.
Administer oxygen per protocol.
Perform physical exam and provide necessary treatment.
Maintain manual stabilization until immobilized.
Monitor vital signs during transport.
Chest Injuries
Methods of Injury
Blunt Trauma: Closed injury, no penetration, but may cause severe damage.
Compression Injury: A form of blunt trauma, where rapid chest compression occurs.
Penetrating Injury: Open injury where chest cavity is penetrated.
Signs and Symptoms of Chest Injury
Tenderness/pain at the injury site
Chest deformity, coughing up blood
Shallow breathing with crackling sensation
Increased pain with breathing
Posture leaning towards injured side
Extensive bruising
Grating (crepitus) upon palpation
Subcutaneous emphysema
Distended neck veins, bloodshot eyes, cyanotic tongue/lips, swollen upper torso
Rib Fractures
Pre-Hospital Treatment
Apply a sling and swathe to hold the arm against the injured side of the chest.
Provide a pillow or blanket for support.
Allow the patient to assume a comfortable position if alert.
Avoid methods that fully encircle the chest.
Introduction to Basic Life Support (BLS)
Kinds of Life Support
Basic Life Support (BLS)
An emergency procedure for recognizing respiratory or cardiac arrest and applying CPR to maintain life until recovery or advanced life support is available.
Advanced Cardiac Life Support (ACLS)
Use of special equipment to support breathing and circulation during a cardiac emergency.
Prolonged Life Support
Used for post-resuscitation and long-term resuscitation efforts.
The Circulatory System
Delivers oxygen and nutrients to tissues and removes waste.
Consists of the heart, blood vessels, and blood.
Breathing and Circulation
Air entering lungs: 21% oxygen, trace of CO2.
Air exhaled: 16% oxygen, 4% CO2.
TIME IS CRITICAL!
0-1 minute: Cardiac irritability.
0-4 minutes: Brain damage unlikely.
4-6 minutes: Brain damage possible.
6-10 minutes: Brain damage likely.
>10 minutes: Irreversible damage
Clinical Death
Heart and breathing stop.
0-4 minutes: Brain damage unlikely.
4-6 minutes: Brain damage probable.
Biological Death
Irreversible brain death.
6-10 minutes: Brain damage probable.
>10 mins: Brain damage certain.
Cardiopulmonary Resuscitation (CPR)
An emergency procedure that provides chest compressions and ventilations when heart and lung action stop.
Cardio: Heart
Pulmonary: Lungs
Apply CPR to patients who have NO BREATHING (American Heart Association - AHA 2005 guidelines).
The AHA recommends the following order:
CPR Revised Guidelines: Think C-A-B
Compressions: Push at least 2 inches on the adult breastbone, 100 times per minute, to move oxygenated blood to vital organs.
Airway: Open the airway and check for breathing or blockage; watch for chest rise and listen for air movement.
Breathing: Tilt the chin back for unobstructed air passage; give two breaths and resume chest compressions.
Note: Those untrained in CPR can do chest compressions only until help arrives. Always wear PPE.
Step-by-Step CPR Guide
Call for HELP or ask someone else to do so.
Try to get the person to respond; if unresponsive, roll the person on their back.
Start chest compressions: Place the heel of your hand on the center of the chest. Place your other hand on top, fingers interlaced.
Compress the chest: At least 2 inches for adults and children, 1.5 inches for infants. Press at a rate of 100 compressions per minute (about the rhythm of "Stayin' Alive").
If trained, open the airway with a head tilt and chin lift.
Give two breaths: Pinch the victim's nose, cover their mouth with yours, and give two 1-second breaths, watching for the chest to rise.
Continue CPR: 30 compressions and 2 breaths until help arrives.
Recovery Position
Once breathing and pulse return, place the person in the recovery position.
Criteria for Not Starting CPR
Patients with a valid "Do Not Resuscitate" (DNR) order.
Patients showing signs of irreversible death:
Livor mortis
Rigor mortis
Decapitation
Decomposition
When to Stop CPR: (STOPSS)
S: Spontaneous circulation is restored.
T: Turned over to medical services.
O: Operator is exhausted and can’t continue.
P: Physician assumes responsibility.
S: Scene becomes unsafe.
S: Signed waiver to stop CPR.
Differences Based on Age
Adult (>8 years): Call EMS immediately after determining unresponsiveness.
Child (1-8 years): Call after 2 minutes of CPR (5 cycles).
Infant (<1 year): Call after 2 minutes of CPR (5 cycles).
CPR Location and Depth
Adult (>8 years): Two hands on the breastbone, between the nipple line, at least 2 inches deep.
Child (1-8 years): One or two hands on the breastbone, between the nipple line, 1/3 to 2 inches deep.
Infant (<1 year): Two fingers on the breastbone just below the nipple line, 1/3 to 1/2 inch deep.
Rescue Breathing
Used when breathing stops or is inadequate, but the person still has a pulse.
Delivers air into the lungs to supply oxygen.
Crucial for keeping the person alive until help arrives.
Foreign Body Airway Obstruction (FBAO) Causes:
Improper chewing of large food pieces.
Excessive alcohol intake:
Relaxation of the tongue back into the throat.
Aspirated vomitus (stomach content).
Presence of loose dentures.
Children running while eating.
Children at the hand-to-mouth stage left unattended.
Two Types of Airway Obstruction
Anatomical Obstruction
Mechanical Obstruction
Classification of Airway Obstruction
Mild Obstruction
Good air exchange
Responsive, can cough forcefully
May wheeze between coughs.
Severe Obstruction
Poor or no air exchange
Weak or ineffective cough or no cough
High-pitched noise while inhaling or no noise
Increased respiratory difficulty
Cyanosis (turning blue)
Unable to speak
Universal sign of choking (clutching the neck)
No air movement.
Treatment Methods
Abdominal Thrust (for conscious adult and child victims):
Used to remove a foreign object from the airway.
Caution: Should not be used on infants under 1 year due to injury risk.
Incorrect application may damage the chest, ribs, and internal organs.
Victim should be examined by a physician to rule out complications.
Back Slaps and Chest Thrusts (for infants with FBAO):
Five back slaps and five chest thrusts used for conscious infants with a foreign body airway obstruction.
Chest Thrust (for pregnant or very obese patients):
Used instead of abdominal thrusts.
Fists are placed against the middle of the breastbone and backward thrusts are applied.
Emergency Rescue Transport
Rapid movement of a patient from an unsafe area to a safe location.
Caution: Incorrect handling and transport may worsen the patient's condition.
Carry Techniques
One-Man Carry: Includes assist to walk, sweetheart's carry, back strap, fireman’s carry (conscious/unconscious).
Two-Man Carry: Includes arms as litter, extremity carry, chair carry (conscious/unconscious).
Three-Man Carry: Includes three-man hammock.