AP Psychology Review
Unit 0
Psychology: The scientific study of behavior and mental processes, exploring how individuals think, feel, and act.
Approaches to Psychology:
Approach | Focus |
Behavioral | How we learn observable responses |
Biological | How the body and brain enable emotions, memories, and sensory experiences; how our genes and our environment influence our individual differences |
Cognitive | How we encode, process, store, and retrieve information |
Evolutionary | How the natural selection of traits has promoted the survival of genes |
Humanistic | How we achieve personal growth and self-fulfillment |
Psychodynamic | How behavior springs from unconscious drives and conflicts |
Social-cultural | How behavior and thinking vary across situations and cultures |
Biopsychosocial | How the brain and nervous system influence mental processes and behavior *best approach |
Types of Psychologists
Clinical Psychologists: Focus on diagnosing and treating mental disorders.
Cognitive Psychologists: Study mental processes such as perception, memory, and problem-solving.
Developmental Psychologists: Examine psychological growth and change throughout the lifespan.
Social Psychologists: Investigate how individuals influence and are influenced by others in social contexts.
Industrial-Organizational Psychologists: Apply psychological principles to workplace environments to enhance productivity and employee well-being.
Personality Psychologists: investigate our persistent traits
Human Factors Psychologists: focus on the interaction of people, machines, and physical environments
Counseling Psychologists: help people cope with challenges and increase their personal and social functioning
Community Psychologists: work to create social and physical environments that are healthy for all
Experimental Psychologists: do experiments to discover information about the workings of behavior and mental processes
Quantitative and Psychometric Psychologists: discover the numbers/math behind psychological principles
Sports Psychologists: work with athletes
Health Psychologists: psychologists that study and promote the relationship between psychological factors and physical health, focusing on how behaviors, stress, and lifestyle choices impact overall well-being.
Rehabilitation Psychologists: psychologists that help people who have lost functioning, often after a traumatic event
Educational Psychologists: psychologists who study the processes of learning and development in educational settings, focusing on how students learn and how to improve educational outcomes.
School Psychologists: psychologists who provide assessment and intervention to individual students, usually work for just one school or district
Neuropsychologists: psychologists that study, diagnose, and treat neurological and neurodevelopmental disorders such as Alzheimer’s disease, attention-deficit/hyperactivity disorder, and autism spectrum disorder.
Scientific Method
The scientific method: a systematic process used in psychology to formulate hypotheses, conduct experiments, collect data, and draw conclusions, ensuring that research findings are reliable and valid.
In science, a theory explains behavior or events by offering ideas to organize observations.
A hypothesis is a testable prediction used in science.
Operational definitions are precise, defined explanations of procedures and concepts used in an experiment that allow other scientists to replicate the research (do it again).
Types of methods:
Experimental Method: Involves manipulating one or more independent variables to observe the effect on a dependent variable, allowing researchers to establish cause-and-effect relationships.
Correlational Method: Examines the relationship between two or more variables to determine if they are associated, but does not imply causation.
Descriptive Method: Describes behaviors, often using case studies and surveys to gather in-depth information, but lacks the ability to establish cause-and-effect relationships.
Correlation coefficient: A number from -1 to 1 that describes how closely related two phenomena are. A correlation coefficient close to 1 implies a close positive relationship, while a correlation coefficient close to -1 implies a close negative relationship.
Correlation does not mean causation!!!
An experiment has an experimental group that receives the treatment and a control group that does not receive the treatment.
A good experiment uses random assignment - participants in the experiment will be randomly assigned to the experimental group or the control group to account for other factors influencing results!
Placebo effect - if someone thinks they are doing something that will help them, they will likely be helped anyway even if the thing actually does nothing (eg a sugar pill vs a real pill)
Single blind study - participants don’t know if they’re receiving the placebo or not, but the researchers do
Double blind study - neither the researchers nor the participants know who is receiving the placebo and who is receiving the experimental treatment
Standard deviation - represents how dispersed the data is from the mean
High SD = data is very spread out, Low SD = data is very close together
68% of data falls within 1 standard deviation of the mean
95% of data falls within 2 standard deviations of the mean
99.7% of data falls within 3 standard deviations of the mean
Null hypothesis - hypothesis that says that the independent variable of an experiment does not affect the dependent variable
Alternate hypothesis - hypothesis that says that the independent variable of an experiment does affect the dependent variable
p-value - likelihood of observing the experimental results under the null hypothesis
p-value < 0.05 is generally considered statistically significant
statistically significant data means that the odds are low enough that the null hypothesis is true, so you can reject the null hypothesis
Unit 1: Biological Bases of Behavior
Physiology of the Brain
Anatomy of a Neuron
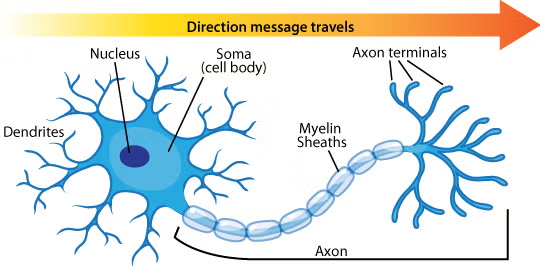
Cell body - also called soma, integrates and processes information coming from dendrites, initiates the action potential
Dendrites - receive messages from other cells
Axon - passes messages via the action potential from the cell body to the terminal bulbs
Myelin sheath - covers the axon, speeds up neural impulses
Terminal bulbs - at the end of the axon, form junctions with other cells
Synapse - gap between two neurons, neurotransmitters pass from terminal bulbs to dendrites
Action potential works because the electrical charge causes sodium channels to open, causing sodium ions to flood in and depolarize the axon. Then, the sodium channels are closed and potassium channels are opened to repolarize the axon and return it to its resting state. This happens like a chain reaction through the axon, allowing it to spread messages far.
Neurotransmitters that are released by neurons bind to receptors on the dendrites of the receiving cell. Neurotransmitters that have already transmitted the signal then get reabsorbed by the cell that originally released it, though this process is inhibited by certain medications like SSRIs (selective serotonin reuptake inhibitors).
Parts of the Brain
3 main parts:
Cerebrum - largest part of the brain, only some animals have it, more advanced function.
Cerebellum “little brain” - back of the brain, contains two hemispheres, influences thoughts, emotions, and social behavior, affects coordination
Brainstem - connects the cerebrum with the spinal cord, mostly basic, essential-for life functions, most animals have one
Parts of cerebrum

frontal lobe - executive functioning, emotional regulation
motor cortex (part of frontal lobe) - responsible for voluntary motor movements
prefrontal cortex (part of frontal lobe) - controls attention, inhibition, emotion, complex learning, theory of mind processing
Broca’s area (part of frontal lobe) - responsible for speech/language production. Someone with an aphasia of Broca’s area would struggle to communicate.
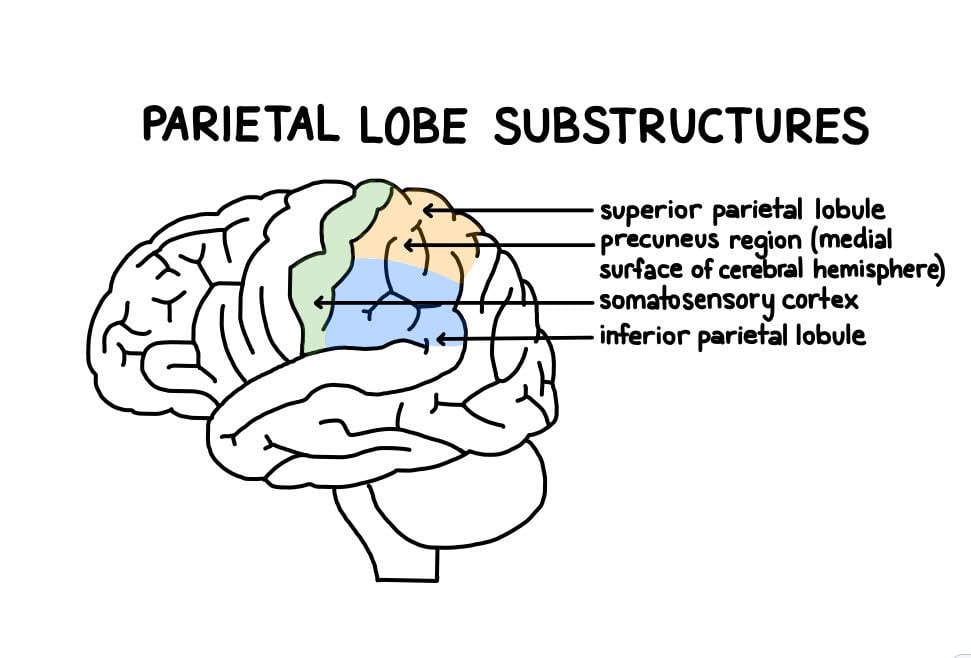
parietal lobe - integrating sensory information, self-perception/proprioception, awareness of body movements, awareness of location in space (kinesthetic sense)
somatosensory cortex (part of parietal lobe) - involves touch, pain, temperature, temperature, position, pressure, and vibration
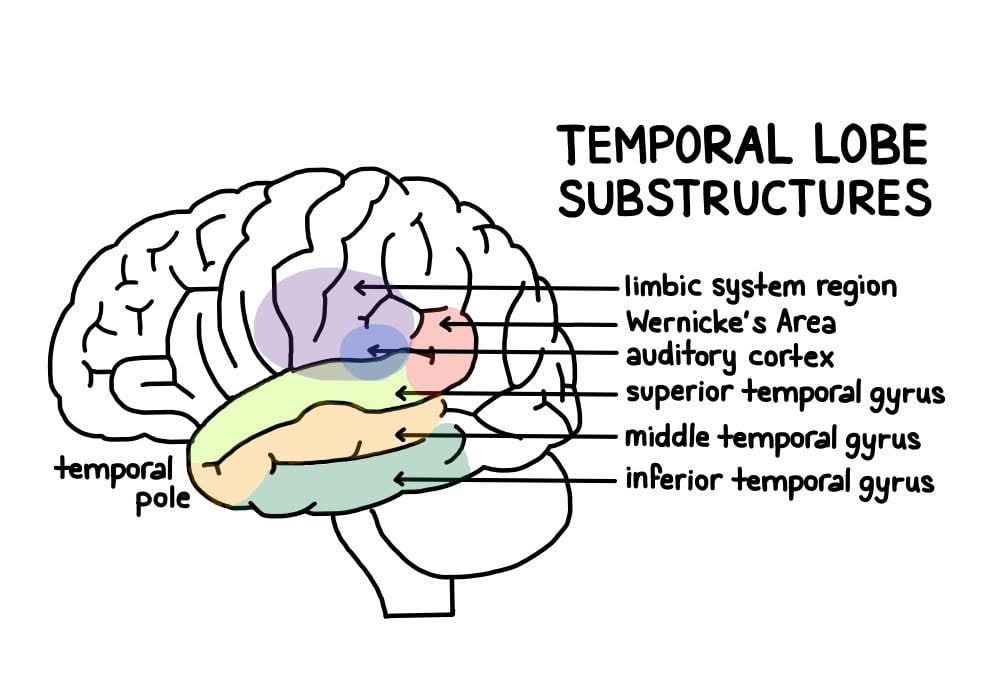
temporal lobe - processing sensory input, particularly auditory
amygdala (part of temporal lobe) - emotional responses, decision making, memory
hippocampus (part of temporal lobe) - memory storage
auditory cortex (part of temporal lobe) - processes auditory information
Wernicke’s area (part of temporal lobe) - processes language. Someone with an aphasia of Wernicke’s area would struggle to understand language, even if they could communicate perfectly.
occipital lobe - processing visual input
visual cortex (part of occipital lobe) - processing visual information
Parts of brainstem
pons - unconscious processes such as the sleep-wake cycle and breathing
midbrain - relays sensory information
medulla - controls processes essential to life such as heart rate and blood pressure
thalamus - lies above brainstem, relays sensory information NOT SMELL
hypothalamus - lies right below thalamus, controls hunger/thirst, body temperature, mood, sleep
pineal gland - responds to light and dark and secretes melatonin, regulating the circadian rhythm
corpus callosum - connects two “halves” of the brain
limbic system - parts of the brain that regulate emotions and behavior, includes thalamus, hypothalamus and amygdala
endocrine system - glands that make hormones and release them into the blood, generally result in slow changes over time (such as puberty)
central nervous system - brain and spinal cord
peripheral nervous system - everything else, delivers messages from brain and spinal cord
autonomic nervous system - governs involuntary processes
sympathetic nervous system (part of autonomic nervous system) - induces “fight or flight” responses
parasympathetic nervous system (part of autonomic nervous system) - calms your body down after “fight or flight” moments
somatic nervous system - governs voluntary processes
Types of Brain Scans
CT scan (computed topography) - uses x-ray beams passed through head, measures brain’s structure but not function
MRI (magnetic resonance imaging) - uses echo waves to discriminate between gray matter, white matter, and cerebrospinal fluid; can show if there’s fracture or bleeding
fMRI (functional MRI) - a series of MRI images taken less than an MRI, can show the brain’s functions
PET scan (positron emission topography) - uses radioactive glucose to measure brain metabolism
Sleep
Consciousness involves levels of awareness of one’s thoughts, feelings, behaviors, and events
Two types of consciousness are sleep and wakefulness
Hypnosis can be used to put someone into a state of suggestibility
We have a circadian rhythm - 24 hour sleep cycle
Memory consolidation and restoration are leading theories on why sleep exists
Sleep disorders and sleep disruptions can disrupt healthy sleep
Stages of Sleep
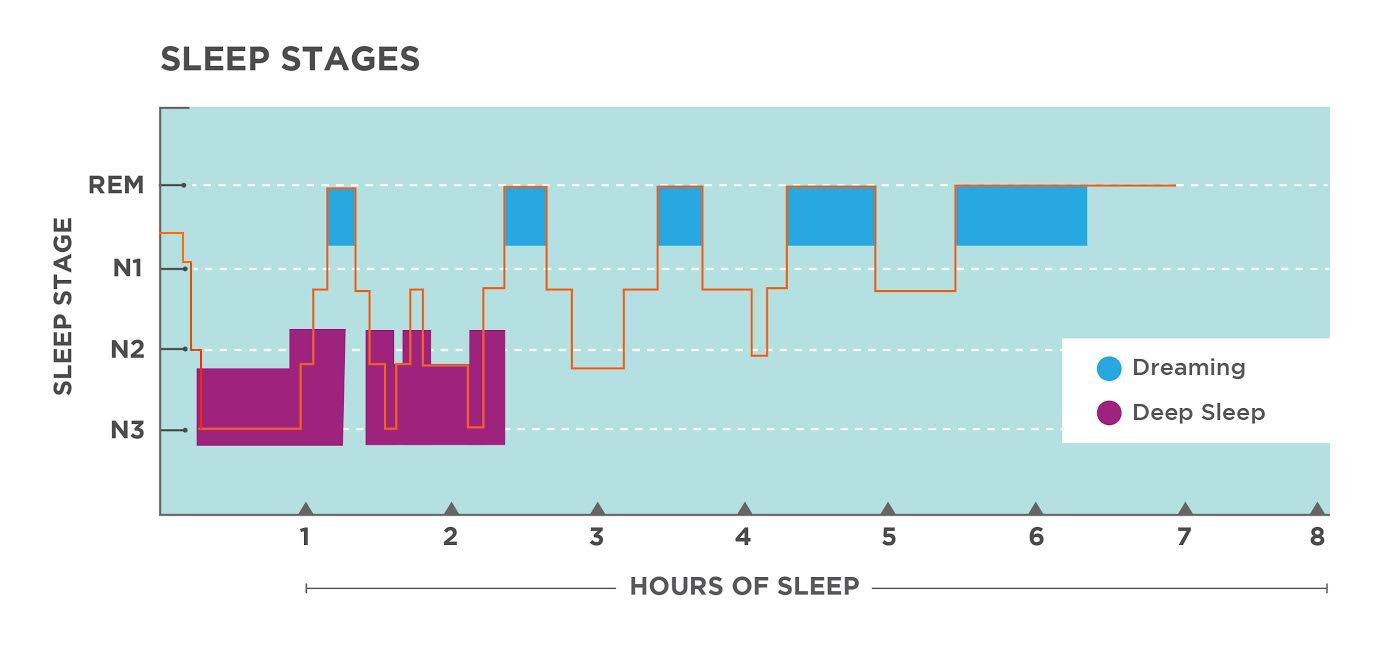
Awake - beta waves (alert) or alpha waves (tired/relaxed)
NREM 1 - alpha waves, hypnogogic hallucinations
NREM 2 - theta waves, sleep spindles, K-complexes
NREM 3 - delta waves, slow breathing/heart rate
REM (rapid eye movement) - temporary paralysis, irregular breathing, elevated heart rate, beta waves, called paradoxical sleep: brain “seems” awake, but you really are asleep - very important to get REM sleep!
Frequency of REM sleep increases the more you sleep, while deep sleep decreases
Sensation
Sensation is the process of detecting information from the environment that meets a certain threshold and transducing stimuli into neurochemical messages for processing (perception) in the brain.
Absolute threshold - threshold where a stimulus can be detected 50% of the time
Difference threshold - the smallest amount by which two stimuli can differ for someone to perceive them as different
Weber’s law - the difference threshold stays proportionally constant as the amount of stimulus gets smaller of larger
Synesthesia - “mixing” up of senses, ex seeing numbers as colors
Transduction - sensory receptors convert sensory input into electrical signals that can be read by neurons
Perceptual Constancies - we tend to view familiar objects as having the same size/shape/color even if the distance/angle/lighting changes
Nociceptors - detect potentially harmful sensations, causing pain sensation
Gate control theory - a painful sensation can be blocked by another nonpainful sensation because the painful messages are slower
Phantom limb - many people who have lost a limb can “feel” their lost limb
Visual
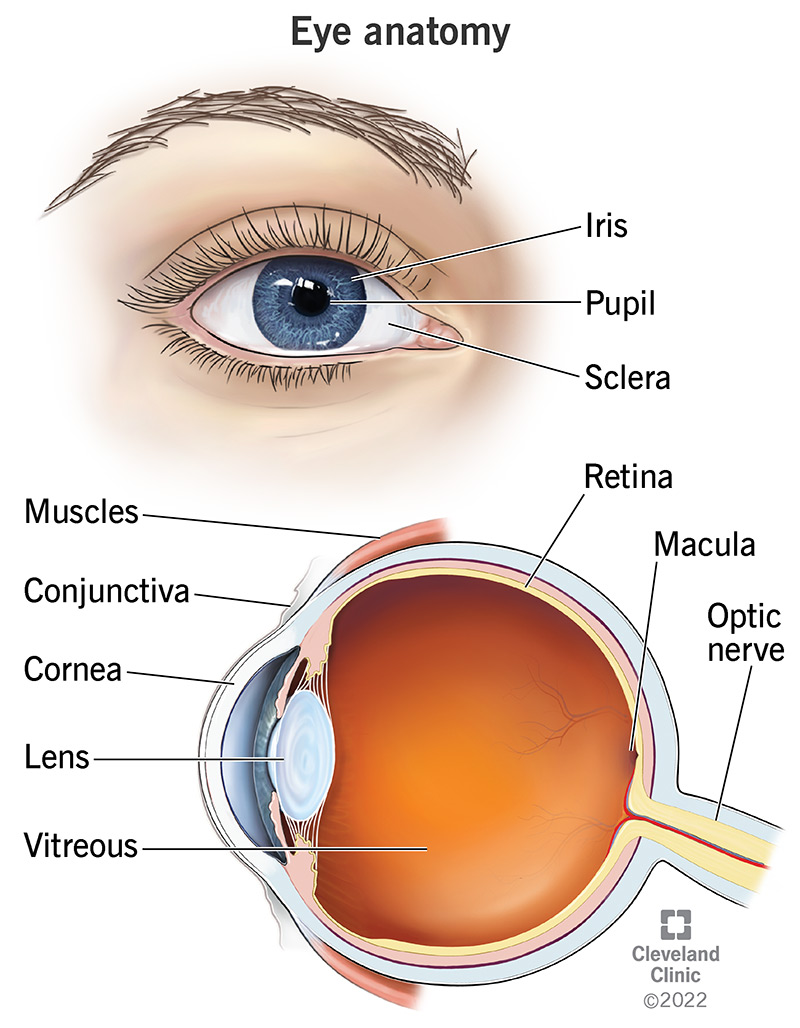
Parts of the eye:
Cornea: clear outer part of the eye’s focusing system located at the front of the eye
Iris: colored part of the eye that regulates the amount of light entering the eye
Lens: clear part of the eye behind the iris that helps to focus light, or an image, on the retina
Optic nerve: largest sensory nerve of the eye. It carries impulses for sight from the retina to the brain.
Pupil: opening at the center of the iris. The iris adjusts the size of the pupil and controls the amount of light that can enter the eye.
Retina: the light-sensitive tissue at the back of the eye. The retina converts light into electrical impulses that are sent to the brain through the optic nerve.
Macula: small, sensitive area of the retina that gives central vision. It is located in the center of the retina.
Vitreous gel: transparent, colorless mass that fills the rear two-thirds of the eyeball, between the lens and the retina.
Color vision:
Trichromatic theory - our eyes have cones that detect colors
Opponent-process theory - differently-colored afterimages are formed when certain ganglion cells are activated while certain ones are not: red/green, blue/yellow, black/white
Color vision deficiency occurs when one or more cones/ganglion cells doesn’t work.
Damage to the occipital lobes can result in blindsight (thinking you can’t see even though you can) and prosopagnosia (face-blindness)
Hearing
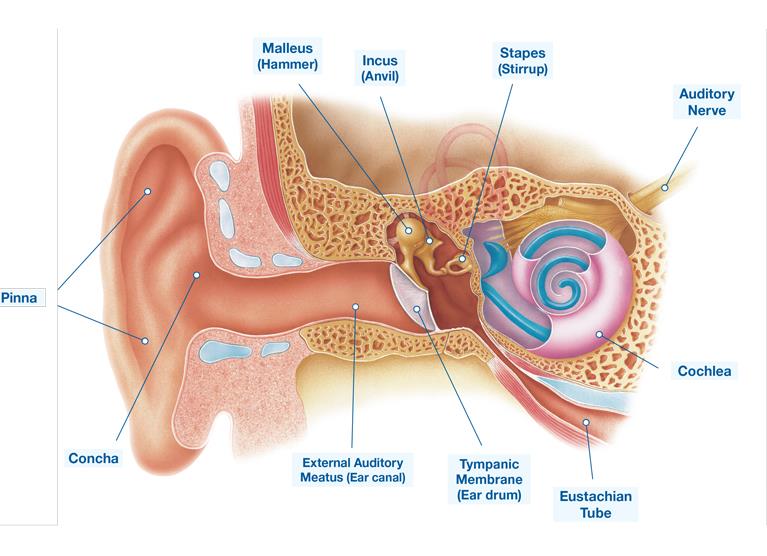
Parts of the ear:
Pinna/outer ear: exterior of the ear
Eardrum: vibrates when sound waves hit it, separates outer ear from middle and inner ear
Hammer/stirrup/anvil: Amplify the vibration from the eardrum
Eustachian tube: equalizes the pressure between the air outside the ear and in the air in the middle ear
Cochlea: has tons of tiny hairs, converts vibrations into electrical signals
Pitch (frequency of a sound wave): how high or low the sound is
Loudness/volume (amplitude of a sound wave): how loud or soft the sound is
How we hear:
Place theory: the brain perceives pitch based on the location of vibration in the cochlea
Frequency theory: the brain perceives pitch based on the number of signals sent to the brain per second
Volley theory: the brain perceives pitch by firing neural impulses at slightly different times to create a greater frequency of messages to the brain (works to perceive high pitched noises)
Sound localization - helps us determine where a sound is coming from, easiest when the sound is directly to our left or right
Conductive hearing loss - sound waves are blocked from reaching the inner ear, hearing aids are a solution
Sensorineural hearing loss - damage inside the inner ear, cochlear implant is a solution
McGurk effect - if you hear someone saying something but see their mouth moving in a different position, you might hear it differently to align with their mouth movements
Other Senses
Smell:
Anatomy of the Nose:

Sinuses: secrete mucus and filter dust
Nasal passage: where the air goes through
Nostril: opening of the nose
Adenoids: stop infection, fight germs
Tonsils: filter out germs, prevent infection
Epiglottis: protects your larynx
Larynx/voice box: allows you to breathe and make sounds
Smell is not first processed in the thalamus!!!
Taste:
Aka gustation
Sweet, sour, bitter, salty, umami, oleogustus (taste of fat)
“Supertasters” are extra sensitive to taste
Each taste bud can detect all different tastes
No taste zones!!!
Without smell, taste is muted
Touch:
Temperature, pressure, texture, temperature, vibration, pain
Cold + pressure = wet
Vestibular sense - sense of balance
Kinesthetic sense - awareness of the position of our body in space
Unit 2: Cognition
Prototypes - our mental example for any given concept
Algorithms - solve problems in a methodical way
Priming - subtly influencing someone based on a stimulus without their knowledge
Framing - the way an issue is posed
Divergent thinking - expanding on an idea
Convergent thinking - narrowing your thinking down to one idea
Obstacles in Decision-Making:
Heuristics - mental shortcuts that often make errors in judgement
Representativeness Heuristic - making assumptions based on stereotypes
Availability Heuristic - recalling the first or most vivid example that comes to mind
Mental set - the tendency to only use strategies that have worked in the past, even if they’re not the best option in that scenario
Sunk cost fallacy - not abandoning something because you have put too much time and effort into it, even if abandonment would be the best option
Gambler’s fallacy - believing that the probability of an event has changed based on previous results, even when those previous results objectively have no connection to the odds of future outcomes (for example, believing that after a losing streak, you have to win soon)
Functional fixedness - believing that objects or methods can be only used for one specific task (generally the one they were designed for)
Perception
2 types of perceptual processing
Top-down processing: using internal prior expectations to interpret a situation
Bottom-up processing: using sensory input to interpret a situation
Schema - the cognitive framework that allows a person to interpret a new situation based on their experience in similar, prior experiences (influenced by cultural experiences/expectations, experiences, and context)
Perceptual Set - our tendency to perceive some aspects of sensory data and ignore others (part of top-down processing)
Accommodation - altering one's existing schemas, or ideas, as a result of new information or new experiences
Assimilation - making new information fit in with your existing understanding of the world
Gestalt Principle
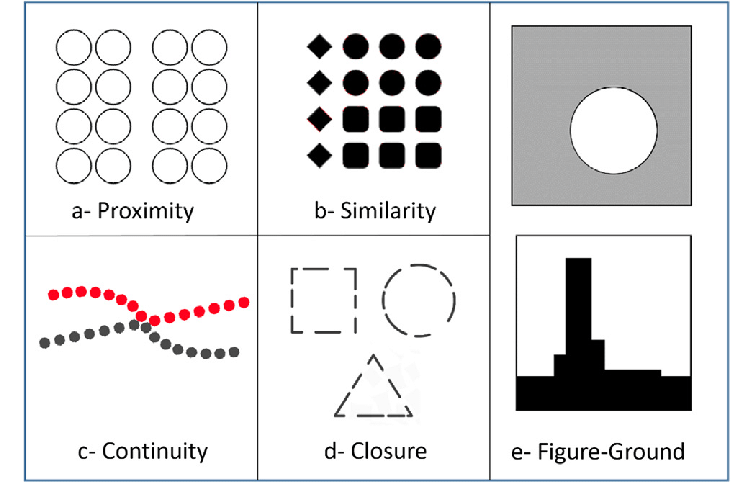
Emergence - seeing groups of clustered objects as part of one whole
Closure - automatically filling in the gaps in images, such as a dashed line
Common Region - things that are part of the same region are part of one group
Continuity - our eyes tend to follow a continuous path in one direction and we group objects based on that
Proximity - we group close-together objects
Figure/ground - we see the foreground first and typically look for solid, stable objects
Invariance - we still see objects/shapes as identical despite transformations
Similarity - when objects share superficial characteristics, we see them as grouped
Change Blindness - a phenomenon in which a person fails to recognize changes to their environment or visual stimuli, despite their being very obvious
Inattentional Blindness - the phenomenon where someone fails to perceive a visible object or event in their direct line of sight because their attention is completely focused on something else
Cocktail Party Effect - the ability to focus one's auditory attention on a particular stimulus while filtering out a range of other stimuli (such as one’s name at a cocktail party)
Memory
Types of memory:
Explicit memory: memory that is easily described or explained to other people
Episodic memory: specific experiences and events from the past
Semantic memory: facts and general knowledge
Implicit memory: memory that is hard to explain or describe to other people
Procedural memory: unconscious memory of how to do a task
Long term potentiation: synaptic connections between neurons become stronger with frequent activation (Kandel)
Memory Models
Working memory model:
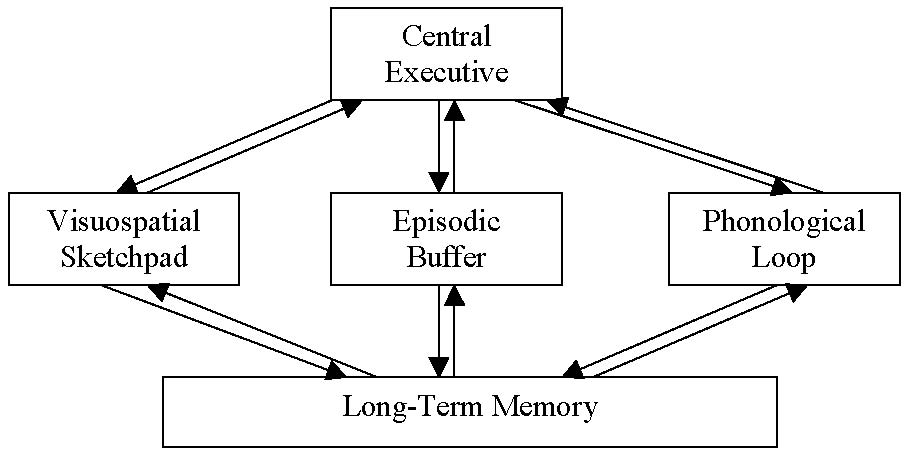
Visuospatial sketchpad: our ability to temporarily hold visual and spatial information in our memory
Phonological loop: stores and recites information in our memory (such as reciting the directions to a location in your head)
Episodic buffer: bridges information from the visuospatial sketchpad and the phonological loop
Central executive: decides which information is attended to and which parts of the working memory to send that information to be dealt with
Levels of Processing Model:
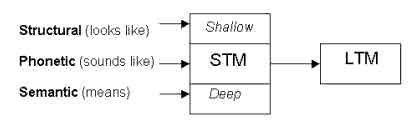
Structural: shallowest, physical characteristics of the word / what the word looks like (eg: does the word start with a vowel?)
Phonetic: medium, auditory characteristics of the word / what the word sounds like (eg: does the word rhyme with train?)
Semantic: deepest, meaning of the word (eg: does the word fit in this sentence?)
Multi-Store Model:
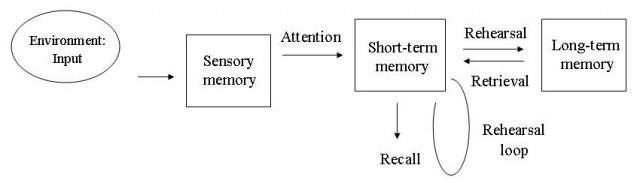
Systems of sensory memory, short-term memory, and long-term memory interact
Sensory memory:
Quick collection of information from your senses
Iconic memory (visual memory) - 0.25 seconds
Echoic memory (auditory memory) - 2-4 seconds
Short term memory:
Temporary storage space that holds information from a few seconds to a few minutes
You can generally store 5-9 pieces of information in short-term memory at a time
Long term memory:
Lasts indefinitely long
Can fade over time
Infinite storage capacity
Encoding and Storage
Encoding - processes and strategies that store memories
Examples of strategies to improve encoding: pneumonic devices, chunking, categorizing and hierarchies
Semantic encoding - converting sensory information into memories by associating it with existing knowledge and experiences
Massed practice (learning all the information at once) is less effective than distributed practice (learning it over time)
Primacy effect - we remember information at the beginning of a list
Recency effect - we remember information at the end of a list
Primacy effect + recency effect = serial position effect
Recognition - remembering information with cues (ie MCQs)
Recall - remembering information without cues (ie FRQs)
Relearning - learning something after a period of time of not having learned it, usually you pick it up faster the second time around (ie studying for finals)
Overlearning - learning past the point where you are actively improving
Automatic processing - does not require conscious awareness or effort
Effortful processing - mental activity that requires conscious attention and effort
Retrieval and Forgetting
Maintenance rehearsal - repeating something over and over
Elaborative rehearsal - rehearsing information in a way that promotes meaning
It’s easier to remember when…
you’re in the same place as when you encoded the memory (context-dependent memory)
you’re feeling the same way as when you encoded the memory (mood-dependent memory)
you’re in the same physical state as when you encoded the memory (state-dependent memory)
Testing effect - remembering is easier when you devote part of the learning process to testing yourself on your knowledge!
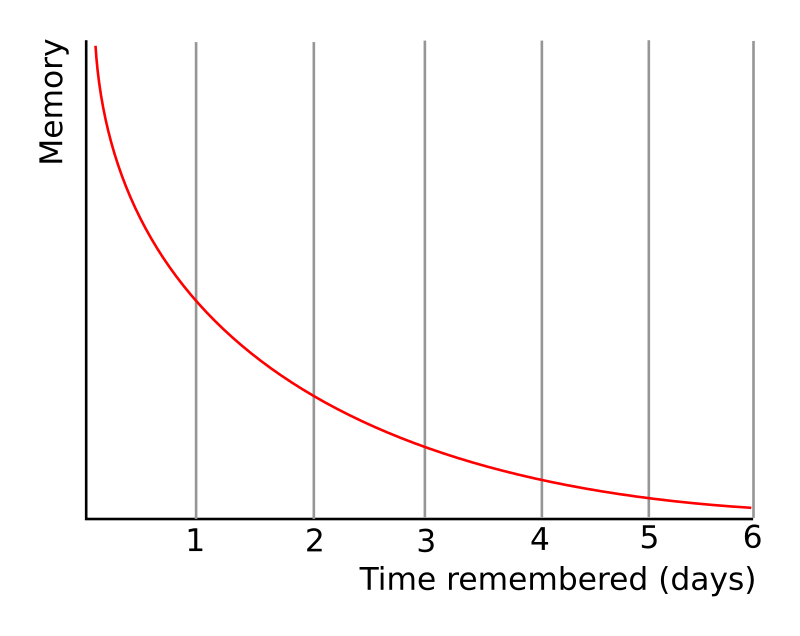
Forgetting
Forgetting curve - memory sharply declines at first but levels off over time
Proactive interference - previously learned information is making it hard to learn new information
Retroactive interference - later learning is making it hard to remember old information
Repression - forgetting distressful memories
Source amnesia - not remembering or misremembering the source of information
Misinformation effect - a person’s memory of the past is changed after being exposed to misleading information (Elizabeth Loftus)
Infantile amnesia - inability to remember information from first 3 years of life
Retrograde amnesia - can’t remember anything from before a brain injury
Anterograde amnesia - can’t make new memories after a brain injury
Intelligence and Achievement
Intelligence and how to measure it has been debated for years by researchers. Researchers debate whether intelligence is a main factor (g) or composed of several different factors.
IQ tests used to be mental age / chronological age * 100. Now, they are normed with a standard deviation (generally 15) and are mostly used to identify students for educational services.
Types of Intelligence:
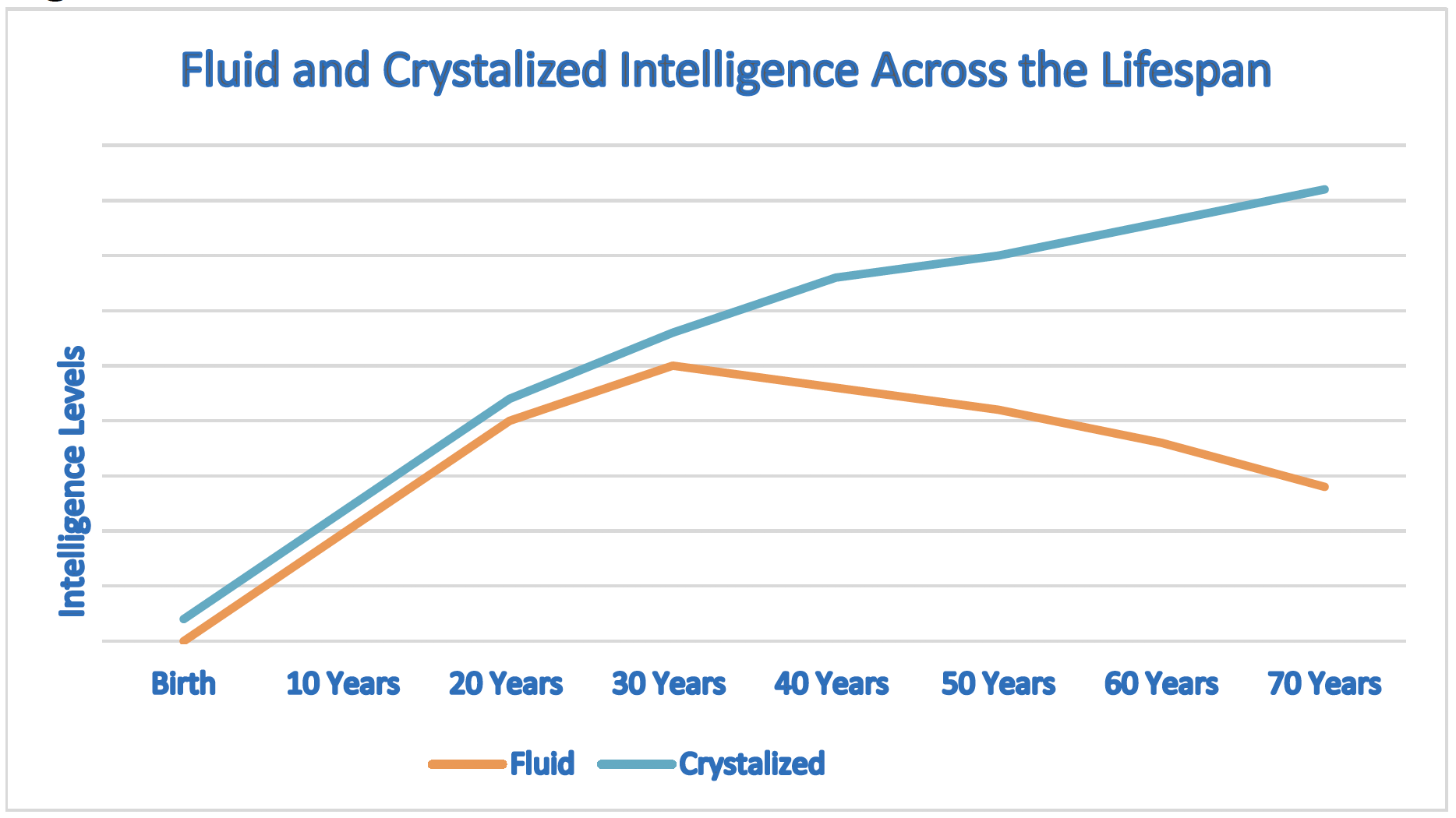
Crystalized - acquired knowledge and skills - goes up as you get older
Fluid - ability to reason in an unfamiliar situation - peaks and then goes down as you get older
Emotional - ability to understand your own and others’ emotions and respond appropriately
Stereotype Threat - fear of representing a stereotype makes you do worse
Flynn Effect - IQ scores have increased over the past century
Discrimination, poverty, and inequity can affect IQ score
Intelligence is highly heritable, meaning that a large part of the distribution of intelligence scores is caused by genetics
Hereditability % does NOT equal % of your intelligence that is due to your genetics!!!
Types of Tests:
Achievement test - measures your knowledge
Aptitude test - measures your ability to learn
People who believe that intelligence is malleable (growth mindset) tend to do better on achievement tests than people who believe that intelligence is inborn (fixed mindset).
Stanford-Binet was initially a popular IQ test
Now, the WAIS-4 (Weschler Adult Intelligence Scale) and WISC-5 (Weschler Intelligence Scale for Children) are more popular
Test Construction:
Standardization: everyone gets tested with consistent procedures and environment
Reliability: test gets similar results every time it is administered
Split-half reliability: if the test is split into two or more parts, does each part yield similar results?
Test-retest reliability: if someone is tested again, will they get a similar score?
Validity: test measures what it’s supposed to measure
Predictive validity: ability of a test to measure future outcome
Construct validity: ability of a test to measure factors that aren’t directly observable
Researchers of Intelligence:
Researcher | Belief |
Alfred Binet | IQ tests do not measure an inborn or permanent level of intelligence and should be used to identify students who needed more academic assistance. Intelligence is too complex to be quantified by a number |
Lewis Terman | IQ is inherited and the strongest predictor of one’s success in life |
Charles Spearman | IQ is made up of S-factors (specific factors) that make up one big G-factor (general intelligence). Specific factors are often positively correlated with each other |
Louis Leon Thurstone | IQ is made up of seven factors: verbal comprehension, verbal fluency, numerical ability, perceptual speed, spatial visualization, inductive reasoning, and memory |
Howard Gardner | IQ is made up of eight factors: naturalist, spatial, musical, kinesthetic, linguistic, intrapersonal, interpersonal, and logical |
Robert Sternberg | IQ is made up of three main factors: analytical intelligence (book smarts), practical intelligence (street smarts), and creative intelligence (creativity) |
Unit 3: Development
Development is the chronological order of development and thematic issues in development across the lifespan.
Three main areas of interest:
Nature vs nurture
Stability vs change
Continuity vs stages
Observational learning - observing and modeling another person’s behaviors, attitudes, or emotional expressions
Bobo doll experiment - an experiment that proved that children can learn by observing another person’s behaviors
Development
Physical Development
Infants have reflexes such as the rooting reflex (when the corner of a baby’s mouth is stroked or touched, it will begin to “root” towards the source of the touch in search of a nipple)
Visual cliff - infants have a basic sense of depth perception that allow them to tell when a large drop is incoming.
Critical periods - there is a period for which children are best able to learn things. If they miss that period, they may never be able to do it.
Adolescence is when puberty and sexual development occur, happens around 8-12 years old.
Adults generally have a stagnation in development and then a gradual decline in older adulthood.
Teratogens are substances that negatively impact development in utero, such as alcohol.
Cognitive Development
Piaget’s Stages of Cognitive Development
Stage | Age | Milestones |
Sensorimotor | Infancy through toddlerhood | Object permanence |
Preoperational | Toddlerhood through early childhood | Usage of mental symbols, pretend play, egocentrism, animism, basic theory of mind |
Concrete operational | Early through late childhood | Conservation, reversibility, thinking logically |
Formal operational | Late childhood through adulthood | Thinking abstractly, thinking hypothetically, understanding abstract concepts |
Note: Piaget theorized that not all people make it to the formal operational stage.
Children are social learners who learn by interacting with other people (Vygotsky)
Zone of proximal development - space between what a learner can do with assistance and what they can do without assistance
Language Development
Language is a shared (mutually agreed upon) system of arbitrary symbols (often expressed as and combined into phonemes, morphemes, and semantics) that are rule-governed (via grammar and syntax) and generative to produce an infinity of ideas.
Phoneme - smallest basic unit of sound
Morpheme - smallest meaningful unit of sound
Semantics - the meaning of language
People of all cultures also use nonverbal gestures to communicate.
Babies learn how to talk in a certain order:
Cooing - doesn’t sound like anything
Babbling - meaningless word sounds, may not be used in parents’ native language
One-word stage - one word sentences or phrases
Telegraphic speech - short sentences where only words that carry information are used (ie “go bed”)
Linguistic determinism - human thought and knowledge is limited by language
Chomsky - psychologist who believed that children are biologically predisposed to want to learn language
Social/Emotional Development
Ecological Systems Theory:
Microsystem - groups that have direct contact with the individual
Mesosystem - the relationships between groups in the microsystem
Exosystem - indirect factors in an individual’s life
Macrosystem - cultural events that affect the individuals and others around them
Chronosystem - the individual’s current stage of life
4 Parenting Styles
Authoritarian - parents are demanding and often don’t listen to their child
Authoritative (best) - parents are demanding but listen to their child and respect their child’s wants and needs
Permissive - parents are lax on rules, have a “friend” relationship with their child
Uninvolved - parents aren’t around much and don’t have much of a relationship with the child

Attachment Styles:
Secure attachment - not too clingy, but not aloof. People with secure attachment generally had attentive parents as babies.
Insecure attachment - often overly clingy, overly aloof, or both. People with insecure attachment generally had inattentive parents as babies.
Anxious attachment - characterized by a persistent fear of abandonment and rejection, insecurity, low self-esteem, and clinginess
Avoidant attachment - characterized by difficulties trusting others, forming relationships, and being emotionally close to others
Disorganized attachment - combination of anxious and avoidant attachment styles
Separation anxiety - babies and young children often feel anxious or upset when separated from their parents
Social Relationships Over Time:
Children - engage in play with peers
Parallel play - playing next to another child, but not with them
Pretend play - playing imaginative games with another child
Adolescents - often egocentric and self-conscious, but with strong desire for social relationships
Imaginary audience - believing people are constantly watching/paying attention to you
Personal fable - the belief that one is special, unique, and protected from life’s consequences
Adults - social pressures influence life choices
Social clock - culture plays a role in determining when adulthood starts and when life milestones (ie marriage, having kids, buying a home) should occur
Erikson’s Stages of Psychosocial Development:

Trust vs mistrust - caregivers meeting basic needs
Autonomy vs shame and doubt - the desire to be independent vs doubting one’s abilities
Initiative vs guilt - initiative leads to a sense of purpose, while failure results in feelings of guilt
Industry vs inferiority - children begin to learn what they are and aren’t good at
Identity vs role confusion - adolescents begin to develop their own concept of self-identity
Intimacy vs isolation - wanting to form close relationships
Generativity vs stagnation - wanting to make a positive impact on the world vs feeling stuck and unproductive
Integrity vs despair - looking back at life as well lived or with regrets
Kohlberg’s Theory of Moral Development:
Preconventional morality - early childhood, focused on doing the right thing to not get punished
Conventional morality - adolescence to adulthood, focused on maintaining social order
Postconventional morality - some adults, rare, focused on doing the right thing even if it violates societal conventions
Adverse childhood experiences - traumatic events in childhood that can have impacts on someone as an adult
Conditioning
Classical Conditioning
Classical conditioning - the association of one stimulus with another to elicit a response
Unconditioned stimulus and neutral stimulus paired together to get unconditioned response. Eventually, the former neutral stimulus becomes the conditioned stimulus, which on its own is enough to get the conditioned response (formerly the unconditioned response).
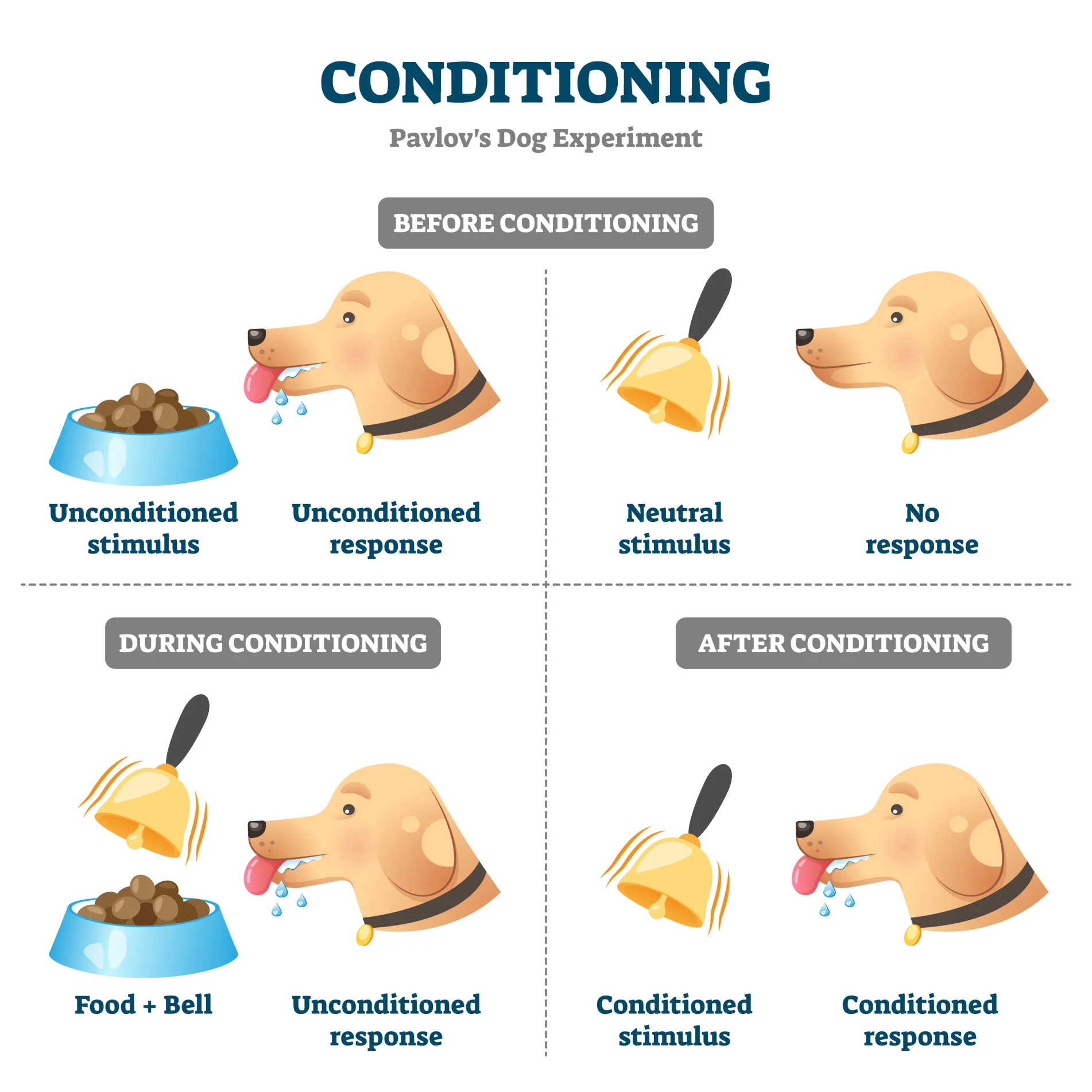
Unconditioned - inborn, innate
Conditioned - learned
After a while, a conditioned response will become extinct! However, if you wait a period of time without the conditioned stimulus and then reintroduce it, the conditioned response will reoccur, albeit with less strength.
Higher order conditioning - using an old conditioned stimulus as the new unconditioned stimulus in a new session of classical conditioning
Stimulus generalization - ability to group several similar stimuli and respond to all of them
Stimulus discrimination - ability to distinguish between several similar stimuli
Habituation - occurs when one gets accustomed to a stimulus, decreasing
response to it
Operant Conditioning
Law of effect - rewarded behaviors are likely to be repeated while punished behaviors are not likely to be repeated (Thorndike)
Operant conditioning - using rewards and punishments to modify behavior (Skinner)
Shaping - gradually getting behavior closer to a goal by having the subject do closer and closer approximations of a goal behavior
Instinctive drift - some behaviors can’t be trained because they go against an animal’s instincts
Latent learning - knowledge acquired without immediate reinforcement (Tolman)
Cognitive maps - people create mental maps of their surroundings that they can use to get around even if they’re forced to take an unfamiliar path (Tolman)
Types of Reinforcement and Punishment:
Reinforcement | Punishment | |
Positive | Positive reinforcement - something good is added to reward a behavior | Positive punishment - something bad is added to punish a behavior |
Negative | Negative reinforcement - something bad is removed to reward a behavior | Negative punishment - something good is removed to punish a behavior |
Reinforcement increases the likelihood of a behavior happening again while punishment decreases it.
Types of Reinforcement Schedules:
Fixed | Variable | |
Interval | Fixed interval - reinforcement is given after every fixed period of time | Variable interval - reinforcement is given after varying amounts of time |
Ratio | Fixed ratio - reinforcement is given after a fixed number of occurrences of the behavior | Variable ratio - reinforcement is given after a varying number of occurrences of the behavior |
Continuous reinforcement schedules reward behaviors after every instance.
Unit 4: Social Psychology
Attributions and Attitudes
Attributions
Attributions - how people explain behavior and mental process of themselves and others
Explanatory style - how people explain good and bad events in their lives and the lives of others
Explanatory style can be optimistic or pessimistic
Locus of control - whether people believe that their lives are controlled by themselves (internal locus of control) or by outside factors they can’t control (external locus of control)
Common cognitive biases:
Actor-observer bias: we tend to attribute the behavior of others to their personality, and our own behavior to the situation
Fundamental attribution error: we tend to attribute the behavior of others to dispositional, rather than situational, factors
Self-serving bias: we tend to credit our successes to our dispositions, but fault the situation for our failures
Mere exposure effect - people tend to like something better simply by being exposed to it repeatedly
Self-fulfilling prophecy - people behave in ways that will cause the thing to happen that they already believe will happen
Social comparison - comparing your own status to others in your social circle or environment
Relative deprivation - a feeling of deprivation (having less) compared to others in your social circle or environment
Beliefs and Stereotypes
Stereotype - generalized concept about a group
Stereotypes can help us reduce cognitive load (the mental load required to process information) when making decisions or judgements
Stereotypes can be the basis of prejudiced attitudes and discriminatory behavior
Implicit attitudes - attitudes people hold but are unaware of
Belief perseverance - continuing to believe something even after evidence suggests that it isn’t true
Cognitive dissonance - mental discomfort when someone’s actions and attitudes/beliefs don’t align
Social Situations
Social norms - expectations and norms that society has for an individual
Social norms can differ for different groups of people (eg men and women)
Social influence theory - social influences pressure people to behave differently
Normative social influence - people do something because everyone else is doing it
Informational social influence - people believe something because everyone else believes it
Conformity - adhering to unspoken rules and norms to fit in with everyone else
Obedience - people tend to do what an authority figure tells them to, even if it doesn’t align with their beliefs
Persuasion - the act of convincing someone of particular ideas, actions, or beliefs
Central route persuasion: using facts and logic to convince someone of an argument
Peripheral route persuasion: using indirect methods of persuasion, such as emotional cues, to convince someone of an argument
Halo effect: the tendency for positive impressions of a person, company, country, brand, or product to positively influence one’s opinions or feelings
Foot-in-the-door phenomenon - agreeing to a small request increases the odds we’ll agree to a large request later
Face-in-the-door phenomenon - agreeing to a large request increases the odds that we’ll agree to additional small requests
Cultural Phenomena:
Individualism - the idea that individuals should control their own lives, rather than being focused on the collective (most Western countries follow this philosophy)
Collectivism - the idea that the needs of the collective, rather than the individual, are most important (most Eastern countries follow this philosophy)
Multiculturalism - integrating ideas and principles from different cultures
Mental Processes in Group Situations:
Group polarization - when members of a group who share a common opinion or belief discuss it, the individuals tend to get more radical in their beliefs
Groupthink - a group makes decisions that may not be optimal in order to preserve the harmony of the group, regardless whether individual members of the group believe it’s the best decision or not
Diffusion of responsibility - people are less likely to take action when many other people are around
Social loafing - people tend to do less work in a group than they would have on their own
Social facilitation - people tend to do better at simple/well-learned tasks and worse at complex/poorly-learned tasks when other people are watching
False consensus effect - people tend to overestimate the extent to which other people agree with them
Superordinate goals - goals that unite an entire group to work towards one goal
Social traps - when members of a group individually seek their own self-interests rather than the interests of the group
Altruism - selfless actions to help other people
Social reciprocity norm - social rule that people should return a favor when someone has helped them
Social responsibility norm - social rule that we should help others in need, even when we don’t expect anything in return
Personality, Motivation and Emotion
Theories of Personality
Psychodynamic Theory
Unconscious processes drive personality
Our brains subconsciously defend our egos from threats
We can use projective tests (tests involving the interpretation of ambiguous stimuli like inkblots) to determine someone’s personality
3 parts of our personality
Id: impulsive, rash, selfish
Superego: selfless, moral, conscientious
Ego: balances the id and superego
Ego defense mechanism | Definition |
Denial | Insisting that something isn’t actually true or real when it is |
Displacement | Redirecting an emotional reaction from one object or person to another |
Projection | Convincing yourself that your own actions or mental processes also apply to other people to protect yourself from internal discomfort |
Rationalization | Justifying your behavior/mental processes or those of others by creating seemingly logical explanations to avoid confronting the actual reason |
Reaction formation | Acting in a way opposite of your true feelings |
Regression | Reverting to more childlike behaviors in response to stress or an overwhelming situation |
Repression | Putting distressing thoughts or memories out of your mind |
Sublimation | Channeling unacceptable or uncomfortable emotions or impulses into constructive, socially acceptable activities |
Freud’s Theory of Psychosexual Development
We go through different stages of development in childhood related to unconscious sexual behaviors and mental processes
If someone becomes “fixated” in a stage, it could have adverse effects for them as an adult
Stage | Age | Description | Results of Fixation |
Oral | 0-1 | Babies like to put things in their mouth | Oral passive - trusting, dependent Oral aggressive - aggressive, dominating |
Anal | 2-3 | Children begin potty training | Anal retentive - tidy, obsessive, perfectionist Anal expulsive - untidy, generous |
Phallic | 3-6 | Children become more attached to their opposite-sex parent | Vain, self-obsessed, envious, feelings of inadequacy, sexual anxiety |
Latency | 6-puberty | No psychosexual impulses in this stage | N/A |
Genital | Puberty and beyond | Teens begin experiencing sexual attraction and wanting to have sex | Well-balanced, warm, caring |
Humanistic Theory
We aim to self-actualize: become the best people we can be
We want to grow and fulfill our potential
Humans are intrinsically good
Carl Rogers and Abraham Maslow were big proponents of this theory
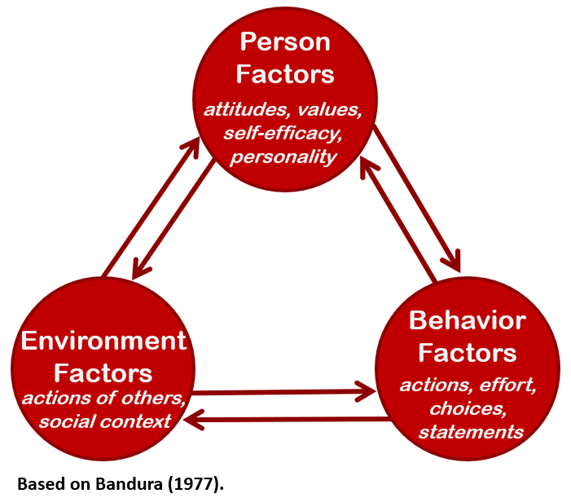
Social-Cognitive Theory
“Reciprocal determinism” shapes personality
Reciprocal determinism - behavior, personal factors, and environmental factors mutually influence each other
Self-concept - how we view ourselves, made up of self-esteem and self-efficacy
Self-esteem - our view of our own worth and value
Self-efficacy - our view of our own competence
Albert Bandura was a proponent of this theory
Trait Theory
Our personalities are made of mostly stagnant traits
Our traits determine our behavior
“Big Five” theory: our personalities are governed by 5 main traits
Openness, conscientiousness, extraversion, agreeableness, neuroticism (OCEAN)
Motivation
Theories of Motivation
Theory | Description |
Drive-reduction | People are motivated to maintain homeostasis |
Arousal | People are driven to maintain an optimal level of arousal |
Self-determination | People are motivated by intrinsic (internal) factors and extrinsic (external) factors |
Instinct | Animals are driven by universal, innate fixed patterns of behavior |
Motivational conflicts | Our behavior is based on our responses to motivational conflicts
|
Sensation seeking | People are driven to experience novel sensations and experiences |
Eating
Eating is a complex behavior driven by both physical and mental processes
Hormones regulated by the hypothalamus and pituitary gland, such as leptin and grehlin, make us hungry
Other factors such as time of day, presence of food, and social gatherings influence hunger
Emotion
Emotions are influenced by internal and external factors affecting an individual
Some psychologists believe that emotions are caused by physical responses, some believe that a cognitive label is needed to experience an emotion, and some believe that they happen simultaneously
Facial-feedback hypothesis: our emotions are influenced by our facial expressions
Broaden-and-build theory: positive emotions tend to broaden awareness and increase new thoughts/actions; negative emotions tend to narrow awareness and decrease new thoughts/actions
Psychologists aren’t sure if there are universally felt emotions, such as anger, disgust, sadness, happiness, surprise, and fear
Social rules and demographics such as culture, age, gender, and socioeconomic status influence how we express and interpret emotions
Mental and Physical Health
Health Psychology
Stress
Stress increases someone’s susceptibility to disease and disorders. It weakens the immune system and can also increase someone’s susceptibility of autoimmune disorders (the immune system attacks itself).
Some physiological conditions that stress contributes to include:
Hypertension
Headaches
Heart attack
Type 2 diabetes
Infertility
Eustress - stress that motivates and excites you
Distress - debilitating, harmful stress
Adverse childhood experiences - a group of 10 childhood experiences that increases someone’s likelihood of experiencing physical and mental conditions as well as poverty
General adaptation syndrome - 3 stage model of stress reactions created by Hans Selye
Alarm reaction - first exposure to the stressor, frequently involves a fight/flight/freeze reaction
Resistance - a phase where the stress is confronted, this phase is difficult but the person is still able to cope with the stressor
Exhaustion - a phase that occurs either when the stressor subsides or someone’s mental/physical resources are spent. They can’t cope well with the stressor anymore if it’s still around and they have a high susceptibility to physical illness
Responses to stress differ among people, cultures, and genders. Some common stress responses and coping mechanisms include:
Tend-and-befriend response: responding to a stressor by interacting with or tending to the needs of other people. This is more common in women than men
Problem-focused coping: focusing on the source of the stressor as a problem to be solved and trying to come up with a solution
Emotion-focused coping: managing emotional responses to the stressor as a way of coping (ex deep breathing, meditation)
Positive Psychology
Positive psychology seeks to identify factors that lead to increased mental well-being, resilience, and positive emotions.
Expressing gratitude and exercising character strengths can increase someone’s mental well-being. Some common character strengths (virtues) include:
Wisdom - being curious and creative, seeking to gain knowledge, trying to see from different perspectives
Courage - bravery, persistence, integrity
Humanity - love, kindness, being a good person, helping others
Justice - fairness, leadership, being an active citizen
Temperance - forgiveness, humility, self-control
Transcendence - gratitude, hope, spirituality, a sense of purpose, a connection with the greater world
Post-traumatic growth may be experienced after experiencing periods of stress (“what doesn’t kill you makes you stronger”)
Mental Disorders
Classification of Mental Disorders
Three main criteria are used to determine if something would be considered a mental disorder or if someone has a mental disorder:
Level of dysfunction: is the person unable to do things that people typically can? To what extent do these things impact their life?
Perception of distress: is the person harmed by these traits? Do these traits decrease their mental wellbeing?
Deviation from the social norm: are the person’s experiences significantly different from what is typical? This can vary between cultures.
Being diagnosed with a mental disorder can be considered positive or negative for a person depending on the specific disorder, the specific person, the level of stigma around the disorder, and factors related to discrimination, racism, sexism, and ageism. Labels can cause us to make unjustified assumptions about people, but they can also be a revelation for other people and help them get access to support.
Psychologists and psychiatrists use two manuals to classify and diagnose mental disorders. The International Classification of Diseases (ICD) is a manual used worldwide that includes many different diseases and disorders, not just psychological ones. The Diagnostic and Statistical Manual of Mental Disorders (DSM) is a manual created by the American Psychological Association and is used primarily in the United States, although also in other countries. The DSM only contains information about mental and psychological disorders.
Frequently, both the ICD and the DSM are revised due to new scientific and psychological information and viewpoints. As of 2025, we are currently on the DSM-5-TR (5th edition, text revision) and the ICD-11 (11th edition).
Psychologists and psychiatrists are not sure what causes mental disorders, but the current scientific consensus is that it’s a mix of genetic, environmental, and biological factors (biopsychosocial approach). The diathesis stress model says that mental disorders develop as a result of genetic predispositions (diathesis) and stressful life experiences (stress).
Perspective | Causes of mental disorders |
Behavioral | Maladaptive (not suitable for the situation) learned associations between or responses to stimuli Example: A veteran associating any explosion with war, even the explosions of fireworks and firecrackers. |
Psychodynamic | Unconscious thoughts and experiences, commonly developed during childhood Example: A child frequently feels angry towards their parents. They begin to have unconscious anger for all authority figures and frequently lash out at their bosses as an adult. |
Humanistic | Lack of social support, inability to fulfill one’s potential Example: A woman in poverty raising 2 small children has very little social support to help her handle the stress and develops an anxiety disorder. |
Cognitive | Maladaptive thoughts, beliefs, attitudes, or emotions Example: After a streak of bad luck, a man starts to believe he is worthless and ends up developing depression. |
Evolutionary | Behaviors and mental processes that reduce the likelihood of survival Example: A person with borderline personality disorder frequently makes rash and emotional decisions, endangering themself and others. |
Sociocultural | Maladaptive social and cultural relationships/dynamics Example: After moving to a new country, a teenager struggles to fit in and understand the country’s culture, and begins to feel depressed and anxious because of it. |
Biological | Physiological and genetic issues Example: A woman and her husband have ADHD. Because ADHD has a significant genetic component, 2 out of her 3 children also have ADHD. |
Most psychologists use an eclectic approach (mix of all of these) when determining the cause of someone’s mental illness or disorder.
Neurodevelopmental Disorders
Neurodevelopmental disorders are disorders that affect the way someone’s brain develops and functions. Unlike most other disorders, neurodevelopmental disorders have an onset before or soon after birth and last someone’s entire life.
Attention-Deficit/Hyperactivity Disorder (ADHD) is a common neurodevelopmental disorder that affects about 10% of the population. It involves a difficulty in executive function, a set of cognitive skills relating to someone’s ability to plan, concentrate, solve problems, and manage emotions. It is made up of 3 types of symptoms: inattention, hyperactivity, and impulsivity.
Inattention - trouble directing one’s attention properly. This is more common in women with ADHD than men and can include lack of attention and abnormally high focus on a specific thing or topic.
Hyperactivity - excessive moment and energy that can result in impatience, restlessness, and overtalkativeness.
Impulsivity - quick and rash decision making—”not thinking before you speak”. This can result in making thoughtless decisions, engaging in dangerous behaviors without thinking about the consequences, or oversharing in a conversation.
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder that impacts social functioning. It was created as a merger of several previously recognized disorders including autistic disorder and Asperger’s disorder. It is called a “spectrum disorder” because it can manifest in many different ways. Autism is characterized by 2 types of traits: social difficulties and restrictive/repetitive behaviors.
Social difficulties are difficulties that impair someone’s ability to communicate and socialize. Autistic people have trouble in the following domains:
Social reciprocity - someone’s ability to hold a back-and-forth conversation and respond to social cues
Nonverbal communication - someone’s ability to use and understand nonverbal gestures and vocal inflection
Maintaining relationships - making and keeping friends, relationships with family members
Restrictive and repetitive behaviors are atypical, strong, fixated behaviors including:
Atypical motor (physical) movements (“stimming”)
Oversensitivity or undersensitivity to sensory stimuli such as sound and touch
Strictly following routines and resistance to change
Very strong and specific interests (“special interests”)
Autism encompasses a wide variety of levels of “functioning” and support needed. Some autistic people may be able to live alone, have a job, and/or hide their autistic traits. Others might need a caregiver and not be able to hold a job.
It is unclear what exactly causes autism, but most psychologists and psychiatrists agree that it is a combination of genetic factors and environmental factors in the womb. Vaccines do not cause autism.
Schizophrenia Spectrum Disorders
Schizophrenia spectrum disorders are a group of severe mental illnesses, such as schizophrenia and schizoaffective disorder, and that can be chronic or temporary. They are characterized by issues in five areas:
Delusions - false beliefs about reality, despite incontrovertible proof to the contrary
Hallucinations - false sensory input, ie seeing or hearing things that aren’t really there
Disorganized speech/thinking - speech or thoughts that are jumbled or don’t make sense, “word salad”
Disorganized motor behavior - nonsensical and abnormal motor (physical) behavior, such as repeating a useless physical motion or being in a state of immobility and irresponsiveness (stupor).
Negative symptoms - symptoms that occur in healthy people but not people with schizophrenia spectrum disorders, such as flat affect (a lack of emotional expression) or a lack of movement (stupor)
Delusions, hallucinations, disorganized speech/thinking, and disorganized motor behaviors are examples of positive symptoms - symptoms that occur in people with schizophrenic spectrum disorders and not healthy people.
Psychosis - a general term for a collection of symptoms where someone is unable to distinguish between what’s real and what’s not. It includes symptoms such as hallucinations and delusions
Schizophrenic spectrum disorders are highly genetic, with a heritability of around 80%. Being born in winter months, prenatal virus exposure, and having a family member with a schizophrenic spectrum disorder increases someone’s risk of having a schizophrenic spectrum disorder.
The dopamine hypothesis of schizophrenic spectrum disorders hypothesizes that these disorders are caused or influenced by increases in dopamine in certain areas of the brain.
Depressive Disorders
Depressive disorders are disorders characterized by the long-term presence of a sad, empty, irritable mood and other psychological changes that affect a person’s ability to function. Depressive disorders can be, but are not necessarily, observable to other people around the depressed person. Having a depressive disorder increases someone’s risk of suicide or a suicide attempt, but not all depressed people will consider or attempt suicide.
Risk factors for depression include both environmental factors and biological factors. A history of abuse, major life changes, and a family history of depression can increase someone’s risk.
Major Depressive Disorder (MDD), also just called “depression”, is one of the most common mental illnesses and is characterized by a depressed mood for at least two consecutive weeks. Symptoms of depression include:
a depressed mood - feelings of sadness, hopelessness, and/or emptiness most of the day, almost every day.
loss of interest or pleasure in day-to-day activities, including typically fun activities such as hobbies
fatigue, insomnia, and/or hypersomnia (oversleeping)
feelings of worthlessness or guilt
thoughts of death or suicide
Major depressive disorder is sometimes called the “common cold” of mental illnesses due to its prevalence.
Persistent Depressive Disorder (PDD), sometimes called “dysthymia”, is a long-term mental illness where someone experiences depressive symptoms most days for two years. It is characterized by the same symptoms of major depressive disorder but is typically not as severe as MDD, but it lasts for a very long period of time. A person can have both persistent depressive disorder and major depressive disorder.
Bipolar Disorders
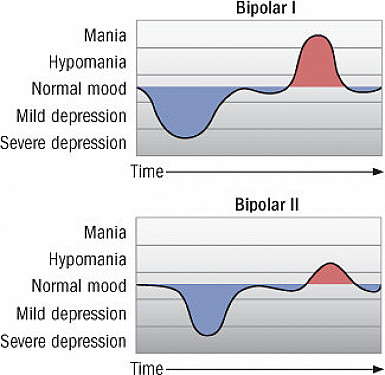
Bipolar disorders are disorders characterized by long-term, cycling periods of depression and mania or hypomania. Each period lasts days to weeks. Bipolar disorder is different from being emotional or rapidly cycling between emotions within a single day.
Depression - a sad, hopeless, or empty mood that lasts for at least 2 weeks.
Mania - an abnormally euphoric or elevated mood that significantly affects social and/or occupational functioning and lasts for at least a week.
Hypomania - a less severe form of mania that doesn’t necessarily significantly affect social or occupational functioning and lasts for at least 4 days.
Bipolar disorders are highly heritable—approximately 80 to 90 percent of people with bipolar disorder also have a relative with bipolar disorder. Stress, sleep disruption, and drug/alcohol use can also trigger bipolar disorders.
Bipolar I Disorder is a disorder characterized by at least one manic episode. Someone with Bipolar I may have had hypomanic or depressive episodes as well, but it’s not necessary for a diagnosis.
Some symptoms of a manic episode associated with Bipolar I disorder include:
inflated (increased) self-esteem
decreased need for sleep
being more talkative than usual
racing thoughts or distractibility
impulsive activities and choices such as shopping sprees
Some people who have a manic episode may need to be hospitalized due to the intensity of their episode. Some people with a manic episode might also experience psychotic features (schizophrenia-like symptoms such as hallucinations and delusions).
Bipolar II disorder is a disorder characterized by at least one hypomanic episode and at least one depressive episode. While a depressive episode is not required for a diagnosis of Bipolar I, it is required for a diagnosis of Bipolar II.
To be diagnosed with Bipolar II, someone should have never had a full manic episode and have only had hypomanic episodes. If they’ve had a manic episode, they should be diagnosed with Bipolar I instead.
Symptoms of a hypomanic episode are similar to symptoms of a manic episode, but don’t last as long, significantly affect occupational/social functioning, cause psychotic features, or result in hospitalization.
Anxiety Disorders
Anxiety disorders are disorders characterized by excessive fear or worry. While everyone experiences stress sometimes, to be diagnosed with an anxiety disorder, someone has to experience anxiety-related symptoms to the point that it is interfering with their life for a long period of time.
Women are more likely than men to have an anxiety disorder. Low self-esteem, past traumatic experiences, and a family history of depressive or anxiety disorders can increase someone’s likelihood of having an anxiety disorder.
Generalized Anxiety Disorder (GAD), sometimes called just “anxiety,” is characterized by abnormally high levels of worry about many different things that lasts at least 6 months. The anxiety is not restricted to social situations or one specific thing/situation. Some symptoms of GAD include:
excessive and/or uncontrollable levels of worry
fatigue
difficulty concentrating
sleep disturbance
restlessness
If MDD is the “common cold” of mental illnesses, GAD is the flu — it is one of the most common mental illnesses and affects about 3% of people per year.
Specific Phobia is a disorder characterized by excessive, disproportionately high anxiety about one specific thing or topic. A lot of people have phobias, but to be diagnosed with specific phobia the phobia must be long-term and negatively affect someone’s wellbeing. Some common phobias include acrophobia (fear of heights) and arachnophobia (fear of spiders)
Social Anxiety Disorder is characterized by an excessive fear of being judged, watched, or scrutinized by others. This anxiety occurs in public situations such as talking with new people, eating dinner in public, or giving a speech. People with social anxiety might avoid triggering social situations, or try to persist through them while feeling extreme fear.
Agoraphobia is characterized by fear of being trapped or unable to escape while in a public space. Some potentially anxiety-inducing situations for a person with agoraphobia could include standing in line, being in a crowded place, or using public transportation.
Panic Disorder is an anxiety disorder in which people experience sudden, unexpected “panic attacks”. Panic attacks can last for minutes to hours and are characterized by extreme fear and physical symptoms. Someone with panic disorder might also feel additional anxiety about not knowing when they might have a panic attack or if one will happen in a public situation.
During a panic attack, someone might feel:
intense terror
a sensation of being unable to breathe
sweating
dizziness
feelings of depersonalization (being disconnected from yourself) or derealization (being disconnected from the world)
Obsessive-Compulsive and Related Disorders
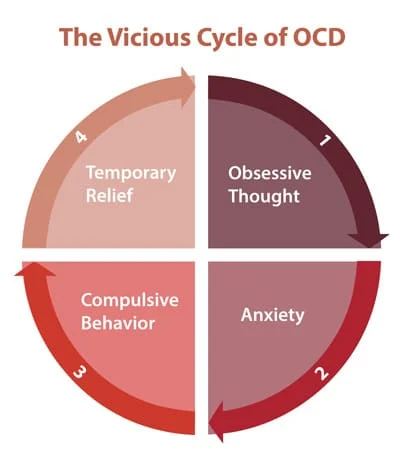
Obsessive-compulsive disorders are disorders that involve uncontrollable and recurring thoughts (obsessions) and actions done to resolve the anxiety caused by those thoughts (compulsions). These disorders may be caused by genetic factors, learned associations between stimuli, or maladaptive thinking.
Obsessive-Compulsive Disorder (OCD) is a mental illness in which someone experiences obsessions and compulsions. Obsessions generally involve an irrational fear of something bad happening or unwanted urges to do things the person would never actually do (intrusive thoughts). To stop these obsessions, a person with OCD feels the need to do a compulsion - a seemingly illogical task that relieves the anxiety caused by the obsession. A compulsion might not seem to have anything to do with an obsession, but it makes sense inside the person with OCD’s head.
Some common topics of obsessions include:
getting sick, having a rare disease, or things being contaminated
having forgotten to do something important, such as lock the door
harming oneself or other people
things being unordered or asymmetric or otherwise “imperfect”.
unwanted sexual or violent imagery
Some common compulsions include:
repeatedly washing one’s hands
checking things repeatedly, such as if a stove is off
counting things
self-harming behaviors
Someone with OCD might repeat a compulsion several times. They might also feel the need to restart a compulsion if they feel they’ve made a mistake.
Hoarding Disorder is a disorder in which people have difficulty throwing things away or getting rid of things, resulting in a large accumulation of extra stuff. Someone with Hoarding Disorder might feel distressed at the idea of getting rid of the items, feel that they need to save the items, or feel that the items will be sad if they throw them away. People with Hoarding Disorder feel this way regardless of an item’s monetary or sentimental value.
Dissociative Disorders
Dissociative disorders are characterized by feelings of disconnect from your consciousness, identity, memory, emotion, perception, and even motor control. Dissociative disorders are thought to be caused by severe stress or trauma, particularly childhood trauma. People with dissociative disorders might experience depersonalization.
Depersonalization - a feeling of detachment from your body, or like your body isn’t real or isn’t really yours
Derealization - a feeling of detachment from the world, or like the world isn’t real
Dissociative Amnesia happens when someone’s brain blocks out certain memories after a very stressful or traumatic experience. It is generally caused by the person’s brain trying to protect them from unpleasant, distressing, or traumatic experiences. People with dissociative amnesia still have the memories, but can’t retrieve them. Some types of dissociative amnesia include:
Localized - all memories from a short, specific period of time
Selective - one or some memories from a short, specific period of time
Generalized - all memories from a long period of time (months to years)
Continuous - memories formed after the onset of the dissociative amnesia (a form of anterograde amnesia)
Systematized - all memories related to a certain topic
Some people with dissociative amnesia might experience dissociative fugue, a temporary state where someone can’t remember personal details about themselves and may impulsively wander away.
Dissociative Identity Disorder (DID) is a disorder in which someone experiences two or more distinct identities or personality states. People with DID frequently experience large gaps in memory and cannot remember anything that their other identities said or did. They might not know they have DID. DID is strongly associated with severe trauma in early childhood. DID was formerly called Multiple Personality Disorder.
Trauma and Stressor-Related Disorders
Trauma and stressor-related disorders are disorders caused by a traumatic event or experience. People with these disorders may experience intense anxiety, but these disorders are different than anxiety disorders because they arise from a specific traumatic experience. Traumatic experiences can be short-term, long-term, or ongoing.
Post-Traumatic Stress Disorder (PTSD) is a disorder in which someone experiences severe anxiety related to a traumatic event they have experienced. PTSD is common among veterans, but can also occur in other groups, such as people who have experienced or witnessed violence or assault. A person with PTSD might have intrusive reminders or thoughts about the traumatic event.
Some symptoms of PTSD include:
recurring, unwanted memories, dreams, or flashbacks
avoidance of things that could remind the person of the traumatic event
persistent negative emotions and inability to experience positive emotions
out-of-proportion negative beliefs about or negative expectations for the world or oneself
hypervigilance
Feeding and Eating Disorders
Feeding and eating disorders involve altered consumption of food. They can involve undereating, overeating, eating non-food objects, and other abnormal eating practices. People who are overweight or obese can have eating disorders. Eating disorders are more common among women than men, but men can have them as well. Eating disorders may be caused by social and sociocultural influences, as well as biological or genetic factors.
Anorexia Nervosa is a disorder in which a person severely limits their eating out of extreme fear of becoming “fat” and a distorted body image. People with anorexia might refuse to eat certain foods, set a calorie limit for themselves, or exercise obsessively. They might also binge-eat or purge the food they have eaten.
Symptoms of anorexia include:
intense fear of gaining weight
underweight
denial of the seriousness of one’s low weight
missed periods
Bulimia Nervosa is a disorder in which a person has repeated episodes of binge-eating followed by compensatory behaviors to get rid of or make up for the food they have eaten. A person with bulimia might throw up the food they just ate, use laxatives, or excessively exercise to “make up” for the food.
Personality Disorders
Personality disorders are groups of stable, persistent traits that interfere with a person’s ability to function socially and/or occupationally. Personality disorders usually onset in childhood, adolescence, or early adulthood and are strongly linked to genetics and adverse childhood experiences. Despite this, personality disorders are typically not diagnosed until someone is an adult because someone’s personality traits can change rapidly while they are a child or teenager.
There are 3 clusters, or groups, of personality disorders, each defined by a specific trait that makes it hard for the person with the personality disorder to fit into society. These clusters are:
Cluster A - Odd, eccentric
Paranoid Personality Disorder - pervasive distrust and suspiciousness of others
Schizoid Personality Disorder - little interest in close relationships, limited emotional expression (note: this disorder is not linked with schizophrenia or psychosis)
Schizotypal Personality Disorder - paranoia, isolation and lack of close relationships, odd or magical thinking (note: this disorder is associated with schizophrenia and schizophrenic spectrum disorders)
Cluster B - Dramatic, emotional, erratic
Histrionic Personality Disorder (HPD) - attention-seeking behavior, overexaggerated displays of emotion
Narcissistic Personality Disorder (NPD) - excessive need for admiration, inflated self-image (ego)
Borderline Personality Disorder (BPD) - unstable and intense relationships, strong fear of abandonment, impulsivity
Antisocial Personality Disorder (ASPD) - lack of empathy and disregard for others
Cluster C - Anxious, fearful
Avoidant Personality Disorder (AVPD) - strong fear of rejection and low self-esteem (Note: this is different from social anxiety disorder because people with social anxiety disorder typically know that their feelings of anxiety are irrational, while people with AVPD don’t.)
Dependent Personality Disorder - long-term need for others to take care of them
Obsessive-Compulsive Personality Disorder (OCPD) - perfectionism and excessive need for rules and order (note: OCPD is different than OCD because it does not involve obsessions or compulsions, and the person with OCPD does not typically realize that their behaviors are irrational.)
Treatment of Psychological Disorders
When someone has a mental disorder, there are many different ways to treat it, and they might work better or worse for different people - similar to physical disorders and conditions.
Before the mid-20th century, many mentally ill and mentally disabled people were institutionalized. However, with the improvement of mental health treatments and the medical model, which treated mental illnesses as something that could be treated just like physical illness, rapid deinstitutionalization began. Most people with mental illness do not live in institutions anymore unless they are a danger to themselves or others.
Dorothea Dix - brought the medical model to America
Psychotherapy
Psychotherapy is a commonly-used treatment for mental illnesses. It tends to be somewhat effective, although people tend to consider it more effective than it actually is.
Different therapists use different psychological theories and perspectives to help people, such as using a psychodynamic approach or a humanistic approach
Cognitive-behavioral therapy - a common type of therapy in which a therapist targets a person’s irrational, self-degrading, or false thoughts (cognitive) and their maladaptive physical actions and behaviors (behavioral).
It’s important for therapists to follow standards of ethics, such as integrity and maleficence (“doing no harm”). Therapists are bound by confidentiality rules and can’t tell anyone what you said in a session unless they think you’re at risk to yourself or others.
Types of Therapy:
Type | What it Treats | Techniques Used | |
Cognitive | Negative thoughts about oneself, the world, and the future | Cognitive restructuring, fear hierarchies | |
Applied Behavior Analysis | Developmental disabilities, mental disorders | Applied conditioning, exposure therapies, aversion therapies, token economy, biofeedback | |
Cognitive-Behavioral | Both the mental and behavioral aspects of mental disorders | Rational-emotive behavior therapy, dialetical behavior therapy | |
Humanistic | Mental disorders | Active listening, unconditional positive regard | |
Psychodynamic | Mental disorders | Free association, dream analysis |
Therapeutic Techniques:
Technique | Type of Therapy | Definition |
Cognitive restructuring | Cognitive | Learning to analyze one’s thoughts to identify irrational thoughts and cognitive distortions |
Fear hierarchies | Cognitive | Using a ranked list to gradually confront your fears |
Exposure therapies | Applied Behavior Analysis | Exposing someone to their fears in order to decrease their anxiety |
Aversion therapies | Applied Behavior Analysis | Creating associations between something one wants to avoid (such as smoking) and a negative or unpleasant stimulus |
Token economy | Applied Behavior Analysis | Trading in “tokens” earned for good behavior to win prizes |
Biofeedback | Applied Behavior Analysis | A technique to gain greater control of physiological responses such as breathing and heart rate |
Rational-emotive behavior therapy | Cognitive-Behavioral | A technique to identify and challenge self-defeating thoughts |
Dialetical behavior therapy | Cognitive-Behavioral | A type of therapy similar to cognitive-behavior, but for people who experience emotions very strongly |
Active listening | Humanistic | Fully attuning to a speaker’s message and nonverbal cues and responding thoughtfully |
Unconditional positive regard | Humanistic | Accepting and supporting a person regardless of what the person says or does |
Free association | Psychodynamic | Saying or writing whatever comes to mind |
Dream analysis | Psychodynamic | Analyzing the deeper meanings of one’s dreams |
Hypnosis has also proven as a useful treatment for pain and anxiety, but not helpful for memory retrieval or age regression.
Psychoactive Drugs
Psychoactive drugs are medications that treat symptoms of mental illnesses. They are frequently most effective when paired with psychotherapy. Psychoactive drugs were a major factor leading to the deinstitutionalization of people with mental illnesses.
Common types of psychoactive drugs:
Type | Treats | Biological Function | Side Effects / Risks | Brand Names |
Antidepressants | Depression, anxiety (sometimes) | Stops reuptake of dopamine or norepinephrine in the brain | tiredness, headaches, nausea, sexual dysfunction, serotonin syndrome, therapeutic lag | Prozac, Zoloft, Wellbutrin |
Anti-anxiety drugs | Anxiety | Enhances the effect of GABA, a neurotransmitter that decreases anxiety | tiredness, confusion, dizziness, loss of balance, risk of addiction | Xanax, Valium |
Lithium | Bipolar disorder | Changes levels of certain neurotransmitters in the brain | nausea, tiredness, tremor, brain fog, weight gain | Eskolith, Priadel, Liskonum |
Antipsychotics | Schizophrenia, bipolar (sometimes) | Block dopamine receptors in the brain | tardive dyskinesia, weight gain, dizziness, tiredness | Abilify, Rexulti |
Stimulants | ADHD | Increase levels of dopamine in the brain | decreased appetite, anxiety, jitteriness, risk of addiction | Adderall, Vyvanse, Ritalin, Concerta |
Psychosurgery
Psychosurgery used to be more common after the invention of the leukotomy by Antonio Egas Moniz, who asserted the procedure’s safety and effectiveness. The leukotomy was brought to America and was renamed the lobotomy by Walter Freeman and James Watts, but declined in use in the 1950s and 1960s due to improvements in psychoactive drugs and a view of the lobotomy as a barbaric and ineffective practice. Today, lobotomies are not performed and psychosurgery is only used in rare cases when all other options have been exhausted.
Transcranial Magnetic Stimulation (TMS) is a noninvasive procedure that uses magnetic fields to stimulate nerve cells in the brain and reduce symptoms of major depression. It’s typically used when other depression treatments, such as antidepressants, haven’t been effective.
Electroconvulsive therapy is a treatment in which small, electric currents are passed through the brain while the patient is under general anesthesia. It typically rewires a person’s brain chemistry and is used in cases of severe or treatment-resistent depression.
Psychosurgery is when surgeons carefully lesion specific areas of brain tissue. It is generally a last resort because it is irreversible. It is used in cases of severe depression, anxiety, and OCD.