Week 12 PSY10007 Lecture and Module Videos - Psychological Disorders And Treatment
Concise Version
Psychological Disorders and Treatment
Introduction
Overview of psychopathology and taxonomy.
Exploration of psychological disorder models, diagnosis, and classification systems.
Discussion of psychological and biological treatment frameworks.
Learning Objectives
Outline and understand psychological disorders.
Identify key aspects of different psychological disorders.
Describe different approaches to the treatment of psychological disorders.
Outline the biological aspects of treatment.
Outline the role of prevention of psychological disorders.
Quote on Therapeutic Situation
"The distortion of truth in the myth of the analytic situation is that analysis is an interaction between a sick person and a healthy one."
"The truth is that it is an interaction between two personalities in both of which the ego is under pressure from the id, the superego and the external world. Each personality has its internal and external dependencies, anxieties and pathological defenses. Each is also a child with his internal parents and each of these whole personalities that of the analysand and that of the analyst responds to every event in the analytic situation."
Highlights the importance of viewing individuals with disorders as people and recognizing the mutual process in treatment.
Psychopathology Definition
Maladaptive, disruptive, or uncomfortable patterns of thinking, feeling, and behaving.
Affects individuals and their interactions with others (families, carers, and the community).
Worldwide, over 400 million people suffer from some form of psychological disorder.
Data from Australia (1993-2011) showed varying prevalence rates:
Severe: ~600,000 Australians
Moderate: ~1 million Australians
Mild: ~2 million Australians
Abnormal Psychology
Abnormal definition:
Deviance from the average or normal.
Distress experienced by the individual.
Dysfunction in expected or desired functioning.
Models of Psychopathology
Biopsychosocial Model
Interaction between biological, psychological, social, and environmental factors in the emergence and maintenance of disorders.
Biological Factors:
Medical model: disorders stem from an underlying illness.
Biological factors (e.g., chemical imbalance in the brain) can cause mental illness.
Psychological Processes:
Influence the emergence and maintenance of disorders.
Includes wants, needs, emotions, attachment history, and cognitive processes.
Sociocultural Context:
Influences what is considered normal or abnormal.
Includes gender, age, cultural values, and traditions.
Integration: The biopsychosocial model integrates these factors to explain psychological disorders.
Diathesis-Stress Model
Builds on the biopsychosocial model.
Biological, psychological, and sociocultural factors predispose individuals to a disorder.
Stress is needed to trigger the disorder.
The strength of diathesis creates vulnerability; individuals with strong diathesis may succumb to mild stress, while those with weaker diathesis may need extreme stress.
Virtually anyone could develop a psychological disorder if the environmental stress is high enough.
Classifying Psychological Disorders
Taxonomy of Disorders
Grouping disorders with similar characteristics.
Classifying disorders helps:
Determine the nature of a problem.
Choose appropriate treatment methods.
Study the causes of mental disorders.
Provide an economy of language.
Classification Systems:
Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
International Classification of Diseases (ICD-11).
International Classification of Impairments, Disabilities, and Handicaps.
Reliability and Validity
Reliability: High for some disorders (e.g., anxiety disorders) but low for others (e.g., personality disorders).
Validity: Stronger for some diagnoses like schizophrenia.
Problems with Diagnostic Systems
Overlap of symptoms in different disorders.
Comorbidity (co-occurrence of disorders) is common.
Potential for bias in diagnosis due to clinician subjectivity.
Insufficient attention to sociocultural variables.
Labeling can be dehumanizing and stigmatizing.
Groups of Disorders
Anxiety Disorders
Phobias:
Specific phobias (e.g., clowns, dogs).
Social phobia (fear of social interaction).
Agoraphobia: fear of fear or panic in situations where escape might be difficult. Fear of not being able to cope if overwhelmed.
Generalized Anxiety Disorder (GAD):
Excessive, long-lasting, unfocused anxiety; free-floating anxiety.
Characterized by worry about various things and worry about worry (Type 1 and Type 2 worries).
Panic Disorder:
Recurrent panic attacks without warning or obvious cues.
Intense surge of anxiety with physical and cognitive symptoms.
Individuals try to avoid situations that trigger panic or panic symptoms.
Obsessive-Compulsive Disorder (OCD)
In DSM-5, OCD is in its own section, separate from anxiety disorders.
Characterized by obsessions and compulsions (not necessarily both).
Compulsions are rituals (e.g., hand washing).
Obsessions are cognitive intrusions (e.g., thoughts about becoming infected).
OCD involves doing and undoing; obsessions involve the doing, and compulsions attempt to undo the obsessions.
Causes of Anxiety Disorders
Genetic influences (twin and family studies).
Neurotransmitter abnormalities in the brain.
Cognitive processes and interpretation of the world.
Learning: Traumatic childhood experiences can increase the risk of developing anxiety disorders.
If you grow up in an environment that is dangerous, that builds up an expectation that the world is going to be dangerous and unpredictable.
Somatic Symptom and Related Disorders
Conversion Disorder: Apparent blindness, deafness, paralysis, or insensitivity to pain.
Hypochondriasis: Anxiety disorder related to health concerns; believing you're sick all the time or developing an incurable disease.
Body Dysmorphic Disorder: Intense distress about an imagined abnormality.
Somatization Disorder: Dramatic but vague reports of a multitude of physical problems.
Somatoform Pain Disorder: Severe, often constant pain with no identifiable physical cause.
Glove anesthesia: Numbness in the hand that stops immediately at the wrist (neurologically impossible, suggesting a psychological cause).
Causes of Somatoform Disorders
Childhood experiences, severe stresses, or cognitive factors.
Childhood example: If a child only receives attention when sick, they may develop a psychological impetus to become sick.
Diathesis-stress approach.
Sociocultural factors can affect manifestation.
Dissociative Disorders
Dissociative Identity Disorder (DID): Formerly known as multiple personality disorder as seen in movies like Split.
Fugue Reaction: Sudden wandering and loss of memory or confusion about personal identity; may adopt an entirely new identity.
Dissociative Amnesia: Sudden loss of memory about personal information.
Causes of Dissociative Disorders
Psychodynamic View: Massive repression of unwanted impulses or memories, creating a new identity to act out these impulses or recall memories.
Social Cognitive View: Everyone behaves differently depending on circumstances; dissociation is a normal function that goes too far in some individuals.
Example: Driving a car and going into a memory, then not remembering a bit of the drive is a form of dissociation.
Affective Disorders
Major Depression:
Symptoms include feeling sad or blue and overwhelmed for most of the time, losing interest in activities and relationships (anhedonia), changes in eating habits (weight loss or gain), sleep disturbance, exaggerated feelings of inadequacy, worthlessness, hopelessness, or guilt.
Extreme cases can include delusions or hallucinations (depression with psychotic features).
Can come on suddenly or gradually, with repeated depressive periods.
Can include suicidal ideation, plans to commit suicide, or completed suicides.
Rates of suicide differ depending on sociocultural factors.
Most suicides are preceded by warnings; people who express suicidal ideation are more likely to attempt suicide.
Encourage individuals expressing suicidal thoughts to contact a mental health professional or crisis hotline.
Bipolar Disorders
Bipolar I Disorder: Mania alternates with deep depression.
Bipolar II Disorder: Hypomania alternates with deep depression.
Cyclothymic Disorder: Less severe version of bipolar disorder.
Causes of Mood Disorders
Biological influences: genetics, malfunctions in brain regions involved in mood, neurotransmitter system imbalances, malfunctioning of the endocrine system, and disruption of biological rhythms.
Inflammation has been seen to have relationship with mood disorders.
Psychological and social factors: environmental stresses, how one thinks about those stresses, and general thinking style can affect depression.
Biases that contribute to negative or catastrophic thinking can lead to mood disruption.
Schizophrenia
Symptoms
Disorganized language (inferred disorganized thoughts).
Disturbed content of thinking, including delusions of influence or persecutions.
Perceptual abnormalities or disorders, such as hallucinations.
Emotional disturbances, such as lack of motivation.
Poor social skills and inability to function on a daily basis.
Causes
Diathesis-stress approach: vulnerability to schizophrenia is mainly biological, but impacted by the individual's environment.
Interaction between vulnerability to the disorder and the number of challenging events.
Psychological Disorders in Childhood
Conduct disorders and neurodevelopmental disorder of ADHD (externalizing or under-control disorders).
Internalizing or over-control disorders, such as separation anxiety disorder.
Pervasive developmental disorders, such as autism spectrum disorder.
Treatment
Overview of classification and thinking about disorders in psychology.
Basic Features of Treatment
Distinction between client and patient (client pays, patient suffers).
Therapist is accepted as able to help.
Special client-therapist relationship.
Therapist uses theory about the causes of the client's problems.
Treatment options: inpatient and outpatient.
Types of Therapy
Psychoanalysis/Psychodynamic Psychotherapy
Assumes that personality and behavior reflect the ego's attempts to resolve conflicts.
Aims at understanding unconscious conflicts.
Freud's structural model: ego, superego, and id.
Understanding and resolving conflicts between the superego and the id.
Unresolved unconscious conflicts can result in anxiety.
Influenced almost all forms of psychotherapy.
Strategies to achieve insight: free associations, exploring manifest and latent content of dreams, analysis of Freudian slips, and analysis of transference.
Humanistic Therapy
Conceptualizes treatment as a human encounter between equals.
It is not necessarily a cure given by an expert.
Clients will improve on their own with ideal conditions established through acceptance and support.
Clients are responsible for choosing how they will think and behave. Client-Centered Therapy (Carl Rogers): *What are the important elements?
Unconditional positive regard or acceptance.
Empathy and active listening or reflection.
Congruence or genuineness.
Cognitive Behavioral Therapy
Behavior therapy based on classical and operant conditioning.
Behavior therapy is based on classical conditioning (stimulus paired stimulus and response.
Behavior modification principles are based on operant conditioning (reinforces and punishes).
Cognitive behavioral therapy focuses on changing both thoughts and behaviors.
Biological Treatments for Psychological Disorders
Psychosurgery: Historically used (e.g., prefrontal lobotomy), but no longer used for psychological treatment.
Electroconvulsive Therapy (ECT): Still used to treat treatment-resistant, severe presentations.
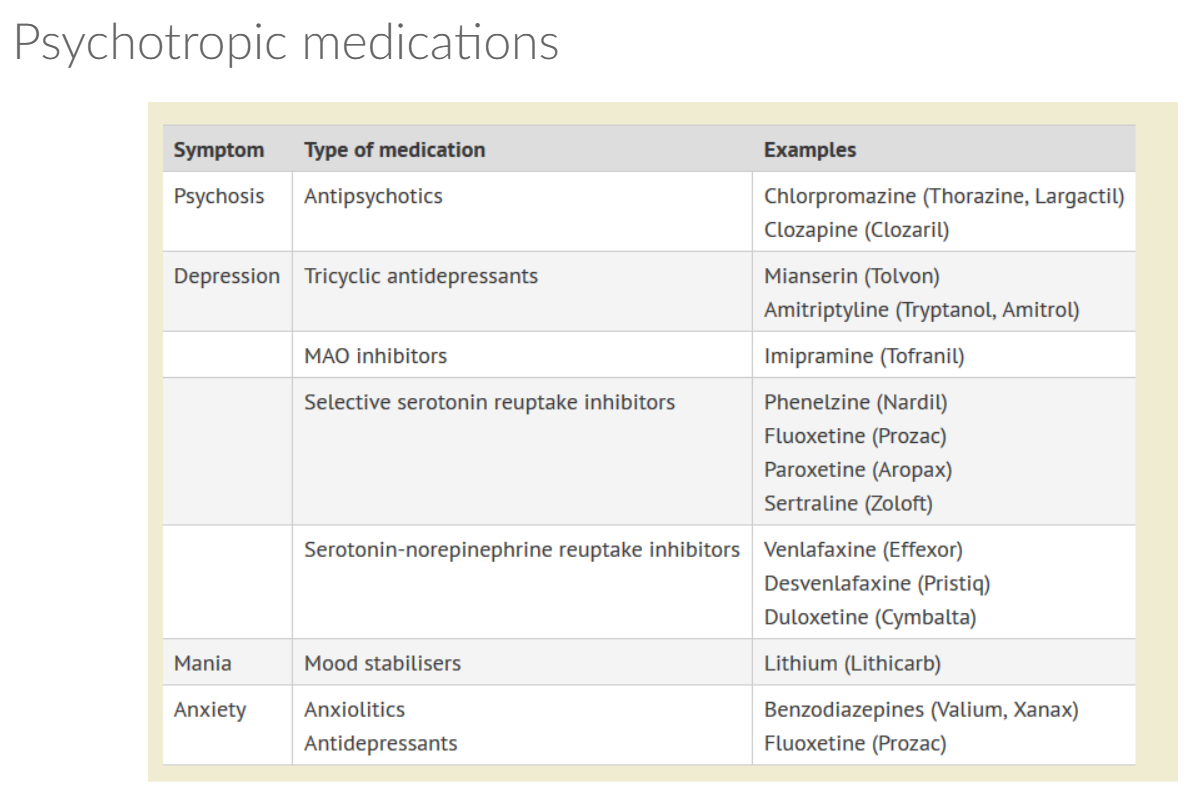
Psychoactive Drugs:
Neuroleptic drugs (antipsychotic drugs).
Antidepressant drugs (e.g., SSRIs).
Lithium and anticonvulsants for treating bipolar disorder.
Tranquilizing drugs (anxiolytics) for treating anxiety.
Advantages of Psychotherapy vs. Biological Approaches
Psychotherapy is as effective as drugs for severe depression, phobias, panic disorder, generalized anxiety, and OCD.
Lower dropout rates in psychotherapy than in drug therapies.
Benefits of psychotherapy may last longer than those from drugs.
Combining Psychotherapy and Drugs
Useful in cases such as bipolar disorder, where maintaining treatment adherence is important.
Slightly better results than either method alone for severe long-term depression.
More effective than either method alone in treating ADHD, OCD, alcoholism, stimmering, and panic disorder.
Useful for clients initially too distressed to benefit from psychotherapy.
Community Psychology
Community mental health movement to move away from hospitalizing patients.
Provide psychotic drugs and other mental health services like psychotherapy through community mental health centers.
Recognizing early signs of psychological or mental health disorders.
Preventing depression and suicide.
Identifying younger individuals at greater risk.
Identifying children at risk due to family or environmental problems.
Preventing and reducing child abuse and domestic violence.
Promoting health consciousness in minority communities.
Conclusion
Hope that studies are progressing well and wishing good luck with the upcoming exam.
Reference to Elizabeth Cochrane's expose, Ten Days in a Madhouse, and David Rosenhan's experiment, On Being Sane in Insane Places, highlighting historical perspectives on mental health treatment.
The way people were being diagnosed with psychiatric issues often revealed less about the patients themselves and more about their situation.
Naturally, people criticized his methods and his findings, but his experiment raised a lot of important questions, like how do we define, diagnose, and classify mental disorders?
At what point does sad become depressed, or quirky become obsessive and compulsive, or energetic become hyperactive?
What are the risks and benefits of diagnostic labeling, and how does the field keep evolving?
Psychological Disorders: Deviant, Distressful, and Dysfunctional Patterns
Defining Psychological Disorder:
Mental health clinicians think of psychological disorders as deviant, distressful, and dysfunctional patterns of thoughts, feelings, or behaviors.
Deviant: Thoughts and behavior that are different from most of the rest of your cultural context.
Distress: A subjective feeling that something is really wrong.
Dysfunction: A person's ability to work and live is clearly, often measurably impaired.
Medical and Biopsychological Perspectives on Mental Illness
Medical Model of Psychological Disorder:
Champions the notion that psychological disorders have physiological causes that can be diagnosed on the basis of symptoms and treated and sometimes even cured.
Biopsychological Approach:
*Everything psychological is simultaneously biological.
*A holistic perspective accounting for physiological and non-physiological factors in order to understand what's happening to us, what might be going wrong, and how it can be treated.
Taking into account psychological influences like stress and trauma and memories,
biological factors like genetics and brain chemistry and social cultural influences, like all the expectations wrapped up in how a culture defines normal behavior.
Diagnostic and Statistical Manual of Mental Disorders (DSM-5)
Used by clinicians, insurance and drug companies, policymakers, and the whole legal system.
Designed to be a work in progress, forever.Each new edition incorporates changes based on the latest research.
Changing attitudes and a developing understanding of sexual orientation led to homosexuality being eliminated as pathology
The growing understanding of the symptoms of post-traumatic stress disorder, changed the name of childhood bipolar disorder to disruptive mood dysregulation disorder because kids were being overdiagnosed and overtreated for bipolar disorder when the condition that they had didn't actually fit that description.New diagnoses are being explored as well, like gambling addiction and what's called Internet gaming disorder, showing that new disorders continue to arise with changing times.
Even though we've come a long way since the Rosenhan experiment, critics still worry about how the DSM might inadvertently promote the over or misdiagnosisBy slapping patients with labels, we're making them vulnerable to judgments and preconceptions that'll affect how others perceive and treat them.
Definitions are powerful, and things can get tricky pretty fast in the world of mental health.
Psychotherapy
Psychotherapy, perhaps the predominant type of psychological treatment, involves a therapist using a range of techniques to help a patient overcome troubles, gain insight, and achieve personal growth.
Psychodynamic Therapy and Freud’s Famous Psychoanalysis.
Freud assumed that we didn't really know, or at least fully understand ourselves or our motivation.
So psychoanalysis served as a kind of historical reconstruction that helped patients access repressed feelings and memories and unconscious thoughts by using free association and dream analysis with helpful interpretations from the therapist until they gained some self insight.
As you free associate, talk about your past, and answer questions, your psychoanalyst picks up on sensitive subjects around which you appear to show resistance, mental blocks that keep you from your consciousness because they cause you anxiety. The psychoanalyst notes these resistances and offers interpretations of what might be going on to help promote insight.
Traditionally Psychoanalysis isn't easy to prove or dis prove
Existential Humanist Therapy and Roger’s Client Centered Focus
Focuses more on conscious material and believe the present and future are worth more attention than the past.
encouraged therapists to help their clients by providing an empathetic, genuine, and accepting environment, and using active listening where the therapist echoes and clarifies what their clients are saying and feeling with a safe, nonjudgmental place where clients could accept themselves, feel valued, and work towards self actualization.
Bringing in more somber topics like Perls, Frankel, and others, incorporated the existentialist perspective. Understanding anxiety and limits to personal growth is driven by the human impulse to deny the fact that, let's face it, we're all gonna die.
Behavioral Therapies: Pavlov, Thorndyke, Skinner
A behavior therapist suggest that the problem behavior is the actual issue, and the best way to get rid of unwanted automatic behavior is to replace it with more functional behavior through new learning and conditioning.Behavior therapy aims to change behavior in order to change emotions and moods.
If Bernice is seeing a behavior therapist because of an intense fear of flying. We know her fear is keeping her from personal and career goals,
*Counter conditioning: evoke new responses to stimuli that trigger this unwanted behavior.
She may use other behavior therapy methods like exposure, systematic desensitization, and aversive conditioning to help Bernice modify her reactions and behavior.
Aversive conditioning is less common and usually involves pairing an unpleasant stimulus with the targeted behavior.
far more common and better studied, the exposure therapies treat an anxiety by having a person face their fears by exposing them to real or imagined situations that they typically avoid.
systematic desensitization is a type of exposure therapy that associates a relaxed state of mind with gradually increasing anxiety inducing stimuli.
Behavior therapy works pretty well in treating specific fears and problems like phobias, and it can also work for people with generalized anxiety disorder or major depression, but it often needs a boost.
Cognitive Therapy:Aaron Beck
If you can change a self defeating thought, you can change the related behavior.
help clients reverse destructive and catastrophic beliefs about themselves, the world, or the future at large, such as everything that could possibly go wrong will go wrong. cognitive therapist helps patients understand that changing what we say to ourselves is a very effective way to cope with our anxieties and modify our behavior.
Not surprisingly, the cognitive and behavior schools have joined forces frequently enough that cognitive behavior therapies are typically considered a single school.
And a lot of therapists use integrative approaches that try to use the best elements of all of these schools of thought.
Group Therapy - Benefits
Fosters therapeutic benefits by interacting with other people; it helps with social aspects of mental health and reminds clients that they're not alone.
Family Therapy:
*Treats a family as a system and views an individual's problem behaviors as being influenced by or directed at other family members. Works with multiple family members to heal relationships, improve insight and communication, and mobilize communal resources.
Research
Client Perceptions are just what they sound like. You see a therapist and someone asks you how you feel after your treatment; it varies by treatment, but client perception tends to be pretty rosy.
One study found that eighty nine percent of folks said they were at least fairly well satisfied with their treatment.
But of course perceptions are inherently subjective, and some believe that the therapeutic relationship lends itself to a positive bias in client reviews.
Basically, if you're sticking to your treatment, you probably like your therapist. Clinician perspectives can be similarly skewed,not only in terms of a self-serving bias, but also because they may not be around to see a client's future relapses or setbacks in mental health.
But we have treatment outcome research, a way of systematically measuring which therapies work best for which problems, and the gold standard of treatment outcome research is the randomized clinical trial, or RCT.
Research Terms
*Effectiveness is whether or not a given therapy works in a real-world setting,
*Efficacy is whether a therapy works better than some other comparable intervention or a control.
Two important terms you should know here are effectiveness and efficacy, Both terms matter, and you'll want to get them straight if you're trying to parse the research literature.
Two important terms you should know here are effectiveness and efficacy.
Dozen of studies have confirmed that psychotherapy is both effective and efficacious,
Important Common Factors That Unite These Therapies Instilling Hope, New Perspective with Empathy From Genuine Relationship.
Biomedical Therapies to Heal the Brain
*Aim to physiologically change the brain's electrochemical state with psychotropic drugs, magnetic impulses, or even electrical currents in surgery.
*pharmacotherapy is by far the most widely used.
*Psychotropic drugs are just any pharmaceutical that affects your mental state, and the most commonly used ones fall into four major categories: antipsychotics, anxiolytics, antidepressants, and mood stabilizer, each aimed at a specific family of problems.
Antipsychotics are used to treat schizophrenia and other types of severe thought disorders,
Most of these medications alter the effects of the neurotransmitter dopamine in the brain by blocking its receptor sites and blocking its uptake.
Anxiolytics or antianxiety meds usually work by depressing activity in the central nervous system, much like a stiff drink might.
The antidepressant are used to treat depression, as you might expect, but also a number of anxiety disorders.
Each type is thought to work a bit differently, mainly by altering the availability of various neurotransmitters like serotonin and norepinephrine in the brain, which in turn appears to help with mood and anxiety.Some of the most common are selective serotonin reuptake inhibitors, or SSRIs, like Zoloft, Paxil, and Prozac, which partially block the normal reuptake of serotonin.
Additional Treatments
Electroshock therapy
*Electrolyteconvulsive (ECT), involves sending a brief electrical current through the brain of an anesthetized patient.This excites the neurons, causing them to fire rapidly until the patient goes through a small, controlled seizure that lasts about two minutes.
*Repetitive Transcranial Magnetic Stimulation (RTMS) which involves the painless application of repeated electromagnetic pulses.
*Deep Brain Stimulation (DBS):is more invasive and calls for surgically implanting a kind of brain pacemaker that sends out electrical impulses to specific parts of the brain.
Lifestyle Affects
Thirty to sixty minutes of daily aerobic exercise has been shown to be effective as antidepressant medications in research on mild depression.
adequate sleep, social interaction, and good nutrition also all play a part in managing moods.
That different sores have different salves, and the same is true here. What works for one person may not work for another, and sometimes a few different kinds of intervention might be needed all at once.
Detailed Version
### Psychological Disorders and Treatment #### Introduction - Overview of psychopathology and taxonomy. - Exploration of psychological disorder models, diagnosis, and classification systems. - Discussion of psychological and biological treatment frameworks. - **Expanded**: Delve deeper into the historical context and evolution of understanding psychological disorders, including shifts in diagnostic criteria and societal attitudes. #### Learning Objectives - Outline and understand psychological disorders. - Identify key aspects of different psychological disorders. - Describe different approaches to the treatment of psychological disorders. - Outline the biological aspects of treatment. - Outline the role of prevention of psychological disorders. - **Expanded**: Introduce specific skills and competencies students will acquire, such as critical evaluation of research, application of diagnostic criteria, and ethical considerations in treatment. #### Quote on Therapeutic Situation - "The distortion of truth in the myth of the analytic situation is that analysis is an interaction between a sick person and a healthy one." - "The truth is that it is an interaction between two personalities in both of which the ego is under pressure from the id, the superego and the external world. Each personality has its internal and external dependencies, anxieties and pathological defenses. Each is also a child with his internal parents and each of these whole personalities that of the analysand and that of the analyst responds to every event in the analytic situation." - Highlights the importance of viewing individuals with disorders as people and recognizing the mutual process in treatment. - **Additional Context**: Discuss the power dynamics, transference, and countertransference phenomena that occur in therapeutic settings. #### Psychopathology Definition - Maladaptive, disruptive, or uncomfortable patterns of thinking, feeling, and behaving. - Affects individuals and their interactions with others (families, carers, and the community). - Worldwide, over 400 million people suffer from some form of psychological disorder. - Data from Australia (1993-2011) showed varying prevalence rates: - Severe: \~600,000 Australians - Moderate: \~1 million Australians - Mild: \~2 million Australians - **Elaboration**: Discuss the criteria used to define 'maladaptive,' 'disruptive,' and 'uncomfortable,' and consider cultural variations in these definitions. #### Abnormal Psychology - Abnormal definition: - Deviance from the average or normal. - Distress experienced by the individual. - Dysfunction in expected or desired functioning. - **Further Detail**: Expand on statistical, moral, and societal norms used to determine deviance, and examples of distress and dysfunction. #### Models of Psychopathology ##### Biopsychosocial Model - Interaction between biological, psychological, social, and environmental factors in the emergence and maintenance of disorders. - Biological Factors: - Medical model: disorders stem from an underlying illness. - Biological factors (e.g., chemical imbalance in the brain) can cause mental illness. - Psychological Processes: - Influence the emergence and maintenance of disorders. - Includes wants, needs, emotions, attachment history, and cognitive processes. - Sociocultural Context: - Influences what is considered normal or abnormal. - Includes gender, age, cultural values, and traditions.
**Integration:** The biopsychosocial model integrates these factors to explain psychological disorders. - **Expansion**: Provide specific examples of biological factors (genetic predispositions, neurotransmitter imbalances), psychological processes (cognitive distortions, emotional regulation), and sociocultural influences (socioeconomic status, cultural norms) that interact to influence mental health. ##### Diathesis-Stress Model - Builds on the biopsychosocial model. - Biological, psychological, and sociocultural factors predispose individuals to a disorder. - Stress is needed to trigger the disorder. - The strength of diathesis creates vulnerability; individuals with strong diathesis may succumb to mild stress, while those with weaker diathesis may need extreme stress. - Virtually anyone could develop a psychological disorder if the environmental stress is high enough. - **Example**: Illustrate with case studies of individuals with varying levels of diathesis and exposure to different types of stressors. #### Classifying Psychological Disorders ##### Taxonomy of Disorders - Grouping disorders with similar characteristics. - Classifying disorders helps: - Determine the nature of a problem. - Choose appropriate treatment methods. - Study the causes of mental disorders. - Provide an economy of language. - Classification Systems: - Diagnostic and Statistical Manual of Mental Disorders (DSM-5). - International Classification of Diseases (ICD-11). - International Classification of Impairments, Disabilities, and Handicaps. - **Historical Context**: Discuss the evolution of diagnostic criteria over time, including changes in the DSM and ICD, and the controversies surrounding these changes. ##### Reliability and Validity - Reliability: High for some disorders (e.g., anxiety disorders) but low for others (e.g., personality disorders). - Validity: Stronger for some diagnoses like schizophrenia. - **Expanded**: Explain different types of reliability (test-retest, inter-rater) and validity (content, construct, criterion) in the context of psychological diagnoses. ##### Problems with Diagnostic Systems - Overlap of symptoms in different disorders. - Comorbidity (co-occurrence of disorders) is common. - Potential for bias in diagnosis due to clinician subjectivity. - Insufficient attention to sociocultural variables. - Labeling can be dehumanizing and stigmatizing. - **Mitigation Strategies**: Address ways to minimize bias and stigma, such as cultural competence training for clinicians and promoting person-centered language. #### Groups of Disorders ##### Anxiety Disorders - Phobias: - Specific phobias (e.g., clowns, dogs). - Social phobia (fear of social interaction). - Agoraphobia: fear of fear or panic in situations where escape might be difficult. Fear of not being able to cope if overwhelmed. - Generalized Anxiety Disorder (GAD): - Excessive, long-lasting, unfocused anxiety; free-floating anxiety. - Characterized by worry about various things and worry about worry (Type 1 and Type 2 worries). - Panic Disorder: - Recurrent panic attacks without warning or obvious cues. - Intense surge of anxiety with physical and cognitive symptoms. - Individuals try to avoid situations that trigger panic or panic symptoms. - **Case Examples**: Provide detailed case studies illustrating the presentation, diagnosis, and treatment of each type of anxiety disorder. ##### Obsessive-Compulsive Disorder (OCD) - In DSM-5, OCD is in its own section, separate from anxiety disorders. - Characterized by obsessions and compulsions (not necessarily both). - Compulsions are rituals (e.g., hand washing). - Obsessions are cognitive intrusions (e.g., thoughts about becoming infected). - OCD involves doing and undoing; obsessions involve the doing, and compulsions attempt to undo the obsessions. - **Neurological Basis**: Describe the role of specific brain circuits (e.g., the cortico-striato-thalamo-cortical circuit) in the pathophysiology of OCD. ##### Causes of Anxiety Disorders - Genetic influences (twin and family studies). - Neurotransmitter abnormalities in the brain. - Cognitive processes and interpretation of the world. - Learning: Traumatic childhood experiences can increase the risk of developing anxiety disorders. - If you grow up in an environment that is dangerous, that builds up an expectation that the world is going to be dangerous and unpredictable. - **Epigenetic Factors**: Discuss how environmental factors can alter gene expression and contribute to the development of anxiety disorders. ##### Somatic Symptom and Related Disorders - Conversion Disorder: Apparent blindness, deafness, paralysis, or insensitivity to pain. - Hypochondriasis: Anxiety disorder related to health concerns; believing you're sick all the time or developing an incurable disease. - Body Dysmorphic Disorder: Intense distress about an imagined abnormality. - Somatization Disorder: Dramatic but vague reports of a multitude of physical problems. - Somatoform Pain Disorder: Severe, often constant pain with no identifiable physical cause. - Glove anesthesia: Numbness in the hand that stops immediately at the wrist (neurologically impossible, suggesting a psychological cause). - **Diagnostic Challenges**: Highlight the difficulties in differentiating these disorders from genuine medical conditions and the importance of a thorough medical evaluation. ##### Causes of Somatoform Disorders - Childhood experiences, severe stresses, or cognitive factors. - Childhood example: If a child only receives attention when sick, they may develop a psychological impetus to become sick. - Diathesis-stress approach. - Sociocultural factors can affect manifestation. - **Attachment Theory**: Explain how insecure attachment styles in childhood can predispose individuals to somatoform disorders in adulthood. ##### Dissociative Disorders - Dissociative Identity Disorder (DID): Formerly known as multiple personality disorder as seen in movies like Split. - Fugue Reaction: Sudden wandering and loss of memory or confusion about personal identity; may adopt an entirely new identity. - Dissociative Amnesia: Sudden loss of memory about personal information. - **Controversies**: Discuss the ongoing debates about the validity and etiology of DID, including the role of trauma and suggestibility. ##### Causes of Dissociative Disorders - Psychodynamic View: Massive repression of unwanted impulses or memories, creating a new identity to act out these impulses or recall memories. - Social Cognitive View: Everyone behaves differently depending on circumstances; dissociation is a normal function that goes too far in some individuals. - Example: Driving a car and going into a memory, then not remembering a bit of the drive is a form of dissociation. - **Neuroimaging Studies**: Describe findings from neuroimaging studies that have examined brain activity patterns in individuals with dissociative disorders. ##### Affective Disorders ###### Major Depression: - Symptoms include feeling sad or blue and overwhelmed for most of the time, losing interest in activities and relationships (anhedonia), changes in eating habits (weight loss or gain), sleep disturbance, exaggerated feelings of inadequacy, worthlessness, hopelessness, or guilt. - Extreme cases can include delusions or hallucinations (depression with psychotic features). - Can come on suddenly or gradually, with repeated depressive periods. - Can include suicidal ideation, plans to commit suicide, or completed suicides. - Rates of suicide differ depending on sociocultural factors. - Most suicides are preceded by warnings; people who express suicidal ideation are more likely to attempt suicide. - Encourage individuals expressing suicidal thoughts to contact a mental health professional or crisis hotline. - **Subtypes**: Differentiate between melancholic, atypical, and seasonal affective disorder (SAD). ###### Bipolar Disorders - Bipolar I Disorder: Mania alternates with deep depression. - Bipolar II Disorder: Hypomania alternates with deep depression. - Cyclothymic Disorder: Less severe version of bipolar disorder. - **Rapid Cycling**: Define rapid cycling and its implications for treatment. ###### Causes of Mood Disorders - Biological influences: genetics, malfunctions in brain regions involved in mood, neurotransmitter system imbalances, malfunctioning of the endocrine system, and disruption of biological rhythms. - Inflammation has been seen to have relationship with mood disorders. - Psychological and social factors: environmental stresses, how one thinks about those stresses, and general thinking style can affect depression. - Biases that contribute to negative or catastrophic thinking can lead to mood disruption. - **Neuroendocrine System**: Describe the role of the hypothalamic-pituitary-adrenal (HPA) axis in mood regulation. ##### Schizophrenia ###### Symptoms - Disorganized language (inferred disorganized thoughts). - Disturbed content of thinking, including delusions of influence or persecutions. - Perceptual abnormalities or disorders, such as hallucinations. - Emotional disturbances, such as lack of motivation. - Poor social skills and inability to function on a daily basis. - **Positive vs. Negative Symptoms**: Contrast positive (e.g., hallucinations, delusions) and negative (e.g., flat affect, avolition) symptoms of schizophrenia. ###### Causes - Diathesis-stress approach: vulnerability to schizophrenia is mainly biological, but impacted by the individual's environment. - Interaction between vulnerability to the disorder and the number of challenging events. - **Genetic Risk**: Quantify the genetic risk associated with schizophrenia based on family and twin studies. ##### Psychological Disorders in Childhood - Conduct disorders and neurodevelopmental disorder of ADHD (externalizing or under-control disorders). - Internalizing or over-control disorders, such as separation anxiety disorder. - Pervasive developmental disorders, such as autism spectrum disorder. - **Developmental Considerations**: Describe how the presentation of psychological disorders can vary across different developmental stages. #### Treatment - Overview of classification and thinking about disorders in psychology. - **Treatment Modalities**: Introduce the spectrum of therapeutic interventions, ranging from individual therapy to community-based programs. ##### Basic Features of Treatment - Distinction between client and patient (client pays, patient suffers). - Therapist is accepted as able to help. - Special client-therapist relationship. - Therapist uses theory about the causes of the client's problems. - Treatment options: inpatient and outpatient. - **Ethical Considerations**: Discuss ethical issues such as confidentiality, informed consent, and dual relationships. ##### Types of Therapy ###### Psychoanalysis/Psychodynamic Psychotherapy - Assumes that personality and behavior reflect the ego's attempts to resolve conflicts. - Aims at understanding unconscious conflicts. - Freud's structural model: ego, superego, and id. - Understanding and resolving conflicts between the superego and the id. - Unresolved unconscious conflicts can result in anxiety. - Influenced almost all forms of psychotherapy. - Strategies to achieve insight: free associations, exploring manifest and latent content of dreams, analysis of Freudian slips, and analysis of transference. - **Defense Mechanisms**: Elaborate on various defense mechanisms (e.g., repression, denial, projection) and their role in psychopathology. ###### Humanistic Therapy - Conceptualizes treatment as a human encounter between equals. - It is not necessarily a cure given by an expert. - Clients will improve on their own with ideal conditions established through acceptance and support. - Clients are responsible for choosing how they will think and behave. Client-Centered Therapy (Carl Rogers): \*What are the important elements? - Unconditional positive regard or acceptance. - Empathy and active listening or reflection. - Congruence or genuineness. - **Self-Actualization**: Define self-actualization and its significance in humanistic psychology. ###### Cognitive Behavioral Therapy - Behavior therapy based on classical and operant conditioning. - Behavior therapy is based on classical conditioning (stimulus paired stimulus and response. - Behavior modification principles are based on operant conditioning (reinforces and punishes). - Cognitive behavioral therapy focuses on changing both thoughts and behaviors. - **Cognitive Restructuring**: Describe techniques for identifying and modifying maladaptive thought patterns. ##### Biological Treatments for Psychological Disorders - Psychosurgery: Historically used (e.g., prefrontal lobotomy), but no longer used for psychological treatment. - Electroconvulsive Therapy (ECT): Still used to treat treatment-resistant, severe presentations. - Psychoactive Drugs: - Neuroleptic drugs (antipsychotic drugs). - Antidepressant drugs (e.g., SSRIs). - Lithium and anticonvulsants for treating bipolar disorder. - Tranquilizing drugs (anxiolytics) for treating anxiety. - **Mechanism of Action**: Explain how different classes of psychoactive drugs affect neurotransmitter systems in the brain. ##### Advantages of Psychotherapy vs. Biological Approaches - Psychotherapy is as effective as drugs for severe depression, phobias, panic disorder, generalized anxiety, and OCD. - Lower dropout rates in psychotherapy than in drug therapies. - Benefits of psychotherapy may last longer than those from drugs. - **Long-Term Outcomes**: Discuss the importance of long-term follow-up studies to assess the durability of treatment effects. ##### Combining Psychotherapy and Drugs - Useful in cases such as bipolar disorder, where maintaining treatment adherence is important. - Slightly better results than either method alone for severe long-term depression. - More effective than either method alone in treating ADHD, OCD, alcoholism, stimmering, and panic disorder. - Useful for clients initially too distressed to benefit from psychotherapy. ##### Community Psychology - Community mental health movement to move away from hospitalizing patients. - Provide psychotic drugs and other mental health services like psychotherapy through community mental health centers. - Recognizing early signs of psychological or mental health disorders. - Preventing depression and suicide. - Identifying younger individuals at greater risk. - Identifying children at risk due to family or environmental problems. - Preventing and reducing child abuse and domestic violence. - Promoting health consciousness in minority communities. - **Social Justice**: Discuss the role of community psychology in addressing social inequalities that contribute to mental health disparities. #### Conclusion - Hope that studies are progressing well and wishing good luck with the upcoming exam. - Reference to Elizabeth Cochrane's expose, Ten Days in a Madhouse, and David Rosenhan's experiment, On Being Sane in Insane Places, highlighting historical perspectives on mental health treatment. - The way people were being diagnosed with psychiatric issues often revealed less about the patients themselves and more about their situation.
Naturally, people criticized his methods and his findings, but his experiment raised a lot of important questions, like how do we define, diagnose, and classify mental disorders?
At what point does sad become depressed, or quirky become obsessive and compulsive, or energetic become hyperactive?
What are the risks and benefits of diagnostic labeling, and how does the field keep evolving? - **Future Directions**: Speculate on emerging trends in mental health research and practice, such as the use of technology, personalized medicine, and integrated care models. ##### Psychological Disorders: Deviant, Distressful, and Dysfunctional Patterns - Defining Psychological Disorder: - Mental health clinicians think of psychological disorders as deviant, distressful, and dysfunctional patterns of thoughts, feelings, or behaviors. - Deviant: Thoughts and behavior that are different from most of the rest of your cultural context. - Distress: A subjective feeling that something is really wrong. - Dysfunction: A person's ability to work and live is clearly, often measurably impaired. ##### Medical and Biopsychological Perspectives on Mental Illness - Medical Model of Psychological Disorder: - Champions the notion that psychological disorders have physiological causes that can be diagnosed on the basis of symptoms and treated and sometimes even cured.
Biopsychological Approach:
\*Everything psychological is simultaneously biological.
\*A holistic perspective accounting for physiological and non-physiological factors in order to understand what's happening to us, what might be going wrong, and how it can be treated.
Taking into account psychological influences like stress and trauma and memories,
biological factors like genetics and brain chemistry and social cultural influences, like all the expectations wrapped up in how a culture defines normal behavior. ##### Diagnostic and Statistical Manual of Mental Disorders (DSM-5) - Used by clinicians, insurance and drug companies, policymakers, and the whole legal system. - Designed to be a work in progress, forever.Each new edition incorporates changes based on the latest research.
Changing attitudes and a developing understanding of sexual orientation led to homosexuality being eliminated as pathology
The growing understanding of the symptoms of post-traumatic stress disorder, changed the name of childhood bipolar disorder to disruptive mood dysregulation disorder because kids were being overdiagnosed and overtreated for bipolar disorder when the condition that they had didn't actually fit that description. - New diagnoses are being explored as well, like gambling addiction and what's called Internet gaming disorder, showing that new disorders continue to arise with changing times.
Even though we've come a long way since the Rosenhan experiment, critics still worry about how the DSM might inadvertently promote the over or misdiagnosis - By slapping patients with labels, we're making them vulnerable to judgments and preconceptions that'll affect how others perceive and treat them.
Definitions are powerful, and things can get tricky pretty fast in the world of mental health. ##### Psychotherapy Psychotherapy, perhaps the predominant type of psychological treatment, involves a therapist using a range of techniques to help a patient overcome troubles, gain insight, and achieve personal growth. ###### Psychodynamic Therapy and Freud’s Famous Psychoanalysis. Freud assumed that we didn't really know, or at least fully understand ourselves or our motivation.
So psychoanalysis served as a kind of historical reconstruction that helped patients access repressed feelings and memories and unconscious thoughts by using free association and dream analysis with helpful interpretations from the therapist until they gained some self insight.
As you free associate, talk about your past, and answer questions, your psychoanalyst picks up on sensitive subjects around which you appear to show resistance, mental blocks that keep you from your consciousness because they cause you anxiety. The psychoanalyst notes these resistances and offers interpretations of what might be going on to help promote insight.
Traditionally Psychoanalysis isn't easy to prove or dis prove ###### Existential Humanist Therapy and Roger’s Client Centered Focus \*Focuses more on conscious material and believe the present and future are worth more attention than the past.\* encouraged therapists to help their clients by providing an empathetic, genuine, and accepting environment, and using active listening where the therapist echoes and clarifies what their clients are saying and feeling with a safe, nonjudgmental place where clients could accept themselves, feel valued, and work towards self actualization.
Bringing in more somber topics like Perls, Frankel, and others, incorporated the existentialist perspective. Understanding anxiety and limits to personal growth is driven by the human impulse to deny the fact that, let's face it, we're all gonna die. ###### Behavioral Therapies: Pavlov, Thorndyke, Skinner A behavior therapist suggest that the problem behavior is the actual issue, and the best way to get rid of unwanted automatic behavior is to replace it with more functional behavior through new learning and conditioning.Behavior therapy aims to change behavior in order to change emotions and moods.
If Bernice is seeing a behavior therapist because of an intense fear of flying. We know her fear is keeping her from personal and career goals,
\*Counter conditioning: evoke new responses to stimuli that trigger this unwanted behavior.
She may use other behavior therapy methods like exposure, systematic desensitization, and aversive conditioning to help Bernice modify her reactions and behavior.
Aversive conditioning is less common and usually involves pairing an unpleasant stimulus with the targeted behavior.
far more common and better studied, the exposure therapies treat an anxiety by having a person face their fears by exposing them to real or imagined situations that they typically avoid.
systematic desensitization is a type of exposure therapy that associates a relaxed state of mind with gradually increasing anxiety inducing stimuli.
Behavior therapy works pretty well in treating specific fears and problems like phobias, and it can also work for people with generalized anxiety disorder or major depression, but it often needs a boost. ###### Cognitive Therapy:Aaron Beck \*If you can change a self defeating thought, you can change the related behavior.\* help clients reverse destructive and catastrophic beliefs about themselves, the world, or the future at large, such as everything that could possibly go wrong will go wrong. cognitive therapist helps patients understand that changing what we say to ourselves is a very effective way to cope with our anxieties and modify our behavior.
Not surprisingly, the cognitive and behavior schools have joined forces frequently enough that cognitive behavior therapies are typically considered a single school.
And a lot of therapists use integrative approaches that try to use the best elements of all of these schools of thought. ###### Group Therapy - Benefits - Fosters therapeutic benefits by interacting with other people; it helps with social aspects of mental health and reminds clients that they're not alone.
Family Therapy:
\*Treats a family as a system and views an individual's problem behaviors as being influenced by or directed at other family members. Works with multiple family members to heal relationships, improve insight and communication, and mobilize communal resources. ##### Research Client Perceptions are just what they sound like. You see a therapist and someone asks you how you feel after your treatment; it varies by treatment, but client perception tends to be pretty rosy.
One study found that eighty nine percent of folks said they were at least fairly well satisfied with their treatment.
But of course perceptions are inherently subjective, and some believe that the therapeutic relationship lends itself to a positive bias in client reviews.
Basically, if you're sticking to your treatment, you probably like your therapist. Clinician perspectives can be similarly skewed,not only in terms of a self-serving bias, but also because they may not be around to see a client's future relapses or setbacks in mental health.
But we have treatment outcome research, a way of systematically measuring which therapies work best for which problems, and the gold standard of treatment outcome research is the randomized clinical trial, or RCT. ###### Research Terms \*Effectiveness is whether or not a given therapy works in a real-world setting,
\*Efficacy is whether a therapy works better than some other comparable intervention or a control.
Two important terms you should know here are effectiveness and efficacy, Both terms matter, and you'll want to get them straight if you're trying to parse the research literature.
Two important terms you should know here are effectiveness and efficacy.
Dozen of studies have confirmed that psychotherapy is both effective and efficacious,
**Important Common Factors That Unite These Therapies Instilling Hope, New Perspective with Empathy From Genuine Relationship**. ##### Biomedical Therapies to Heal the Brain \*Aim to physiologically change the brain's electrochemical state with psychotropic drugs, magnetic impulses, or even electrical currents in surgery.
\*pharmacotherapy is by far the most widely used.
\*Psychotropic drugs are just any pharmaceutical that affects your mental state, and the most commonly used ones fall into four major categories: antipsychotics, anxiolytics, antidepressants, and mood stabilizer, each aimed at a specific family of problems.
Antipsychotics are used to treat schizophrenia and other types of severe thought disorders,
Most of these medications alter the effects of the neurotransmitter dopamine in the brain by blocking its receptor sites and blocking its uptake.
Anxiolytics or antianxiety meds usually work by depressing activity in the central nervous system, much like a stiff drink might.
The antidepressant are used to treat depression, as you might expect, but also a number of anxiety disorders.
Each type is thought to work a bit differently, mainly by altering the availability of various neurotransmitters like serotonin and norepinephrine in the brain, which in turn appears to help with mood and anxiety.Some of the most common are selective serotonin reuptake inhibitors, or SSRIs, like Zoloft, Paxil, and Prozac, which partially block the normal reuptake of serotonin. #### Additional Treatments - Electroshock therapy
\*Electrolyteconvulsive (ECT), involves sending a brief electrical current through the brain of an anesthetized patient.This excites the neurons, causing them to fire rapidly until the patient goes through a small, controlled seizure that lasts about two minutes.
\*Repetitive Transcranial Magnetic Stimulation (RTMS) which involves the painless application of repeated electromagnetic pulses.
\*Deep Brain Stimulation (DBS):is more invasive and calls for surgically implanting a kind of brain pacemaker that sends out electrical impulses to specific parts of the brain. #### Lifestyle Affects Thirty to sixty minutes of daily aerobic exercise has been shown to be effective as antidepressant medications in research on mild depression.
adequate sleep, social interaction, and good nutrition also all play a part in managing moods.
That different sores have different salves, and the same is true here. What works for one person may not work for another, and sometimes a few different kinds of intervention might be needed all at once.
Images