Chapter 34: Neurotoxics
34.1: Neurotoxics
- Neurotoxics are the %%poisons acting on the nervous system%%.
Cerebral Neurotoxics
Somniferous Poisons
- These poisons %%produce analgesia and sleep and are often used therapeutically%%, e.g. opium and its derivatives, pethidine, etc.
Inebriant Poisons
- Classical inebriants — Alcohols (ethyl alcohol, methyl alcohol, ethylene glycol, etc.) •
- Anesthetics — Chloroform, ether, etc.
- Sedatives and hypnotic poisons — Chloral hydrate, barbiturates, etc.
- Benzodiazepines — diazepam, flurazepam, etc.
- Hydrocarbons — Aliphatic (e.g. diesel oil, petrol, kerosene, etc.), aromatic (e.g. benzene) and halogenated (e.g. carbon tetrachloride)
- Insecticides — Organophosphorous compounds, Carbamates and Organochloro compounds
Deliriant Poisons
- These are poisons which produce %%well-marked deliriant or confusional stage%%, e.g. Datura, Belladonna, Hyoscyamus, Cannabis, Cocaine, etc.
Spinal Neurotoxics
- These are poisons, which a%%ct primarily on the spinal co%%rd, e.g. Nux-vomica, and its alkaloids, gelsemium.
Peripheral Neurotoxics
- These are poisons, which %%act especially on the end plates of the motor nerve terminals%%, e.g. hemlock, curare, conium, etc.
Opium Derivatives
- Opium is a grey mass with bitter taste, obtained on drying the milky latex of unripe seed capsule of poppy plant, Papaver somniferum.
- The opium is usually collected after all the flower petals have fallen off from the capsule, by making slits along its circumference, allowing the milky latex to ooze out and harden.
- After the plastic gummy opium is removed, it can be refined into heroin, morphine, and codeine.
Opium Plant
- Botanical Name: Papaver somniferum.
- Common Name: White poppy plant.
- It is an herb growing up to 1 meter in height. The leaves are oblong, irregularly toothed, and slightly lobed. Flowers are large and may be bluish-white, purple, or white in color. Each plant bears 5-10 capsules.
- Unripe fruit capsule, which yields the latex, juice on incision. The opium is collected after all the flower petals have fallen off. Slits are made along the circumference of the seed capsule allowing the milky latex to ooze out and harden.
Active Principles
- Capsule latex juice has opium alkaloids.
- An alkaloid is a complex substance with a nitrogenous base that behaves like alkali and unites with acid-forming salts.
- Phenanthrene Derivatives
- Morphine (10%): In its pure form is a white crystalline powder, having a bitter taste, freely soluble in alcohol and water.
- Morphine has a mode of action of the depressing cerebral cortex, most of the centers of the medulla, including the respiratory center, and stimulates the vagal nucleus and vomiting center.
- Codeine (0.5%): It is a white, crystalline powder, with a bitter taste, is chemically CH3 morphine, and is soluble in water. Its principal action is depression of the cough center.
- Thebaine (0.3%): It is a convulsant poison that can produce tetanic convulsions, resembling tetanus/strychnine.
- Semisynthetic and synthetic preparations of opium
- Heroin (Diacetyl morphine) or brown sugar: Previously used as a sedative, but for its narcotic and addiction-forming effect its production has been banned. It is considered as health hazard for younger generation, all over the world.
- Dionin (Ethyl morphine): It is being used as a cough sedative in intractable cough, as it depresses the cough center.
- Benzyl-isoquinoline Derivatives
- Papaverine (1%): It has no narcotic effect, but has a smooth muscle relaxant effect.
- Narcotine (Noscapine) (6%)
Pethidine
- Pethidine is an opioid, narcotic analgesic drug, which is a synthetic derivative of opium.
- It is colorless, crystalline powder with bitter taste.
- Action of pethidine resembles that of morphine and produces a degree of euphoria and therefore is not free from the risk of addiction.
- An overdose on account of cerebral excitation can produce flushing of face, dilated pupils, disturbances of vision, dry mouth, tachycardia, raised temperature, vomiting, excitement, tremors, convulsions, etc.
- These may be followed by drowsiness, coma, and death from respiratory depression.
- Fatal dose: 1 to 2 gm with monoamino oxidase (MAO) inhibitor or phenothiazine, even a much smaller dose can be fatal.
- Fatal period: 24 hours.
- Toxicity rating: 5
Pethidine Addiction
- It is quite severe, difficult to treat and has high mortality rate. Pethidine is often used for its analgesic, sedative and tranquilizing effects, establishing tolerance rapidly.
- Common victims of addiction are doctors, nurses or other paramedical professionals to whom the drug is easily available. Continued use can lead to addiction, characterized by
- Euphoria
- Dulling of intelligence
- Impairment of memory
- Withdrawal symptoms when drug is withheld or when more dose is required
- Larger doses can result in confusional state with hallucinations, illusions and personality changes rapidly than with morphine.
- Accidental poisoning with therapeutic doses is also reported
34.2: Alcohol
- Alcohol is an inebriant cerebral neurotoxic poison. Alcohol is also classified as sedative and hypnotic.
- It refers to an aqueous solution containing 95% ethyl alcohol.
- It is one of the oldest intoxicants ever known to man.
Alcohols are hydroxyl derivatives of aliphatic hydrocarbons.
- Monohydroxy alcohols — It has only one hydroxyl group and includes:
- Ethyl alcohol, methyl alcohol, isopropyl alcohol, isobutyl alcohol, & amyl alcohol.
- Dihydroxy alcohols — These have two hydroxyl groups and often called as glycols.
- Tryhydroxy alcohols — These are not really alcohols, but their derivatives, such as the propane derivative, glycerol or glycerine.
Ethyl Alcohol (Ethanol, Grain Alcohol)
- In a pure form ethyl alcohol is transparent, colorless, volatile liquid, having a spirituous odor and burning taste. It is both water-soluble and lipid soluble.
Production of Ethyl Alcohol
- Ethanol is obtained by fermentation of sugars, molasses, grains, fruit juices and starch. It is a complex enzymic process.
- The enzymes are obtained from yeast. It is carried out under controlled conditions.
- The final fermented mass contains about 10% alcohol. It is then purified by distillation.
- Absolute alcohol or alcohol dehydratum (contains 99.95% ethyl alcohol by volume).
- Rectified spirit (contains 90% ethyl alcohol by volume).
- Industrial methylated spirit or denatured alcohol (contains 95% ethyl alcohol and 5% wood naphtha by volume).
- Surgical spirit: It refers to methylated spirit which contains in addition small amounts of castor oil and oil of Wintergreen (methyl salicylate).
- Alcoholic beverages: The active ingredient of all beverages/ liquors is alcohol.
- They are mixtures of absolute ethyl alcohol, water and congeners formed during fermentation process as in most of the alcoholic beverages; exception being in wine and brandy wherein the congener is methyl alcohol.
- Proof spirit: It refers to a standard mixture alcohol and water of relative density.
- It means that strength of absolute alcohol which when poured onto gunpowder gets it burnt completely.
Absorption of Ethyl Alcohol
- Absorption of ethyl alcohol is mainly from the stomach (20%) and intestine (80%).
- It commences almost immediately after ingestion within 5 minutes and is completed within one to two and half an hour of ingestion.
Causes of Death
- Direct depressive effect of brainstem
- Direct depressive effect of respiratory center
- Aspiration of the vomit, choking (Café coronary), drowning, etc
- Severe bleeding from trivial trauma, esp. subdural/ epidural intracranial hemorrhages Irreversible complications of brain and liver damage
- Poisoning by various toxic substances present in cheap industrial/ illicit alcoholic.
Alcohol Poisoning
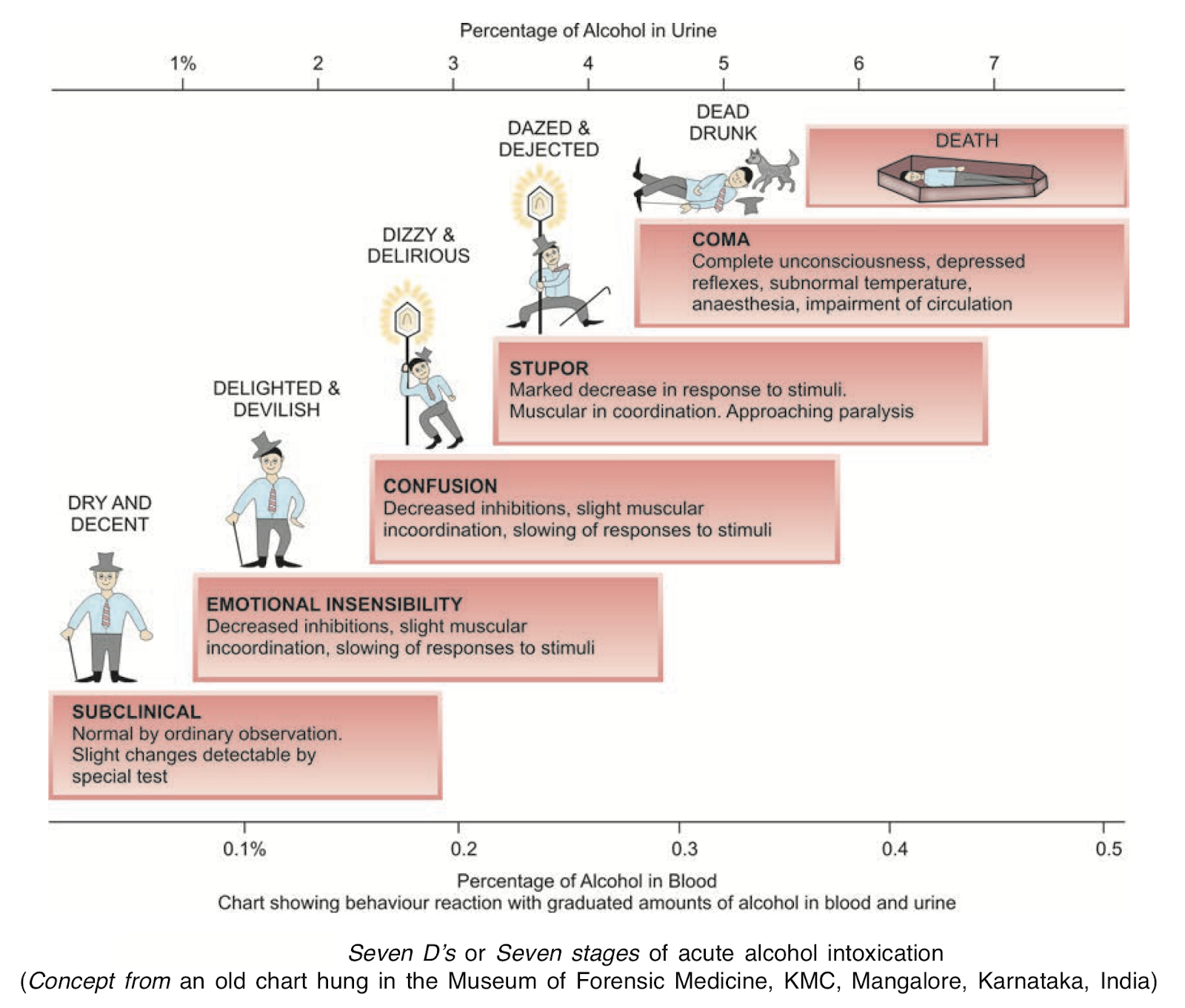
Acute Alcohol Poisoning
- Consumption of any preparation containing alcohol either in small doses at short intervals, or in one big dose beyond his/ her capacity with the blood alcohol concentration exceeding 150 mg/100 ml, constitutes acute alcohol poisoning.
- Fatal dose: (in a non-addict)
- Adult: 150-250 ml of absolute alcohol (Approximately 6 gm of ethanol/kg body weight).
- Children: 60 ml of absolute alcohol (Approximately 3 gm of ethanol/kg body weight).
- Fatal period: 12 to 24 hours though death may be delayed for 5 to 6 days.
- Toxicity rating: 2
Alcohol Hangover
- It comprises throbbing headache, irritability, lethargy, nausea, and abdominal discomfort.
- While the abdominal discomfort is due to alcoholic gastritis, the other symptoms are due to the effect of congeners and other impurities present in the alcoholic beverages consumed, which causes mild cerebral edema.
- The hangover manifestations may also be partly due to alcohol-induced hypoglycemia.
Death
- If the victim does not recover from a coma within 5 hours, the prognosis is worse and may result in a fatality, due to asphyxia or shock.
- It is appropriate to mention here that stage VII (Death) is extremely rare with ingestion of pure ethanol.
Chronic Alcohol Poisoning
Various types of chronic alcoholism
- Alpha: Before the abuser develops psychological dependence on alcohol.
- Beta: Long-continued alcoholism develops cirrhosis, but no psychological dependence.
- Gamma: Alcohol abuser goes on increasing, resulting in physical and social problems.
- Delta: Long continued abuse which can not be abstained, will lead to serious physical complications.
- Epsilon: The abuser develops a habit of dipsomania when he technically drinks to death.
- Reactive: The victim drinks alcohol and seeks relief from psychological stress and strain.
- Essential: It is he who has got a drink for inherent genetic or biological factors but not for any psychological or cultural one.
- Symptomatic: Who drinks for long-standing psychological illness, psychosis/severe depression.
Common Abstinence Syndrome
- The syndrome complex comprises manifestations such as tremors in the hands, legs, and trunk.
- He/she will present with a mental state of extreme emotional disturbance (agitation), sweating, nausea, headache, and insomnia.
- All these events come into sight within 6 to 8 hours of stopping the alcohol intake.
- Treatment: Studies with clonidine 0.2 mg orally given several times daily over a 4-day period suggest that it is effective in plummeting some of the adrenergic manifestations of alcohol withdrawal.
Alcoholic Hallucinosis
- The person starts seeing objects with distorted shape and their shadows moving.
- He/she will complain of hearing some one shouting at him or snatches of music, etc.
- All these events come into sight within 24 to 36 hours of stopping the alcohol intake.
- Treatment: Administration of phenothiazine (Chlorpromazine 100 mg, 8th hourly).
Alcohol Seizures (Rum Fits)
- These comprise of clonic-tonic movements, with or without loss of consciousness.
- These manifestations appear within 6 to 48 hours of either cessation or precipitous decline of alcohol intake. True alcohol seizures will usually manifest prior to the onset of delirium tremens (TD).
- These seizures do not require any longterm anticonvulsant therapy since the seizures are self limited.
- Risk Factors:
- Usually this is reported among 40% of adults with seizures admitted to a hospital and in about 15% of patients with status epilepticus.
- This necessitates routine questioning about alcohol intake in all patients arriving with seizures to an emergency department of a hospital.
- Some of the risk factors associated with alcohol withdrawal and considered most likely to precipitate seizures are hypoglycemia, hypomagnesemia, and respiratory alkalosis.
- Alcoholic withdrawal also heightens the photic sensitivity and can lead to television-induced seizures.
Alcohol Ketoacidosis
- This is found to develop with sudden withdrawal of or heavy drinking of alcohol.
- Gastritis or pancreatitis, which has lead to sudden reduction in alcohol intake, might be the other cause.
- Features: Include drowsiness, confusion, tachycardia, and tachypnea, and may progress to Kussmaul’s breathing and coma.
Delirium Tremens
- Delirium tremens is medicolegally important toxicological problem as it has an element of unsoundness of mind due to acute insanity associated with chronic alcoholism, is the most dangerous complication of alcoholism.
- It is a dramatic onset of disordered mental activity due to long continued action of alcohol in chronic alcoholics when its consumption is suddenly stopped18 for 3 to 5 days.
- Certain other factors that might precipitate delirium tremens are:
- Temporary excess consumption or sudden withdrawal of alcohol in an alcohol addict.
- Shock on severe trauma such as fractured bone or undergoing surgery in a chronic alcoholic.
- Acute infection in chronic alcoholic.
Wernicke-Korsakoff Syndrome
- This is a rare form of withdrawal syndrome, which is a combination of Wernicke’s encephalopathy and Korsakoff’s psychosis.
- Wernicke’s encephalopathy is an acute form, characterized by drowsiness, amnesia, ataxia, peripheral neuropathy, horizontal nystagmus, and external ocular palsies.
- When the recovery from this is incomplete, a chronic amnesic syndrome develops called Korsakoff’s psychosis, which is characterized by impairment of memory and confabulations (falsification of memory).
Alcohol and Heart
- Cardiac Dysfunction:
- A supraventricular arrhythmia can be induced by drinking binges. Also known as ‘Holiday Heart Syndrome’ is developed with more than 6 drinks a day.
- Atrial fibrillation is the most common arrhythmia, but atrial flutter, atrial tachycardia, junction tachycardia, and multiple atrial premature beats have also been noticed.
- Alcohol Cardiomyopathy:
- It shares certain features with beriberi, heart failure found in malnourished, vitamin-deficient alcoholics:
- Cardiac chamber dilatation, tachycardia, elevated venous pressure, and peripheral edema.
- Cardiac conduction:
- Cardiovascular death is the most important cause of mortality in alcoholics, yet alcohol may protect against ischemic heart disease.
- QT-interval prolongation in some patients with alcoholic liver disease is associated with an adverse prognosis, especially sudden death.
Treatment of Chronic Alcohol Poisoning
- Psychotherapy
- Group psychotherapy of supportive nature is considered to be more effective than individual psychotherapy.
- Alcohol Anonymous (AA) — a self-support organization, plays a vital role.
- This organization has a base at USA and started as early as in 1935, has more than 35,000 groups all over the world.
- There is no membership fees to join AA.
- The only requirement to get the membership is the ‘desire to stop drinking’
- Treatment of Withdrawal Syndrome
- Carbamazepine: It has been found useful in treating alcohol withdrawal, as well as delirium tremens. It does not require any adjunctive medication. It also offers advantage of rapid return to work or early induction into an alcoholism treatment program.
- Chloromethiazole: This is a drug of choice in Britain for alcohol withdrawal. It has hypnotic, anxiolytic, and anticonvulsant properties. It is given in a rapidly tapering dose schedule for 6-7 days. It is also known that alcoholics rapidly become dependent to this drug.
- Clonidine: Preliminary report suggests use of clonidine in a dose of 60-180 microgram/hour intravenously with gamma hydroxybutyric acid in a dose of 50 mg/kg orally is useful in withdrawal syndrome symptoms.
- Aversion Therapy
- Usually needs hospitalization for a period of several days, under close medical supervision. Effective tackling of insatiable craving for alcohol is to be achieved here by deterrent measures.
- Action of Disulfiram: Disulfiram is widely used all over the world as an alcohol deterrent. In spite of large number of individuals maintained on disulfiram and the common occurrence of disulfiram (Antabuse) reactions, reports of overdose are relatively uncommon.
- Therapeutic Dose
- Manufacturer’s recommendation—in USA:
- One to two weeks use of disulfiram orally 500 mg/day.
- Then 15 ml (1/2 Oz) of 100-proof whiskey taken orally slowly, not to exceed 30 ml (1 Oz).
- Patient should be hospitalized or have equivalent facilities available including oxygen.
- Manufacturer’s recommendation—Overseas:
- First day: 4 tablets (800 mg) of disulfiram
- Second day: 3 tablets (800 mg) of disulfiram
- Third day: 2 tablets (800 mg) of disulfiram
- Fourth day: 1 tablet (800 mg) of disulfiram
- Fifth day: Challenge dose, 15 to 30 mL pure ethanol.
- Manufacturer’s recommendation—in USA:
Methyl Alcohol
- It is colorless, clear, volatile liquid with a characteristic odor (felt to be similar to that of ethyl alcohol) and a bitter taste.
- Methyl alcohol is rapidly absorbed through the stomach and intestines, and also through the lungs and skin.
- Methanol is oxidized in the liver to formaldehyde, which is 33 times more toxic than methanol. Formaldehyde in turn is oxidized to formic acid, which is 6 times more toxic than methanol.
- Formic acid is responsible for associated metabolic acidosis and the retinal toxicity.
- Methanol is excreted unchanged from lungs to an extent of 80% while kidneys excrete another 3-5% in urine unchanged.
- Fatal dose: 60 to 200 ml.
- Fatal period: 24 to 36 hours. May be delayed for 2-4 days.
- Toxicity rating: 3.
Isopropanol (Isopropyl Alcohol, IPA)
- Isopropanol is an inebriant neurotoxic substance.
- IPA is a colorless, clear, volatile liquid with aromatic odor and a burning bitter taste, mainly now used as an industrial solvent. It can be an ingredient of antifreeze, liquid detergent, paint and varnish remover, racing motor fuel,
- Fatal Dose: About 250 ml.
Ethylene Glycol
- Ethylene glycol is an inebriant neurotoxic substance.
- It is colorless, nonvolatile liquid with a bittersweet taste.
- Toxic action is mainly due to the metabolites-glycolic acid, lactic acid and oxalic acid.
- Fatal dose: 100 to 200 ml.
- Fatal period: 24 hours or so.
Chloroform
- Chloroform is an inebriant cerebral poison.
- Chloroform is a heavy, colorless, volatile liquid with a strong odor and a burning sweet taste.
- It acts as an anesthetic and respiratory depressant.
- Fatal dose: 30 ml by mouth (>0.04% in blood).
- Fatal period: 30 minutes.
Ether
- Ether is an inebriant cerebral poison.
- Ether is a colorless, volatile, highly inflammable liquid with penetrating ethereal odor and sweetish pungent taste.
- Ether acts as an anesthetic and respiratory depressant.
- Fatal dose: 30 ml by mouth.
- Fatal period: May be immediate due to syncope during anesthesia—rarely.
- Treatment: Gastric lavage, demulcents, stimulants and anticonvulsants. Maintain blood pressure.
Chloral Hydrate
Chloral hydrate is a sedative (induces calming effect on CNS) and hypnotic (induces sleep).
- It is a crystalline substance
- Taste — peculiarly bitter sweet, but nauseating
- Odor — aromatic.
- Fatal dose: 5 to 10 gm. However, recoveries are reported even with large doses.
- Fatal period: 8 to 12 hours, but may be delayed for 2 to 3 days.
34.3: Barbiturates
- Barbiturates are basically derived from barbituric acid, the oldest being veronal barbitone.
- Using barbiturates in conjunction with alcohol is especially dangerous; alcohol is a central nervous system (CNS) depressant so the harmful effects of each are multiplied.
- Overdose deaths are more frequent when alcohol and barbiturates are mixed, whether accidentally or deliberately.
- Fatal period: 24-48 hrs.
- Toxicity Rating: Ranges 4 and 5.
Four Types of Barbituates
- Long-acting:
- Acts within 2 hours and duration of action lasts for 6 to 12 hours, e.g. barbitone, phenobarbital, mephobarbitone, methyl phenobarbital, diallylbarbiuric acid, etc.
- Fatal Dose: 3-4 mg.
- Intermediate-acting:
- Acts within 1/2 to 1 hour and the duration of action lasts for 3 to 6 hours, e.g. amylobarbitone, butobarbitone, probarbitone sodium, amobarbitone, aprobarbital, vinbarbital, allobarbitone, etc.
- Fatal Dose: 2-3 mg.
- Short-acting:
- Acts within minutes and the duration of action lasts <3 hours, e.g. cyclobarbitone, pentobarbitone, amobarbitone, aprobarbitone, butobarbitone, hexabarbitone, seconal, ortal, etc.
- Fatal Dose: 1-2 mg.
- Ultra-short acting:
- Acts immediately and the duration of action lasts for < 15-20 minutes.
- Fatal Dose: 8 to 10 mg per 100 ml.
Barbiturates Effects
- Central Nervous System Effects
- Barbiturates mainly act in the CNS and, as a consequence, affect other organ systems.
- Direct effects include sedation and hypnosis at lower dosages.
- The lipophilic barbiturates, such as thiopental, cause rapid anesthesia because of their tendency to penetrate brain tissue quickly.
- Barbiturates all have anticonvulsant activity because they hyperpolarize cell membranes; therefore, they are effective adjuncts in the treatment of epilepsy.
- Pulmonary Effects
- Barbiturates can cause a depression of the medullary respiratory center and induce respiratory depression.
- Patients with underlying chronic obstructive pulmonary disease (COPD) are more susceptible to these effects, even at doses that would be considered therapeutic in healthy individuals.
- Barbiturate overdose fatality is usually secondary to respiratory depression.
- Cardiovascular Effects
- Cardiovascular depression may occur following depression of the medullary vasomotor centers; patients with underlying congestive heart failure (CHF) are more susceptible to these effects.
- At higher doses, cardiac contractility and vascular tone are compromised, which may cause cardiovascular collapse.
- Mortality/Morbidity
- Mortality rates range from 1-10%.
- Fatality associated with barbiturate overdose is rare, but life-threatening complications are abundant.
- Morbidity by complications includes pneumonia, pulmonary edema, shock, hypoxia, acute renal failure and coma.
- Pregnancy
- Barbiturates freely cross the placenta and can have adverse effects on the fetus, such as a decrease in fetal intelligence, possible addiction, and possible withdrawal.
- Overactivity, visible tremors, hypertonicity, hyperphagia, and vasomotor instability characterize neonatal withdrawal syndrome, while withdrawal begins 4-7 days after birth and may last up to 4 months.
Management of Poisoned Patient
- Assess the airway and adequacy of respiration and perform ET intubation as necessary.
- Provide oxygen continuously to improve cyanosis. Artificial respiration may be necessary
- If the patient is hypothermic, immediately perform a careful rewarming.
- If the patient has low blood pressure/ in hypovolemia shock, initiate fluid therapy. Give pressors (e.g. norepinephrine, dopamine) if shock persists or worsens.
- GI decontamination
- Alkalinization of the urine enhances the elimination of phenobarbital and, likely, other long-acting barbiturates by ion trapping. Urinary alkalinization is not recommended for short-acting barbiturate toxicity.
- If the coma is prolonged, give:
- I/V fluids
- Amphetamine sulfate 10 mg, every 30 minutes till improvements occur.
- Prophylactic antibiotics to prevent pulmonary infection and complications.
- Dialysis.
34.4: Benzodiazepines
- Death by benzodiazepines alone in the absence of other significant toxicological agents or pathology is uncommon, although benzodiazepines alone can cause death in absence of significant natural diseases or advanced age.
- Acute overdose toxicity has been associated with short-acting benzodiazepines such as midazolam and triazolam and intermediate-acting flunitrazepam than with diazepam, lorazepam, and nitrazepam.
- It acts as a CNS depressant and can bring about relief of anxiety. It also acts as a muscle relaxant and is used to control convulsions.
- Fatal Dose and Period: Not Known.
- Toxicity Rating: 3
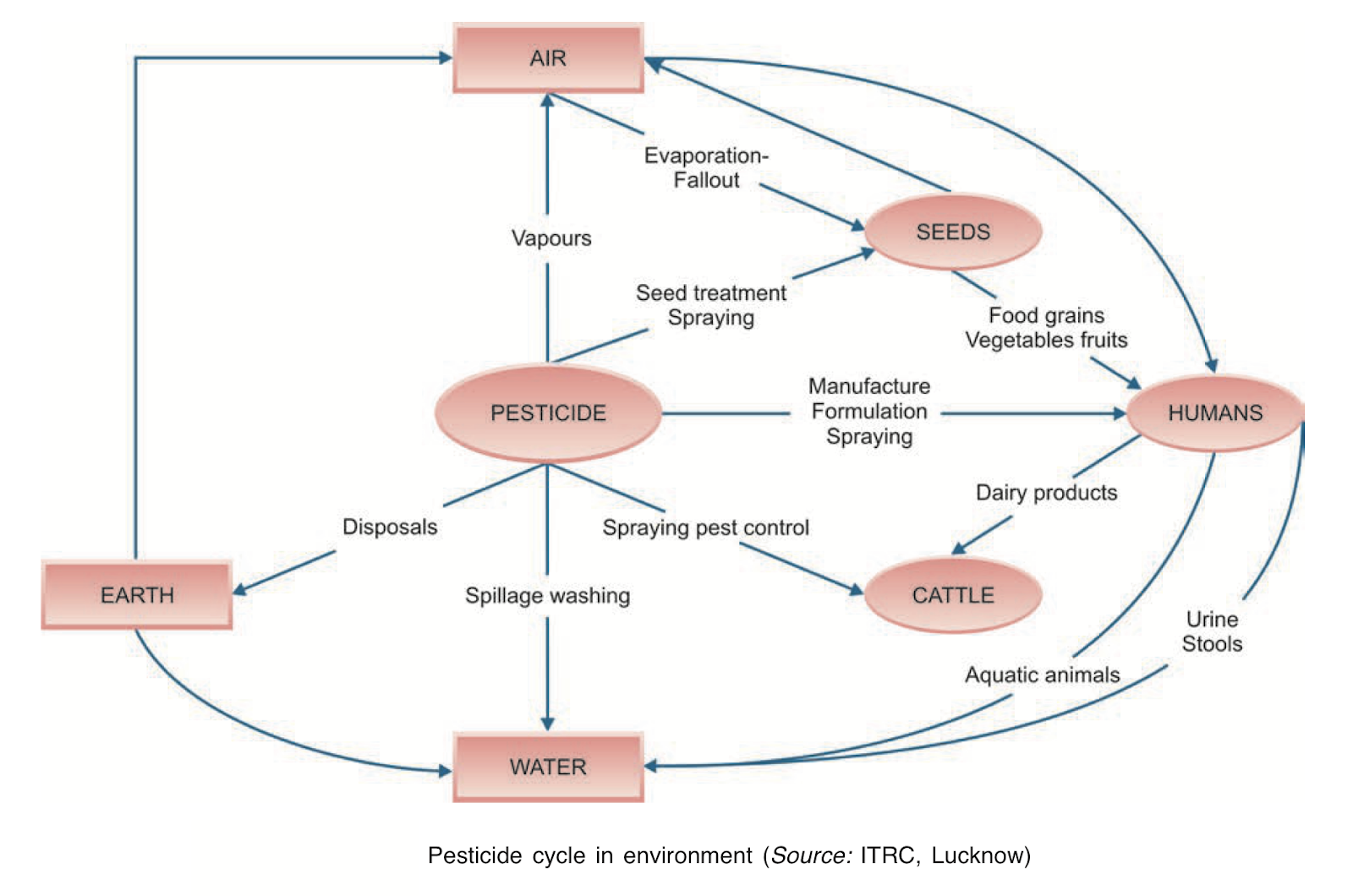
34.5: Pesticides & Insecticides
- Pesticide — any substance or mixture of substances intended for preventing, destroying or controlling any pest (insects, rodents, fungi, mites, ticks, mollusks, weeds, and herbs) including vectors of human or animal diseases.
- Insecticide — any substance or mixture of substances intended for killing insects.
Classification of pesticides depending on the type of pests controlled
- Insecticides: Used for insects.
- Organochlorine Compounds: Endosulfan, Aldrin, BHC, DDT, Chlordane, etc.
- Organophosphorus Compounds: Malathion, Parathion, Monocrotophos, Phorate, etc.
- Carbamate Compounds: Aldicarb, Carbaryl, Carbofuran, Methomyl, etc.
- Herbicide: Used for weeds.
- Paraquat, Diquat, Atrazine, chlorates, Nitrogen, 2, 4-D, Chlorophenoxyacetate (hormone) weed killers, etc.
- Fungicide: Used for fungus.
- Captan, Captafol, Bavistin, Vitavax, Carbamates Thiocarbamates, Hexachlorobenzene, Sodium azide, etc.
- Rodenticide: Used for rodents.
- Zinc Phosphide, Coumachlor, Warfarin, Thallium, P, As, Strychnine, etc.
- Nematicide: Used for nematodes.
- Ethylene Dibromide (EDB), DBCP, etc
- Acaricide: Used for mites, ticks, and spiders.
- Azobenzene, Chlorobenzilate, Tedion, Kelthane, etc.
Hazards from Pesticides
- The pesticide hazards include not only hazards to human health but also hazardous to a rural environment, pest resistance and resurgence, and impact on food.
- Pesticides can result in cancer, birth defects, endocrine disruption, immunosuppression, allergies, and decreased fertility with chronic exposures.
Human health hazards
- Nausea, vomiting and dizziness.
- Loss of memory, loss of appetite.
- Skin and allergic reactions.
- Delayed neurotoxicity.
- Behavioral changes.
- Lesions
- Changes in CNS.
- Peripheral neuritis.
- Carcinogenic and oncogenic diseases.
- Effects on human reproduction leading to sterility, miscarriage, and birth defects.
- Cataract formation.
- Lung and Kidney changes.
- Effect on immune system.
- Enzyme imbalance cholinesterase.
- Cholinesterase inhibition.
Organochlorines
- Organochlorines (OC) are cerebral poisons.
- These are also used as insecticide agents at home, garden and agricultural fields, which were popular once, now they are phasing out all over the world due to its cumulative effect and health hazards.
- These are insoluble in water. DDT is a volatile solid (slow of course) having a faint odor.
- It is highly soluble in benzene and chloroform and moderately soluble in kerosene (11%) and slightly soluble in ethyl alcohol (2%).
- They act by interference with nerve impulse transmission. It initially stimulates the CNS and later on depresses it resulting in death. Sometimes their solvents are toxic than themselves.
- Fatal dose: 15-30 gm for DDT and Lindane, 5-7 gm for Chlordane, 2.5 gm for Aldrin, Dieldrin and Endrin.
- Fatal period: Up to 6 hours.
- Toxicity rating: 4 for DDT and Lindane, 5 for others.
Organophosphorus Insecticides
- Organophosphorus (OP) insecticides are most popular insecticides, often involved in serious/fatal human poisoning incidences. Victims are usually children, farmers and unskilled laborers.
- Older Classification
- Alkyl compounds — hexaethyl tetraphosphates (HETP), tetraethyl pyrophosphates (TEPP), octamethyl pyrophosphoramide (OMPA), malathion, cystox, dipterex, etc.
- Aryl compounds — parathion, para-oxon, methyl parathion, chlorothion, diazinon, (Tick-20), etc.
- Modern Classification
- Agriculture insecticides (highly toxic) — OMPA, TEPPParathion, Phosdrin, Disyston, etc.
- Animal insecticides (moderately toxic) — Ronnel, Coumephos, Trichlorfon, etc.
- Household insecticides (low toxic) — Malathion (Kill bug, Cimexol, Jyothi oil, Bugsolin-20, etc.), Diazinon (Tick-20), Vapona, etc.
Uses of Organophosphorus (OP) Compounds
- In agriculture fields these are either used as aerial spray, mixed with suitable liquid or dust as their vehicle, or they are mixed with soil.
- When sprayed in air, absorption in plants occurs through leaves and stems.
- When used by mixing with soil, absorption occurs through the roots of plants.
- In cases of herbicidal agents, no harm is caused to the plant.
- When the insect sits on the plant, the poison is absorbed through their exoskeleton or when it eats the leaves of the plant, it consumes the poison along with.
- In human beings consuming the grain, fruits or other parts of plants causes no harm.
Diagnosis
- Normal RBC (Red Blood Cell) cholinesterase levels are 5300- 10,000 units/L. Markedly decreased RBC cholinesterase levels (<30% normal) are diagnostic.
- RBC cholinesterase levels regenerate slowly (0.5-1% per day).
- Depending on the RBC cholinesterase activity the levels of poisoning have been also classified into:
- Mild poisoning — activity is 20-50% of baseline activity
- Moderate poisoning — activity is 10-20% of baseline.
- Severe poisoning — activity is < 10% of the baseline activity.
Treatment
- Prehospital measures
- Decontamination, which is of paramount importance with organophosphate poisoning cases.
- Supportive care, including airway control, oxygenation, ventilation, and seizure management, is a must and equally important.
- Placement of an IV line and cardiac monitoring are indicated.
- The presence of agricultural spray equipment, bottles of insecticides, odors (garlic/ kerosene like), and other clues to diagnosis are often unavailable to other health care personnel.
- Hospital Care
- Maintain and protect airway
- Supplemental Oxygen
- Gastrointestinal decontamination
- Administration of Specific Antidotes
- Atropine Administration: Atropine is administered immediately to save life and continued till the achievement of the state of “Atropinisation”, which is diagnosed by clinical manifestations (in the patients) of flushing, dry mouth, pupillary dilation, etc.
- Pralidoxime Administration: Pralidoxime brings about anticholinergic “atropine-like” effects resulting in freeing and reactivating cholinesterase enzymes by cleaving phosphorylation — acetyl cholinesterase bond. It directly reacts and detoxifies organophosphate molecules.
- Furosemide (Lasix): It is given in a dose of 40 to 160 mg IV to alleviate the pulmonary congestion remaining after full atropinization.
- Benzodiazepine: It is given in a dose of 5 to 10 mg slow IV push for seizures, repeated every 5 to 10 minutes to control or maximum upto 30 mg in adults; 0.2 to 0.5 mg/kg IV every 5 minutes to maximum of 10 mg in children > 5 years, 5 mg in children < 5 years; Lorazepam may also be used.
Precautions during Treatment
- Person nursing should wear gloves, mask, etc. to prevent getting poisoned by absorption via skin or inhalation of poisonous fumes through the respiratory tract
- Never give the following drugs
- Morphine
- Aminophylline
- Phenothiazine
- Reserpin
- Perform blood cholinesterase level estimation to diagnose the case or assess prognosis with treatment.
Fatal dose, period and toxicity rating of the important organophosphates compounds
| Compounds | Fatal Dose | Fatal Period | Toxicity Rating |
|---|---|---|---|
| TEPP | 100 mg | 0-6 hrs | 6 |
| OMPA | 200 mg | 0-6 hrs | — |
| Malathion | 1 gm | 0-6 hrs | 4 |
| Parathion | 100 mg | 0-6 hrs | 6 |
| Diazinon | 1 gm | 0-6 hrs | 4 |
Carbamates
- Carbamate poisoning exhibits a similar clinical picture to organophosphate toxicity.
- Carbamate compounds temporarily bind cholinesterase for approximately 6 hours with no permanent damage.
- Carbamates have poor CNS penetration and cause minimal CNS symptoms.
- Carbamates are cerebral poisons. They are also popular insecticides producing similar manifestations as organophosphates.
- Fatal dose and fatal period: Uncertain.
- Toxicity Rating: 4-5.
- Highly toxic — e.g. Aldicarb, Aprocarb (Baygon), Carbofuran.
- Moderately toxic — e.g. carbaryl (Sevin), primicarb, propoxur (Hit spray).
Aluminum Phosphide
- Aluminum phosphide is a solid fumigant pesticide, widely used as a grain preservative in India. It is marketed as greyish-green tablets.
- On exposure to air or moisture, it liberates phosphine and can produce multiorgan damage.
- Metallic taste, garlicky odor, nausea, pain in gullet, stomach, abdomen, vomiting, diarrhea, cough dyspnea, respiratory failure, headache, anxiety, hypotension tachy/bradycardia, CCF, myocarditis, hepatosplenomegaly renal failure, coma, etc.
- Fatal Dose: 5 gm.
- Fatal Period: Up to 24 hrs.
Naphthalene
- Naphthalene is an insecticide, a solid volatile substance obtained from the middle fraction of coaltar distillation and has chemical properties similar to benzene.
- It occurs as large, lustrous, crystalline plates with characteristic odor. Soluble in water, but dissolves freely in ether, chloroform, alcohol and oils.
- Naphthalene is an irritant, nephrotoxic, hemolytic and hepatotoxic.
- Fatal dose: 2 gm
- Fatal period: Uncertain.
34.6: Datura
- Datura is a vegetable deliriant type of cerebral poison.
- Datura plant is about 1.2-2 meter height with widely spread branches. Fruit is about the size of a walnut, spherical and covered with sharp spiny projections.
- Each fruit on an average contains about 500 seeds. They are yellowish-brown in color and resemble chilly seeds. The leaves are dark green, alternate and broadly ovate in shape.
- Poisoning occurs only if seeds are masticated and swallowed. It is bitter in taste and can initially lead to, stimulation of higher centers of brain.
- Active principle of the plant has several medicinal uses such as, Mydriatic, spasmolytic, antidote in organophosphorus and carbamate poisoning, preanesthetic medication, bronchial asthma.
- Fatal dose: 50 to 75 seeds (0.6-1 gm)
- Fatal period: 3 to 4 hours to 24 hours
- Toxicity rating: Seeds-3, atropine-5.
34.7: Cannabis
- Cannabis is classified under deliriant cerebral neurotic plant poison.
- It is also classified as a mild hallucinogen or a sedative or a narcotic. In fact the drug is believed to produce all these effects in various individuals in a different way.
- It is a collective term used for psychoactive compounds derived from the plant Cannabis sativa or hemp plant. It belongs to the botanical family Cannabinaceae and is a tall weed growing up to 15 feet in height.
- Lethal dose is:
- 2000 mg of charas
- 8000 mg of ganja
- 10,000 mg/kg body wt of bhang.
- For mere excitement effects just 1 to 5 gm of Cannabis Indica is sufficient (equivalent to 3 refer cigarettes) for non-addict.
- Fatal Period: 12 hrs.
Cannabis Preparations
- Cannabis is usually dried and either smoked or eaten. The cannabis preparations usually emit a peculiar odor which is described as that of burnt rope.
- Cannabis is usually used in three forms in India and they are:
- Ganja: It is the resinous mass composed of small leaves and bracts of inflorescence from female plants, which contains about 25% of the active principle. It is usually mixed with tobacco and smoked in pipe.
- Charas: It is also called as Hashish and is the purest form of cannabis. It is the dried resinous exudate from the flower tops. It is dark green or brown in color, and contains 25 to 40% of the active principle.
- Bhang: Also called as siddhi, patti or sabji is the crudest form of cannabis. It is prepared as a decoction of dried mature leaves and flower stems, and contains 15% of active principle. It is usually consumed in the form of a beverage.
- Other forms of cannabis are:
- Marijuana — the most common illicit drug used.
- It refers to any part of the cannabis plants or its extract that is used to induce psychotomimetic or therapeutic effects. It is eaten alone or as a part of confection, or drunk in beers, or some other beverage, or smoked in pipes or after being rolled into cigarettes.
34.8: Cocaine
- Cocaine is a deliriant cerebral neurotic.
- Cocaine is an alkaloid obtained from the dried leaves of coca plant (Erythroxylon coca).
- Cocaine hydrochloride is a white, colorless, crystalline substance, which has a bitter numbing taste. It is slightly soluble in water, but freely soluble in alcohol.
- Crack cocaine is a cocaine preparation which has been separated from its hydrochloride base (free base) by adding baking soda and water, followed by heating and then drying, which can be mixed with tobacco and smoked.
- Chronic consumption can develop addiction to cocaine.
- Fatal Dose: 1gm
- Fatal period: 2 hrs.
Severe Complications of Acute Cocaine Poisoning
- Stroke, including subarachnoid and intracerebral hemorrhage and cerebral infarcts.
- Cardiovascular complications such as myocardial infarction, ventricular arrhythmias and cardiac arrest.
- Intestinal ischemia.
Essential Investigations in Cocaine Intoxication Cases
- Early and frequent blood pressure recording and ECG monitoring.
- Detect cocaine in urine by simple drug of abuse screening tests.
- Metabolites of cocaine may be detected in the urine even after 2-3 days postexposure.
- Cocaine is unstable in blood and hence must be collected in fluoride oxalate bulbs/ tubes.
Cocainism
- Chronic cocaine poisoning, cocainophagia, cocainomania, cocaine addiction.
- Chronic consumption of cocaine, for the euphoric effects of cocaine. Addicts usually take cocaine by subcutaneous injection or eat in paan or inhale it as snuff.
Magnan’s Symptom
- Magnan’s symptom is a type of tactile hallucination making the addict feel like insects (bugs) are crawling under the skin of the part of their body.
- He or she may even complain of presence of sand grain under the skin
34.9: Strychnine
- Strychnine is a spinal poison.
- Seeds are the toxic part of the plant. These seeds are grayish brown in color, and measure about 2.5 cm in diameter 0.65 cm in thickness, and are discoidal in shape with central depression.
- For the onset of action the seeds must be masticated and swallowed, the site of action being anterior horn cells of the spinal cord. It acts by competitive antagonism of inhibitory neurotransmitter glycine at the postsynaptic spinal cord motor neurons.
- Fatal Dose: 1-2 crushed seeds (15 to 50 mg/ 5-8 mg/kg body weight of strychnine).
- Fatal period: 1-2 hrs.
\n