MATERNAL-MIDTERMS
NCM 107 MATERNAL
CARE OF MOTHER, CHILD AND ADOLESCENT (WELL CLIENT)
https://www.youtube.com/watch?v=k6jqx9kZgPM
UNIT 1
Obstetrics
the care of women during childbirth
from the Greek word obstare, which means to keep watch
Obstetrics involves care during pregnancy, childbirth, and the postpartum period
Gynecology
deals with reproductive health and the functions and diseases specific to women and girls
Pediatrics
derived from the Greek word pais, meaning "child."
Although the field of nursing typically divides its concerns for families during childbearing and childrearing into two separate entities, maternity care and child health care, the full scope of nursing practice in this area is not two separate entities but rather a continuum:
maternal and child health nursing
Foundation of Maternal and Child Health Nursing Practices/Biophysical Aspects of Human Reproduction
.
Philosophy of Maternal and Child Health Nursing
- Maternal and child health nursing is family centered
- Maternal and child health nursing is community centered
- Maternal and child health nursing is evidence based
- Maternal and child health nurse serves as an advocate.
- Maternal and child health nursing includes a high degree of independent nursing functions.
- Promoting health and disease prevention are important nursing roles
- Maternal and child health nurses serve as important resources for families during childbearing and childrearing.
- Personal, cultural, and religious attitudes and beliefs influence the meaning and impact of childbearing and childrearing on families.
- Circumstances such as illness or pregnancy are meaningful only in the context of a total life.
- Maternal and child health nursing is a challenging role for nurses and a major factor in keeping families well and optimally functioning,
2. Goals
- The Primary GOAL of maternal and child health nursing is the promotion and maintenance of optimal family health to ensure cycles of optimal childbearing and childrearing
The range of practice includes:
Pre conceptual health care
- Care of women during three trimesters of pregnancy and the puerperium.
- Care of children during the perinatal period (6 weeks before conception to 6 weeks after birth)
- Custody of children from birth through adolescence
- Care in settings as varied as the birthing room, the pediatric intensive care unit, and the home in all environments and types of care, keeping the family at the center of care delivery is an essential goal
If a family's level of functioning is low, the emotional, physical, and social health and potential of individuals in that family can be adversely affected.
What is the childbearing-childrearing continuum? By childbearing we mean the act of having children, while childrearing is how they are brought up.
- The continuum for maternal, newborn and child health usually refers to the continuity of individual care.
- It is the population level or public health framework based on integrated service delivery throughout the life cycle and promote health for mothers, babies and children.
Many of the changes in childbearing and childrearing over this period come as direct result of the other trends.
- The provision of pre conceptual health care
- Provision of nursing care of women throughout pregnancy birth, and postpartum
- Provision of nursing care to families in all settings.
Department of Health (DOH)'s Safe Motherhood Program
- The program's main objective is to ensure that Filipino women will have full access to quality maternal health care services so they will have a safer pregnancy and delivery of their child.
The Program contributes to the national goal of improving women's health and well-being by:
(DOH)Objectives
- Collaborating with Local Government Units in establishing sustainable, cost-effective approach of delivering health services that ensure access of disadvantaged women to acceptable and high quality maternal and newborn health services and enable them to safely give birth in health facilities near their homes
- Establishing core knowledge base and support systems that facilitate the delivery of quality maternal and newborn health services in the country
Four phases of health care are:
- Health promotion
Educating parents and children to follow health practices through teaching and role modeling
- Health Maintenance
Intervening to maintain health when risk of illness is present
- Health Restoration
Using conscientious assessment to be certain that symptoms of illness are identified and
interventions are begun to return client to wellness most rapidly principles
- Health Rehabilitation
Helping prevent complications from illness; helping a client with residual effects achieve an optimal state of wellness and independence; helping a client to accept inevitable death
To understand the Concepts, theories, principles and Standards of Care
- Nursing Intervention
- Nursing Theories
- Nursing process
- Nursing Research
Common Measures to Ensure Family Centered Maternal and Child Health Care Principle
- The family is the basic unit of society. cultural and socioeconomic
- Families represent racial, ethnic, cultural, and socioeconomic diversity
- Children grow both individually and a part of a family.
Nursing Interventions
key measures for the delivery of family centered maternal and child health care.
- Consider the family as a whole as well as its individual members
- Encourage families to reach out to their community so that family members are not isolated from their community or from each other.
- Encourage family bonding through rooming-in in both maternal and child health hospital settings.
- Participate in early hospital discharge programs to reunite families as soon as possible.
- Encourage family and sibling visits in the hospital to promote family contacts.
- Assess families for strengths as well as specific needs or challenges
- Respect diversity in families as a unique quality of that family.
- Encourage families to give care to a newborn or ill child Include developmental stimulation in nursing
- Share or initiate information on health planning with family member so that care is family oriented
Concepts, Theories, Principles and Standards of Care Nursing Theory
One of the requirements of a profession (together with other critical determinants, such as member- set standards, monitoring of practice quality, and participation in research) is that the concentration of a discipline's knowledge flows from a base of established theory
- Another issue most nursing theorists address is how nurses should be viewed or what the goals of nursing care should be
- Extensive changes in the scope of maternal and child health nursing have occurred as health promotion, or keeping parents and children well, has become a greater priority.
- With health promotion as a major nursing goal, teaching, counseling, supporting, and advocacy are also common roles.
- Because care of women during pregnancy and of children during their developing years helps protect not only current health but also the health of the next generation, maternal child health nurses fill these expanded roles to a unique and special degree
The Nursing Process
- Using an organized series of steps, to ensure quality and consistency of care (Carpenito, 2007)
- The nursing process is a form of problem solving based on the scientific method, serves as the basis for assessing making a nursing diagnosis, planning organizing and evaluating care.
- The nursing process is applicable to all health care settings, from the prenatal clinic to the pediatric intensive care unit
Evidence-Based Practice
Nursing research and use of evidence-based practice are methods by which maternal and child health nursing expands and improves
Evidence-Based Practice is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of patients and can be a combination of research and clinical expertise
The worth of evidence is ranked according to
Level I: Evidence obtained from at least one properly designed randomized controlled trial
Level II: Evidence obtained from well-designed controlled trials without randomization, well- designed cohort or case-control analytic studies, or multiple time series with or without an
Level III: Opinions of respected authorities, based on clinical experience, descriptive studies, or reports of expert committees
Nursing research
Is the controlled investigation of problems that have implications for nursing practice, provides evidence and justification for implementing activities for outcome achievement
Nursing research and use of evidence based practice are methods by which maternal and child health nursing expands and improves
Nursing Research
Anatomy and Physiology
Although the structures of the female and male reproductive systems differ greatly in both appearance and function, they are homologues that is, they arise from the same or matched embryonic origin.
Gynecology study of the female reproductive organs.
Andrology study of the male reproductive organs.
Female Reproductive System
- External Genitalia
- Vulva: The structures that form the female external genitalia
- Mons Veneris: is a pad of adipose tissue located over the symphysis pubis, the pubic bone joint.
It is covered by a triangle of course, curly hairs.
The purpose of the mons were is to protect the junction of the public bone from trauma.
- Labia Minora: Just posterior to the mons veneris spread two hairless folds of connective tissue, the labia minora.
- Before menarche, these folds are fairly small; by childbearing age, they are firm and full;
- After menopause, they atrophy and again become much smaller. Normally the folds of the labia minora are pink; the internal surface is covered with mucous membrane, and the external surface with skin.
- Labia Majora: are two folds of adipose tissue covered by loose connective tissue and epithelium that are positioned lateral to the labia minora.
- Labia Minora: Just posterior to the mons veneris spread two hairless folds of connective tissue, the labia minora.
Covered by pubic hair
Other External Organs
- Vestibule is the flattened, smooth surface inside the labia. The openings to the bladder (the urethra) and the uterus (the vagina) both arise from the vestibule.
- Clitoris is a small (approximately 1 to 2 cm),rounded organ of erectile tissue at the forward junction of the labia minora. It is covered by a fold of skin, the prepuce.
Function of the labia majora serve as protection for the external genitalia and the distal urethra and vagina.
Function: The clitoris is sensitive to touch and temperature and is the center of sexual arousal and orgasm in a woman.
- Two Skene's glands (paraurethral glands) are located just lateral to the urinary meatus, one on each side. Their ducts open into the urethra.
- Bartholin's glands (vulvovaginal glands) are located just lateral to the vaginal opening on both sides. Their ducts open into the distal vagina.
Function: Secretions from both of these glands help to lubricate the external genitalia during coitus. The alkaline pH of their secretions helps to improve sperm survival in the vagina.
- Fourchette is the ridge of tissue formed by the posterior joining of the two labia minora and the labia majora.
- This is the structure that is sometimes cut (episiotomy) during childbirth to enlarge the vaginal opening,.
- Posterior to the fourchette is the perineal muscle or the perineal body.
- Function: this is a muscular area and it is easily stretched during childbirth to allow for enlargement of the vagina and passage of the fetal head.
- Hymen is a tough but elastic semicircle of tissue that covers the opening to the vagina in childhood.
- It is often torn during the time of first sexual intercourse
- However, because of the use of tampons and active sports participation, many girls who have not had sexual relations do not have intact hymens at the time of their first pelvic examination
- Fourchette is the ridge of tissue formed by the posterior joining of the two labia minora and the labia majora.
Female Internal Structures
- OVARIES are approximately 4 cm long by 2 cm in diameter and approximately 1.5 cm thick, or the size and shape of almonds. They are grayish white and appear pitted, or with minute indentations on the surface. Ovaries are located close to and on both sides of the uterus in the lower abdomen.
- The function of the two ovaries (the female gonads) is to produce, mature, and discharge ova (the egg cells).
- Ovarian function, therefore, is necessary for maturation and maintenance of secondary sex
- An unruptured, glistening, clear, fluid-filled graafian follicle (an ovum about to be discharged).
- or a miniature yellow corpus luteum (thestructure left behind after the ovum has been discharged)
- OVARIES are approximately 4 cm long by 2 cm in diameter and approximately 1.5 cm thick, or the size and shape of almonds. They are grayish white and appear pitted, or with minute indentations on the surface. Ovaries are located close to and on both sides of the uterus in the lower abdomen.
Ovaries have three principal divisions:
- Protective layer of surface epithelium
- Cortex, where the immature (primordial) oocytes mature into ova and large amounts of estrogen and progesterone are produced
- Central medulla, which contains the nerves, blood vessels, lymphatic tissue, and some smooth muscle tissue.
The ovaries produce estrogen and progesterone and initiate and regulate menstrual cycles
After menopause, or cessation of ovarian function, the uterus, breasts, and ovaries all undergo atrophy or a reduction in size because of a lack of estrogen
The estrogen secreted by ovaries is also important to prevent osteoporosis, or weakness of bones, because of
Cholesterol is incorporated into estrogen, the production of estrogen is thought to also keep
cholesterol levels reduced, thus limiting the effects of atherosclerosis (artery disease) in
Estrogen used to be prescribed for women at menopause to help prevent osteoporosis and cardiovascular disease. However, this type of long- term estrogen supplementation may contribute to breast cancer and cerebrovascular accidents.
Because they are suspended in position rather than being firmly fixed in place, an abnormal tumor or cyst growing on them can enlarge to a size easily twice that of the organ before pressure on surrounding organs or the ovarian blood supply leads to symptoms of compression.
This is the reason that ovarian cancer continues to be one of the leading causes of death from cancer in women (ie the tumor grows without symptoms for an extended period)
Division of Reproductive Calls (Gametes)
At birth, each ovary contains approximately 2 million immature ova (cocytes), which were formed during the first 5 months of intrauterine life.
Although these cells have the unique ability to produce a new individual, they basically contain the usual components of cells:
- cell membrane, an area of dear cytoplasm
- and a nucleus containing chromosomes
- The oocytes, like sperm, differ from all other body cells in the number of chromosomes they contain in the nucleus. (Genetic material)
- The nucleus of all other human body cells contains 46 chromosomes, consisting of 22 pairs of autosomes (paired matching chromosomes) and 1 pair of sex chromosomes (two X sex chromosomes in the female, an X and a Y sex chromosome pair in the male).
- In Reproductive cells both ova and spermatozoa) have only half the usual number of chromosomes, so that, when they combine (fertilization), the new individual formed from them will have the normal number of 46 chromosomes.
- FALLOPIAN TUBES. The fallopian tubes arise from each upper corner of the uterine body and extend outward and backward until ach opens at its distal end, next to an ovary. Fallopian tubes are approximately 10 cm long in a mature woman
- Their function is to convey the ovum from the ovaries to the uterus and to provide a place for fertilization of the ovum by sperm
It is anatomically divided into four separate parts.
- the interstitial portion. The most proximal division and the part of the tube that lies within the uterine wall. This portion is only about 1 cm in length; the lumen of the tube is only 1 mm in diameter at this point.
The isthmus is the next distal portion. It is approximately 2 cm in length and like the interstitial tube, is extremely narrow. This is the portion of the tube that is cut or sealed in a tubal ligation, or tubal sterilization procedure.
- The ampulla is the third and also the longest portion of the tube. It is approximately 5 cm in length.
It is in this portion that fertilization of an ovum usually occurs.
- The infundibular portion is the most distal segment of the tube. It is approximately 2 cm long and is funnel shaped. Migration of the ovum is also aided by the action of the diliated lining and the mucus, which acts as a lubricant.
Function: The mucus produced may also act as a source of nourishment for the fertilized egg, because it contains protein, water and salts.
- Uterus, is a hollow, muscular pear-shaped organ located in the lower pelvis, posterior to the bladder and anterior to the rectum. Uterus is approximately 5 to 7 cm long, 5 cm wide, and, in its widest upper part, 2.5 cm deep.
- In a nonpregnant state, it weighs approximately 60 9.
- After a pregnancy, the uterus never returns to its nonpregnant size but remains approximately 9 cm long, 6 cm wide, 3 cm thick, and 80 g in weight.
The function of the uterus is to :
- receive the ovum from the fallopian tube;
- provide a place for implantation and nourishment;
- furnish protection to a growing fetus; 4. and, at maturity of the fetus, expel it from a woman's body
The uterus consists of three divisions:
- the body or corpus,
- the isthmus,
- the cervix.
- The body of the uterus is the uppermost part and forms the bulk of the organ. During pregnancy, the body of the uterus is the portion of the structure that expands to contain the growing fetus.
The fundus is also the portion that can be palpated abdominally to determine the amount
of uterine growth occurring during pregnancy
To measure the force of uterine contractions during labor, and to assess that the uterus is returning to its nonpregnant state after childbirth.
- The isthmus of the uterus is a short segment between the body and the cervix. It is the portion of the uterus that is most commonly cut when a fetus is born by a cesarean birth.
- The cervix is the lowest portion of the uterus. It represents approximately one third of the total uterus size and is approximately 2 to 5 cm long The opening of the canal at the junction of the cervix and isthmus is the internal cervical os the distal opening to the vagina is the external cervical os.
Three Separate layers of Uterine tissue:
- endometrium is the inner layer of mucous membrane
- myometrium is the middle layer of muscle
- perimetrium is the outer layer of connective tissue
- Endometrium layer of the uterus is the one that is important for menstrual function. It grows and becomes so thick and responsive each month under the influence of estrogen and progesterone that it is capable of supporting a pregnancy. If pregnancy does not occur, this is the layer that is shed as the menstrual flow
- The myometrium or muscle layer of the uterus, is composed of three interwoven layers of smooth muscle, the fibers of which are arranged in longitudinal transverse, and oblique directions
- This network offers extreme strength to the organ.
- serves the important function of constricting the tubal junctions and preventing regurgitation of menstrual blood into the tubes.
- It also holds the internal cervical os closed during pregnancy to prevent a preterm birth
- When the uterus contracts at the end of pregnancy to expel the fetus, equal pressure is exerted at all points throughout the cavity because of its unique arrangement of muscle fibers.
- After childbirth, this interlacing network of fibers is able to constrict the blood vessels coursing through the layers, thereby limiting the loss of blood in the woman.
- The perimetrium or the outermost layer of the uterus, serves the purpose of adding strength and support to the structure
Male Reproductive System
Male External Structures include:
- Penis.
- 3 cylindrical masses of erectile tissue in the penis shaft: two termed the corpus cavernosa, and a third termed the corpus spongiosum
- with sexual excitement, nitric oxide is released from the endothelium of blood vessels This results in dilation of blood vessels and an increase in blood flow to the arteries of the penis (engorgement)
- The ischiocavernosus muscle at the base of the penis then contracts, trapping both venous and arterial blood in the three sections of erectile tissue and leading to distention and erection of the penis.
- At the distal end of the organis a bulging, sensitive ridge of tissue, the glans.
- A retractable casing of skin, the prepuce, protects the nerve-sensitive glans at birth
- Scrotum is a rugated, skin-covered, muscular pouch suspended from the perineum.
- Its functions are to support the testes and to help regulate the temperature of sperm
- In very cold weather, the scrotal muscle contracts to bring the testes closer to the body
- In very hot weather, or in the presence of fever, the muscle relaxes, allowing the testes to fall away from the body.
- In this way, the temperature of the testes can remain as even as possible to promote the production and viability of sperm.
- Testes are two avoid glands, 2 to 3 cm wide, that lie in the scrotum.
- Each testes is encased by a protective white fibrous capsule and is composed of several lobules, with each lobule containing interstitial cells (Leydig's cells) and a seminiferous tubule.
- Seminiferous tubules produce spermatozoa.
- Leydig's cells are responsible for the production of testosterone
- Although spermatozoa are produced in the testes, they reach maturity, surrounded by Semen, in the external structures through a complex sequence of regulatory events.
The Male Internal Reproductive Organs:
- First, the hypothalamus releases GnRH, which in turn influences the anterior pituitary gland to release FSH and LH
- FSH is then responsible for the release of androgen binding protein (ABP).
- LH is responsible for the release of testosterone.
- ARP binding of testosterone promotes sperm formation
- As the amount of testosterone increases, a feedback effect on the hypothalamus and anterior pituitary gland is created that slows the production of FSH and LH and ultimately decreases or regulates sperm production
The Male Internal Reproductive Organs:
- Epididymis. The seminiferous tubule of each testis leads to a tightly coiled tube over 20 ft long.
- Responsible for conducting sperm from the tubule to the vas deferens
- and secrete a portion of the alkaline fluid that will surround sperm at maturity semen, or
seminal fluid that contains a basic sugar and mucin, a form of protein)
- Sperm are immobile and incapable of fertilization as they pass or are stored at the epididymis level.
- It takes at least 12 to 20 days for them to travel the length of the epididymis and a total of 64 days for them to reach maturity
- This is one reason that aspermia (absence of sperm) and oligospermia (20 million sperm/ml) are problems that do not appear to respond immediately to therapy but rather only after 2 months
- Vas Deferens (Ductus Deferens) is an additional hollow tube surrounded by arteries and veins and protected by a thick fibrous coating
- Function is it carries sperm from the epididymnis through the inguinal canal into the abdominal cavity.
- Sperm mature as they pass through the vas deferens
- They are still not mobile at this point, probably because of the fairly acidic medium of the semen produced at this level
- A varicocele, or a varicosity of the internal spermatic vein, was once thought to contribute to male subfertility by causing congestion with increased warmth in the testes but this appears to actually make little difference
- Vasectomy (severing of the vas deferens to prevent passage of sperm) is a popular means of male birth control
- Seminal Vesicles are two convoluted pouches that lie along the lower portion of the posterior surface of the bladder and empty into the urethra by way of the ejaculatory ducts.
- These glands secrete a viscous alkaline liquid that has a high sugar, protein, and prostaglandin content.
- Sperm become increasingly motile with this added fluid, because it surrounds them with nutrients and a more favorable pH.
- Ejaculatory Ducts. The two ejaculatory ducts pass through the prostate gland and join the seminal vesicles to the urethra.
- Prostate Gland. The prostate is a chestnut sized gland that lies just below the bladder.
- The urethra passes through the center of it, like the hole in a doughnut.
- The prostate gland secretes a thin, alkaline fluid. When added to the secretion from the seminal vesicles and the accompanying sperm from the epididymis, This alkaline fluid further protects sperm from being immobilized by the naturally low pH level of the urethra.
- Bulbourethral Glands. Two bulbourethral or Cowper's glands lie beside the prostate gland and empty via short ducts into the urethra.
- Like the prostate gland and seminal vesicles, they secrete an alkaline fluid that helps counteract the acid secretion of the urethra and ensure the safe passage of spermatozoa.
Semen is derived from the
- prostate gland (60%)
- seminal vesicles (30%)
- epididymis (5%)
- bulbourethral glands (5%)
- Urethra. The urethra is a hollow tube leading from the base of the bladder, which, after passing through the prostate gland, continues to the outside through the shaft and glans of the penis.
It is approximately 8 in (18 to 20 cm) long.
Process of Spermatogenesis
Sperm maturation begins at 13 years old
Testes – produce sperm cell and responsible for the production of the male hormone; testosterone
LEYDIG'S cells - produce sperm cell
SERTOLI cells -nourished the sperm cells; "nurse cells
- hypothalamus releases GnRH that Stimulates APG (Anterior pituitary gland) = secrete FSH & LH = stimulates seminiferous tubules to produce spermatozoa
- Epididymis - maturation of the sperm cell occurs.( 12-24 days)
- Vas deferens - passageway of the matures sperm.
- Seminal vesicle - produce sugar fluid known as fructose to increase motility:
- Ejaculatory duct-passageway
- Prostate gland - secretes fluid that lubricates and nourished sperm cell.
- Cowper's gland -bulbourethral gland - Secretes alkaline fluid that helps counteract the acid secretion of the urethra and ensure the safe passage of the spermatozoa.
- Urethra - a hollow tube leading from the base of the bladder continues to the outside through the shaft and glands of the penis. 8 inches long
UNIT 2
D. Sexuality
- It is a multidimensional phenomenon that
includes feelings, attitudes, and actions.
- It has both biologic and cultural components.
- It encompasses and gives direction to a person's physical, emotional, social, and intellectual responses throughout life.
Biologic gender
denote a person's chromosomal sex: male (XY) or female (XX).
Gender identity or sexual identity
inner sense a person has of being male or female, which may be the same as or different from biologic gender.
Gender role is the male or female behavior a person exhibits, which, again, may or may not be the same as biologic gender or gender identity.
Several Theories Exist Regarding the Development of Gender Identity arises from primarily a Biologic or a Psychosocial focus.
- The amount of testosterone secreted in
utero (a process termed sex typing) may affect how gender develops.
- Role models portray their gender roles may also influence how a child envisions himself or herself.
- Gender role is also culturally influenced.
4 Discreet Stages in Sexual Response
- Excitement
- Plateau
- Orgasm
- Resolution
Excitement
- It occurs with physical and psychological
stimulation (i.e.sight, sound, emotion, or thought)
- This leads to arterial dilation and venous constriction in the genital area leading to vasocongestion and increasing muscular tension.
- WOMEN: vasocongestion causes the clitoris to increase in size and mucoid fluid to appear on vaginal walls as lubrication.
- The vagina widens in diameter and increases in length.
- The nipples become erect.
- MEN: penile erection, scrotal thickening and elevation of the testes.
- In both sexes, there is an increase in heart and respiratory rates and blood pressure.
Plateau stage
It is reached just before orgasm.
- In woman, the clitoris is drawn forward and retracts under the clitoral prepuce; the lower part of the vagina becomes extremely congested (formation of the orgasmic platform), and there is increased nipple elevation.
- In men, the vasocongestion leads to distention of the penis, heart rate increases to 100 to 175 beats per minute and respiratory rate to approximately 40 respirations per minute.
Orgasm
It occurs when stimulation proceeds through the plateau stage to a point at which the body suddenly discharge accumulated sexual tension.
- Resolution:
It is a 30-minute period during which the external and internal genital organs return to an unaroused state.
Types of Sexual Orientation
- Heterosexuality is a person who finds sexual fulfillment with a member of the opposite gender
- Homosexuality is a person who finds sexual fulfillment with a member of his or her own sex. Many homosexual men prefer to use the term "gay." "Lesbian" refers to a homosexual woman.
- Bisexuality if they achieve sexual satisfaction from both homosexual and heterosexual relationships. Like men who have sex with men, bisexual men may be at greater risk for HIV and STIs than are others.
- Trans-sexuality or transgender person is an individual who, although of one biologic gender, feels as if he or she is of the opposite gender. Such people may have sex change operations so that they appear cosmetically.
Other Types of Sexual Expression
Sexual Abstinence (celibacy) is separation from sexual activity). It is the avowed state of certain religious orders.
Masturbation is self-stimulation for erotic pleasure.
Erotic Stimulation is the use of visual materials such as magazines or photographs for sexual arousal.
Fetishism is sexual arousal resulting from the use of certain objects or situations. Leather, rubber, shoes, and feet are frequently perceived to have erotic qualities.
Transvestism is an individual who dresses in the clothes of the opposite sex. Transvestites can be heterosexual, homosexual, or bisexual.
Voyeurism is obtaining sexual arousal by looking at another person's body. Almost all children and
adolescents pass through a stage when voyeurism is appealing. Dr. Bev Knox.
Sadomasochism involves inflicting pain (sadism) or receiving pain (masochism) to achieve sexual satisfaction.
Exhibitionism is revealing one's genitals in public.
Bestiality is sexual relations with animals.
Pedophiles are individuals who are interested in sexual encounters with children. Known pedophiles are registered as sex offenders.
Controversy about Sexual Orgasm
The female orgasm has been a topic of much controversy over the years, beginning with Freud, who deducted that there were two types of female orgasms:
- clitoral orgasm
- vaginal orgasm
- Freud believed that clitoral orgasms (originating from masturbation or other noncoital acts) represented sexual immaturity.
- And that only vaginal orgasms were the authentic, mature form of sexual behavior in women. Accordingly, he considered women to be neurotic if they could not achieve orgasm through intercourse.
- Masters (1998) showed that there is no physiologic difference between an orgasm achieved through intercourse and one achieved by direct stimulation of the clitoris.
- Women have reported a difference in intensity and character between orgasms achieved through coitus and through other means, and some prefer one to the other, but there is no physiologic change between them.
- For most women, adequate time for foreplay is
essential for them to be orgasmic.
- In recent years, a subject of controversy regarding female sexuality has arisen: the existence or not of "the G spot."
- First described in 1950 by the German physician Gräfenberg, the G spot, presumably located on the inner portion of the vaginal wall, halfway between the pubic bone and the cervix, has been promoted as an area of heightened erotic sensitivity (Baram & Basson, 2007).
- Several studies carried out in the past 10 years have not been able to verify the existence of this particular anatomic site, although some women do claim to possess such an erotic trigger.
Influence of Pregnancy on Sexual Response
- During the second half of the menstrual cycle- the luteal phase-there is increased fluid retention and vasocongestion in a woman's lower pelvis. Because some vasocongestion is already present at the beginning of the excitement stage of the sexual response, women appear to reach the plateau stage more quickly and achieve orgasm more readily during this time.
- Women also may be more interested in initiating sexual relations at this time
- Pregnancy is another time in life when there is vasocongestion of the lower pelvis because of the blood supply needed by a rapidly growing fetus.
- This causes some women to experience a first orgasm during their first pregnancy.
- Following a pregnancy, many women experience increased sexual interest because the new growth of blood vessels during pregnancy lasts for some time and continues to facilitate pelvic vasocongestion.
- This is why discussing sexual relationships is an important part of health teaching during pregnancy.
- At a time when a woman may want sexual contact very much, she needs to be free of myths and misconceptions, such as the notion that orgasm will cause a spontaneous miscarriage. Although the level of oxytocin does appear to rise in women after orgasm, this rise is not sufficient to lead to worry that sexual relations will lead to premature labor in the average woman.
Sexual harassment: is unwanted and repeated sexual advances, remarks, or behavior toward another that is:
- offensive to the recipient and
- Interferes with job or school performance.
- It can involve actions as obvious as a job superior demanding sexual favors or a job superior
sending sexist jokes by e-mail to a person supervised.
- In school it can refer to bullying (Gruber & Fineran, 2007).
- QUID PRO QUO (an equal exchange), in which an employer asks for something in return for sexual favors, such as a hiring or promotion preference.
- HOSTILE WORK ENVIRONMENT, in which
an employer creates an environment in which an employee feels uncomfortable and exploited (e.g., being addressed as "honey," asked to wear revealing clothing, working where walls are decorated with sexist posters).
- Sexual harassment rules apply to same-gender asnwell as opposite-gender harassment.
- In addition to causing occupational disruption, sexual harassment may be so distressing that it leads to short- and long-term psychosocial
consequences for victims and their families such as emotional distress (anxiety, depression, posttraumatic stress disorder, substance abuse), interpersonal conflict, and impaired intimacy and sexual function.
- Nurses should be aware of the sexual harassment guidelines in their own work setting and likewise report such behavior to keep their workplace free of this type of strain.
Disorders of Sexual Functioning
Disorders involving sexual functioning can be:
(PRIMARY) LIFELONG
- (SECONDARY) OR ACQUIRED
- They can have a psychogenic origin (produced by psychic rather than organic factors)
- a biogenic origin (produced by biologic processes), or both.
- They occur in both men and women
Inhibited Sexual Desire
- Lessened interest in sexual relations is normal in some circumstances, such as after the death of a family member, a divorce, or a stressful job change.
- The support of a caring sexual partner or relief of the tension causing the stress allows a return to sexual interest
- Decreased sexual desire can also be a side effect of many medicines.
- Chronic diseases, such as peptic ulcers or chronic pulmonary disorders that cause frequent pain or discomfort may interfere with a man's or a woman's overall well-being and interest in sexual activity
- Obese men and women may not feelas much satisfaction from sexual relations as others,
because they have difficulty achieving deep penetration because of the bulk of their abdomens.
- An individual with an STI such as genital herpes may choose to forgo sexual relations rather than inform a partner of the disease.
- Some women experience a decrease in sexual desire during perimenopause.
- The failure of a woman to achieve orgasm can be a result of poor sexual technique, concentrating too hard on achievement, or negative attitudes toward sexual relationships.
Treatment
- Treatment includes:
- Administration of androgen (testosterone) may be helpful at that time, because it can improve interest in sexual activity.
- relieving the underlying cause. It may include instruction and counseling for the couple about sexual feelings and needs.
Erectile Dysfunction:
formerly referred to as IMPOTENCE, is the inability of a man to produce or maintain an erection long enough for vaginal penetration or partner satisfaction (Wessells et al., 2007).
Most causes of ED are:
- Physical, such as aging, atherosclerosis, or diabetes, which limit blood supply.
- Side effect of certain drugs.
Examples of drugs prescribed today for ED are: sildenafil (Viagra), tadalafil (Cialis), and vardenafil (Levitra), which are taken up to once a day to stimulate penile erection (Karch, 2009).
Sildenafil Citrate (Viagra) Classification: A phosphodiesterase (PDE) inhibitor. Prescribed as therapy for erectile dysfunction;
Action: Causes smooth muscle relaxation and inflow of blood to the corpus cavernosum of the penis, achieving erection (Karch, 2009) Dosage: 50 mg PO prn 1 hour before sexual activity, up to one dose per day
Possible Adverse Effects:
The most common side effects are headache, facial flushing, and upset stomach.
- Less commonly, ventricular arrhythmia, bluish vision, blurred vision, impairment of blue/green discrimination, or sensitivity to light may briefly occur.
- Advise patients not to take this drug within 4
hours of taking an alpha-blocker agent.
Nursing Implications
Assess patient for pre-existing cardiovascular risk.
- Caution patient that dose should be limited to one time per day; use is contradicted if the patient is taking nitrates or an alpha-blocker.
- Erection lasting more than 4 hours (priapism) can occur. Caution patient to alert health care provider if this occurs to avoid penile tissue damage.
- Caution patients that this drug does not protect against sexually transmitted infections or pregnancy, so the user must continue to use safer sex practices.
- In rare instances, men taking PDE5 inhibitors have reported a sudden decrease or loss of vision.
-Caution patient that if he experiences sudden decrease or loss of vision to stop taking the medication and call a doctor right away.
Alternative Treatment
1. A surgical implant to aid erection by the use of vacuum pressure is a possible alternative (Hossein, 2007).
- Testosterone injections may be helpful in some men.
- In all instances, frank discussion about the cause of the problem and currently available therapies is helpful.
- Various herbal products such as fennel extracts are available for women that may improve sexual libido.
- Vibration or vacuum devices are also available to increase clitoral enlargement and sexual arousal in women.
Premature Ejaculation
is ejaculation before penile-vaginal contact (Docherty, 2007).
- The term also is often used to mean ejaculation
- before the sexual partner's satisfaction has been achieved.
- Premature ejaculation can be unsatisfactory and frustrating for both partners.
- Premature ejaculation occurs in men when semen leave the body (ejaculate) sooner than wanted during sex.
- Premature ejaculation is a common sexual complaint
- As many as 1 out of 3 people say they have it at some time.
- Premature ejaculation isn't cause for concern if it doesn't happen often. But you might be diagnosed with premature ejaculation if you:
- Always or nearly always ejaculate within 1 to 3 minutes of penetration
- Are not able to delay ejaculation during sex all or nearly all the time
- Feel distressed and frustrated, and tend to avoid sexual intimacy as a result
Premature ejaculation can be classified as:
Lifelong PE
occurs all or nearly all the time beginning with the first sexual encounter.
Acquired PE
develops after having previous sexual experiences without problems with ejaculation.
Psychological causes Psychological factors that might play a role include:
- Early sexual experiences
- Sexual abuse
- Poor body image
- Depression
- Worrying about premature ejaculation
- Guilty feelings that can cause you to rush through sex
Other factors that can play a role include:
- Erectile dysfunction.
- Anxiety.
- Relationship problems.
Other reasons suggested are doubt about masculinity and fear of impregnating a partner, which prevent the man from sustaining an erection.
Treatment: Sexual counseling for both partners to reduce stress, as well as serotonergic antidepressants such as Mirtazapine, may be helpful in alleviating the problem.
PERSISTENT SEXUAL AROUSAL SYNDROME
- (PSAS) is excessive and unrelenting sexual arousal in the absence of desire
- is spontaneous, persistent, unwanted and uncontrollable genital arousal in the absence of sexual stimulation or sexual desire, and is typically not relieved by orgasm.
- It may be triggered by medications or psychological factors.
- When assessing someone with the disorder, be certain to ask if the person is taking any herbal remedies such as Ginkgo biloba because some of these can have arousal effects.
PAIN DISORDERS
- Because the reproductive system has a sensitive nerve supply, when pain occurs in response to sexual activities, it can be acute and severe and impair a person's ability to enjoy this segment of their life.
- Vaginismus is involuntary contraction of the muscles at the outlet of the vagina when coitus is attempted that prohibits penile penetration.
Other causes are unknown, but it could also be the result of early learning patterns in which sexual relations were viewed as bad or sinful.
Treatment: sexual or psychological counseling to reduce this response may be necessary.
- Dyspareunia is pain during coitus.
This can occur because of endometriosis (abnormal placement of endometrial tissue)
Symptoms If you have painful intercourse, you might feel:
Pain only at sexual entry (penetration) Pain with every penetration, including putting in a tampon Deep pain during thrusting
Burning pain or aching pain
Throbbing pain, lasting hours after intercourse
Causes:
Physical causes of painful intercourse differ, depending on whether the pain occurs at entry or with deep thrusting.
Emotional factors might be associated with many types of painful intercourse.
Entry pain
Pain during penetration might be associated with a range of factors, including:
- Not enough lubrication. This is often the result of not enough foreplay.
- Certain medications are known to affect sexual desire or arousal, which can decrease lubrication and make sex painful.
- Injury, trauma or irritation.
- Inflammation, infection or skin disorder.
- Vaginismus.
- A problem present at birth. Not having a fully formed vagina (vaginal agenesis) or the development of a membrane that blocks the vaginal opening (imperforate hymen) could cause dyspareunia.
Deep pain
Causes include:
- Certain illnesses and conditions: endometriosis, pelvic inflammatory disease, uterine prolapse, retroverted uterus, uterine fibroids, cystitis, irritable bowel syndrome, pelvic floor dysfunction, adenomyosis, hemorrhoids and ovarian cysts.
- Surgeries or medical treatments. Scarring from pelvic surgery, including hysterectomy, can cause painful
intercourse. Medical treatments for cancer, such as radiation and chemotherapy, can cause changes that make sex painful.
- Emotional factors
- Psychological issues. -Anxiety, depression, concerns about your physical appearance, fear of intimacy or relationship problems can contribute to a low level of arousal and a resulting discomfort or pain.
- Stress.
History of sexual abuse.
It can be difficult to tell whether emotional factors are associated with dyspareunia.
Initial pain can lead to fear of recurring
pain, making it difficult to relax, which can lead to more pain. You might start avoiding sex if you associate it with the pain.
- Vestibulitis (inflammation of the vestibule), vaginal infection, or hormonal changes such as those that occur with menopause and cause vaginal drying. A psychological component may be present.
- Vulvar vestibulitis, also known as VVS, is a type of vulvodynia, or pain around the vulva -- the sex organs outside a woman's body.
- The pain is in your vestibule, the part of your vulva around the opening of your vagina.
- it can be aggravated by acid foods in the diet, by low levels of estrogen hormone, and by any infections that happen to occur while it is there. At the same time, it seems that many treatments bring about at least some relief in some women.
- Treatment: is aimed at the underlying cause. Encouraging open communication between sexual partners can be instrumental in resolving the problem.
MENSTRUATION
Definition of Terms
MENSTRUATION
a periodic discharge of blood, mucus and epithelia cell from the uterus.
MENSTRUAL CYCLE
is a beginning of menstruation to the beginning of the next menstruation
MENARCHE
is the first menstruation in women
DYSMENORRHEA
is a severe pain during menstruation
METRORRHAGIA
complete bleeding at completely irregular interval
MENORRHAGIA
excessive bleeding during menstruation
AMENORRHEA
absence of menstruation leading to pregnancy
MENOPAUSE
end of menstruation/cessation of menstruation
- The mean age for menarche is 12.87 years or 1-3 years after breast budding.
- Pregnancy can occur from the very first menstrual cycle.
- Menses is actually the end of an arbitrary defined menstrual cycle.
- The menstrual phase varies in length for most women.
- Average period: 5 days
- Average cycle 28 days
- Normal Blood Loss: 50 cc
Four Body Structures Involved In Physiology Of Menstrual Cycle
For menstrual cycle to be complete, all four structures must contribute their part Therefore, inactivity of any parts results in an incomplete or ineffective cycle.
- Hypothalamus
- Pituitary gland
- Ovaries
- Uterus
Interplay of 4 Major Organs
HYPOTHALAMUS:
Produces GnRH or Gonadotropin Releasing Hormone to stimulate the anterior Pituitary gland.
ANTERIOR PITUITARY GLAND:
Secretes Gonadotropins (FSH and LH): stimulates the ovary (estrogen and progesterone)- if estrogen/progesterone increase in blood vessels, this gives positive feedback to the hypothalamus to decrease all hormones.
OVARIES
After an upsurge of LH, the graafian follicle raptures and the ovum is set free from the ovary, called ovulation and swept into an open end of a fallopian tube, the FSH has done its work and now decreases its amount. it occurs approximately on the 14" day before the onset of the next menstrual cycle. Because ovulation happens at the midpoint of a 28-day cycle.
Example: if the cycle is only 20 days long 20-14=6 day of ovulation not the 10TH or middle day
UTERUS
If conception occurs, the fertilized ovum implants on the endometrium of the uterus in the corpus luteum remains throughout
Menstrual flow is composed of:
- Blood from ruptured capillaries
- Mucin from the glands
- Fragments of the endometrial tissue
- The microscopic, atrophied, unfertilized ovum.
Indications of Ovulation
- There is slight drop in temperature one day prior to ovulation with a ½ to 1 degree rise in temperature at ovulation that remains elevated for 12-14 days.
- Cervical mucus is abundant, watery, clear and more alkaline, Cervical of dilates slightly, softens and rises in the vagina.
- Presence of Spinnbarkeit (egg-white stretchiness of cervical mucus) and Ferning under microscope
Description: Menstrual Cycle is Composed of Four phases
- The menstrual cycle is the monthly hormonal
cycle a female’s body goes through to prepare for
pregnancy.
- Your menstrual cycle is counted from the first day of your period up to the first day of your next period. Your hormone levels (estrogen and progesterone) usually change throughout the menstrual cycle and can cause menstrual symptoms.
The four main phases of the menstrual cycle are:
- MENSTRUATION
- FOLLICULAR PHASE
- OVULATION
- LUTEAL PHASE
MENSTRUATION
- Menstruation is the elimination of the thickened lining of the uterus (endometrium) from the body through the vagina.
- Menstrual fluid contains blood, cells from the lining of the uterus (endometrial cells) and mucus.
- The average length of a period Is between three days and one week.
If conception does not occur, the unfertilized ovum trophies after 4 days: and the corpus luteum remain for only 8- 10 days and regresses. stimulation from the hormones produced by the ovaries causes specific monthly effects on the uterus and uterine changes occur during the menstrual cycle.
PROLIFERATIVE OR FOLLICULAR PHASE
- starts on the first day of menstruation and ends with ovulation.
- Prompted by the HPT, the pituitary gland releases follicle stimulating hormone (FSH).
- stimulates the ovary to produce around five to 20 follicles (tiny nodules / cysts), which bead on the surface.
- Each follicle houses an immature egg. Usually, only 1 follicle will mature into an egg, while the others die.
- This can occur around day 10 of a 28-day cycle.
- The growth of the follicles stimulates the lining of the uterus to thicken in preparation for possible pregnancy
OVULATION
- release of a mature egg from the surface of the ovary.
- usually occurs mid-cycle, around two weeks or so before menstruation starts.
- During the follicular phase, the developing follicle causes a rise in the level of oestrogen. The HPT in the brain recognises these rising levels and releases a chemical called gonadotrophin-releasing hormone (GnRH).
- This hormone prompts the pituitary gland to produce raised levels of luteinising hormone (LH) and FSH. Within two days, ovulation is triggered by the high levels of LH. The egg is funneled into the fallopian tube and toward the uterus by waves of small, hair-likeprojections.
- The life span of the typical egg is only around 24 hours. Unless it meets a sperm during this time, it will die.
- If a fertilized egg implants in the lining of the uterus, it produces the hormones that are necessary to maintain the corpus luteum. This includes human chorionic gonadotrophin (HCG), the hormone that is detected in a urine test forpregnancy.
- The corpus luteum keeps producing the raised levels of progesterone that are needed to maintain the thickened lining of the uterus.
- If pregnancy does not occur, the corpus luteum withers and dies, usually around day 22 in a 28- day cycle.
- The drop in progesterone levels causes the lining of the uterus to fall away. This is known as menstruation. The cycle then repeats.
LUTEAL PHASE
During ovulation, the egg bursts from its follicle, but the ruptured follicle stays on the surface of the ovary. For the next two weeks or so, the follicle
transforms into a structure known as the corpus luteum. This structure starts releasing
along with small amounts of combination of hormones maintains the thickened lining of the uterus, waiting for a fertilized egg to implant.
MENSTRUAL PHASE -Days 1-5 cycle.
- Shedding of the endometrium occurs as uterine bleeding, approximately 50 to 60 mi (<2 ounces).
- PROLIFERATIVE (FOLLICULAR) PHASE -Day 5 of
ovulation.
Endometrium is restored under primary hormone influence of estrogen. In this preovulatory phase, FSH Is secreted by the anterior pituitary. Preovulatory surge of LH affects one follicle and ovulation occurs.
- SECRETORY PHASE -(OVULATION) Ovulation to
Approximately 3 days before menstrual cycle. Estrogen Levels off and progesterone level increase
ISCHEMIC PHASE -(LUTEAL)
If fertilization did not occur, The corpus luteum degenerates and estrogen and progesterone levels drop off causing the endometrium to become “blood starved” leading to menstruation.
2 common causes of irregular menstrual periods are:
polycystic ovary syndrome (PCOS)
- hypothyroidism
* PCOS is a hormone imbalance that can affect ovulation, and make it more difficult to get pregnant.
Estrogen: female hormone that is produced by the ovaries. Tt helps control and guide sexual development, including the physical changes. associated with puberty.
Progesterone a hormone that helps to regulate your cycle. But its main function is to help thicken the lining of the uterus to prepare for a fertilized egg.
The Menstrual Cycle
The menstrual cycle is the hormonal process a woman's body goes through each month to prepare for a possible pregnancy.
Regular menstrual periods in the years between puberty and menopause are usually a sign that your body is working normally.
RESPONSIBLE PARENTHOOD
RESPONSIBLE PERSON
a man or woman who is able and willing to give the proper response to the demands of given situation with specific reference to marriage and family life.
RESPONSIBLE SPOUSE
one who gives the proper responses to the needs of his/ her spouse, as well
As his own, and of their life together
RESPONSIBLE PARENTS give proper responses to the needs of their children.
Family Planning
Refers more specifically to the voluntary and positive action of a couple to plan and decide the number of children they want to have and when to have them.
Reproductive Life Planning Includes all decisions an individual or couple make about having children:
- If and when to have children
- How many children to have
- How children are spaced
The concept of family planning includes these elements:
- Responsibility of parents to themselves and to each other
- Responsibility to their present and future children
- Responsibility to their community and count
Purposes of Family Planning
- Improvement of health
- Promotion of human right to determine reproductive performance
- Relation of demographic change to economic development
The Ultimate Goal of Family Planning is directed towards:
- Birth spacing, to allow the mothers time to rest and regain their health before the next pregnancy
- Birth limitation, when the desired number of children is reached
- Helping those who do not have children to have children
Advantages of Family Planning To the mother:
- Enables the mother to regain her health after the delivery
- Gives mother enough time and opportunity to love and provide attention to her husband and children
- Provides mother who has chronic illness enough time for treatment and recovery without further exposure to the physiologic burden of pregnancy
- Prevents high risk pregnancy
- Gives mother more time to herself, family and community
To the children
The practice of family planning will make that healthier, happier, feel wanted and satisfied, secure
To the fathers
- Lightens his burden and responsibility in supporting his family
- Enables him to give his children a good home,
good education and better future
- Enables him to give his family a happy and contented life
- Gives him time for his personal advancement
- Provides a father who has chronic illness enough time for treatment and recovery from his illness
To the family:
- Gives the family members more opportunity to enjoy each other’s company with love and affection
- Enables the family to save some amount for improvement of standard of living and for emergencies
To the community
- Improves the economic and social status of the community
- Better job opportunities
- Health status will improve
- Extra resources in the community (less congestion, less pollution, potable water supply, etc)
- Members will have more time to socialize with each other; to participate in socio-civic activities.
CONTRACEPTION
Is any device used to prevent fertilization of an egg leading to pregnancy.
The Considerations are:
- Personal values
- Ability to use method correctly
- How method will affect sexual enjoyment
- Financial factors
S. Status of couple's relationship
- Prior experiences
- Future plans
- Contraindications
Kinds of Contraceptives
NATURAL METHODS
a. rhythm method or calendar method
HORMONAL METHODS
- oral contraceptives
- injected or implanted steroidal contraceptive
BARRIER METHODS
- CHEMICAL BARRIERS
- Spermicides
- Gels
- Vaginal suppositories
- Sponges
- MECHANICAL BARRIERS
- Condoms
- Cervical cap
- Diaphragm
- Intrauterine device / IUD
- CHEMICAL BARRIERS
CALENDAR/ RHYTHM
Teaching;
Entails keeping a day-by-day record of your cycle for 6 consecutive months, noting the onset of bleeding as day 1 and the last day before your next menstrual bleeding as the final day of your cycle.
First unsafe day: subtract 18 from the
number of days in Last unsafe day:
subtract 11 from the number of days in your longest cycle.
Ex: shortest: 26 - 18 = day 8
longest: 31-11 = day 20
UNSAFE PERIOD! Days 8 -20, avoid coitus or use a contraceptive during this period.
This 6 month record will show you your longest and shortest cycles- from which you can calculate your FERTILE days
Life span of an egg from the woman lives for only around 24 hours
Sperm from the man can survive for up to 3 days, possibly longer.
COITUS INTERRUPTUS
Is a periodic abstinence from intercourse during fertile period: based on the regularity of ovulation: variable effectiveness. The oldest method.
Couple proceeds with coitus until the moment of ejaculation, then the man withdraws and spermatozoa are emitted outside the vagina.
Offers little protection because ejaculation may occur before withdrawal is complete and despite the care used, spermatozoa may be deposited in the vagina
BASAL BODY TEMPERATURE
Involves taking the temperature every morning BEFORE the woman gets out of bed and recording it.
The temperature drops slightly 24 hours before ovulation, then rises to about half a degree higher than normal and remains thus for up to three days: UNSAFE period!
Not a very efficient method unless combines with calendar and mucus methods. there are factors that
affect BBT: Sore throat, cold, flu, fever, toothache, vomiting, diarrhea,
Anxiety, medications, travel, sleep disturbance, alcoholic beverages.
CERVICAL MUCUS BILLINGS METHOD
Involves becoming aware of the normal changes in the cervical secretions that occur throughout your cycle by inserting the forefinger into the vagina first thing in the morning. A few days after menstrual bleeding, there is little secretion, vagina is dry and gradually, secretion increases and becomes thicker, cloudy white and sticky.
As ovulation approaches, this secretion or mucus becomes copious. clear, thin, less viscous, more liquid, slippery or stringy: as soon as this change begins and for
3 full days later: UNSAFE PERIOD How to check
- Begin checking the mucus:
when the menstrual bleeding ends or becomes light enough for you to be able to see mucus, if there is no prior sexual Intercourse and if a woman is not sexually stimulated
Checking the sensation of wetness or dryness:
While standing, Inspect underwear regularly for the presence of mucus, wipe with the middle or index finger and the thumb test for the consistency. slipperiness, stretchiness of the mucus. Observe also its color
Cervical Changes
- Spinnbarkeit test
Cervical mucus is thin, watery and can be stretched into long strands means there is high level of estrogen and ovulation is about to occur,
Ferning or arborization of cervical mucus
At the height of estrogen stimulation just before ovulation. Ferning is due to crystallization of sodium chloride on mucus fibers.
Client Instructions:
During fertile period - mucus is abundant, slippery, watery, thin and stretchable. It has a ferning pattern when viewed under the microscope. As soon as you notice changes in your mucus, consider yourself fertile. Avoid sexual intercourse.
During infertile period - mucus is thick, scant, yellowish or absent, Sexual intercourse is allowed.
SYMPTO - THERMAL METHOD
Combines BBT and cervical mucus methods. The woman takes her temperature daily, watching for the rise in tem that marks ovulation. She also analyzes her cervical mucus daily:
Abstain from intercourse until 3 days after the rise in temperature or the fourth day after the peak of mucus change.
When the baby sucks the breast & nipple, the!
nerves in the mothers’ breast send messages to the brain. The greater the frequency & duration of sucking the more pronounced the suppression of ovulation due to constant secretion of prolactin.
Thus, when a woman breastfeeds her baby she is unlikely to ovulate.
98 % effective when all the following conditions are present if she is fully breastfeeding,
amenorrheic and within 6 months’ postpartum
period.
LACTATION AMENORRHEA METHOD
As long as a woman is breastfeeding an infant, there is some natural suppression of ovulation. Not dependable- woman may be fertile even if she has not had a period since childbirth.
After 6 months, she should use another ~ method of contraception.
The effectivity of this method is greatly dependent on the frequency & duration of, sucking.
HORMONAL METHODS
ORAL CONTRACEPTIVES
Composed of varying amounts of estrogen combined with small amount of progesterone. 99% effective. Estrogen suppresses FSH and LH, thereby suppressing ovulation. Progesterone decreases the permeability of cervical mucus
Effects on the cervical mucus
The pill makes the cervical mucus thick, scanty & cellular so that sperms have difficulty in penetrating it & reaching the uterus. Prevention of implantation due to the effect of progestin on the endometrium.
Effects on the sperm
Capacitation, the activation of enzymes that permit the sperm to penetrate the ovum, maybe inhibited. This makes the sperm unable to penetrate and fertilize the ovum.
Types of Oral Contraceptives
- MONOPHASIC Fixed doses of estrogen and progesterone: 21-28 day cycle.
The preparation may come w/ 21 tablets thus with a seven day pill free interval/ seven iron/ vitamin tablets substituted for that interval.
Safe & effective and are close to100% (98%), effective but the actual rate is lower because of poor compliance in women.
- BIPHASIC There is constant amount of —
estrogen with increased progesterone
- TRIPHASIC Varying levels of estrogen and progesterone
Benefits of Oral Contraceptives are: Decreased incidences of:
- Dysmenorrhea
- Premenstrual dysphoric syndrome
- Iron deficiency anemia
- Acute PID with tubal scarring
- Endometrial and ovarian cancer
- and ovarian cysts
- Fibrocystic breast disease
Side Effects
Nausea,weight gain, headache, breast tenderness, breakthrough bleeding, monilial vaginal infections, mild hypertension, Depression
Absolute Contraindications to OC's
Breastfeeding, family history of CVA or CAD, history of thromboembolic disease, history of liver disease, Undiagnosed vaginal bleed
Possible Contraindications to OC's
- Age 40+
- Breast or reproductive tract malignancy
- Diabetes Mellitus
- Elevated cholesterol or triglycerides
- High blood pressure
- Migraine or other vascular type headaches
- Obesity
- Pregnancy
- Seizure disorders
- Sickle cell or other hemoglobinopathies
- smoking
- Use of drug with interaction effec
Other Contraceptives
- Continuous or extended regimen pills
- Estrogen-progesterone patch
- Vaginal rings
ESTROGEN-PROGESTERONE PATCH
Highly effective, weekly hormonal birth control patch that’s worn on the skin. Combination of estrogen and progestin. It is absorbed on the skin and then transferred into the bloodstream. Can be worn on the upper outer arm, buttocks, upper torso or abdomen. Worn for 1 week, replaced on the
same day of the week for 3 consecutive weeks. No patch-4* week.
EMERGENCY POSTCOITAL CONTRACEPTIVES
The "Morning-after pills”. High level of estrogen. Must be initiated within 72 hours of unprotected intercourse.
How to take the pill:
Take 1 pill every day, always start your pill on the day one of your menstruation. Those taking a 2iday pill have a 7day pill free period then start taking the ist pill om the next pack. For the 28 day pill start the next day after all 28 pills have been taken. There is no pill free.
SUBCUTANEOUS IMPLANTS (eg, Norplant)
6 nonbiodegradable Silastic implants with synthetic progesterone embedded under the skin on the inside of the upper arm.
Slowly release the hormone over the next 5 years.
Suppress ovulation, stimulating thick cervical mucus and changing the endometrium so implantation is difficult.
INTRAMUSCULAR INJECTIONS
Administered every12weeks,and contain Medroxy progesterone (depo provera). 100% effective.
Advantages
- Highly effective (99.6%)
- Safe, convenient, easy to use
- Can be used by breast feeding
- mothers
- Does not interfere w/ intercourse.
- Easily administered by non ~ physician
- Does not contain estrogen, so that the
- heart & blood- clotting effects do not occur.
- Rapidly effective
Disadvantages
- Menstrual irregularities maybe experienced.
- Weight gain in some women due to increase in appetite
MECHANICAL BARRIER
INTRAUTERINE DEVICES
A T-shaped plastic device with copper. With progesterone.
Must be fitted by physician, nurse practitioner or midwife, Insertion is performed in ambulatory setting after pelvic examination and pap smear. Device is contained within uterus with a string protrudes into vagina. Effective for 5-7 years (mirena typ.e) or 8 years (Copper T380).
Mechanism of Action
- Inactivating the sperm due to the action of the copper.
- interfering w/ the transport of sperm in the genital tract due to the production of
- Seeding the ovum's transport through the wife become pregnant immediately
fallopian tubes. 3. Inexpensive: it can be used for & Effectiveness: 98-99
Precautions: The IUD should not be given to women w/ pregnancy, active recent/recurrent pelvic infections.
Advantages
- Very low pregnancy rate, thus it is very effective
- Easy to remove if couple wants
- prostaglandin & enzymes. another child.
- Once IUD remove, wife become pregnant easily
- Only requires yearly check-up to make sure the IUD is still in place.
- Creates no mess.
Disadvantages
- Client may feel slight pain during the 1few days after an IUD insertion
- The IUD maybe expelled
- Clients may not protected from STDs Side Effects:
Spotting or uterine cramping, Increased risk
for PID; heavier menstrual flow, dysmenorrhea and ectopic pregnancy
Other Barrier Methods Spermicidal products
- Diaphragms
- Cervical caps
- Condoms
SPERMICIDAL AGENT
Goal: to kill the sperm before the sperm enters the cervix
Nonoxynol-9 made up of Gel, creams, films, foams, suppositories, It is 82 % effective.
Advantages
Safe to use, protection against STDs Disadvantages
Need to use for every act of coitus, messy & sometimes _ irritating, temporary skin irritations to the vulva/ penis caused by sensitivity.
Precautions
Hypersensitivity to the spermicidal foam, jelly, cream/ tablets
Diaphragm
Mechanically blocks sperm from entering the cervix soft latex dome supported by a metal rim can be inserted 2 hours before
intercourse; removed at least 6 hours after coitus or within 24 hours. size must fit the individual, washable, may be used for 2-3 years.
Cervical cap
similar to diaphragm but smaller thimble- shaped rubber cap held onto the cervix by suction.
Male condom
Is widely used method both in developing & developed countries. Mechanical barriers covering the penis had been used for protection against pregnancy.
Mechanism of action
Condom is a rubber sheath worn over an erect penis during sexual intercourse. It acts as barrier that blocks the man’s sperm from entering the vagina in order to prevent pregnancy
Effectiveness
85-87%
Advantages:
No serious side effects no prescription. Encourage male participation in contraception
Disadvantages:
- Decrease sensation
- New condom should be used for each act of coitus
- Sexual activity is interrupted Precaution
- Couples who are allergic to rubber
- Men who cannot maintain erection while using condom
Instruction
- Put the condom on the erect penis
- Condom can tear, so be careful with them
- Leave % inch of empty space at the tip of the condom
- Wait until the vagina is well lubricated, because a condom can tear if the vagina is dry
- If extra lubrication is needed, use water, ky jelly, gel. cream
- After ejaculation while the penis is still erect, hold on to the rim of the condom & withdraw the penis immediately.
- Check condom for tears, then throw It away.
Surgical Methods
TUBAL LIGATION
28%oF all women in US. Fallopian tubes are cut, tied/ cauterized to block passage of ova and sperm.
Laparoscopy is the procedure to perform tubal sterilization.
Advantages
- Very effective & safe
- No long term side effect
- Does not interrupt sexual activity
- Permanent method
- Does not interfere w/ sexual activity Disadvantages
- Discomfort during & shortly after the procedure
- Discomfort of serious bleeding injury to internal organs/ infection soon after the procedure.
- irreversible
VASECTOMY
Almost 11% of all men in US. Incisions are made in the sides of scrotum: vas deferens is cut and tied. Then plugged or cauterized. IT blocks the passage of sperm. The sperm is viable for 6 months post op.
It is
reversible 95%. Advantages
- Very effective (99.5-99:9%) safe procedure
- No long term side effect
- Does not interfere w/ sexual activity
Disadvantage
The client feel some discomfort during & shortly after the procedure.
Complications
There is scrotal swelling discoloration, discomfort & pain, hematomas, wound infection
PREGNANCY-ANTEPARTUM
Pregnancy-Antepartum
Refers to the medical and nursing care given to the pregnant woman between conception and the onset of labor.
Consideration is given to the physical, emotional, and social needs of the woman, the unborn child, her partner, and other family members.
Classification of Pregnancy Terminologies
GESTATION: The process of carrying or being carried in the womb between conception and birth
VIABILITY: is the ability of a fetus to survive outside of the womb at the end of 20 weeks
GRAVIDA: is the number of times pregnant, regardless of duration and outcome, including the present pregnancy.
NULLIGRAVIDA: is a Woman who has not and never has been pregnant
PRIMIGRAVIDA: is a woman pregnant for the first time.
MULTIGRAVIDA : is a pregnant for second or subsequent time.
PARA: is the number of pregnancies that lasted more than 20 weeks, regardless of outcome.
NULLIPARA: is a woman who has not given birth to a baby beyond 20 weeks gestation.
PRIMIPARA: is a woman who has given birth to one baby more than 20 weeks gestation.
MULTIPARA : is a woman who has had two or more births at more than 20 weeks gestation.
TPAL: Para is subdivided to reflect births that went to Term, Premature births, Abortions, and Living children.
PRETERM: is a newborn born before 37 weeks of gestation,
TERM: is a newborn born after 37 weeks to 40 weeks of gestation.
POST TERM: is a newborn born after 40 weeks
LMP: Last Menstrual Period
EDC: refers to the Expected Date of Delivery/ confinement
AOG : is the Age of Gestation
CIL: refers to the Cephalic in Labor
Duration of pregnancy
The duration of pregnancy is 266-280 days, 38-42 weeks, 9 calendar months, 10 lunar months
(28 days).
Periods of Pregnancy
First Trimester: period of organogenesis; teratagens are highly damaging.
SECOND TRIMESTER: most comfortable period for the mother, fetal growth continues.
THIRD TRIMESTER:
rapid deposition of fats, thus period of most rapid growth, with rapid iron and calcium deposition
Conditions for Fertilization
Postcoital test demonstrates:
- Live, motile, normal sperm present in cervical mucus.
- Fallopian tubes patent.
- Endometrial biopsy indicates adequate progesterone and secretory endometrium.
- Semen is supportive to pregnancy at least 2 ml semen and contain at least 20million sperm/ml; >60 % normal and > 50 % motile (moving forward).
Process of Reproduction
Procreation
The production of offspring; in general humans copulate purely for the purpose of procreation
Related theories
There are two main theories:
Creation - God created the world and all that's in it, including humans, and they reproduce through sexual intercourse.
Evolution - Darwin's theory that humans evolved over the years through natural occurrences and from the growth and development of monkeys and other creatures.
FERTILIZATION
A SPERM AND AN EGG FORM A ZYGOTE
- During sexual intercourse, some sperm ejaculated from the male penis swim up through the female vagina and uterus toward an oocyte (egg cell) floating in one of the uterine tubes.
- Fertilization takes place in ampula (outer 1/3) portion of the Fallopian tube.
- The sperm and the egg are gametes.
They each contain half the genetic information necessary for reproduction. When a sperm cell penetrates and fertilizes an egg, that genetic information combines.
- The 23 chromosomes from the sperm pair with 23 chromosomes in the egg, forming a 46- chromosome cell called a zygote.
- The zygote starts to divide and multiply. As it travels toward the uterus it divides to become a blastocyst, which will burrow into the uterine wall.
IMPLANTATION
The Zygote Becomes an Embryo: Development Prior to and During Implantation
- A fertilized egg, or zygote, takes about 5 days to reach the uterus from the uterine tube. As it moves, the zygote divides and develops into a blastocyst, with an inner mass of cells and a protective outer ring.
- The blastocyst attaches to the wall of the uterus and gradually implants itself into the uterine lining.
- During implantation, its cells differentiate further. At day 15 after conception, the cells that will form the embryo become an embryonic disc.
- Other cells begin to form support structures.
- The yolk sac, on one side of the disc, will become part of the digestive tract.
- As the cells multiply, they will also separate into two distinctive masses:
- the outer cells will eventually become the placenta and umbilical cord, which will bring in nutrients and eliminate waste
- the inner cells form the embryo.
- On the other side, the amnion fills with fluid and will surround the embryo as it develops.
By week 4, the embryo has a distinct head and tail and a beating heart.
Over the next 6 weeks, limbs, eyes, brain regions, and vertebrae form. Primitive versions of all body systems appear.
In 8 Weeks, the Embryo Develops. The embryo contains a flat embryonic disc that now differentiates into three layers: The Endoderm, Mesoderm and the Ectoderm.
Note: Pregnancy is often measured in terms of gestational age—age of the fetus starting with the first day of a woman's last menstrual period—and embryonic or fetal age—actual age of the growing fetus. We are referring to the gestational age of the fetus.)
By the end of 10th week of pregnancy,
your baby will change names from an embryo to a fetus, There are about 40 weeks to a typical pregnancy. These weeks are divided into three trimesters.
STAGES OF FETAL DEVELOPMENT
Ovum - From ovulation to fertilization
Zygote - (12-14 days after Fertilization)-from the time the ovum is fertilized until it is implanted in the uterus.
Embryo - from implantation to 5-8 weeks. During this period, embryo is most vulnerable to teratogens: viruses, drugs, radiation or infection can cause major congenital anomalies.
Fetus - 8- 10 weeks until term (38-41 weeks).
Conceptus is the developing embryo or fetus and placental structures throughout pregnancy.
Age of viability the earliest age at which fetuses could survive if they were born at that time, generally accepted as 24 weeks, or fetuses.
During intra uterine life the fetus derives O2 and excrete carbon dioxide, not from 02 exchange in the lungs but from the placenta. Fetal circulation differs from extra-uterine circulation in several
SPECIAL STRUCTURE IN FETAL DEVELOPMENT
The fetus is connected by the umbilical cord to the placenta, the organ that develops and implants in the mother’s uterus during pregnancy.
Through the blood vessels in the umbilical cord,
the fetus receives all the necessary nutrition, oxygen, and life support from the mother thru placenta
Circulating blood bypasses the lungs and liver by flowing in different pathways and through special openings called shunts.
Placenta- where the gas exchange takes place during fetal life
Umbilical arteries- carry unoxygenated blood from the fetus to the placenta
Umbilical vein- brings oxygenated bloodcoming from the placenta to the fetus.
Foramen ovale- connects the left and the right atrium. It pushes blood from the right atrium to the left atrium so that blood can supplied to brain, kidney and heart,
Ductus venosus- carry oxygenated blood from umbilical vein to vena cava, by passing fetal liver. (vein to vein)
Ductus arteriosus- carry unoxygenated blood from pulmonary artery to aorta, by passing
(artery to artery) FETAL CIRCULATION
- The oxygenated blood enters the umbilical vein from the placenta. (direction of blood is toward the fetal heart).
- Enters ductus venosus that connects the umbilical vein to the inferior vena cava, w/c allows oxygenated blood to be supplied directly to the fetal liver.
- It passes through inferior venacava,
- enters the right atrium (heart),
- enters the foramen ovale (opening bet. rt.
- atrium and left atrium.)
- Goes to the left atrium
- passes through the left ventricle
- flows to ascending aorta to supply nourishment to the brain and upper extremities.
- It enters superior venacava (return to the heart), goes to the right atrium.
- enters the right ventricle,
- enters pulmonary artery with some blood going to the lungs to supply oxygen and nourishment.
- It flows to ductus arteriosus (channel bet. aorta and main pulmonary artery. Allows blood to bypass the fetal lung. It closes during normal respiration
- It enters descending aorta (some blood going to the lower extremities) and enters hypogastric arteries that return the blood to the placenta (unoxygenated blood because it is away from the fetal heart)
- and goes back to the placenta.
MATERNAL CHANGES
- During pregnancy, the pregnant mother under significant anatomical and physiological changes in order to nurture and accommodate the developing fetus.
- These changes begin after conception and affect every organ system in the body. These changes resolve after pregnancy with minimal residual effects.
- It is important to understand the normal physiological changes occurring in pregnancy
Maternal Changes (8 weeks AOG)
- Nausea persists up to 12 weeks.
- Uterus changes from pear to globular shape
- Hegar's sign: softening of the isthmus of cervix
- Goodell's sign: softening of the cervix
- Leukorrhea increases
- Ambivalence about pregnancy may occur
- No noticeable weight gain
- Chadwick's sign appears (dark bluish or purplish) appears as early as 4 weeks
Fetal Development (8 weeks AOG)
- Rapid development.
- Heart begins to pump blood.
- Limb buds are well developed.
- Facial features discernible.
- Major divisions of brain discernible.
- Ears develop from skin folds.
- Tiny muscles are formed beneath this skin
- embryo Weighs 2 grams.
Ectoderm: Skin and nervous system Endoderm: Digestive and respiratory Systems
Mesoderm: Muscle and skeletal systems; all organs of the human body derive from these three tissues. They begin to curve and fold and to form an oblong body.
Nursing Interventions (8 weeks AOG)
- Teach prevention of nausea:
- Eat dry crackers before getting out of bed in the morning.
- Eat small, frequent meals and avoid fatty foods.
- Increase fluid intake to 3L/day,
- Teach safety:
- Avoid hot tubs, saunas, and steam rooms throughout pregnancy (hypotension may cause fainting).
- Prepare for pregnancy:
- Discuss attitudes toward pregnancy.
- Discuss value of early pregnancy classes that focus on what to expect during pregnancy.
- Provide information about childbirth preparation classes
- Include father/family in preparation for childbirth (Expectant fathers experience eager for delivery experienced by the expectant mother).
Maternal Changes (28 weeks AOG)
- Fundus halfway between umbilicus and
- xiphoid process.
- Thoracic breathing replaces abdominal breathing.
- Fetal outline palpable.
- Woman becomes tired of pregnancy and eager for delivery
- Heartburn may begin
- Hemorrhoids may develop.
Fetal Development ( 28 weeks AOG)
- Fetus can breathe, shallow, regulate temperature.
- Surfactant forms in lungs.
- Fetus is 2/3 birth size
- Baby can hear.
- Eyelids open.
- Period of greatest fetal weight gain begins.
- Fetus weighs 1100 gms (21/2 Ibs).
Nursing Interventions (28 weeks AOG)
Treatment for Hemorrhoids:
Sit'z bath
- Gentle reinsertion of hemorrhoids with lubricated fingertip.
- Suppositories as ordered.
- Topical anesthetic agents.
- Stool softeners as ordered.
Teach comfort measures:
- Elevate legs when sitting.
- Assume side-lying position when resting
Maternal Changes (32 weeks AOG)
- Fundus reaches xiphoid process.
- Breast full and tender.
- Urinary frequency returns.
- Swollen ankles may occur.
- Sleeping problems may develop.
- Dyspnea may develop.
Teach measures to avoid heartburn:
- Eat small frequent meals.
- Avoid fatty foods.
- Avoid lying down after meals.
- Maalox or Mylanta may be helpful.
- Avoid sodium bicarbonate.
Prepare for delivery and parenthood:
- Discuss mother’s/father’s/family expectations of
labor and delivery.
- Discuss mother’s/father’s/family expectations of
caring for infant.
- Start childbirth preparation classes.
Fetal Development (32weeks AOG)
- Brown fat develop beneath skin to insulate baby following birth
- Fetus is 15-17 inches in length energy.
- Begins storing iron, calcium and phosphorous.
- Fetus weighs 1800-2200 gms (4-5 Ibs).
Maternal Changes (38 weeks AOG)
- Lightening occurs.
- Placenta weighs approximately 20 oz.
- Mother eager for birth, may have burst of
- Backaches increases
- Urinary frequency increases.
- Braxton Hick’s contractions intensify (cervix and
- lower uterine segment prepare for labor
Fetal Development (38 weeks AOG) Fetus occupies entire uterus; activity is restricted.
Maternal antibodies are transferred to fetus (provides immunity for approximately 6 months, until infant’s own immune system can take over).
Fetus weighs 3200 gms. and more (7 Ibs.).
Nursing Interventions (38 weeks AOG)
Teach safety measures:
Wear low-heeled shoes or flats. Avoid heavy lifting.
Sleep on side to relieve bladder pressure; urinate frequently.
Prepare for delivery:
Continue pelvic tilt exercises. Pack a suitcase for delivery. Fundus reaches xiphoid process. Breast full and tender.
Urinary frequency returns. Swollen ankles may occur. Sleeping problems may develop. Dyspnea may develop.
Nursing Care
Ankle edema is probably caused by reduced blood circulation due to uterine pressure and gen fluid retention.
Management
- Sitting with your feet elevated.
- Resting in left side lying position.
- Avoid standing for long periods of time
- Avoid using restrictive garments on the Backache to maintain balance that may lead to backache (lumbar —_lordosis) or the “pride of pregnancy.”
Management
Apply local heat
Avoid long periods of standing.
Advise to squat rather than bent to pick up objects. Wear low-heeled shoes.
Maintain correct posture. Used of firm mattress
Tailor sitting, pelvic rocking and shoulder circling exercises to strengthen back.
Acetaminophen (Tylenol) in usual adult dose may help.
Breast tenderness
Management
Wear supportive bra with a wide shoulder strap Decrease the amount of caffeine and carbonated beverages instead
Heartburn
is due to increase progesterone that slows gastric motility
Management
Eat small, frequent meals each day.
Avoid overeating as well as spicy, fatty and fried foods.
Constipation
As the weight of the growing uterus presses against the bowel that slows down the peristalsis and also due to increase progesterone level.
Management:
Increase fiber in your diet drink additional fluids.
Have inhibits gastric motility a regular time for bowel movements.
Exercise and use stool softener as prescribed. Enema is contraindicated
Difficulty sleeping
A pregnant women experiencing difficulty in sleeping due to enlarged abdomen that compresses the diaphragm.
Management
Drink a warm caffeine-free drink before bedtime. and practice relaxation techniques.
Fatigue
Fatigue is a feeling of constant tiredness or weakness and cat
physical, mental or a combination of both.
Management
Schedule rest periods daily.
Have a regular bedtime routine and use extra pillow for comfort
Faintness
Management Move slowly. Avoid crowds.
Remain in a cool environment,
Always lie on your left side when at rest.
Headache
Is due to expanding blood volume which put pressure on cerebral arteries.
Management
Avoid eye strain. Visit your eye doctor. Rest with a cool cloth on your forehead, and report immediately on persistent headaches to your primary care provider.
Heartburn
is due to increase progesterone that slows gastric motility
Management
Eat small, frequent meals each day.
Avoid overeating as well as spicy, fatty and fried foods.
Ptyalism
Ptyalism is a condition that causes the overproduction of saliva.
Is due to hyperacidity that increases salivation
Management
Use mouthwash as needed. Chew gum or suck on hard candy.
Brush and floss daily, Watch your diet
Round ligament pain/ Abdominal discomfort Round ligament pain is an uncomfortable sensation in the abdomen near the hips or into the groin area
Management
Avoid twisting motions
Rise to a standing position slowly and use your hands to support the abdomen
Bend forward to relieve discomfort.
Rest and yoga exercises may help, and you may want to sudden movements.
Shortness of breath
due to compression in the diaphgram related to growing fetus
Management
Use proper posture.
Use pillows behind the head and shoulders at night.
Adequate rest period
Urinary Frequency
1st trimester there is increase urination due to increase blood supply to the kidney
2nd trimester - decrease urination
3rd trimester- increase urination due to increase pressure.
Management
Void as necessary, at least every 2 hours. Increase fluid intake.
Avoid caffeine.
Practice Kegel exercises (contracting and relaxing perineal muscles) to decrease urinary incontinence.
Vaginal discharge/ Leukorrhea
due to increase progesterone level.
Management
Wear cotton underwear and bathe daily. Avoid tight pantyhose and use of perineal pad.
Varicose veins
Due to pressure on the veins returning blood from the lower extremities. This causing blood to pool
Management
Walk regularly.
Rest with feet elevated for 15- 20 minutes. - Avoid long periods of standing,
do not cross your legs when sitting. Avoid knee-high stockings,
wear support hosiery and take vitamin C orfresh fruits.
Hemorrhoids
varicosities of rectal veins due to gravid uterus.
Management
Avoid constipation and straining with a bowel movement.
Practice regular bowel movement.
Knee chest position for 10 t0 15 min to relieve pressure and replacing hemorrhoids with gentle finger can be helpful.
take a sitz bath.
Use of stool softener as prescribed.
Leg cramps
Is due to increased calcium levels and decrease phosphorous level and interference with circulation due to increase pressure due to gravid uterus.
Management
Avoid pointing your toes.
Lie on her back straighten your leg and dorsiflex your ankle.
Lowering milk intake and supplementing this with calcium lactate.
Stretching
- Pregnancy, as well as certain medical conditions, can also increase your risk of experiencing leg cramps.
- See your doctor if you’re pregnant or have any of these conditions and are experiencing more leg cramps than usual:
- Addison's disease
- Alcohol use disorder
- Kidney failure
- thyroid issues
- Parkinson's disease
- type 2 diabetes
- sarcoidosis
- cirrhosis
- vascular disease
In addition, medications can contribute to leg cramps, such as:
- birth control pills
- diuretics
- naproxen (Aleve)
- albuterol, an asthma medication
- statins
Nausea
due to increase HCG resulting to increase gastric acid.
Management
Eat 6 small meals / day rather than three.
Eat a piece of dry toast or some crackers before getting out of bed.
Avoid foods or situations that worsen the nausea If it persists, report this problem to your primary care Drink fluids separately rather than with your meals and avoid fried, greasy, gas-producing, or spicy foods
Nasal stuffiness
This causes nasal congestion. Increased blood flow to the nasal passages and enlargement of the nasal veins also play a role.
Management
Use cool air vaporizer or humidifier Increase fluid intake
Place moist towel on the sinuses, and Massage the sinuses.
BIRTH SETTING AND ALTERNATIVE METHODS OF DELIVERY
HOSPITAL BIRTH
Is a mother-friendly based on, through its practices, if the hospital expects that birth is a normal, natural, and healthy process and a woman has the opportunity to:
- Experience a healthy and joyous birth regardless of her age or circumstances
- Give birth as she wishes in an environment in which she feels nurtured and secure. Have access to the full range of options for pregnancy, birth, and nurturing her baby
- Receive accurate and up-to-date information about the benefits and risks of all procedures, drugs, and tests suggested for use during pregnancy, birth, and the postpartum period, with the rights to informed consent and informed refusal.
- Receive support for making informed choices about what is best for her and her baby based on her individual values and beliefs.
Characteristics of a Mother-Friendly Hospital :
- Offers a birthing mother:
- Unrestricted access to the birth companions of her choice, including fathers, partners,
children, family members, and friends
- Unrestricted access to continuous emotional and physical support from a skilled woman— for example, a doula or labor-support professional
Access to professional midwifery care.
- Provides accurate descriptive and statistical inform to the public about its practices and procedures for birth care, including measures of interventions and outcomes.
- Provides culturally competent care—that is, care that is sensitive and responsive to the specific beliefs, values, and customs of the mother’s ethnicity and religion.
- Provides a birthing woman with the freedom to walk, move about, and assume the positions of her choice during labor and birth (unless restriction is specifically required to correct a complication), and discourages the use of the lithotomy position.
- Has clearly defined policies and procedures for:
- Collaborating and consulting throughout the perinatal period with other maternity services.
- Linking the mother and baby to appropriate community resources, including prenatal and post- discharge follow-up and breastfeeding support
- Does not routinely employ practices and procedures that are unsupported by scientific evidence such as routine perineal shaving
- Educates staff in nondrug methods of pain relief and does required to not promote the use of analgesic or anesthetic drugs not specifically correct a complication.
- Encourages all mothers and families, including those with sick or premature newborns or infants with congenital problems, to touch, hold, breastfeed, and care for their babies to the extent compatible with their conditions.
- Discourages nonreligious circumcision of the newborn.
Promotes successful breastfeeding by:
- Having a written breastfeeding policy that is routinely communicated to all health care staff
- Educating all health care staff in skills necessary to implement this policy
- Informing all pregnant women about the benefits and management of breastfeeding
- Helping mothers initiate breastfeeding within a halfhour of birth
- Showing mothers how to breastfeed and how to maintain lactation even if they should be separated from their infants
- Giving newborn infants no food or drink other than breast milk unless medically indicated
- Practicing rooming in to allow mothers and infants to remain together 24 hours a day
- Encouraging breastfeeding on demand
- Giving no pacifiers to breastfeeding infants
- Fostering the establishment of breastfeeding support groups
Advantages
- A woman is encouraged to be prepared to control the discomfort of labor through nonmedication measures such as controlled breathing although anesthesia such as an epidural is readily available.
- A woman is encouraged to be knowledgeable about the labor process and make decisions about procedures performed.
- A woman is encouraged to consider breastfeeding to aid uterine contraction and infant bonding after birth.
- Labor, birth, and immediate postpartal care can all be scheduled in a single room.
- A woman is attended by skilled professionals during labor and birth and the postpartal period.
- Emergency care and extended high-risk care are immediately available.
Disadvantages
- Separation of the family for at least one night.
- Mother may not feel as much in control of the childbirth experience as she may wish
- Care may be fragmented, particularly if a woman's physician is not present during the entire labor and birth, or if labor nurses change shifts in the middle of labor.
ALTERNATIVE BIRTHING CENTERS (ABCS)
Are wellness-oriented childbirth facilities designed to remove childbirth from the acute care hospital setting while still providing enough medical resources for emergency care should a complication of labor or birth arise:
- The birth attendants tend to be nurse- midwives.
- Women who deliver in ABCs are screened for complications before being admitted.
- Like hospitals, ABCs have LDRP rooms where a woman and her support person can invite friends and siblings to participate in the birth.
- A minimum of analgesia and anesthesia is provided, and she can choose a birth position.
- She can bring her own music or distraction objects, and the partner can perform such tasks as cutting the umbilical cord if he or she chooses.
- Women remain in an ABC from 4 to 24 hours after birth
Advantages
- A woman is encouraged to be prepared to control the discomfort of labor through nonmedication measures such as controlled breathing.
- A woman is encouraged to be knowledgeable about the labor process and to help care providers with decision making.
- A woman is encouraged to breastfeed to aid uterine contraction and infant bonding after birth.
Disadvantages
- Extended high-risk care is not immediately available.
- A woman may be fatigued after birth because of brief health care setting stay.
- She must independently monitor her postpartal status because of brief health care setting stay.
FREE BIRTHING
Refers to a woman giving birth without any health care provider supervision also refer to it as unassisted birth or couples birth.
- A woman learns pregnancy care from reading articles on the Internet and then arranges to have her child at home.
- Education can enhance the chances of a positive childbirth experience.
- Client attends the chosen preparation for childbirth class before the 38th week of pregnancy.
HYDROTHERAPY AND WATER BIRTH
Reclining or sitting in warm water during labor can be soothing. The baby is born underwater and then immediately brought to the surface for a first breath.
A potential difficulty is contamination of the bath water with feces expelled with pushing efforts during the second stage of labor could lead to uterine infection in the mother or aspiration of contaminated bath water by » newborn, which could lead to pneumonia.
Advantage of Home Birth
- Knowledgeable about the birth process and be an active participant in independently reducing the discomfort of labor.
- Has the greatest freedom for expressing her individuality.
- There is no separation of the family at birth
- A skilled professional can attend the birth.
Disadvantages
- Adequate equipment other than first-line emergency equipment is unavailable.
- An abrupt change of goals is necessary if hospitalization is required.
- A woman and support person may become exhausted because of the responsibility placed on them.
- Interference with the “taking-in phase” may
occur postpartally because a woman must
“take hold.”
- A woman must independently monitor her postpartal status.
- Family integrity can be maintained because family members may accompany a woman to the birthing
- A woman is attended by skilled professionals during labor and birth.
- Emergency care is immediately available.
Extended high-risk care is easily arranged.
- PHYSIOLOGICAL AND PSYCHOLOGICAL CHANGES OF PREGNANCY
“Physiologic changes of pregnancy occur gradual eventually affect all of a woman’s organ systems.
- They are changes that are necessary to allow a woman able to provide oxygen and nutrients for her growing fetus well as extra nutrients for her own increased metabolism during the pregnancy.
- Psychological changes of pregnancy occur in response only to the physiologic alterations that are happening but also to the increased responsibility associated with welcoming a new and completely dependent person into a family” (Pillitteri, 2010).
Physiologic changes that occur during pregnancy can be categorized as:
- local (confined to the reproductive organs)
- systemic (affecting the entire body).
Both symptoms (subjective findings) and Signs (objective findings) of the physiologic
changes of pregnancy are used to diagnose and
mark the progress of pregnancy” (Pillitteri, 2010).
Establishing Pregnancy
- Pregnancy may be assumed based on the presence of certain signs and symptoms
- PRESUMPTIVE signs are subjective and recorded under history of present illness.
- PROBABLE and POSITIVE signs of pregnancy are objective and recorded as physical assessment findings.
PRESUMPTIVE
- amenorrhea
- breast changes-more erect
- areolas darken and increase in diameter
- Colostrum is formed
- montgomery gland become bigger
- Skin changes: presence of choasma/melasma due
- to hyperpigmentation in the face and armpit
- linea negra and striae gravidarum
- there is morning sickness
- frequency of urination and
- dizziness-can be the first sign of pregnancy
PROBABLE
- Enlargement of the abdomen-umbilicus push out
- Chadwick's sign-deep purle/violet discoloration of the vagina due to increased vascularity
- Goodell’s sign-cervix becomes more vascular and edematous. (softening of Cervix)
- Hegar’s sign-(softening of the segment) .
- Braxton Hick's contraction, Ballotment- (bounching back of the uterus).
- Changes in the level of HCG
- Quickening-(1* uterine contraction during pregnancy)
- Positive pregnancy test
POSITIVE
- Fetal Heart Tone can be heard or auscultated
- Fetal movement felt by the examiner and outlining of the
- fetal body through evidence sonography
- MATERNAL ADAPTATIONS TO PREGNANCY
First Trimester
- Ambivalence, fear, fantasies and anxiety
- Pregnant woman places main focus on self
Second Trimester
- Tranquil period
- Acceptance of the reality of pregnancy
- Increased interest in fetus
Third Trimester
- Anticipates labor and delivery; assumes mothering role
- Fantasies and dreams about labor common
- Nestling behaviors
Developmental Task of Pregnancy
Physiologic changes that occur during pregnancy can be categorized as local (confined to the reproductive organs) or systemic (affecting the entire body). Both symptoms (subjective findings) and signs (objective findings) of the physiologic changes of pregnancy are used to diagnose and mark the progress of pregnancy” (Pillitteri, 2010).
“I am Pregnant”
acceptance of the biological fact of pregnancy
“I am Going To Have a Baby ”
acceptance of the fetus as a distinct individual and a person to care for.
“I am Going To Be A Mother”
prepare realistically for the birth and parenting of the child.
Activities During First Prenatal visit
“screening includes an extensive health history, a complete physical examination, including a pelvic examination, and blood and urine specimens for laboratory work. Manual pelvic measurements can be taken to determine pelvic adequacy” (Pillitteri, 2010)
- Obtain History
- Medical history
- Obstetric history
- History of current pregnancy
- Determine gravity and parity
- Physical exam including pelvic exam
- Calculate EDC and AQG,
- vital Signs
Components of initial visit
If on subsequent visits a symptom is mentioned, establishing a baseline health picture at the initial pregnancy allows you to be able to verify that it is truly a new symptom and a woman is not just
becoming more aware of it” (Pillitteri, 2010).
1.History taking
(chief concern for coming to the health care facility)
Personal data
“Information about a woman's current nutrition, elimination, sleep, recreation, and interpersonal interactions can be elicited best by asking a woman to describe a typical day of her life. If any of this information is not reported spontaneously as she describes her day, ask for additional details” (Pillitteri, 2010).
Age
- Below 15 years are at risk for anemia, CPD, congenital deformity
- Above 35 are at risk for HPN, DM, Placenta Previa and Abruptions
- Below 15 years are at risk for anemia, CPD, congenital deformity
placenta, C/S, Ectopic pregnancy, Fetal growth retardation, Macrosomia, Down syndrome
Weight
- Below 95 lb.is at risk for prematurity, Low birth weight infant, Stillbirth and Congenital defects.
- Qbese woman prone to develop DM, HPN and thrombophlebitis.
Height
Women less than 5 feet tall are at risk for CPD.
Occupation
Handling toxic substances and highly stressful work places woman at risk.
Civil Status
- Menstrual History
Includes: menarche, length and regularity of menses, interval between periods, amount of flow by asking the number of pads used every menstrual period, dysmenorrhea and other discomforts and actions taken.
Breast Health
Includes breast surgery, breast disorders breastfeeding of previous infants.
Contraceptives Used
- IUD in placed to be removed
- Contraceptive pills should be stopped
Medical History
Include childhood diseases, drug allergies, past surgery existing medical conditions, immunizations, alcohol intake, cigarette smoking and use of drugs
Obstetrical History
a. History of past pregnancies include number, outcome, complications, labor time, method of delivery, Puerperium, and complication of puerperium.
GTPALM
G Gravida (number of pregnancy)
T Number of full term infants born after 37 weeks P Number of preterm infants born before 37 weeks A Number of spontaneous or induced abortions
L Number of living children
M Multiple birth (twins)
- Schedule future visit/prenatal check-up:
- Low risk clients
Every month until 28 weeks.
Every 2 weeks from 28 weeks until 36 weeks. Every week from 36 weeks until delivery.
- High risk clients schedule is determined by
client’s needs; visits are scheduled as needed.
- Obtained laboratory data: 1.Hgb, pregnant valuees10-14 f/dl. 2.Hct, pregnant values 32-42 %.
- WBC and differential.
- Hgb electrophoresis (sickle cell).
- Pap Smear and cytology AntibodyScreens:HIV,HBsAg, Toxoplasmosis,Rubella (> 1:8=immunity), SY/VDRL, Cytomegalovirus.
- PPD.
- Rh and BT.
- Urinalysis.
Prenatal Health History
Performing a thorough health in the prenatal essential to planning nursing care and identifying risk women.
Medical History
Chronic Illness
Current and recent medication Recent Acute Illness
Childhood illnesses
Surgical History Problems with anesthesia Previous Surgeries
Uterine/ Cervical Surgeries.
Obstetrical History
Type of Deliveries: Vaginal/Cesarean Complications with the past pregnancies Infertility
Documentation of obstetrical history. Prenatal Health History
Gravida ( G) = Number of pregnancy
Term ( T) = Number of deliveries after 37 weeks Preterm (P) = # of deliveries after 20 weeks but before 38 weeks
Abortion (A) = # of deliveries before 20 either spontaneous or induced.
Living ( L ) = # of living children
G.History of Present Pregnancy Expected date of delivery
- Inquire for last menstrual period (LMP) and compute for expected date of delivery/confinement (EDD/ EDC).
a. Naegele’s rule To get the EDD, the formula is the first day of the last menstrual period then, subtract 3 months, add 7 days to the first day of LMP, and add one year.
Ex: LMP -Sept. 16, 2018
3 months - June 16
Add 7 days June 23
Add 1 year - June 23, 2019
EDC = June 23, 2019
09 16 2018
03 + 7 + 1 year
06 23 2019 = EDC
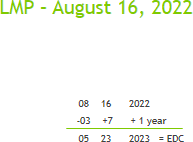
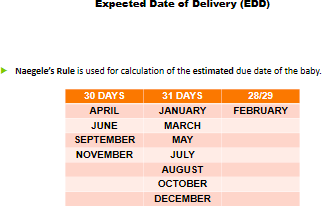
Note: pregnant women may deliver two weeks after or 2 weeks before the EDC.
If the woman cannot remember her LMP, ask her when she first felt quickening.
- To get the EDC for primigravida, add 22 weeks to the date of quickening 15 weeks 22weeks
- To get EDC for multigravida, add 24 weeks to the date of quickening 16 weeks
24 weeks
- Determination of the age of gestation/ duration of pregnancy
- The clinical parameters that can be used to measure the duration of pregnancy are the following:
- Last menstrual period this involves calculating the span of time from the last menstrual period up to the present.
- Problems encountered with the use of the LMP are the following:
a. Failure to record LMP
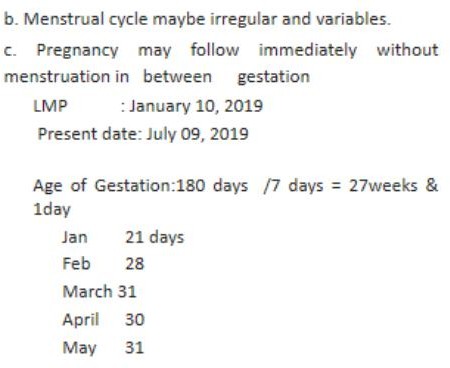
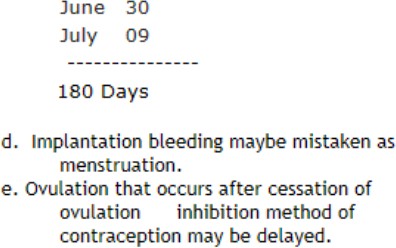
- Basal body temperature record if an isolated coitus can be dated or BBT record is available, the precise onset of pregnancy can be dated.
- Quickening is noted at 20 weeks is and at 16 weeks in multis.
3. Assessment of Fundic height
The FUNDIC HEIGHT is measured to estimate AOG (Age of gestation),EDC, and fetal growth and is measured from top of symphysis pubis to the top of the fundus with the bladder empty.
Weeks Gestation
12 weeks — Just above symphysis pubis.
16 weeks — halfway between symphysis and the umbilicus.
20 weeks — At the umbilicus
21 — 36 weeks — Fundal height generally matches weeks gestation in centimeter
Greater fundic height indicates:
- Multiple pregnancy
- Miscalculated due date
- Poly hydramnios
- Hydatidiform mole
Lesser fundic height indicates:
- fetal growth retardation
- Fetal death
- Error in estimating AOG 4.Oligohydramnios
MCDONALDS RULE
To determine the age of gestation in months by measuring the distance from the fundus to the symphysis pubis(in centimeters) is measured
(FH) in the second trimester when the uterus can be palpated above the symphysis pubis with the :
women lying on her back, bladder empty, and legs slightly flexed.
From 22 weeks to term, it is roughly equal to the age of gestation in weeks
Formula:
- Fundic Height (cm) x 8/7 =
AOG duration of pregnancy in weeks . Ex. 20 cm. x8 /7 = 22. 85
- Fundic height (cm) x_2/7 =
AOG duration of pregnancy in lunar months .
Ex. 20 cm. x2/7 =5.71
BARTOLOMEWS RULE
is used to calculate AOG by the relative position of the uterus in the abdominal cavity and is determined by palpation and by relating to the different landmarks in the abdomen:
- Above the level of symphysis bet. 12 - 14 weeks
- At the umbilicus or 20 cm — about 20 wks.
- Rises about 1 cm/week until 36, after which it varies.
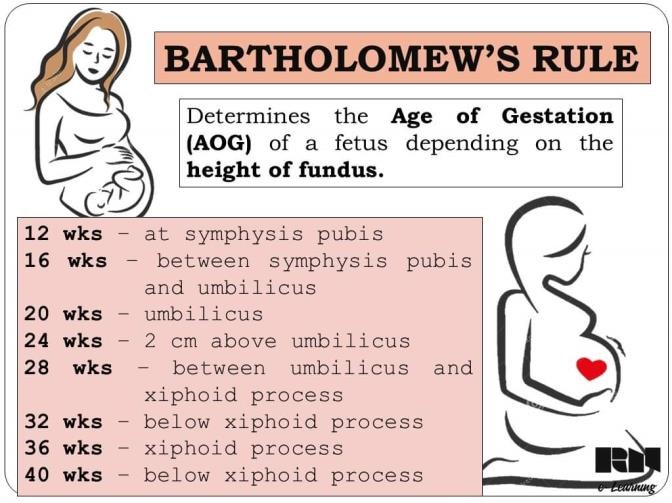
Treatment of disease
- TT immunization
tetanus toxoid is a cornerstone intervention to prevent
tetanus neonatorum and is administered IM
- TT1 as early as possible during pregnancy or anytime during pregnancy=
- TT2 one month after TT1=3 years protection from tetanus and neonatal tetanus
- TT3 six months after TT2 =5 years protection |
- 1T4 one year after TT3 or next pregnancy = 10 years protection
- TTS one year after TT4 or next pregnancy= lifetime protection
Note: If the woman received DPT in infancy and 2 or 3 doses of DPT during pregnancy, is
should be considered as TTi and TT2. succeeding doses will be TT3 and so forth.
- Iron supplementation
“Iron is needed to build this high level of hemoglobin. In addition, after week 20 of pregnancy, a fetus begins to store iron in the liver to last through the first 3 months of life, when intake will consist mainly of milk, typically low in iron” (Pillitteri, 2010)
From 5 months to 2 months post-partum 100- 120 mg simple iron salts for 210 days
- Health education
“In early pregnancy, be certain that you establish a trusting relationship with a woman so she will see you as a person who is capable of counseling her and helping her solve problems, and in whom she is willing to confide as she is about to undergo what could be a stressful 9 month time period” (Pillitteri, 2010).
- Normal signs and symptoms of pregnancy
- Amenorrhea
- Breast changes it is more erect, areolas darken and increase in diameter, colostrum is formed, montgomery gland become bigger.
- Skin changes: Chloasma/melasma (due to hyperpigmentation of the fac eand armpit, lines negra and striae gravidarum
- Nausea and vomiting -morning sickness.
- Frequency of urination
- Dizziness-can be the first sign of pregnancy
- Minor discomforts, prevention and management
- Danger signs and symptoms
- Nutrition and diet
- Rest, exercise and relaxation
- Avoidance of drugs, alcohol, cigarettes, and too much caffeine
- Clothing
- Sexual relations
- Employment
- Travel
- Preparation for baby’s
- Normal signs and symptoms of pregnancy
- Laboratory examination
- Oral dental examination
- Referral when necessary
- Physical Examination
Should be performed systematically, one technique is by cephalocaudal method
- Maternal assessment
Vital Signs
- Blood Pressure no significant changes occur during pregnancy.
In the second trimester, it may drop slightly but return to normal in the third trimester. Blood
pressure is highest when the woman is sitting, intermediate in supine pos. and lowest in left lateral position.
Supine hypotensive syndrome when pregnant woman lies on her back, the gravid uterus compresses the blood vessels that drains blood from the lower extremities and this results in decrease amount of blood going back to the heart, which consequently decreases cardiac output, resulting in less blood supply to the brain that leads to dizziness and hypotension.
- Pulse rate
Pulse rate increases by about 10 beats per faster during pregnancy
- Respiratory Rate
Increases in depth, no significant change in rate, shortness of breath and dyspnea late in pregnancy is common
- Temperature
Slight elevation early in pregnancy due to the thermogenic effect of progesterone. It drops to normal after 16 weeks
Head and Scalp
- Normal findings are: Hair tends to grow faster during pregnancy. Oily hair is also not uncommon.
- Abnormal findings are: excess hair dryness indicates poor nutrition
Eyes
- Abnormal findings are:
- Pale conjunctiva indicates anemia
- and edema of the eyelids accompanied by visual disturbances are signs of HPN.
Nose
- Normal nasal congestion occur as a result of estrogen stimulation
Ears
- Nasal stuffiness results in blockage of eustachian tube which may affect a pregnant woman's hearing
Mouth and Teeth
It is normal to find swollen gums (epulis) due to estrogen stimulation.
Abnormal findings are:
Cracked corners of the mouth maybe caused by vitamin deficiency which pregnant woman are prone to develop.
Dental caries should be treated during pregnancy as they may become site of infection. Major dental operations such as tooth extraction should be postponed until the post-partum period
Neck
Slight thyroid enlargement is brought about by increased basal metabolic rate.
Breast Normal findings :
includes enlargement of the breast with wider and darker areola, prominent veins and montgomery tubercles.
Colostrum, a thin watery fluid, can be expressed from the nipple as early as the
first trimester.
Abnormal findings such as:
breast masses, nodules and bloody nipple discharge are abnormal findings and should be reported to the physician right away.
Skin
Normal findings are:
- linea negra, mask of pregnancy, spider nevi, palmar erythema are common
findings.
Abnormal findings are:
- pallor, rashes, and skin lesions.
Back
Exaggerated lumbar curve late in pregnancy occurs as a result of the shifting of the pregnant woman's center of gravity.
Rectum
- Hemorrhoids
- May be present especially in the last months of pregnancy.
Extremities
- Ankle swelling is a normal finding in the second half of pregnancy.
- Leg edema especially in the late afternoon is common to pregnant women.
- Wadding gait is due to relaxation of pelvic joint.
- Edema of upper extremities, face and hands are danger signs.
Abdominal Examinations
Leopold's Maneuver Preferably performed after 24 weeks gestation when fetal outline can already be palpated.
Common and systematic way to determine the position of a fetus inside the woman's uterus important because they help determine the position and presentation of the fetus
Actual position can only be determined by ultrasound performed by a competent technician or professional.
Named after the gynecologist Christian Gerhard Leopold.
Purposes
To determine the number of fetuses
To identify the presentation, position, degree of descent, and attitude of the fetus
To identify the point of maximum intensity of the fetal heart tone in relation to the woman's abdomen
FACTORS AFFECTING THE PERFORMANCE OF LEOPOLDS MANEUVER
- Difficult to perform in obese women.
- Women with hydramios.
- Women with full bladder
Preparation
"Leopold's maneuvers are a systematic method of observation and palpation to determine fetal presentation and position" (Pillitteri, 2010).
- Cardiac rule-instruct woman to empty her bladder first.
- Place woman in dorsal recumbent position, supine with knees flexed to relax abdominal muscles. Place a small pillow under the head for comfort.
Perform Leopold Manuever.
To determine the fetal position.
1st maneuver
- palpate fetal body part in fundus or Presentation
"Pacing to the women"
Determine the size, consistency, shape, and mobility of the form that is felt.
The Fetal Head (hard, firm, round and moves independently of the trunk while the
Buttocks fell (softer, are symmetric and shoulder and limbs have bony processes, unlike the head, they move with the trunk)
Purpose:
To determine fetal part lying in the fundus
Procedure:
Using both hands, feel for the fetal part lying in the fundus.
Findings:
If the nurse-midwife feels the head which is round, smooth, with transverse groove of the neck, the fetus is in breech presentation. If the nurse- midwife feels the buttocks which is soft and angular, it is in vertex presentation.
2nd Maneuver Umbilical Grip
- Palpate for fetal back. "Pacing the women"
First the right remains steady on one side of the abdomen while the left hand explores the right side of the woman's uterus. This is then repeated using theopposite side and hands.
- Fetal Back = fell firm and smooth.
- Fetal Extremities = arms, legs.
The fetal back, once determined should connect with the form found in the upper abdomen and also a mass in the maternal inlet, lower abdomen.
Purpose:
To identify location of fetal back To determine position
Procedure: One hand is used to steady the uterus on one side of the abdomen while the other hand moves slightly on a circular motion from top to the lower segment of the uterus to feel for fetal back and small fetal parts. Use gentle but deep pressure.
Findings:
Small fetal parts feel nodular with numerous angular nodulations. Fetal back feels smooth, hard, like a resistant PLANE.
3RD MANEUVER : PAWLICK'S GRIP
- Palpate the presenting part
- Engagement
- To determine what fetal part is lying above the inlet, or lower abdomen.
"in the side of the mother, grasp the lower portion."
- The individual performing the maneuver first grasp the lower portion of the abdomen just above the pubic symphysis with the thumb and fingers of the right hand.
This is the part which will most likely come first in a vaginal birth. If it is the head and is not actively engaged in the birthing process,
Purpose
To determine engagement of presenting part.
Procedure:
Using thumb and finger, grasp the lower portion of the abdomen above the symphysis pubis, press in
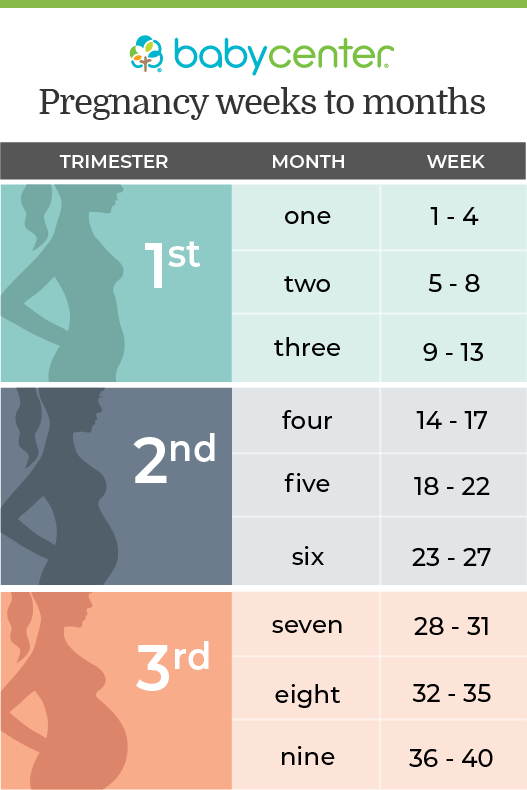 slightly and make gentle movements from side to side.
slightly and make gentle movements from side to side.
Findings: The presenting part is engaged if it is not movable. It is not yet engaged if it is still movable.
4th Maneuver: Pelvic Grip
- Palpate for attitude of presenting part.
"Face the woman's Feet"
Attempt to locate the fetus brow.
- The fingers of both hands are moved gently down the sides of the uterus
towards the pubis.
The side where there is resistance to the descent of the fingers toward the pubis is greatest is where the brow is located.
Purpose
To determine degree of flexion of fetal head To determine attitude or habitus
Procedure
Facing foot part of the woman, palpate fetal head pressing downward about 2 inches above the inguinal ligament.
Use both hands. Findings
If descended deeply, only a small portion of the fetal head will be palpated.
If cephalic prominence or brow of the baby is on the same side of the small fetal parts, the head is flexed.
If cephalic prominence is on the same side of the fetal back, the head is extended.