
Lecture 3: Genes, Environment, Life Style, and Common Diseases
disease in populations:
well established measures are used to define how common a disease could be in a given population
incidence rate- the number of new cases of a disease are reported during a specific period (usually a year) divided by the number of individuals in the population
prevalence rate- the proportion of the population affected by a disease at a specific point in time
determined (affected?) by both the incidence rate and the length of survival period of affected individuals
ex. the prevalence of aids is larger than the incidence rate bc there are more ppl who are affected by it currently than those were only diagnosed with it this year (especially since the prevalence rate includes the people from the incidence rate)
risk factors:
relative risk- incidence rate of a disease among individuals exposed to a risk factor divided by the incidence rate of a disease among individuals not exposed to that risk factor
ex. the incidence rate of lung cancer in people who smoked divided by the incidence rate of lung cancer in people who didn’t smoke
multifactorial inheritance:
polygenic- ‘many genes’, variation in traits caused by the effects of multiple genes
multifactorial trait- variation in traits caused by genetic and environmental/lifestyle factors (aka affected by more than one thing)
(from notes of what he said) the 2 main factors for disease are nature (aka genetics, cannot change) and nurture (aka environmental factors, can change)
most diseases are affected by both (but some are affected by only 1)
quantitative traits- traits that are measured on a continuous numeric scale (he emphasized those words)
threshold model-
liability distribution
threshold of liability
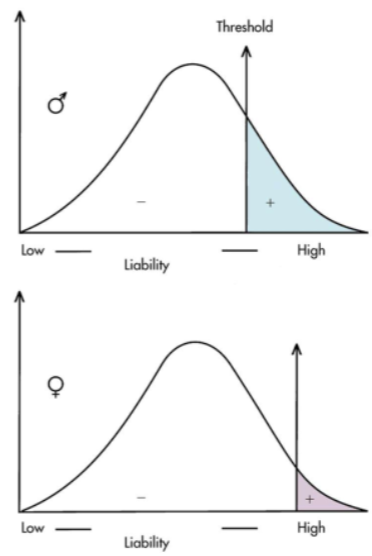
it doesn’t say anything else on that so guess ig??
recurrence risks:
recurrence risks of multifactorial diseases can change substantially bc gene frequencies as well as environment and lifestyle factors can differ among populations
recurrence risk becomes higher if more than one family member is affected
if the expression of the disease in the proband is more severe, the recurrence risk is higher
the recurrence risk is higher if the proband is of the less commonly affected sex
the recurrence risk for the disease usually decreases rapidly in more remotely related relatives
nature and nurture:
family members share the gene and common environment
nature- genetics
nurture- environmental-lifestyle
blood pressure reflects both genetic and environmental-life style commonality (nature and nurture)
few traits are caused by gene or environment only, most are influenced by both
twin studies:
monozygotic twins happen when a developing embryo divides to form separate but identical (genetically) embryos
differences between them are caused only by environmental effects
dizygotic twins result from double ovulation and fertilization of each egg by a dif sperm
concordant trait- a trait that is shared by both members of a twin pair
for a trait determined only by gene, identical twins should be concordant whereas non identical twins will/can be discordant
discordant trait- a trait that isn’t shared by both members of a twin pair
adoption studies:
children born to parents who have a disease but are then subsequently adopted by parents lacking the disease are studied for the recurrence of the disease
this provides evidence that a gene may be involved in the causation of disease (bc the adopted child doesn’t share an environment with their biological parent that has the disease)
genetics of common diseases:
some common multifactorial disorders present at birth and some present as adolescents and adults
congenital diseases- diseases that are present at birth or shortly after birth
most congenital diseases are multifactorial in etiology
etiology- what causes a disease
ex of common congenital malformations:
cleft lip/palate
clubfoot
congenital heart defect
neural tube defect (spina bifida i think)
adult multifactorial diseases:
coronary heart disease:
is a risk factor for: potential mi caused by atherosclerosis
risk increases if:
there are more affected relatives
affected relatives are female rather than male
females are less commonly affected
age of onset is younger than 55 yrs
risk factors for coronary heart disease: autosomal dominant familial hypercholesterolemia, high fat diet, lack of exercise, smoking, and obesity
familial hypercholesterolemia (fh):
autosomal dominant
1 in 500 is heterozygous for the fh gene; 1 in 1 million is homozygous for the trait
serum cholesterol 300 to 400 mg/dl in heterozygotes; 600 to 1200 mg/dl in homozygotes (i’m guessing this can be used as a test as well as what causes the problem)
cholesterol deposits in arteries and skin (xanthomas)
xanthoma- raised, waxy appearing, yellowish skin lesions (maybe also not on the skin but anywhere) that contain cholesterol and fats (aka spots where the cholesterol deposits)
cellular cause/steps:
LDL receptors are synthesized by er
ldl receptors go the the cell surface
circulating ldl particles bind to the LDL receptor and are brought into the cell
ldl particle is separated from the receptor and the receptor is recirculated back to cell surface and LDL particle is taken to lysosome, and broken down into its constituents and free cholesterol is released
excess cholesterol is stored or removed by hdl
high cholesterol in cell, reduces cholesterol synthesis
idk what this is trying to tell me
hypertension:
high blood pressure
is a risk factor for: heart disease, stroke, and kidney disease
studies show that 20-40% of blood pressure variations are genetic
therefore 60-80% are environmental
causes of hypertension (environmental): sodium intake, lack of exercise, stress, obesity, smoking, high fat intake
breast cancer:
affects 12% of American women who live to be 85
if a woman has a first degree relative w breast cancer, her risk doubles
recurrence risk increases if the age of onset in the affected relative is early and if the cancer is bilateral
an autosomal dominant form of breast cancer (5% of breast cancers) has been linked to chromosomes 13 and 17
other genes are implicated
colorectal cancer:
1 in 20 Americans will develop colorectal cancer
second only to lung cancer
risk factor for colorectal cancer: genetics, high fat and low fiber diet are contributers
diabetes:
the etiology is complex and not fully understood, but the genetic basis of the disorder is well studied
leading cause of blindness, heart disease, and kidney failure
2 major types:
type 1- insulin dependent diabetes melltus
type 2- non insulin dependent diabetes mellitus
type 1 diabetes:
characterized by tcell infiltration of pancreas and destruction of insulin producing beta cells
pathologic manifestation and other findings (ex. Ab against beta cells and human leukocyte antigen ‘hla’ class 2 alleles) suggest that type 1 diabetes is an autoimmune disorder
onset usually occurs before 40 years of age
higher incidence w the offspring of diabetic fathers
recurrence risk:
.55 monozygotic twin concordance rate (but obviously 100% concordant therefore there must be an environmental factor to the disease)
1-6% sibling recurrence
type 2 diabetes:
accounts for more than 80-90% of all diabetes cases
neither hla nor autoantibodies are commonly seen in type 2
patient has insulin resistance or diminished insulin production
aka the pancreas probably produces insulin but the cells kinda just ignore it (which is why giving insulin isn’t helpful)
risk factors for it: high carbohydrate diet and obesity
recurrence risk:
.9 mz twin concordance rate
10-15% sibling recurrence
obesity:
commonly defined as a bmi above 30
bmi- aka body mass index, w/h² (weight in kg and height in meters)
bmi- ugh 🙄
obesity is a substantial risk factor for heart disease, stroke, and type 2 diabetes
adoptive studies:
body weights of adopted individuals correlated significantly with their biological parents body weights
so its mostly genetic
twin studies:
higher concordance in mz twins than dz twins
also suggests large genetic component
alzheimer disease:
progressive dementia and loss of memory
formation of amyloid plaques and neurofibrillary tangles in the brain
risdk of developing ad doubles in individuals who have an affected first degree relatives
mutations in any of three genes that affect amyloid beta deposition
presenilin 1 (ps1)
presenilin 2 (ps2)
amyloid beta precursor protein gene (app)
alcoholism:
alcoholism risk is 3-5 times higher in individuals w an alcoholic parent
adoption studies:
offspring of nonalcoholic parents when raised by alcoholic parents did not have an increased risk
so probably not environmental?
twin studies:
concordance rates:
mz: >60%
dz: <30%
psychiatric disorders:
schizophrenia:
severe emotional disorder characterized by delusions, hallucinations, and bizarre, withdrawn, or inappropriate behavior
recurrence risk among the offspring of one affected parent is 10 times higher than the general population
twin and adoption studies indicate that genetic factors are likely to be involved
bipolar affective disorder:
genetics
minimal environmental influence
disease in populations:
well established measures are used to define how common a disease could be in a given population
incidence rate- the number of new cases of a disease are reported during a specific period (usually a year) divided by the number of individuals in the population
prevalence rate- the proportion of the population affected by a disease at a specific point in time
determined (affected?) by both the incidence rate and the length of survival period of affected individuals
ex. the prevalence of aids is larger than the incidence rate bc there are more ppl who are affected by it currently than those were only diagnosed with it this year (especially since the prevalence rate includes the people from the incidence rate)
risk factors:
relative risk- incidence rate of a disease among individuals exposed to a risk factor divided by the incidence rate of a disease among individuals not exposed to that risk factor
ex. the incidence rate of lung cancer in people who smoked divided by the incidence rate of lung cancer in people who didn’t smoke
multifactorial inheritance:
polygenic- ‘many genes’, variation in traits caused by the effects of multiple genes
multifactorial trait- variation in traits caused by genetic and environmental/lifestyle factors (aka affected by more than one thing)
(from notes of what he said) the 2 main factors for disease are nature (aka genetics, cannot change) and nurture (aka environmental factors, can change)
most diseases are affected by both (but some are affected by only 1)
quantitative traits- traits that are measured on a continuous numeric scale (he emphasized those words)
threshold model-
liability distribution
threshold of liability
it doesn’t say anything else on that so guess ig??
recurrence risks:
recurrence risks of multifactorial diseases can change substantially bc gene frequencies as well as environment and lifestyle factors can differ among populations
recurrence risk becomes higher if more than one family member is affected
if the expression of the disease in the proband is more severe, the recurrence risk is higher
the recurrence risk is higher if the proband is of the less commonly affected sex
the recurrence risk for the disease usually decreases rapidly in more remotely related relatives
nature and nurture:
family members share the gene and common environment
nature- genetics
nurture- environmental-lifestyle
blood pressure reflects both genetic and environmental-life style commonality (nature and nurture)
few traits are caused by gene or environment only, most are influenced by both
twin studies:
monozygotic twins happen when a developing embryo divides to form separate but identical (genetically) embryos
differences between them are caused only by environmental effects
dizygotic twins result from double ovulation and fertilization of each egg by a dif sperm
concordant trait- a trait that is shared by both members of a twin pair
for a trait determined only by gene, identical twins should be concordant whereas non identical twins will/can be discordant
discordant trait- a trait that isn’t shared by both members of a twin pair
adoption studies:
children born to parents who have a disease but are then subsequently adopted by parents lacking the disease are studied for the recurrence of the disease
this provides evidence that a gene may be involved in the causation of disease (bc the adopted child doesn’t share an environment with their biological parent that has the disease)
genetics of common diseases:
some common multifactorial disorders present at birth and some present as adolescents and adults
congenital diseases- diseases that are present at birth or shortly after birth
most congenital diseases are multifactorial in etiology
etiology- what causes a disease
ex of common congenital malformations:
cleft lip/palate
clubfoot
congenital heart defect
neural tube defect (spina bifida i think)
adult multifactorial diseases:
coronary heart disease:
is a risk factor for: potential mi caused by atherosclerosis
risk increases if:
there are more affected relatives
affected relatives are female rather than male
females are less commonly affected
age of onset is younger than 55 yrs
risk factors for coronary heart disease: autosomal dominant familial hypercholesterolemia, high fat diet, lack of exercise, smoking, and obesity
familial hypercholesterolemia (fh):
autosomal dominant
1 in 500 is heterozygous for the fh gene; 1 in 1 million is homozygous for the trait
serum cholesterol 300 to 400 mg/dl in heterozygotes; 600 to 1200 mg/dl in homozygotes (i’m guessing this can be used as a test as well as what causes the problem)
cholesterol deposits in arteries and skin (xanthomas)
xanthoma- raised, waxy appearing, yellowish skin lesions (maybe also not on the skin but anywhere) that contain cholesterol and fats (aka spots where the cholesterol deposits)
cellular cause/steps:
LDL receptors are synthesized by er
ldl receptors go the the cell surface
circulating ldl particles bind to the LDL receptor and are brought into the cell
ldl particle is separated from the receptor and the receptor is recirculated back to cell surface and LDL particle is taken to lysosome, and broken down into its constituents and free cholesterol is released
excess cholesterol is stored or removed by hdl
high cholesterol in cell, reduces cholesterol synthesis
idk what this is trying to tell me
hypertension:
high blood pressure
is a risk factor for: heart disease, stroke, and kidney disease
studies show that 20-40% of blood pressure variations are genetic
therefore 60-80% are environmental
causes of hypertension (environmental): sodium intake, lack of exercise, stress, obesity, smoking, high fat intake
breast cancer:
affects 12% of American women who live to be 85
if a woman has a first degree relative w breast cancer, her risk doubles
recurrence risk increases if the age of onset in the affected relative is early and if the cancer is bilateral
an autosomal dominant form of breast cancer (5% of breast cancers) has been linked to chromosomes 13 and 17
other genes are implicated
colorectal cancer:
1 in 20 Americans will develop colorectal cancer
second only to lung cancer
risk factor for colorectal cancer: genetics, high fat and low fiber diet are contributers
diabetes:
the etiology is complex and not fully understood, but the genetic basis of the disorder is well studied
leading cause of blindness, heart disease, and kidney failure
2 major types:
type 1- insulin dependent diabetes melltus
type 2- non insulin dependent diabetes mellitus
type 1 diabetes:
characterized by tcell infiltration of pancreas and destruction of insulin producing beta cells
pathologic manifestation and other findings (ex. Ab against beta cells and human leukocyte antigen ‘hla’ class 2 alleles) suggest that type 1 diabetes is an autoimmune disorder
onset usually occurs before 40 years of age
higher incidence w the offspring of diabetic fathers
recurrence risk:
.55 monozygotic twin concordance rate (but obviously 100% concordant therefore there must be an environmental factor to the disease)
1-6% sibling recurrence
type 2 diabetes:
accounts for more than 80-90% of all diabetes cases
neither hla nor autoantibodies are commonly seen in type 2
patient has insulin resistance or diminished insulin production
aka the pancreas probably produces insulin but the cells kinda just ignore it (which is why giving insulin isn’t helpful)
risk factors for it: high carbohydrate diet and obesity
recurrence risk:
.9 mz twin concordance rate
10-15% sibling recurrence
obesity:
commonly defined as a bmi above 30
bmi- aka body mass index, w/h² (weight in kg and height in meters)
bmi- ugh 🙄
obesity is a substantial risk factor for heart disease, stroke, and type 2 diabetes
adoptive studies:
body weights of adopted individuals correlated significantly with their biological parents body weights
so its mostly genetic
twin studies:
higher concordance in mz twins than dz twins
also suggests large genetic component
alzheimer disease:
progressive dementia and loss of memory
formation of amyloid plaques and neurofibrillary tangles in the brain
risdk of developing ad doubles in individuals who have an affected first degree relatives
mutations in any of three genes that affect amyloid beta deposition
presenilin 1 (ps1)
presenilin 2 (ps2)
amyloid beta precursor protein gene (app)
alcoholism:
alcoholism risk is 3-5 times higher in individuals w an alcoholic parent
adoption studies:
offspring of nonalcoholic parents when raised by alcoholic parents did not have an increased risk
so probably not environmental?
twin studies:
concordance rates:
mz: >60%
dz: <30%
psychiatric disorders:
schizophrenia:
severe emotional disorder characterized by delusions, hallucinations, and bizarre, withdrawn, or inappropriate behavior
recurrence risk among the offspring of one affected parent is 10 times higher than the general population
twin and adoption studies indicate that genetic factors are likely to be involved
bipolar affective disorder:
genetics
minimal environmental influence

