Strength and Conditioning Exam 2
Chapter 5: Adaptations to Anaerobic Training Programs
Key Point
anaerobic training: High intensity intermittent bouts of exercise such as weight lifting; plyometrics, and speed agility intervals training
With heavy resistance training, all muscle fibers get larger because motor units are recruited in a sequential order by their size to produce high levels of force. In advanced lifters, the central nervous system may adapt by allowing recruitment in non-consecutive order, by recruiting larger ones first to promote great power or speed in a movement. large muscle groups first in a lift
hypertrophy involves the synthesis of the contractile proteins actin and myosin within the myofibril, (sliding filament theory)
Neural Adaptations
Anaerobic training may elicit adaptations along the neuromuscular chain, beginning in the higher brain centers and continuing down to the level of individual muscle fibers.
Muscular Adaptations
Skeletal muscle adapts to anaerobic training primarily by increasing its size, facilitating fiber type transitions, and enhancing its biochemical and ultra-structural components. These changes result in enhanced muscular strength, power, and muscular endurance.
Muscular growth
–Muscle hypertrophy: refers to a muscular enlargement from an increase in the cross-sectional area of the existing fiber (horizontally)
–Hyperplasia: an increase in the number of muscle fibers via longitudinal fiber splitting. (vertical) this is hard to see but you can feel the increase in strength.
Fiber size changes
–Resistance training results in increases in both type I and type II muscle fiber area
type II fibers have greater increase then type I
Fiber type transitions
–Continuum of fiber types: I, Ic, IIc, IIac,
IIa, IIax, IIxStructural and architectural changes
–Resistance training increases myofibrillar volume, cytoplasmic density, sarcoplasmic reticulum and
T-tubule density, and sodium–potassium ATPase activity.–Sprint training enhances calcium release.
–Resistance training increases angle of pennation.
Other muscular adaptations
–Reduced mitochondrial density
–Decreased capillary density
–Increased buffering capacity (acid–base balance)
–Changes in muscle substrate content and enzyme activity
Key Point
Forces that reach or exceed a threshold stimulus initiate new bone formation in the area experiencing the mechanical strain. Bones will align with the stress that is placed upon it (Wolff’s Law)
Connective Tissue Adaptations
Anaerobic training and bone growth
–Muscle strength and hypertrophy gains increase
the force exerted on the bones, which may result in
a corresponding increase in–bone mineral density (BMD) : the quantity of mineral deposited in a given area of bone.
How can athletes stimulate bone formation?
–Use exercises that directly load particular regions of the skeleton.
–Use structural exercises to direct force vectors through the spine and hip and allow the use of greater absolute loads in training.
–Overload the musculoskeletal system and progressively increase the load as the tissues become accustomed to the stimulus.
–Vary exercise selection to change the distribution of the force vectors to continually present a unique stimulus.
Adaptations of tendons, ligaments, and fascia to anaerobic training
–The primary stimulus for growth of tendons, ligaments, and fascia is the insult from mechanical forces created during exercise.
–The degree of tissue adaptation is proportional to the intensity of exercise. (If you don’t push past you won’t get stronger)
–Consistent anaerobic exercise that exceeds the threshold of strain stimulates connective tissue changes.
Sites where connective tissues can increase strength and load-bearing capacity:
—At the junctions between the tendon (and ligament) and bone surface
—Within the body of the tendon or ligament
—In the network of fascia within skeletal muscle
Cartilage adaptations to anaerobic training
–Main functions of cartilage (avascular meaning no blood supply) depends on diffusion of oxygen and nutrients from synovial fluid. Once its gone it cannot regenerate itself
•Provide a smooth joint articulating surface
•Act as a shock absorber for forces directed through the joint
•Aid in the attachment of connective tissue to the skeleton
–Therefore, joint mobility is linked with joint health.
–Movement about a joint creates changes in pressure in the joint capsule that drive nutrients from the synovial fluid toward the articular cartilage of the joint.
How can athletes stimulate connective tissue adaptations?
–Cartilage
•Weight-bearing forces and complete movement throughout the range of motion seem to be essential to maintaining tissue viability.
•Moderate aerobic exercise seems adequate for increasing cartilage thickness.
•Strenuous exercise does not appear to cause joint degeneration
Endocrine Responses and Adaptations to Anaerobic Training
Acute anabolic hormonal responses
–The acute anabolic hormonal response to anaerobic exercise is critical for exercise performance and subsequent training adaptations. (Testosterone)
–Upregulation of anabolic hormone receptors is important for mediating the hormonal effects.
Chronic changes in the acute hormonal response
–Consistent resistance training may improve the acute hormonal response to an anaerobic workout.
Cardiovascular and Respiratory Responses to Anaerobic Exercise
Acute cardiovascular responses to anaerobic exercise
–An acute bout of anaerobic exercise significantly increases the cardiovascular responses, especially
if the individual uses the Valsalva maneuver.
Chronic cardiovascular adaptations at rest
–Anaerobic training leads to decrease heart rate and decrease in blood pressure
–Resistance training alters cardiac dimensions.
Key Point
What are the components of mechanical load that stimulate bone growth?
Magnitude of the load (intensity), The rate of the load (speed), The direction of the force, The volume of the load (Reps)
Acute anaerobic exercise results in increased
–Cardiac output
–Stroke volume
–Heart Rate
–Oxygen uptake
–Systolic Blood Pressure
– blood flow to active muscles
Compatibility of Aerobic and Anaerobic Modes of Training
Combining resistance and aerobic endurance training may interfere with strength and power gains primarily if the aerobic endurance training is high in intensity, volume, and frequency. (if you do cardio first you may not lift as heavy due to fatigue)
No adverse effects on aerobic power result from heavy resistance exercise
What Are the Performance Improvements From Anaerobic Exercise?
Its harder to get more gains in experienced lifters. Must increase. so when doing your program you should go to 110%-125% of your max by the end of your program. You should test for maxes in the beginning, middle, and end.
Power: Heavy resistance training with slow velocities of movement leads primarily to improvements in maximal strength. (slow and cotrolled heavy lifting)
–Power training increases force output at higher velocities and rate of force development. Power is 1-4 reps.
hypertrophy is 6-10 reps
4-8 reps is strength
Peak power output is maximized during the jump squat with loads corresponding to 30% to 60% of squat 1RM.
–For the upper body, peak power output can be maximized during the ballistic bench press throw using loads corresponding to 46% to 62% of 1RM bench press.
Local muscular endurance
Skeletal muscle adaptations to anaerobic muscular endurance training include increased mitochondrial density and capillary number. Helps get more oxygen and blood to the muscles helping deliver more energy to the muscles being worked.
Body composition
Resistance training can increase fat-free mass and reduce body fat by 1-9%
Increases in lean tissue mass, daily metabolic rate, and energy expenditure during exercise are outcomes of resistance training.
Flexibility
Anaerobic training potentially can have a positive impact on flexibility, primarily if the individual has poor flexibility to begin with.
The combination of resistance training and stretching appears to be the most effective method to improve flexibility with increasing muscle mass.
Aerobic capacity
Heavy lifting does not affect aerobic capacity unless the individual is initially deconditioned.
The exception is in relatively untrained people, who can experience increases in VO2max ranging from 5% to 8% as a result of resistance training.
Circuit training using high volume and short rest periods (i.e., 30 seconds or less) have been shown to improve VO2max.
Motor performance
Anaerobic training enhances motor performance; the magnitude of change is based on the specificity of the exercises or modalities performed.
Resistance training has been shown to increase: running economy(makes running easier), vertical jump, sprint speed, tennis serve, swinging and throwing, kicking performance
Overtraining
Overtraining is defined as excessive frequency, volume, or intensity of training that results in extreme fatigue, illness, or injury (which is often due to a lack of sufficient rest, recovery, and perhaps nutrient intake).
Excessive training on a short-term basis is called over-reaching
What are the markers of anaerobic overtraining?
Psychological effects of overtraining: Decreased desire to train, decreased joy in training
Acute epinephrine and norepinephrine increases beyond normal exercise-induced levels (sympathetic overtraining syndrome)
Performance decrements, although these occur too late to be a good predictor ( if you fall off or plateau this may be an indicator)
Mistakes that can lead to anaerobic overtraining: Chronic use of high intensity or high volume or a combination of the two, Too rapid a rate of progression
Detraining
Defined as the decrease in performance and loss of accumulated physiological adaptations following the cessation of anaerobic training.
Can also occur when there is a substantial decrease in training frequency, volume, or intensity.
Chapter 6: Adaptations to Aerobic Endurance Training Programs
Key Terms
cardiac output (or Q):The amount of blood that is pumped by the heart in a minute measured in liters (strove vol x hr)
stroke volume: The quantity of blood ejected by the heart each time it beats
Acute Responses to Aerobic Exercise
Cardiovascular responses
From rest to steady-state aerobic exercise, cardiac output initially increases rapidly, then more gradually, and subsequently reaches a plateau.
With maximal exercise, increase up to 4x the resting levels
Stroke volume: End-diastolic volume is significantly increased. At onset of exercise, sympathetic stimulation increases stroke volume.
Oxygen uptake: Increases during an acute bout of aerobic exercise and Is directly related to the mass of exercising muscle, metabolic efficiency, and exercise intensity.
Maximal Oxygen Uptake : The greatest amount of oxygen that can be used at the cellular level for the entire body.
Resting Oxygen Uptake : Estimated at 3.5 ml of oxygen per kilogram of body weight per minute (ml·kg–1·min–1); this value is defined as 1 metabolic equivalent (MET).
Cardiovascular responses
Blood pressure - 120 mmHg
Systolic blood will raise depending on the intensity and the conditioning of the person.
Diastolic blood pressure : measures the amount of pressure between the arterial walls between beats (at rest). Will stay the same 80 mmHg
Cardiovascular responses
–Control of local circulation
During aerobic exercise, blood flow to active muscles is dialated to local arteries
At the same time, blood flow to other organ systems is reduced by constriction of local arterioles.
What increases with Acute aerobic exercise: cardiac output, stroke volume, heart rate, oxygen uptake, systolic blood pressure, blood flow to active muscles
–Decreased diastolic blood pressure
Respiratory responses
–Aerobic exercise provides for the greatest impact on both oxygen uptake and carbon dioxide production, as compared to other types of exercise.
–Significant increases in oxygen delivered to the tissue, carbon dioxide returned to the lungs, and minute ventilation provide for appropriate levels of alveolar gas concentrations during aerobic exercise.
Key Point
During aerobic exercise, large amounts of oxygen diffuse from the capillaries into the tissues
During high-intensity aerobic exercise, the pressure gradients of oxygen and carbon dioxide cause the movement of gases across cell membranes. (at the end of the race when you kick the gasses in teh body move more)
Respiratory responses
Blood transport of gases and metabolic by-products
Most oxygen in blood is carried by hemoglobin (RBC).
Most carbon dioxide removal is from its combination with water and delivery to the lungs in the form of bicarbonate.
During low- to moderate-intensity exercise, enough oxygen is present that we don’t have lactic acid because the removal rate is greater than or equal to the production rate.
The aerobic exercise level at which lactate buildup begins is called Onset Blood Lactate Accumulation (OBLA)
Chronic Adaptations to Aerobic Exercise
Cardiovascular adaptations
Aerobic endurance training requires proper progression, variation, specificity, and overload if physiological adaptations are to take place.
–Increases in maximal cardiac output, stroke volume, and fiber capillary density
–Increased parasympathetic tone leads to decreases in resting and submaximal exercise heart rates
Respiratory adaptations
–Ventilatory adaptations are highly specific to activities that involve the type of exercise used in training.
–Training adaptations include increased tidal volume and breathing frequency with maximal exercise.
Neural adaptations
–Efficiency is increased and fatigue of the contractile mechanisms is delayed.
Muscular adaptations
–One of the fundamental adaptive responses to aerobic endurance training is an increase in the aerobic capacity of the trained musculature.
–This adaptation allows the athlete to perform a given absolute intensity of exercise with greater ease after aerobic endurance training.
Bone and connective tissue adaptations
–In mature adults, the extent to which tendons, ligaments, and cartilage grow and become stronger is proportional to the intensity of the exercise stimulus, especially .
Endocrine adaptations
–Aerobic exercise leads to increases in hormonal circulation and changes at the receptor level.
–High-intensity aerobic endurance training augments the absolute secretion rates of many hormones in response to maximal exercise.
–Trained athletes have blunted responses to submaximal exercise.
Adaptations to Aerobic Endurance Training
One of the most commonly measured adaptations to aerobic endurance training
is an increase in maximal oxygen uptake associated with an increase in maximal cardiac output.The intensity of training is one of the most important factors
Key Point
Aerobic endurance training results in
–Reduced body fat
–Increased maximal oxygen uptake
–Increased respiratory capacity
–Lower blood lactate
–Increased mitochondrial and capillary densities
–Improved enzyme activity
External and Individual Factors Influencing Adaptations
to Aerobic Endurance Training
Altitude
–Changes begin to occur at elevations greater than 1200 m
•Increased pulmonary ventilation (hyperventilation)
•Increased cardiac output at rest and during submaximal exercise due to increases in heart rate
–Values begin to return to normal within two weeks
Several chronic physiological and metabolic adjustments occur during prolonged altitude exposure.
Hyperoxic breathing
–Breathing oxygen-enriched gas mixtures during rest periods or following exercise may positively affect exercise performance.
–The procedure remains controversial.
Smoking
Acute effects of tobacco smoking could impair exercise performance (bad for aerobic conditioning)
Blood Doping: Artificially increasing red blood cells mass is unethical and illegal but can improve aerobic exercise performance and may enhance tolerance to certain environmental conditions.
Genetic potential
–The upper limit of an individual’s genetic potential dictates the absolute magnitude of the training adaptation.
Age and sex
–Maximal aerobic power
–Aerobic power values of women range from 73% to 85% of the values of men.
The general physiological response to training is similar in men and women.
Overtraining
Cardiovascular responses
–Greater volumes of training affect heart rate.
Biochemical responses
–High training volume results in increased levels of creatine kinase, indicating muscle damage.
–Muscle glycogen decreases with prolonged periods of overtraining.
•Endocrine responses
–Overtraining may result in a decreased testosterone-to-cortisol ratio, decreased secretion of GH, and changes in catecholamine levels.
What are the markers of aerobic overtraining?
–Decreased performance
–Decreased percentage of body fat
–Decreased maximal oxygen uptake
–Altered blood pressure
–Increased Decreased muscle glycogen
–Altered resting HR
Chapter 4: Endocrine Responses to resistance Exercise
Key Terms
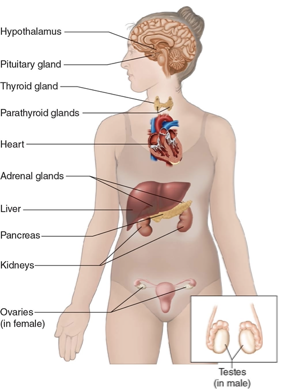
Hormones: Chemical messengers that synthesized, store, and release into the blood by Endocrine Glands and some other cells
Endocrine Glands: Specialized body structures that release hormones into the blood. (everyone has the same hormones but not the same amount)
Muscle as the Target for Hormone Interactions
Hormones are intimately involved with protein synthesis and degradation mechanisms that are part of muscle adaptations to resistance exercise.
This includes both anabolic (promote tissue building) and catabolic (degrade cell proteins) hormones.
Lock and Key Theory: Hormones can only bind at certain sites (one key only fits one lock) Hormone A goes to receptor A, Hormone A goes to receptor A.
Categories of Hormones
Steroid hormone interactions
Fat soluble and passively diffuse across the cell membrane
Heavy Resistance Exercise and Hormonal Increases
The more resistance training and progressive overload you do the more hormones you secrete.
As few as 1 or 2 resistance exercise sessions can increase the amount of androgen receptors (testosterone, estrogen, Human growth horomone) increases binding sites and hormones causing you to get bigger, stronger, faster.
Resistance training and Hypertrophy will cause neural factors that provide important signals to the skeletal muscle and thus can augment anabolic processes.
Hormone responses are tightly linked to the characteristics of the resistance exercise protocol. Training Multijoint, large muscle groups will produce the biggest hormone response.
Primary Anabolic Hormones
Testosterone
Heavy resistance training using 1 or 2 reps and low vol (weight) may not cause any changes in testosterone concentrations after a workout
Large muscle group exercises with adequate volume of work result in an increase in total testosterone concentration in men.
Testosterone
–Exercise variables that can increase serum testosterone concentrations:
•Large muscle group exercises (deadlift, squats)
•Heavy resistance (85-95% of 1RM)
•Moderate to high volume of exercises
•Short rest intervals (30 seconds to 1 minute)
•Two years or more of resistance training experience
Heavy resistance exercise (e.g., six sets of 10 repetitions at 80% of 1RM) can acutely increase free testosterone in men and women, although the increase is much smaller for women.
Free testosterone: not bound to anything or anywhere
Women have about 15- to 20-fold lower concentrations of circulating testosterone than men do.
Training adaptations
Testosterone increases in response to the demands of an exercise protocol, you will have greater production and greater binding sites.
Growth hormone
Important for the normal development of a child
Appears to play a vital role in adapting to the stress of resistance training
automatically produced in the pituitary gland. It secrets more
Main physiological roles of GH and its superfamily:
Decreases glucose utilization
Increases protein synthesis
Increases collagen synthesis
Stimulates cartilage growth
Enhances immune cell function
Increases lipolysis (fat breakdown)
Key Point
Growth hormone release is affected by the type of resistance training protocol
Responses in women: Hormone concentrations and hormone responses to exercise vary with menstrual phase.
Adrenal Hormones
Cortisol (stress horomone)
–Exerts its major catabolic effects by
stimulating the conversion of amino acids to carbohydrates,
increasing the level of proteolytic enzymes (enzymes that break down proteins),
inhibiting protein synthesis, and suppressing many glucose-dependent processes such as glycogenesis and immune cell function.
Cortisol has a greater effect on type 2 than type 1 fibers
Cortisol Resistance exercise responses
Increases in cortisol might not have negative effects in men after a period of training to which the body has adapted;
Resistance exercise protocols that use high volume, large muscle groups, and short rest periods result in increased serum cortisol values.
Chapter 11: Performance-Enhancing Substances and Methods
Ergogenic Aids : Any substance, mechanical aid, or training method that improves sport performance; for the purposes of this chapter, the term refers specifically to pharmacologic aids.
An athlete’s first priority should be to apply sound principles of training, including adequate nutrition, before using any nutritional supplement or ergogenic aid
You can suggest a supplement but not a specific brand. This is unethical.
Types of Performance- Enhancing Substances
A product that is intended to supplement a diet
Products that can be sold as dietary supplements
Must be intended for ingestion
cannot be advertised as a food (meal replacement)
Products that can be sold as dietary supplements
Contain one or more of the following: A vitamin, A mineral, An herb or other botanical, An amino acid, A dietary substance for use by humans to supplement the diet by increasing the total dietary intake, A concentrate, metabolite, constituent, extract, or combination of any of the above ingredients
The difference between a drug and dietary supplement is that it drugs (Pharmaceutical Aids) researched and approved by the FDA
Hormones
Anabolic steroids: The synthetic (man-made) derivatives of the male sex hormone testosterone
Elevations in testosterone concentrations stimulate protein synthesis, resulting in improvements in muscle size, body mass, and strength
Dosing
Athletes typically use anabolic steroids in a “stacking” regimen, in which they administer several different drugs simultaneously.
The potency of one anabolic agent may be enhanced when it is consumed simultaneously with another anabolic agent.
Most users use the drugs for several weeks or months and alternate these cycles with periods of discontinued use.
Often athletes administer the drugs in a pyramid (step-up) pattern in which dosages are steadily increased over several weeks. Toward the end of the cycle, the athlete “steps down” to reduce the likelihood of negative side effects.
Who uses anabolic steroids? Olympic athletes, professional athletes, collegiate athletes, and high school athletes have been reported to use steroids.
Many users are not involved in sports; they use steroids to improve appearance.
Muscle mass and strength: Increase in protein synthesis leading to an increase in Lean Body mass. The same changes occur in profession and recreational uses.
The purported ergogenic benefits commonly attributed to anabolic steroid use are increased muscle mass, strength, and athletic performance, but these changes depend on the training status of the individual.
Anabolic steroids Psychological effects
Anabolic steroid use can cause changes in aggression, arousal, and irritability.
The medical problems related to anabolic steroids may be somewhat overstated.
Many of the side effects of anabolic steroids that are linked to drug abuse are reversible upon when you stop.
HCG (human chorionic gonadotropin)
When injected into men, HCG can increase testicular testosterone production.
Cited anecdotally as useful for males who take anabolic steroids.
Endogenous testosterone production is suppressed at the end of a steroid cycle. If HCG is used by athletes, it is likely used by those who are finishing a cycle of anabolic steroids and are looking to activate their own endogenous testosterone production.
The side effects that are common to injection of HCG are pain, swelling, and tenderness or infection around the injection site.
Insulin
Insulin Facilitates the uptake of glucose and amino acids into the cells
There are several reports that postworkout carbohydrate ingestion suppresses muscle protein breakdown via the anti-catabolic effects of insulin.
Theoretically, if protein breakdown is suppressed over several weeks to months, gains in lean muscle mass could be realized.
Death, diabetes, or coma can be a result from having too much insulin
Human growth hormone
HGH Stimulates bone and skeletal muscle growth, Helps maintain blood glucose levels, and Stimulates the release of fatty acids from fat cells
Little research has been done with athletes.Research with healthy elderly persons, as well as children and adults with growth hormone deficiencies, shows improvements in lean body tissue with decreases in body fat.
Excess HGH after puberty causes acromegaly (a disfiguring disease characterized by a widening of the bones, arthritis, organ enlargement especially in the heart).
Abuse of HGH can also lead to diabetes in prone individuals; cardiovascular dysfunction; muscle, joint, and bone pain; hypertension; abnormal growth of organs; and accelerated osteoarthritis.
Dietary Supplements
Creatine
the rapid rephosphorylation of ADP (adenosine diphosphate) relies on creatine kinase and the availability of creatine phosphate (CP) in muscles
Creatine supplementation: Increases the creatine content of muscles by approximately 20%, but there is a saturation limit.
Creatine supplementation has shown to increase maximal strength, power, and lean body mass
Prolonged creatine supplementation has been generally associated with increases in body weight, especially increases in fat-free mass.
Concerns of taking too much creatine includes GI issues and strain kidneys
True or False: there is no reason to believe that creatine enhances the risk for these side effects. True
Caffeine
Effects on sprint or power performance unclear
Adverse effects of caffeine can include Anxiety, Gastrointestinal disturbances, Restlessness, Insomnia, Tremors, Heart arrhythmias, Increased risk for heat illness, Addiction.
Preworkout energy drinks
Preworkouts is Effective for increasing resistance training volume performance
Other types of anaerobic exercise (including Wingate tests and speed/agility performance) not as responsive to energy drink consumption
Due to the presence of caffeine, the same potential adverse effects that exist for caffeine also exist for energy drinks.
Ephedrine
Ephedrine (basically speed) is effective only when it is taken in combination with caffeine. It improves aerobic endurance performance. Was used for weight loss.,
Adverse effects of ephedrine including death. It is Banned by most sport governing bodies, including the International Olympic Committee
Citrus aurantium
Citrus aurantium Is thought to contribute to appetite suppression, increased metabolic rate, and lipolysis. When combined with caffeine and other herbal products, significant improvements in time to fatigue reported. On NCAA list of banned performance-enhancing drugs