Pathology of the Kidneys and UUT Part 1 Flashcards
Cysts
Types of Cysts
Simple Cysts: Anechoic, imperceptible wall, round shape. No workup required, approximately 0% chance of malignancy.
Complex Cysts: Considered malignant until proven benign. Can have multiple internal features (septations, nodularity, etc.).
Parapelvic Cysts: Typically ovoid, originate from renal hilum; asymptomatic but may cause pain or obstruction.
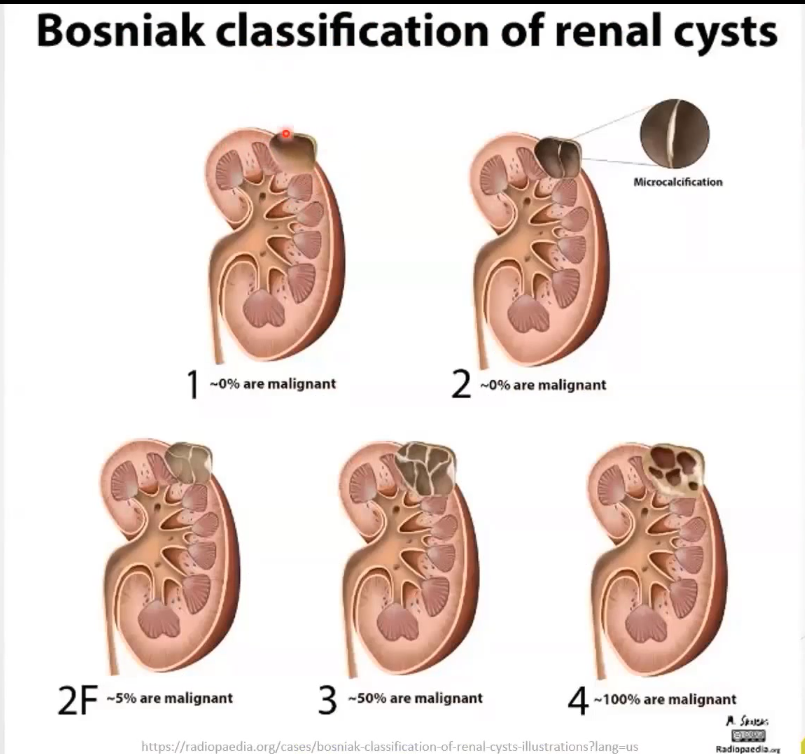
Bosniak Classification of Renal Cysts: grading to determine risk of malignancy
Class | Description | Features | Workup | % Malignant |
|---|---|---|---|---|
1 | Simple cyst | Anaechoic, thin-walled, round | Nil | ~0% |
2 | Minimally complex | Single thin septation, thin calcification | Nil | ~0% |
2F | Complex (need follow up) | Thin septation, thick calcification, hyper dense on CT | US or CT | ~5% |
3 | Indeterminate | Thick/multiple septations, mural nodules; colour flow | Partial nephrectomy | ~50% |
4 | Clearly malignant | Solid mass with cystic spaces | Patrtial or Total nephrectomy | ~100% |
Detailed Characteristics
Simple Cysts
Aetiology: Unknown, more common as people age
Presentation: Asymptomatic; occasionally causes flank or abdominal pain when large, do not affect renal function.
Sonographic Appearance: Anaechoic, well-defined, fluid-filled structure, with posterior enhancement.
Complex Cysts
Presentation: May have septations, thick walls, and calcifications.
US Presentation: Internal echoes and mural nodularity are common
Parapelvic Cysts
Characteristics: Ovoid, originate from within the renal hilium, close to the renal pelvis and calcyes NOT within the renal parenchyma, lymphatic origin, does not communicate with the collecting system.
Clinical Consequence: Usually asymptomatic but can cause pain, haematuria, obstruction or hypertension.
SEPARATE CYSTIC STRUCTURES
Multicystic Dysplastic Kidney Disease (MCDK)
Definition: Abnormal development in utero, often genetic; affects one kidney.
Presentation: Multiple cysts of various sizes; described as resembling a "bunch of grapes."
Non-functioning kidney
Polycystic Kidney Disease (PKD)
Types
Autosomal Dominant (ADPKD): More common; displayed later in life (age 40+). 50% progression to end-stage renal disease by age 60.
Presentation: Bilateral disease with multiple asymmetrical cysts leading to enlarged kidneys.
Autosomal Recessive (ARPKD): Diagnosed at birth or utero; bilateral enlargement with echogenic kidneys retaining shape; collecting duct dilatations.
In older children, kidneys are enlarged with echogenic cortex and medulla and corticomedullary differentiation is lacking
Renal Benign Solid Tumours
Overview: Constitute about 15-20% of all solid renal tumours.
Types
Renal Adenomas: Most common benign tumours; arising from mature tubular cells, typically <3cm.
Subtypes: Renal oncocytoma, papillary adenomas.
US Appearance: Echogenic or isoechoic, well-circumscribed lesions and can be >4cm
Angiomyolipomas: Tumours composed of fat, muscle, and blood vessels; size varies (1-20cm).
US Appearance: Well-defined, echogenic solid lesions, often asymptomatic; no colour flow
Lipomas: Rare; composed of adipose tissue.
Leiomyomas: Rare smooth muscle tumours; echogenicity can vary.
Summary
Review key sonographic terminology related to renal pathologies.
List differential diagnoses for hypoechoic and hyperechoic lesions in the kidney.
Describe sonographic features of various cyst classifications and their malignancy risks.