Biopsychology
The Nervous System
The nervous system has two main functions: to collect, process, respond to environmental stimuli, and to coordinate the working of different organs and cells in the body.
The nervous system can be divided into two main systems.
The Central Nervous System (CNS)
The CNS is made up of the brain and the spinal cord. The brain is the centre of conscious awareness and the spinal cord is responsible for reflex actions. The CNS passes messages to and from the brain and connects nerves to the PNS. It is responsible for receiving, processing and responding to sensory information, controlling behaviour, and regulating the body’s physiological processes.
The brain receives information from sensory receptors and sends messages to muscles and glands in the body. The spinal cord is an extension of the brain - it consists of a collection of nerve cells which are attached to the brain and run the length of the spinal column.
The Peripheral Nervous System (PNS)
The PNS transmits sensory information to the CNS and back via nerve impulses. It transmits information from the CNS to muscles and glands in the body and back. All other nerves which do not from the CNS are apart of the PNS, it reaches all the way down to the toes and all the way to internal organs. It is further divided into two parts: the somatic nervous system; the autonomic nervous system.
PNS Sub-Divisions
Somatic Nervous System | Autonomic Nervous System |
Controls skeletal muscles and a typical reflex arc by receiving information from sensory organs, transmitting it to the CNS and then back to the relevant muscles. (Smooth (heart, lungs) muscles are not controlled). | Divided into the sympathetic and parasympathetic nervous systems. (Only one is active at one time - like a seesaw). It regulates involuntary actions such as heart rate. |
Consists of 12 pairs of cranial nerves and 31 pairs of spinal nerves, including both sensory receptors and motor pathway. | It has an important role in homeostasis (balance among all the body systems). |
The sensory neurons for nerve cells carry sensory information to the CNS. The motor pathways run the opposite way taking information from the CNS out. | Sympathetic Nervous System: this is responsible for emergency situations and is involved in the flight or fight response. Activated by the Hypothalamus. |
Primarily voluntary actions. | Parasympathetic Nervous System: this restores natural order, it relaxes the body after an emergency and is sometimes called “rest and digest.” |
The Endocrine System
The Endocrine System works alongside the nervous system to control vital functions in the body. It is generally much slower than the Nervous System due to the use of hormones. Various glands in the body produce hormones which are released into the bloodstream and transported to the relevant receptors.
The hormone levels in human bodies work in a feedback loop - similar to a thermostat. A signal is sent from the hypothalamus to the pituitary glad in the form of a “releasing hormone”. This causes the pituitary to secrete a “stimulating hormone” to signal the target gland to secret its hormone. As the levels of this hormone increase, the hypothalamus stops secreting the releasing hormone, the pituitary gland shuts down the secretion of the stimulating hormone.
The Pituitary Gland
Regulates the functions of other endocrine glands.
The Adrenal Glands
Located on top of each kidney, the adrenals produce hormones that help the body control blood sugar, burn protein and fat, react to stressors, and regulate blood pressure. Two of the most important adrenal hormones are cortisol and aldosterone.
Fight or Flight Response
The Autonomic Nervous System (ANS) and the Endocrine System work together when a stressor is perceived. A stressor is something that instigates a response from the endocrine system, for example an attacking bear, money troubles, jobs etc. The hypothalamus triggers activity in the sympathetic nervous system (SNS) causing adrenaline to be released from the adrenal medulla into the bloodstream. This is an acute, automatic reaction to a stressor. When the threat has passed, the parasympathetic nervous system regains control and the body reverts to a resting state.
Stressful Event | |
The Nervous System | The Endocrine System |
Activates the Sympathetic Nervous System. | Hypothalamus activates the pituitary gland (Hypothalamic Pituitary Axis), which releases ACTH into the bloodstream. |
Sympathetic branch maintains activation | ACTH makes the adrenal glands release adrenaline to maintain the activation of the SNS. |
Stressful Event Ends | |
Activates the Parasympathetic Nervous System. | Releases ACh which calms the body. |
Long-term/Chronic Stress
This works similarly to acute stress (table) yet instead of adrenaline, the adrenal glands produce the hormone cortisol. Cortisol enables the body to maintain steady supplies of blood sugar. Adequate and steady blood sugar levels help people to cope with prolonged stressor, and helps the body to return to normal. This is why heart issues, eating issues like overweight, are associated with chronic stress.
Structure of Neurons
Neurons are a type of cell that receives and sends messages from the body to the CNS. This enables communication within the nervous system. These are sent using action potential (electrical signal or neural impulse).
There are three types of neurons:
Sensory Neurons
These send nerve impulses from the senses to the brain and spinal cord. The sensory receptor triggers the action potential which travels down the axon, jumping between the nodes of Ravier to the soma (cell body) to the synaptic endings. The terminal knobs are at the end of the axons ready to pass the action potential to the next neuron.
Relay Neuron
These allow sensory and motor neurons to communicate, primarily found in the CNS. Dendrites receive information from other neurons, carry it through the short axon, and pass it to the next neuron via the terminal knobs (or terminal buttons).
Motor Neuron
These are responsible for either directly or indirectly controlling muscles. The messages are sent along long axons from the brain to the effectors (muscles or glands).
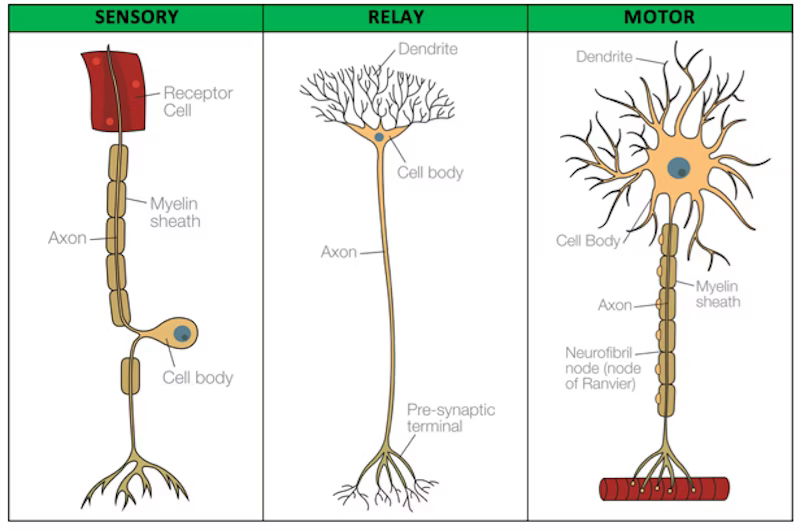
The soma contains the nucleus including chromosomes. The dendrites extend from the cell body, these carry action potential from the other neurons towards the cell body. The axon is an extension of the neuron, it carries the impulses away from the cell body and is covered by a sheath of myelin, a fatty substance. The main purpose of this is to increase the speed at which the impulse propogate. There are breaks of between 0.2mm and 2mm called nodes of Ranvier. Action potentials travelling down the axon “jump” from node to node speeding up the transmission.
Synaptic Transmission
The gap between the terminal knob of one neuron and the dendrite of another is called the synapse. Signals cross between the neurons here.
The action potential triggers vesicles to move to the pre-synaptic cell membrane.
These vesicles fuse with the membrane and release neurotransmitters into the synaptic cleft.
Neurotransmitters diffuse across the cleft down a concentration gradient and bind to specific receptors on the post-synaptic membrane.
When they bind, they may trigger an electrical impulse in a neuron which causes an effector to move.
The impulses are one-directional, so any neurotransmitters that are not bound to receptors are taken back by the presynaptic cleft, or are broken down by enzymes so the impulse does not keep on repeating.
Excitation and Inhibition
When neurotransmitters bind to the post-synaptic receptor sites, positive (if the neurotransmitter is excitatory) or negative (if it is inhibitory) ion channels open. Excitatory increase the positive charge of the post-synaptic neuron and increases the likelihood of it firing. Inhibitory increase the negative charge of the post-synaptic neuron and decreases the likelihood of it firing.
Inhibitory neurotransmitters such as GABA, calm down the brain and nervous system. GABA is produced after periods of stress to return the body to calm. The inhibitory synaptic potential (IPSP) means the impulse is less likely to fire.
Excitatory neurotransmitters stimulate activity in areas of the brain. Dopamine can make a person feel alert and able to focus for a short period of time. The excitatory synaptic potential (EPSP) means that the impulse is more likely to fire.
A cell can receive both EPSP and IPSP at the same time, therefore firing or not is determined by summation (adding together the excitatory and inhibitory neurons).
The strength of an EPSP can be increased in two ways:
In spatial summation, a large number of EPSPs are generated at many different synapses on the same post-synaptic neuron at the same time.
In temporal summation, a large number of EPSPs are generated at the same synapse by a series of high frequency action potentials on the post-synaptic neuron.
The rate at which particular cells fire is determined by what goes on in the synapses. If excitatory synapses are more active, the cells fire at a high rate. Whereas, with more inhibitory synapses, the cells fire at a much lower rate, if at all.
Neurotransmitters
Dopamine is a neurotransmitter which increases addictive effects of reinforcement. It contributes to control of movement, an excess of it is linked with schizophrenia. Antipsychotic drugs work by blocking some of the receptor sites preventing as much dopamine to bind reducing the frequency of the neuron firing.
Serotonin is associated with mood, eating, and arousal. It is linked with depression, aggression, OCD and eating disorders.
GABA (gamma-aminobutyric acid) is the main inhibitory neurotransmitter, it is linked with epilepsy.
Localisation of Function
Localisation: The principle that specific functions have specific locations in the brain.
The Brain
Weighs approximately 1.5kg
Is made of approx. 100 billion neurons
Each neuron may be connected to up to 15000 other neurons
Meaning there are over 1500 trillion synaptic connections.
Estimated processing power is one exaflop (1 billion billion calculations per second).
In 2014, researchers in Japan tried to match the processing power in one second from one percent of the brain. It took the 4th fastest supercomputer in the world (the K Computer) 40 minutes to crunch the calculations for a single second of brain activity.
Background
The early 19th century saw a growth in interest of localisation of brain functions stemming from Franz Gall’s theory of phrenology which was discredited quickly. Pierre Flourens was able to demonstrate that there were main divisions in the brain responsible for different functions using animal experimentation. Since, the techniques have grown considerably more sophisticated along with understanding of the functional organisation of the human brain.The first sensible (most scientific) research into localisation of functions is in the late 19th century with Broca and Wernicke.
Phrenology is the study of the structure of the skull to determine a person’s character and capacity.
Localisation of Function
The human brain can be viewed as being formed of four concentric layers:
The Central Core
The Central Core is made up of the brain stem, medulla and pons. This controls life functions, sleep, appetite, and reproduction. The main core regulates other primitive and involuntary behaviours such as breathing, sleeping, or sneezing. It includes the hypothalamus and regulates the endocrine system in order to maintain homeostasis.
The Limbic System
Around the central core, interconnected with the hypothalamus, it contains structures such as the hippocampus which key role in memory. The hippocampus is important for memory, the hypothalamus regulates the endocrine system and the ANS, the amygdala regulates emotions and aggression.
The Cerebrum
The Cerebrum regulates higher intellectual processes. The outermost layer is the Cerebral Cortex - this appears grey because of the location of cell bodies. The cerebrum is made up of the left and right hemispheres which is further divided into the four lobes (frontal, parietal, temporal, and occipital).
The Cerebral Cortex
Each of the sensory systems sends messages to and from the cerebral cortex. It has a very large surface area due to folds and ridges. The two hemispheres are connected by a bundle of fibres called the corpus callosum. This enables messages to enter the right hemisphere to be conveyed to the left and vice versa. The corpus callosum is approximately 250 million axons that run between the hemispheres allowing information to be shared.
The Motor Cortex
Controls voluntary movement, found in both hemispheres but each side controls the muscles on the opposite side of the body.
The Somatosensory Cortex
Processes information from our senses relating to pain, pressure, and temperature. Located in the parietal lobe.
The Visual Cortex
Processes visual information received by the eyes via the optic nerve. The visual cortex is located in the occipital lobe at the posterior of the brain.
The Auditory Cortex
Processes auditory information such as pitch, tone, loudness in order to make sense of sound and respond appropriately to them. Located in the temporal lobe on each side near the ears.
The Hemispheres
In most respects, the two hemispheres are very similar. One difference is the presence of the language areas, which are only found on the left-hand side. Broca’s and Wernicke’s area important areas associated with language located in the left posterior frontal lobe and the posterior temporal lobe.
Broca’s Area is considered to be the main centre of speech production. Broca found that patients with speech problems had lesions to this area, yet patients with lesions on the right hemisphere did not have any speech problems. The region plays a central role in speech generation, language processing and when there is damage it is difficult for patients to formulate a full sentence. This is known as Broca’s Aphasia.
Wernicke’s Area is located in the left hemisphere in the temporal lobe. It is concerned with comprehension of speech. Wernicke’s Aphasia cause patients to have difficulty producing language and understanding it.
Localisation of Function: Evaluation
Brain Scan Evidence
There is objective, scientific evidence providing support for the theory of localisation of many neurological functions, particularly in relation to language and memory.
Peterson (1988) used brain scans to demonstrate how Wernicke’s area was active during a listening task whereas Broca’s area was active during a reading task, suggesting these areas do perform a specific function.
Tulving et al (1994) used a brain scanning technique (Tulving’s Gold Study) to show that semantic and episodic memories reside in different parts of the brain.
Counter Point: Dick and Tremblay (2016) showed really language neural processes occur in all parts of the brain in some way.
Counter Theory
Karl Lashley (1950) suggests that the basic motor and sensory functions were localised but higher mental functions are not - Lashley’s Equipotentiality Theory. This means that each part of the brain has equal potential for specific functions.
He claimed that intact areas of the cortex could take over responsibility for specific cognitive functions following injury to the area normally responsible for that function. The effects of the damage to the brain would be determined by the extent rather than the location of the damage. This received some support from the discovery that humans were able to regain some of their cognitive abilities following damage to specific areas of the brain.
Lashley carried out surgical procedures on hundreds of animals, mostly rats. He found that removal of anything up to 50% of a rat’s brain had no impact on its ability to learn and to run a maze. Suggesting that learning is not isolated to one specific brain area but does appear to be more globally organised requiring the involvement of most of the brain. He concluded that simpler functions such as sensory and motor functions were localised but higher mental functions such as learning, memory and problem solving were distributed more globally. Outcomes following brain damage would not depend so much on the area damaged but on the size of the damage.
Case Study: Phineas Gage
Damasio et al (1994) aimed to explain the cause of Gage’s change of personality after experiencing extensive damage to his prefrontal cortex.
Situation: Phineas Gage had an iron, tamping pole hurled through his face and skull, through his left eye to his right prefrontal cortex and out from the top of his skull. It was found 25-30 years behind covered in bits of his brain, he was believe to not have lost consciousness.
Results: Surviving, and after months of recovery, his personality had changed completely. According to verified friends and family, Gage had been a most capable and efficient foreman, of a well-balanced mind, and a smart businessman. After the accident, he was boisterous, rude and grossly blasphemous.
Conclusion: Damasio et al concluded that the accident has taught us a great deal about the complexity of psychological processes that occur in the human brain.
Support of LOBF: Phineas Gage demonstrates that functions such as decision making, personality expression, moderating social behaviour, and future planning are located in the prefrontal cortex. After the accident, he was violent, blasphemous showing an impaired future planning, and moderating social behaviour functions within the brain. It shows that other functions, such as motor control, speech, and vision are located else where in the brain as these were not impacted.
Counterpoints
Issues with Case Studies
Lacks generalisability
Does not show causation
Lacks replicability
CP
Verified accounts of his personality means that PG can show causation and is unlike most case studies.
CP
Cannot determine whether the change in personality was solely due to the injury.
It cannot be determined that the change in lifestyle, his face, and the general trauma did not cause the change in personality.
There may be a third intervening variable.
Neurosurgical Evidence
Lobotomy: removal of brain tissue
Leucotomy: cutting the connections to particular parts of the brain.
Walter Freeman pioneered this in the 30s - 60s, with some success, but was outed for fraud and lost his medical licence. He would preform neurosurgery on patients with epilepsy, removing or disconnecting different areas to cure it, yet had little theory and evidence to support which areas he decided to work with. Although he had success with some patients, roughly 50% lost their lives to him.
Neurosurgery is still used today for treatment-resistant severe depressives and extreme cases of OCD. (Dougherty et al 2002) The success of these procedures strongly suggests that symptoms and behaviours associated with serious mental disorders are localised.
Neuroplasticity and Functional Recovery
Plasticity (neuroplasticity, cortical remapping): The brain’s ability or tendency to change and adapt, functionally and physically, as a result of experiences and or new learning.
Functional Recovery is a form of neuroplasticity where the brain is able to transfer functions to other areas of the brain after cranial trauma (damage) has occurred. After cranial trauma, secondary neural pathways around the area activate, finding a different route for communication with other parts of the brain. This enables functioning to continue. (Doidge 2007) There are numerous ways this occurs:
Functional Recovery through reformation of blood vessels
Blood vessels reform to ensure adequate blood supply to the area. This ensures the area has enough oxygen and glucose transported to it.
Neural Regeneration - the growth of new neurons, and/or connections to compensate for damaged areas.
Axonal Sprouting occurs when new nerve endings form, and attach to undamaged nerve endings, forming new neural pathways. Similar to how a tree grows a new branch when one gets broken.
Synaptic Bridging (synaptic re-weighting) is how an active synapse will physically grow (the terminal knobs get fatter); this creates more synaptic vesicles which in turn release more neurotransmitters. An increase in neurotransmitters means that more will bind to the post-synaptic dendrite, increasing the action potential of the neuron. The opposite occurs when a synapse is underused - it will shrivel up.
Neural Reorganisation - the transfer of functions to undamaged areas.
Recruitment of homologous areas provides limiting evidence for localisation of brain function. Similar areas on the opposite side of the brain are ‘recruited’ to preform the function of the damaged area.
Lashley argued that the only higher functions were localised in the brain and proposed the Theory of Equipotentiality. Neural reorganisation supports this theory as it also states that various areas of the brain have equal potential to preform the same function, this is evident after cranial trauma.
Synaptic Pruning is the loss of neurons when they are underused. It is also the strengthening of neurons when information is reinforced and consistently used. The number of synaptic connections in the brain peaks at 2-3 years old with around 15000 connections. (Gopnick et al 1999) However, as you age these connections are “pruned” and lost. Rarely used connections are deleted but recent research suggests that neural connections can be formed or changed at any time in life as a result of experience.
Maguire et al (2000)
Maguire et al studied the brains of London taxi drivers using an MRI and found that the hippocampus had changed significantly physically compared to the matched control group. The navigational and spatial skills associated with the training for London Cabbies for the complex test called ‘the Knowledge’ made the structural difference pronounced. Furthermore, the longer they had done the job made the structural difference more pronounced.
Human Echolocation
Similar to how dolphins use echolocation for hunting, human echolocation is a learnt ability for humans to sense their environment. This ability is used by some blind people to navigate their surroundings. Studies in 2010 and 2011 using FMRI techniques have shown that parts of the brain associated with visual processing were adapted for the new skill of echolocation. Studies with blind patients suggest that the click-echoes heard by these patients were processed by brain regions devoted to vision rather than audition.
Neuroplasticity and Functional Recovery: Evaluation
Gopnick et al (1999)
Infants have enormous growth in the number of synaptic connections in their brain, peaking at around 3 years old. Infants have up to 15000 synaptic connections per neuron, this halves by adulthood.
Draganski et al (2006)
Medical students showed changes to their posterior hippocampus and their parietal cortex following their final exams.
Mechelli et al (2004)
Bilingual people have a larger parietal cortex than monolingual people.
Maguire et al (2000)
This study is research support for neuroplasticity as there was significant increase in grey matter in the posterior hippocampus of the London taxi drivers.
A strength is that it uses scientific, objective measurements. The MRI scans show empirical evidence of a structural change.
Furthermore, the study utilised a control group, allowing significant difference to be established.
However, it does not show causation only correlation because the taxi drivers were not tested before “The Knowledge.” The group may have become taxi drivers because of the difference - they might have naturally better navigational skills because of the natural difference.
However, there is a positive correlation between time experience and changes in structure suggesting that the difference is in-fact due to the learning. The longer time spent as a taxi driver, the larger the difference in hippocampus.
Schneider et al (2014)
This study is research support for functional recovery as patients with cranial damage were able to recover functions with little to no lasting damage.
The study also found that the recovery times of patients who had a higher level of education, prior to the accident, had much faster levels of recovery and a higher likelihood of no lasting damage. This suggests that education can affect how adaptive the brain is following trauma because of the greater “cognitive reserve.”
A strength of the study is that it had a large sample size of 769 patients, therefore the evidence has high validity. It also contained a range of levels of education including 24% who did not finish schooling and 25% who had graduated university.
However, this research is extremely socially sensitive as it suggests that the higher level of education gained the better recovery. Higher level of education is not easily accessible thus is socially controversial for different social classes.
Lateralisation
Lateralisation is the view that distinct brain hemispheres perform certain functions. Contralateral control is how one hemisphere of the brain controls the opposite side of the body.
The cerebrum is made up of the left and right hemispheres, connected by the corpus callosum (approximately 300 million axons make up the corpus callosum).
Split Brain Studies
Sperry studied the functioning of split-brain patients, patients who had a commissurotomy (cuttting the corpus callosum), in the 1960’s. He was able to show that certain functions were houses either fully or mainly in one particular hemisphere. It was found that commissurotomies could control very serve cases of epilepsy.
Sample: 11 patients who had undergone commissurotomy as treatment for epilepsy.
He compared their functioning to people without epilepsy who had not undergone the procedure.
Method: Using a tachistoscope, participants focused on a dot in the middle of the screen whilst a word flashed up for 1/10 of a second. This is done so that the participant cannot move their eyes to look at the word. On the table under a screen, items could be handled in the tactile tests. The participants were asked to repeat the word that they saw.
Findings: It was found that when the word was flashed on the right side of the screen, the patient could repeat what they saw. This is because language and speech is found in the left hemisphere and the contralateral control of the eyes. Oppositely, when the word was on the left side, the patient could not repeat the word. However, when asked to draw it, the left hand could draw what was seen. The right hemisphere cannot share information with the left, but can control the left hand. In the tactile tests, the participants could repeat the right-hand word whilst finding the left-hand word which is processed by the right hemisphere.
Another example: Faces are matched by the right brain only. When a composite faces was used in studies, the right-side face could be described due to it entering the left hemisphere where Broca and Wernike’s areas are. The left-side face, however, was picked out when asked to match the picture.
When the participants realised what they picked out in the tactile and facial recognition tests, the left brain tried to make sense of why the answers did not match. The left hemisphere is responsible for logical thinking.
Lateralisation: Evaluation
Sperry: Methodological Evaluation
Strengths | Limitations |
Research support for the theories of brain lateralisation. Evidence showed that without the corpus callosum an image on the left side cannot be verbally communicated. | Sample size reduces the population validity- only 11, epileptic patients means that the sample may not be large enough to generalise. |
Controlled conditions as the participants only had a tenth of a second to see the words- standardised procedures improves repeatability of the experiment, improving internal validity. | Lack of control over the extent of disconnection and previous therapy. The extent of disconnection varied and some patients had experienced drug therapies for much longer than others. |
Pucetti (1977) - agreed with the results and furthered it with psychological theory. He advocated the idea of duality for the brain. | Lack of mundane realism - low ecological validity. In reality the patients are able to compensate by adjusting their visual field. |
Fundamental impact on the understanding of consciousness and identity. | Lack of valid control group - the control group was not matched with experimental as they did not experience a commissurotomy nor did they have epilepsy. It cannot be certain which affected the findings, the commissurotomy or the epilepsy. |
Counterstudy: Gazzaniga (1998) |
Gazzaniga (1998)
It was suggested that early discoveries from split-brain research has been disconfirmed by more recent studies. Older split-brain research has suggested that the right hemisphere was unable to handle even the most rudimentary language. However, case studies have demonstrated that this is not necessarily the case. J.W. developed the capacity to speak out of the right hemisphere, with the result that J.W can now speak about information regardless of which hemisphere it was presented to.
Lateralisation and Age
Szaflarski et al (2006) found that language became more lateralised to the left hemisphere with increasing age in children and adolescence. Meanwhile, after the age of 25, lateralisation decreased with each decade of life. This suggests that lateralisation changes with normal aging. It was also found that lateralised functions in younger individuals tend to switch to bilateral in healthy older adults.
Pop-Psychology
Split brain research has considerable real-world application for people with epilepsy.
Split brain research has provided considerable evidence supporting the lateralisation of verbal and analytical tasks to the left and more spatial and creative tasks to the right. However, as a consequence, pop-psychology has over-emphasised and over-simplified the differences between the hemispheres.
Cortical Specialisation
Cortical specialisation is the way humans have tried to investigate the brain in order to better understand it.
Techniques
fMRI - Functional Magnetic Resonance Imaging
Blood oxygenation and flow (metabolic function) is detected to show which specific areas are activated (using most oxygen). It works on the premise that neurons in the brain which are most active in a task, use the most energy. This is called haemodynamic response. A fMRI creates a dynamic 3D activation map of the brain, highlighting, like a heat-map, which areas are involved in different neural activities.
EEGs - Electroencephalograms
A skull cap lined with electrodes measuring brainwaves to show overall brain activity. It works on the premise that information is processed and exchanged through the brain as electrical activity as action potential. These electrical charges are detected by the electrodes and graphed over a period of time. It usually picks up on (irregular) arrhythmic patterns.
ERP - Event-Related Potentials
Brainwaves from an EEG are isolated to allow for specific brainwaves related to certain activity to be examined. Measuring their activity shows the event-related potential. Key difference: A stimulus is presented and the researcher looks for activity related to that stimulus.
Post-Mortem Examinations
Following death, a brain can be examined and compared to a neurotypical brain for any potential neurological differences or defects.
Cortical Specialisation: Evaluation
fMRI
Strengths:
It is a non-invasive technique as it does not require radiation or any instruments directly into the brain therefore is virtually risk-free. More data can be gathered as the risk-free nature should allow more patients/participants to undertake fMRI scans developing the understanding of localisation of function.
The fMRI scan has high spatial resolution: spatial resolution refers to the smallest measurement that a scanner can detect. Spatial resolution is an important feature of brain scanning techniques. The higher the resolution allows psychologists and scientists to discriminate between different brain regions with greater accuracy such as the distinction between the somatosensory and the motor cortex. fMRIs have a spatial resolution of approximately 1-2mm which is significantly greater than the other techniques.
Weaknesses:
A limitation is the temporal resolution: temporal resolution refers to the accuracy of the scanner in relation to time or how quickly the scanner can detect changes in brain activity. The temporal resolution of fMRI scans is 1-5 seconds which is significantly worse than other techniques. Consequently, psychologists are unable to predict with a high degree of accuracy the onset of brain activity.
5 Second Rolling Average
Each still-picture scan comes from approximately 5 seconds of brain activity in an fMRI. The still is a 5 second rolling average. Steady increase of brain activity would result in a fairly accurate 5-second average, whereas the still scan of activity continuously spiking and falling would not be accurate, the average would not show the full picture of brain activity. This demonstrates poor temporal resolution.
Causation is hard to establish as the scans do not provide a direct measure of neural activity. It is impossible to infer causation when the scanners only measure changes in blood flow. It clearly shows neural activity of certain brain areas, but psychologists are unable to conclude whether this brain region is associated with a particular function.
EEG and ERP
Strengths:
Both techniques are non-invasive and do not use radiation or involve inserting instruments directly into the brain therefore is virtually risk-free. The expense of EEGs and ERPs make it readily available which should allow more patients/participants to undertake them increasing the data gathered for psychologists developing understanding for phenomena such as sleeping, and Alzheimer’s.
The techniques have good temporal resolution as it takes readings every millisecond. This means that it can record the brain’s activity in practically real-time as opposed to looking at a passive brain. The high temporal resolution leads to an accurate measurement of electrical activity when undertaking a specific task.
Weaknesses:
The electrodes on the skull cap are uncomfortable for the participants which may result in unrepresentative readings due to the patient’s discomfort affecting cognitive responses to situations.
The main limitation of EEG and ERP’s are the poor spatial resolution. EEGs and ERPs only detect the activity in superficial regions of the brain, this makes them unable to provide information on what is happening in areas located deeper in the brain structure. For example, EEGs and ERPs can detect activity in the motor cortex but would not be able to detect activity in the hypothalamus. This limits the techniques.
Biological Rhythms
Biological Rhythms are natural rhythmic cycles in life which are influenced by external (Exogenous Zeitgebers) and internal (Endogenous Pacemakers) factors. It is a change in the body processes or behaviour in response to cyclical changes within the environment.
Circadian: A cycle lasting approximately 24-hours.
Example: Sleep/Wake Cycle and Core body temperature.
The Sleep/Wake cycle makes humans feel drowsy at night-time and alert during the day demonstrating the effect of daylight.
Ultradian: A cycle which occurs more than once in a day.
Example: Different Stages of Sleep
Infradian: A cycle that takes longer than 24-hours to complete.
Example: Menstrual Cycle and Seasonal Affective Disorder
All biological rhythms are regulated and governed by two factors:
Endogenous Pacemakers
The body’s internal body clocks that regulate biological rhythms.
The Suprachiasmatic Nucleus, a structure in the brain near the hypothalamus, detects light, even when eyes are closed.
Exogenous Zeitgebers
External factors in the environment which reset biological clocks.
Light and Social Cues
Chronotype
Chronotypes are the preference of an individual for the time they carry out daily activities. The standard circadian profile is neither (N) ‘night owls’ or ‘early birds,’ meaning people who wake up between 7 and 8 am and go to bed between 11pm and midnight. The N type is most likely to be alert in the morning and early evening and least alert in the early afternoon.
The MM and ME types are still within the standard range, showing similar. patterns of alertness and sleepiness, though MMs may have trouble if they must work through the overnight hours.
The DMs and DEs are off by about two hours from the standard day-night cycle around which the typical work is based. DMs work best around 8:00-9:00 and are pretty much done for the day by 9 or 10pm.
Age affects chronotypes the most, parental patterns and different responsibilities also are reflected in chronotypes.
Circadian Rhythms
Circadian rhythms are biological cycles that last approximately 24-hours, for example the sleep/wake cycle.
Michel Siffre - The Cave Study (1962)
Aim: To discover how the natural rhythms of human life would be affected by living ‘beyond time.’ How natural rhythms are affected by external factors.
A French speleologist spent 2 months living in total isolation in a subterranean cave, without access to a clock, calendar, or the sun. He repeated this cave stay for 6 months finding that he settled into a sleep/wake cycle of 25 to 30 hours. The supports the assumption that endogenous pacemakers exert an influence on circadian rhythms.
Steel et al (2008)
Studied 6 participants living in the Arctic for 6 weeks during constant daylight. The participants kept sleep logs; these showed that 5 participants developed free-running sleep/wake cycles longer than 24 hours. No synchronised patterns emerged.
Aschoff and Wever (1976)
In a Siffre-style experiment, participants lived in a WW2 bunker for 4 weeks with no natural light and were isolated from external time cues. Their sleep patterns were monitored, revealing that most participants exhibited a free-running rhythm of about 24 -25 hours. Only one participant had settled into a cycle of 29 hours. These findings suggest that while humans have an innate circadian rhythm, environmental factors such as light exposure are crucial in regulating sleep patterns. It supports the importance of endogenous pacemakers and exogenous zeitegebers.
Core Body Temperature
Core body temperature fluctuates by around two degrees within a 24 hour cycle. It is at its lowest (36 degrees Celsius) at around 4am and peaks around 6pm (38 degrees Celsius).
A higher body temperature may be linked to enhanced cognitive performance.
Folkard et al (1977) revealed superior recall and comprehension of stories in children when the stories were read at 3pm as opposed to 9pm one week prior to testing.
Gupta (1991) found improved performance on IQ tests when participants were assessed at 7pm as opposed to 2pm and 9am.
Wright et al (2002) have speculated that higher core body temperature leads to increased physiological arousal which enhances cognition.
Circadian Rhythms: Evaluation
Research Evidence
Siffre (1962 and 1972)
After spending 2 months in the caves, deprived of light and sound, he determined his circadian rhythm remained between 24-25 hours. This was further supported by Aschoff and Wever.
Aschoff and Wever (1976)
Placed participants in a bunker for 4 weeks with no natural light to do research similar to Siffre’s. They settled into sleep/wake cycle of between 25 and 27 hours.
This suggests that endogenous pacemakers control the sleep/wake cycle in the absence of light cues.
Folkard et al (1985)
12 volunteer participants were placed in temporal isolation for 3 weeks. The cave had no external light and a single large clock that the researchers were able to control. The participants agreed to go to bed when the clock showed 11:35pm and to get up at 7:45am. Initially the researchers set the clock to run at a normal 24-hour cycle, however gradually increased its speed so that eventually a day passed in just 22 hours. Only one participant comfortably synchronised their sleep/wake cycles to the pace of the clock.
These studies suggest that the body’s internal clock is set 24-25 hours in the absence of external cues, and is intolerant of any major alterations.
Poor Control in Studies
In the cave studies, the exposure to artificial lights was not controlled.
It was assumed it was only natural light that has an influence on biological rhythms, however research found that dim artificial lighting could adjust the circadian rhythm between 22-28 hours.
Czeisler et al (1999) had volunteers try 20 and 28 hour long days. These participants seemed to revert to 24 hour days, but when dim artificial lighting was introduced to assist them into the longer days, the participants managed to go from 22 to 28hour days. It was found there were individual differences, 13-65 hour circadian rhythms.
The results of the original studies may lack validity and the sleep/wake cycle may vary considerably more. The impact of artificial lighting on circadian rhythms also has practical applications when it comes to the use of electronic devices during different times of the day.
Issues with Case Study
The Siffre study was one individual, similar studies (Aschoff and Wever, and Folkard et al) were conducted on a handful of people.
It is difficult to generalise to the wider population, even though the findings have been backed up by other research. There may be individual differences in the research sample that makes participants respond to the changes in atypical ways. Siffre noted that at 60 his body responded very differently with his body clock following more of a 48 hour cycle.
This suggests that results cannot be generalised from these small samples onto everyone, as factors such as age, gender, etc may have significant impacts on circadian rhythms.
Real World Application
Application to shift work
Shift work has been found to lead to desynchronisation of circadian rhythms and can lead to adverse cognitive and physiological effects.
Research has shown that night shift workers suffer a concentration lapse at 6am, increasing the likelihood of accidents, (Boivin et al, 1996) and shift workers are also three times more likely to suffer from heart disease as a result from the stress of adjusting to sleep/wake cycles (Knutsson, 2003).
Other reported health effects include, fatigue and sleep disorders, obesity, type 2 diabetes, digestive disorders, mental health illnesses, some evidence suggests there is an impact on reproductive health and increased incidence of cancer. (Health and Social Care Information Centre, 2014)
This research has many economic implications, in terms of maintaining worker productivity and preventing accidents in the workplace. It also has had an implication on how shift work is allocated in industries, eg in the NHS. Furthermore, laws have been placed to limit the maximum time spent on a night shift to only 8 hours in an average of 24 hour period (The Working Time Regulations 1998).
Application to Pharmocokinetics
By understanding circadian rhythms and their impacts on health, it can help determine the best time to administer drug treatments.
For example, the risk of heart attack is greatest in the early morning so drugs can be taken at night which are not released until they will be most effective at dusk.
Bonten et al (2015) found that timing of drug-taking is key, finding that late-night aspirin for heart attacks had high efficiency.
This means that there are peak times for administration and dosage of a variety of drugs that treat a range of disorders such as cancer, epilepsy and respiratory issues that increase their efficacy.
Application to School
The understanding of circadian rhythms has an application on the education system and wider educational policy.
Kelly (2010) conducted a pilot study at a high school near Newcastle, which showed that starting school at 10am (roughly 1.5 hours after a typical start) had increased positive outcomes on the students.
Outcomes included improvements to sleep issues, academic improvements, increased attendance, behaviour and mood improvements.
Despite numerous studies with strong evidence indicating school timings should be synchronised with adolescent’s biology, this change, on a wide-scale, would have implications on families because of the typical adult work day.
Infradian Rhythms
Infradian rhythm: A type of rhythm with a frequency of less than one cycle in 24 hours, such as menstruation and Seasonal Affective Disorder.
Menstrual Cycle
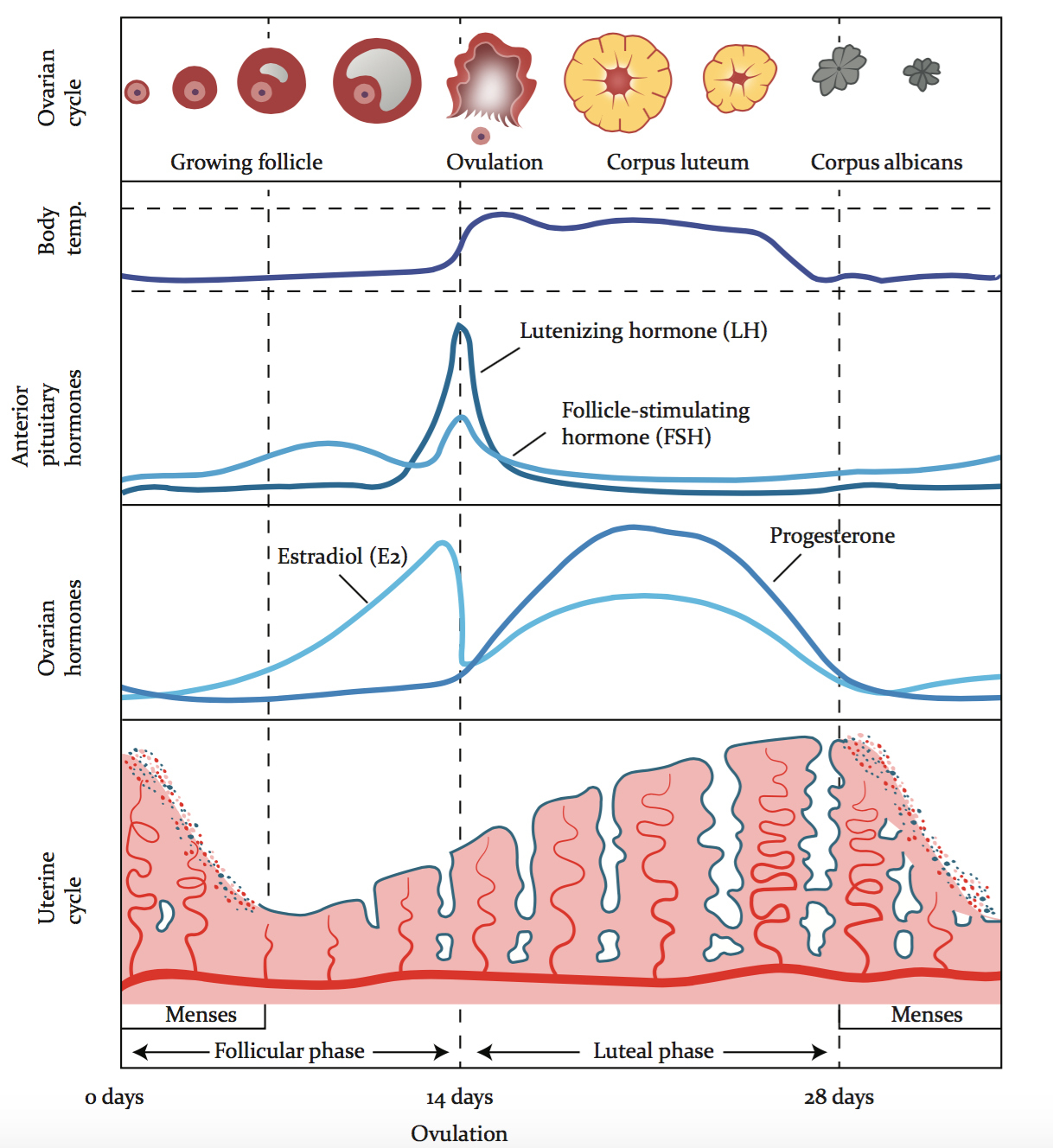
The Menstrual cycle takes approximately 28 days to complete, and is influenced primarily by hormones but also exogenous zeitgebers. It is the process of ovulation and discharge of the womb lining in a cycle.
Endogenous Pacemakers:
There are four hormones involved in the menstrual cycle: oestrogen, progesterone, follicle-stimulating hormone (FSH), and lutenizing hormone (LH).
The start of the cycle begins with a rise in oestrogen levels which stimulates the growth of an egg. The womb lining begins to shed due to the lack of fertilisation, this is menses, a period.
FSH remains steady the majority of the cycle, it triggers the growth of eggs in the ovaries. It has a small spike when the egg is released into the fallopian tube
As the egg matures, LH spikes in order for the egg to be released from the follicle. This happens around the 14 day mark.
Progesterone helps the uterus lining grow thicker, in preparation of an implantation and pregnancy.
If there is no fertilisation, no pregnancy, the uterus lining is shed and the. egg is absorbed into the body. This repeats the cycle where oestrogen rises stimulating the growth of the next egg.
Exogenous Zeitgebers
There are four main external factors which impact the menstrual cycle:
Diet
Exercise
Stress
Sleep
Stern and McClintock (1998)
The study aimed to find out whether menstrual cycles synchronise as a result of pheromones. Pheromones are chemical substances produced and released into the environment by an animal affecting the behaviour or physiology of others of its species.
Methods: 29 female participants, with a history of irregular periods, were chosen for the study. 9 of the women, at all different stages of the cycle, had cotton pads put under their armpits every day, to collect pheromones. The remaining 20 women rubbed the cotton pads on their top lip every day. Each day represented the respective day of the cycle for whichever sample they were given.
Results: 68% of the women experienced changes to their cycle, bringing them closer to the cycle of their ‘donor.’
Seasonal Affective Disorder
Seasonal Affective Disorder (SAD) is a type of depression that comes and goes in a seasonal pattern.
Annual rhythms are related to the seasons, this may affect human behaviour, seasonal variations in mood. Some people become severely depressed in the winter months.
SAD is a circannual rhythm where melatonin (associated with sleep and drowsiness) is secreted for a longer period of time due to a lack of light. As part of the sleep/wake cycle, the Suprachiasmatic Nucleus detects light and thus activates the secretion of melatonin when it gets dark. In the winter months, the hours of daylight are shorter than “typical” meaning more melatonin is secreted for longer time periods affecting the neurotransmitter serotonin. Serotonin production is prevented by melatonin simply because it is not needed when asleep. This causes depressive symptoms.
Ultradian Rhythms
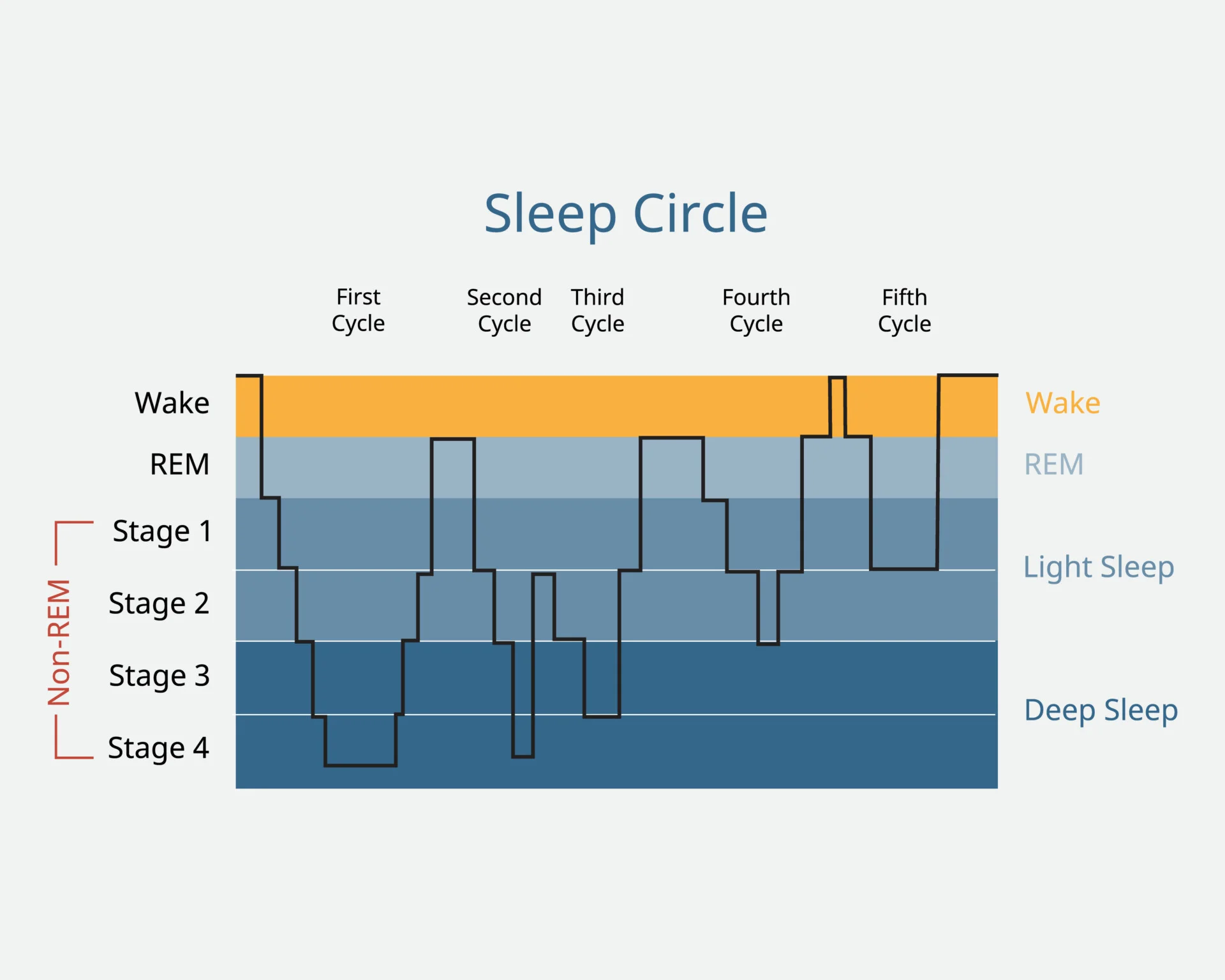
Ultradian rhythm: A type of rhythm with a frequency of more than one cycle in 24 hours, such as Sleep Cycle.
Stage 1: Brainwaves become slower and more regular, increasing in amplitude. This is an alpha wave. This is non-Rapid Eye Movement.
Stage 2: nREM. These are slower, shown by greater wave amplitude. Theta waves are produced.
In stage 1 and 2, there are sleep spindles which are a pattern of brain waves during nREM responsible for jerking awake. There also are K Complexes which are increased wave amplitudes.
Stage 3 and 4: Slow-Wave Sleep (SWS) produce delta waves resulting in the body being in its lowest state of arousal. The heart rate and body temperature falls, metabolism slows, growth hormones are produced. nREM.
Stage 5: After going through stage 1 to 4 then out again, stage 5 is the lightest level of sleep. Fast desynchronised electrical activity occurs which resembles the awake brain. Eyeballs move rapidly in their sockets and dreaming with vivid imagery is commonly reported, if the person is aroused. This is REM. The thalamus paralyses the body, to prevent it enacting the dreams, but the brain and eyes are active.
During Slow-Wave Sleep, sensory information is largely inhibited by the thalamus. This is in order to maintain sleep by stopping external distractions. SWS is found in stage 3 and 4 the deeper levels of sleep. There is also a move to conserve energy by decreasing heart rate, blood pressure, and respiratory rate.
During Rapid Eye Movement, (REM), motor regions are activated but the motor neurons controlling skeletal muscles are inhibited, leading to temporary paralysis. During REM, information can seep from the external world into the subconscious and may be incorporated into dreams.
The sleep cycle lasts approximately 90 minutes, with the majority of people having 5 cycles in a night.
Kleitman (1969)
Described that the movement between stages of sleep as Basic Rest and Activity Cycle (BRAC). He then suggested that this not only occurs at night but also in the day, where a similar cycle of alertness and fatigue occurs. Research suggests that humans can concentrate for approximately 90 minutes before losing concentration and feeling fatigued.
This is supported by Ericsson et al (1993), who found that the best performers would practice 3 times for 90 minutes during a day, with a break in between to ‘recharge.’
Infradian and Ultradian: Evaluation
Infradian
Evolutionary Basis to Menstrual Synchrony
It may have been advantageous for females to menstruate together and fall pregnant at the same time. This would increase chance of survival as the new-borns could be cared for collectively.
However, Schank (2004) argued that this was not advantageous for males. If too many females were cycling together, there would be increased competition for the “highest quality” males (the healthiest, strongest suitors). This would lower the quality of any offspring (due to lack of genetic diversity) and so avoidance of synchrony seems to be more adaptive.
Stern and McClintock (1998): Methodological Issues
There was no control group to compare the potential synchrony to, nor a control group of females with strongly regular cycles to test whether it was not a coincidence.
The sample consisted of only females with irregular cycles therefore the results cannot be generalised to females with regular cycles.
Trevathan et al (1993) failed to find any evidence of menstrual synchrony.
Many extraneous variables were not controlled for. The proximity to other females was not controlled, therefore it cannot be certain whether the collected pheromones affected the cycles of the participants or whether other peoples pheromones affected the cycles.
SAD
Terman (1988) found that Seasonal Affective Disorder was more common in the most northernly countries where there is less daylight and longer nights.
There are practical applications of understanding infradian rhythms such as to the treatment of SAD. Phototherapy has been found to be an effective treatment for SAD (Eastman - morning light-treatment group showed significantly more complete or near-complete remission of SAD symptoms compared to placebo group). Furthermore it has resulted in the development of “sunlight” lamps which mimic the full light spectrum to counteract the lack of natural sunlight and levels of vitamin D in the body.
Ultradian
Dement and Kleitman (1957)
It was demonstrated that there was a link between REM sleep and dreaming. Brain activity was measured using an EEG. The effects of caffeine and alcohol were controlled for, because caffeine is a stimulant keeping the body awake, and alcohol, despite being a depressant, prevents stage 4 sleep. It was reported that REM sleep was highly correlated with dreaming, the more vivid the dream the more active the brain was. Recall was more clear when awoken in this stage.
However, dreaming was reported outside REM sleep. Yet this most likely is the participant recalling their most recent REM stage.
Individual Differences
Tucker et al (2007) found that there were biologically determined individual differences in the sleep cycle. Participants in a sleep lab were tested to measure their sleep. It was found that there was significant differences in the duration of each stage especially stage 3 and 4. An idiographic approach may be better.
Endogenous Pacemakers and Exogenous Zeitgebers
The control of circadian, infradian, and ultradian rhythms can be due to:
Internal biological ‘clocks’ called endogenous pacemakers.
External cues from environment, called exogenous zeitgebers, such as sunlight, food and noise.
If the rhythm can work without external cues, this is called free-running. If the cycle can work with external cues, this is called entrainment. A blended system is having a free-running cycle which can be focussed by external cues.
Endogenous Pacemaker
The main endogenous pacemaker (EP) is the suprachiasmatic nucleus found next to the optic chiasm.
The Suprachiasmatic Nucleus (SCN) is a cluster of cells in the hypothalamus which is stimulated by light obtained by the optic nerve. The morning light stimulates the SCN, putting one’s biological clock in time with the surroundings. The SCN is located in both hemispheres, each consists of a ventral (front) and a dorsal (back) section. When stimulated, it sends messages to the pineal gland to inhibit the secretion of the hormone melatonin promoting wakefulness.
Pineal Gland secrets melatonin which promotes sleep.
DeCoursey et al (2000)
Investigated the consequences of lesioning (damaging) the SCN connections in 30 chipmunks.
Method: One group of chipmunks under went surgery to purposely damage the SCN before being returned to their natural habitat and observed for 80 days. This was compared to two control groups, the first control had no surgery at all, the second was a surgical control who had experienced brain damage to areas other than the SCN.
Results: The sleep/wake cycle of the experimental group had disappeared and by the end of the study, a significant number had been killed by weasels. The controls had all survived. Therefore, the researchers speculated that the chipmunks remained awake in their burrows and the weasels were able to locate them by the noise.
Ralph et al (1990)
Ralph et al bred hamsters to give them sleep/wake cycles of 20 hours. He then transplanted the SCNs of the “mutant” hamsters into “normal” ones to investigate whether they would have normal sleep/wake cycles or whether they would revert to the bred 20 hours cycle. It was found that the transplanted SCN resulted in those hamsters adopting 20-hours cycles too.
Exogenous Zeitgebers
Light is the most dominant zeitgeber in humans, this was supported by Campbell and Murphy (1998). Social cues such as conventions like meal-times and age-appropriate bedtimes are also EZs.
Campbell and Murphy (1998)
The aim was to see if light could be detected not just by the optic nerve but also by skin receptors.
Method: 15 participants were awoken at various times by shining a light to the back of the knee. This area was chosen as it is far from the eyes which would have caused the SCN to pick up the light, and is not affected by bones.
Results: They found that cycles could deviated to up to 3 hours.
EPs and EZs: Evaluation
Animal Studies
Cannot generalise the results from animals to humans
Ethical issues
Research Evidence
The SCN may be overestimated.
Damiola (2000) demonstrated how changing the feeding patterns in mice could alter the circadian rhythms in their liver by up to 12 hours. This had no effect on the SCN rhythm. This suggests that there are various circadian rhythms in the body, not necessarily inextricably linked to the SCN.
Miles et al (1977) reported a case study of a blind man who had a circadian rhythm of 24.9 hours which made it difficult to function. He was exposed to various EZs but his endogenous mechanisms did not shift. As a consequence he was prescribed stimulants and sedatives to entrain his biological rhythm. This showed the reliance on external cues.
Conclusion: The biological rhythm is a blended system, therefore it’s an interactionist system.