OTR 527 Exam 3 Study Guide
Kinesiology Exam 3 Study Guide
Exam 3: Concepts to Review
Guiding questions in italics.
Wrist
Carpal Bones
- Identification: Know the names and positions of the carpal bones.
- Difference Between Proximal and Distal Carpal Rows: Understand their unique features and functions.
- Anatomical Pulley: The carpal bones have an anatomical pulley, specifically the pisiform bone.
- Function: This pulley increases the torque of the muscle it deflects (which muscle, and how?)
Ligaments
- You do not need to know all individual ligaments, because ligaments function as a capsule to create a closed-pack system.
- What is a closed-pack system?
- Importance: This system is crucial for the sliding and gliding movements of the carpal bones. (Why?)
Movements
- Synergistic Movements: Understand in detail the coordinated movements of the wrist bones.
- Know the specific carpal bone movements involved during radial/ulnar deviation and wrist flexion/extension. (The markers)
- Tenodesis questions will be present.
- Concepts to Review: Active and passive insufficiency. (What are they and how do they affect tenodesis?)
Know these Muscles
- Know the muscles involved in:
- Wrist flexion and extension
- Wrist radial and ulnar deviation
Clinical Considerations
- Carpal Tunnel Syndrome: Review notes on this condition.
- Eccentric and Concentric Motions: Understand these concepts and how they apply to wrist movements.
- Will not cover this for hand movements.
Functional Use of Wrist and Hand
- Observation: Think about how you use your wrist and hands in daily activities.
- Analysis: This will help you understand how to analyze vignettes provided in the exam.
Hand
Know These Muscles
- Power Grasps: Know the specific muscles involved.
- Hook
- Cylinder
- Sphere
- Precision Handling: Know the specific muscles involved.
- Pad-to-Pad
- Tip-to-tip
- Pad-to-Side
- Snuff Box: Be familiar with the muscles and components of the snuffbox.
- Extensor hood mechanism: know the muscles and components involved.
Grasps and Pinches
Think about pinches and grasps used in various and specific occupations.
Know the types of grasps and pinches:
- Power Grasps (When would these be used? How would they be modified in each of those uses?)
- Cylinder
- Sphere
- Hook
- Precision Handling (When would these be used? How would they be modified in each of those uses?)
- Pad-to-Pad
- Tip-to-Tip
- Pad-to-Side/Lateral Pinch
Arches of the Hand
- Importance: Understand why the arches of the hand are important.
- Clinical Consideration: Intrinsic minus hand, including the creation of the lumbrical bar splint.
- Wear Time for Splints: Understand the guidelines for wearing splints (e.g., lumbrical bar splint worn during the day).
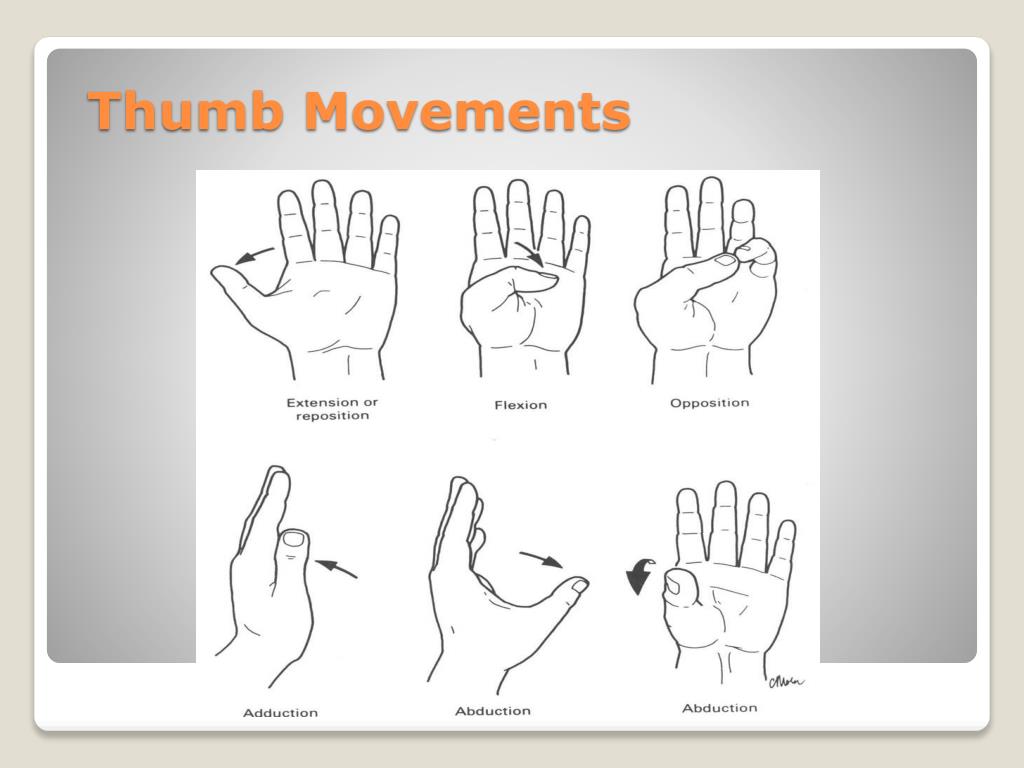
Thumb Movements
- Know the movements of the thumb. Be able to identify and explain these movements.
- Extension/flexion
- Abduction/adduction
- Opposition and rotation
Extensor Hood Mechanism
- Components: Know all parts and their functions.
- Diagram in lab will be on the exam
Practical Prep and Exam Format
- Question Types: Expect seventy-seven questions and one vector. Will NOT test concentric/eccentric for the hand.
- Movement Analysis: Be prepared to analyze movements at different joints (e.g., CMC, MCP, PIP).
- Diagrams and Models: Review the diagrams provided in your modules.
- Lab Practice: Use lab sessions for rigorous practice to make the exam easier.
- Clinical Insight: Practice observing and analyzing movements in clinical settings.
Miscellaneous
- Understanding Insertions: Know that the lumbrical muscles insert on the radial side of the digits.
Week 7: The Hand
Importance of the Hand in Occupational Therapy
- Vital for daily tasks: The hand allows for forceful grips and intricate object manipulation essential for self-care and activities of daily living (ADLs).
- Examples of hand functions: Picking up a coin, using a parking meter, sewing, crocheting, buttoning a shirt, and putting toothpaste on a toothbrush.
Bones of the Hand
- Metacarpals: Located in the mid-hand region, they articulate proximally with the carpal bones.
- Phalanges: Divided into proximal, middle, and distal phalanges. The thumb has only proximal and distal phalanges.
Thumb
Has a special motion, opposition, that occurs as a combination of abduction, rotation, and flexion at CMC joint. Because it’s the thumb lol.
REMEMBER: flexion/extension = frontal; abduction/adduction = sagittal
Joints | Extrinsic Muscles | Intrinsic Muscles | |||||
|---|---|---|---|---|---|---|---|
Flexor Pollicis Longus - FPL | Extensor Pollicis Longus - EPL (Snuffbox 👃) | Extensor Pollicis Brevis - EPB (Snuffbox 👃) | Abductor Pollicis Longus - APL (Snuffbox👃) | Adductor Pollicis - AP | Flexor Pollicis Brevis - FPB | Opponens Pollicis - OP | |
Carpometacarpal Joint (CMC) - Saddle | +Flexion ~Crosses over joint | +Extension ~Crosses over joint | +Extension | +Abduction | +Limited adduction | +Flexion | +Rotation for opposition (note) |
Metacarpophalangeal Joint (MCP) - Condyloid | +Flexion ~Crosses over joint | +Extension ~Crosses over joint | +Extension | +Limited adduction | +Flexion | ||
Interphalangeal Joint (IP) - Hinge | +Flexion ~Crosses over joint | +Extension ~Crosses over joint | |||||
Joints of the Thumb
- Carpometacarpal (CMC) Joint - Saddle Joint
- Movements: Flexion/extension (frontal plane), abduction/adduction (sagittal plane).
- Special Movement: Opposition (combination of abduction, rotation, and flexion).
- Metacarpophalangeal (MCP) Joint - Condyloid Joint
- Movements: Flexion/extension, limited abduction/adduction (primarily at CMC).
- Interphalangeal (IP) Joint - Hinge Joint
- Movements: Flexion/extension.
Soft Tissue Structures of the Thumb
- Joint Capsule: Contains synovial membrane and fluid.
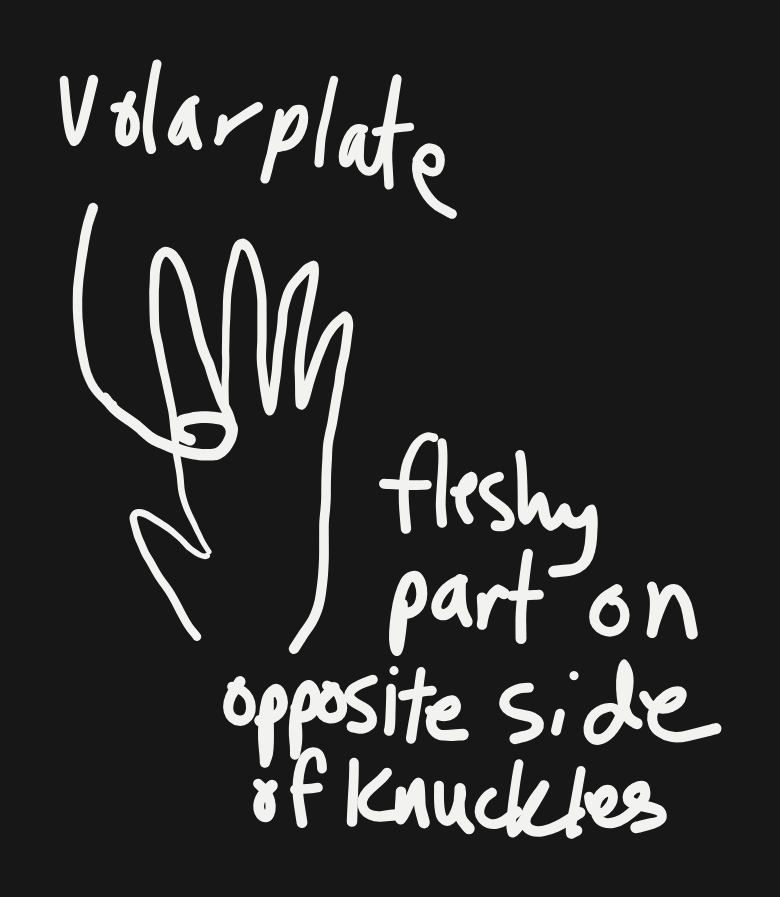
- Volar Plate: Fibrocartilage structure preventing pinching of flexor tendons during joint flexion.
- Collateral Ligaments: Y-shaped ligaments providing stability, loose in extension and tight in flexion.
Musculature of the Thumb
Extrinsic Muscles
- Flexor Pollicis Longus (FPL):
- Function: Flexes IP, MCP, and CMC joints.
- Location: Crosses CMC, MCP, and IP joints.
- Extensor Pollicis Longus (EPL):
- Function: Extends IP joint.
- Location: Crosses IP, MCP, and CMC joints.
- Extensor Pollicis Brevis (EPB):
- Function: Extends MCP and CMC joints.
- Location: Inserts on proximal phalanx.
- Abductor Pollicis Longus (APL):
- Function: Abducts thumb at CMC joint.
- Location: Inserts on radial side of thumb.
Intrinsic Muscles
- Adductor Pollicis:
- Function: Adducts thumb at CMC and MCP joints.
- Location: Encased within the hand.
- Flexor Pollicis Brevis (FPB):
- Function: Flexes MCP and CMC joints.
- Location: Inserts on proximal phalanx.
- Opponens Pollicis:
- Function: Rotates and opposes thumb.
- Location: Wraps around the metacarpal bone.
Phases of Thumb Opposition
- Initial Phase: Depending on girth, if grabbing an object, snuff box muscles may pull the thumb away from the palm.
- Opposition Phase: Preparing to grasp. Thenar muscles → thumb into palm:
- Abduction from abductor pollicis brevis
- Rotation from opponens pollicis
- Flexion from flexor pollicis brevis
- Pinch Down Holding Phase: Flexor pollicis longus and adductor pollicis provide strong grip.
- Release Phase: Snuff box muscles release the thumb.
Fingers
Joints | Extrinsic Muscles | Intrinsic Muscles | ||||
|---|---|---|---|---|---|---|
Flexor Digitorum Superficialis | Flexor Digitorum Profundus | Extensor Digitorum | Lumbricals | Dorsal Interossei | Palmar Interossei | |
2-4th Digit Carpometacarpal Joint (CMC) - Plane | ~Crosses this joint | ~Crosses this joint | ||||
Metacarpophalangeal Joint (MCP) - Condyloid | +Flexion ~Crosses this joint | +Flexion ~Crosses this joint | +Extension ~Crosses this joint | +Flexion ~Crosses this joint (extensor hood) | +Abduction | +Adduction |
Proximal Interphalangeal Joint (PIP) - Hinge | +Flexion ~Crosses this joint | +Flexion ~Crosses this joint | +Extension ~Crosses this joint (extensor hood) | +Extension ~Crosses this joint (extensor hood) | ||
Distal Interphalangeal Joint (DIP) - Hinge | +Flexion ~Crosses this joint | +Extension ~Crosses this joint (extensor hood) | +Extension ~Crosses this joint (extensor hood) | |||
Muscles Specific to 1st, 2nd and 5th Digits
Joints | Extrinsic Muscles | Intrinsic Muscles | |||
|---|---|---|---|---|---|
Extensor Indicis | Extensor Digiti Minimi | Abductor Digiti Minimi | Flexor Digiti Minimi | Opponens Digiti Minimi | |
2nd Digit Carpometacarpal Joint (CMC) - Plane | ~Crosses this joint | ||||
5th Digit Carpometacarpal Joint (CMC) - Saddle | ~Crosses this joint | ~Crosses this joint | ~Crosses this joint | Rotation for opposition ~Crosses this joint | |
Metacarpophalangeal Joint (MCP) - Condyloid | Extension ~Crosses this joint (extensor hood) | Extension ~Crosses this joint (extensor hood) | +Abduction ~Crosses this joint | +Flexion ~Crosses this joint | |
Proximal Interphalangeal Joint (PIP) - Hinge | Extension ~Crosses this joint (extensor hood) | Extension ~Crosses this joint (extensor hood) | |||
Distal Interphalangeal Joint (DIP) - Hinge | Extension ~Crosses this joint (extensor hood) | Extension ~Crosses this joint (extensor hood) | |||
Joints of the Fingers
- Carpometacarpal (CMC) Joint:
- Type: Plane joints (2nd-4th digits), saddle joint (5th digit).
- Movements: flexion/extension, abduction/adduction (5th digit).
- Metacarpophalangeal (MCP) Joint:
- Type: Condyloid joint.
- Movements: Flexion/extension, abduction/adduction.
- Interphalangeal Joints:
- Type: Hinge joint.
- Movements: Flexion/extension
- Locations:
- Proximal Interphalangeal (PIP) Joint: Second most distal knuckle of fingers.
- Distal Interphalangeal (DIP) Joint: Most distal knuckle of fingers.
Musculature of the Fingers
Extrinsic Muscles
- Flexor Digitorum Superficialis (FDS):
- Function: Flexes PIP joints.
- Location: Crosses MCP and PIP joints.
- Flexor Digitorum Profundus (FDP):
- Function: Flexes DIP joints.
- Location: Crosses MCP, PIP, and DIP joints.
- Extensor Digitorum:
- Function: Extends MCP, PIP, and DIP joints.
- Location: Inserts on extensor hood.
- Extensor Indicis:
- Function: Extends second digit
- Location: originates on dorsal surface of ulna and inserts onto
Intrinsic Muscles
- Lumbricals:
- Function: Flex MCP and extend PIP/DIP joints.
- Location: Origin at FDP tendons.
- Interossei (Dorsal and Palmar):
- Function: Dorsal (abduction), Palmar (adduction) of MCP joints.
- Location: Between metacarpals.
Soft Tissue Structures of the Fingers
- Joint Capsules: Contain synovial fluid.
- Volar Plates: Prevent pinching of flexor tendons.
- Collateral Ligaments: Provide stability to MCP, PIP, and DIP joints.
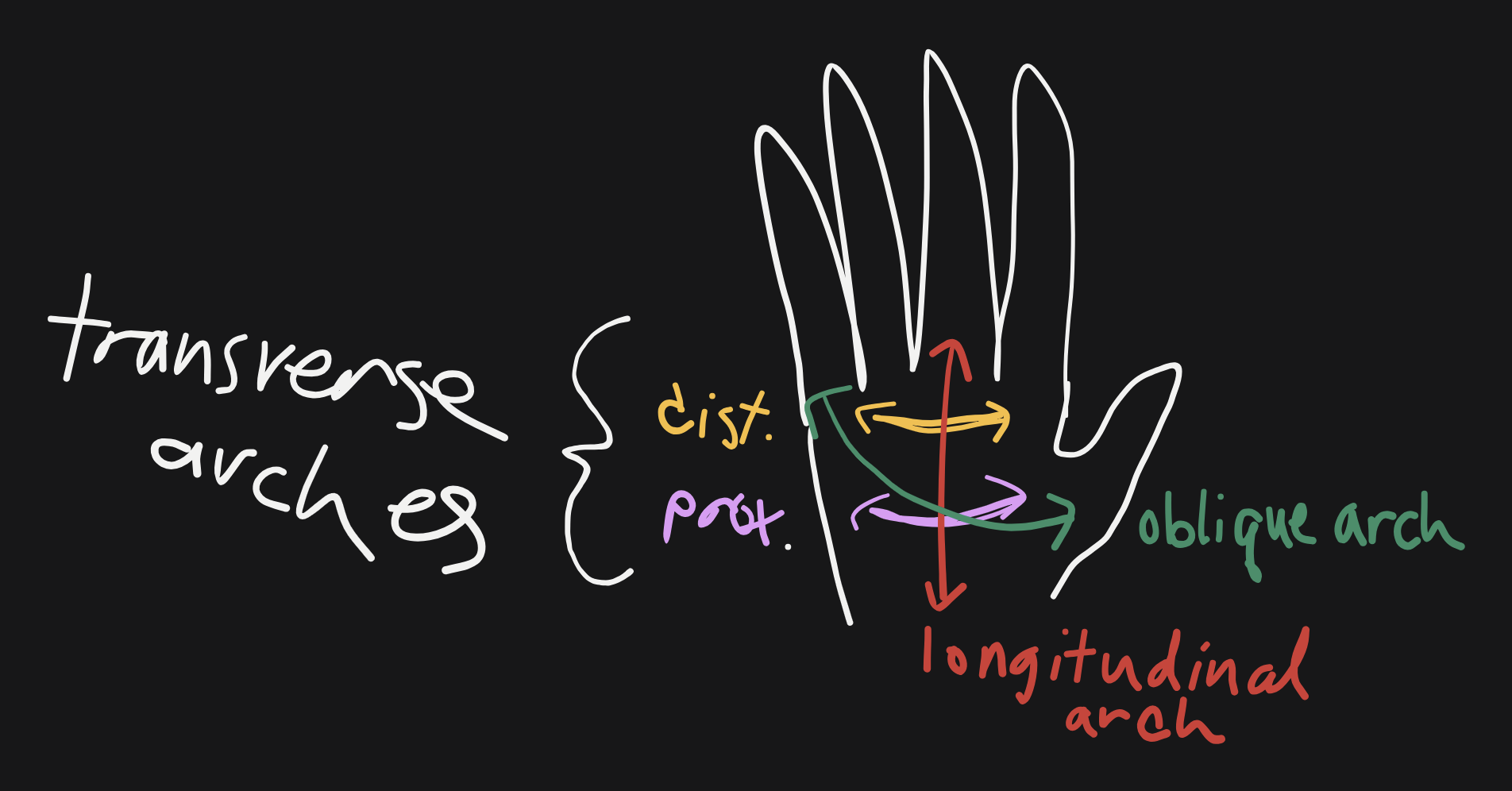
Arches of the Hand
- Longitudinal Arch: Extends from wrist to base of 3rd digit.
- Oblique Palmar Arch: Extends from thumb to 5th digit.
- Proximal Transverse Arch: Runs across the palm near the base of the metacarpals.
- Distal Transverse Arch: Runs across the palm at the level of the MCP joints.
Clinical Relevance
- Edema Management: Proper splinting and understanding of hand arches are crucial to prevent complications like reduced circulation and pain.
- Functional Implications: Hand arches enhance grasp stability, sensory input, and object manipulation.
Week 7: Extensor Hood Mechanism
This mechanism is what’s primarily causing extension of the proximal and distal interphalangeal joints (PIP and DIP, aka your two distal knuckles). It lets the hand have a variety of movements.
Components of the Extensor Hood Mechanism:
- Extensor Digitorum Communis (EDC):
- Tendons of the EDC are accompanied by Extensor Indicis (EI) and Extensor Digiti Minimi (EDM) of 2nd and 5th digits, respectively.
- Prime mover for Metacarpophalangeal (MCP) extension.
- Assists in Interphalangeal (IP) extension, but cannot extend IPs without other components of the extensor hood mechanism.
- Extensor Hood (Dorsal Hood):
- Consists of fibers from the Extensor Digitorum, Palmar and Dorsal Interossei, and Lumbricals.
- Breaks into one central tendon and two lateral bands.
- Extends the MCP joint and also contributes to MCP flexion when pulled distally.
- Conjoined Central Tendon (Central Slip):
- Comes out from the extensor hood (fibers from EDC, Interossei, and Lumbricals).
- Crosses the Proximal Interphalangeal (PIP) joint to the middle phalanx.
- Extends the PIP joint.
- Conjoined Lateral Bands:
- Arise from the extensor hood (fibers from the EDC, Interossei, and Lumbricals).
- Insert on the distal phalanx.
- Extend the Distal Interphalangeal (DIP) and PIP joints.
- Conjoined Terminal Tendon:
- Formed when the lateral bands converge.
- Inserts on the distal phalanx.
- Extends the DIP joint.
- Dorsal Interossei:
- Prime movers for abduction at the MCP when fingers are extended.
- Contribute to MCP flexion when fingers are flexed.
- Assist in PIP and DIP extension through their fibers going to the extensor hood, lateral bands, and central tendon.
- Palmar Interossei:
- Prime movers for adduction at the MCP when fingers are extended.
- Contribute to MCP flexion when fingers are flexed.
- Assist in PIP and DIP extension through their fibers going to the extensor hood, lateral bands, and central tendon.
- Lumbricals:
- Proximally attached to the Flexor Digitorum Profundus (FDP), pulling distally to release passive tension of the FDP.
- Distally attached to the lateral bands, extensor hood, and central tendon, pulling proximally for PIP and DIP extension.
- Located volarly at the MCP joint, thus facilitating MCP flexion.
- Triangular Ligament:
- Dorsally connects the two lateral bands.
- Prevents lateral bands from falling too volarly during IP flexion.
- Contributes to DIP extension through lateral bands when IP is extended.
- Oblique Retinacular Ligament (ORL):
- Proximally attached to the distal phalanx and digital tendon sheath, extending to the lateral bands.
- Slack when IPs are flexed, but tightens when IPs are extended, pulling proximally on the lateral bands to contribute to DIP extension.
Functions of the Extensor Hood Mechanism:
The extensor hood mechanism allows coordinated extension and flexion of the fingers, crucial for various hand functions like gripping objects, typing, and other fine motor skills.
Full Finger Extension:
- EDC extends MCP and causes tension on the extensor hood, lateral bands, and central tendon.
- Lumbricals release passive tension of the FDP.
- Dorsal and Palmar interossei extend the MCP and contribute tension to the extensor hood, lateral bands, and central tendon.
- Central tendon extends the PIP.
- Lateral bands extend PIP and DIP.
- Terminal tendon, triangular ligament, and ORL all contribute to DIP extension.
Injuries
Injuries to different parts of the extensor mechanism can lead to specific deformities such as:
- Mallet Finger: Due to tear in the terminal slip, causing extensor lag at the DIP joint.
- Boutonniere Deformity: Tear in the central slip, causing flexion at the PIP joint and hyperextension at the DIP joint.
- Intrinsic Minus Hand (Claw Hand)
- Appearance/Sign: Hyperextension of MCPs with flexed PIPs and DIPs.
- Cause: Paralysis or absence of intrinsic muscles, particularly the Lumbricals. The EDC can extend MCPs but without lumbricals, passive tension of the FDP is not released, preventing the transfer of tension to the extensor hood mechanism, leading to hyperextension of the dorsal hood, lateral bands, and central tendon.
- Intervention: Use a splint with a lumbrical bar to provide passive stretch of the FDP, enabling proper extension of PIP and DIP through the extensor mechanism .
Clinical Relevance
- Understanding the extensor hood mechanism helps in diagnosing and treating hand injuries and deformities.
- Various splints and interventions can be used to manage conditions arising from damage to the extensor mechanism.
Common Grasp Patterns
- Power Grips: Involve the whole hand and include the cylindrical and spherical grips.
- Cylindrical grip: Holding a bottle.
- Spherical grip: Holding a ball.
- Hook grip: holding a briefcase (thumb extended)
- Cylindrical grip: Holding a bottle.
- Precision Grips: Involve the thumb and fingertips.
- Pinch grip: Picking up small objects.
![]()
Summary
- The extensor hood mechanism is a complex and crucial part of hand anatomy that facilitates intricate finger movements.
- Each component of the mechanism has a specific role in the extension and flexion of finger joints.
- Injuries and pathologies affecting the extensor hood can significantly impact hand function, highlighting the importance of understanding this mechanism in clinical practice.
Week 6: Wrist
Introduction
- Importance of the wrist in daily activities: eating, dressing, leisure activities, washing, etc.
- Objectives:
- Learn the two joints of the wrist complex and their motions.
- Identify muscles and analyze their contractions.
- Understand synergistic effects of wrist muscles in movement.
- Discuss clinical considerations like carpal tunnel syndrome.
Overview of the Wrist Complex
- Wrist Functionality:
- Controls the length-tension relationship of hand muscles for fine adjustments (pinching, grasping).
- Optimal wrist extension (5-10 degrees) maximizes power; flexion or full extension reduces power.
Bones of the Wrist
- Carpal Bones:
- Proximal Row: Scaphoid, Lunate, Triquetrum, Pisiform.
- Distal Row: Trapezium, Trapezoid, Capitate, Hamate.
- Pisiform: Not part of the proximal row, serves as an attachment for the abductor digiti minimi, acts as an anatomical pulley increasing torque of the flexor carpi ulnaris (FCU).
Joints of the Wrist
- Radiocarpal Joint:
- Formed by the radius, radioulnar disc, and proximal row of carpals.
- Allows more flexion, extension, and ulnar deviation than radial deviation.
- Midcarpal Joint:
- Articulation between the proximal and distal rows of carpal bones.
- Allows for extension, flexion, and radial and ulnar deviation.
- Synovial joint with a loose but strong joint capsule reinforced by ligaments.
Ligaments of the Wrist
- Dorsal Radiocarpal Ligament:
- Connects radial styloid to lunate, stabilizes joint during flexion.
- Palmar Radiocarpal Ligament:
- Attaches radius to hand bones, maintains joint stability.
- Ulnar and Radial Collateral Ligaments:
- Assist in radial and ulnar deviation, stabilize wrist complex.
- Intercarpal Ligaments:
- Provide stability and mobility within the wrist.
- Flexor Retinaculum:
- Fibrous band located on the palmar side, creates a tunnel for nerves and tendons, protection.
- Compression leads to carpal tunnel syndrome, treated with Z-cuts to relieve pressure.
- Extensor Retinaculum:
- Fibrous band located on the dorsal side, prevents bowstringing of extensor tendons, maintaining muscle alignment.
Muscles of the Wrist
- Flexors:
- Flexor Carpi Radialis (FCR): Strong flexor, aids in radial deviation.
- Flexor Carpi Ulnaris (FCU): Strong ulnar deviator, aids in flexion.
- Palmaris Longus: Acts as an assistor, not present in 10-15% of the population.
- Extensors:
- Extensor Carpi Radialis Longus (ECRL): Aids in extension and radial deviation.
- Extensor Carpi Radialis Brevis (ECRB): Aids in extension and radial deviation.
- Extensor Carpi Ulnaris (ECU): Aids in extension and ulnar deviation.
Movements of the Wrist
- Radial Deviation: Proximal row slides ulnarly, distal row slides radially.
- Ulnar Deviation: Proximal row slides radially, distal row slides ulnarly.
- Flexion: Distal row rolls volarly, proximal row rolls dorsally.
- Extension:
- Distal row rolls dorsally, proximal row rolls volarly.
Synergistic Actions of Wrist Muscles
- Flexion: Performed by FCR and FCU.
- Extension: Performed by ECRL, ECRB, and ECU.
- Radial Deviation: Performed by FCR, ECRL, and ECRB.
- Ulnar Deviation: Performed by FCU and ECU.
Clinical Considerations
- Carpal Tunnel Syndrome:
- Compression of nerves under the flexor retinaculum, relieved by Z-cut surgery.
- Tenodesis Effect:
- Utilized in spinal cord injury patients for grasping objects by extending the wrist to create a grip.
Summary
- The wrist's complex structure and its ligaments, muscles, and joints allow for a wide range of movements essential for various functions and activities.
- Understanding the mechanics and clinical considerations of the wrist is crucial for effective diagnosis and treatment of related conditions.