HPFW CLASS NOTES.docx
Week 1: Theories, Vitals
Health Belief Model:
- Taking action on a health behavior depends on individuals perceptions of its cost and benefits
- 6 constructs
- Perceived:
- Susceptibility, severity, benefits, barriers
- Cue to action
- Self-efficacy (health motivation)
- Perceived:
Transtheoretical Model:
- 5 stage cyclic stages of behavior change
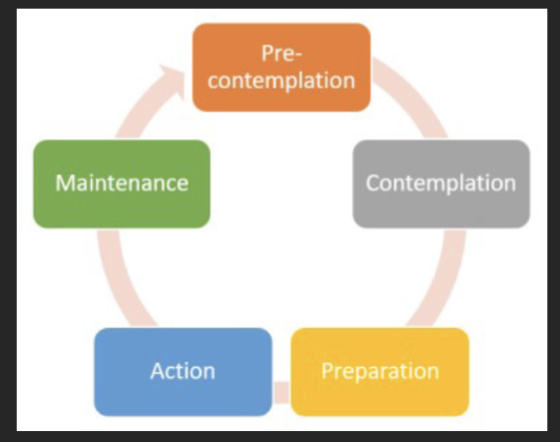
Preparation: within 30 days planning
Action: doing it for at least 6 months
Social Cognitive Theory:
- Learning occurs in a social context
- Behavior is influenced by personal, environmental, and behavioral factors
- 5 primary constructs:
- Psychological determinants of behavior
- observational learning, environmental determinants of behavior
- self-regulation
- moral disengagements (following)
- (perseverance)
- 4 methods:
- Mastery experience (sternest, set your patient up for success. Have your patient do something they feel confident in- achieving small goals. Mastery in their life while achieving things
- social modeling (mentorship, addiction recovery, if someone did it, you want to too)
- improving physical and emotional states (can you do something to make someone sleep/feel better, help someone with fatigue by making sure they sleep well- performance will go up)
- verbal persuasion (least strongest, saying that someone should exercise)
Self-determination Theory
- Meeting basic human needs: competence, autonomy (free will, involved in decisions- give then a choice, helps motivation), relatedness(feeling connected) - facilitates behavior change
- Motivation
- Intrinsic (personal reason, what you really want to do- more powerful
- Extrinsic (rewards, prize money)
- Motivation
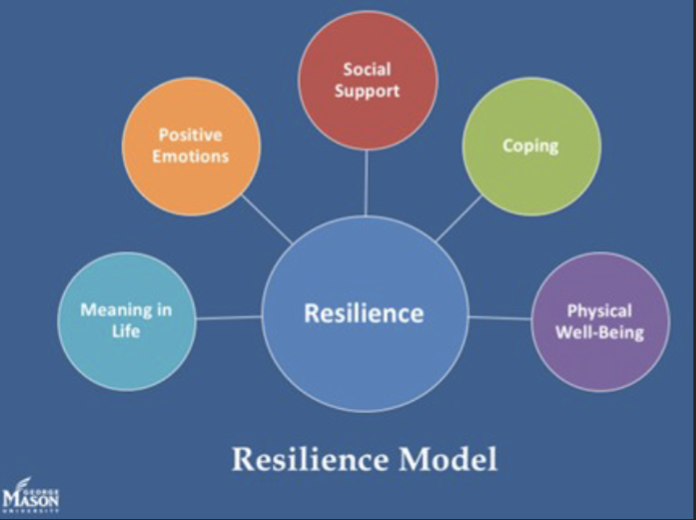
Resilience Theory
Pain:
- Pain is an unpleasant sensory and emotional experience
- It is whatever the patient says it is and exists wherever and whenever the patient say it does
- Self-report: of pain is the most reliable indicator or pain
- Each patient should be screened for pain on admission and asked is they have pain
- A pain screen is a quantitative rating of intensity of pain and is reported using a standardized instrument that has demonstrated reliability and validity
Week 2
Unit 2: Healthy People 2030 and moving, Pre-Post-exercise vitals
Prevention:
- Chronic conditions are often attributed to behaviors
Health:
- A state of complete physical, mental and social well being-
Healthy people 2030
Vision:
- A society in which all people can achieve their full potential for health and well being across the lifespan and live long, healthy lives
Mission:
- To promote, strengthen and evaluate the nations efforts to improve the health and well-being of all people
5 goals for Healthy People 2030:
- Attain healthy, thriving lives and well-being, free of preventable disease, disability, injury and premature death
- Eliminate health disparities, achieve health equity, and attain health literacy to improve the health and wellbeing of all
- Create social, physical and economic environments that promote attaining full potential for health and well-being for all
- Promote healthy development, healthy behaviors, and well-being across all life stages
- Engage leadership, key constituents, and the public across multiple sectors to take action and design policies that improve the health and well-being of all
355 core objectives divided into 5 topic areas
- Health conditions
- Health behaviors
- Population groups
- Setting and systems (healthcare falls in it)
- SDOH
- Leading Indicators of Health (LIH) are a subset of high-priority objectives that are selected drive action to improve health and well-being
5 key areas of the framework
- Health disparities
- Health equity
- Health literacy
- Wellbeing
- Social determinants of health
Social Determinants of health
- Economic stability (income)
- education access and quality (clean schools, good curriculum, dropout rate
- Health care access and quality (quality of the care, is the doc office too far)
- Neighborhood and built environment (safety, parks, or in city, opportunity for recreation, water and air quality, noise, smoke, food desert of places to find food)
- Social and community context (support systems, interactions with people, service groups)
- Include age, gender, social status, and social support
- Social risk factors are the adverse social conditions that may lead to poor health
Physical Therapist Role
Biopsychosocial Model
- A person’s health status is determined by the interplay of the biological, psychological and social domains
ICF Framework:
- International Classification of Functioning, disability and health
- Used by PTs to prevent, minimize, or eliminate impairments of body functions and structures, activity limitations, and participation restrictions by optimizing movement
Role of PTs
- Prevention
- PTs can facilitate behavior change to reduce risk factors in the individuals with whom they work with
- Movement Specialists
- PTs collaborate with physicians and other health care providers and fitness professionals to promote active lifestyles and reduce risk behaviors
- Consider the APTA vision statement, “transforming society by optimizing movement to improve the human experience”
- Optimal movement:
- Purposeful, efficient- especially in terms of energy expenditure- and reduces risk of injury or onset of impairment or disease
- Quality of life:
- Improves with the ability to move well
- Optimal movement:
Transformation
Physical Therapists can facilitate transformation of society through the typical practice of working with patients in rehabilitation after onset of injury or illness or after surgery
Education:
- Educating patients. Clients to enhance health and wellness
Improving physical literacy to promote optimal movement
- Include the components of motivation, confidence, physical competence, knowledge and understanding
Identifying community resources available to the client to support a healthy lifestyle, advocating for community systems and resources to support-health enhancing behaviors and environments
Advocating for reduction in health disparities
Starting and Stopping Exercise/ Testing
Starting exercise:
- Initial screen/evaluation; physical activity readiness Questionnaire for everyone (PAR-Q) and or provider clearness
- Absence of:
- Angina or angina like symptoms
- Shortness of breath, wheezing, leg cramps or claudication
- Signs of poor perfusion:
- Light headedness, confusion, ataxia, pallor, cyanosis, nausea, or cold and clammy skin
Stopping exercise:
- Onset of angina-like symptoms
- Drop in SBP >or equal to 10mmHg with an increase in work rate or if SBP decreases below the value obtained in the same position prior to testing
- Excessive rise in BP: systolic pressure >250 mmHg and or diastolic pressure >115mmHg
- Shortness of breath, wheezing, leg cramps or claudication
- Signs of poor perfusion: light headedness, confusion, ataxia, pallor, cyanosis, nausea or cold and clammy skin
- Failure of HR to increase with increased exercise intensity
- Noticeable change in heart rhythm by palpation or auscultation
- Individual requests to stop
- Physical or vernal manifestations of severe fatigue
- Failure of the testing equipment
Normal Response to Exercise
HR:
- Increases with progressive workloads at a rate of around 10 bpm per MET
SBP:
- Increases with increasing workloads at a rate of around 10 mmHg per 1 MET
DBP:
- Normally no change (or slight decrease)
Pulse OX:
- Should remain stable
RR:
- Increases with progressive workloads
Post exercise:
- SBP typically returns to pre-exercise levels (or lower) by 6 minutes or recovery
Week 3
PT’s in Primary Care
- Physician shortage may reach 120,000 by 2030
- Capabilities model:
- work at their full level of training, share responsibilities, get the right patient to right provider, timely
- identify recourses- match them to patient
- Barriers:
- Hight copays, Medicare lack of recognition (policy)
- We don’t want to replace but help within our scope to triage and refer
- Important to know IP team members roles
PT’s in the ER
- Gait training
- Assistive device fitting
- Discharge needs assessment/ disposition planning
- Vertigo
- Early neurologic assessment
- More
Our Value in Emergency Care
- Wait time (1/2 with PT involved) less and shorter length of stay (LOS)
- Decreased hospital admissions, less LOS and $ (falls, mobility)
- Less readmissions for falls and MSK disorders.
- Increased patient satisfaction; value in care and education provided.
- Patient Outcomes: LBP; less immobilization, meds, improved function.
- MD acceptance and value on education, safety, prevention, gait training,
pain alternatives and D/C planning. Network! Advocate! - MSK Dx: as effective, Dx concordance, time efficient, less referrals.
- Good interrater agreement with physicians.
- Evidence Based guide: judicious imaging, meds, early mobility
- Opioid crisis and alternative Rx’s for pain.
- Cost: $ PT as extra service vs type of service.
- Still, we decrease : less time, imaging, referral, meds, return to work
Primary Health Services Enhancement Act (H.R. 5365)
- Position The APTA strongly urges Congress to pass the Primary Health Services
Enhancement Act (H.R. 5365). This bipartisan legislation would expand patient
access to essential PT services to children and adults who receive care at
rural health clinics and federally qualified health centers, also known as
community health centers (CHCs). H.R. 5365 was introduced by Reps Ron
Kind, D-Wis, Diana DeGette, D-Colo., Jackie Walorski, R-Ind., and Don Bacon R-
Neb. - Background CHCs provide primary health services to more than 30 million
people in over 12,000 rural and urban communities across America, including
nearly 3 million Medicare beneficiaries and one in five Medicaid beneficiaries.
These facilities provide a lifeline to communities in need of essential health
services whose barriers to health care include, cost, lack of insurance, distance,
and language. Presently, CHCs offer a range of health services, including
access to physicians, advanced practice nurses, dentists, clinical
laboratory, emergency medical, behavioral health, and COVID-19 testing
and vaccine distribution. However, CHCs are restricted in how physical
therapy services are provided and reimbursed. - Pain Management and COVID-19 Between 2015 and 2018, 73% of CHCs reported
an increase in opioid use disorder, and 69% reported an increased number of
patients addicted to prescription opioids. This abuse is widespread in rural and
medically underserved areas where CHCs are often the only option for medical
care. COVID-19 has caused health, social, and economic stress that has
exacerbated the opioid epidemic. This legislation would afford Medicare and
Medicaid beneficiaries greater access to their physical therapy benefit.’’
*we are not reimbursed (main point)
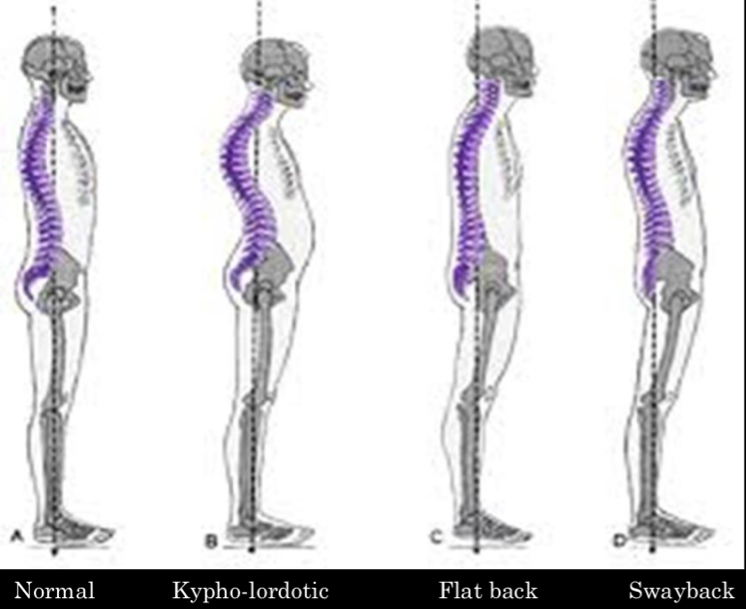
Posture:
- Observing your patients when they aren’t looking
Seated Posture
- Switch sitting positions often
- Take brief walks around your office or home
- Gently stretch your muscles every so often to help relieve muscle tension
- Don't cross your legs; keep your feet on the floor, with your ankles in front of
your knees - Make sure that your feet touch the floor, or if that's not possible, use a footrest
- Relax your shoulders; they should not be rounded or pulled backwards
- Keep your elbows in close to your body. They should be bent between 90 and 120
degrees. - Make sure that your back is fully supported. Use a back pillow or other back
support if your chair does not have a backrest that can support your lower
back's curve. - Make sure that your thighs and hips are supported. You should have a well-
padded seat, and your thighs and hips should be parallel to the floor.
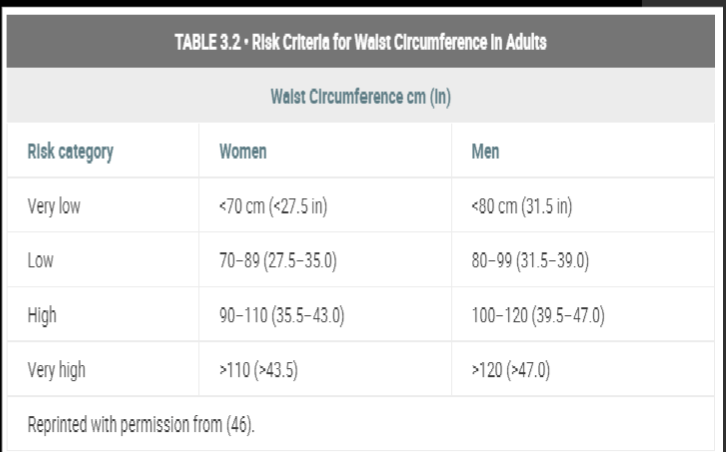
Weist Circumference
Android Fat Distribution
- Excess upper body/visceral fat (central fat) associated with metabolic complications
- HTN T2DM, CVD, dyslipidemia, sleep, apnea
Gynoid Fat Distribution
- Lower body fat associated with reduced metabolic complications
- Hips area
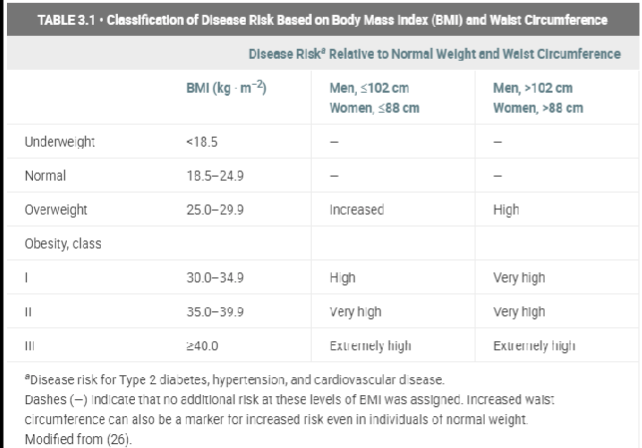
BMI (weight in kg / height in m^2)
- To test for quick/ convenient but no distribution for muscle mass, bone density, body type, fat distribution, racial or gender differences
Anthropometric Measures
- Height/Weight
- BMI
- Circumference
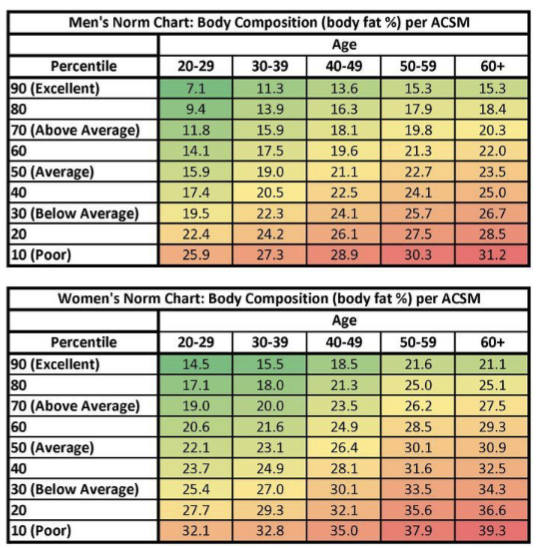
- Body fat composition
Body Fat Percentage Calculation by Skinfold Measurement
- Better estimates body fat percentage +/- accurate as around 1/3 of fat is subcutaneous
- Variations with age, sex, race, training
- Other options:
- Densitometry
- DEXA scan
- Bioelectrical impedance
- Body density formula
- 1.109380 – (0.0008267 × sum of three skinfolds) + (0.0000016 × [sum of
three skinfolds]2) – (0.000257 × age)
- 1.109380 – (0.0008267 × sum of three skinfolds) + (0.0000016 × [sum of
- Jackson-Pollock 3-site formula
- Women: triceps, suprailiac, thigh
- Men: chest, abdomen, thigh
Week 4