|
| | Action potentials- Action potential: The membrane is reversed (from negative to positively charged) Very quick (~1millisecond) Action potentials are all-or-none-responses
Ionic basis- Resting potential: voltage gated ion channels are closed Depolarisation: Na+ (sodium ion) channels open, rapid influx of Na+ into cell Peak: Na+ channels begin to close, K+ (potassium) channels open Repolarisation: Na+ stops entering cell, K+ ions move out Hyperpolarisation: K+ channels start to close but some K+ ions continue to move out of cell
Refractory period- the potential after the signal has been sent Absolute refractory period - brief period when it is impossible to generate an action potential Relative refractory period - higher than normal levels of stimulation required to generate an action potential
Refractory period is responsible for: Direction of travel - soma to axon
Rate of firing - indicating strength of stimulus
Weak stimulus will not generate an action potential until relative refractory period has ended Conduction along the axon (propagation) Travel along the axon of the neurone depolarising the axon as it goes In grey matter - active process: none-decremental As with AP generation, the conduction of AP along the axon occurs dues to the influx of sodium
Myelinated axon Saltatory conduction - within the myelinated sections of the axon the signal is conducted passively (therefore decrementally) without requiring opening of channels. This has an augmenting effect on efficiency and speed of transmission. Summary of PSPs and Aps- Neurons are polarised due to an imbalance of ions on either side of the membrane Binding of a neurotransmitter at its receptor contributes to either an Excitatory or Inhibitory post-synaptic potential and changes the degree of polarisation Summation (temporal or spatial) determines the overall response of the postsynaptic neurone If membrane potential exceeds the threshold of excitation an action potential fires which is propagated along the neuron Saltatory conduction increases speed of signalling in myelinated axons A refractory period follows an action potential which dictates the direction of travel and restricts how often the cell can fire
| |
| | Brain plasticity Sometimes referred to as neural plasticity/neuroplasticity Refers to changes in the micro (cellular) and macro (global) structures of the brain Changes result from alterations in neural pathways and synapses
Brain plasticity changes are a natural part of our growth and development. But they also occur- Historical perspective- The immutable brain Traditional view (until 1970's) of medical science was that brain structure remained relatively immutable after a critical period of development during early childhood Now research evidence supports the theory that many aspects of brain structure and function are plastic in adulthood
The degree of plasticity is the subject of considerable research: "Brain plasticity"- William James (1842-1910) N American psychologist and philosopher- brain functions are not fixed throughout life (James, Principle of Psychology, 1890) Mechanisms of Brain plasticity There are a variety of reasons which necessitate brain plasticity changes throughout the lifespan Brain development Degeneration
But others may be dependent on environmental factors or external changes Brain plasticity likely utilises some distinct and overlapping mechanisms to elicit these various changes in brain structure Hebbian theory Sometimes Hebb's Law or Hebbian learning Donald Hebb (1904-1985) Canadian psychologist He postulated that brain structure could be adapted as a result of its function "…two cells or systems of cells that are repeatedly active at the same time will tend to become 'associated,' so that activity in one facilitates activity in the other." - Hebb, D.O (1949) the organisation of behaviour: a neurophysiological theory. "Neurons that fire together, wire together. Those out of sync fail to link" Importantly this refers to SYSTEMS as well as CELLS
Brain development Structural Changes in the 'growing' Brain Synaptic Pruning At birth each neuron in the babies cerebral cortex has approximately 2500 synapses per neuron This number rapidly expands in a period of post-natal development as babies brain is flooded with sensory information. Peaking in young children at up to 15,000 synapses per neuron As we progress towards adulthood the number of synaptic connections are steadily reduced The resulting synaptic connections are more efficient Pruning may represent the learning process Pruning can occur (to a lesser extent than childhood) throughout the lifespan
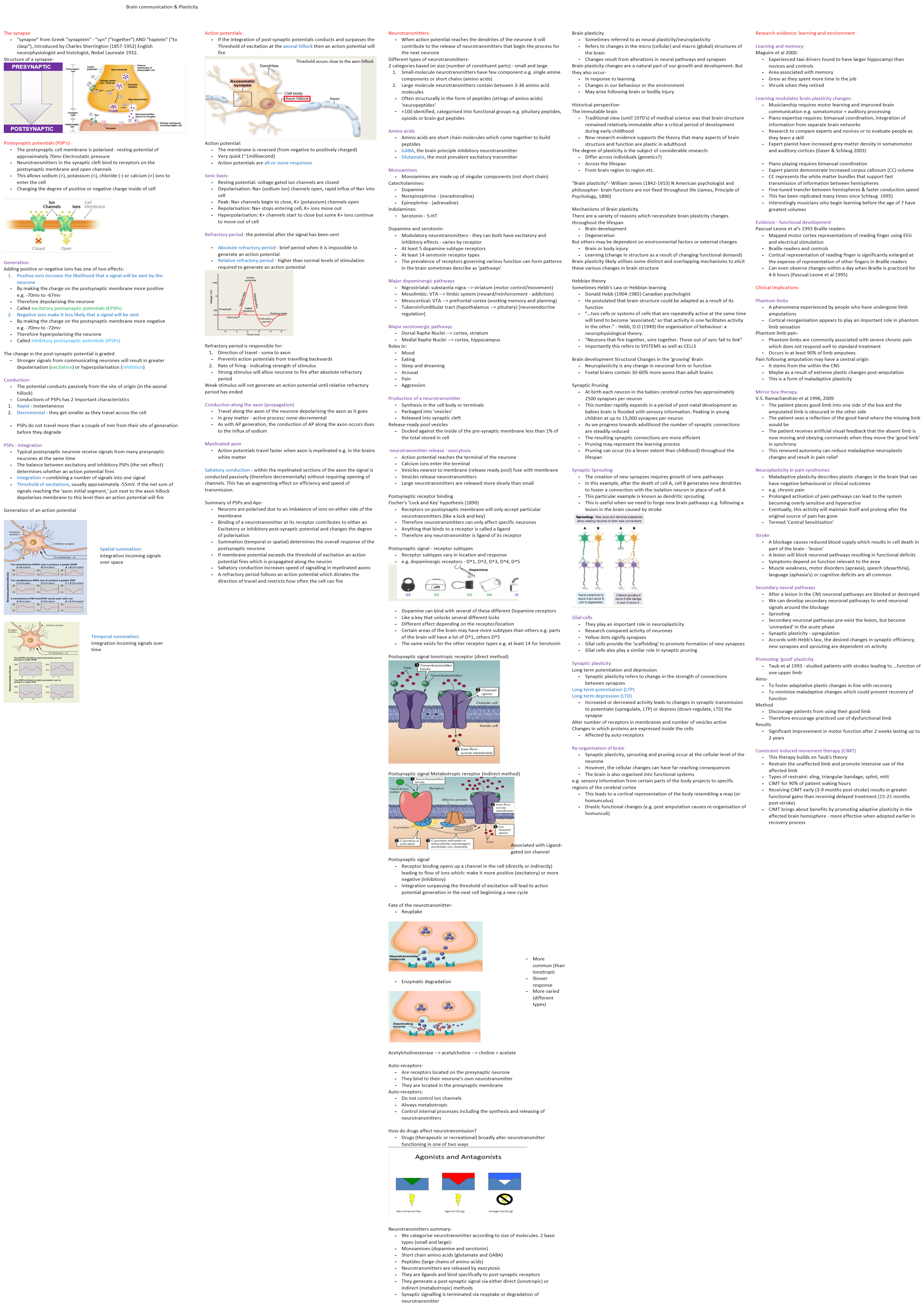
Synaptic Sprouting The creation of new synapses requires growth of new pathways In this example, after the death of cell A, cell B generates new dendrites to foster a connection with the isolation neuron in place of cell A This particular example is known as dendritic sprouting This is useful when we need to forge new brain pathways e.g. following a lesion in the brain caused by stroke
Glial cells They play an important role in neuroplasticity Research compared activity of neurones Yellow dots signify synapses Glial cells provide the 'scaffolding' to promote formation of new synapses Glial cells also play a similar role in synaptic pruning
Synaptic plasticity Long term potentiation and depression Long term potentiation (LTP) Long term depression (LTD) Alter number of receptors in membranes and number of vesicles active Changes in which proteins are expressed inside the cells Re-organisation of brain Synaptic plasticity, sprouting and pruning occur at the cellular level of the neurone However, the cellular changes can have far reaching consequences The brain is also organised into functional systems
e.g. sensory information from certain parts of the body projects to specific regions of the cerebral cortex | | Research evidence: learning and environment Learning and memory- Maguire et al 2000: Experienced taxi drivers found to have larger hippocampi than novices and controls Area associated with memory Grew as they spent more time in the job Shrunk when they retired
Learning modulates brain plasticity changes- Musicianship requires motor learning and improved brain communication e.g. somatomotor + auditory processing Piano expertise requires: bimanual coordination, integration of information from separate brain networks Research to compare experts and novices or to evaluate people as they learn a skill Expert pianist have increased grey matter density in somatomotor and auditory cortices (Gaser & Schlaug 2003)
Piano playing requires bimanual coordination Expert pianist demonstrate increased corpus callosum (CC) volume CC represents the white matter bundles that support fast transmission of information between hemispheres Fine-tuned transfer between hemispheres & faster conduction speed This has been replicated many times since Schlaug 1995) Interestingly musicians who begin learning before the age of 7 have greatest volumes
Evidence - functional development Pascual-Leone et al's 1993 Braille readers Mapped motor cortex representations of reading finger using EEG and electrical stimulation Braille readers and controls Cortical representation of reading finger is significantly enlarged at the expense of representation of other fingers in Braille readers Can even observe changes within a day when Braille is practiced for 4-6 hours (Pascual-Leone et al 1995)
Clinical implications Phantom limbs Phantom limb pain- Pain following amputation may have a central origin It stems from the within the CNS Maybe as a result of extreme plastic changes post-amputation This is a form of maladaptive plasticity
Mirror box therapy V.S. Ramachandran et al 1996, 2009 The patient places good limb into one side of the box and the amputated limb is obscured in the other side The patient sees a reflection of the good hand where the missing limb would be The patient receives artificial visual feedback that the absent limb is now moving and obeying commands when they move the 'good limb' in synchrony This renewed autonomy can reduce maladaptive neuroplastic changes and result in pain relief
Neuroplasticity in pain syndromes Maladaptive plasticity describes plastic changes in the brain that can have negative behavioural or clinical outcomes e.g. chronic pain Prolonged activation of pain pathways can lead to the system becoming overly sensitive and hyperactive Eventually, this activity will maintain itself and prolong after the original source of pain has gone Termed 'Central Sensitisation'
Stroke A blockage causes reduced blood supply which results in cell death in part of the brain - 'lesion' A lesion will block neuronal pathways resulting in functional deficits Symptoms depend on function relevant to the area Muscle weakness, motor disorders (apraxia), speech (dysarthria), language (aphasia's) or cognitive deficits are all common
Secondary neural pathways After a lesion in the CNS neuronal pathways are blocked or destroyed We can develop secondary neuronal pathways to send neuronal signals around the blockage Sprouting Secondary neuronal pathways pre-exist the lesion, but become 'unmasked' in the acute phase Synaptic plasticity - upregulation Accords with Hebb's law, the desired changes in synaptic efficiency, new synapses and sprouting are dependent on activity
Promoting 'good' plasticity Aims- Method Results Constraint-induced movement therapy (CIMT) This therapy builds on Taub's theory Restrain the unaffected limb and promote intensive use of the affected limb Types of restraint: sling, triangular bandage, splint, mitt CIMT for 90% of patient waking hours Receiving CIMT early (3-9 months post-stroke) results in greater functional gains than receiving delayed treatment (15-21 months post-stroke) CIMT brings about benefits by promoting adaptive plasticity in the affected brain hemisphere - more effective when adopted earlier in recovery process
|