Neurotransmitters
Axon & Synapse Function
Resting Membrane Potential: Value of potential across the membrane when a neuron is not transmitting information
- Steady-state condition with no NET FLOW of ions across the membrane…no change in the distribution of ions across the membrane, although individual ions may move across through leaky channels
- A neuron at rest = a capacitor, separation of the electrical charges on either side of the plasma membrane
- unequal distribution of ions is necessary for the neuron to be excitable
Electrical Potential: difference in electrical charge carried by ions
- Rapid change in electrical charge across the membrane → transmits info/signal along the axon → release of chemical transmitters
Flow of Information in a Neuron
- Signals (neurotransmitters) enter through the dendrite and converges on the axon hillock
- Signals are summated and converted to an action potential (AP)
- An “All-or-Nothing” action potential is sent down the axon
- Communication between the pre-synaptic & post-synaptic cells
Propagation of Information by Neurons
Four types of membrane channels allow ions to flow across the membrane
- Leaky channels
- Modality-gated channels: activated bye physical change…ex: temperature, pressure, etc.
- Ligand-gated channels: ion/neurotrransmitter molecule binds to a receptor on the surface of a channel
- Voltage-gated channels: electric current (ion flow) dependent
* Gated: the channel will open ion response to a stimulus
Synapse Mechanics
Chemical vs Electrical
Chemical: where we see synaptic vesicles holding the neurotransmitters travel through the presynaptic membrane, then released into the synaptic cleft to bind to the receptors on the postsynaptic membrane
Electrical: typically seen as communication through gap junctions, where we see electrical/ion flow dependent channels
Chemical Synapse
3 components: Presynaptic axon, presynaptic terminal, postsynaptic cell
- Action potential travels down presynaptic axon to the presynaptic terminal
- Once the AP reaches the presynaptic terminal it opens the Ca2+ channel and the influx of Ca2+ pushes the vesicles carrying the neurotransmitters out
- The vesicles will “pop” releasing the neurotransmitters into the synaptic cleft where they will flow and bind to its receptors on the postsynaptic cell (the dendrite)
- The binding → alters the postsynaptic cell function
- Direct Activation of ion channels = ONLY ONE RESPONSE per synapse/cell
Excitation vs Inhibition
The neurotransmitters that travel through the synapse can influence the next cell/nerve in one of two ways…
- Excitatory
- Inhibitory
- Excitatory: elicits a response
* vesicles appear to be round clear or have a dense core
* postsynaptic thickening will occur (asymmetrical)
* prevalent on distal dendrites - Inhibitory: inhibits the response
* multiform or oval(ish) vesicles
* Symmetrical pre/post membranes
* prevalent on the soma, proximal dendrite and axon terminal - Postsynaptic membrane, changes in membrane potential are either Excitatory (local depolarization) or Inhibitory (local hyper-polarization)
- Inhibition by Chloride Hyper-polarization: neurotransmitter stimulates Cl- channel to open, the negative change of CL- hyper-polarizes the neuron, causing the membrane potential to be lower than normal requiring additional stimulation to reach action potential
- Presynaptic Facilitation & Excitation: more neurotransmitters are released …happens as the presynaptic axon releases that slightly depolarize the axon terminal on the second axon
* changes the amount and type of neurotransmitter released
* happens a lot on in the cerebellum
* modifies the job so that the muscle activity is an appropriate response - Presynaptic Facilitation and Inhibition: less neurotransmitter is released…occurs when the axon releases neurotransmitters that hyper-polarize the second axon
- Types of synapse endings:
* Terminal passant: precision, found in motor system (1to1)
* Bouton passant: mass communication, found in the cerebellum & other locations (memory sensors)
Interactions b/w Neurons
- Divergence & Convergence contribute to the distribution of information throughout he nervous system
* Convergence: MULTIPLE INPUTS from a variety of cells terminate on a single neuron (loose one there are “backups”)
* Divergence: a single neuron with many branches that end on many cells (ex: within the cerebellum…recovering from polio is dependent on divergence, maintaining posture…communication to many muscles, loss of one neuron=major effect)
Why is inhibition more prevalent?
* Because in order to produce a productive and reasonable outcome there must be a component of inhibition to balance the amount of excitation
Neuromodulation
Neuromodulators: alter neural function by acting away from (not directly on) the synaptic cleft
- effects have a slow onset but usually last longer (minutes to days long) than the effect of neurotransmitters (happens in seconds)
* Substance P “pain neurotransmitter released during cell damage”..involved in pain perception, released into extracellular space
* diffuses into the extracellular fluid → stimulate multiple neurons - G-Protein Modulators - receptor indirect ion channel activation
* modifies the receptor on the postsynaptic cell to change the function and sends a new/modified signal to next cell → can cause multiple responses in one cell
* Binding to multiple sites can be more efficient in large responses (amplifies the signal) - Ligand gated receptor
* receptor channels → briefly opens ion →causing local depolarization/hyper-polarization of membrane - Receptor Regulation: Dendrite mediated
* Cells regulate activity in several ways
* In response to frequent stimulation by a ligand, cell will decrease receptor activity by…
* receptor internalization (to much stimulation the cell will slowly shut down)
* receptor inactivation (drug tolerance can be due to lack of receptors)
* Overstimulation of postsynaptic receptors can cause a decrease in the number of receptors at the surface
* activated receptors are internalized when part of postsynaptic membrane folds into the cell
* Inactivation leaves the total number of receptors at the membrane constant but switches off (they can come back because the system has plasticity)
Myasthenia Gravis
- Grave muscle weakness: presents as fluctuating fatigue and weakness
- problem of the postsynaptic region of the neuromuscular end plate
- associated with a family history of autoimmune disease
- likely to see other autoimmune diseases ion these patients
* high incidence of thymic disease…demonstrates as thymic hyperplasia, 10-15% have thymomas - In MG there is a deficiency in the number of acetylcholine receptors at neuromuscular junction → clinically seen as muscle fatigue w/sustained or repeated activity
- Presenting symptoms
* Hoarse voice
* Difficulty chewing or swallowing
* Fatigue with talking (oropharyngeal muscles)
* Decreased respiratory function
* Drooping eyelids
* Double vision/eye movement fatigue
* Difficulty walking up stairs
* Muscles with small motor units are the muscles MOST AFFECTED (ocular muscles and hands)
* Overall facial weakness (almost always present) - Treatment Options
* Removing thymus/thymectomy: try to induce remission
* Plasmapheresis, corticosteroids and immunosuppressant drugs: reduce the levels of antibody to ACH receptor
* Increasing the amount of ACH available at the neuromuscular junction w/cholinesterase inhibitors (cholinesterase is responsible for the breakdown of ACH)
Neurotransmitters
Two types:
- Fast-acting: they act directly
* transmission takes 1/1000 of a second
* directly by activating ion channels - Slow-acting: they act indirectly
* transmission requires 1/10 of a second
* indirectly by activating proteins inside the postsynaptic neuron
Synaptic Receptors
Typically named for the transmitter/modulator they bind to, produce either direct or indirect actions
- Act directly: the receptor and ion channel make up a single functional unit
- Act indirectly: using a cascade of intracellular molecules to activate ion channels or other changes (multiple changes)
Specific Neurotransmitters: formulate different action in the nervous system
AMINES
- Dopamine (DA): affects motor activity, cognition, & behavior
- Norepinephrine (NE): plays a vital role in active surveillance by increasing attention to sensory information
- Serotonin: affects sleep, general arousal, cognition, perception, motor activity and mood
- Histamine: Concentrated in hypothalamus…autonomic functions
Cholinergic Pathways: Excitatory (+)
- Arise in the nucleus basalis → projects to Cortex & Fornix Hippocampus
- Important for learning and memory, involved w/Dementia
Dopaminergic Pathways: Excitatory (+)
- Arise from 2 sites
* Substantia Nigra → Corpus Striatum - Ventral Tegmental Area (VTA) → septum, amygdala and to cortex (frontal lobe)
Dopamine is important…
- Too little → Parkinson’s
- Too much → Schizophrenia
Noradrenergic Pathways: Excitatory/Mixed (+/-)
- Locus Ceruleus → moves rostrally in the Median Forebrain Bundle & supply broad areas of cortex
- Noradrenergic projections are thought to be important for learning and “plasticity” of the brain
Serotonergic Pathways: Excitatory/Regulatory (+/-)
- Arise from Raphe Nuclei → arise in the midbrain, runs in the Median Forebrain Bundle
- Serotonin plays a role sleep wake cycle and mood regulation
* Too little → depressed, use of an SSRI (inhibitor, leaves extra serotonin in the brain)
Amino Acids:
- Glutamate: (primary) fast excitatory transmitter of CN
* over activity of NMDA receptors may cause epileptic seizures
* MAIN EXCITATORY transmitter in CNS
* high levels → seizures
* Neuron death increases Glutamate Levels in CNS
* Excitotoxicity = neuron dies, releases Glu→ exciting neighboring neurons, too much excitement → overwhelmed neurons die (and the cycle repeats)
* “propagating problem” = increased metabolic demand → increased ischemia
* Seen in Brain injury & Stroke
* Damage leads to swelling and edema = pressure on all regions of the brain, lack of O2
* Glycine: inhibits postsynaptic membranes, mainly in the brainstem and spinal cord - GABA: slow-acting responses
* Linked to ion channels as a second messenger system
* inhibitory in the spinal cord
* MAIN INHIBITORY TRANSMITTER in CNS → Prevalent effects in the PNS
* Helps provide smooth controlled movements, w/out it very spastic movements and will “Stay On” all the time
Peptides
- Opioid Peptides: endorphins, enkephalins & dynorphins…feel good chemicals in our body
* inhibits neurons in the CNS that involved in pain perception - Substance P
* stimulates nerve endings at the site of injury…(supposed to balance out w/opioid peptides)
* increases sensation and awareness of pain
* PNS: released by nerve endings in skin, mm and joints
* CNS: released by substantial nigra, amygdala, hypothalamus & cerebral cortex
* increased levels → chronic pain syndromes
* NOT A SYNAPTIC RELEASE - Calcitonin gene-related peptide
- Endorphins (-)
* opioid receptors: inhibit pain signaling, runners high & can be activated by stress hormones
Other
- Nitric Oxide: regulates the vascular system in the periphery and also active in the brain …changes in pain perception
* does not require a receptor, just diffuses across the membrane - involved in persistent changes in the postsynaptic response to repeated stimuli and in cell deaths
Disorders of Synaptic Function: Channelopathy
- Disease involves dysfunction of ion channels
- In some cases causes epilepsy & migraines
- Channelopathies affecting skeletal muscles cause paralysis or slow relaxation following muscle contraction
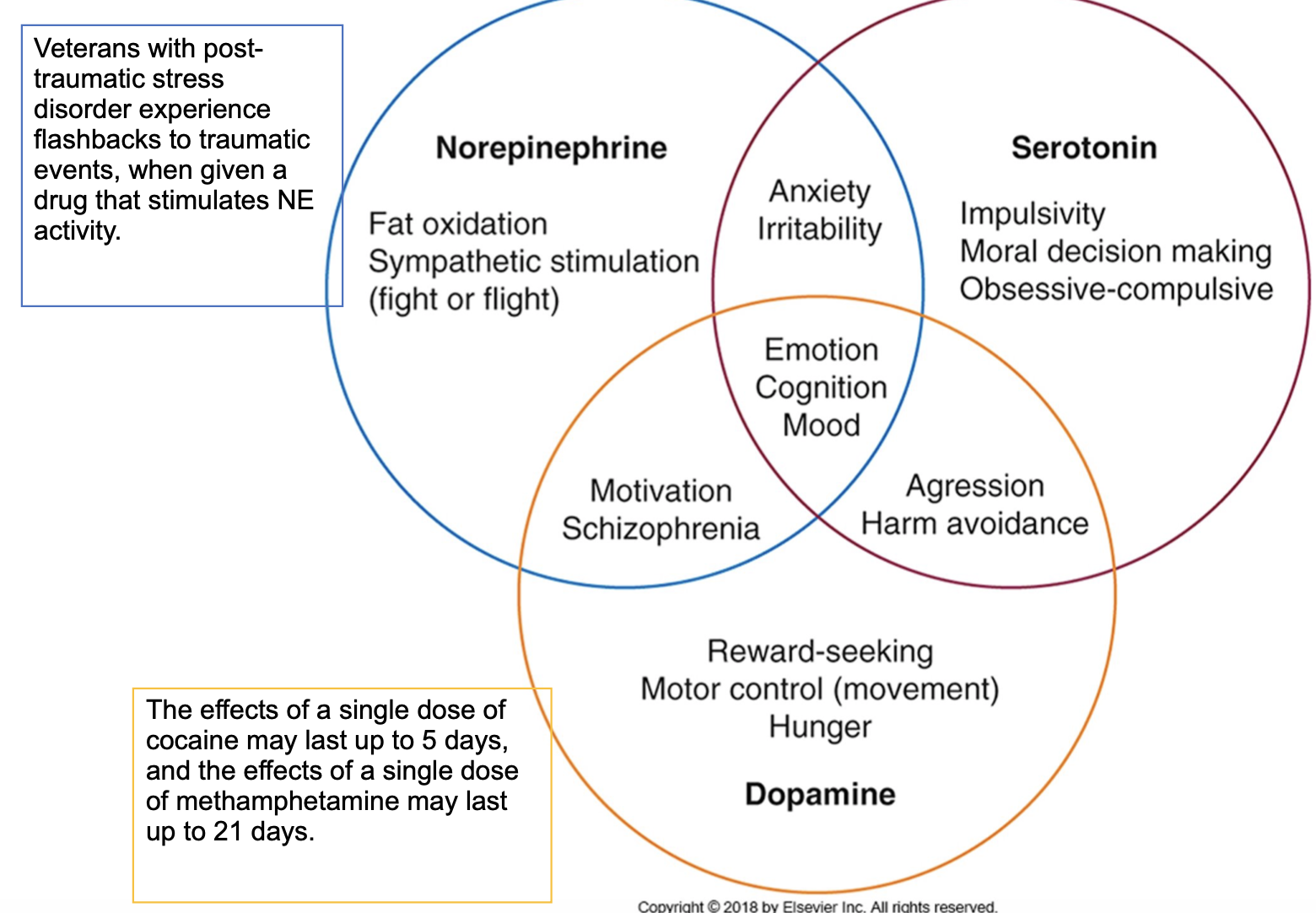
Clinical Application of Neurotransmitter
- Norepinephrine: Fat oxidation, sympathetic stimulation (fight or flight)
- Serotonin: Impulsivity, Moral Decision making, Obsessive-Compulsive
- Dopamine: Reward-seeking, Motor Control (movement), Hunger
- Norepinephrine, Serotonin & Dopamine → Emotion, Cognition & Mood
- Norepinephrine & Serotonin → Anxiety & Irritability
- Norepinephrine & Dopamine → Motivation & Schizophrenia
- Dopamine & Serotonin → Aggression & Harm avoidance