Week 3: The Cardio-Respiratory System – The Lungs
The Lungs:
- Size of about 4-6 litres, about the size of a basketball worth of space within lungs
- Larger the surface area, the more oxygen we can exchange.
- Surface area between 50-100 metres squared, which is about half a tennis court.
- If we put a sheet of plastic out over half a tennis court, we’d then be crumpling it up and trying to fit all the plastic within the size of a basketball. So huge surface area, allows us to have more exchange of gases.
- Chris Froom cyclist: At rest, around 6 litres of air will go in and out of his lungs. Like 3 bottles of coke
- At maximal exercise, this increases to somewhere between 150-200 litres. This is like two bath full of air within a minute.
4 key functions:
- Gas exchange: oxygen into system, co2 out of system
- Regulate PH: PH is acidity, we don’t want acidic blood.
- Protect ourselves from inhaled pathogens: lungs can filter the pathogens out so they are not getting in the system.
- Allow us to talk by forcing air through lungs and vocal cords allows us to talk
External respiration:
The movement of gases from the environment to the cells of our body.
- 4 processes to external respiration:
· Exchanges air between the atmosphere between the atmosphere and the lung.
· Exchanges oxygen and carbon dioxide between the lungs and blood.
· Transport oxygen and carbon dioxide in blood
· Exchange gases between blood and cells.
Anatomy of the respiratory system:
First step of respiratory system – getting air from environment into lungs.
- We have a muscular and bone system.
- Important muscles:
Ø Intercostals – muscles in between ribs
Ø Diaphragm – large flat muscle that sits at the bottom of rib cage.
Ø Scalene – muscle that attached from neck to top of clavicle.
Ø Abdominal muscles
- Our respiratory system can be split into an upper and lower respiratory system:
- Upper respiratory system:
Ø Nasal cavity
Ø Vocal cords
Ø Larynx (voice box)
Ø Pharynx (throat)
- Lower respiratory system:
Ø Trachea
Ø Bronchus and bronchioles
- This is an external view of our lungs.
- Trachea and bronchiole coming down into lungs,
- Lungs fill most of the top of our chest.
- This notch is what the heart sits in.
- The right lung is divided into 3 lobes.
- The left lung is divided into 2 lobes.
|

- This is viewing down on the lungs.
- We have two-layer plural membranes.
- The outer layer is attached to the rib cage.
- Inner layer covers the lungs.
- The Pleural cavity is the space in between the two plural membranes.
- In the pleural cavity it is filled with liquid.
- This liquid provides a slippery surface, which ensures the lungs don’t get damaged by touching the rib cage.
- Another thing this liquid does is that it holds the lungs close to the rib cage. This means that the lungs can follow, expand and contract along with the rib cage.
- The liquid makes it easy for the lungs to move up and down because it is like a slippery surface.
- However, it would be difficult to pull these apart because of water tension.
- Airway has several different processes:
· They warm air, we don’t want cold air going into the alveoli for two reasons:
- Can affect core body temperature.
- Can damage alveoli.
· Add water vapour, this will add moisture to the air as it goes down the respiratory tract.
· Humidity and moisture allow us to do gas exchange later.
· Filters out foreign materials like pathogens
- This is done by a layer of mucus which covers all of this.
- The mucus is sticky, and any pathogens will stick to it.
- We can then push the mucus up and get rid of it.
· Doesn’t do any gas exchange, just moves air down until it reaches the alveoli.
- Alveoli allows us to do gas exchange.
- Alveoli are like sacks, by being like small balls it increases the surface area. The larger the surface area, the more exchange
- Almost 80-90% of the surface areas is going to be covered by blood vessels.
- This means it is very efficient at taking oxygen from the alveoli to the circulatory system and getting carbon dioxide out the respiratory system and back through the lungs.
- The other part that makes this system effective is how thin the membrane is.
- Very small diffusion distance.
- The smaller the diffusion distance the easier it is the oxygen through the membrane and the carbon dioxide out the membrane.
Gas Laws – how gases behave. Important to how lungs function to move gases in and out of the system.
1) Boyles Law: P1 X V1 = P2 X V2
Pressure is created by collisions of gases within a container.
- These gases are constantly moving.
- Each time one of these molecules of gases hits the side it will create pressure.
- The pressure is directly proportional to the size of the container.
- A smaller container, with the same amount of gas, equals more collisions so there is more pressure.
- Gases move down a pressure gradient.
- With the lungs, we get a change in the size of the container.
- Reducing the size and volume of container, will increase the pressure and force the gases out.
- This happens when we breathe out.
- When we breathe in, we increase the size of the lungs.
- This will increase the volume and drop the amount of pressure, and we now have high pressure versus low pressure.
- The gasses move down the pressure gradient and into the lungs.
- When we reduce the lungs again, that will reduce the volume and increase the pressure, which will force the gases out the lungs and back into the atmosphere.
2) Daltons Law: what makes up atmospheric pressure.
- The atmosphere is made up of several different gases.
- 78% of nitrogen
- 21% of oxygen
- 0.4% of carbon dioxide
- 0.96% other gases
- Atmospheric pressure is 760mm Hg. Hg = Mercury
- The pressure of all those gases come together to make up the atmospheric pressure.
- The total pressure of a mixture of gases = the sum of the pressures of the individual gases
- The pressure of an individual gas = partial pressure (Pgas)
- Partial pressures together make up atmospheric pressure.
PO2 = 21% of 760 mm Hg = 160mm Hg
- Individual gases move down a concentration (partial pressure) gradient.
- Move from an area of high partial pressure to an area of low partial pressure.
- In the left container oxygen has a partial pressure of 33mm Hg. Whereas in the right container it has 17mm Hg. So there is a high partial pressure area and a low partial pressure area.
- So, oxygen will move into the area with a low concentration.
- If you think of the left container being the alveoli, and the right being the blood.
- The alveoli have a higher partial pressure of oxygen than blood, so the oxygen will move down this partial pressure gradient.
- This will happen until it reaches equilibrium, the same partial pressure on both sides.
How do we use these gas laws to get moving air moving in and out of lungs?
- For air to move into the alveoli, pressure in the lungs must be lower than atmospheric pressure.
We do this by: Ventilation: Inspiration – allows air to flow into lungs.
- This is our lungs at rest.
- Diaphragm is raised.
- First thing we do is our diaphragm will contract; this makes it flatten.
- By flattening, it will pull the bottom of the lungs down, which will increase surface area of the lungs.
- The ribs also move up and out.
- This will increase the volume and reduce the pressure.
- This will draw air into the lungs.
Ventilation: expiration – involves gases leaving the lungs.
- The diaphragm will go from flat and contracted to being relaxed and pushed up.
Static Lung Volumes:
· Tidal volume: volume of air going in and out of the lungs with each breath.
- At rest tidal volume is about 0.5-1 litres per breath.
· Inspiratory Reserve volume: how much more we could breathe in.
- If we were breathing normally, then took a deep breathe, this would reduce inspiratory reserve volumes.
- At rest it is around 2.5/3.5 litres
- These volumes are always changing depending on how deeply we are breathing.
· Expiratory reserve volume: how much more we could breathe out.
- At rest it is around 1/1.5 litres.
· Forced Vital capacity: is our maximum inspiration and expiration, the largest breath we can do.
- Total lung capacity will always be larger than vital capacity, this is because there will always be a slight residual volume.
- This is because of the elastic nature of the lungs; we will never get the lungs fully emptying.
- Residual volume is around 1 litre.
- This will decline with age because we will have less elasticity.
Dynamic lung volumes
- How much air can we force out in an amount of time.
FVC = Forced Vital Capacity
FEV1 = Forced expiratory volume in one second
- This can show us if we have a normal lung function, or whether we have a problem with obstruction or restriction.
· Restriction
- Is going to lower our FVC.
- One thing that can cause this is fibrotic disease.
- Fibrotic disease will reduce the elasticity of the lungs, which will reduce the volume the lungs can expand.
- Would have a lower FEV1, but proportion would be the same as obstruction.
· Obstruction:
- An obstruction disease is asthma.
- FVC would be same as a normal lung volume but the amount you can get out within one second is lower.
- For normal lung volumes FEV1 is about 80% FVC, having asthma would make it much lower.
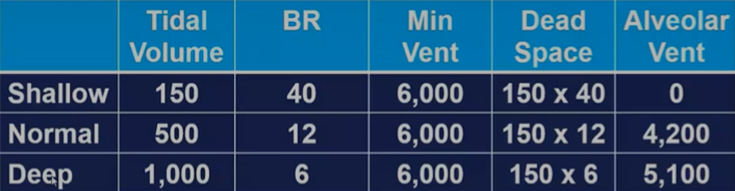
Pulmonary Ventilation:
Minute ventilation = tidal volume X breathing rate
- Tidal volume increases because we reduce our inspiratory and expiratory reserve volume.
- So, we breathe in and out slightly more.
However, Minute Ventilation is not a good indicator of how much fresh air reaches the alveoli.
A better equation for ventilation would be:
Alveoli ventilation = breathing rate X (tidal volume – dead space)