Study Guide Speech Path I - Lea + Bee
Speech Path 1 Final Study Guide:
- Hearing: the perception of sound, or in combination, the perception of speech
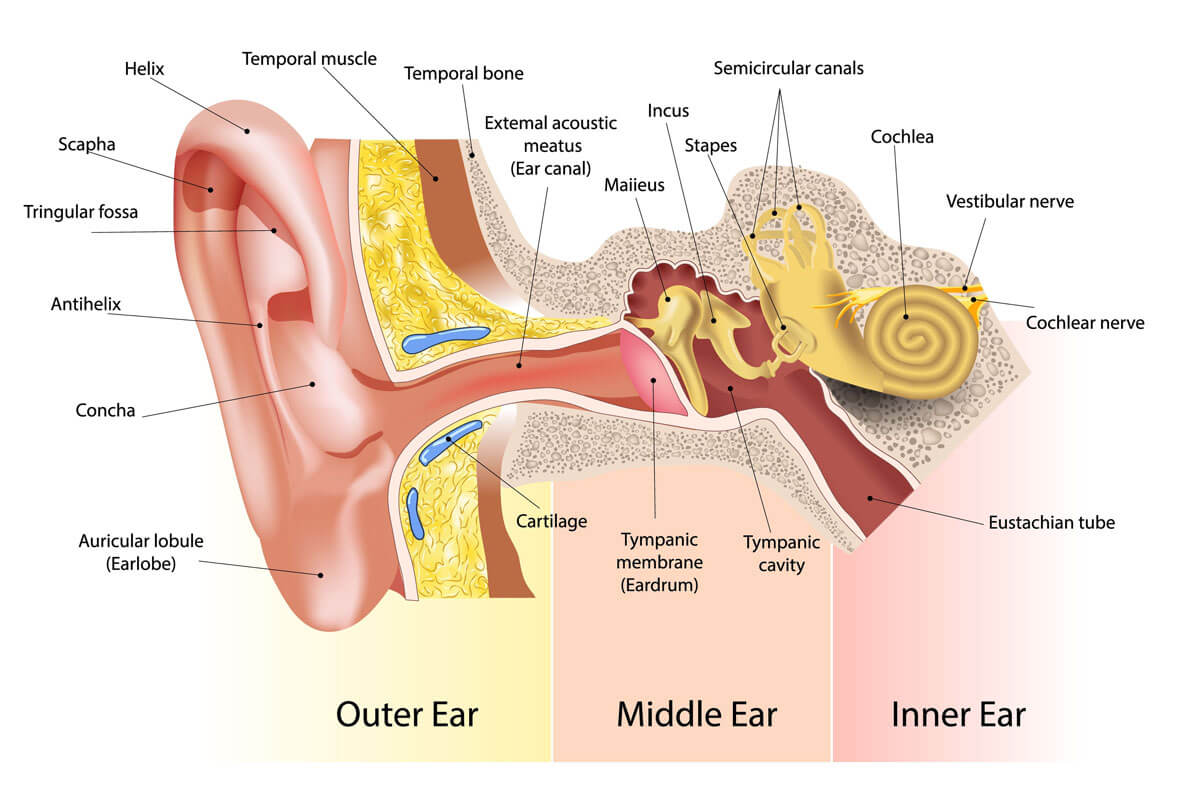
Three sections of Ear
- Inner ear: is a fluid-filled cavity inside the temporal bone that has three major cavities
* Vestibule Nerve
* Semicircular Canals
* Cochlear: Hearing Organ - Middle ear: The middle ear’s function is to communicate with the pharynx, equilibrates with external pressure and transmits the eardrum vibrations to the inner ear can be separated into:
* Hammer (malleus)
* Anvil (incus)
* Stirrup (stapes)
* Oval window
* Round window
* Eustachian tube
Outside ear:
- outer ear consists of the pinna, or auricle
* visible projecting portion of the ear
* external acoustic meatus
* outside opening to the ear canal
* external ear canal, which leads to the eardrum - outer ear concentrates air vibrations on the eardrum to make the eardrum vibrate
Hearing Loss
- Conductive Hearing Loss:
* Hearing loss that affects the middle and outer ear - Sensorineural hearing loss
* Affects the inner ear or the auditory nerve that connects the inner ear to the brain - Auditory Processing Disorder: affects the processing of sounds in the auditory center in the brain
Hearing Loss Affecting Language Development in 3 Domains of Language
- Semantics
* Children with hearing loss tend to learn nouns, but articles, conjunctions, and verbs are more difficult.
* Cause verbs + articles change, abstract
* Nouns = concrete, not abstract
* Syntax
* Common sense structures and word use = difficult
* Morphology
* Past tense -ed, plural, possessive -s, and p
* Present progressive -ing
* Difficult to hear ‘cuz they’re quieter
* Phonology
* Difficult for children with hearing loss to (accurately) produce the sounds they can’t hear
* Pragmatics
* Children with hearing loss miss parts of the conversation,
* Making it difficult for them to negotiate with peers
* Initiate communication with others
* Navigate turn taking
Without appropriate early intervention, children with hearing loss = at risk for poor academic achievement
Gap between children with + without hearing is on SLPs, audiologists, caregivers
- Etiology: cause(s) of a disease/condition
* Both genetic + environmental causes, age of onset + type of loss
* 50% is pediatric hearing loss = genetic
* Environmental factors
* Infection, injury or illness
* Noise-included hearing loss
Age of Onset + Causes
- Developmental: prelingual hearing loss
- Acquired: postlingual hearing loss
* after language has been acquired - Hearing Loss
* Conductive: damage to outer/middle ear
* Inner ear + cochlea in tact
* Sensorineural: damage to cochlea or auditory nerve
* Outer + inner ear in tact
* Mixed: both conductive + sensorineural - Unilateral: hearing loss in one ear
- Bilateral: hearing loss in both ears
- Causes of conductive hearing loss in children:
* Most common = Otitis media
* Starts with infectious organism, viral/bacteria, in pharyngeal area
* Infection makes way to Eustachian tube
* Which dysfunctions + negative pressure builds behind eardrum
* Fluid builds up + lining of middle ear cavity swells
* Fluid may eventually perforate/tear tympanic membrane
Can be temporary or permanent, affecting a person’s mood
Causes of sensorineural hearing loss in children:
* Genetics, Environment, + Exposure to Ototoxins
* Illness, infections, drug use, or other maternal problems during pregnancy
* Complicated birth or poor infant health
* Family history of pediatric hearing loss
* Most common = Noise exposure
* 90 dB + = greater risk of damaging hair cells/ cochlea
* Syndrome associated with hearing loss
* Down Syndrome
* Recurrent or persistent otitis media with fluid for at least 3 months
* Associated with deficits in speech perception + decreased ability to distinguish speech from background noise
* Can experience reduced loudness + clarityCauses of mixed hearing loss in children:
* Child with congenital sensorineural hearing loss could also have conductive hearing loss
* ‘cuz of otitis media or cerumen (earwax)Causes of conductive hearing loss in adults:
* Allergies, sinus-related problems, and a history of otitis media
* make adults more likely to have otitis media
* Head trauma that tears tear drum or dislocates ossicles
* Otosclerosis is an abnormal bone growth around the ossicles
* Build up of ear wax, water trapped in ears, etc.Causes of sensorineural hearing loss in adults:
* Presbycusis: degeneration of inner ear + other auditory structures as result of aging
* Things start to work less efficiently as you age
* Noise induced hearing loss: caused by exposure to damaging lvls of noise
* Greater than 90+ dB
* Ototoxic drugs in certain antibiotics
* Aspirin in large quantitiesCauses of Mixed hearing loss in adults:
* Combination of permanent reduction of sound + temporary hearing loss
* Also have conductive hearing loss ‘cuz of impacted earwax
Ototoxic drugs
- Oto = hearing, toxic
* Drugs harmful to hearing
Mixed hearing loss manifest in an individual with hearing loss
- Impacted earwax = hearing loss goes to mixed hearing loss
Otitis media
- Otitis media: an infection of the middle ear, the air-filled space behind the eardrum that contains the tiny vibrating bones of the ear
* Fluid may eventually perforate/tear tympanic membrane
* Can be temporary or permanent, affecting a person’s mood
* Can also lead to:
* hole (perforation) of the eardrum
* hearing loss
* Mastoiditis
* Life-threatening complications:
* Meningitis = infection in the fluid surrounding the brain)
* brain abscess = pocket of pus in the brain)
* blood clots in veins in head brain
Noise-induced hearing loss
- Noise-induced hearing loss = caused by exposure to damaging levels of noise
* (90dB+)
m. Know how hearing loss is treated for adults and children.
- Adults involves amplification + listening devices an aural habilitation
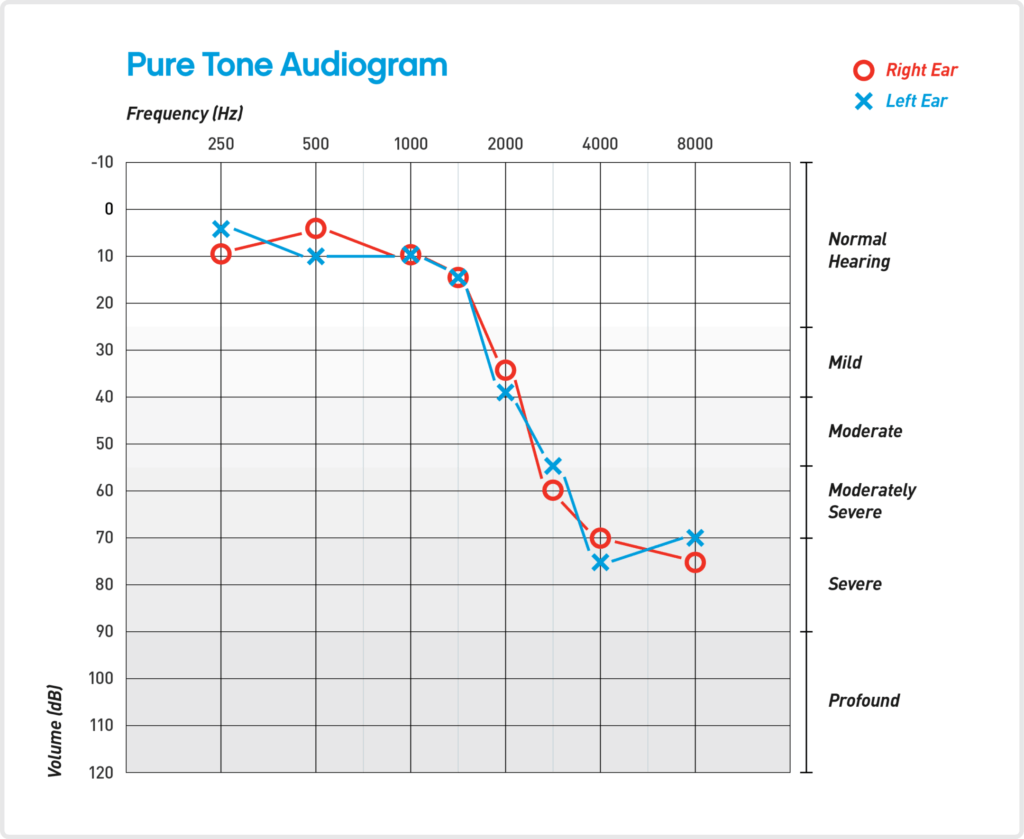
- Audiogram
* Graph that shows the threshold of a person's hearing based on frequency + intensity
* Shows information about a person's hearing ability - Difference between pure tone audiometry + bone conduction
* Pure tone:
* Sounds are played through child's ear changing the decibel + frequency
* Child presses button or raise hand when they hear a sound
* Bone conduction:
* Device that attaches to the child's head (on temporal bone region)
* Helps localize the damage
* Vibration goes to the inner ear, or cochlea,
* Skips outer + middle ear
* Test tells the audiologist how well you hear + if problem in the outer or middle ear
Audiogram
Youtube video gives a good tutorial: https://www.youtube.com/watch?v=bP-nJp3yBK4
- Data Line
* Right ear is red O
* Left ear is blue X - Normal hearing: -10 to 15
- Hearing Loss Severity Ranges:
* -16 to -25: minimal hearing loss
* -26 to -40: mild hearing loss
* -41 to -55: moderate hearing loss
* -56 to -70: moderately severe hearing loss
* -71 to -90: severe hearing loss
* -91+: profound hearing loss - Axis
* X axis is frequency
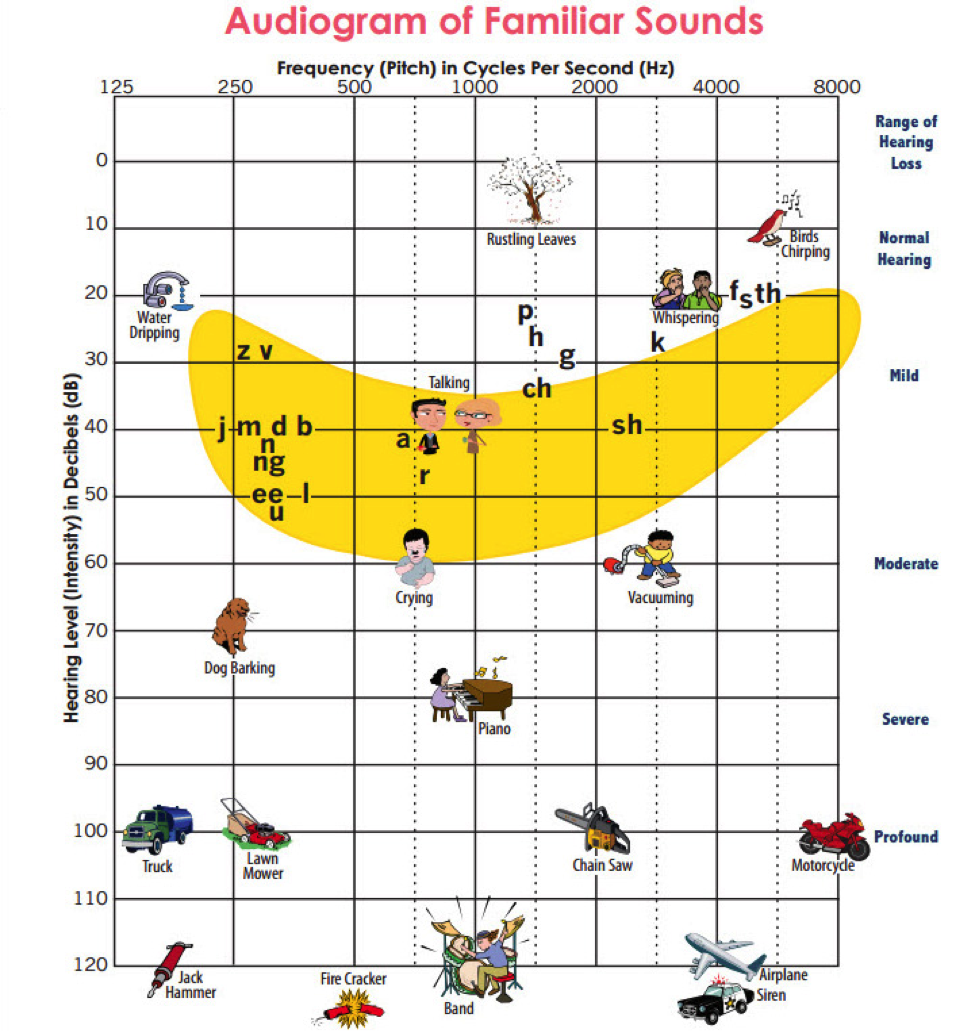
* Y axis is intensity - Speech Banana know: Speech zone, Type of speech, Sounds that are high frequency vs low frequency, + General decibel range sounds lie
- Hearing Problems Reported by Adults with Hearing Loss:
* Environmental Challenges
* Background noise
* Large groups
* Phones
* Speaker challenges
* Conversations with too many speakers
* Unfamiliar topics
* Listener challenges
* Isolation
* Trying to concentrate
* Fatigue - Significant Others Problems:
* Speaking challenges
* Remembering to get person's attention first
* Facing them
* Interpersonal challenges
* Not knowing when the person understands
* Repeating
* Being patient
* Acting as an interpreter
Hearing Assessment
- General Assessment Process:
* Referral
* Screening
* Newborn hearing screenings
* Otoacoustic emissions + evoked auditory potentials
* Conventional hearing screenings
* Audiometer, Headphones, + Tone in both ears
* Audiological Evaluation
* Case history + evaluation
* Otoscopic examination
* Audiometry - Difference between Newborn Screenings + Conventional Screenings:
* Newborn Screening = not require response from newborn
* Uses technology to see if child’s hearing falls in range
* Evoked Potentials (AEPs) measure
* Used as estimation of hearing sensitivity in newborns, young children, + difficult to test adult
* Identify tumors on the nerves and brainstem
Treatment for adults and children:
- Adults
* Amplification
* Listening devices
* Aural rehabilitation - Children
* Same as adults but with Communication Choices
* Some families decide to maximize hearing so their child can hear + speak
* Other families decide to communicate through sign language
* Lot of families do a combination of both
Amplification + Assistive Listening Devices
- Hearing aids
* purpose to provide the impaired ear with amplified signal to improve speech perception - Cochlear implants
* surgically implanted devices that electrically stimulates the auditory nerve - FM systems
* used to help a person with hearing loss listen in noisy areas - Aural (re-)habilitation: intervention for persons who have not developed listening, speech, and language skills
* For children - Communication strategies for people who are Deaf or Hard-of-hearing
* American Sign Language (ASL)
* Contact Language (ASL + Manual English)
* Signing Exact English (SEE)
* Auditory Verbal unisensory (one-one therapy for listening + verbal skills)
* Cued Speech
* Oral Auditory (hearing aid, assistive listening devices (ald)
Old Material
- Communication: the process of sharing information between two or more people
- Four main processes of communication
* Formulation: getting thoughts and ideas together
* Transmission: Conveying thoughts and ideas to another person, often by speech
* Reception: Receiving information from another person, often by hearing
* Comprehension: Making sense of the information - Role of feedback in a communicative exchange:
* Information provided by the receiver to the sender → informing the sender of the integrity of their message - Language: socially shared code that uses a system of symbols including sounds and words to represent ideas to others
* Components
* Content (semantics): are rules for the meaning of words and word combinations
* Form: includes syntax, morphology, + phonology (which are rules for the organization of words and sounds)
* syntax : rules for the international organization of sentences
* Yoda’s sentence “strong is Vader.” = unacceptable vs “Vader is strong”
* Morphology: rules for the internal organization of words
Words can be morphed to change their meaning
“Walk”, “walked”, “walker”, “walking”, “walks”, “cookie”
Cookie monster fails to add plural -s to cookie
- Phonology: rules for the sounds, Or phonemes, in syllables and words
* 43 sounds in English + more than 100,000 words
* None of those words contain an “s” followed by “g” = breaks phonotactic rules of English
* Use/pragmatics are rules for the social use of language
* Using language for different purposes
* Organizing language for a conversation - Speech: neuromuscular process that allows people to express language through voice
* Respiration
* Phonation
* Articulation
* Resonation - Hearing: perception of sound/ speech sounds
* Sound source creates a set of vibrations in surrounding air particles
* Vibration of air particles create sound waves
* Frequency = how fast the air particles move back + forth
* Frequency is correlated with pitch
* Intensity = how far the air particles move back + forth
* Intensity correlated with volume
* Ear receives the sound waves
* Brain processes the frequency + intensity of the sound waves as pitch + loudness
* Differentiates speech and nonspeech sounds - Communication disorders
* Communication disorder = variation WITHIN a linguistic community
* Communication difference = variation BETWEEN linguistic communities - Speech disorders
* affect respiration, phonation and articulation
* Types:
* Articulation + phonological disorders
* Fluency disorders
* Motor speech disorders - Language disorders
* Affect semantics, syntax, morphology, phonology and/or pragmatics
* Types:
* Child and adult language disorders
* Reading disabilities (dyslexia) - Hearing disorders
* affect auditory pathways from the ear to the brain - Different types of hearing disorders:
* Sensorineural hearing loss
* Conductive hearing loss
* Auditory process disorder - Age of onset
* when the disorder starts - Difference between Organic + Inorganic (functional) Disorders
* Organic disorders: have clear neurological, biological, or physiological causes
* Aphasia = caused by brain injury + laryngectomies
* Functional disorders: have no known cause that may have behavioral, emotional, or functional components
* Childhood Language Disorders
* Autism - Difference between Degenerative + Non-Progressive Disorders
* Degenerative disorders
* Health conditions maintain over time
* TBI, Down syndrome
* Non-progressive
* Health conditions deteriorate over time
* ALS, MS, Muscular dystrophy - Typical Levels of Severity of Disorder
* Mild
* Moderate
* Severe
* Profound
Communication Development
- Joint attention: Engagement of two or more individuals (in mental focus) on the same object or event at the same time
- Rituals of infancy: Helps children learn the rituals of speech by giving them comfort predictability, and opportunities to learn language
* Engage in joint reference and attention
* Ex if they keep hearing "put your arm in your sleeve", they will learn the label for arm - Caregiver responsiveness: Caregivers' responses to infants encourage them to keep communicating.
* ex: Waiting and listening, following the child's lead, joining in and playing, being face-to-face - Caregivers role: encourage infants to keep communicating by =
* Waiting and Listening
* Follow the child’s lead
* Join in and playing
* Being face to face - Markers of intentionality
- 1. Intentionality = baby says "mama" when gesturing towards her mom
* Imitation = baby says "mama" after being told to say "mama" - 2. Has to approximate adult form of word
- 3. Uses words with consistency + multiple contexts
* Ex: All dogs are called "doggie" by the baby, not just the dog the baby sees everyday
Types of babbling + Speech
- Marginal Babbling: 4-6 months one syllable sound
- Reduplicated Babbling: 7-10 months = uses more syllables and repetition
* Children speak first words around 12 months
* Combine words around 12-18 months
* Develop CVC words around 18-24 months - Childhood language disorders: Significant impairment in the acquisition + use of language across modalities due to deficits in comprehension and/or production across any of the five language domains
* Phonology, morphology, syntax, semantics, pragmatics
* Language disorders may persist across the lifespan + symptoms may change over time - Receptive Language Disorder
* Difficulty understanding language - Expressive Language Disorder
* Difficulty sharing spoken or written thoughts + language
* Ex: ideas + feelings - Mixed Language Disorder
* Both Receptive + Expressive - Effect of language disorder on reading
* Language disorders affect reading + writing
* Phonological awareness:ability to recognize and manipulate sounds in words
* Decoding: using letter-sound correspondence to understand printed words in texts - Specific language impairment (SLI): primary developmental language disorder
* impairment of expressive or receptive language in preschool + school-age children - Autism spectrum disorder (ASD): developmental disability that causes secondary language disorders
* Criteria of Symptoms
* Emerge during childhood
* Affect individual's everyday functioning
* Include problems with social communication + social interaction
* Include restrictive + repetitive pattern of behavior - Factors increasing risk of SLI + ASD
* Family History
* Having children later in life
* Problems with pregnancy - Brain Injuries can lead to language disorders
- Intellectual Disability (ID): developmental disability that causes secondary language disorders
* Primary Language Disorders: language disorders that happen in absence of any other language disorder
* Secondary language disorder: language disorders caused by another disorder - Areas of communication language disorders can manifest in
* Receptive or expressive language
* Domains of language
* Reading + writing - Assessment: evaluations of speech, language, cognitive-communication, + swallowing skills by SLP
* Assessment = drives intervention - Purposes of assessment
* Identify skills in a particular area of communication
* Guide the design of interventions to improve person's skills in a particular area of communication
* Monitor person's communicative growth + performance over time
* Qualify a person for services - Common techniques for assessment
* Formal tests
* Surveys/ norm-based
* Referenced test
* Criterion referenced tests - Evidence-based practice: process of integrating four areas of knowledge
* Scientific knowledge
* Clinical expertise
* Client perspective
* Internal evidence
* Data informed
* Evaluation of client
* Performance
e. What are the 5 stages of assessment?
- screening and referral
- -designing and administering the assessment protocol
- -interpreting assessment findings
- -developing an intervention plan
- -monitoring progress and outcomes
- Basic components of a comprehensive assessment protocol
* Record review/case history
* Interview
* Systematic observation
* Formal standardized tests
* Questionnaire/survey
* Criterion referenced tests
* Instrumentation - Calculate MLU: total number of morphemes/total number of utterances
- Difference between Criterion-referenced test + Norm-referenced test
* Criterion referenced tests are used to determine an individual's level of achievement or skill in a particular area
* Ex: driver's test
* Norm referenced tests-compare individuals' performance in a specific area with that of their same aged peers
* Ex: state test - Diagnosis: when an area of communication is markedly different from what is observed in the typical population or form what is expected in the individual being assessed
- Differential diagnosis: process of systematically differentiating a disorder from other possible disorders
- Intervention: Implementation of a plan to improve a person's communication
- Three purposes of intervention
* Prevention: attempt to prevent a disorder
* directed at people who are at risk for developing a communication disorder but do not yet show signs of one
* Remediation: slow the progress or reverse the course of the disorder
* delivered to people who have been diagnosed with a communicative disorder
* Compensation: help people cope with symptoms that are unlikely to go away
* when significant communication difficulties remain after a course of remediation intervention
* when a disorder is not amenable to remediation
* when it's unlikely that the progression of a disorder will be reversed - Intervention is considered “one size fits all” vs individualized
* Preventative= one type size fits all
* Remediation and compensatory= individualized
Articulation and Phonology
- Phonemes: Smallest meaningful unit of sound
* Phonemes are units of sound
* Language is written representation of sounds - IPA (International Phonetic Alphabet)
* Vowels described by
* Tongue height
* vowels classified as having high, mid, or low tongue height
* Tongue advancement
* vowels classified as being front, central or back
* Roundness
* vowels classified as being rounded, neutral or unrounded
* Tension
* vowels classified as being tense or lax - Consonants described by
- Voice
* whether or not the vocal folds vibrate - Place
* Where the sound is produced
* bilabial, labiodental, interdental, alveolar, palatal, velar, glottal - Manner
* How the sound is produced
* stops, fricatives, affricates, nasals, liquids, glides
* Ex: /m/ = voiced, bilabial, nasal - General patterns of speech sound acquisition in children
* Stops, nasals, and glides develop before fricative, affricates and liquids
* Anterior sounds develop before posterior sounds
* Word final consonant clusters develop before words initial clusters
* Stop clusters develop before fricative clusters - Articulation impairment:involves problems making sound
* Omission
* “Nana” for “banana”
* Distortions
* “Slushy” or lateral /s/
* Substitutions
* “Wabbit” for “rabbit”
Phonological processes
- Phonological impairment:involves patterns of sound errors
* such as… - Unstressed Syllable Deletion: unstressed syllable in a word is omitted
* Ex: pajamas-jamas - Final Consonant Deletion: final consonant of a word is omitted
* Ex: Book→boo - Consonant Harmony: one consonant in a word takes on features of another consonant
* Ex: coat→tote - Reduplication: first syllable in a word is repeated
* Ex: mommy→mama - Fronting: back sounds are replaced with front sound
* Ex: cool →tool - Cluster Reduction: two or more consonants that occur together are reduced to a single consonant
* Ex: stick→tick - Stopping: fricatives + affricates replaced with stops
* Ex: sun→ton
Functional/Organic + Speech Sound Disorder SSD
- Functional speech sound disorders = unknown causes
- Organic speech sound disorders = known causes
* Causes an Organic Speech Sound Disorder
* cleft lip and/or palate - Referring a child for a Speech Sound Disorder (SSD) Assessment
* Can be made by:
* Caregivers/Parents
* Pediatricians
* Teacher - Family’s cultural (linguistic) background during the case history portion of a SSD assessment
* If child shows signs of a speech sound disorder = important to look into their family's cultural background ‘cuz error could be speech variation/difference not disorder - Speech variation: differences in speech that arises from dialect or foreign accent
- Oral mechanism exam necessary during a SSD assessment
* oral mech exams examine structures and functioning of the speech mechanism
* Look at articulators
* Check for deviations that may hinder speech - Hearing screening + language eval necessary in SSD Assessment
* Rule out hearing impairments causing speech sound errors
* Ex: weak or breathy voices, problems with nasalization, deletion of syllables, confusion between nasal and plosive phonemes, confusions between voiced and voiceless consonants - Stimulability: examines the child's ability to produce or imitate a misarticulated sound correctly
* when a model is provided by the clinician - Three treatment approaches for SSDs
* Goal writing
* Cognitive based therapy (CBT)
* Mindfulness - Contrastive approach
* Maximal oppositions: contrast one sound the child has with an unknown sound
* the unknown sound is maximal different based on voice, place, and manner
* used for severe phonological disorders + when the child is missing many sounds
Stuttering + Cluttering
- Fluent speech = smooth, effortless + automatic
- Disfluencies
* Normal disfluencies
* Between 18 months - 3 years
* Repetition of sounds, syllables, + words
* After 3-years
* Repetition of words and phrases
* Disfluencies increase with fatigue excitement, upset
* Disfluencies come + go
* Unaware of disfluencies
* Disfluencies Associated with Stuttering
* Between 3 - 5 years
* Frequent repetition of sounds, syllables + words
* Prolongations
* Blocks
* Disfluencies persist - Core stuttering behavior: observable, uncontrollable disfluencies that a person makes when speaking
* Repetitions: when speakers repeat sounds, syllables, words, or phrases
* Prolongations: when the speaker stretches a sound in a word
* Blocks: when the speaker stops or gets stuck before or during the production of a sound - Secondary behaviors
* Responses to core behaviors (like fight or flight responses)
* responses to core behaviors
* Blinking eyes
* Closing eyes
* Shifting eyes (up/down)
* Widening eyes
* Flaring nostrils
* Wrinkling nose
* Licking lips
* Develops so that individual can get out of disfluent moment
* behaviors only work for a certain time + then individual picks a different secondary behavior to help
* List just keeps getting bigger and bigger which does not help stuttering in the long run
* Ex: tapping, blinking - Avoidance behaviors: person who stutters does to avoid the disfluent moment
* Ex: if they know a specific word they will stutter on, they won't use that word + will choose another word that means the same thing
* Negative feelings + attitudes
* Can affect participation + achievement in school, home, + work environments + quality of life - Causes of Stuttering
* Predisposing Factors: Make a person susceptible to stuttering
* Family history
* Genetics
* Gender
* Differences in brain morphology and neural physiology
* Precipitating Factors
* Developmental + Environmental factors making a person's stuttering worse - Goal of Fluency Shaping = Not to Stutter
- Goal of Stuttering Modification = Stutter more Fluently
- Cluttering
* People who have rapid or unusual rates of speech (ROS)
* Results in disfluencies
* Frequent + unusual pauses in their speech
* Fewer repetitions, but more errors because of ROS
* Disrupts flow with unexpected pauses
* Blending of sounds in words
* No awareness of errors + subsequently, no signs of struggle, tension, or avoidance
* Not paying attention to listener cues
“Did you eat” → “Jeet”
Difference between Direct + Indirect treatment
- Direct treatment = important for adolescents + adults
* Utilizes both stuttering modification + fluency shaping approaches or both together
* Treatment emphasizes:
* Knowledge about stuttering
* Understand, demystify, + confront
* Reduce negative feelings
* Fluency building
* through combination of fluency shaping + stuttering modification - Indirect treatment involves training the parent
* Environmental modification
* Reduce demands
* Operant training models - Keep in mind when talking to PWS
* Don’t:
* Finish sentences
* Fill in words for them
* Say slow down relax or take a breath
* Do:
* Let person know by your manner you are listening to what they say
* Not how they are saying it