
pg 932-940, 946-959 - Vascular Disorders
1. Relate the etiology and pathophysiology of peripheral artery disease (PAD) to the major risk factors.
2. Describe the clinical manifestations and interprofessional and nursing management of the patient with PAD of the lower extremities
3. Plan appropriate nursing and interprofessional management for the patient with acute arterial ischemic disorders
4. Distinguish the pathophysiology, clinical manifestations, and nursing and interprofessional management of the patient with thromboangiitis obliterans (Buerger disease) and Raynaud phenomenon.
5. Distinguish the pathophysiology, clinical manifestations, and interprofessional and nursing management of patients with different types of aortic aneurysms.
6. Select appropriate nursing interventions for a patient undergoing an aortic aneurysm repair.
7. Describe the pathophysiology, clinical manifestations, and interprofessional and nursing management of the patient with aortic dissection.
8. Evaluate the patient’s risk factors for developing superficial vein thrombosis or venous thromboembolism (VTE).
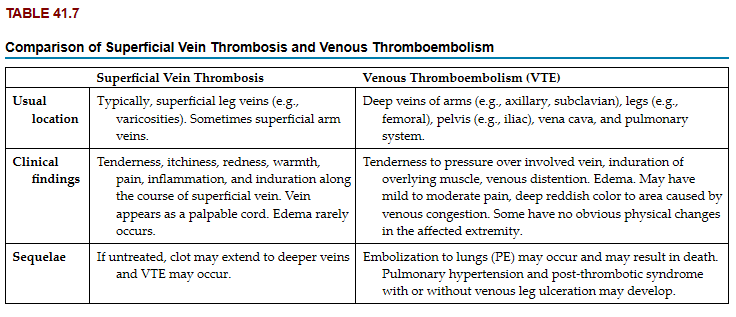
9. Distinguish between the clinical characteristics of superficial vein thrombosis and VTE.
10. Outline the interprofessional and nursing management of patients with superficial vein thrombosis and VTE.
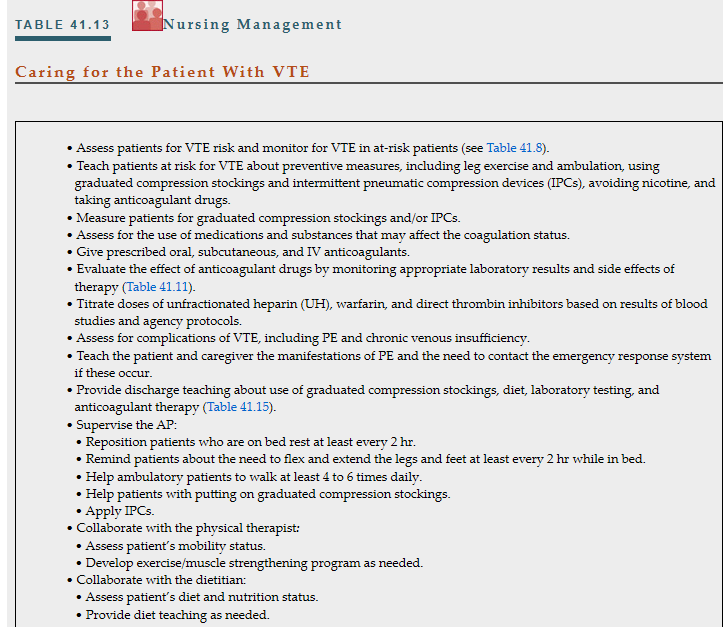
11. Prioritize the key aspects of nursing management for the patient receiving anticoagulant therapy.
12. Relate the pathophysiology and clinical manifestations to the interprofessional care of patients with varicose veins, chronic venous insufficiency, and venous leg ulcers.
acute arterial ischemia
aneurysm
aortic dissection
chronic venous insufficiency (CVI)
critical limb ischemia
deep vein thrombosis (DVT)
intermittent claudication
peripheral artery disease (PAD)
post-thrombotic syndrome (PTS)
superficial vein thrombosis
thromboangiitis obliterans (Buerger disease)
varicose veins
venous thromboembolism (VTE)
venous thrombosis
Virchow’s triad
Phlebitis = Acute inflammation of small, cannulated veins
Manifestations: pain, tenderness, warmth, redness, swelling, palpable cord
Risk Factors
Mechanical irritation from IV catheter
Infusion of irritating drugs
IV catheter location in flexion areas (e.g., wrist, antecubital area)
Avoid IV catheter insertion in flexion areas
phlebitis = rarely infectious
Resolves quickly after catheter removal
Elevate extremity if edema present → promote fluid reabsobtion
Apply warm, moist heat
Give oral NSAIDs (e.g., ibuprofen) or topical NSAIDs (e.g., diclofenac gel) for pain and inflammation
Venous Thrombosis = Formation of a thrombus (blood clot) with vein inflammation
Most common disorder of the veins
Classification = superficial or deep vein thrombosis
Superficial Vein Thrombosis
Thrombus in superficial veins (e.g., greater or lesser saphenous vein)
Deep Vein Thrombosis (DVT)
Thrombus in deep veins (e.g., iliac and/or femoral veins)
Venous Thromboembolism (VTE) = prefered terminology
Represents the spectrum from DVT to Pulmonary Embolism (PE)
Severity
Superficial vein thrombosis is serious
25% of patients with superficial vein thrombosis have DVT or PE at diagnosis
Patients at risk for recurrent VTE
The 3 key factors (called Virchow triad) that cause venous thrombosis are
(1) venous stasis
(2) damage of the endothelium (inner lining of the vein)
(3) hypercoagulability
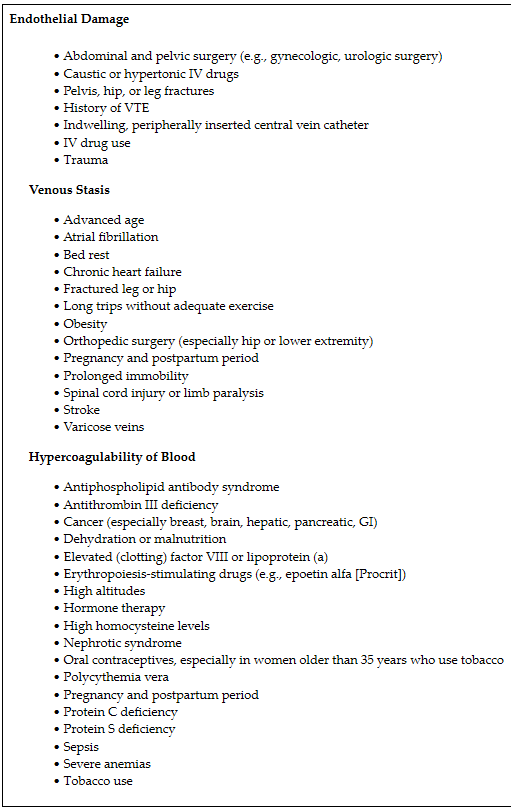
The patient at risk for developing VTE usually has predisposing conditions to these 3 factors
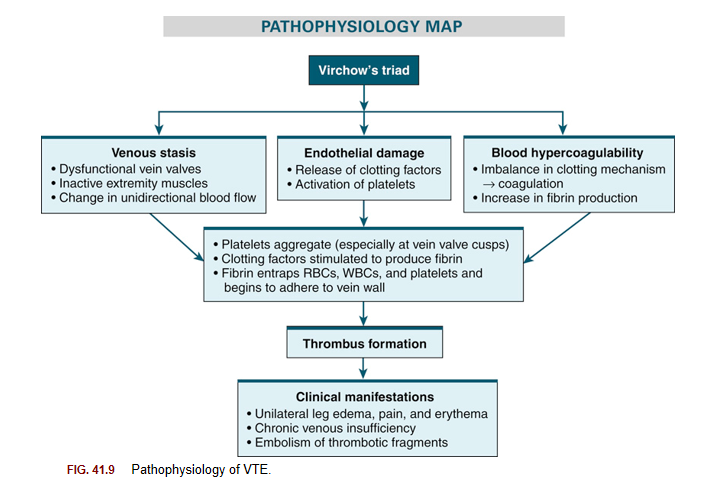
Normal Venous Blood Flow Depends on:
Action of muscles in the extremities
Function of venous valves → allow one-directional flow
Venous Stasis
Occurs when:
Valves are dysfunctional
Muscles of extremities are inactive
High-Risk Groups for Venous Stasis
Obese individuals
Pregnant women
Patients with chronic HF or atrial fibrillation
Individuals on long trips without exercise
prolonged surgical procedure patients
Immobilized individuals due to injury or medical conditions
Damage to the endothelium may be caused by direct (e.g., surgery, intravascular catheterization, trauma, burns, prior VTE) or indirect (chemotherapy, diabetes, sepsis) injury.
Damaged endothelium stimulates platelet activation and starts the coagulation cascade.
This predisposes the patient to thrombus development.
Causes of Blood Hypercoagulability
Severe anemias
Polycythemia
Cancers (e.g., breast, brain, pancreas, GI tract)
Nephrotic syndrome
High homocysteine levels
Deficiency in protein C, protein S, and antithrombin
Sepsis (due to endotoxins released from bacteria)
Certain drugs (e.g., corticosteroids, estrogens)
Risk Factors for VTE in Women = very high risk factors
Tobacco use
Smoking causes hypercoagulability by increasing plasma fibrinogen and homocysteine levels and activating the intrinsic coagulation pathway.
Estrogen-based oral contraceptives
Postmenopausal women on oral hormone therapy
Women over 35 years old with a family history of VTE
Women who smoke and take oral contraceptives double their risk
Localized platelet aggregation and fibrin entrap RBCs, WBCs, and more platelets to form a thrombus
frequent site: valve cusp of vein → venous statis occurs there
thrombus enlarges → increased numbers of blood cells and fibrin collect behind it → makes are larger clot with tail that eventually blocks the lumen of vein
thrombus only partially blocks vein, endothelial cells cover thrombus and stop thrombotic process
thrombus does not become detached → undergoes lysis or becomes firmly organized and adherent within 5-7 days
organized thrombus may detach and result in an embolus
turbulent blood flow is major factor in embolization
thrombus become an embolus and flows through venous circulation to heart and lodges in pulmonary circulation becoming PE
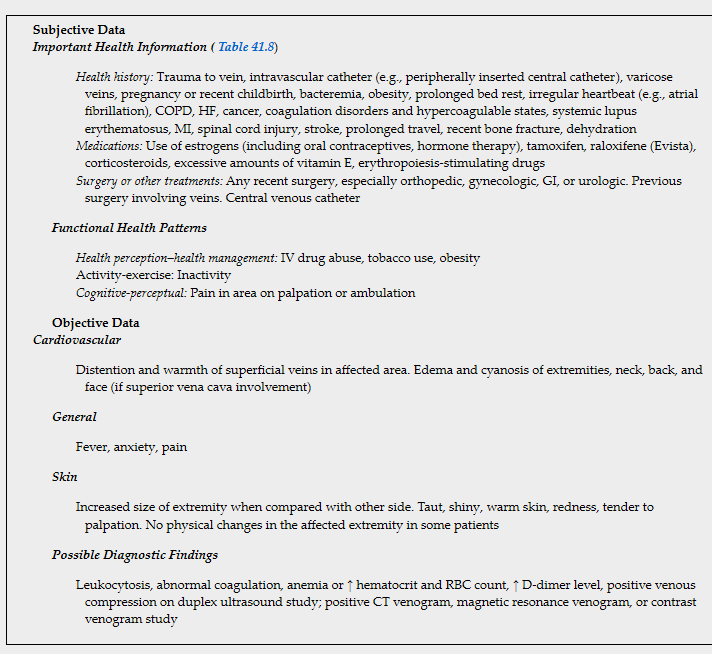
Clincal Manifestations
patient with superficial vein thrombosis may have palpable, firm SQ cordlike vein
area around vein - itchy, painful to touch, reddened, warm, mild temp elevation and leukocytosis may be present
extremity edema may occur
LE superficial vein thombosis often involes varicose veins
Risk Factors
increased age, pregnancy, obesity, cancer, recent fracture(s), estrogen therapy, recent sclerotherapy (e.g., treatment for varicose veins), recent surgery or long-distance travel, hypercoagulability, and a history of chronic venous insufficiency (CVI), superficial vein thrombosis, or VTE. It can occur in people with endothelial problems (e.g., Buerger disease)
Interprofessional Care
US can confirm diagnosis (clot 5cm or larger) and rule out clot extension to a deep vein
superficial vein thrombosis affects very short vein segment and not near saphenofemoral junction → anticoagulants may not be needed
Oral NSAIDs can ease symptoms
other intervetions:
tell pt to wear graduated compression stockings/bandages
apply warm compresses
elevate affected limb above level of heart
apply topical NSAIDs
mild exercise
Clinical Manifestations
Pt with LE VTE → may have unilateral leg edema, pain, tenderness with palpation, dilated superficial veins, sense of fullness in thigh or calf, paresthesias, warm skin, redness, or systemic temperature greater than 100.4F (38C)
inferior vena cava involved → both legs may be edematous and cyanotic
~10% of VTEs involve upper extremity veins → may extend into internal Jugular vein or superior vena cava
if superior vena cava involved → similar symptoms may occur in arms, neck, back, face
complication
most serious complications of VTE are PE, chronic thromboembolic pulmonary hypertension, post-thrombotic syndrom, and phlegmasia cerulea dolens
Chronic Venous Hypertension
Vein wall and vein valve damage (acute inflammation and thrombus reorganization)
venous valve reflux
persistent venous outflow obstruction
Post-Thrombotic Syndrome (PTS)
Occurs in 8% to 70% of VTE patients
Results from chronic inflammation and venous hypertension
Symptoms: pain, swelling, cramps, tingling, etc.
Manifestations: edema, spider veins, ulcers, etc.
Symptoms
pain, aching, fatigue, heaviness, sensation of swelling, cramps, pruritus, tingling, paresthesia, bursting pain with exercise, and venous claudication.
Manifestations
persistent edema, spider veins (telangiectasia), venous dilation (ectasia), redness, cyanosis, increased pigmentation, eczema, pain during compression, atrophie blanche (white scar tissue), and lipodermatosclerosis
Venous ulceration can occur with severe PTS.
Signs of PTS typically begin within a few months to a few years of a VTE.
Risk factors include persistent leg symptoms 1 month after VTE, proximal VTE location (e.g., near the iliofemoral junction), extensive VTE, recurrent VTE on the same side, asymptomatic VTE, and residual thrombus. Other factors include obesity, older age, poor INR control, daily tobacco use before pregnancy, increased D-dimer levels, elevated inflammatory markers, and varicose veins.
Phlegmasia cerulea dolens (swollen, blue, painful leg) is a rare complication of severe lower extremity VTE.
It involves the major leg veins, causing near-total occlusion of venous outflow.
Patients typically have sudden, massive swelling; deep pain; and intense cyanosis of the extremity.
If untreated, the venous obstruction causes arterial occlusion and gangrene, requiring amputation.
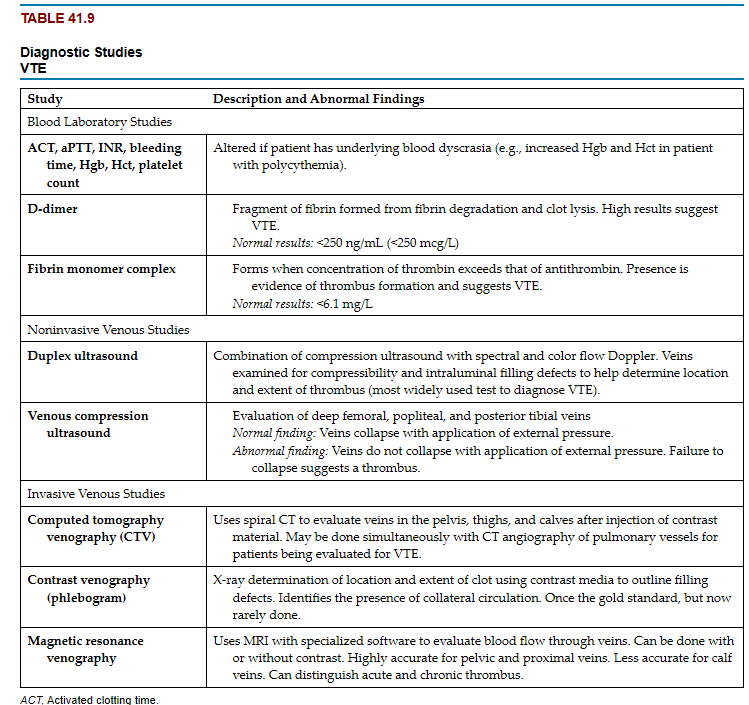
Diagnosis of an initial VTE is based on the assessment combined with D-dimer testing and/or ultrasound. Table 41.9 presents the diagnostic studies used to determine the site or location and extent of a VTE.
 Interprofessional Care
Interprofessional CarePrevention
VTE prevention is a core measure of high-quality health care in high-risk hospitalized patients developed by The Joint Commission (TJC) and the National Quality Forum
. In patients at risk for VTE, interventions used are based on bleeding and thrombosis risk, medical history, current drugs, medical diagnoses, scheduled procedures, and patient preferences.
early aggressive mobilization = easiest and most cost effective method to decrease VTE risk
reposition every 2 hours if on bed rest
teach to flex and extend feet, knees, and hips ~2-4 hours while awake
pt should take meals out of bed in chair
walk 4-6x per day
anticoagulation and mechanical prophylaxis are not recommended for auctely ill medical pt at low risk for VTE
Graduated compression stockings
used along with anticoagulation
toes hole is under toes , heel patch over heel, thight gusset is on inner thigh and there are no wrickles
do not roll down stockings or alter them → impedes venous return
an cause arterial ischemia, edema, skin breakdown, and VTE.
not recommended in pt with VTE already
Intermittent pneumatic compression devices (IPCs)
inflatable sleeves or boot to compress calf an thigh and/or foot and ankle to improve venous return
may be used with graduated compression stockings
not effective if not fitted correctly or worn continuously at rest
not worn with pt has active VTE because of risk for PE
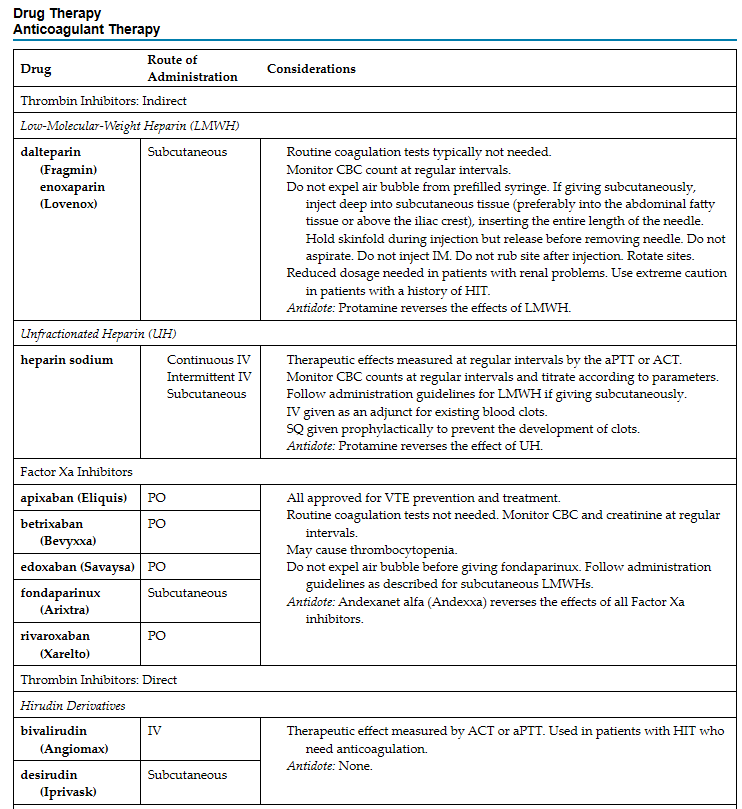
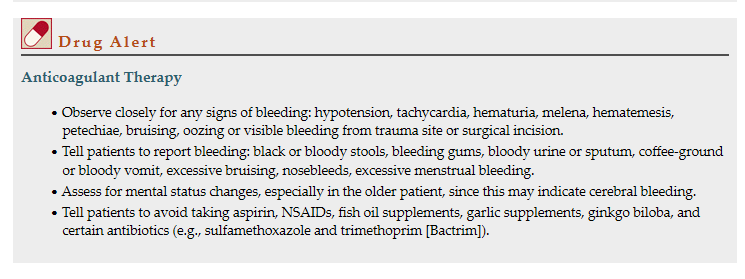
Drug Therapy
Anticoagulants are used routinely for VTE prevention and treatment.
goal of VTE prevention : prevent clot formation
goal for confirmed VTE: prevent new clot formation,spread of clot, embolization
3 major classes of anticoagulants available:
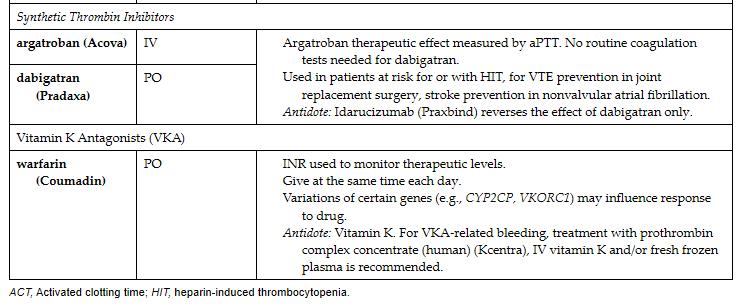
(1) vitamin K antagonists (VKAs)
for longterm or extended anticoagulation = warfarin (a VKA)
Warfarin inhibits activation of vitamin K dependent coagulation factors II, VII, IX, and X and anticoagulation proteins C and S
takes effect 48-72hrs and achieves max effect several days later
overlap of parenteral anticoagulant (UH or lowmolecular weight heparin [lmwh]) and warfarin typically required for 5 days
monitor level of anticoagulation daily using INR → INR standardized system of reporting prothrombin time (PT)
Take careful hx before starting warfarin
do not give antiplatelet drugs or NSAIDs with warfarin → increase bleeding risk
many other drugs, vitamins, mineral, and herbal supplements interact with warfarin
diet that varies in vitamin K intake can make it hard to achieve and maintain a target INR level
genetic variants in genes VKORC1 and cytochome P450 2C9 may influence how some people respond to warfarin
(2) thrombin inhibitors (both indirect and direct)
two major classes of indirect thrombin inhibitors: UH and LMWH
UH → affects both intrinsic and common pathways of blood coagulation by way of plasma antithrombin
antithrombin inhibits thrombin-mediated conversion of fibrinogen to fibrin by affecting factors II (prothrombin), IX, X, XI, and XII
heparin given given SQ for VTE prevention or by continuous IV infusion for VTE treatment
IV heparin use requires frequent monitoring of clotting status by measuring activated partial thromboplastin time (aPTT)
side effects
heparin induced thrombocytopenia (HIT) → immune reaction to heparin causes severe sudden decrease in platelet count along with paradoxical increase in veous or arterial thombosis
diagnose HIT → measuring presence of heparin antibodies in blood
treatment HIT → immediately stopping heparin therapy - give nonheparin anticoagulant
another effect of long term heparin therapy = osteoporosis
LMWHs → derived from UH
more predictable dose response, longer half life and fewer bleeding complications than UH
less likely to cause HIT and osteoporosis
typically do not require ongoing anticoagulant montiroing and dose adjustment
antiinflammatory properties may help prevent PTS and veous ulcer development
protamine reverses effect of LMWH
Direct thrombin inhibitors
classified as hirudin derivative or synthetic thrombin inhibitors
hirudin = made using recombinant DNA technology → binds specifically thrombin and directly inhibits its function without causing plasma protein and platelet interactions
hirudin derivatives given by continuous IV infusion (bivalirudin) → bivalirudin given to pt with or at risk for HIT having a percutaneous coronary intervention
anticoagulation monitored using aPTT or activaed clotting time (ACT)
if bleeding occurs → not antidoe for hirudin derivatives
Argatroban
synthetic direct thrombin inhibitor → hinders thrombin
like bivalirudin, alternative to heparin for prevention and treatment of HIT and for pt with or at risk for HIT needing percutaneous coronary interventions
effect of argatroban not reversible
anticoagulant effect monitored using aPTT or ACT
Dabigatran (Pradaxa)
oral direct thrombin inhibitor
used for VTE prevention after elective join replacement for stroke prevention in nonvalvular atrial fibrillation and as a treatment for VTE
5 major advantages compared to warfarin:
rapid onset
no need to monitor anticoagulation
few drug-food interactions
lower risk for major bleeding, and predictable dose response
(3) factor Xa inhibitors
Factor Xa inhibitors inhibit factor Xa directly or indirectly, producing rapid anticoagulation.
These include fondaparinux (Arixtra), rivaroxaban (Xarelto), apixaban (Eliquis), and edoxaban (Savaysa).
All are used for both VTE prevention and treatment.
Fondaparinux is contraindicated in patients with severe renal disease.
Although coagulation monitoring or dose adjustment is not needed, anticoagulant activity can be measured using anti-Xa assays
anticoagulation does not dissolve clot → clot lysis begins naturally through body’s intrinsic fibrinolytic system
Anticoagulant Therapy for VTE prevention
For VTE prevention in the hospitalized medical patient at risk for thrombosis who is not bleeding, low-dose UH, LMWH, or fondaparinux is used.
If the patient is at low VTE risk, drug prophylaxis is not needed.
Patients with moderate VTE risk (e.g., general, gynecologic, urologic surgery) should receive either UH or LMWH.
Patients with high VTE risk (e.g., trauma) should receive UH or LMWH until discharge.
Patients having abdominal or pelvic surgery for cancer or major orthopedic surgery (e.g., total knee or hip replacement) should receive VTE prophylaxis.
Anticoagulant therapy for VTE treatment
Patients with confirmed VTE should receive initial treatment with either LMWH, UH, or an oral factor Xa drug.
Oral VKA therapy may be an option.
A therapeutic INR is maintained between 2.0 and 3.0 if VKA therapy is used.
Active treatment of VTE should continue for at least 3 months.
Patients with multiple co-morbidities, complex medical issues, or a very large VTE usually are hospitalized for parenteral UH administration.
Depending on the presentation and home situation, patients may be safely managed as outpatients.
Thrombolytic therapy for VTE treatment
Another treatment option for patients with a thrombus is catheter-directed administration of a thrombolytic drug (e.g., urokinase, tPA).
It dissolves the clot(s), reduces the acute symptoms, improves deep venous flow, reduces valvular reflux, and may help to decrease the incidence of PTS.
Catheter-directed thrombolysis is an option for patients who have a low risk of bleeding and present with an acute, extensive, symptomatic, proximal VTE.
Systemic anticoagulation is needed before, during, and after catheter-directed thrombolysis.
ome pt with extensive, acute, proximal VTE who are not candidates for catheter-directed thromolysis and/or interventional radioolgy therapies may have surgery
Surgical Options
Open venous thrombectomy
Removal of clot through vein incision
Followed by anticoagulant therapy
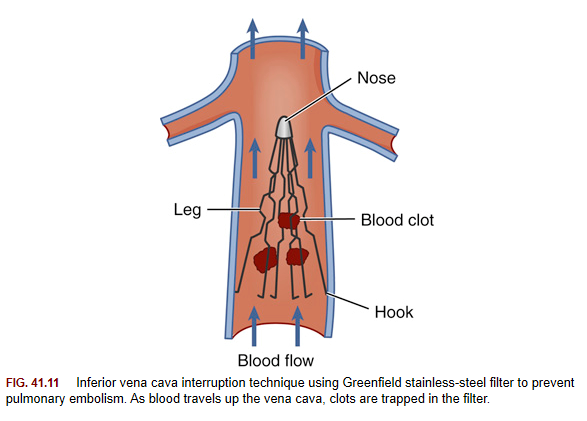
Inferior vena cava interruption
Devices like Greenfield, Vena Tech, TrapEase filters
Percutaneous placement through femoral or internal jugular veins
Act as "sieve-type" device to filter clots without interrupting blood flow
Complications: air embolism, migration, perforation of vena cava
Filter may need removal and replacement over time due to clots clogging filter and completetly block vena cava
A filter device is recommended with acute PE or proximal VTE of the leg in patients with active bleeding or if anticoagulant therapy is contraindicated or ineffective.
Percutaneous endovascular interventional radiology procedures can be used along with catheter-directed thrombolytic therapy
Used for severely symptomatic patients with iliocaval or iliofemoral obstruction
Similar to lower extremity PAD treatments → difference = accessing an occluded vein instead of an artery
Options: mechanical thrombectomy, pharmacomechanical devices, angioplasty, stenting
Anticoagulation therapy recommended post iliofemoral interventional radiology procedure
Post-Procedure Nursing Care
Maintain catheter systems (if continuous infusions)
Monitor for bleeding, embolization, impaired perfusion
Provide VTE prevention teaching
Clinical problems for the patient with VTE include:
• Inadequate tissue perfusion
• Pain
• Impaired tissue integrity
• Impaired respiratory function
• Musculoskeletal problem
The overall goals for the patient with VTE include
(1) pain relief
(2) decreased edema
(3) increased knowledge of disorder and treatment plan
(4) no skin ulceration
(5) no bleeding complications
(6) no evidence of PE
focus on preventing thrombi and reducing inflammation
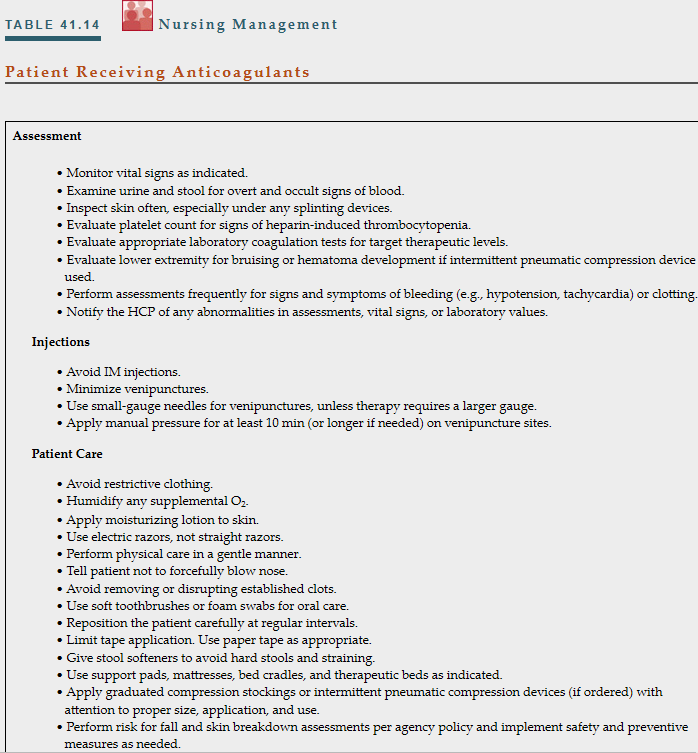
Review medications, vitamins, minerals, and herbal supplements that may interfere with anticoagulant therapy
Monitor various levels depending on anticoagulant ordered:
INR, aPTT, ACT, anti-factor Xa levels
CBC, creatinine, factor X levels, hemoglobin, hematocrit, platelet levels, liver enzymes
Monitor platelet counts for patients on UH or LMWH to assess for HIT
May need to Adjust direct thrombin inhibitors for patients with renal or liver disease
Check pertinent test results before initiating, administering, or changing anticoagulant therapy
Identify factors increasing bleeding risk:
Active gastroduodenal ulcer, prior bleeding history, low platelet count
Hepatic or renal failure, rheumatic disease, cancer, age >85 years
Patients with INR >5.0 on warfarin have higher bleeding risk
Administer reversal agents or adjust dosages for anticoagulation above target goals
Early ambulation post-VTE does not increase short-term PE risk
Benefits of early ambulation:
Rapid decrease in edema and limb pain
Fewer post-thrombotic syndrome symptoms
Improved quality of life
Educate patient and caregiver on the importance of physical activity
Encourage ambulation multiple times a day
Consider bed rest with limb elevation for patients with severe edema and limb pain initially
Discuss Modifying VTE Risk Factors
Stop smoking and avoid all nicotine products
Avoid constrictive clothing
Discontinue oral contraceptives or hormone therapy for women with a history of VTE
Limit standing or sitting in a motionless, leg-dependent position
Exercise calf muscles, take short walks, and stay hydrated during long-distance travel
Consider knee-high graduated compression stockings for high-risk individuals during travel
Monitoring Laboratory Values and Drug Instructions
Regularly monitor INR levels with home monitoring devices
Educate on subcutaneous administration of LMWH or fondaparinux
Follow consistent diet with vitamin K-containing foods for warfarin users
Avoid vitamin K supplements, excess vitamin E, and alcohol
Ensure routine blood tests and immediate medical attention for specific symptoms
Diet and Lifestyle Recommendations
Maintain a well-balanced diet
Encourage hydration to prevent hypercoagulability
Implement weight management plan for overweight patients
Develop an exercise program focusing on leg strength training and aerobic activity
Consider graduated compression stockings or IPCs for swelling and PTS management
Follow-Up Guidelines
Contact emergency services for signs of PE
Review drug dosage, actions, and side effects
Emphasize the importance of routine follow-up and adherence to recommendations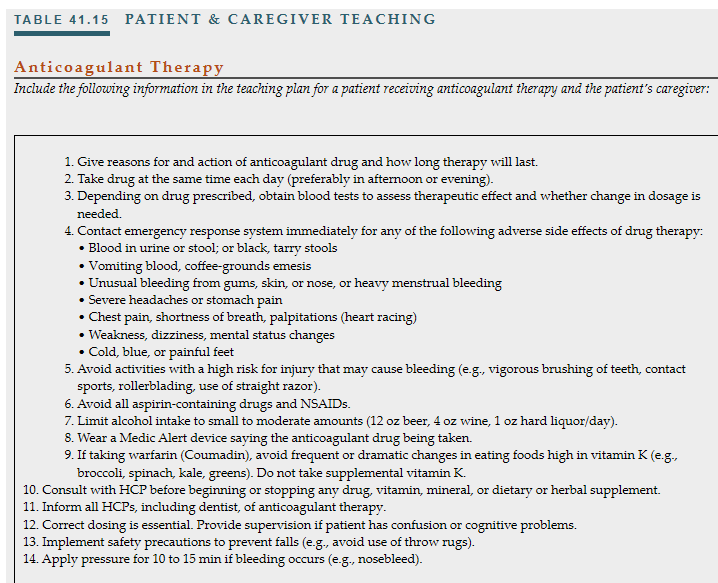
The expected outcomes are that the patient with VTE will have:
• Minimal to no pain
• Intact skin
• Increased knowledge of disorder and treatment plan
• No signs of hemorrhage or occult bleeding
varicose veins = dilated tortuous superficial veins → often found in saphenous vein system
may be small and harless or large and bulging
primary varicose veins (idiopathic) → due to weakness of vein wals more common in women
secondary varicose veins → result from direct injury, previous VTE, or excess vein distention
may occur in esophagus, vulva, spermatic cords, and anorectal area (hemorrhoids) and abnormal ateriovenous connections (AV)
congenital varicose veins = chromosomal defects that cause abnormal development of venous system
reticular veins = smaller varicose veins that appear flat, less tortuous, and blue green in color
Telangiectasias (spider veins) = small visible vessels that appear bluish, black, purple or red
superficial veins in LE become dilated and tortuous in response to backward blood flow and increased venous pressure
risk factors:
family hx of chornic venous disease
weak vein structure
female
tobacco
inc age
obesity
multiparity
hx of VTE
venous obstruction resulting of extrinsic pressure by tumors
thrombophilia
phlebitis
previous leg injury
occupation that reuiqre prolonged standing of sitting
primary varicose veins → weak veins walls allow vein valve ring to enlarge - leaflets no longer fit together properly incompetent
incompetent vein valves allow backward blood flow → particularly when pt is standing
results in increased venous pressure and further venous distention
high pressure in superficial veins can be caused by vein valve dysfunction in deep veins or perforator veins
veins that perforate the deep fascia of muscles to connect the superficial veins to the deep veins
Variability of Discomfort
Varies among individuals
Intensifies after episodes of superficial vein thrombosis
Prevalence
More common in women than men
Common Symptoms
Heavy, achy feeling or pain after prolonged standing or sitting
Pain relieved by walking or limb elevation
Pressure, itching, burning, tingling, throbbing, or cramp-like leg sensations
Swelling, restless or tired legs, fatigue, and nocturnal leg cramps
Complications
Superficial venous thrombosis is the most frequent complication
Spontaneous occurrence or post-trauma, surgery, or pregnancy
Rare complications include:
Rupture of varicose veins leading to external bleeding
Skin ulcerations
Superficial varicose veins often can be diagnosed by physical assessment.
Duplex ultrasound imaging is the gold standard to evaluate venous anatomy, valvular competence, and venous obstruction.
Conservative treatment involves rest with limb elevation; graduated compression stockings; leg strengthening exercise, such as walking; and weight loss, if indicated.
Venoactive drugs stimulate release of chemicals in vein walls
Strengthen circulation, reduce inflammation, and edema
Types of Venoactive Agents
Micronized purified flavonoid fraction
Rutosides (e.g., horse chestnut seed extract)
Proanthocyanidins (from grapes and apples)
Ruscus (butcher’s broom)
Therapeutic Benefits
Pain relief
Edema reduction
Decreased leg cramping and restless legs
Usage and Approval
Widely used in Europe
Not FDA approved
Available over the counter as diet or herbal supplements
sclerotherapy → direct IV injection of liquid or foam sclerosing substance that chemically ablates treated veins
hypertonic saline, polidocanol, glycerin
used on telangiectasias, perforator veins, reticular veins, smaller varicose veins, and venous malformations
done inoffice setting - minimal discomfort
transcutaneous laser therapy for telangiectasias and high-intensity pulsed-light therapy for reticular veins.
used for pt in whom sclerotherapy is contraindicated or ineffective
works by heating hemoglobin in vessels → results in vessel sclerosis
complications
pain, blistering, hyperpigmentation, and superficial erosions
endovenous ablation using thermal energy from radiofrequency or laser therapy → for saphenous vein reflux (minimally invasive)
inserts a catheter into the vein to heat the vein wall, which then causes the vein to collapse
complications
bruising, skin burns, hyperpigmentation, infection, paresthesia, superficial or deep vein thrombosis, and PE
graduated compression stockings and bandages are worn afterwards
Endovenous thermal ablation may be done in combination with surgical ligation or phlebectomy.
surgical intervention → for recurrent superficial venous thrombosis or when symptoms cannot be controlled with other therapy
The traditional surgical intervention involves ligation of the entire vein (usually the greater saphenous vein) and removal of its incompetent branches.
An alternative but time-consuming technique is ambulatory phlebectomy. This involves pulling the varicosity through a “stab” incision followed by excision of the vein.
Transilluminated powered phlebectomy involves the use of a tissue resector to destroy clusters of varicosities and removes the pieces via aspiration. Complications include bleeding, bruising, and infection.
prevention = key in varicose veins
avoid sitting and standing long periods
maintain ideal body weight
precautions against injury to extremities
avoid wearing constrictive clothing
walk daily
after vein ligation surgery:
deep breathe → promote venous return
check extremities for color, movement, sensation, temp, edema, quality of pedal pulses
some brusing and discoloration is normal
elevate legs 15 degrees → limit edema
remove graduated compression stockings or bandages every 8 hours for short period and then reapply them
long-term managment directed toward improving ciruclation and appearance → relieving discomfort and avoiding complications
can reoccur in other veins after surgery
teach pt proer use and care of custom fitted graduated compression stockings
pt should apply stockings in bed before rising in morning
emphasize importantace of periodic positioning of legs above heart
overweight pt may need help with weight loss
pt with job that requires long periods of standing or sitting needs to be frequently flex and extend hips, legs, and ankles and changes positions
Chronic venous insufficiency (CVI) = abnormalities of venous system that result in adv signs and symptoms such ad edema, skin chagnes and/or venous leg ulcers
CVI can lead to venous leg ulcers
not life threatening but painful, slow to heal , debilitating, costly conditions → adversely affect pt quality of life
common in older adults
both long standing pirmary varicose veins and PTS can progress to CVI
ambulatory venous hypertension causes serous fluid and RBCs to leak from capillaries and venules into tissue
causes edema and chronic inflammatory changes
enzymes in tissue eventually break down RBCs
this released hemosiderin → causes brownish skin discoloration
overtime → fibrous tissue replaces skin and SQ tissue around ankle
results in thick harded contracted skin - caused of CVI known, exact pathophysiology of venous leg ulcers is unknown
Skin Appearance
Leathery texture in lower leg
Brownish or "brawny" appearance due to hemosiderin deposition
Edema
Persistent for prolonged period
May lead to pain, especially with infection
Eczema
Itching and scratching common
Associated with skin changes and discomfort
Venous Ulcers
Location: above the medial malleolus
Painful, especially with edema or infection
Pain worsens in dependent leg position
Progression
Untreated ulcers widen and deepen
Increased risk of infection and complications
Compression = essential for venous ulcer healing and preventing venous ulcer recurrence
options for compression thearpy:
custom-fitted graduated compression stockings
elastic tubular support bandages
a Velcro wrap (CircAid)
IPCs
multilayer (3 or 4) bandage systems (e.g., Profore).
assess to make sure PAD not present → ABI of 0.4 or less suggests severe PAD → compression thearpy contraindicated
wear daily to prevent recurrent leg ulcers
replace stockings ~4-6 months
Activity
avoid standing or sitting for long periods → dec blood return from LE
teach pt elevate legs above level of heart to reduce edema
daily walking program once an ulcer heals
avoid tauma limbs
teach foot care
Dressings
moist environemtn dressings = basis of wound care
variety of dressings:
include transparent film dressings, hydrocolloids, hydrogels, foams, alginates, gauze, and combination dressings.
Dressing decisions should be based on wound characteristics, cost, best evidence, and clinician judgment
Evaluate pt nutrition
balanced diet (below best for healing)
high protein
vitamin a
vitamin C
zinc
pt with diabetes → maintain normal blood glucose levels and aids in healing process
venous leg ulcers are colonized by bacteria → routine use of antibiotics is not indicated
signs of infection:
quantity, color, or odor of the drainage; pus; redness of the wound edges; change in sensation around the wound; and warmth around the wound.
There may be increased local pain, edema, or both; dark-colored granulation tissue; induration around the wound; delayed healing; and cellulitis.
If signs of infection occur, obtain a wound culture.
Culture results guide antibiotic therapy.
The usual treatment for infection is wound debridement, wound excision, and systemic antibiotics.
if does not heal with conservative therapy → drug thearpy should be considered
Pentoxifylline is recommended with compression therapy to improve healing
Pentoxifylline minimizes WBC activation and adhesion to capillary endothelium and decreases oxidative stress.
Other treatments are considered for large venous leg ulcers that do not respond to standard therapy after 4 to 6 weeks.
These include coverage with a skin replacement or substitute, such as split-thickness skin grafts or artificial bioengineered skin.
Although grafts help with healing, they do not replace the need for lifelong compression therapy.
Patients with CVI have dry, flaky, itchy skin.
Daily moisturizing decreases itching and prevents skin cracking.
Contact dermatitis may result from contact with sensitizing products.
These include such as topical antimicrobial agents (e.g., gentamicin); additives in bandages or dressings (e.g., adhesives); ointments containing lanolin, alcohols, or benzocaine; and over-the-counter creams or lotions with fragrance or preservatives.
Assess wounds for signs of infection with each dressing change
Peripheral Artery Disease
Peripheral artery disease (PAD) is a progressive narrowing and degeneration of the arteries of the upper and lower extremities. In most cases, it is a result of atherosclerosis.
Significant risk factors for PAD are tobacco use (most important), chronic kidney disease, diabetes, uncontrolled hypertension, and hypercholesterolemia.
Peripheral Artery Disease of the Lower Extremities
PAD of the lower extremities affects the iliac, femoral, popliteal, tibial, or peroneal arteries.
The severity of manifestations depends on the site and extent of blockage and the amount of collateral circulation.
The classic symptom of PAD of the lower extremities is intermittent claudication. Other symptoms include paresthesia, numbness or tingling in the toes or feet, rest pain, and the loss of both pressure and deep pain sensations.
Physical findings include thin, shiny, and taut skin with loss of hair on the lower legs; decreased or absent pedal, popliteal, or femoral pulses; elevation pallor; and reactive hyperemia when the limb is in a dependent position.
Complications of PAD include nonhealing ulcers over bony prominences on the toes, feet, and lower leg, and gangrene. Amputation may be needed if blood flow is not restored.
Tests used to diagnose PAD include Doppler ultrasound with segmental blood pressures, calculating the ankle-brachial index (ABI), and angiography.
The overall goals for the patient with lower-extremity PAD include adequate tissue perfusion, relief of pain, increased exercise tolerance, and intact, healthy skin on extremities.
The first treatment goal for patients with PAD is to aggressively modify all cardiovascular risk factors. All tobacco use must be stopped.
Drug therapy includes statins, antiplatelet agents, and angiotensin-converting enzyme (ACE) inhibitors. Two drugs approved to treat intermittent claudication are cilostazol and pentoxifylline.
The main nondrug treatment for claudication is tobacco cessation and a formal exercise training program. Walking is the most effective exercise.
Interventional radiologic procedures for PAD include percutaneous transluminal balloon angioplasty with stenting or atherectomy.
The most common surgical procedure for PAD is a peripheral arterial bypass operation with autogenous vein or synthetic graft material to bypass or carry blood around the lesion.
Teach patients with PAD the importance of meticulous foot care.
Critical limb ischemia is a chronic condition in advanced PAD characterized by ischemic rest pain, arterial leg ulcers, and/or gangrene of the leg.
ACUTE ARTERIAL ISCHEMIC DISORDERS
Acute arterial ischemia is a sudden interruption in the arterial blood supply to a tissue, organ, or extremity. If untreated, it results in tissue death.
Common causes include embolism, thrombosis, or trauma.
Signs and symptoms of an acute arterial ischemia usually have an abrupt onset and include the
“6 Ps”: pain, pallor, pulselessness, paresthesia, paralysis, and poikilothermia.
Treatment options include anticoagulation, thrombolysis, embolectomy, surgical revascularization, or amputation.
Thromboangiitis Obliterans
Thromboangiitis obliterans (Buerger’s disease) is a nonatherosclerotic, segmental, recurrent inflammatory disorder of the small and medium arteries, veins, and nerves of the arms and legs. • Patients may have intermittent claudication of the feet, hands, or arms. As the disease progresses, rest pain and ischemic ulcerations develop.
There are no laboratory or diagnostic tests specific to Buerger’s disease.
Treatment includes complete cessation of tobacco use in every form. Conservative management includes the use of antibiotics to treat any infected ulcers and analgesics to manage the ischemic pain.
Surgical options include revascularization, implantation of a spinal cord stimulator, and sympathectomy.
Raynaud’s Phenomenon
Raynaud’s phenomenon is an episodic vasospastic disorder of small cutaneous arteries, most often involving the fingers and toes. The exact cause is unknown.
Manifestations include vasospasm-induced color changes of the fingers, toes, ears, and nose (white, blue, and red). An episode usually lasts only minutes. In severe cases, may last for several hours.
Symptoms usually are precipitated by exposure to cold, emotional upsets, caffeine, and tobacco use.
Diagnosis is based on persistent symptoms for at least 2 years. There is no diagnostic test.
Teach patients to prevent recurrent episodes by avoiding temperature extremes and all tobacco products.
Calcium channel blockers are the first-line drug therapy.
AORTIC ANEURYSMS
Aortic aneurysms are outpouchings or dilations of the arterial wall.
The causes of aortic aneurysms are degenerative, congenital, mechanical, inflammatory, or infectious.
Aortic aneurysms may involve the aortic arch and thoracic aorta. Most are found in the abdominal aorta below the level of the renal arteries.
Thoracic aortic aneurysms are often asymptomatic. The most common manifestations are deep, diffuse chest pain that may extend to the interscapular area; hoarseness; and dysphagia.
Abdominal aortic aneurysms (AAAs) are often asymptomatic, but symptoms may mimic pain associated with abdominal or back disorders.
The most serious complication related to an untreated aneurysm is rupture and bleeding.
Diagnostic tests for AAAs include chest x-ray, electrocardiogram (to rule out myocardial infarction), echocardiography, computed tomography (CT) scan, and magnetic resonance imaging (MRI) scan.
The goal of management is to prevent the aneurysm from rupturing.
Surgical repair is done for aneurysms that are greater than 5 cm in size, are rapidly expanding, or have a high risk for rupture, and in patients who are symptomatic.
Minimally invasive endovascular aneurysm repair is an alternative to conventional surgical repair and involves the placement of a sutureless aortic graft into the abdominal aorta inside the aneurysm.
The overall goals for a patient undergoing aortic surgery include normal tissue perfusion, intact motor and sensory function, and no complications related to surgical repair, such as thrombosis or infection.
After surgery, the patient typically needs close monitoring in an ICU setting.
Monitoring for graft patency and adequate renal perfusion is a priority.
Maintenance of an adequate BP is extremely important.
Antibiotics are given to prevent infection.
Peripheral pulses, skin temperature and color, capillary refill time, and sensation and movement of the extremities are assessed and recorded per hospital policy.
Hourly urine outputs and daily weights are recorded.
On discharge, teach the patient to gradually increase activities but to avoid heavy lifting for 6 weeks.
Aortic Dissection
Aortic dissection results from the creation of a false lumen between the intima (inner lining) and the media (middle layer) of arterial wall.
The most likely causes of aortic dissection are degeneration of the elastic fibers in the medial layer and chronic hypertension.
Type A aortic dissection affects the ascending aorta and arch. Type B aortic dissection starts in the descending aorta.
Dissections are classified as acute (first 14 days), subacute (14 to 90 days) or chronic (greater than 90 days) based on symptom onset.
Patients with an acute ascending aortic dissection report sudden, severe onset of excruciating chest and/or back pain radiating to the neck or shoulders. Patients with acute descending aortic
dissection are more likely to report pain in their back, abdomen, or legs and describe the pain as
“sharp” and “worst ever” followed less often by “tearing” or “ripping.”
Diagnostic studies used to assess aortic dissection are similar to those done for AAA.
The initial goal of therapy for aortic dissection without complications is to lower the heart rate and BP and manage pain.
β-blockers are the drugs of choice to lower the heart rate and BP.
An acute Type A aortic dissection is a surgical emergency.
Otherwise, surgery is indicated when drug therapy is ineffective or when complications of aortic dissection are present.
Venous Thrombosis
Phlebitis is the inflammation of the walls of the small, cannulated veins of the hand or arm and presents with 2 or more of the following symptoms: pain, tenderness, warmth, erythema, swelling, and a palpable cord.
Venous thrombosis is the most common disorder of the veins and involves the formation of a thrombus (clot) in association with inflammation of the vein. Venous thromboembolism (VTE) represents the spectrum of pathology from deep vein thrombosis (DVT) to pulmonary embolus.
DVT involves a thrombus in a deep vein, most often the iliac and femoral veins. It can result in embolization of thrombi to the lungs.
Three key factors (called Virchow’s triad) that cause venous thrombosis are (1) venous stasis,
(2) damage of the endothelium, and (3) hypercoagulability of the blood.
Superficial vein thrombosis involves a thrombus in a superficial vein, presenting as a palpable, firm, subcutaneous cordlike vein. The surrounding area may be tender to the touch, reddened, and warm. A mild systemic temperature elevation and leukocytosis may be present.
Recommended treatment for lower leg superficial vein thrombosis consists of a prophylactic dose of fondaparinux (Arixtra).
Graduated compression stockings, elevation of leg, oral and topical nonsteroidal antiinflammatory drugs, and exercise, such as walking, are recommended for symptom relief. • The patient with lower extremity VTE may or may not have unilateral leg edema, pain, tenderness with palpation, dilated superficial veins, a sense of fullness in the thigh or calf, paresthesia, warm skin, erythema, and/or a systemic temperature greater than 100.4° F (38° C). • The most serious complications of VTE are PE, chronic thromboembolic pulmonary hypertension, post-thrombotic syndrome (PTS), and phlegmasia cerulea dolens.
Post-thrombotic syndrome (PTS) results from chronic inflammation and chronic venous hypertension caused by vein wall and vein valve damage, venous valve reflux, and persistent venous obstruction.
Symptoms include pain, aching, heaviness, swelling, cramps, itching, and tingling. Signs include persistent edema, increased pigmentation, eczema, secondary varicosities, and lipodermatosclerosis.
VTE prophylaxis for hospitalized patients depends on individual risk and may involve early ambulation, graduated compression stockings, intermittent pneumatic compression devices, and anticoagulation.
The goals in the treatment of VTE are to prevent propagation of the clot, development of any new thrombi, and embolization. Anticoagulation therapy is routinely used.
Three major classes of anticoagulants are available: (1) vitamin K antagonists, (2) thrombin inhibitors (direct and indirect), and (3) factor Xa inhibitors.
Warfarin, a vitamin K antagonist, inhibits activation of the vitamin K-dependent coagulation factors.
Indirect thrombin inhibitors include unfractionated heparin (UH) and low-molecular-weight heparin (LMWH)
Examples of direct thrombin inhibitors include dabigatran (Pradaxa) and the hirudin derivatives, bivalirudin (Angiomax) and desirudin (Iprivask).
Factor Xa inhibitors include subcutaneous fondaparinux (Arixtra) and oral agents including rivaroxaban (Xarelto), apixaban (Eliquis), and edoxaban (Savaysa).
Some VTE patients need surgical or endovascular therapy, including thrombectomy and placement of vena cava interruption devices, such as the Greenfield filter.
Nursing and collaborative care for the patient with VTE revolve around managing acute pain, the risk for impaired tissue integrity, and the potential complications of bleeding related to anticoagulant therapy and pulmonary embolism.
Discharge teaching should focus on elimination of modifiable risk factors for VTE, the importance of graduated compression stockings and monitoring of laboratory values, medication instructions, and guidelines for follow-up.
Varicose Veins
Varicose veins, or varicosities, are dilated, tortuous subcutaneous veins most often found in the saphenous system.
The cause of varicose veins is unknown. Risk factors include family or personal history of chronic venous disease, weak vein structure, female gender, tobacco use, increasing age, obesity, multiparity, venous obstruction resulting from thrombosis or extrinsic pressure by tumors, thrombophilia, phlebitis, previous leg injury, or occupations that require prolonged standing.
The most common symptom is an ache or pain after prolonged standing, which is relieved by walking or by elevating the limb. Nocturnal leg cramps in the calf may occur.
Interprofessional care involves rest with the affected limb elevated, compression stockings, and exercise, such as walking.
Several treatment options exist, including sclerotherapy, transcutaneous laser or high-intensity pulsed-light therapy, endovenous thermal ablation and surgical procedures, such as phlebectomy and vein ligation.
Prevention is a key factor related to varicose veins. Teach the patient measures to promote venous circulation.
Chronic Venous Insufficiency and Venous Leg Ulcers
Chronic venous insufficiency (CVI), a common medical problem in older adults, describes functional abnormalities of the venous system that result in advanced venous signs and symptoms, such as edema, skin changes, and/or venous leg ulcers.
CVI can result from long-standing varicose veins or post-thrombotic syndrome and can lead to venous leg ulcers.
Manifestations include the skin of the lower leg appearing leathery, with a characteristic brownish or “brawny” appearance, edema and eczema, and pruritus.
Venous ulcers classically occur above the medial malleolus. The wound margins are irregularly shaped, and the tissue is typically a ruddy color. Ulcer drainage may be extensive. Pain is present and may be worse when the leg is in a dependent position.
Compression is essential for venous ulcer healing and prevention of ulcer recurrence.
Compression options include elastic wraps, custom-fitted graduated compression stockings, elastic tubular support bandages, a Velcro wrap, intermittent pneumatic compression devices, and multilayer (3 or 4) bandage systems.
Moist environment dressings are the basis of wound care and include transparent film dressings, hydrocolloids, hydrogels, foams, alginates, impregnated gauze, dextranomer, flax, and combination dressings.
Assess nutritional status.
Monitor wounds for signs of infection. The usual treatment for infection is debridement, wound excision, and systemic antibiotics.
Adjuvant treatments include coverage with a split-thickness skin graft, cultured epithelial autograft, allograft, bioengineered skin, or porcine small intestinal submucosal tissue construct.
Long-term management of venous leg ulcers should focus on teaching the patient about self-care measures because the incidence of recurrence is high.
Proper foot and leg care is essential to avoid further trauma to the skin.
The patient with CVI should avoid standing or sitting with the feet dependent for long periods.
Teach patients with venous ulcers to elevate their legs above the level of the heart to reduce edema.
Once an ulcer is healed, encourage a daily walking program.
Prescription graduated compression stockings should be worn daily and replaced every 4 to 6 months to limit edema and reduce ulcer recurrence.
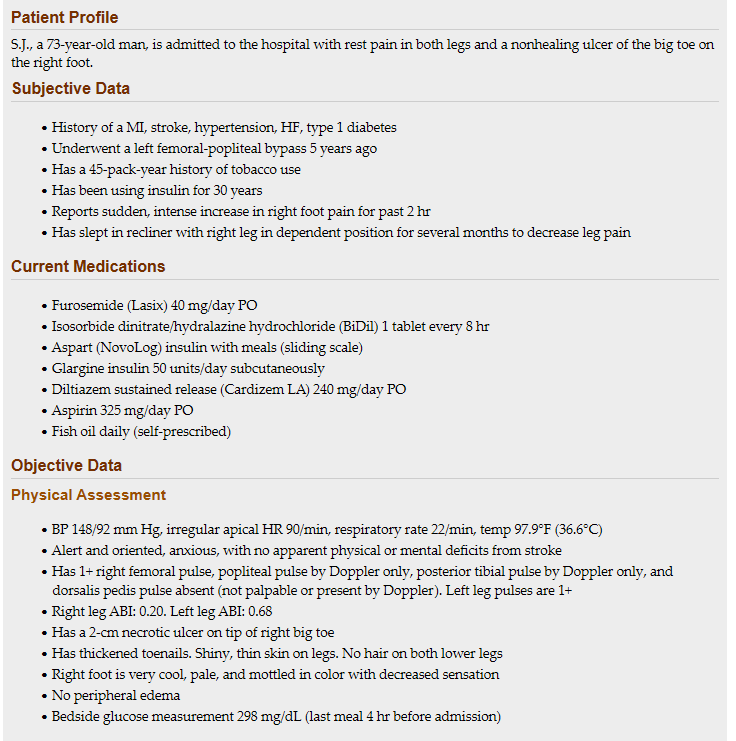 1. Recognize: What risk factors do you identify that led to S.J. having PAD?
1. Recognize: What risk factors do you identify that led to S.J. having PAD?
Risk factors for PAD include: Black, advanced age, past medical history of myocardial infarction, high blood pressure and diabetes, previous femoral-popliteal bypass, long-term smoking, and sedentary lifestyle.
2. Analyze: What are the important findings from S.J.’s assessment?
The important assessment findings include the sudden intense increase in pain to the right foot; the right foot is very cool, pale, and mottled in color with decreased sensation; and no right dorsalis pedis pulse. This worsening pain and change in pulses/skin condition are due to the sudden decrease in oxygen and blood supply distal to the occluded artery. The most likely cause for the sudden increase in right foot pain is acute arterial ischemia resulting from a thrombus development at an existing atherosclerotic plaque of the lower leg
3. Plan: What treatment options are possible?
The first priorities of interprofessional care would be prevention of thrombus propagation or further embolization and control of ischemic pain followed by restoring blood flow by removal of the thrombus via either surgical or catheter-based treatments described previously. Options for embolus/thrombus removal consist of percutaneous catheter-directed thrombolytic therapy, percutaneous mechanical thrombectomy with or without thrombolytic therapy, surgical thrombectomy, or surgical bypass. Determining which intervention to use is dependent upon stenosis location and the type and severity of the occlusion. Open surgical techniques for salvage of an ischemic limb include bypass procedures to direct blood flow beyond the occlusion and endarterectomy with or without patch angioplasty and intraoperative isolated limb thrombolysis. He has a strong history of cardiovascular problems. Drug therapy can decrease his risk of cardiovascular mortality. Other drug therapy options include a lipid-lowering statin and a beta adrenergic blocker. Evaluation of his lipid profile would determine if drug therapy is needed for high triglycerides and low HDL. He will likely be discharged on warfarin (Coumadin) and will require thorough education about the drug, side effects, and associated precautions
4. Prioritize: What is the important thing the team can do for S.J.?
Immediate priorities for S.J. include: (1) maximizing tissue perfusion, (2) relieving pain, and (3) preparing the patient for treatment procedures. A key nursing responsibility will be giving IV anticoagulants as ordered to prevent thrombus propagation. The lower extremities should be checked frequently for color, temperature, capillary refill, presence of peripheral pulses, and sensation and movement. Any deterioration in vascular status immediately needs to be reported to the HCP. Keep the limb warm to maximize perfusion. The use of a bed cradle/frame for the lower extremities to keep blankets from contact with the ischemic limb may reduce patient discomfort and tissue injury. If dehydration is a predisposing factor to the thrombosis, IV fluid hydration may need to be given. Depending on the planned treatment, you will be responsible for preparing the patient and caregiver for either a surgical or catheter-based procedure.
5. Act: What role do APs have in providing care?
The UAP can obtain vital signs; perform bedside glucose testing (per agency policy); helping S.J. with toileting, personal hygiene needs, and meals; monitoring oral intake and output; and reporting any changes in pain
6. Evaluate: What do you need to continually monitor?
You would need to continually monitor S. J’s pain; peripheral pulses (posterior tibial pulse and dorsalis pedis pulse) in both extremities; signs of bleeding (bruising, purpura, bloody stools, bleeding for intravenous sites); and intake/output.
7. Safety: What safety precautions should we consider?
Remind S.J. that he cannot get out of bed without assistance because of his risk of falling, consider using a bed alarm; S.J. needs to be monitored for bleeding, he is receiving a medication to help dissolve the clot in his leg, which significantly increases his risk of bleeding. S.J. and his caregiver will need to be educated on precautions related to anticoagulant use upon discharge.
1. A 50-year-old woman who weighs 95 kg has a history of high blood pressure, high sodium intake, tobacco use, and sedentary lifestyle. Which is the most important risk factor for peripheral artery disease (PAD) to address in the nursing plan of care?
a. Salt intake
b. Tobacco use
c. Excess weight
d. Sedentary lifestyle
The most important risk factor for peripheral artery disease is tobacco use. Other risk factors include increased levels of high-sensitivity C-reactive protein, diabetes, uncontrolled hypertension, family history, high triglyceride and lipid levels, hyperuricemia, increasing age, obesity, sedentary lifestyle, and stress.
2. Which information would the nurse include when explaining the cause of rest pain with PAD?
a. Vasospasm of cutaneous arteries in the feet
b. Decrease in blood flow to the nerves of the feet
c. Increase in retrograde venous perfusion to the lower legs
d. Constriction in blood flow to leg muscles during exercise
Rest pain most often occurs in the forefoot or toes when arterial blood flow is insufficient to meet basic metabolic requirements of the distal tissues. Nerves transmit pain messages because of the tissue ischemia. Rest pain occurs more often at night because cardiac output tends to drop during sleep and the limbs are at the level of the heart. Patients often try to achieve some pain relief by dangling the leg over the side of the bed or sleeping in a chair to allow gravity to maximize blood flow.
3. A patient with infective endocarditis develops sudden left leg pain with pallor, paresthesia, and a loss of peripheral pulses. Which action would the nurse take first?
a. Notify the HCP of the change in perfusion.
b. Start anticoagulant therapy with IV heparin.
c. Elevate the leg to improve the venous return.
d. Position the patient in reverse Trendelenburg.
The patient may have acute arterial ischemia (sudden interruption in the arterial blood supply to the extremity), caused by an embolism from a cardiac thrombus that occurred as a complication of infective endocarditis. Manifestations include any or all of the 6 Ps: pain, pallor, paralysis, pulselessness, paresthesia, and poikilothermia. Without immediate intervention, ischemia may progress quickly to tissue necrosis and gangrene within a few hours. If the nurse detects these signs, the HCP should be notified immediately.
4. Which clinical manifestations can the nurse expect to see in both patients with Buerger disease and patients with Raynaud phenomenon? (select all that apply)
a. Intermittent low-grade fevers
b. Sensitivity to cold temperatures
c. Gangrenous ulcers on fingertips
d. Color changes of fingers and toes
e. Episodes of superficial vein thrombosis
Buerger’s disease and Raynaud’s phenomenon have these manifestations in common:
cold sensitivity, ischemic and gangrenous ulcers on fingertips, and color changes of the distal extremity (fingers or toes).
5. A patient is admitted to the hospital with a diagnosis of abdominal aortic aneurysm. Which signs and symptoms would suggest that the aneurysm has ruptured?
a. Rapid onset of shortness of breath and hemoptysis
b. Sudden low back pain and bruising along the flank
c. Patchy blue mottling on feet and toes and rest pain
d. Gradually increasing substernal chest pain and diaphoresis
The manifestations of a ruptured abdominal aortic aneurysm include severe back pain, back or flank ecchymosis (Grey Turner’s sign), and hypovolemic shock (tachycardia, hypotension, pale clammy skin, decreased urine output, altered level of consciousness, and abdominal tenderness).
6. Which nursing interventions are the priority 8 hours after an abdominal aortic aneurysm repair?
a. Assessing nutrition status and diet preferences
b. Starting IV heparin and monitoring anticoagulation
c. Administering IV fluids and watching kidney function
d. Elevating the legs and applying compression stockings
Postoperative priorities include giving IV fluids and maintaining renal perfusion. An adequate blood pressure is important for maintaining graft patency, and administration of IV fluids and blood components (as indicated) is essential for adequate blood flow. The nurse should evaluate renal function by measuring hourly urine output and monitoring daily blood urea nitrogen (BUN) and serum creatinine levels. Irreversible renal failure may occur after aortic surgery, particularly in patients at high risk.
7. Which goal is the first priority of interprofessional care for a patient with a suspected acute aortic dissection?
a. Reduce anxiety
b. Monitor chest pain
c. Control blood pressure
d. Increase myocardial contractility
The initial goals of therapy for acute aortic dissection without complications are blood pressure (BP) control and pain management. BP control reduces stress on the aortic wall by reducing systolic BP and myocardial contractility.
8. Which patient is at highest risk for venous thromboembolism (VTE)?
a. a. A 62-year-old man with spider veins who is having arthroscopic knee surgery
b. b. A 32-year-old woman who smokes, takes oral contraceptives, and is planning a long flight
c. A 26-year-old woman who is 3 days postpartum and received maintenance IV fluids for 12 hours during her labor
d. d. An active 72-year-old man at home recovering from transurethral resection of the prostate for benign prostatic hyperplasia
Three key factors (called Virchow’s triad) that cause venous thrombosis are (1) venous stasis, (2) damage of the endothelium (inner lining of the vein), and (3) hypercoagulability of the blood. Patients at risk for venous thrombosis usually have predisposing conditions for these 3 disorders. The 32-yr-old woman has the highest risk: long trips without adequate exercise (venous stasis), tobacco use, and use of oral contraceptives.
9. Which clinical findings would the nurse expect in a person with an acute lower extremity VTE? (select all that apply)
a. Pallor and coolness of foot and calf
b. Mild to moderate calf pain and tenderness
c. Grossly decreased or absent pedal pulses
d. Unilateral edema and induration of the thigh
e. Palpable cord along a superficial varicose vein
The patient with lower extremity venous thromboembolism (VTE) may or may not have unilateral leg edema, extremity pain, a sense of fullness in the thigh or calf, paresthesia, warm skin, erythema, or a systemic temperature greater than 100.4 F (38 C). If the calf is involved, it may be tender to palpation.
10. Which treatment would the nurse anticipate for an otherwise healthy person with an initial VTE?
a. IV argatroban as an inpatient
b. IV unfractionated heparin as an inpatient
c. Subcutaneous unfractionated heparin as an outpatient
d. Subcutaneous low-molecular-weight heparin as an outpatient
Patients with confirmed VTE should receive initial treatment with low-molecular weight heparin (LMWH), unfractionated heparin (UH), fondaparinux, or rivaroxaban, followed by warfarin for 3 months to maintain the international normalized ratio (INR) between 2.0 and 3.0 for 24 hours. Patients with multiple comorbid conditions, complex medical issues, or a very large VTE usually are hospitalized for treatment and typically receive intravenous UH. LMWH for 3 months is another option for patients with acute VTE. Depending on the presentation, patients often can be managed safely and effectively as outpatients.
11. Which instruction is a key aspect of teaching for the patient on anticoagulant therapy?
a. Monitor for and report any signs of bleeding.
b. Do not take acetaminophen (Tylenol) for a headache.
c. Decrease your dietary intake of foods containing vitamin K.
d. Arrange to have blood drawn twice a week to check drug effects.
Teach patients taking anticoagulants to monitor and report any signs of bleeding, which can be a serious complication. Other important patient teaching includes maintaining a consistent intake of foods containing vitamin K and avoiding supplements that contain vitamin K. If a patient is taking warfarin, routine coagulation laboratory studies are needed. The frequency is patient dependent, not necessarily twice a week.
12. The nurse is planning care and teaching for a patient with venous leg ulcers. Which patient action is the most important in healing and control of this condition?
a. Following activity guidelines.
b. Using moist environment dressings.
c. Taking horse chestnut seed extract daily.
d. Applying graduated compression stockings.
Compression is essential for treating chronic venous insufficiency (CVI), healing venous ulcers, and preventing ulcer recurrence. Use of custom-fitted graduated compression stockings is an option for compression therapy.
A postoperative patient asks the nurse why the provider ordered daily administration of enoxaparin (Lovenox). Which reply would the nurse provide?
“This medication will help prevent breathing problems after surgery, such as pneumonia.”
“This medication will help lower your blood pressure to a safer level, which is very important after surgery.”
“This medication will help prevent blood clots from forming in your legs until your level of activity returns to normal.”
“This medication is a narcotic pain medication that will take away muscle aches caused by positioning during surgery.”
Enoxaparin is an anticoagulant that is used to prevent DVTs postoperatively.
The nurse is caring for a postoperative patient who had been receiving warfarin and diltiazem before surgery as treatment for atrial fibrillation. If the warfarin was discontinued the week before surgery, for which complication would the nurse monitor?
Decreased cardiac output
Increased blood pressure
Cerebral or pulmonary emboli
Excessive bleeding from incision
Warfarin is an anticoagulant that is used to prevent thrombi from forming on the walls of the atria during atrial fibrillation. When the medication is terminated, thrombi could again form. If one or more thrombi detach from the atrial wall, they could travel as cerebral emboli from the left atrium or pulmonary emboli from the right atrium.
The nurse is reviewing the laboratory test results for a patient whose warfarin therapy was stopped before surgery. On postoperative day 2, the international normalized ratio (INR) result is 2.2. Which action would the nurse take?
Hold the daily dose of warfarin.
Give the prescribed dose of warfarin.
Call the health care provider to request discontinuing the warfarin.
Call the health care provider to request an increased dose of warfarin.
The therapeutic range for INR is 2.0 to 3.0 for many clinical diagnoses. To maintain therapeutic values, the nurse will administer the medication as ordered. Holding the medication would lower the INR, which would increase the risk of clot formation. Conversely, the higher the INR is, the more prolonged the clotting time. Calling the health care provider is not indicated.
Which new assessment finding would alert the nurse that a postoperative patient is not receiving the beneficial effects of enoxaparin (Lovenox)?
Crackles bilaterally in the lung bases
Pain and swelling in a lower extremity
Inability to initiate urination since surgery
Abdominal pain with decreased bowel sound
Enoxaparin is a low-molecular-weight heparin used to prevent the development of deep vein thromboses (DVTs) in the postoperative period. Pain and swelling in a lower extremity can indicate development of DVT and therefore may signal ineffective medication therapy.
The nurse is caring for a preoperative patient who has an order for vitamin K by subcutaneous injection. Which laboratory result would the nurse expect to be abnormal before administering the dose?
Hematocrit (Hct)
Hemoglobin (Hgb)
Prothrombin time (PT)
Activated partial thromboplastin time (aPTT)
Vitamin K counteracts hypoprothrombinemia and/or reverses the effects of warfarin and thus decreases the risk of bleeding. High values for either the PT or the international normalized ratio demonstrate the need for this medication.
The nurse is preparing to administer a scheduled dose of enoxaparin (Lovenox) 30 mg subcutaneously. Which action would the nurse take to administer this medication correctly?
Rub the injection site to enhance absorption.
Bunch up the skin before inserting the needle.
Remove the air bubble in the prefilled syringe.
Aspirate before injection to prevent IV administration.
The nurse should gather together or “bunch up” the skin between the thumb and the forefinger before inserting the needle into the subcutaneous tissue. The nurse should not remove the air bubble in the prefilled syringe, aspirate, nor rub the site after injection.
Which medications prescribed for patients with PAD would the nurse identify as being intended to decrease the risk of cardiovascular events ? (Select all that apply.)
Ramipril (Altace)
Cilostazol (Pletal)
Simvastatin (Zocor)
Clopidogrel (Plavix)
Warfarin (Coumadin)
Aspirin (acetylsalicylic acid)
Angiotensin-converting enzyme inhibitors (e.g., ramipril [Altace]) are used to control hypertension. Statins (e.g., simvastatin [Zocor]) are used for lipid management. Aspirin is used as an antiplatelet agent. Clopidogrel may be used if the patient cannot tolerate aspirin. Cilostazol (Pletal) is used for intermittent claudication, but it does not reduce CVD morbidity and mortality risks. Anticoagulants (e.g., warfarin [Coumadin]) are not recommended to prevent cardiovascular disease events in PAD patients.
A patient was admitted for possible ruptured aortic aneurysm. Ten minutes later, the nurse notes sinus tachycardia 138 beats/min, blood pressure is palpable at 65 mm Hg, increasing waist circumference, and no urine output. How would the nurse interpret the findings?
The renal arteries are involved.
Perfusion to the legs is interrupted
Tamponade will soon stop the bleeding.
Bleeding into the abdomen is continuing.
The patient is likely bleeding into the abdominal space, and it is likely to continue without surgical repair. A tamponade blockade of the blood flow will not occur in the abdominal space as it would in the retroperitoneal space, where surrounding anatomic structures may control the bleeding. The lack of urine output does not indicate renal artery involvement but that the bleeding is occurring above the renal arteries, which decreases the blood flow to the kidneys. There is likely to be decreased rather than interrupted perfusion to the legs.
An older adult with dementia has a venous ulcer related to chronic venous insufficiency. Which type of diet would the nurse explain to the patient and caregiver?
Low-fat diet
High-protein diet
Calorie-restricted diet
High-carbohydrate diet
A patient with a venous ulcer should have a balanced diet with adequate protein, calories, and micronutrients; this type of diet is essential for healing. Nutrients most important for healing include protein, vitamins A and C, and zinc. Foods high in protein (e.g., meat, beans, cheese, tofu), vitamin A (green leafy vegetables), vitamin C (citrus fruits, tomatoes, cantaloupe), and zinc (meat, seafood) must be provided. Restricting fat or calories is not helpful for wound healing or in patients of normal weight. For overweight individuals with no active venous ulcer, a weight-loss diet should be considered.
The nurse is caring for a patient with a recent history of deep vein thrombosis (DVT) who is scheduled for an emergency appendectomy. The patient’s international normalized ratio (INR) value is 1.0. Vitamin K is prescribed for immediate administration. Which nursing action is most appropriate?
Administer the medication as ordered.
Hold the medication and notify the surgical staff.
Hold the medication until the lab result is repeated to verify results.
Administer the medication and request an increased dose from the surgeon
Vitamin K is the antidote to warfarin, which the patient has likely been taking before admission for treatment of DVT. Warfarin is an anticoagulant that impairs the ability of the blood to clot. Therefore, it may be necessary to give vitamin K before surgery to reduce the risk of hemorrhage. However, the INR value is normal, and vitamin K is not required, so the medication would be held, and the surgical staff notified that it was not given.
The nurse is caring for a patient with vascular insufficiency who is prescribed enoxaparin (Lovenox) 30 mg subcutaneously. Which action would the nurse take to correctly administer this medication?
Spread the skin before inserting the needle.
Leave the air bubble in the prefilled syringe.
Use the back of the arm as the preferred site.
Place the patient in prone position before the injection.
The nurse would not expel the air bubble from the prefilled syringe because it should be injected to clear the needle of medication and avoid leaving medication in the needle track in the tissue.
A patient was just diagnosed with acute arterial ischemia in the left leg secondary to atrial fibrillation. Which early clinical manifestation must be reported to the provider promptly?
Paralysis
Cramping
Paresthesia
Referred pain
The provider must be notified immediately if any of the six Ps of acute arterial ischemia occur to prevent ischemia from quickly progressing to tissue necrosis and gangrene. The six Ps are paresthesia, pain, pallor, pulselessness, and poikilothermia, with paralysis being a very late sign indicating the death of nerves to the extremity. Crampy leg sensation is more common with varicose veins. The pain is not referred.
A patient with critical limb ischemia had peripheral artery bypass surgery to improve circulation. Which intervention would the nurse plan on the first postoperative day?
Keep the patient on bed rest.
Assist the patient to walk several times.
Have patient sit in the chair for 2 hours after meals.
Position the patient on their side with knees flexed.
To avoid blockage of the graft or stent, the patient should walk several times on postoperative day one and subsequent days. Having the patient’s knees flexed for sitting in a chair or in bed increase the risk of venous thrombosis and may place stress on the suture lines.
Which assessment findings of the left leg would the nurse identify as consistent with arterial occlusion? (Select all that apply.)
Edematous
Cold and mottled
Reports of paresthesia
Pulse not palpable with Doppler
Warmer than right lower extremity
Capillary refill less than 3 seconds
Arterial occlusion may result in loss of limb if not timely revascularized. When an artery is occluded, perfusion to the extremity is impaired or absent. On assessment, the nurse would note a cold, mottled extremity with impaired sensation or numbness. The pulse would not be identified, even with a Doppler. In contrast, the nurse would find edema, erythema, and increased warmth in the presence of a venous occlusion (deep vein thrombosis). Capillary refill would be greater than 3 seconds in an arterial occlusion and less than 3 seconds with a venous occlusion.
A patient is prescribed diltiazem for Raynaud’s phenomenon. Which assessment finding would indicate to the nurse that the medication is effective?
Resilient skin turgor
Decreased heart rate
Prompt capillary refill
Decreased mean arterial pressure
Raynaud’s phenomenon is an episodic vasospastic disorder of small cutaneous arteries, most frequently involving the fingers and toes. Diltiazem is a calcium channel blocker that relaxes smooth muscles of the arterioles by blocking the influx of calcium into the cells, thus reducing the frequency and severity of vasospastic attacks. Perfusion to the fingertips is improved, and vasospastic attacks are reduced. Diltiazem may decrease heart rate and blood pressure, but that is not the purpose in Raynaud’s phenomenon. Skin turgor is most often a reflection of hydration status.
Which intervention is a nursing priority for the care of a patient with chronic venous insufficiency (CVI)?
Applying topical antibiotics to venous ulcers
Positioning the patient’s legs below heart level
Administering oral or subcutaneous anticoagulants
Teaching the patient how to use compression stockings
CVI requires conscientious and consistent application of compression stockings. Anticoagulants are not necessarily indicated and antibiotics, if required, are typically oral or IV, not topical. The patient should avoid prolonged positioning with the limb in a dependent position.
A patient with peripheral artery disease is seen in the primary care clinic. Which symptom reported by the patient would indicate to the nurse that the patient is experiencing intermittent claudication?
Patient reports chest pain with strenuous activity.
Patient says leg muscle pain occurs with continued exercise.
Patient has numbness and tingling of all the toes and both feet.
Patient states the feet become red when they are in a dependent position.
Intermittent claudication is an ischemic muscle ache or pain that is precipitated by a consistent level of exercise, resolves within 10 minutes or less with rest, and is reproducible. Angina is the term used to describe chest pain with exertion. Paresthesia is the term used to describe numbness or tingling in the toes or feet. Reactive hyperemia is the term used to describe redness of the foot; if the limb is in a dependent position, the term is dependent rubor.
A nurse is caring for a patient with a diagnosis of deep venous thrombosis (DVT). The patient has 30 mg enoxaparin (Lovenox) prescribed. Which injection site would the nurse use to administer this medication?
Buttock, upper outer quadrant
Abdomen, anterior-lateral aspect
Back of the arm, 2 in away from a mole
Anterolateral thigh, with no scar tissue nearby
Enoxaparin (Lovenox) is a low-molecular-weight (LMW) heparin that is given as a deep subcutaneous injection in the right and left anterolateral abdomen. All subcutaneous injections should be given away from scars, lesions, or moles.
The nurse observes that phlebitis has developed at a patient’s peripheral IV site. Which intervention would the nurse implement first?
Remove the patient’s IV catheter.
Decrease the IV rate to 30 mL/hr.
Apply an ice pack to the affected area.
Administer prophylactic anticoagulants.
The priority intervention for superficial phlebitis is removal of the offending IV catheter. Decreasing the IV rate is insufficient. Anticoagulants are not normally required. Warm, moist heat is often therapeutic after catheter removal.
A middle-aged patient with diabetes has been diagnosed with peripheral artery disease (PAD). The patient smokes and has a history of gout. Which topic is the priority in patient teaching?
Smoking cessation
Appropriate vaccinations
Managing hypoglycemia
Drug therapy for gout flares
The first treatment goal for patients with PAD is to reduce CVD risk factors. Smoking is a significant PAD risk factor for this patient, and is modifiable with behavior change. Tobacco cessation is essential to reduce PAD progression, CVD events, and mortality. While diabetes and gout are risk factors, these topics are not related to hyperglycemia and hyperuricemia.
The assistive personnel (AP) suggests applying compression stockings to a patient with peripheral vascular disease. Which assessment finding would indicate that applying compression stockings could harm the patient?
Leg pain at rest
High blood pressure
Dry, itchy, flaky skin
Elevated blood glucose
Rest pain occurs as peripheral artery disease (PAD) progresses and involves multiple arterial segments. Compression stockings should not be used on patients with PAD. Elevated blood glucose, possibly indicating uncontrolled diabetes, and hypertension may or may not indicate arterial problems. Dry, itchy, flaky skin indicates venous insufficiency. The RN should be the one to obtain the order and instruct the AP to apply compression stockings if they are ordered.
A middle-aged woman with a history of smoking and oral contraceptive use is admitted with a venous thromboembolism (VTE) and prescribed unfractionated heparin. Which laboratory test would the nurse review to evaluate the effect of the heparin?
Platelet count
Activated clotting time (ACT)
International normalized ratio (INR)
Activated partial thromboplastin time (aPTT)
Unfractionated heparin can be given by continuous IV for VTE treatment. When given IV, heparin requires frequent laboratory monitoring of clotting status as measured by activated partial thromboplastin time (aPTT). Platelet counts can decrease as an adverse reaction to heparin.
The patient reports tenderness over a leg vein. The nurse assesses warmth and a palpable cord in the area. Which complication would the nurse plan to prevent?
Pulmonary embolism
Pulmonary hypertension
Postthrombotic syndrome
Venous thromboembolism
The manifestations are characteristic of a superficial vein thrombosis. If untreated, the clot may extend to deeper veins, and venous thromboembolism may occur. Pulmonary embolism, pulmonary hypertension, and postthrombotic syndrome are the sequelae of venous thromboembolism.
When the patient is being examined for venous thromboembolism (VTE) in the calf, which diagnostic test would the nurse expect to explain to the patient first?
Duplex ultrasound
Contrast venography
Magnetic resonance venography
Computed tomography venography
The duplex ultrasound is the most widely used test to diagnose VTE. Contrast venography is rarely used now. Magnetic resonance venography is less accurate for calf veins than pelvic and proximal veins. Computed tomography venography may be used but is invasive and much more expensive than the duplex ultrasound.
A patient with varicose veins has been prescribed compression stockings. Which instruction would the nurse give?
“Try to keep your stockings on 24 hours a day, as much as possible.”
“While you’re still lying in bed in the morning, put on your stockings.”
“Dangle your feet at your bedside for 5 minutes before applying your stockings.”
“The stockings are most effective if you remove and reapply them several times a day.”
The patient with varicose veins should apply stockings in bed before rising in the morning. Stockings should not be worn continuously and should not be removed several times daily. Dangling at the bedside before application is likely to decrease their effectiveness.
Which person would the nurse identify as having the highest risk for abdominal aortic aneurysm?
A 70-yr-old man with high cholesterol and hypertension
A 40-yr-old woman with obesity and metabolic syndrome
A 60-yr-old man with renal insufficiency who is physically inactive
A 65-yr-old woman with high homocysteine levels and substance use
The most common cause of descending abdominal aortic aneurysm (AAA) is atherosclerosis. Male gender, age 65 years or older, and tobacco use are the major risk factors for AAAs of atherosclerotic origin. Other risk factors include the presence of coronary or peripheral artery disease, high blood pressure, and high cholesterol.
The nurse is admitting a patient who has a suspected leaking abdominal aortic aneurysm (AAA). The medication history reveals that the patient has been taking warfarin daily. Which medication would the nurse be prepared to give?
Vitamin K
Cobalamin
Heparin sodium
Protamine sulfate
A patient with a leaking aneurysm may go to surgery for repair. Warfarin is a vitamin K antagonist anticoagulant that could cause excessive bleeding during surgery if clotting times are not corrected. Vitamin K is given as the antidote for warfarin.
Which priority intervention will help maintain graft patency for a patient who had aortic aneurysm repair 6 hours ago?
Assess urine output for renal dysfunction.
Give IV fluids to maintain adequate perfusion.
Administer diuretics to improve renal blood flow.
Maintain a low BP to prevent pressure on surgical site.
The priority is to maintain an adequate blood pressure (BP) (determined by the surgeon) to maintain graft patency. A prolonged low BP may result in graft thrombosis, and hypertension may cause undue stress on arterial anastomoses resulting in leakage of blood or rupture at the suture lines, which is when IV antihypertensives may be used. Renal output will be assessed when the aneurysm repair is above the renal arteries to assess graft patency, not maintain it.
1. Relate the etiology and pathophysiology of peripheral artery disease (PAD) to the major risk factors.
2. Describe the clinical manifestations and interprofessional and nursing management of the patient with PAD of the lower extremities
3. Plan appropriate nursing and interprofessional management for the patient with acute arterial ischemic disorders
4. Distinguish the pathophysiology, clinical manifestations, and nursing and interprofessional management of the patient with thromboangiitis obliterans (Buerger disease) and Raynaud phenomenon.
5. Distinguish the pathophysiology, clinical manifestations, and interprofessional and nursing management of patients with different types of aortic aneurysms.
6. Select appropriate nursing interventions for a patient undergoing an aortic aneurysm repair.
7. Describe the pathophysiology, clinical manifestations, and interprofessional and nursing management of the patient with aortic dissection.
8. Evaluate the patient’s risk factors for developing superficial vein thrombosis or venous thromboembolism (VTE).
9. Distinguish between the clinical characteristics of superficial vein thrombosis and VTE.
10. Outline the interprofessional and nursing management of patients with superficial vein thrombosis and VTE.
11. Prioritize the key aspects of nursing management for the patient receiving anticoagulant therapy.
12. Relate the pathophysiology and clinical manifestations to the interprofessional care of patients with varicose veins, chronic venous insufficiency, and venous leg ulcers.
acute arterial ischemia
aneurysm
aortic dissection
chronic venous insufficiency (CVI)
critical limb ischemia
deep vein thrombosis (DVT)
intermittent claudication
peripheral artery disease (PAD)
post-thrombotic syndrome (PTS)
superficial vein thrombosis
thromboangiitis obliterans (Buerger disease)
varicose veins
venous thromboembolism (VTE)
venous thrombosis
Virchow’s triad
Phlebitis = Acute inflammation of small, cannulated veins
Manifestations: pain, tenderness, warmth, redness, swelling, palpable cord
Risk Factors
Mechanical irritation from IV catheter
Infusion of irritating drugs
IV catheter location in flexion areas (e.g., wrist, antecubital area)
Avoid IV catheter insertion in flexion areas
phlebitis = rarely infectious
Resolves quickly after catheter removal
Elevate extremity if edema present → promote fluid reabsobtion
Apply warm, moist heat
Give oral NSAIDs (e.g., ibuprofen) or topical NSAIDs (e.g., diclofenac gel) for pain and inflammation
Venous Thrombosis = Formation of a thrombus (blood clot) with vein inflammation
Most common disorder of the veins
Classification = superficial or deep vein thrombosis
Superficial Vein Thrombosis
Thrombus in superficial veins (e.g., greater or lesser saphenous vein)
Deep Vein Thrombosis (DVT)
Thrombus in deep veins (e.g., iliac and/or femoral veins)
Venous Thromboembolism (VTE) = prefered terminology
Represents the spectrum from DVT to Pulmonary Embolism (PE)
Severity
Superficial vein thrombosis is serious
25% of patients with superficial vein thrombosis have DVT or PE at diagnosis
Patients at risk for recurrent VTE
The 3 key factors (called Virchow triad) that cause venous thrombosis are
(1) venous stasis
(2) damage of the endothelium (inner lining of the vein)
(3) hypercoagulability
The patient at risk for developing VTE usually has predisposing conditions to these 3 factors
Normal Venous Blood Flow Depends on:
Action of muscles in the extremities
Function of venous valves → allow one-directional flow
Venous Stasis
Occurs when:
Valves are dysfunctional
Muscles of extremities are inactive
High-Risk Groups for Venous Stasis
Obese individuals
Pregnant women
Patients with chronic HF or atrial fibrillation
Individuals on long trips without exercise
prolonged surgical procedure patients
Immobilized individuals due to injury or medical conditions
Damage to the endothelium may be caused by direct (e.g., surgery, intravascular catheterization, trauma, burns, prior VTE) or indirect (chemotherapy, diabetes, sepsis) injury.
Damaged endothelium stimulates platelet activation and starts the coagulation cascade.
This predisposes the patient to thrombus development.
Causes of Blood Hypercoagulability
Severe anemias
Polycythemia
Cancers (e.g., breast, brain, pancreas, GI tract)
Nephrotic syndrome
High homocysteine levels
Deficiency in protein C, protein S, and antithrombin
Sepsis (due to endotoxins released from bacteria)
Certain drugs (e.g., corticosteroids, estrogens)
Risk Factors for VTE in Women = very high risk factors
Tobacco use
Smoking causes hypercoagulability by increasing plasma fibrinogen and homocysteine levels and activating the intrinsic coagulation pathway.
Estrogen-based oral contraceptives
Postmenopausal women on oral hormone therapy
Women over 35 years old with a family history of VTE
Women who smoke and take oral contraceptives double their risk
Localized platelet aggregation and fibrin entrap RBCs, WBCs, and more platelets to form a thrombus
frequent site: valve cusp of vein → venous statis occurs there
thrombus enlarges → increased numbers of blood cells and fibrin collect behind it → makes are larger clot with tail that eventually blocks the lumen of vein
thrombus only partially blocks vein, endothelial cells cover thrombus and stop thrombotic process
thrombus does not become detached → undergoes lysis or becomes firmly organized and adherent within 5-7 days
organized thrombus may detach and result in an embolus
turbulent blood flow is major factor in embolization
thrombus become an embolus and flows through venous circulation to heart and lodges in pulmonary circulation becoming PE
Clincal Manifestations
patient with superficial vein thrombosis may have palpable, firm SQ cordlike vein
area around vein - itchy, painful to touch, reddened, warm, mild temp elevation and leukocytosis may be present
extremity edema may occur
LE superficial vein thombosis often involes varicose veins
Risk Factors
increased age, pregnancy, obesity, cancer, recent fracture(s), estrogen therapy, recent sclerotherapy (e.g., treatment for varicose veins), recent surgery or long-distance travel, hypercoagulability, and a history of chronic venous insufficiency (CVI), superficial vein thrombosis, or VTE. It can occur in people with endothelial problems (e.g., Buerger disease)
Interprofessional Care
US can confirm diagnosis (clot 5cm or larger) and rule out clot extension to a deep vein
superficial vein thrombosis affects very short vein segment and not near saphenofemoral junction → anticoagulants may not be needed
Oral NSAIDs can ease symptoms
other intervetions:
tell pt to wear graduated compression stockings/bandages
apply warm compresses
elevate affected limb above level of heart
apply topical NSAIDs
mild exercise
Clinical Manifestations
Pt with LE VTE → may have unilateral leg edema, pain, tenderness with palpation, dilated superficial veins, sense of fullness in thigh or calf, paresthesias, warm skin, redness, or systemic temperature greater than 100.4F (38C)
inferior vena cava involved → both legs may be edematous and cyanotic
~10% of VTEs involve upper extremity veins → may extend into internal Jugular vein or superior vena cava
if superior vena cava involved → similar symptoms may occur in arms, neck, back, face
complication
most serious complications of VTE are PE, chronic thromboembolic pulmonary hypertension, post-thrombotic syndrom, and phlegmasia cerulea dolens
Chronic Venous Hypertension
Vein wall and vein valve damage (acute inflammation and thrombus reorganization)
venous valve reflux
persistent venous outflow obstruction
Post-Thrombotic Syndrome (PTS)
Occurs in 8% to 70% of VTE patients
Results from chronic inflammation and venous hypertension
Symptoms: pain, swelling, cramps, tingling, etc.
Manifestations: edema, spider veins, ulcers, etc.
Symptoms
pain, aching, fatigue, heaviness, sensation of swelling, cramps, pruritus, tingling, paresthesia, bursting pain with exercise, and venous claudication.
Manifestations
persistent edema, spider veins (telangiectasia), venous dilation (ectasia), redness, cyanosis, increased pigmentation, eczema, pain during compression, atrophie blanche (white scar tissue), and lipodermatosclerosis
Venous ulceration can occur with severe PTS.
Signs of PTS typically begin within a few months to a few years of a VTE.
Risk factors include persistent leg symptoms 1 month after VTE, proximal VTE location (e.g., near the iliofemoral junction), extensive VTE, recurrent VTE on the same side, asymptomatic VTE, and residual thrombus. Other factors include obesity, older age, poor INR control, daily tobacco use before pregnancy, increased D-dimer levels, elevated inflammatory markers, and varicose veins.
Phlegmasia cerulea dolens (swollen, blue, painful leg) is a rare complication of severe lower extremity VTE.
It involves the major leg veins, causing near-total occlusion of venous outflow.
Patients typically have sudden, massive swelling; deep pain; and intense cyanosis of the extremity.
If untreated, the venous obstruction causes arterial occlusion and gangrene, requiring amputation.
Diagnosis of an initial VTE is based on the assessment combined with D-dimer testing and/or ultrasound. Table 41.9 presents the diagnostic studies used to determine the site or location and extent of a VTE.
Interprofessional CarePrevention
VTE prevention is a core measure of high-quality health care in high-risk hospitalized patients developed by The Joint Commission (TJC) and the National Quality Forum
. In patients at risk for VTE, interventions used are based on bleeding and thrombosis risk, medical history, current drugs, medical diagnoses, scheduled procedures, and patient preferences.
early aggressive mobilization = easiest and most cost effective method to decrease VTE risk
reposition every 2 hours if on bed rest
teach to flex and extend feet, knees, and hips ~2-4 hours while awake
pt should take meals out of bed in chair
walk 4-6x per day
anticoagulation and mechanical prophylaxis are not recommended for auctely ill medical pt at low risk for VTE
Graduated compression stockings
used along with anticoagulation
toes hole is under toes , heel patch over heel, thight gusset is on inner thigh and there are no wrickles
do not roll down stockings or alter them → impedes venous return
an cause arterial ischemia, edema, skin breakdown, and VTE.
not recommended in pt with VTE already
Intermittent pneumatic compression devices (IPCs)
inflatable sleeves or boot to compress calf an thigh and/or foot and ankle to improve venous return
may be used with graduated compression stockings
not effective if not fitted correctly or worn continuously at rest
not worn with pt has active VTE because of risk for PE
Drug Therapy
Anticoagulants are used routinely for VTE prevention and treatment.
goal of VTE prevention : prevent clot formation
goal for confirmed VTE: prevent new clot formation,spread of clot, embolization
3 major classes of anticoagulants available:
(1) vitamin K antagonists (VKAs)
for longterm or extended anticoagulation = warfarin (a VKA)
Warfarin inhibits activation of vitamin K dependent coagulation factors II, VII, IX, and X and anticoagulation proteins C and S
takes effect 48-72hrs and achieves max effect several days later
overlap of parenteral anticoagulant (UH or lowmolecular weight heparin [lmwh]) and warfarin typically required for 5 days
monitor level of anticoagulation daily using INR → INR standardized system of reporting prothrombin time (PT)
Take careful hx before starting warfarin
do not give antiplatelet drugs or NSAIDs with warfarin → increase bleeding risk
many other drugs, vitamins, mineral, and herbal supplements interact with warfarin
diet that varies in vitamin K intake can make it hard to achieve and maintain a target INR level
genetic variants in genes VKORC1 and cytochome P450 2C9 may influence how some people respond to warfarin
(2) thrombin inhibitors (both indirect and direct)
two major classes of indirect thrombin inhibitors: UH and LMWH
UH → affects both intrinsic and common pathways of blood coagulation by way of plasma antithrombin
antithrombin inhibits thrombin-mediated conversion of fibrinogen to fibrin by affecting factors II (prothrombin), IX, X, XI, and XII
heparin given given SQ for VTE prevention or by continuous IV infusion for VTE treatment
IV heparin use requires frequent monitoring of clotting status by measuring activated partial thromboplastin time (aPTT)
side effects
heparin induced thrombocytopenia (HIT) → immune reaction to heparin causes severe sudden decrease in platelet count along with paradoxical increase in veous or arterial thombosis
diagnose HIT → measuring presence of heparin antibodies in blood
treatment HIT → immediately stopping heparin therapy - give nonheparin anticoagulant
another effect of long term heparin therapy = osteoporosis
LMWHs → derived from UH
more predictable dose response, longer half life and fewer bleeding complications than UH
less likely to cause HIT and osteoporosis
typically do not require ongoing anticoagulant montiroing and dose adjustment
antiinflammatory properties may help prevent PTS and veous ulcer development
protamine reverses effect of LMWH
Direct thrombin inhibitors
classified as hirudin derivative or synthetic thrombin inhibitors
hirudin = made using recombinant DNA technology → binds specifically thrombin and directly inhibits its function without causing plasma protein and platelet interactions
hirudin derivatives given by continuous IV infusion (bivalirudin) → bivalirudin given to pt with or at risk for HIT having a percutaneous coronary intervention
anticoagulation monitored using aPTT or activaed clotting time (ACT)
if bleeding occurs → not antidoe for hirudin derivatives
Argatroban
synthetic direct thrombin inhibitor → hinders thrombin
like bivalirudin, alternative to heparin for prevention and treatment of HIT and for pt with or at risk for HIT needing percutaneous coronary interventions
effect of argatroban not reversible
anticoagulant effect monitored using aPTT or ACT
Dabigatran (Pradaxa)
oral direct thrombin inhibitor
used for VTE prevention after elective join replacement for stroke prevention in nonvalvular atrial fibrillation and as a treatment for VTE
5 major advantages compared to warfarin:
rapid onset
no need to monitor anticoagulation
few drug-food interactions
lower risk for major bleeding, and predictable dose response
(3) factor Xa inhibitors
Factor Xa inhibitors inhibit factor Xa directly or indirectly, producing rapid anticoagulation.
These include fondaparinux (Arixtra), rivaroxaban (Xarelto), apixaban (Eliquis), and edoxaban (Savaysa).
All are used for both VTE prevention and treatment.
Fondaparinux is contraindicated in patients with severe renal disease.
Although coagulation monitoring or dose adjustment is not needed, anticoagulant activity can be measured using anti-Xa assays
anticoagulation does not dissolve clot → clot lysis begins naturally through body’s intrinsic fibrinolytic system
Anticoagulant Therapy for VTE prevention
For VTE prevention in the hospitalized medical patient at risk for thrombosis who is not bleeding, low-dose UH, LMWH, or fondaparinux is used.
If the patient is at low VTE risk, drug prophylaxis is not needed.
Patients with moderate VTE risk (e.g., general, gynecologic, urologic surgery) should receive either UH or LMWH.
Patients with high VTE risk (e.g., trauma) should receive UH or LMWH until discharge.
Patients having abdominal or pelvic surgery for cancer or major orthopedic surgery (e.g., total knee or hip replacement) should receive VTE prophylaxis.
Anticoagulant therapy for VTE treatment
Patients with confirmed VTE should receive initial treatment with either LMWH, UH, or an oral factor Xa drug.
Oral VKA therapy may be an option.
A therapeutic INR is maintained between 2.0 and 3.0 if VKA therapy is used.
Active treatment of VTE should continue for at least 3 months.
Patients with multiple co-morbidities, complex medical issues, or a very large VTE usually are hospitalized for parenteral UH administration.
Depending on the presentation and home situation, patients may be safely managed as outpatients.
Thrombolytic therapy for VTE treatment
Another treatment option for patients with a thrombus is catheter-directed administration of a thrombolytic drug (e.g., urokinase, tPA).
It dissolves the clot(s), reduces the acute symptoms, improves deep venous flow, reduces valvular reflux, and may help to decrease the incidence of PTS.
Catheter-directed thrombolysis is an option for patients who have a low risk of bleeding and present with an acute, extensive, symptomatic, proximal VTE.
Systemic anticoagulation is needed before, during, and after catheter-directed thrombolysis.
ome pt with extensive, acute, proximal VTE who are not candidates for catheter-directed thromolysis and/or interventional radioolgy therapies may have surgery
Surgical Options
Open venous thrombectomy
Removal of clot through vein incision
Followed by anticoagulant therapy
Inferior vena cava interruption
Devices like Greenfield, Vena Tech, TrapEase filters
Percutaneous placement through femoral or internal jugular veins
Act as "sieve-type" device to filter clots without interrupting blood flow
Complications: air embolism, migration, perforation of vena cava
Filter may need removal and replacement over time due to clots clogging filter and completetly block vena cava
A filter device is recommended with acute PE or proximal VTE of the leg in patients with active bleeding or if anticoagulant therapy is contraindicated or ineffective.
Percutaneous endovascular interventional radiology procedures can be used along with catheter-directed thrombolytic therapy
Used for severely symptomatic patients with iliocaval or iliofemoral obstruction
Similar to lower extremity PAD treatments → difference = accessing an occluded vein instead of an artery
Options: mechanical thrombectomy, pharmacomechanical devices, angioplasty, stenting
Anticoagulation therapy recommended post iliofemoral interventional radiology procedure
Post-Procedure Nursing Care
Maintain catheter systems (if continuous infusions)
Monitor for bleeding, embolization, impaired perfusion
Provide VTE prevention teaching
Clinical problems for the patient with VTE include:
• Inadequate tissue perfusion
• Pain
• Impaired tissue integrity
• Impaired respiratory function
• Musculoskeletal problem
The overall goals for the patient with VTE include
(1) pain relief
(2) decreased edema
(3) increased knowledge of disorder and treatment plan
(4) no skin ulceration
(5) no bleeding complications
(6) no evidence of PE
focus on preventing thrombi and reducing inflammation
Review medications, vitamins, minerals, and herbal supplements that may interfere with anticoagulant therapy
Monitor various levels depending on anticoagulant ordered:
INR, aPTT, ACT, anti-factor Xa levels
CBC, creatinine, factor X levels, hemoglobin, hematocrit, platelet levels, liver enzymes
Monitor platelet counts for patients on UH or LMWH to assess for HIT
May need to Adjust direct thrombin inhibitors for patients with renal or liver disease
Check pertinent test results before initiating, administering, or changing anticoagulant therapy
Identify factors increasing bleeding risk:
Active gastroduodenal ulcer, prior bleeding history, low platelet count
Hepatic or renal failure, rheumatic disease, cancer, age >85 years
Patients with INR >5.0 on warfarin have higher bleeding risk
Administer reversal agents or adjust dosages for anticoagulation above target goals
Early ambulation post-VTE does not increase short-term PE risk
Benefits of early ambulation:
Rapid decrease in edema and limb pain
Fewer post-thrombotic syndrome symptoms
Improved quality of life
Educate patient and caregiver on the importance of physical activity
Encourage ambulation multiple times a day
Consider bed rest with limb elevation for patients with severe edema and limb pain initially
Discuss Modifying VTE Risk Factors
Stop smoking and avoid all nicotine products
Avoid constrictive clothing
Discontinue oral contraceptives or hormone therapy for women with a history of VTE
Limit standing or sitting in a motionless, leg-dependent position
Exercise calf muscles, take short walks, and stay hydrated during long-distance travel
Consider knee-high graduated compression stockings for high-risk individuals during travel
Monitoring Laboratory Values and Drug Instructions
Regularly monitor INR levels with home monitoring devices
Educate on subcutaneous administration of LMWH or fondaparinux
Follow consistent diet with vitamin K-containing foods for warfarin users
Avoid vitamin K supplements, excess vitamin E, and alcohol
Ensure routine blood tests and immediate medical attention for specific symptoms
Diet and Lifestyle Recommendations
Maintain a well-balanced diet
Encourage hydration to prevent hypercoagulability
Implement weight management plan for overweight patients
Develop an exercise program focusing on leg strength training and aerobic activity
Consider graduated compression stockings or IPCs for swelling and PTS management
Follow-Up Guidelines
Contact emergency services for signs of PE
Review drug dosage, actions, and side effects
Emphasize the importance of routine follow-up and adherence to recommendations
The expected outcomes are that the patient with VTE will have:
• Minimal to no pain
• Intact skin
• Increased knowledge of disorder and treatment plan
• No signs of hemorrhage or occult bleeding
varicose veins = dilated tortuous superficial veins → often found in saphenous vein system
may be small and harless or large and bulging
primary varicose veins (idiopathic) → due to weakness of vein wals more common in women
secondary varicose veins → result from direct injury, previous VTE, or excess vein distention
may occur in esophagus, vulva, spermatic cords, and anorectal area (hemorrhoids) and abnormal ateriovenous connections (AV)
congenital varicose veins = chromosomal defects that cause abnormal development of venous system
reticular veins = smaller varicose veins that appear flat, less tortuous, and blue green in color
Telangiectasias (spider veins) = small visible vessels that appear bluish, black, purple or red
superficial veins in LE become dilated and tortuous in response to backward blood flow and increased venous pressure
risk factors:
family hx of chornic venous disease
weak vein structure
female
tobacco
inc age
obesity
multiparity
hx of VTE
venous obstruction resulting of extrinsic pressure by tumors
thrombophilia
phlebitis
previous leg injury
occupation that reuiqre prolonged standing of sitting
primary varicose veins → weak veins walls allow vein valve ring to enlarge - leaflets no longer fit together properly incompetent
incompetent vein valves allow backward blood flow → particularly when pt is standing
results in increased venous pressure and further venous distention
high pressure in superficial veins can be caused by vein valve dysfunction in deep veins or perforator veins
veins that perforate the deep fascia of muscles to connect the superficial veins to the deep veins
Variability of Discomfort
Varies among individuals
Intensifies after episodes of superficial vein thrombosis
Prevalence
More common in women than men
Common Symptoms
Heavy, achy feeling or pain after prolonged standing or sitting
Pain relieved by walking or limb elevation
Pressure, itching, burning, tingling, throbbing, or cramp-like leg sensations
Swelling, restless or tired legs, fatigue, and nocturnal leg cramps
Complications
Superficial venous thrombosis is the most frequent complication
Spontaneous occurrence or post-trauma, surgery, or pregnancy
Rare complications include:
Rupture of varicose veins leading to external bleeding
Skin ulcerations
Superficial varicose veins often can be diagnosed by physical assessment.
Duplex ultrasound imaging is the gold standard to evaluate venous anatomy, valvular competence, and venous obstruction.
Conservative treatment involves rest with limb elevation; graduated compression stockings; leg strengthening exercise, such as walking; and weight loss, if indicated.
Venoactive drugs stimulate release of chemicals in vein walls
Strengthen circulation, reduce inflammation, and edema
Types of Venoactive Agents
Micronized purified flavonoid fraction
Rutosides (e.g., horse chestnut seed extract)
Proanthocyanidins (from grapes and apples)
Ruscus (butcher’s broom)
Therapeutic Benefits
Pain relief
Edema reduction
Decreased leg cramping and restless legs
Usage and Approval
Widely used in Europe
Not FDA approved
Available over the counter as diet or herbal supplements
sclerotherapy → direct IV injection of liquid or foam sclerosing substance that chemically ablates treated veins
hypertonic saline, polidocanol, glycerin
used on telangiectasias, perforator veins, reticular veins, smaller varicose veins, and venous malformations
done inoffice setting - minimal discomfort
transcutaneous laser therapy for telangiectasias and high-intensity pulsed-light therapy for reticular veins.
used for pt in whom sclerotherapy is contraindicated or ineffective
works by heating hemoglobin in vessels → results in vessel sclerosis
complications
pain, blistering, hyperpigmentation, and superficial erosions
endovenous ablation using thermal energy from radiofrequency or laser therapy → for saphenous vein reflux (minimally invasive)
inserts a catheter into the vein to heat the vein wall, which then causes the vein to collapse
complications
bruising, skin burns, hyperpigmentation, infection, paresthesia, superficial or deep vein thrombosis, and PE
graduated compression stockings and bandages are worn afterwards
Endovenous thermal ablation may be done in combination with surgical ligation or phlebectomy.
surgical intervention → for recurrent superficial venous thrombosis or when symptoms cannot be controlled with other therapy
The traditional surgical intervention involves ligation of the entire vein (usually the greater saphenous vein) and removal of its incompetent branches.
An alternative but time-consuming technique is ambulatory phlebectomy. This involves pulling the varicosity through a “stab” incision followed by excision of the vein.
Transilluminated powered phlebectomy involves the use of a tissue resector to destroy clusters of varicosities and removes the pieces via aspiration. Complications include bleeding, bruising, and infection.
prevention = key in varicose veins
avoid sitting and standing long periods
maintain ideal body weight
precautions against injury to extremities
avoid wearing constrictive clothing
walk daily
after vein ligation surgery:
deep breathe → promote venous return
check extremities for color, movement, sensation, temp, edema, quality of pedal pulses
some brusing and discoloration is normal
elevate legs 15 degrees → limit edema
remove graduated compression stockings or bandages every 8 hours for short period and then reapply them
long-term managment directed toward improving ciruclation and appearance → relieving discomfort and avoiding complications
can reoccur in other veins after surgery
teach pt proer use and care of custom fitted graduated compression stockings
pt should apply stockings in bed before rising in morning
emphasize importantace of periodic positioning of legs above heart
overweight pt may need help with weight loss
pt with job that requires long periods of standing or sitting needs to be frequently flex and extend hips, legs, and ankles and changes positions
Chronic venous insufficiency (CVI) = abnormalities of venous system that result in adv signs and symptoms such ad edema, skin chagnes and/or venous leg ulcers
CVI can lead to venous leg ulcers
not life threatening but painful, slow to heal , debilitating, costly conditions → adversely affect pt quality of life
common in older adults
both long standing pirmary varicose veins and PTS can progress to CVI
ambulatory venous hypertension causes serous fluid and RBCs to leak from capillaries and venules into tissue
causes edema and chronic inflammatory changes
enzymes in tissue eventually break down RBCs
this released hemosiderin → causes brownish skin discoloration
overtime → fibrous tissue replaces skin and SQ tissue around ankle
results in thick harded contracted skin - caused of CVI known, exact pathophysiology of venous leg ulcers is unknown
Skin Appearance
Leathery texture in lower leg
Brownish or "brawny" appearance due to hemosiderin deposition
Edema
Persistent for prolonged period
May lead to pain, especially with infection
Eczema
Itching and scratching common
Associated with skin changes and discomfort
Venous Ulcers
Location: above the medial malleolus
Painful, especially with edema or infection
Pain worsens in dependent leg position
Progression
Untreated ulcers widen and deepen
Increased risk of infection and complications
Compression = essential for venous ulcer healing and preventing venous ulcer recurrence
options for compression thearpy:
custom-fitted graduated compression stockings
elastic tubular support bandages
a Velcro wrap (CircAid)
IPCs
multilayer (3 or 4) bandage systems (e.g., Profore).
assess to make sure PAD not present → ABI of 0.4 or less suggests severe PAD → compression thearpy contraindicated
wear daily to prevent recurrent leg ulcers
replace stockings ~4-6 months
Activity
avoid standing or sitting for long periods → dec blood return from LE
teach pt elevate legs above level of heart to reduce edema
daily walking program once an ulcer heals
avoid tauma limbs
teach foot care
Dressings
moist environemtn dressings = basis of wound care
variety of dressings:
include transparent film dressings, hydrocolloids, hydrogels, foams, alginates, gauze, and combination dressings.
Dressing decisions should be based on wound characteristics, cost, best evidence, and clinician judgment
Evaluate pt nutrition
balanced diet (below best for healing)
high protein
vitamin a
vitamin C
zinc
pt with diabetes → maintain normal blood glucose levels and aids in healing process
venous leg ulcers are colonized by bacteria → routine use of antibiotics is not indicated
signs of infection:
quantity, color, or odor of the drainage; pus; redness of the wound edges; change in sensation around the wound; and warmth around the wound.
There may be increased local pain, edema, or both; dark-colored granulation tissue; induration around the wound; delayed healing; and cellulitis.
If signs of infection occur, obtain a wound culture.
Culture results guide antibiotic therapy.
The usual treatment for infection is wound debridement, wound excision, and systemic antibiotics.
if does not heal with conservative therapy → drug thearpy should be considered
Pentoxifylline is recommended with compression therapy to improve healing
Pentoxifylline minimizes WBC activation and adhesion to capillary endothelium and decreases oxidative stress.
Other treatments are considered for large venous leg ulcers that do not respond to standard therapy after 4 to 6 weeks.
These include coverage with a skin replacement or substitute, such as split-thickness skin grafts or artificial bioengineered skin.
Although grafts help with healing, they do not replace the need for lifelong compression therapy.
Patients with CVI have dry, flaky, itchy skin.
Daily moisturizing decreases itching and prevents skin cracking.
Contact dermatitis may result from contact with sensitizing products.
These include such as topical antimicrobial agents (e.g., gentamicin); additives in bandages or dressings (e.g., adhesives); ointments containing lanolin, alcohols, or benzocaine; and over-the-counter creams or lotions with fragrance or preservatives.
Assess wounds for signs of infection with each dressing change
Peripheral Artery Disease
Peripheral artery disease (PAD) is a progressive narrowing and degeneration of the arteries of the upper and lower extremities. In most cases, it is a result of atherosclerosis.
Significant risk factors for PAD are tobacco use (most important), chronic kidney disease, diabetes, uncontrolled hypertension, and hypercholesterolemia.
Peripheral Artery Disease of the Lower Extremities
PAD of the lower extremities affects the iliac, femoral, popliteal, tibial, or peroneal arteries.
The severity of manifestations depends on the site and extent of blockage and the amount of collateral circulation.
The classic symptom of PAD of the lower extremities is intermittent claudication. Other symptoms include paresthesia, numbness or tingling in the toes or feet, rest pain, and the loss of both pressure and deep pain sensations.
Physical findings include thin, shiny, and taut skin with loss of hair on the lower legs; decreased or absent pedal, popliteal, or femoral pulses; elevation pallor; and reactive hyperemia when the limb is in a dependent position.
Complications of PAD include nonhealing ulcers over bony prominences on the toes, feet, and lower leg, and gangrene. Amputation may be needed if blood flow is not restored.
Tests used to diagnose PAD include Doppler ultrasound with segmental blood pressures, calculating the ankle-brachial index (ABI), and angiography.
The overall goals for the patient with lower-extremity PAD include adequate tissue perfusion, relief of pain, increased exercise tolerance, and intact, healthy skin on extremities.
The first treatment goal for patients with PAD is to aggressively modify all cardiovascular risk factors. All tobacco use must be stopped.
Drug therapy includes statins, antiplatelet agents, and angiotensin-converting enzyme (ACE) inhibitors. Two drugs approved to treat intermittent claudication are cilostazol and pentoxifylline.
The main nondrug treatment for claudication is tobacco cessation and a formal exercise training program. Walking is the most effective exercise.
Interventional radiologic procedures for PAD include percutaneous transluminal balloon angioplasty with stenting or atherectomy.
The most common surgical procedure for PAD is a peripheral arterial bypass operation with autogenous vein or synthetic graft material to bypass or carry blood around the lesion.
Teach patients with PAD the importance of meticulous foot care.
Critical limb ischemia is a chronic condition in advanced PAD characterized by ischemic rest pain, arterial leg ulcers, and/or gangrene of the leg.
ACUTE ARTERIAL ISCHEMIC DISORDERS
Acute arterial ischemia is a sudden interruption in the arterial blood supply to a tissue, organ, or extremity. If untreated, it results in tissue death.
Common causes include embolism, thrombosis, or trauma.
Signs and symptoms of an acute arterial ischemia usually have an abrupt onset and include the
“6 Ps”: pain, pallor, pulselessness, paresthesia, paralysis, and poikilothermia.
Treatment options include anticoagulation, thrombolysis, embolectomy, surgical revascularization, or amputation.
Thromboangiitis Obliterans
Thromboangiitis obliterans (Buerger’s disease) is a nonatherosclerotic, segmental, recurrent inflammatory disorder of the small and medium arteries, veins, and nerves of the arms and legs. • Patients may have intermittent claudication of the feet, hands, or arms. As the disease progresses, rest pain and ischemic ulcerations develop.
There are no laboratory or diagnostic tests specific to Buerger’s disease.
Treatment includes complete cessation of tobacco use in every form. Conservative management includes the use of antibiotics to treat any infected ulcers and analgesics to manage the ischemic pain.
Surgical options include revascularization, implantation of a spinal cord stimulator, and sympathectomy.
Raynaud’s Phenomenon
Raynaud’s phenomenon is an episodic vasospastic disorder of small cutaneous arteries, most often involving the fingers and toes. The exact cause is unknown.
Manifestations include vasospasm-induced color changes of the fingers, toes, ears, and nose (white, blue, and red). An episode usually lasts only minutes. In severe cases, may last for several hours.
Symptoms usually are precipitated by exposure to cold, emotional upsets, caffeine, and tobacco use.
Diagnosis is based on persistent symptoms for at least 2 years. There is no diagnostic test.
Teach patients to prevent recurrent episodes by avoiding temperature extremes and all tobacco products.
Calcium channel blockers are the first-line drug therapy.
AORTIC ANEURYSMS
Aortic aneurysms are outpouchings or dilations of the arterial wall.
The causes of aortic aneurysms are degenerative, congenital, mechanical, inflammatory, or infectious.
Aortic aneurysms may involve the aortic arch and thoracic aorta. Most are found in the abdominal aorta below the level of the renal arteries.
Thoracic aortic aneurysms are often asymptomatic. The most common manifestations are deep, diffuse chest pain that may extend to the interscapular area; hoarseness; and dysphagia.
Abdominal aortic aneurysms (AAAs) are often asymptomatic, but symptoms may mimic pain associated with abdominal or back disorders.
The most serious complication related to an untreated aneurysm is rupture and bleeding.
Diagnostic tests for AAAs include chest x-ray, electrocardiogram (to rule out myocardial infarction), echocardiography, computed tomography (CT) scan, and magnetic resonance imaging (MRI) scan.
The goal of management is to prevent the aneurysm from rupturing.
Surgical repair is done for aneurysms that are greater than 5 cm in size, are rapidly expanding, or have a high risk for rupture, and in patients who are symptomatic.
Minimally invasive endovascular aneurysm repair is an alternative to conventional surgical repair and involves the placement of a sutureless aortic graft into the abdominal aorta inside the aneurysm.
The overall goals for a patient undergoing aortic surgery include normal tissue perfusion, intact motor and sensory function, and no complications related to surgical repair, such as thrombosis or infection.
After surgery, the patient typically needs close monitoring in an ICU setting.
Monitoring for graft patency and adequate renal perfusion is a priority.
Maintenance of an adequate BP is extremely important.
Antibiotics are given to prevent infection.
Peripheral pulses, skin temperature and color, capillary refill time, and sensation and movement of the extremities are assessed and recorded per hospital policy.
Hourly urine outputs and daily weights are recorded.
On discharge, teach the patient to gradually increase activities but to avoid heavy lifting for 6 weeks.
Aortic Dissection
Aortic dissection results from the creation of a false lumen between the intima (inner lining) and the media (middle layer) of arterial wall.
The most likely causes of aortic dissection are degeneration of the elastic fibers in the medial layer and chronic hypertension.
Type A aortic dissection affects the ascending aorta and arch. Type B aortic dissection starts in the descending aorta.
Dissections are classified as acute (first 14 days), subacute (14 to 90 days) or chronic (greater than 90 days) based on symptom onset.
Patients with an acute ascending aortic dissection report sudden, severe onset of excruciating chest and/or back pain radiating to the neck or shoulders. Patients with acute descending aortic
dissection are more likely to report pain in their back, abdomen, or legs and describe the pain as
“sharp” and “worst ever” followed less often by “tearing” or “ripping.”
Diagnostic studies used to assess aortic dissection are similar to those done for AAA.
The initial goal of therapy for aortic dissection without complications is to lower the heart rate and BP and manage pain.
β-blockers are the drugs of choice to lower the heart rate and BP.
An acute Type A aortic dissection is a surgical emergency.
Otherwise, surgery is indicated when drug therapy is ineffective or when complications of aortic dissection are present.
Venous Thrombosis
Phlebitis is the inflammation of the walls of the small, cannulated veins of the hand or arm and presents with 2 or more of the following symptoms: pain, tenderness, warmth, erythema, swelling, and a palpable cord.
Venous thrombosis is the most common disorder of the veins and involves the formation of a thrombus (clot) in association with inflammation of the vein. Venous thromboembolism (VTE) represents the spectrum of pathology from deep vein thrombosis (DVT) to pulmonary embolus.
DVT involves a thrombus in a deep vein, most often the iliac and femoral veins. It can result in embolization of thrombi to the lungs.
Three key factors (called Virchow’s triad) that cause venous thrombosis are (1) venous stasis,
(2) damage of the endothelium, and (3) hypercoagulability of the blood.
Superficial vein thrombosis involves a thrombus in a superficial vein, presenting as a palpable, firm, subcutaneous cordlike vein. The surrounding area may be tender to the touch, reddened, and warm. A mild systemic temperature elevation and leukocytosis may be present.
Recommended treatment for lower leg superficial vein thrombosis consists of a prophylactic dose of fondaparinux (Arixtra).
Graduated compression stockings, elevation of leg, oral and topical nonsteroidal antiinflammatory drugs, and exercise, such as walking, are recommended for symptom relief. • The patient with lower extremity VTE may or may not have unilateral leg edema, pain, tenderness with palpation, dilated superficial veins, a sense of fullness in the thigh or calf, paresthesia, warm skin, erythema, and/or a systemic temperature greater than 100.4° F (38° C). • The most serious complications of VTE are PE, chronic thromboembolic pulmonary hypertension, post-thrombotic syndrome (PTS), and phlegmasia cerulea dolens.
Post-thrombotic syndrome (PTS) results from chronic inflammation and chronic venous hypertension caused by vein wall and vein valve damage, venous valve reflux, and persistent venous obstruction.
Symptoms include pain, aching, heaviness, swelling, cramps, itching, and tingling. Signs include persistent edema, increased pigmentation, eczema, secondary varicosities, and lipodermatosclerosis.
VTE prophylaxis for hospitalized patients depends on individual risk and may involve early ambulation, graduated compression stockings, intermittent pneumatic compression devices, and anticoagulation.
The goals in the treatment of VTE are to prevent propagation of the clot, development of any new thrombi, and embolization. Anticoagulation therapy is routinely used.
Three major classes of anticoagulants are available: (1) vitamin K antagonists, (2) thrombin inhibitors (direct and indirect), and (3) factor Xa inhibitors.
Warfarin, a vitamin K antagonist, inhibits activation of the vitamin K-dependent coagulation factors.
Indirect thrombin inhibitors include unfractionated heparin (UH) and low-molecular-weight heparin (LMWH)
Examples of direct thrombin inhibitors include dabigatran (Pradaxa) and the hirudin derivatives, bivalirudin (Angiomax) and desirudin (Iprivask).
Factor Xa inhibitors include subcutaneous fondaparinux (Arixtra) and oral agents including rivaroxaban (Xarelto), apixaban (Eliquis), and edoxaban (Savaysa).
Some VTE patients need surgical or endovascular therapy, including thrombectomy and placement of vena cava interruption devices, such as the Greenfield filter.
Nursing and collaborative care for the patient with VTE revolve around managing acute pain, the risk for impaired tissue integrity, and the potential complications of bleeding related to anticoagulant therapy and pulmonary embolism.
Discharge teaching should focus on elimination of modifiable risk factors for VTE, the importance of graduated compression stockings and monitoring of laboratory values, medication instructions, and guidelines for follow-up.
Varicose Veins
Varicose veins, or varicosities, are dilated, tortuous subcutaneous veins most often found in the saphenous system.
The cause of varicose veins is unknown. Risk factors include family or personal history of chronic venous disease, weak vein structure, female gender, tobacco use, increasing age, obesity, multiparity, venous obstruction resulting from thrombosis or extrinsic pressure by tumors, thrombophilia, phlebitis, previous leg injury, or occupations that require prolonged standing.
The most common symptom is an ache or pain after prolonged standing, which is relieved by walking or by elevating the limb. Nocturnal leg cramps in the calf may occur.
Interprofessional care involves rest with the affected limb elevated, compression stockings, and exercise, such as walking.
Several treatment options exist, including sclerotherapy, transcutaneous laser or high-intensity pulsed-light therapy, endovenous thermal ablation and surgical procedures, such as phlebectomy and vein ligation.
Prevention is a key factor related to varicose veins. Teach the patient measures to promote venous circulation.
Chronic Venous Insufficiency and Venous Leg Ulcers
Chronic venous insufficiency (CVI), a common medical problem in older adults, describes functional abnormalities of the venous system that result in advanced venous signs and symptoms, such as edema, skin changes, and/or venous leg ulcers.
CVI can result from long-standing varicose veins or post-thrombotic syndrome and can lead to venous leg ulcers.
Manifestations include the skin of the lower leg appearing leathery, with a characteristic brownish or “brawny” appearance, edema and eczema, and pruritus.
Venous ulcers classically occur above the medial malleolus. The wound margins are irregularly shaped, and the tissue is typically a ruddy color. Ulcer drainage may be extensive. Pain is present and may be worse when the leg is in a dependent position.
Compression is essential for venous ulcer healing and prevention of ulcer recurrence.
Compression options include elastic wraps, custom-fitted graduated compression stockings, elastic tubular support bandages, a Velcro wrap, intermittent pneumatic compression devices, and multilayer (3 or 4) bandage systems.
Moist environment dressings are the basis of wound care and include transparent film dressings, hydrocolloids, hydrogels, foams, alginates, impregnated gauze, dextranomer, flax, and combination dressings.
Assess nutritional status.
Monitor wounds for signs of infection. The usual treatment for infection is debridement, wound excision, and systemic antibiotics.
Adjuvant treatments include coverage with a split-thickness skin graft, cultured epithelial autograft, allograft, bioengineered skin, or porcine small intestinal submucosal tissue construct.
Long-term management of venous leg ulcers should focus on teaching the patient about self-care measures because the incidence of recurrence is high.
Proper foot and leg care is essential to avoid further trauma to the skin.
The patient with CVI should avoid standing or sitting with the feet dependent for long periods.
Teach patients with venous ulcers to elevate their legs above the level of the heart to reduce edema.
Once an ulcer is healed, encourage a daily walking program.
Prescription graduated compression stockings should be worn daily and replaced every 4 to 6 months to limit edema and reduce ulcer recurrence.
1. Recognize: What risk factors do you identify that led to S.J. having PAD?
Risk factors for PAD include: Black, advanced age, past medical history of myocardial infarction, high blood pressure and diabetes, previous femoral-popliteal bypass, long-term smoking, and sedentary lifestyle.
2. Analyze: What are the important findings from S.J.’s assessment?
The important assessment findings include the sudden intense increase in pain to the right foot; the right foot is very cool, pale, and mottled in color with decreased sensation; and no right dorsalis pedis pulse. This worsening pain and change in pulses/skin condition are due to the sudden decrease in oxygen and blood supply distal to the occluded artery. The most likely cause for the sudden increase in right foot pain is acute arterial ischemia resulting from a thrombus development at an existing atherosclerotic plaque of the lower leg
3. Plan: What treatment options are possible?
The first priorities of interprofessional care would be prevention of thrombus propagation or further embolization and control of ischemic pain followed by restoring blood flow by removal of the thrombus via either surgical or catheter-based treatments described previously. Options for embolus/thrombus removal consist of percutaneous catheter-directed thrombolytic therapy, percutaneous mechanical thrombectomy with or without thrombolytic therapy, surgical thrombectomy, or surgical bypass. Determining which intervention to use is dependent upon stenosis location and the type and severity of the occlusion. Open surgical techniques for salvage of an ischemic limb include bypass procedures to direct blood flow beyond the occlusion and endarterectomy with or without patch angioplasty and intraoperative isolated limb thrombolysis. He has a strong history of cardiovascular problems. Drug therapy can decrease his risk of cardiovascular mortality. Other drug therapy options include a lipid-lowering statin and a beta adrenergic blocker. Evaluation of his lipid profile would determine if drug therapy is needed for high triglycerides and low HDL. He will likely be discharged on warfarin (Coumadin) and will require thorough education about the drug, side effects, and associated precautions
4. Prioritize: What is the important thing the team can do for S.J.?
Immediate priorities for S.J. include: (1) maximizing tissue perfusion, (2) relieving pain, and (3) preparing the patient for treatment procedures. A key nursing responsibility will be giving IV anticoagulants as ordered to prevent thrombus propagation. The lower extremities should be checked frequently for color, temperature, capillary refill, presence of peripheral pulses, and sensation and movement. Any deterioration in vascular status immediately needs to be reported to the HCP. Keep the limb warm to maximize perfusion. The use of a bed cradle/frame for the lower extremities to keep blankets from contact with the ischemic limb may reduce patient discomfort and tissue injury. If dehydration is a predisposing factor to the thrombosis, IV fluid hydration may need to be given. Depending on the planned treatment, you will be responsible for preparing the patient and caregiver for either a surgical or catheter-based procedure.
5. Act: What role do APs have in providing care?
The UAP can obtain vital signs; perform bedside glucose testing (per agency policy); helping S.J. with toileting, personal hygiene needs, and meals; monitoring oral intake and output; and reporting any changes in pain
6. Evaluate: What do you need to continually monitor?
You would need to continually monitor S. J’s pain; peripheral pulses (posterior tibial pulse and dorsalis pedis pulse) in both extremities; signs of bleeding (bruising, purpura, bloody stools, bleeding for intravenous sites); and intake/output.
7. Safety: What safety precautions should we consider?
Remind S.J. that he cannot get out of bed without assistance because of his risk of falling, consider using a bed alarm; S.J. needs to be monitored for bleeding, he is receiving a medication to help dissolve the clot in his leg, which significantly increases his risk of bleeding. S.J. and his caregiver will need to be educated on precautions related to anticoagulant use upon discharge.
1. A 50-year-old woman who weighs 95 kg has a history of high blood pressure, high sodium intake, tobacco use, and sedentary lifestyle. Which is the most important risk factor for peripheral artery disease (PAD) to address in the nursing plan of care?
a. Salt intake
b. Tobacco use
c. Excess weight
d. Sedentary lifestyle
The most important risk factor for peripheral artery disease is tobacco use. Other risk factors include increased levels of high-sensitivity C-reactive protein, diabetes, uncontrolled hypertension, family history, high triglyceride and lipid levels, hyperuricemia, increasing age, obesity, sedentary lifestyle, and stress.
2. Which information would the nurse include when explaining the cause of rest pain with PAD?
a. Vasospasm of cutaneous arteries in the feet
b. Decrease in blood flow to the nerves of the feet
c. Increase in retrograde venous perfusion to the lower legs
d. Constriction in blood flow to leg muscles during exercise
Rest pain most often occurs in the forefoot or toes when arterial blood flow is insufficient to meet basic metabolic requirements of the distal tissues. Nerves transmit pain messages because of the tissue ischemia. Rest pain occurs more often at night because cardiac output tends to drop during sleep and the limbs are at the level of the heart. Patients often try to achieve some pain relief by dangling the leg over the side of the bed or sleeping in a chair to allow gravity to maximize blood flow.
3. A patient with infective endocarditis develops sudden left leg pain with pallor, paresthesia, and a loss of peripheral pulses. Which action would the nurse take first?
a. Notify the HCP of the change in perfusion.
b. Start anticoagulant therapy with IV heparin.
c. Elevate the leg to improve the venous return.
d. Position the patient in reverse Trendelenburg.
The patient may have acute arterial ischemia (sudden interruption in the arterial blood supply to the extremity), caused by an embolism from a cardiac thrombus that occurred as a complication of infective endocarditis. Manifestations include any or all of the 6 Ps: pain, pallor, paralysis, pulselessness, paresthesia, and poikilothermia. Without immediate intervention, ischemia may progress quickly to tissue necrosis and gangrene within a few hours. If the nurse detects these signs, the HCP should be notified immediately.
4. Which clinical manifestations can the nurse expect to see in both patients with Buerger disease and patients with Raynaud phenomenon? (select all that apply)
a. Intermittent low-grade fevers
b. Sensitivity to cold temperatures
c. Gangrenous ulcers on fingertips
d. Color changes of fingers and toes
e. Episodes of superficial vein thrombosis
Buerger’s disease and Raynaud’s phenomenon have these manifestations in common:
cold sensitivity, ischemic and gangrenous ulcers on fingertips, and color changes of the distal extremity (fingers or toes).
5. A patient is admitted to the hospital with a diagnosis of abdominal aortic aneurysm. Which signs and symptoms would suggest that the aneurysm has ruptured?
a. Rapid onset of shortness of breath and hemoptysis
b. Sudden low back pain and bruising along the flank
c. Patchy blue mottling on feet and toes and rest pain
d. Gradually increasing substernal chest pain and diaphoresis
The manifestations of a ruptured abdominal aortic aneurysm include severe back pain, back or flank ecchymosis (Grey Turner’s sign), and hypovolemic shock (tachycardia, hypotension, pale clammy skin, decreased urine output, altered level of consciousness, and abdominal tenderness).
6. Which nursing interventions are the priority 8 hours after an abdominal aortic aneurysm repair?
a. Assessing nutrition status and diet preferences
b. Starting IV heparin and monitoring anticoagulation
c. Administering IV fluids and watching kidney function
d. Elevating the legs and applying compression stockings
Postoperative priorities include giving IV fluids and maintaining renal perfusion. An adequate blood pressure is important for maintaining graft patency, and administration of IV fluids and blood components (as indicated) is essential for adequate blood flow. The nurse should evaluate renal function by measuring hourly urine output and monitoring daily blood urea nitrogen (BUN) and serum creatinine levels. Irreversible renal failure may occur after aortic surgery, particularly in patients at high risk.
7. Which goal is the first priority of interprofessional care for a patient with a suspected acute aortic dissection?
a. Reduce anxiety
b. Monitor chest pain
c. Control blood pressure
d. Increase myocardial contractility
The initial goals of therapy for acute aortic dissection without complications are blood pressure (BP) control and pain management. BP control reduces stress on the aortic wall by reducing systolic BP and myocardial contractility.
8. Which patient is at highest risk for venous thromboembolism (VTE)?
a. a. A 62-year-old man with spider veins who is having arthroscopic knee surgery
b. b. A 32-year-old woman who smokes, takes oral contraceptives, and is planning a long flight
c. A 26-year-old woman who is 3 days postpartum and received maintenance IV fluids for 12 hours during her labor
d. d. An active 72-year-old man at home recovering from transurethral resection of the prostate for benign prostatic hyperplasia
Three key factors (called Virchow’s triad) that cause venous thrombosis are (1) venous stasis, (2) damage of the endothelium (inner lining of the vein), and (3) hypercoagulability of the blood. Patients at risk for venous thrombosis usually have predisposing conditions for these 3 disorders. The 32-yr-old woman has the highest risk: long trips without adequate exercise (venous stasis), tobacco use, and use of oral contraceptives.
9. Which clinical findings would the nurse expect in a person with an acute lower extremity VTE? (select all that apply)
a. Pallor and coolness of foot and calf
b. Mild to moderate calf pain and tenderness
c. Grossly decreased or absent pedal pulses
d. Unilateral edema and induration of the thigh
e. Palpable cord along a superficial varicose vein
The patient with lower extremity venous thromboembolism (VTE) may or may not have unilateral leg edema, extremity pain, a sense of fullness in the thigh or calf, paresthesia, warm skin, erythema, or a systemic temperature greater than 100.4 F (38 C). If the calf is involved, it may be tender to palpation.
10. Which treatment would the nurse anticipate for an otherwise healthy person with an initial VTE?
a. IV argatroban as an inpatient
b. IV unfractionated heparin as an inpatient
c. Subcutaneous unfractionated heparin as an outpatient
d. Subcutaneous low-molecular-weight heparin as an outpatient
Patients with confirmed VTE should receive initial treatment with low-molecular weight heparin (LMWH), unfractionated heparin (UH), fondaparinux, or rivaroxaban, followed by warfarin for 3 months to maintain the international normalized ratio (INR) between 2.0 and 3.0 for 24 hours. Patients with multiple comorbid conditions, complex medical issues, or a very large VTE usually are hospitalized for treatment and typically receive intravenous UH. LMWH for 3 months is another option for patients with acute VTE. Depending on the presentation, patients often can be managed safely and effectively as outpatients.
11. Which instruction is a key aspect of teaching for the patient on anticoagulant therapy?
a. Monitor for and report any signs of bleeding.
b. Do not take acetaminophen (Tylenol) for a headache.
c. Decrease your dietary intake of foods containing vitamin K.
d. Arrange to have blood drawn twice a week to check drug effects.
Teach patients taking anticoagulants to monitor and report any signs of bleeding, which can be a serious complication. Other important patient teaching includes maintaining a consistent intake of foods containing vitamin K and avoiding supplements that contain vitamin K. If a patient is taking warfarin, routine coagulation laboratory studies are needed. The frequency is patient dependent, not necessarily twice a week.
12. The nurse is planning care and teaching for a patient with venous leg ulcers. Which patient action is the most important in healing and control of this condition?
a. Following activity guidelines.
b. Using moist environment dressings.
c. Taking horse chestnut seed extract daily.
d. Applying graduated compression stockings.
Compression is essential for treating chronic venous insufficiency (CVI), healing venous ulcers, and preventing ulcer recurrence. Use of custom-fitted graduated compression stockings is an option for compression therapy.
A postoperative patient asks the nurse why the provider ordered daily administration of enoxaparin (Lovenox). Which reply would the nurse provide?
“This medication will help prevent breathing problems after surgery, such as pneumonia.”
“This medication will help lower your blood pressure to a safer level, which is very important after surgery.”
“This medication will help prevent blood clots from forming in your legs until your level of activity returns to normal.”
“This medication is a narcotic pain medication that will take away muscle aches caused by positioning during surgery.”
Enoxaparin is an anticoagulant that is used to prevent DVTs postoperatively.
The nurse is caring for a postoperative patient who had been receiving warfarin and diltiazem before surgery as treatment for atrial fibrillation. If the warfarin was discontinued the week before surgery, for which complication would the nurse monitor?
Decreased cardiac output
Increased blood pressure
Cerebral or pulmonary emboli
Excessive bleeding from incision
Warfarin is an anticoagulant that is used to prevent thrombi from forming on the walls of the atria during atrial fibrillation. When the medication is terminated, thrombi could again form. If one or more thrombi detach from the atrial wall, they could travel as cerebral emboli from the left atrium or pulmonary emboli from the right atrium.
The nurse is reviewing the laboratory test results for a patient whose warfarin therapy was stopped before surgery. On postoperative day 2, the international normalized ratio (INR) result is 2.2. Which action would the nurse take?
Hold the daily dose of warfarin.
Give the prescribed dose of warfarin.
Call the health care provider to request discontinuing the warfarin.
Call the health care provider to request an increased dose of warfarin.
The therapeutic range for INR is 2.0 to 3.0 for many clinical diagnoses. To maintain therapeutic values, the nurse will administer the medication as ordered. Holding the medication would lower the INR, which would increase the risk of clot formation. Conversely, the higher the INR is, the more prolonged the clotting time. Calling the health care provider is not indicated.
Which new assessment finding would alert the nurse that a postoperative patient is not receiving the beneficial effects of enoxaparin (Lovenox)?
Crackles bilaterally in the lung bases
Pain and swelling in a lower extremity
Inability to initiate urination since surgery
Abdominal pain with decreased bowel sound
Enoxaparin is a low-molecular-weight heparin used to prevent the development of deep vein thromboses (DVTs) in the postoperative period. Pain and swelling in a lower extremity can indicate development of DVT and therefore may signal ineffective medication therapy.
The nurse is caring for a preoperative patient who has an order for vitamin K by subcutaneous injection. Which laboratory result would the nurse expect to be abnormal before administering the dose?
Hematocrit (Hct)
Hemoglobin (Hgb)
Prothrombin time (PT)
Activated partial thromboplastin time (aPTT)
Vitamin K counteracts hypoprothrombinemia and/or reverses the effects of warfarin and thus decreases the risk of bleeding. High values for either the PT or the international normalized ratio demonstrate the need for this medication.
The nurse is preparing to administer a scheduled dose of enoxaparin (Lovenox) 30 mg subcutaneously. Which action would the nurse take to administer this medication correctly?
Rub the injection site to enhance absorption.
Bunch up the skin before inserting the needle.
Remove the air bubble in the prefilled syringe.
Aspirate before injection to prevent IV administration.
The nurse should gather together or “bunch up” the skin between the thumb and the forefinger before inserting the needle into the subcutaneous tissue. The nurse should not remove the air bubble in the prefilled syringe, aspirate, nor rub the site after injection.
Which medications prescribed for patients with PAD would the nurse identify as being intended to decrease the risk of cardiovascular events ? (Select all that apply.)
Ramipril (Altace)
Cilostazol (Pletal)
Simvastatin (Zocor)
Clopidogrel (Plavix)
Warfarin (Coumadin)
Aspirin (acetylsalicylic acid)
Angiotensin-converting enzyme inhibitors (e.g., ramipril [Altace]) are used to control hypertension. Statins (e.g., simvastatin [Zocor]) are used for lipid management. Aspirin is used as an antiplatelet agent. Clopidogrel may be used if the patient cannot tolerate aspirin. Cilostazol (Pletal) is used for intermittent claudication, but it does not reduce CVD morbidity and mortality risks. Anticoagulants (e.g., warfarin [Coumadin]) are not recommended to prevent cardiovascular disease events in PAD patients.
A patient was admitted for possible ruptured aortic aneurysm. Ten minutes later, the nurse notes sinus tachycardia 138 beats/min, blood pressure is palpable at 65 mm Hg, increasing waist circumference, and no urine output. How would the nurse interpret the findings?
The renal arteries are involved.
Perfusion to the legs is interrupted
Tamponade will soon stop the bleeding.
Bleeding into the abdomen is continuing.
The patient is likely bleeding into the abdominal space, and it is likely to continue without surgical repair. A tamponade blockade of the blood flow will not occur in the abdominal space as it would in the retroperitoneal space, where surrounding anatomic structures may control the bleeding. The lack of urine output does not indicate renal artery involvement but that the bleeding is occurring above the renal arteries, which decreases the blood flow to the kidneys. There is likely to be decreased rather than interrupted perfusion to the legs.
An older adult with dementia has a venous ulcer related to chronic venous insufficiency. Which type of diet would the nurse explain to the patient and caregiver?
Low-fat diet
High-protein diet
Calorie-restricted diet
High-carbohydrate diet
A patient with a venous ulcer should have a balanced diet with adequate protein, calories, and micronutrients; this type of diet is essential for healing. Nutrients most important for healing include protein, vitamins A and C, and zinc. Foods high in protein (e.g., meat, beans, cheese, tofu), vitamin A (green leafy vegetables), vitamin C (citrus fruits, tomatoes, cantaloupe), and zinc (meat, seafood) must be provided. Restricting fat or calories is not helpful for wound healing or in patients of normal weight. For overweight individuals with no active venous ulcer, a weight-loss diet should be considered.
The nurse is caring for a patient with a recent history of deep vein thrombosis (DVT) who is scheduled for an emergency appendectomy. The patient’s international normalized ratio (INR) value is 1.0. Vitamin K is prescribed for immediate administration. Which nursing action is most appropriate?
Administer the medication as ordered.
Hold the medication and notify the surgical staff.
Hold the medication until the lab result is repeated to verify results.
Administer the medication and request an increased dose from the surgeon
Vitamin K is the antidote to warfarin, which the patient has likely been taking before admission for treatment of DVT. Warfarin is an anticoagulant that impairs the ability of the blood to clot. Therefore, it may be necessary to give vitamin K before surgery to reduce the risk of hemorrhage. However, the INR value is normal, and vitamin K is not required, so the medication would be held, and the surgical staff notified that it was not given.
The nurse is caring for a patient with vascular insufficiency who is prescribed enoxaparin (Lovenox) 30 mg subcutaneously. Which action would the nurse take to correctly administer this medication?
Spread the skin before inserting the needle.
Leave the air bubble in the prefilled syringe.
Use the back of the arm as the preferred site.
Place the patient in prone position before the injection.
The nurse would not expel the air bubble from the prefilled syringe because it should be injected to clear the needle of medication and avoid leaving medication in the needle track in the tissue.
A patient was just diagnosed with acute arterial ischemia in the left leg secondary to atrial fibrillation. Which early clinical manifestation must be reported to the provider promptly?
Paralysis
Cramping
Paresthesia
Referred pain
The provider must be notified immediately if any of the six Ps of acute arterial ischemia occur to prevent ischemia from quickly progressing to tissue necrosis and gangrene. The six Ps are paresthesia, pain, pallor, pulselessness, and poikilothermia, with paralysis being a very late sign indicating the death of nerves to the extremity. Crampy leg sensation is more common with varicose veins. The pain is not referred.
A patient with critical limb ischemia had peripheral artery bypass surgery to improve circulation. Which intervention would the nurse plan on the first postoperative day?
Keep the patient on bed rest.
Assist the patient to walk several times.
Have patient sit in the chair for 2 hours after meals.
Position the patient on their side with knees flexed.
To avoid blockage of the graft or stent, the patient should walk several times on postoperative day one and subsequent days. Having the patient’s knees flexed for sitting in a chair or in bed increase the risk of venous thrombosis and may place stress on the suture lines.
Which assessment findings of the left leg would the nurse identify as consistent with arterial occlusion? (Select all that apply.)
Edematous
Cold and mottled
Reports of paresthesia
Pulse not palpable with Doppler
Warmer than right lower extremity
Capillary refill less than 3 seconds
Arterial occlusion may result in loss of limb if not timely revascularized. When an artery is occluded, perfusion to the extremity is impaired or absent. On assessment, the nurse would note a cold, mottled extremity with impaired sensation or numbness. The pulse would not be identified, even with a Doppler. In contrast, the nurse would find edema, erythema, and increased warmth in the presence of a venous occlusion (deep vein thrombosis). Capillary refill would be greater than 3 seconds in an arterial occlusion and less than 3 seconds with a venous occlusion.
A patient is prescribed diltiazem for Raynaud’s phenomenon. Which assessment finding would indicate to the nurse that the medication is effective?
Resilient skin turgor
Decreased heart rate
Prompt capillary refill
Decreased mean arterial pressure
Raynaud’s phenomenon is an episodic vasospastic disorder of small cutaneous arteries, most frequently involving the fingers and toes. Diltiazem is a calcium channel blocker that relaxes smooth muscles of the arterioles by blocking the influx of calcium into the cells, thus reducing the frequency and severity of vasospastic attacks. Perfusion to the fingertips is improved, and vasospastic attacks are reduced. Diltiazem may decrease heart rate and blood pressure, but that is not the purpose in Raynaud’s phenomenon. Skin turgor is most often a reflection of hydration status.
Which intervention is a nursing priority for the care of a patient with chronic venous insufficiency (CVI)?
Applying topical antibiotics to venous ulcers
Positioning the patient’s legs below heart level
Administering oral or subcutaneous anticoagulants
Teaching the patient how to use compression stockings
CVI requires conscientious and consistent application of compression stockings. Anticoagulants are not necessarily indicated and antibiotics, if required, are typically oral or IV, not topical. The patient should avoid prolonged positioning with the limb in a dependent position.
A patient with peripheral artery disease is seen in the primary care clinic. Which symptom reported by the patient would indicate to the nurse that the patient is experiencing intermittent claudication?
Patient reports chest pain with strenuous activity.
Patient says leg muscle pain occurs with continued exercise.
Patient has numbness and tingling of all the toes and both feet.
Patient states the feet become red when they are in a dependent position.
Intermittent claudication is an ischemic muscle ache or pain that is precipitated by a consistent level of exercise, resolves within 10 minutes or less with rest, and is reproducible. Angina is the term used to describe chest pain with exertion. Paresthesia is the term used to describe numbness or tingling in the toes or feet. Reactive hyperemia is the term used to describe redness of the foot; if the limb is in a dependent position, the term is dependent rubor.
A nurse is caring for a patient with a diagnosis of deep venous thrombosis (DVT). The patient has 30 mg enoxaparin (Lovenox) prescribed. Which injection site would the nurse use to administer this medication?
Buttock, upper outer quadrant
Abdomen, anterior-lateral aspect
Back of the arm, 2 in away from a mole
Anterolateral thigh, with no scar tissue nearby
Enoxaparin (Lovenox) is a low-molecular-weight (LMW) heparin that is given as a deep subcutaneous injection in the right and left anterolateral abdomen. All subcutaneous injections should be given away from scars, lesions, or moles.
The nurse observes that phlebitis has developed at a patient’s peripheral IV site. Which intervention would the nurse implement first?
Remove the patient’s IV catheter.
Decrease the IV rate to 30 mL/hr.
Apply an ice pack to the affected area.
Administer prophylactic anticoagulants.
The priority intervention for superficial phlebitis is removal of the offending IV catheter. Decreasing the IV rate is insufficient. Anticoagulants are not normally required. Warm, moist heat is often therapeutic after catheter removal.
A middle-aged patient with diabetes has been diagnosed with peripheral artery disease (PAD). The patient smokes and has a history of gout. Which topic is the priority in patient teaching?
Smoking cessation
Appropriate vaccinations
Managing hypoglycemia
Drug therapy for gout flares
The first treatment goal for patients with PAD is to reduce CVD risk factors. Smoking is a significant PAD risk factor for this patient, and is modifiable with behavior change. Tobacco cessation is essential to reduce PAD progression, CVD events, and mortality. While diabetes and gout are risk factors, these topics are not related to hyperglycemia and hyperuricemia.
The assistive personnel (AP) suggests applying compression stockings to a patient with peripheral vascular disease. Which assessment finding would indicate that applying compression stockings could harm the patient?
Leg pain at rest
High blood pressure
Dry, itchy, flaky skin
Elevated blood glucose
Rest pain occurs as peripheral artery disease (PAD) progresses and involves multiple arterial segments. Compression stockings should not be used on patients with PAD. Elevated blood glucose, possibly indicating uncontrolled diabetes, and hypertension may or may not indicate arterial problems. Dry, itchy, flaky skin indicates venous insufficiency. The RN should be the one to obtain the order and instruct the AP to apply compression stockings if they are ordered.
A middle-aged woman with a history of smoking and oral contraceptive use is admitted with a venous thromboembolism (VTE) and prescribed unfractionated heparin. Which laboratory test would the nurse review to evaluate the effect of the heparin?
Platelet count
Activated clotting time (ACT)
International normalized ratio (INR)
Activated partial thromboplastin time (aPTT)
Unfractionated heparin can be given by continuous IV for VTE treatment. When given IV, heparin requires frequent laboratory monitoring of clotting status as measured by activated partial thromboplastin time (aPTT). Platelet counts can decrease as an adverse reaction to heparin.
The patient reports tenderness over a leg vein. The nurse assesses warmth and a palpable cord in the area. Which complication would the nurse plan to prevent?
Pulmonary embolism
Pulmonary hypertension
Postthrombotic syndrome
Venous thromboembolism
The manifestations are characteristic of a superficial vein thrombosis. If untreated, the clot may extend to deeper veins, and venous thromboembolism may occur. Pulmonary embolism, pulmonary hypertension, and postthrombotic syndrome are the sequelae of venous thromboembolism.
When the patient is being examined for venous thromboembolism (VTE) in the calf, which diagnostic test would the nurse expect to explain to the patient first?
Duplex ultrasound
Contrast venography
Magnetic resonance venography
Computed tomography venography
The duplex ultrasound is the most widely used test to diagnose VTE. Contrast venography is rarely used now. Magnetic resonance venography is less accurate for calf veins than pelvic and proximal veins. Computed tomography venography may be used but is invasive and much more expensive than the duplex ultrasound.
A patient with varicose veins has been prescribed compression stockings. Which instruction would the nurse give?
“Try to keep your stockings on 24 hours a day, as much as possible.”
“While you’re still lying in bed in the morning, put on your stockings.”
“Dangle your feet at your bedside for 5 minutes before applying your stockings.”
“The stockings are most effective if you remove and reapply them several times a day.”
The patient with varicose veins should apply stockings in bed before rising in the morning. Stockings should not be worn continuously and should not be removed several times daily. Dangling at the bedside before application is likely to decrease their effectiveness.
Which person would the nurse identify as having the highest risk for abdominal aortic aneurysm?
A 70-yr-old man with high cholesterol and hypertension
A 40-yr-old woman with obesity and metabolic syndrome
A 60-yr-old man with renal insufficiency who is physically inactive
A 65-yr-old woman with high homocysteine levels and substance use
The most common cause of descending abdominal aortic aneurysm (AAA) is atherosclerosis. Male gender, age 65 years or older, and tobacco use are the major risk factors for AAAs of atherosclerotic origin. Other risk factors include the presence of coronary or peripheral artery disease, high blood pressure, and high cholesterol.
The nurse is admitting a patient who has a suspected leaking abdominal aortic aneurysm (AAA). The medication history reveals that the patient has been taking warfarin daily. Which medication would the nurse be prepared to give?
Vitamin K
Cobalamin
Heparin sodium
Protamine sulfate
A patient with a leaking aneurysm may go to surgery for repair. Warfarin is a vitamin K antagonist anticoagulant that could cause excessive bleeding during surgery if clotting times are not corrected. Vitamin K is given as the antidote for warfarin.
Which priority intervention will help maintain graft patency for a patient who had aortic aneurysm repair 6 hours ago?
Assess urine output for renal dysfunction.
Give IV fluids to maintain adequate perfusion.
Administer diuretics to improve renal blood flow.
Maintain a low BP to prevent pressure on surgical site.
The priority is to maintain an adequate blood pressure (BP) (determined by the surgeon) to maintain graft patency. A prolonged low BP may result in graft thrombosis, and hypertension may cause undue stress on arterial anastomoses resulting in leakage of blood or rupture at the suture lines, which is when IV antihypertensives may be used. Renal output will be assessed when the aneurysm repair is above the renal arteries to assess graft patency, not maintain it.