Contraception: Study guide
Core Goals and Epidemiology of Contraception
Epidemiology:
of pregnancies are unintended; the highest rates occur in individuals aged years.
of unintended pregnancies occur in couples who were reportedly using contraception.
Teen pregnancy rates have declined by since the high in .
Typical contraceptive age range: years (menarche to menopause).
Primary Goals:
Prevent unintended pregnancy.
Improve pregnancy outcomes (birth spacing, family planning).
Non-Contraceptive Benefits:
Regularity of menstrual cycles (hormonal only).
Management of perimenopause symptoms.
Improvement in iron deficiency anemia and relief from menstruation-related problems.
Prevention of ovarian and endometrial cancer.
Reduced incidences of ectopic pregnancy, ovarian cysts, Pelvic Inflammatory Disease (PID), endometriosis, and uterine fibroids.
Provider Requirements: A physical exam or Pap smear is not strictly required to prescribe, but blood pressure (BP) must be checked.
Categorization of Contraceptive Methods and Efficacy
Long-Acting Reversible Contraception (LARC): Most effective methods; include IUDs and implants (easiest adherence: "set it and forget it").
Typical Use Efficacy (1-Year Pregnancy Rates):
>99\% effective: ***Copper IUD, ***Levonorgestrel IUD, ****Progestin-only implant.
effective: ****Depot medroxyprogesterone acetate injection.
effective: ***Combined Hormonal Contraceptives (CHC) including vaginal rings,*** transdermal patches, and ***oral pills.
effective: ***Progestin-only oral contraceptives (POPs).
Note: All products have a <1\% pregnancy rate with ideal (perfect) use.
Non-Pharmacologic / On-Demand Methods (Typical Use Efficacy):
Protective for STI/STDs:**** External male condoms (), ***Internal female condoms ().
Use water based lube and not oil based lube when using latex condoms to prevent degradation of the material, ensuring maximum efficacy and preventing breakage.
Some STI/STD Protection: ***Diaphragm with spermicide (), ***Cervical cap with spermicide (). These have to be fitted therefore they are prescription only.
Not Protective for STI/STDs:*** Fertility awareness methods (), *** Natural membrane condoms (), ***pH regulating gel (), this is prescription only PHEX.
May Increase STI Risk: ***Spermicides () these are good when combined with other contraceptives, *****Contraceptive sponge ( if nulliparous; if parous) goal is to absorb all sperm.
Know the patient is not pregnant before administering a contraceptive.
Two Types of Hormonal Contraceptive
PROGESTIN: Main contraceptive hormone
Reduces likelihood of ovulation (Block LH surge)
Reduces likelihood of fertilization by thickening cervical mucus, making it more difficult for sperm to reach the egg.
Reduces likelihood of implantation by altering the endometrial lining, making it less suitable for a fertilized egg to attach. Lighter bleeding patterns during cycle
ESTROGEN:
Helps prevent contraception by suppressing FSH
Provide cycle control (know when the cycle is going to happen) by regulating menstrual periods and reducing symptoms associated with premenstrual syndrome (PMS).
ADE ON ESTROGEN :
Blood clotting
Cervical Cancer
PILL, PATCHES, RINGS
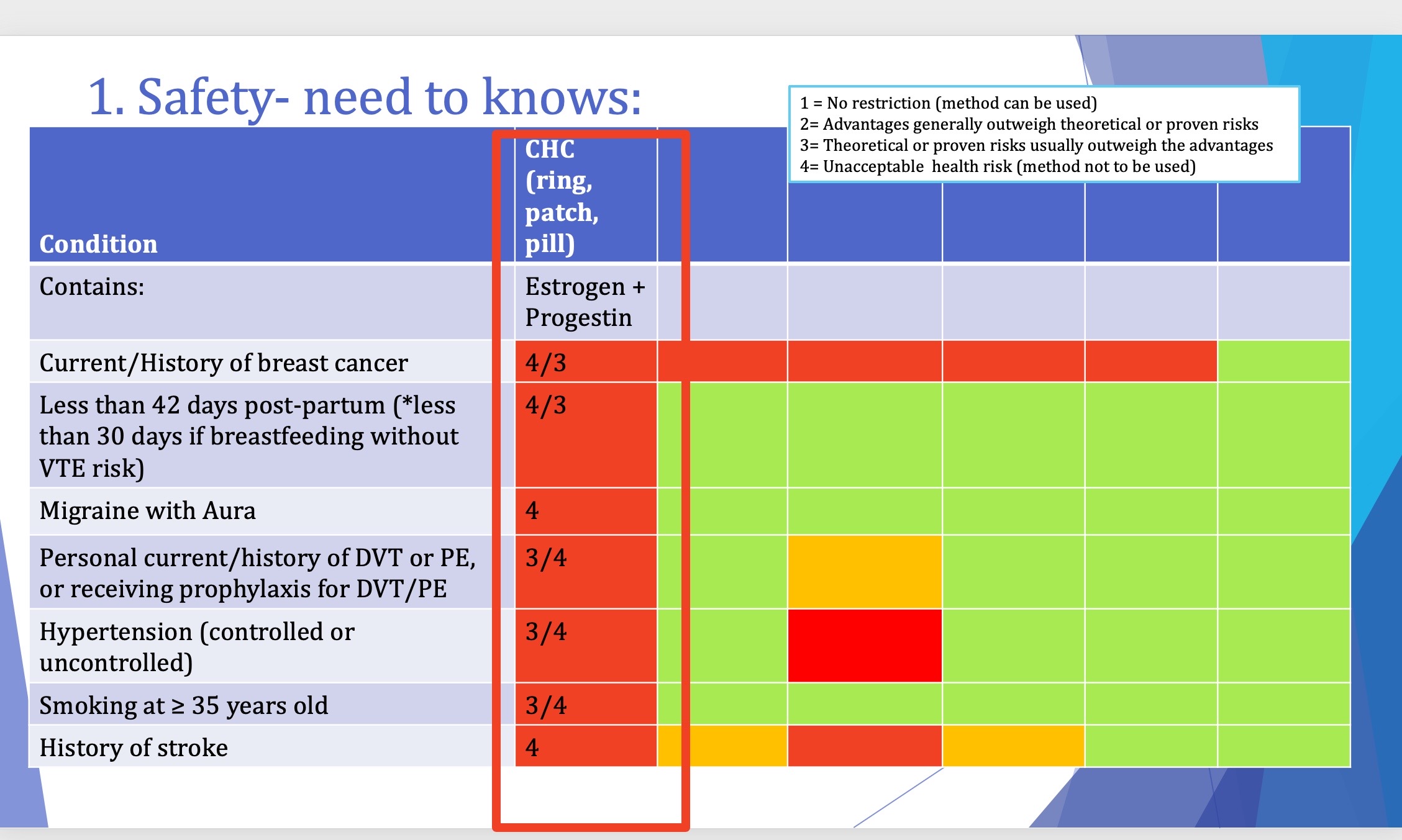
Hypertension: Category 3/43/4 (Contraindicated if BP≱160/100 mmHgBP≱160/100mmHg).
Oral Contraceptive:
ROA : oral
Duration of contraception: 1 day (TAKE EVRY 24 HOURS)
Return to fertility (IMMEDIATE)
Easiest to access and less expensive
Ability adherence
Cycle control
ETHINYL ESTRADIOL (EE)
A commonly used synthetic form of estrogen in combined oral contraceptives that enhances the effectiveness of contraception by providing reliable cycle control and reducing hormonal fluctuations.
Very low dose (10-20)
Low dose ideal (20-29)
Moderate dose for pt who is non adherent (30-49)
Do not prescribe high dose (50 or higher)
Generation | Name | Androgen Activity | Notes |
|---|---|---|---|
1st | Norethindrone | Ethynodiol diacetate | Well tolerated, spotting may be a problem |
2nd | Norgestrel | Levonorgestrel | Most high androgenic activity = anti-estrogenic activity = least VTE risk. Androgenic activity can improve libido, worsen acne, worsen dyslipidemia, and cause hirsutism. |
3rd | Norgestimate | Desogestrel, Norelgestromin, Etonogestrel | Less androgenic activity; beneficial in patients with acne but increased VTE risk compared to 2nd gen. |
4th | Drospirenone | Dienogest | Anti-androgenic; highest VTE risk. Good for acne, dyslipidemia, and hirsutism. Monitor potassium levels because the use of Drospirenone can lead to hyperkalemia, particularly in patients with renal impairment or those taking other potassium-sparing medications. |
Combined Hormonal Contraceptive (CHC) : pt usually does not see a period of if they do it is thinner
Estrogen + Progestin
Combined oral contraceptive pill
intravaginal ring
transdermal patch
Intrauterine device (IUD) - A form of long-acting reversible contraception that can be hormonal or non-hormonal.
Injectable contraceptives - Typically given every three months, providing an alternative to daily pills.
Progestin only : A hormonal method that contains only progestin, effectively preventing ovulation and thickening cervical mucus. Pt still sees a period every month
Safety
Patient specific factors (preference)
Efficacy may vary based on individual patient factors such as age, weight, smoking status, and underlying health conditions, thus necessitating a thorough evaluation before prescribing.
SAFTEY NEED TO KNOW
Known Drugs Affecting Efficacy:
Rifampin, Rifabutin (Category 3): Use backup during and at least 77 days after (some suggest 28days).
Anticonvulsants: phenobarbital, carbamazepine, phenytoin, lamotrigine, topiramate, oxcarbazepine (Category 3): Switch to DMPA, IUD, or implant.
Drospirenone = hyperkalemia: Caution with other hyperkalemia inducing drugs;
HIV medications (protease inhibitors): may decrease effectiveness. Watch for fosamprenavir (Category 3); all others are (Category 1 or 2) but may need moderate dose (35 mcg) of EE to compensate (atazanavir); may increase risk of ADE (acne, hyperkalemia, VTE/dyslipidemia).
St. John’s Wort: may decrease effectiveness (Category 2).
POPs have concern for interaction; DMPA, IUD, and Implant are generally okay.
Case reports: Tetracyclines, penicillin derivatives (not shown in studies) but MEC states they may be given (Category 1).
Monophasic vs. Multiphasic:
Considered equal in efficacy and safety.
Monophasic preferred when first initiating:
Easiest to dose adjust therapy.
Multiphasic aimed to mimic natural physiologic hormone cycling:
Enables lower doses earlier in cycle, possibly resulting in fewer adverse drug events (ADE).
Typical regimen: 21 active pills followed by 7 placebo "reminder" pills.
28-Day, Extended-Cycle, and Continuous Contraceptive Options:
28-Day Regimen: Standard cycle with 21 active pills followed by 7 placebo pills.
Extended-Cycle Regimen:
Reduces hormone fluctuations by extending the active pill phase.
Typically designed for 3 extra days, resulting in fewer menstrual cycles (approximately every 3 months).
Helpful for severe PMS or for convenience.
Continuous Regimen:
Eliminates the placebo week altogether, allowing for continuous hormone delivery.
A regular pack can be turned into a continuous regimen by skipping the placebo week and beginning a new pack immediately.
Providing iron (Fe) tablets instead of placebo pills can be beneficial for patients with iron deficiency anemia, ensuring adequate iron intake while on hormonal contraceptives.
Initiation Methods:
Day 1 Start: No backup needed.
Sunday/Quick Start: Use backup for .
Starting: “DAY 1 START” refers to taking it on the first day of your period therefore no backup needed
if you start on any other day use back up for 7 days such as condoms
Lighter predictable monthly
SEVER ACHES: Abdominal pain, Chest pain, Headache, Eye problems, Severe leg pain
ACHES Checklist (Discontinue immediately if):
: Abdominal pain (severe).
: Chest pain.
: Headaches (severe sudden).
: Eye problems (blurred vision).
: Severe leg pain (DVT symptom).
Dose Adjustment/Managing of ADE
Wait 2-3 months!
Managing breakthrough bleeding:
Early in the cycle (Days 1-9): Follicular phase; estrogen too low.
Later in the cycle (Days 10-21): Luteal phase; progestin too low.
Symptoms and their indications:
Nausea, headaches, or breast tenderness: Indicate too much estrogen.
Skin breakouts: Indicate too much androgen.
Adherence and Missed Doses:
Missed 1 pill: Take ASAP (even if it means 2 at once). No backup needed.
Missed 2+ consecutive pills: Take last missed pill and discard extras. Use backup for .
Missed during Week 3: Skip placebo week; start new pack immediately; backup for .
If two or more doses are missed start a new pack
The Patch
Apply patch weekly on the same day of the week for 3 weeks. Do not wear a patch for the 4th week.
Missed doses:
If missed <24 hours: apply new patch. This is the new “change day”.
If missed more than 24 hours: use backup for 7 days.
Contraindicated with BMI ≥ 30 kg/m² due to risk of venous thromboembolism (VTE).
The Ring
Brand Name: NuvaRing is a monthly vaginal ring. It is a form of combined hormonal contraception that releases hormones (estrogen and progestin) to prevent ovulation and regulate menstrual cycles. It is inserted into the vagina and needs to be replaced monthly for effective contraceptive use.
Insert for 3 weeks; remove for 1 week. Discard and replace monthly.
Stored in refrigerator at pharmacy. OK at room temperature for 3 months. Avoid douching; all other vaginal products are okay to use (tampons, antifungal vaginal creams, etc.)
Brand Name: Annovera is a yearly vaginal ring. Insert for 3 weeks; remove for 1 week. Clean, save, and reuse for 12 month
Mini Pill aka POP(Progesterone only pills) = No placebo has to be taken continously no period associated , No for breast cancer pt .
3 hour missed dose window ; if a dose is missed by more than 3 hours, use a backup method of contraception for the next 48 hours, one exception is SLYND with 24 hour missed dose window.
Biological Mechanisms of Hormonal Contraception
Synthetic Estrogens:
Ethinyl Estradiol (EE): Most common.
Mestranol: Prodrug converted to EE (less potent).
Estradiol valerate: Plant-based.
Estetrol (E4): Fourth generation synthetic.
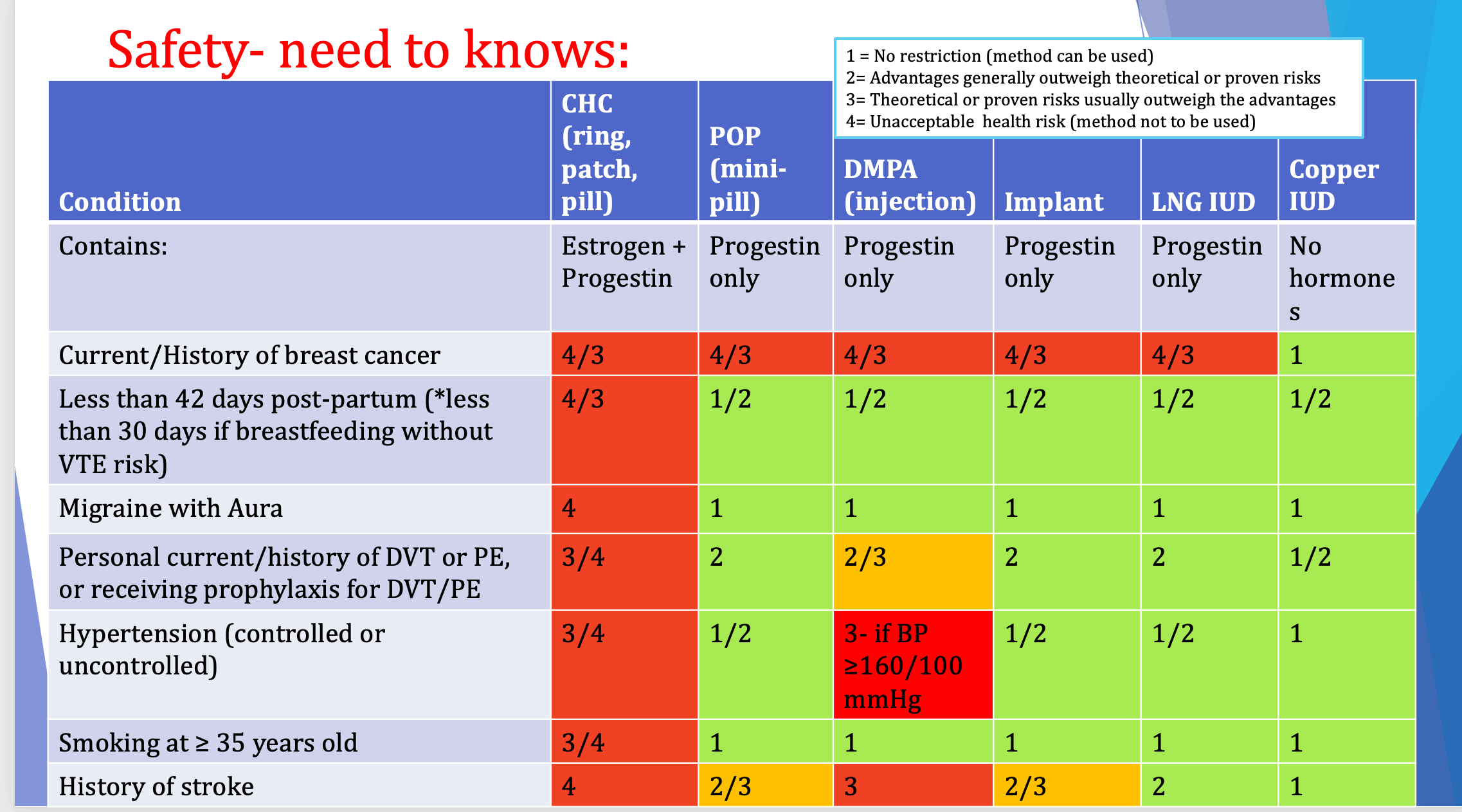
Medical Eligibility Criteria (MEC) Classifications
Category 1: No restriction; method can be used.
Category 2: Advantages generally outweigh theoretical or proven risks.
Category 3: Theoretical or proven risks usually outweigh the advantages.
Category 4: Unacceptable health risk; method NOT to be used.
Progestin-Only Methods (Long-Acting and Oral)
DMPA Injection (Depo-Provera):
Dosed every ; window before considered missed.
ADE: Weight gain (), Black Box Warning for Bone Mineral Density (BMD) loss (limit to use usually).
Slow return to fertility (up to ).
Progestin-Only Pills (POPs/Mini-pill):
Timing is critical: missed dose window is only (except Slynd, which is ).
If missed >3\text{ hours}, use backup for .
Preferred for smokers , breastfeeding, or those with estrogen contraindications.
LARCs: Most effective with typical use, Progestin only.
Copper IUD: No hormones; causes heavy bleeding/cramping; effective for . Can cause anemia and cramping. Can be used in breast cancer patients
LNG IUD (Levonorgesterone): Thins lining; effective for depending on brand.
Lighter infrequent or no periods. Predictable bleeding.
Implant:(Nexplanon) Etonogestrel; effective for ; most effective overall.
Unpredictable bleeding..
Drug Interactions
Enzyme Inducers: Rifampin, Rifabutin, Anticonvulsants (Phenobarbital, Carbamazepine, Phenytoin) decrease efficacy. Use backup or switch to DMPA/IUD/Implant.
St. John's Wort: Decreases effectiveness.
Drospirenone: Caution with potassium-sparing drugs (ACE inhibitors, ARBs, Spironolactone).
Weight Loss/Diabetes (GLP-1/GIP):
Semaglutide/Liraglutide: No significant effect.
Tirzepatide (Mounjaro): Bioavailability is reduced; use backup for at start and after each dose change.
Emergency Contraception (EC)
Levonorgestrel (Plan B):
Within (off-label up to ).
Efficacy declines with weight >165\text{ lbs} or BMI > 25\,kg/m^2.
Restart regular contraception immediately; backup for .
Ulipristal Acetate (Ella) (Prescription only): more effective than plan b
Within (efficacy does not decline with time within window).
Efficacy declines if .
Interaction: Must wait to restart hormonal contraception; backup until next menses.
Copper IUD: Most effective EC if inserted within ; not influenced by BMI.
Most effective
Medication Abortion
Indication: Up to ( ) of gestation.
Regimen:
Mifepristone orally (Blocks progesterone). Buccally 24-48 hours later (2 tabs in each cheek) First to end the pregnancy causes cramping and menstrual bleeding.
Misoprostol buccally later (Causes contractions). Second for expelling the material therefore increased bleeding.
Effectiveness: for combination; for misoprostol only.
Counseling: Expect bleeding heavier than menses; pain peaks after misoprostol; treat with NSAIDs. Contact provider if bleeding exceeds for >2\text{ hours}.
Questions & Discussion
Acne Recommendation: A patient (e.g., 14-year-old) with bad acne should consider a or generation progestin CHC (e.g., Yaz, Ortho-Tri-Cyclen) to leverage anti-androgenic effects.
Amenorrhea Preference: A 30-year-old wanting oral birth control with no periods should use a continuous regimen or skip the placebo week of a standard pack (e.g., Seasonique).
BMI and Patch: A patient with a of should NOT be given the CHC patch due to VTE risk and decreased efficacy.
Postpartum/Breastfeeding: CHCs should be avoided for at least the first postpartum due to high clotting risk and potential impact on milk supply; POPs or LARCs are safer alternatives.
History of Stroke: Patients with a history of stroke are MEC Category for CHCs; they should be recommended Copper IUD (Category 1) or POPs (Category 2/3).
- **Hypertension**: Category (Contraindicated if ).