Learning and Memory: Anatomical Perspectives
Learning and Memory: Anatomical Perspectives
Memory is complex and is related to truth.
Case Study: Oscar
Oscar, a 62-year-old man with a history of alcohol abuse, was hospitalized with dehydration and malnutrition. He exhibited forgetfulness, delusions, and hallucinations. In the ER, he was confused, disoriented, agitated, and believed he was hospitalized for an appendectomy, estimating his age as 35. A neurological exam revealed nystagmus, dysmetria on finger-to-nose testing, poor rapid alternating movements, and a mildly ataxic gait. He was alert but only oriented to person, not knowing the date or hospital name. Immediate attention was intact, recalling 3 of 3 words after 30 seconds but none after 5 minutes.
Dynamic Nature of Memory
Human memory is dynamic. Memories are not statically archived in the neocortex but are subject to constant change. Remembering is not simply reading stored data; recall is reconstruction, involving changes and distortions.
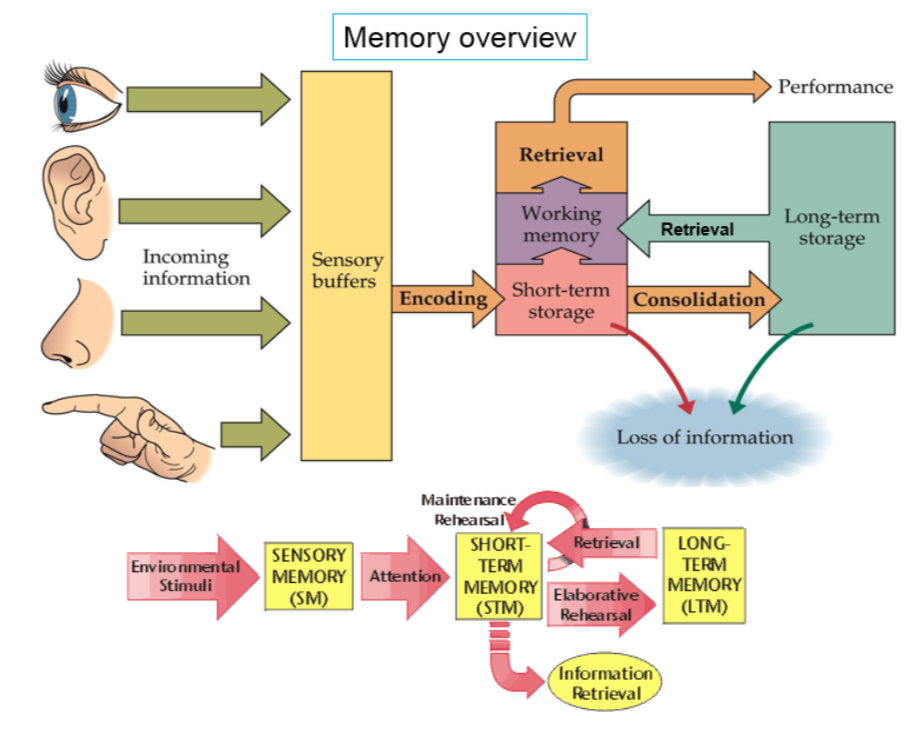
Memory Overview
Memory involves several stages:
Sensory Memory (SM): Initial processing of environmental stimuli.
Short-Term Memory (STM): Temporary storage with maintenance through rehearsal.
Long-Term Memory (LTM): Retrieval storage with consolidation.
Information flow:
Incoming information enters sensory buffers.
Attention moves information to short-term storage.
Elaborative rehearsal consolidates information into long-term storage.
Information can be lost at various stages.
Time Courses of Different Memories
Different types of memories have different time courses:
Iconic Memory: Less than a second, in each sensory buffer.
Short-Term Memory: About 30 seconds.
Intermediate-Term Memory: Not permanent, like what you ate yesterday.
Long-Term Memory: Lasts for years.
Learning vs. Memory
Learning is the process of storing new information. Memory is the stored information itself.
Amnesia
Anterograde Amnesia: Inability to form new memories after the onset of a disorder.
Retrograde Amnesia: Loss of memories formed before the onset of amnesia.
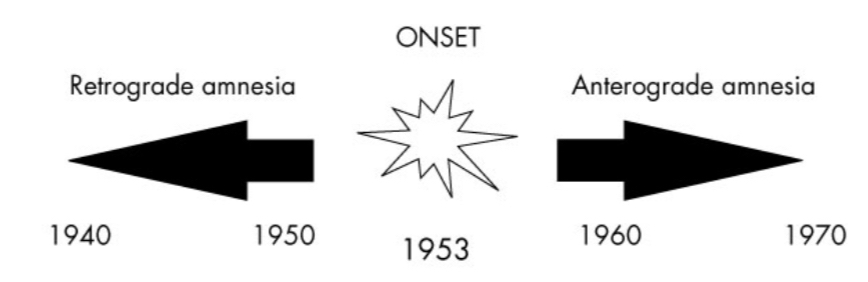
Patient H.M. (Henry Molaison)
In 1953, H.M. had surgery removing the amygdala, hippocampus, and temporal cortex on both sides.
Resulted in profound anterograde amnesia.
Short-term memory remained normal.
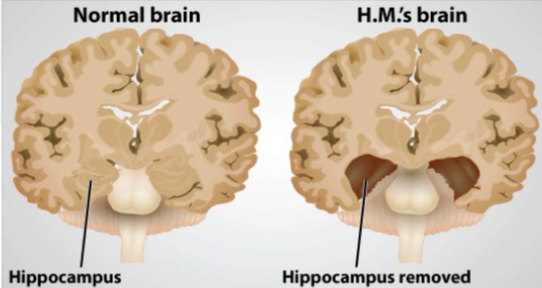
H.M.'s Memory Deficit
H.M.'s memory deficit was severe but primarily affected verbal tasks. He could still learn non-verbal tasks, such as the mirror-tracing task, demonstrating improvement over days despite no conscious recollection of doing the task before.
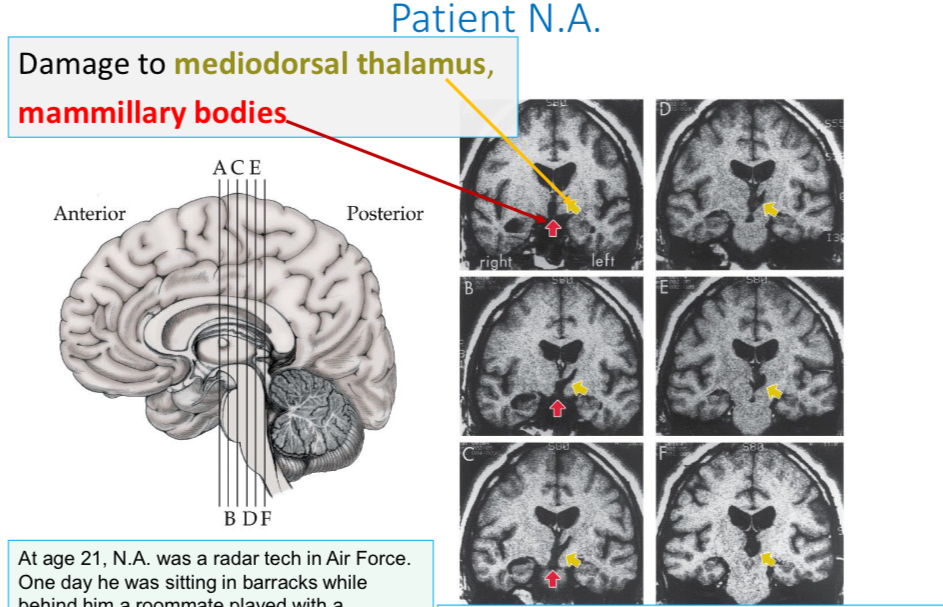
Patient N.A.
Similar to H.M., N.A. had normal short-term memory but could not form long-term declarative memories. This was due to damage to the mediodorsal thalamus and mammillary bodies.
At age 21, N.A. was stabbed through his right nostril into his brain by a miniature fencing foil.
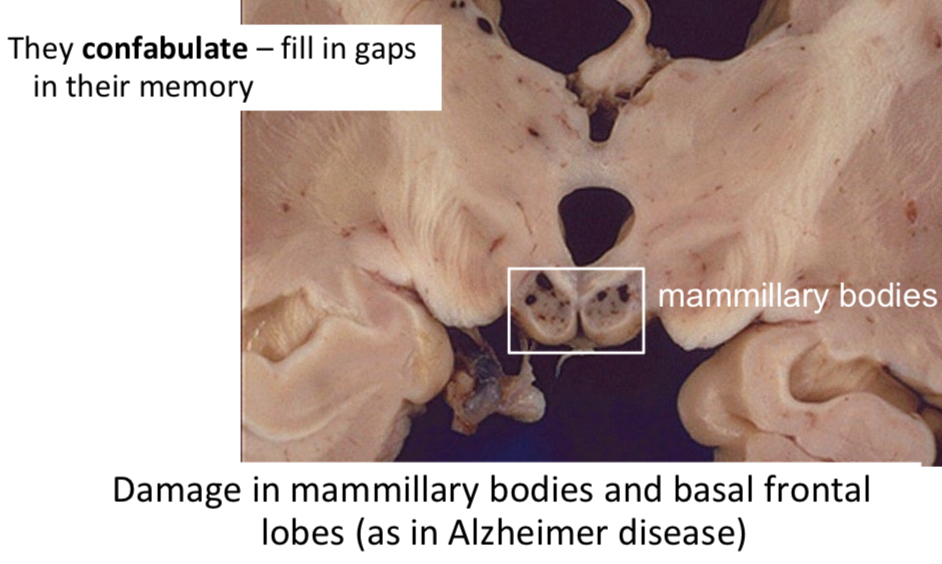
Korsakoff Syndrome
Amnesia caused by thiamine deficiency, especially in alcoholics.
Patients confabulate, filling in gaps in their memory.
Damage occurs in the mammillary bodies and basal frontal lobes, similar to Alzheimer's disease.
Patient K.C.
At age 30, K.C. had a motorcycle accident, resulting in a coma and dilated fixed pupils.
K.C.'s Bilateral Hippocampal Injury
K.C. suffered bilateral hippocampal damage.
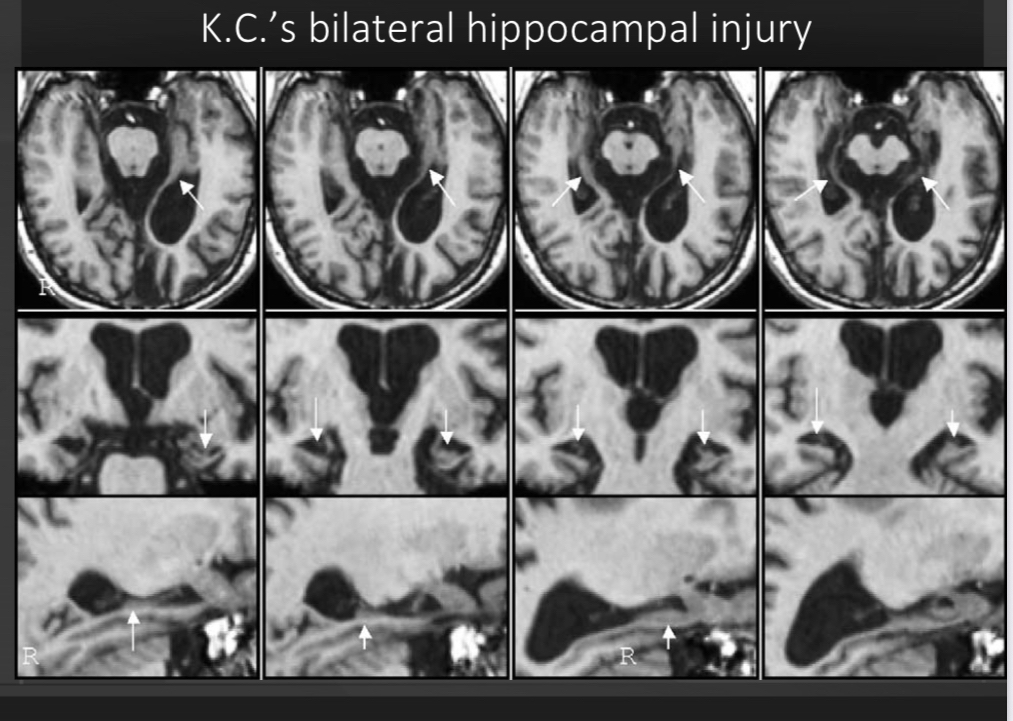
K.C.'s Memory
Semantic knowledge was spared; he could acquire new semantic memories, describing layouts without recalling specific events. Episodic memory was gone; no personal details could be recalled.
Emotion and Memory
Emotional events are remembered better. Emotional arousal, rather than the importance of information, promotes memory.
Storing emotional memories involves:
Initial Experience: A strongly arousing experience.
Memory Storage: Stored in a network with separate nodes for emotions, sounds, smells, colors, tactile, and other sensations.
Recall: Posttraumatic Stress Disorder (PTSD)
Ecstasy is now approved for PTSD treatment, increasing serotonin and oxytocin while inhibiting the amygdala. Psilocybin is also being considered.
Unwanted recall of fearful stimuli creates a feed-forward loop.
Each recall reinforces the memory.
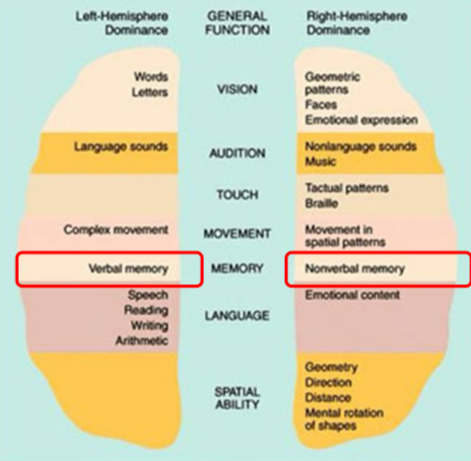
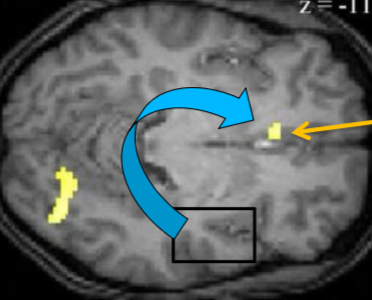
Brain Regions That Encode Memories
Recalling Pictures: Right prefrontal cortex and left and right parahippocampal cortex are activated.
Recalling Words: Same structures on the left side are activated.
Words and pictures are linked in our brain.
Hippocampus and Memory Consolidation
The hippocampus is not the location of long-term memory but is involved in memory consolidation.
Consolidation takes time and is vulnerable to change.
Most memories are stored in the cortex.
Sleep after learning enhances memory processing in the hippocampus and induces information transfer between the hippocampus and medial prefrontal cortex (mPFC).
This transfer consolidates memories, making them stable.
fMRI shows that correct word recall activates the mPFC and occipital cortex, but not the hippocampus, months after learning.
Eye-Witness Testimony
Memory is changed upon recall/restorage. Elizabeth Loftus demonstrated this with an experiment about car accidents:
Participants estimated higher speeds when the word "smashed" was used compared to "hit."
More people remembered seeing broken glass when "smashed" was used.
The more often a false memory is recalled, the more certain people are of it.
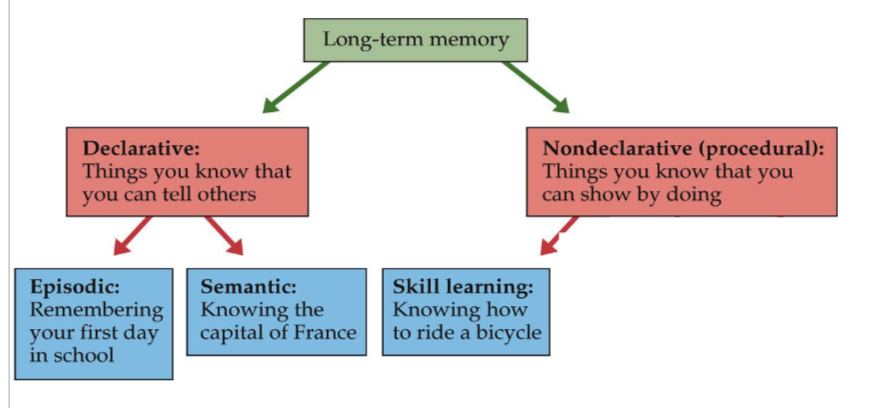
Episodic Memory Systems
Encoding Episodic Memories: Anterior medial temporal system.
Retrieving Episodic Memories: Posterior medial temporal system.
Nondeclarative Memory
Skill learning includes:
Sensorimotor skills, like mirror-tracing.
Perceptual skills, like reading mirror-reversed text.
Cognitive skills, like planning and problem-solving.
These skills are impaired in patients with basal ganglia injury.
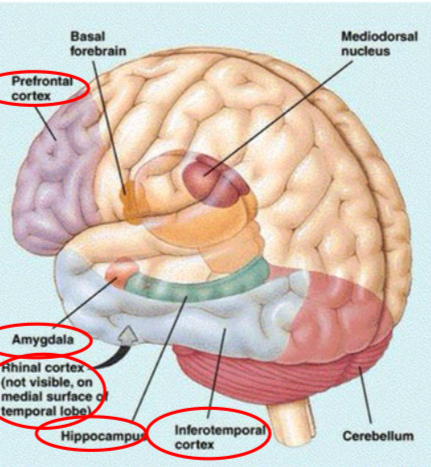
Summary: Areas Involved in Learning & Memory
Hippocampus: New declarative memories; temporal/spatial memory.
Amygdala: Memories involving emotions.
Inferotemporal Cortex: Visual images.
Prefrontal Cortex: Source memory; remembering HOW you learned something.
Basal Ganglia and Cerebellum: Nondeclarative (skill learning) for sensorimotor and motor patterns.
Mediodorsal Nucleus (Thalamus): Connects to the prefrontal lobe, integrating and sorting memories.
Memory Decline with Age
Older people show impaired internally generated memory but respond well to external cues. Autobiographical and semantic memories remain stable, but executive function and navigation skills decline.
Case Study: 73-Year-Old Woman
A 73-year-old woman with a 3-year history of memory impairment, noticed by her brother, had worsening memory and word-finding difficulty. She became angry at the suggestion of impairment and showed decline in financial affairs. She was alert and friendly but had anomic and paraphasic speech. She knew her name but not her age or the current year.
Alzheimer's Dementia (AD)
AD spreads through the brain.
The cerebral cortex shrinks as neurons die.
Alzheimer's Disease Progression
Mild Cognitive Impairment: Loss of recent memory, faulty judgment, personality changes.
Moderate: Verbal and physical aggression, agitation, wandering, sleep disturbances, delusions.
Severe: Loss of all reasoning, bedridden, incontinence.
Average duration is 8 years, ranging from 2-20 years, ultimately leading to death from pneumonia and other comorbidities.
AD: Plaques and Tangles
AD is characterized by:
Extracellular accumulation of beta-amyloid (plaques).
Intracellular accumulation of tau (neurofibrillary tangles).
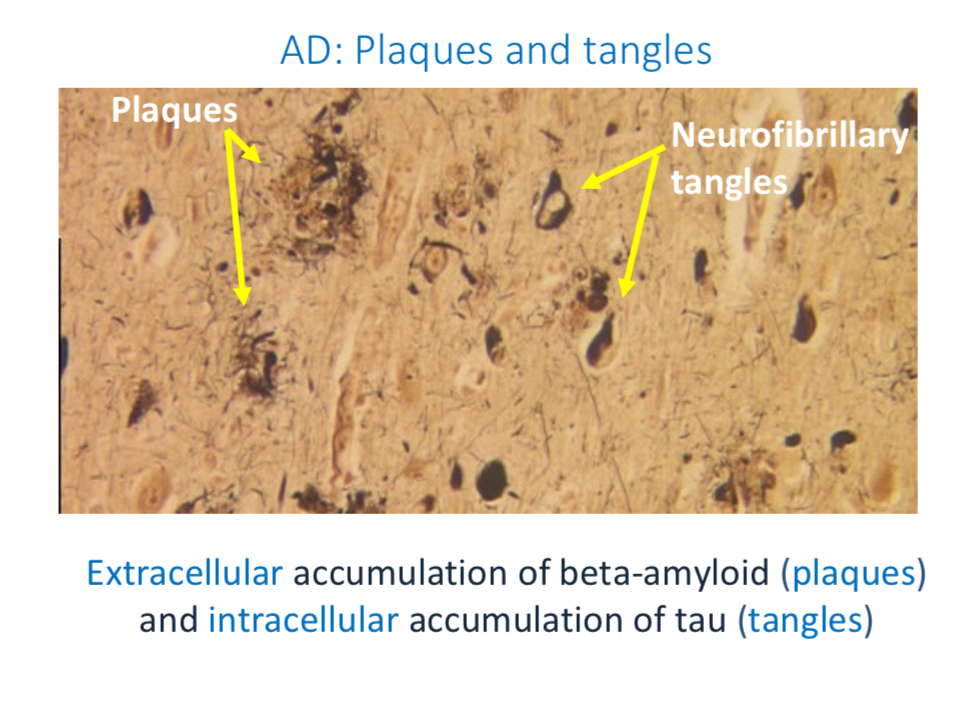
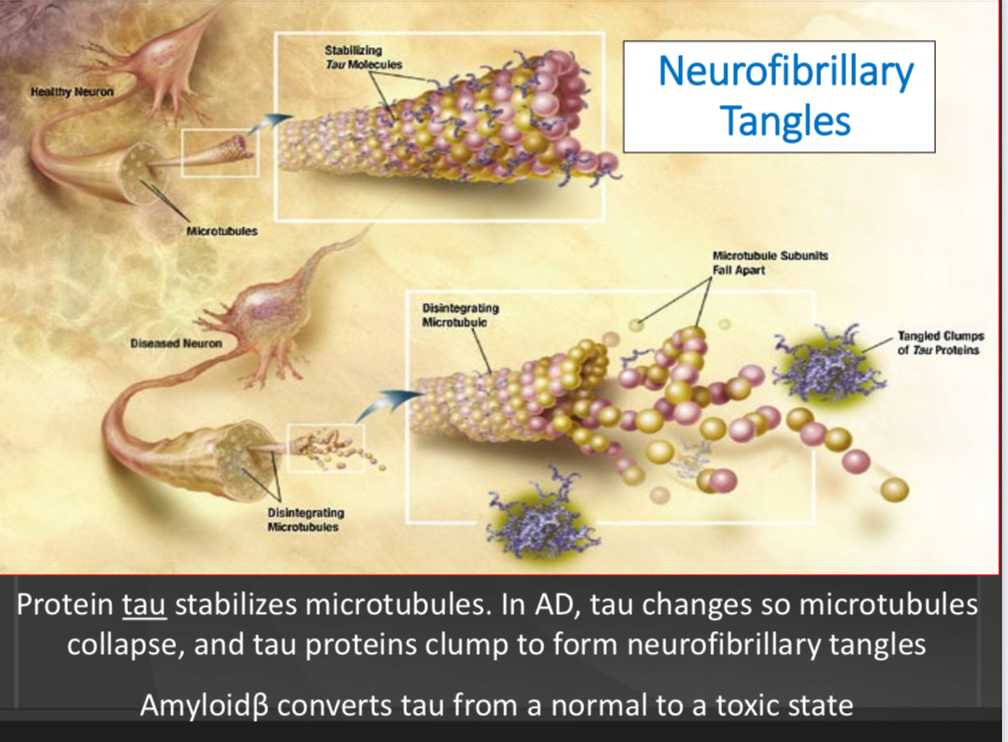
Neurofibrillary Tangles
Protein tau stabilizes microtubules. In AD, tau changes, collapsing microtubules, and tau proteins clump to form neurofibrillary tangles. Amyloidβ converts tau from a normal to a toxic state.
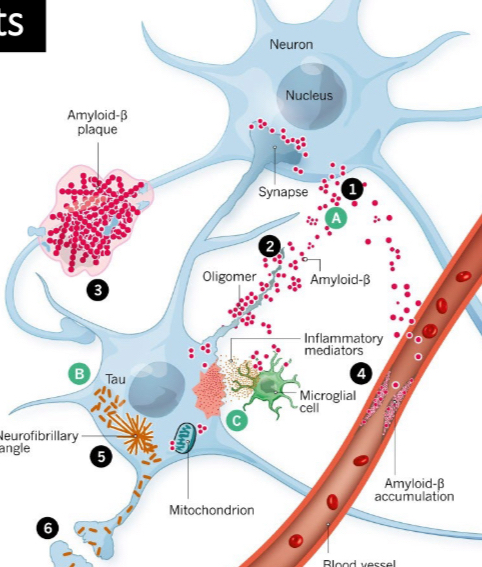
Amyloid Plaques Formation
Amyloid-β is produced from amyloid precursor protein in the membrane of neurons.
Amyloid-β clumps (plaques) in synapses between neurons.
Amyloid-β clumps outside cells and in blood vessels.
This activates microglial cells to release inflammatory chemicals.
Misfolded tau clumps into neurofibrillary tangles inside neurons.
Misfolded tau passes through synapses to other neurons, triggering further misfolding of tau.
The process repeats, and the disease spreads from neuron to neuron.
Normal Forgetfulness vs. Dementia
Normal age-related forgetfulness includes:
Forgetting where you left things.
Trouble remembering what you just read.
Walking into a room and forgetting why you entered.
Not being able to retrieve information ‘on the tip of your tongue.’
Blocking, such as calling a grandson by your son’s name.
Changes in Synapses: Mechanisms of Memory Storage
In 1894, Ramón y Cajal proposed that memory is stored as an anatomical change in the strength of neuronal connections. A synapse is plastic if it can change the strength with which it affects its target.
Anatomical Changes at Synapses
Anatomical changes at synapses store memory:
Presynaptic, postsynaptic, or both.
Increased neurotransmitter release, or effectiveness of receptors.
Inputs from other neurons increase or decrease neurotransmitter release.
Don Hebb's Hypothesis
Experience changes brain structure:
Neurons that fire together wire together: If a presynaptic axon and postsynaptic neuron are active at the same time, the synapse is strengthened.
Neurons that fire out of sync lose their link: If a presynaptic axon is active but the postsynaptic neuron is inactive, the synapse is weakened.
Environmental Enrichment and Learning
Rats raised in enriched environments (EC) showed better learning compared to those in standard (SC) or impoverished (IC) conditions.
Effects of Enrichments on Learning
Enriched environments promote better learning.
Dendritic Branching
Rats in enriched conditions showed increased dendritic branching.
Cerebral Changes and Behavioral Benefits
Rats in enriched conditions had:
Increased AChE activity, thicker cortex, especially occipital.
Increased dendritic branching, especially basal dendrites.
Increased synaptic contacts.
Behavioral Benefits:
Promoted better learning and problem-solving.
Aided recovery from conditions such as malnutrition.
Protected against age-related decline in memory.
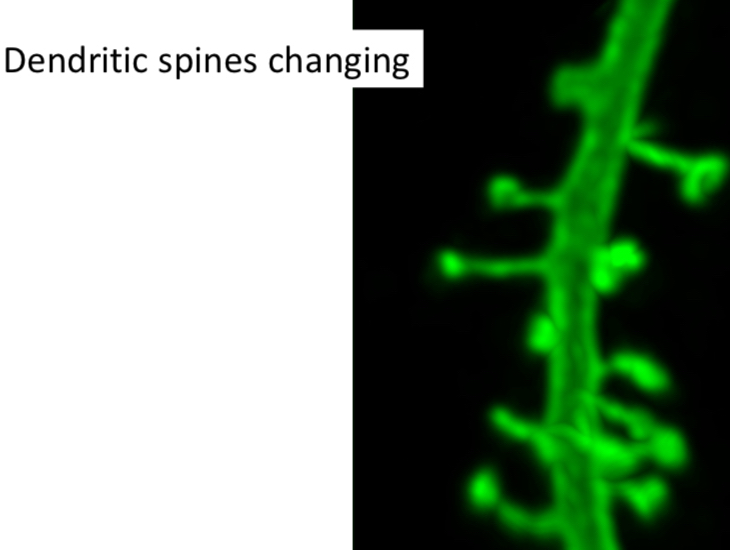
Structural Changes in Neurons
Dendritic spines change to produce a memory.
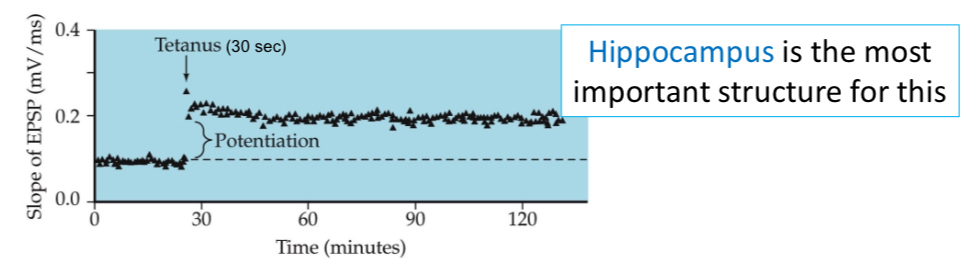
Long-Term Potentiation (LTP)
Synapses in LTP are like Hebb synapses:
Tetanus drives repeated firing.
Postsynaptic targets fire repeatedly due to stimulation.
Synapses get stronger.
Tetanus: Brief electrical stimulation triggers thousands of axon potentials.
After 30 seconds of tetanus, EPSPs remain high for hours.
The hippocampus is the most important structure for this.
AMPA and NMDA Receptors in LTP in Hippocampus
Glutamate first activates AMPA receptors.
NMDA receptors at rest have a magnesium ion (Mg^{++}) block of their calcium channels.
NMDA receptors do not respond until enough AMPA receptors are stimulated to partly depolarize the neuron.
After partial depolarization, Mg^{++} is removed, and the NMDA receptor allows Ca^{++} to enter in response to glutamate.
The large Ca^{++} influx activates protein kinases, enzymes that phosphorylate (activate) many things.
Now there are 2 AMPA receptors in the membrane, which unblock more NMDA receptors (AMPA upregulation is short-lived, though).
Neurochemical Cascade During Induction of LTP
CREB binds to DNA promoter regions.
CREB changes the transcription rate of genes.
These genes produce proteins to change synapse structure and contribute to LTP.
Inhibiting LTP
Other proteins block CREB from altering gene transcription.
Inducible cAMP early repressor (ICER) makes CREB antagonists.
They compete with CREB for binding sites, disrupting the formation of long-term memories.
Retrograde Signaling
Induction of LTP activates a retrograde signal for the presynaptic neuron to release more transmitter, creating a feed-forward process.
LTP Summary
LTP makes synapses more effective by:
Increasing postsynaptic receptors.
Increasing transmitter release.
Long-Term Potentiation/Depression (LTP/LTD)
Spikes occurring in a presynaptic cell a few milliseconds before those in the postsynaptic cell trigger long-term potentiation (LTP), strengthening the synapse.
Spikes in the opposite temporal order weaken the synapse, causing long-term depression (LTD).
Learning and Glia
Glial cells (astrocytes) are needed for LTP to develop. Spatial memory is altered in mice with disrupted glial cells. Enriched environments produce new glial cells.
Brain Mass Decline
Brain mass decline starts by age 25! Shrinkage of the hippocampus correlates with memory impairment. In normal aging, hippocampal atrophy reflects a change in volume, but not a loss of neurons. There may be a loss of dendritic branches, decreased cell size, or loss of glial cells. In Alzheimer's dementia, neurons die.
Spatial-Location Recognition Memory
Hippocampal lesions impair spatial-location recognition memory.
Compensatory Recruitment in Older Brains
Some old brains compensate by recruiting additional brain areas.
Early Experience and Aging
Enriched early experience:
Reduces cortisol (which causes hippocampal atrophy), allowing a better response to transient stress.
Prompts nerve growth factor expression in the hippocampus, preventing hippocampal degeneration.
Enlarges neural networks, cushioning the loss of synapses in aging.
Late Enriched Experience
Living in active environments and involvement in cognitive activities reduces cognitive decline.