PS101 EXAM PREP
Chapter 1: Overview
What is psychology?
The scientific study of mental processes and behaviour
Mental processes: activities of our brain when thinking
Behaviour: observable activities of an organism
Level of Analysis (3 levels)
Mental processes and behaviours can be studied at multiple levels of analysis:
The brain- brain structure and function
How does stimulation of the amygdala affect aggression?
How do certain personality factors influence aggression?
The person - thoughts and feelings
How do personality factors influence aggressive behaviour?
The group - family, friends, culture
How does exposure to violence in the media affect aggression
Psychology roots (parents)
Philosophy - approx. 400 BCE
Aristotle, Plato, Socrates asked questions about the mind, questioned behaviour and God.
Developed scientific methods
Physiology - 1600’s
Descrates contemplated mind-body dualism (Nativist)
Believed mind and body were separate and connected through the pineal gland
Believed if physical brain was dead, the mind would live on
Locke argued we learn by experience (believed we are not born with anything, a blank slate)
Believed everything we learn today is because of learning
Psychophysics - 1800s
The relationship between physical stimuli and their psychological effects
Fencher quantified mental events
Fencher quantified mental events
The early days of Psychology
Wilhelm Wundt
Opened the first ever psychology lab in 1879 in Leipzig, Germany
Made psychology a science by adding carefully measured observations and experiments
He studied consciousness
Defined consciousness as a immediate awareness
G. Stanley Hall
1883 - established the first psychology lab in North America
1887 - launched America’s first psychology journal
1892 - one of 3 & major player in establishing the American Psychological Association (APA)
James Mark Baldwin
1890 - established the first psychology lab in Canada at U of T
Heard about Wundt’s idea and was very interested - which was another student of Wundt’s
What should be the focus of Psychology?
Structuralism - led by Edward Tichener
Sough to understand the basic elements of consciousness
Relied of introspection
Reporting on sensations and other elements of experience
Not very scientific
The whole idea of making in objective had failed - everybody had different answer for the same thing
*playing sound of ticking clock and have to write adjectives about the clock*
Slow, monotonous, steady, faint,
Functionalism - led by William James - went to Harvard
Sought to understand the function or purpose of consciousness
Wrote principles of Psychology which was published in 1890
Led other schools of thought, behaviourism, applied psychology
Impressed by charles darwin ideas
Gestalt psychologists
Said consciousness cannot be broken down into elements
We perceive things as whole perceptual units
The whole is greater than the sum of its parts
Learning is tied to what we perceive
We perceive the whole simulation by whole not part by part
Perspectives on Behaviour
Perspectives on behaviour: different vantage points for analyzing behaviour and its causes
Major perspectives in psychology:
Psychoanalysis
Behaviourism
Humanistic psychology
Cognitive psychology
Psychobiology / neuroscience
Psychoanalysis
Founded by Sigmund Freud in the early 1900s
Focused on the unconscious
Drives, wishes, needs, and desires of which we are not aware
Emphasized the importance of early childhood experiences
The way resolve these unconscious is what you see on the outside- for example- personality
Behaviourism
Dominant school of thought in the early 1900s
Founded by John B. Watson
Emphasized psychology’s focus on observable behaviour
Showed that phobias can be learned
Iven Pavlov
Studied classical conditioning in dogs
B.F. Skinner
Showed how consequences of behaviour can influence future behaviour
Studied rats and pigeons- consequences of actions
Albert Bandura
Described learning by social observation
Bobo doll experiment
More cognitive/observational focused
Humanistic Psychology
Argued that psychoanalysis and behaviourism were de-humanizing
Emphasized the unique qualities of humans
Focused on freedom and personal growth
Led by Abraham Maslow and Carl Rogers
Cognitive Psychology
Cognition: mental processes involved in acquiring knowledge
1950’s and 1960a: Neisser, Miller, and Chomsky
Applied the scientific method to study the mind
Became the dominant perspective in psychology
Psychobiology / neuroscience
Explained behaviour in terms of physiological processes - highly dependant on technology
Kart Lashley (1950s)
Observed behavioural changes in rats after removing parts of their brain
Donald Hebb (1950s)
Cell assemblies describe neural networks
Wilder Penfield (1970s)
Mild electrical stimulation of different areas of the brain evokes different responses
Roger Sperry (1980s)
Left and right brain functions
Ba
Chapter 2:Overview & Appendix B
What is Science?
Basic assumption – events are governed by some lawful order that can be observed, measured, and tested
The scientific method is designed to help the scientific process remain as accurate and precise as possible: - psychology uses the scientific method
How Do Psychologists Conduct Research?
Step 1- make observations, review literature
Example - You’re working at camp and notice that kids who eat more sugar are less able to follow rules and instructions for the games and activities you create for them. Makes you wonder about the link between refined sugar consumption and hyperactivity, so you review previous studies
What do we already know about this???
Step 2 - develop a testable hypothesis
Hypothesis - a tentative prediction about the relationship between two or more variable
Variable - any measurable condition that is controlled or observed in a study
Best if the variables are operatioanlly defined in such a way that it is testable and observable
Example is on the slideshow(slide#6)
Children who consume more calories from sugar will ask more questions and make more errors during activities.
Children who eat a minimum of 3 chocolate bars per day will spend more time in time-out during activities.
Children who consume more than 50 mg of refined sugar in a day will be less able to sit still in a chair for 15 minutes.
Step 3- Choose participants, select the research method, collect data
A random sample sample of participants is chosen from the population
Population- the entire group that is of interest to researchers
Sample - the portion of the population that is used the study
Sample bias- choosing a sample that does NOT represent your population
To make conclusions about a population based on your sample, and avoid sampling bias, you need:
sample=population
We can do this by random sampling- making sure that every individual in the population has an equal chance of being included in you sample
There are three methods of data collection psychologists on to describe the characteristics of behaviour:
Case studies
Naturalistics observation
Surveys and questionnaires
The case study: an in depth investigation of a single participant using different data collection techniques
Advantages
Useful method to study rare behaviours
Very detailed
Can be a source of support for the cause of?
Disadvantages
Results may not generalise to other people
Potential for researcher bias: when they see only what they expect to see
Cannot determine cause and effect
The survey and questionnaire: participants are asked a series of question about certain aspects of their behaviour (written or interview)
Advantages
Quick and cheap data collection
Good to study behaviours that cannot be observed
Disadvantages
Careful of wording effects
Results depend on what participants themselves say
Potential for participant bias- when participant answer according to what they think they should say rather than truthfully
Cannot determine cause and effect
Naturalistic observation: observing and recording the participants natural behaviour, without influencing the participant
Advantages
Behaviour studied under natural
Good to use in conjunction with lab experiments
Disadvantages
Time consuming
Difficult not to influence behaviour
Potential for hawthorne effect: when participants act differently because they know they're being observed
Cannot determine cause and effect
Select the research method, collect data
There are two main types of research methods that psychologists use to test their hypotheses
Experimental research: research that is used to demonstrate cause and effect
The researcher manipulates a variable
There are different groups of participants, and each group is exposed to something different
Allows cause-effect conclusions
Experimental research definition
Independent variable (iv): the variable that is manipulated
Dependant variable (dv): the variable that is measured
Experimental group: the group that receives the manipulation
Control group: the group that does not receive the manipulation and serves as a comparison
Two types of groups in experimental research:
Need to ensure that the experimental group is the sae as the control group except for the dose of sugar consumption
Experimental group: Consumption of 50 mg or more of refined sugar within a 24 hour period for 7 consecutive days.
Measure sit-still score in the stabilimeter chair for 15 minutes
Control group: Consumption of less than 20 mg of refined sugar within a 24 hour period for 7 consecutive days
Measure sit-still score in
the stabilimeter chair for 15 minutes
This is how experiments allow for cause and effect conclusions, because:
If only difference between the experimental and control group is the independent variable, then any difference found between groups must be caused by the independent variable
Example: If the only difference between our two groups of children is the amount of sugar consumption, then any difference in sit-still scores between the two groups must be caused by the sugar consumption
Correlational research: research that asks how variables are related to each other
Advantages
Useful for studying topics that can be studied using experimental methods due to ethical/practical reasons
Can study behaviours under more natural conditions
Disadvantage
Does not allow causal conclusions
Double blind procedure- neither the participants nor the researcher knows who is in which group
Neither the children themselves nor the person collecting the data from the sit still chair know who consumed sugar and who didn't
Step 4: analyse the data, accept or reject the hypothesis
Use stats
If hypothesis was supported
Confidence in theory increases
Theory- a set of interrelated ideas used to explain a set of observations
Consider alt explanations
Inspect data and research methods for possible errors
If hypothesis was not supported
Confidence in theory decreases
Revise, refine or discard theory
Step 5: seek scientific review, publish, replicate
Allows your work to be reviewed, criticised and scrutinised by other experts in the field
Ensures that the research you read in peer-reviewed journals is top notch
Step 6: build a theory
Incorporates your results into existing theories or develop a new theory
Process starts over again at step 1
How do psychologists make sense of the research results
Statistics!
Recall two main types of research methods:
Correlation research: no manipulation, the researcher just measures two variables
The correlation coefficient indicates if there is a relationship between the two variables, represented by the statistics “r”
Experimental research: researcher manipulates a variable and compares performance across different groups
Inferential statistics: indicate if the difference between groups is meaningful
Correlations describe relations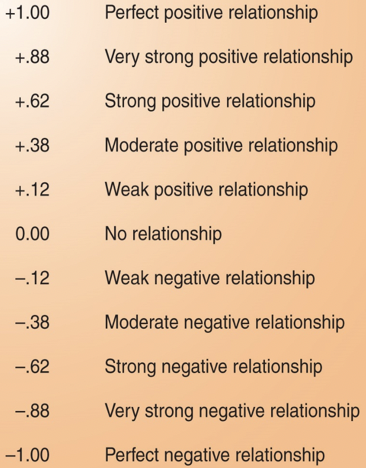
What can we say about the relation between variables when we know the correlation coefficient r
Positive correlation- when one variable increases. The other increases
Negative correlation- when one increases, the other decreases
Zero correlation- when the variation in one variable has nothing to do with variations in the other
Chapter 3:
About the brain
Brain facts
Weighs 3 pounds or 1400g
2 % of body weight but uses 20% of our oxygen
Wrinkly, greyish beige colour, feels like soft tofu
75% water
Made up of 100+ billion neurons or brain cells
Techniques to study the brain
Two approaches to learning about the brain
Study what happens when part of the brain isn't working normally
Case studies of brain damage, lesioning, electrical stimulation, magnetically deactivating
Use fancy equipment to study normal brain structure and function
CT scans, MRI, fMRI, PET scans, EEG, ERP, DTI
Techniques to Study the brain
Case studies of brain damage
When a stroke or injury damages part of the brain, we have a chance to see the impact on the mind
Lesioning
Surgical destruction of the brain tissue performed on animals
Has yielded some insights about less complex brain structures
eg : morris water
Electrical stimulation
Parts of the brain and even neurons can be stimulated electrically, chemically or magnetically]
This can result in behaviours such as giggling, head turning or stimulated vivid recall
Magnetically deactivating
Transcranial magnetic stimulation (TMS)
A procedure in which an electromagnetic pulse is delivered to a specific region of the brain to temporarily inactive that region
Using a weaker pulse can stimulate areas and has therapeutic uses
Depression, gambling
Computed tomographic scans (CT scans)
When a computer constructs a three dimensional x-ray image from a series of two dimensional images
Magnetic resonance imaging scan (MRI scan)
Brain structure is mapped out using magnetic fields
Different areas of the brain are made up of slightly different molecular compositions which have different magnetic properties
Produces a picture of the brain that is very clear
Functional magnetic resonance imaging scan (fmri scan)
It relies on the fact that oxygen is sent to the regions of the brain that are active
fMRI scanner can measure differences in blood oxygen over time while the person is doing a task
This functional map is then put on top of the structural map to get an overall map of how much each region of the brain is working on a given task
Positron emission tomography scan (PET scan)
Allows us to see what part of the brain is active by tracing where a radioactive form of glucose goes while the brain performs a given task
Electroencephalogram
A recording of the electrical waves sweeping across the brains surface
Useful for studying seizures and sleep
Event related potential (ERP)
When the change in electrical activity is time locked to the presentation of a stimulus
Requires many trials averaged over many EEG signals to remove the fluctuations in EEG signals
Diffusion Tensor imaging (DTI)
A structural neuroimaging technique that allows researchers to measure white matter pathways in the brain
These pathways are often damaged in individuals who suffer concussions
The nervous system
The nervous system contains two main categories of cells
Glial cells
Found throughout the nervous system
Provides support for neurons
Recent evidence that they also modulate neural activity
Neurons
Directly involved in communication
Receive, integrate, and transmit information to and from other neurons
Four classes of glial cells:
Astrocytes
Largest glia, star shaped, many functions
Oligodendrocytes
Myelinate axons in CNS
Microglia
Response to injury or disease
Schwann cells
Myelinate axons in PNS
Neurons vary in form, location and interconnectivity within the nervous system
Parts of the neuron
Dendrites: Branching extensions that receive inputs from other neurons
Many different forms, depending on type and location of neuron
Axon: single process that extends from the cell and represents the outburst side of the neuron
Can take many forms
Cell body: contains the metabolic machinery that maintains the neurons
Organization of cells in the cells in the nervous system:
Neurons and glia are bunched together in various ways
The two main divisions of the nervous system
Central Nervous system (CNS)
Brain and Spinal cord
The CNS makes decisions for the body
Peripheral nervous system (PNS)
All neural pathways outside of the brain and spinal cord
Connects CNS with muscles, glands and sensory receptors
The PNS sends and receives information to and from the rest of the body
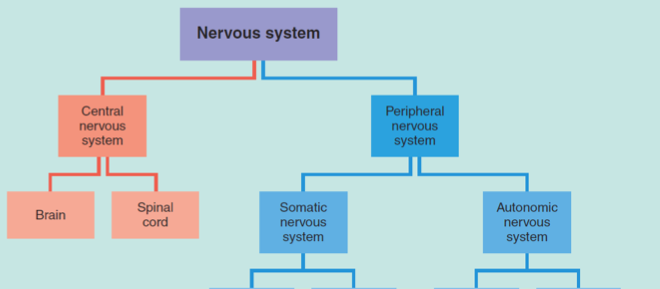

The autonomic nervous system:
Sympathetic NS arouses (fight or flight)
Parasympathetic NS calms (rest and digest)
Central nervous system:
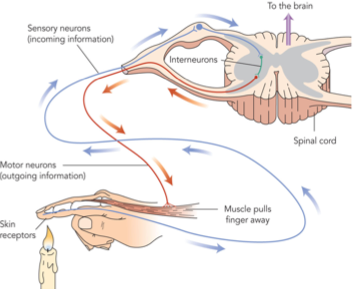
Spinal cord:
Most nerves enter/leave through spinal cord
Spinal reflexes do not involve the brain
Brain
Number of structures controlling behaviour
Both voluntary and involuntary
Two hemispheres (left & right)
Number of structures within and beneath
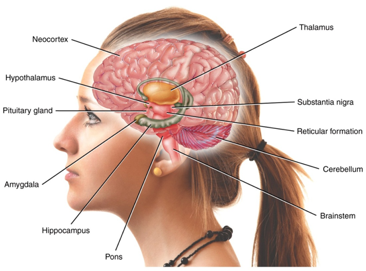
Organization of the Brain
Three major regions
Hindbrain: survival functions
Midbrain: sensation & action
Forebrain: memory, thought & emotion
Each region corresponds to where they are located relative to the spinal cord
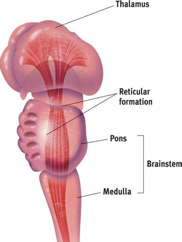
Hindbrain:
Medulla:
Automatic survival functions
Breathing, blood circulation, reflexes
Pons:
Sleep and wakefulness
Coordinates automatic and unconscious movements
Swallowing, posture, facial expressions, eye movements
Cerebellum:
Balance, coordination, and timing of movements
Attention and emotion
Reticular formation:
A network of neurons in the brainstem
Enables alertness
Also filters incoming sensory information
Midbrain:
Substantia nigra:
The nucleus from which dopamine neurons send their axons to the striatum (Forebrain)
Involved in movement control
Damaged in parkinson's
Forebrain:
Everything above the midbrain, including the cerebral ventricles
Spaces in the brain filled with cerebrospinal fluid that provides nutrition and cushioning for many parts of the brain
Composed of the:
Thalamus, hypothalamus, pituitary gland
Limbic system
Basal ganglia
Cerebral cortex
Thalamus:
The sensory switchboard
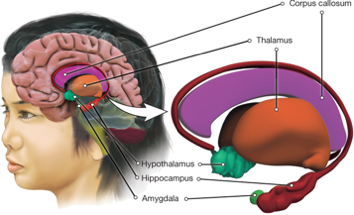
All sensory messages (except smell) are routed through the thalamus on the way to the cortex
Also sends messages from the cortex to the medulla and cerebellum
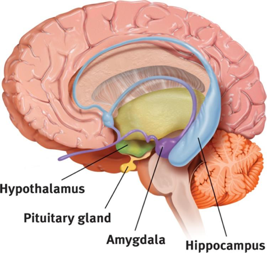
Hypothalamus:
Lies below (‘hypo) the thalamus
Regulates body temperature
Ensures adequate food and water intake (homeostasis)
Involved in sex drive
Directs the endocrine system via messages sent to the pituitary gland
Pituitary gland:
The ‘master gland’ of the endocrine system
Produces hormones that regulates other glands
Controlled by the hypothalamus
Limbic system
An integrated network involved in emotion and memory
Made of 4 structures
Amygdala
Hippocampus
Hypothalamus
Thalamus
Amygdala
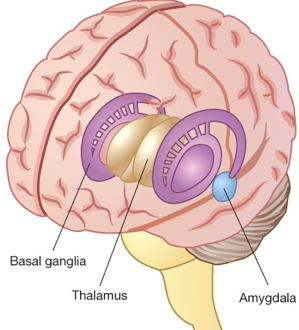
Helps process emotions, especially fear and aggression
Mediates memory formation for emotional events
Hippocampus
Processes continuous, episodic memories
Important in the formation of new memories
Basal ganglia
Functions in both voluntary movement and responses rewarding stimuli
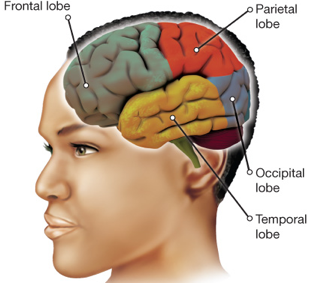
The cerebral cortex:
The outermost layer of the brain, 3mm thick
Measures 2200-2400 cm2, with many folds
Allows more cortical surface packed into skull
Made up of mostly cell bodies, which are grey in colour, so cerebral cortex often called the grey matter
Deeper grooves are used to define the boundaries of the four lobes found in each hemisphere
Occipital lobe
Processes visual information
Contains the primary visual cortex, after which visual information is routed along two different pathways
Object recognition via temporal lobe
Where objects are via parietal lobe
Processes body sensations
Contains the somatosensory cortex
Temporal lobe
Processes auditory information
Contains the primary auditory cortex
Contains Wernicke’s area
Important in speech comprehension
Frontal lobe
Speech and skeletal motor functions
Contains the primary motor cortex
Contains Broca’s area
Contains the prefrontal cortex
Important in executives functions like planning, decision making, and controlling attention
Cerebral cortex:
Primary motor cortex
Controls movement on opposite side of body of over 600 voluntary muscles
Laid out in a pattern represented by a motor homunculus
Amount of cortical space devoted to each motor area is proportional to the sensitivity of the motor function
Somatosensory cortex:
Receives sensory information from opposite side of the body
Laid out in a pattern represented by sensory homunculus
Amount of cortical space devoted to each sensory input is proportional to the sensitivity of the sensory function
Primary motor cortex and somatosensory cortex:
Topographically organised
Neural communication?
What happens between neurons?
Resting potential:
If an axon is not sending or receiving any signals, then it is negatively charged at about -70mV
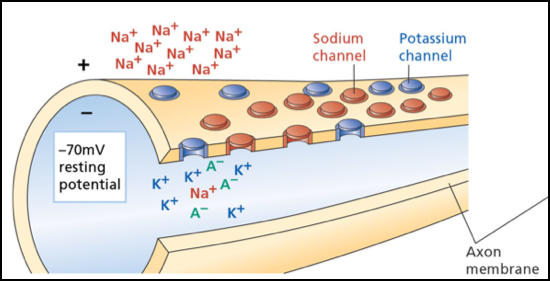
Two reasons for negative charge when neuron is in this balanced, resting state:
Concentration gradient
The tendency for molecules, which are always in motion, to distribute themselves evenly in their environment
Electrostatic pressure
Ions (molecules with a positive or negative) will attract or repel each other depending on their electric charge
Opposites attract
Organic ions (A-)
Stuck inside cell
Potassium ions (K+)
Flows relatively freely
Concentration gradient wants to push K+ outside cell
Electrostatic pressure wants to keep K+ inside cell
Sodium ions (Na+)
Concentration gradient and electrostatic pressure want to push Na+ inside cell
So why does Na+ stay concentrated outside the cell?
Difficult to move across the membrane
Na+ ion channels closed
Sodium-Potassium pump:
Continuously pushes three Na+ ions outside the cell in exchange for two K+ ions?
Action Potential:
Na+ ions would rush into the cell
This is what causes an action potential:
A sudden and brief increase in the permeability of the cell’s membrane to Na+
Done with help from the voltage-gated sodium channel
Detects the charge separation across the membrane and opens up channels for Na+ to cross the membrane
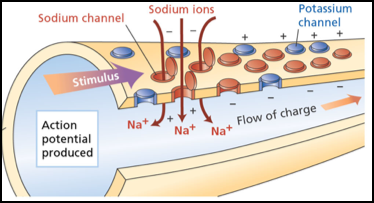
First, the membrane must be depolarized, or made less negative, by 10 or 20 mV
If cell depolarization reaches a certain level, called threshold, then Na+ channels open
Cell’s electric charge swings dramatically to the positive side, reaching a charge of + 40 mV
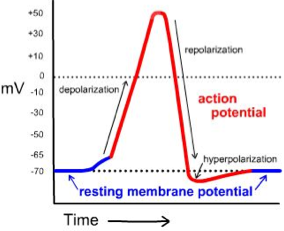
Voltage-gated sodium channels close until cell returns to resting state
Potassium channels also open, but with a bit of a lag
Concentration gradient & electrostatic pressure work harder to force K+ ions outside the cell
Causes cells to be hyperpolarized
All-or-none principle:
Once a neuron’s electric charge reaches threshold and an action potential is triggered, that action potential will always occur with the same strength
Like the firing of a gun – once the trigger is pulled, bullet always comes out the same
So how can our brain represent information that isn’t all-or-none, but continuous?
Can vary rate of firing and number of neurons firing
Neurotransmitters:
100-150 different neurotransmitters
More substances suspected
Each has a different effect
Specific excitatory or inhibitory effect
Several linked to specific psychological phenomenon
Glutamate
Most common inhibitory neurotransmitter
Used by most neurons in the CNS and PNS
GABA
Most common inhibitory neurotransmitter
Used by approximately 30% of neurons in brain
Epilepsy involves abnormal function GABA neurons
Acetylcholine (ACH)
Involved in memory and muscle activity
Dopamine
Linked with voluntary movements and positive emotions
Norepinephrine
Important for mood stability and arousal
Serotonin
Influences mood, eating, sleep, and sexual behaviour
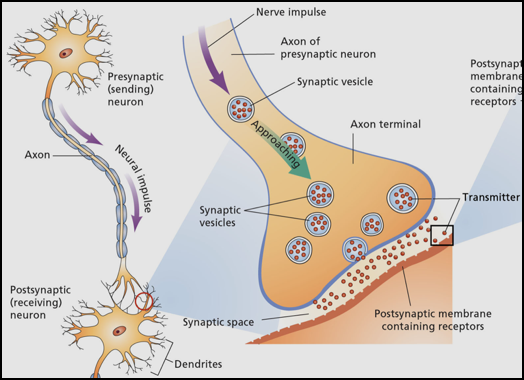
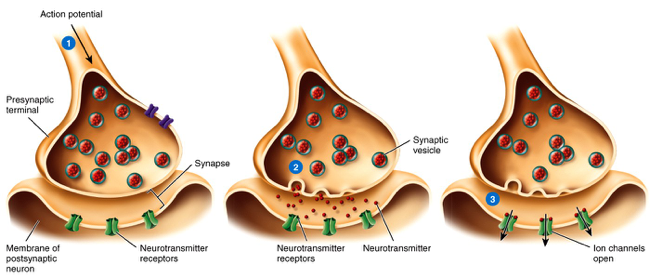
From electrical to chemical to electrical:
Action potential reaches terminal buttons
Eac terminal button contains many synaptic vesicles, or small, balloon like objects that contain molecules of a neurotransmitters
Causes some of the synaptic vesicles to open
Neurotransmitters are released into the synaptic cleft
Some neurotransmitters reach the postsynaptic neuron and bind with postsynaptic receptors
Causes specific ion channels to open, allowing a specific type of ion to pass in or out of the cell
From electrical to chemical to electrical
Depending on what ion channels open, can cause:
Excitatory postsynaptic potential (EPSP)
If a positive ion channel opens that allow positive ions to flow into the cell, the cell will depolarize and it will be easier to reach the threshold of an action potential
Inhibitory postsynaptic potential (IPSP)
If a negative ion channel opens and negative ions are forced into the cell, the cell will hyperpolarize and it will be harder to reach threshold of an action potential
Can also occur if potassium channels open and k+ is forced outside the cell (leaves the cell more negative)
One neuron can receive many EPSPs and IPSPs at the same time
Not an all or none process like the action potential
Summed effect of EPSPs and IPSPs determine the neuron’s polarisation
Reuptake
Occurs when the terminal buttons quickly remove the neurotransmitters from the synapse
Can inhibit inhibitory neurons
Behaviour would increase
Excite inhibitory neurons
Behaviour would decrease
The cell body has to make sense of all these inputs:
Some are quick, some are long-lasting, some excitatory, some inhibitory, some big, some small, some arrive early or late, and some may cancel each other out at the dendrites
Brain Lateralization
Hemispheric Lateralization= the fact that each hemisphere of the brain performs somewhat different functions
Left hemisphere
Language, mathematical, logical abilities
Positive emotions
Right hemisphere
Spatial relations, non-linguistic sounds (music), facial processing
Negative emotions
Handedness and language:
90% of people are right-handed
95% have left hemisphere language dominance
Among those who are left-handed:
50% have left hemisphere language dominance
25% have right hemisphere language dominance
25% have language functions in both hemispheres
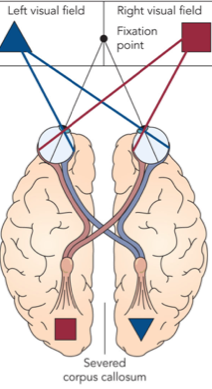
Right visual field is processed in the left hemisphere
Left visual field is processed in the right hemisphere
Normally hemispheres share information, but this can be prevented in split-brain patients
Patients with severed corpus callosum
Band of fibres connecting the two hemispheres
Split brain experiments:
If present picture to right visual field, information sent to left hemisphere only

Can name & describe picture
If present picture to left visual field, information sent to right hemisphere only
Can't name or describe picture, but can point to the picture they saw with their left hand
Brain Plasticity
Neuroplasticity: the capacity of the brain to change and rewire itself based on individual experience
Rats in enriched vs impoverished environments
String musicians
Neural reorganisation after amputation
Rewiring in the the adult visual cortex
Neuroplasticity: implications for recovery from brain injury
Chance of recovery best if injury occurred < 8 Years of age
Recovery better if damage is gradual as opposed to sudden
Left-handers have a better chance of recovering language processing than right handers
Chapter 6
Overview:
The nature of consciousness
Sleep and dreaming
Hypnosis
Psychoactive drugs
The nature of consciousness
Consciousness = the moment-to-moment awareness of ourselves and our environment
Several characteristics:
Subjective and private
Dynamic
Self-reflective
Intimately linked with attention
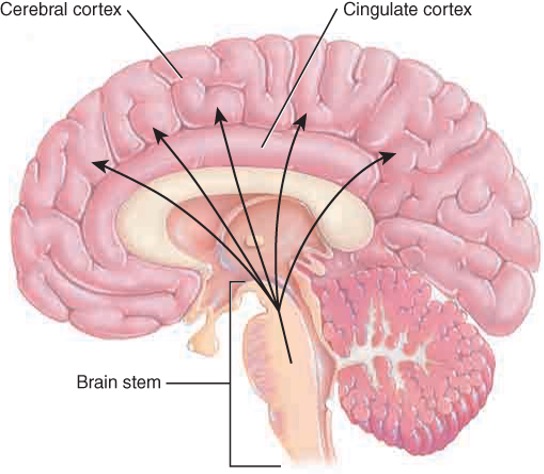
Two brain areas that are important for consciousness:
Thalamus: relays sensory information to the cerebral cortex
Cerebral cortex: responsible for being aware of one’s attention
Eg: patients with blindsight
Levels of consciousness:
Consciousness: mental events we are currently aware of
Eg: reading this slide
Preconsciousness: outside of current awareness and easily accessed
Eg: what you had for dinner last night
Unconsciousness: information that is not easily accessed by consciousness
Contents of which have been debated
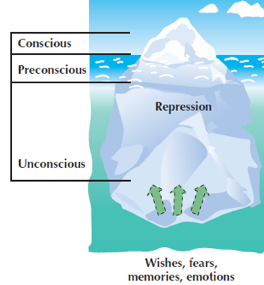
Freud’s view of the unconscious:
Contains thoughts and memories that are too painful for consciousness
Contents may seep into consciousness by accident
No supportive evidence
Cognitive view of the unconscious
Explicit vs implicit memories
Implicit memory = knowledge of which we are not typically aware
Egs: skills, classical conditioning, past experiences
Controlled vs automatic processing:
Automatic processing: processing that requires no consciousness
Egs: routine, well-learned tasks
Sleep and dreaming
Why do we sleep?
Adaptive theory: says that organisms sleep for self-preservation and to stay safe from predators
Restorative theory: says that sleep restores our brains and bodies
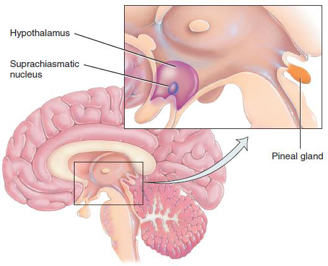
Circadian rhythm: a daily, rhythmic biological cycle
Controlled by the suprachiasmatic nucleus (SCN) of the hypothalamus
Circadian rhythms influence whether we are a morning person or a night person
Disruptions to circadian rhythms
Changes in season
Shift work jet lag
Stages of sleep:
Cycle through stages roughly every 90 minutes
Brain activity, other psychological responses change
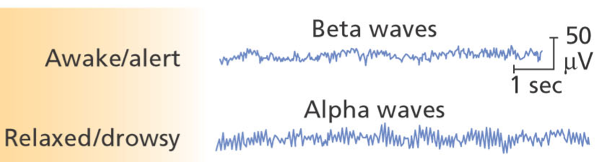
Beta waves occur when awake and alert (13-24 cps)
Alpha waves occur when relaxed and drowsy (8-12 cps)
Stage 1
Light sleep
Theta waves (4-7 cps)
Lasts few minutes
May experience ‘body jerks’
Stage 2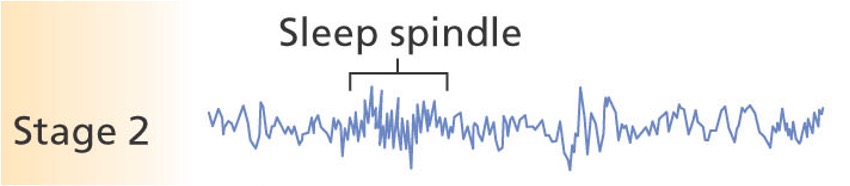
Sleep deepens, muscles more relaxed, harder to awaken
Sleep spindles (1-2 seconds bursts of rapid brain activity)
Stage 3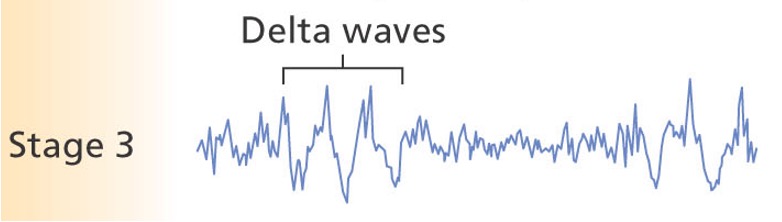
Sleep deepens
Regular appearance of delta waves (<4 cps)
Stage 4
Sleep deepens
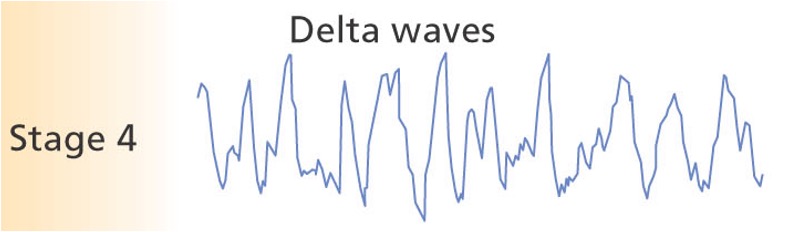
Delta waves dominate pattern
Stage 4 and stage 3 together called “slow wave sleep”
REM sleep:
Frequent dreaming
Heart rate increases, breathing rapid and irregular
Brain wave activity increases
REM sleep paralysis
Difficult for voluntary muscles to contract


After stage 4 period, sleeper goes back through earlier stages
Stage 3, stage 2, REM, stage 2, stage 3, stage 4, stage 2, REM, etc
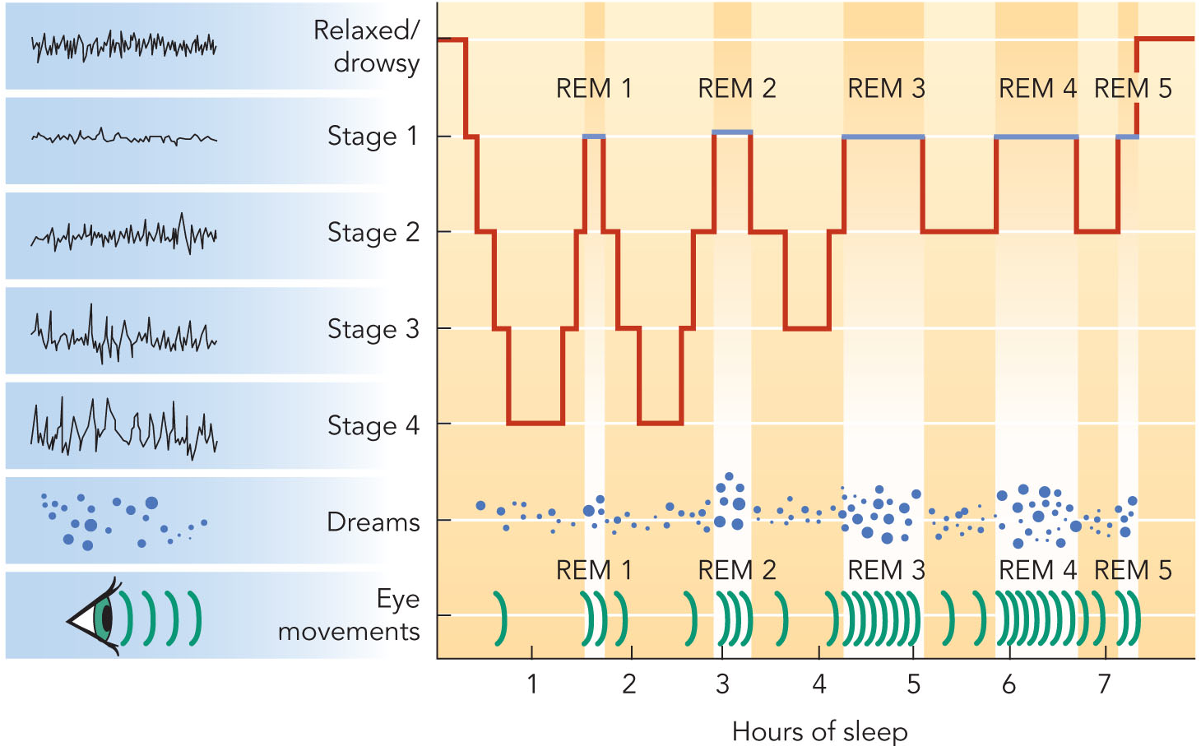
As the night goes on, see less Stage 4 and more REM
Special function of REM sleep
All mammals and birds experience both REM and NREM sleep patterns
REM sleep increases after being deprived of it
May be vital for mental functioning, especially for learning and memory consolidation
When do we dream?
Most dreams occur during REM sleep (more story like and vivid) but dreaming can occur in any sleep stage
What do we dream about?
Negative or unpleasant content is common
Content os affected by cultural background, life experiences, current concerns
Why do we dream?
Information processing theory: says dreams involve processing information from the day
Could be mental realm where we can solve problems and think creatively
Activation synthesis model of dreaming: says dreams reflect the brain’s attempt to make sense of random brain activity
Freudian dream theory: says that dreams reflect the unconscious wishes and desires
Freud called dreams the “royal road to the unconscious”
Two types of contents in a dream:
Manifest content: surface story of a dream
Latent content: disguised psychological meaning of a dream
Types of dreams
Nightmares: dreams filled with intense anxiety
Dreamers feel as though the situation is really happening
Lucid dreams: dreams in which people fully recognize that they are dreaming
Daydreams: fantasies that occur while one is awake and aware of eternal events and yet not fully conscious
Changes in sleep with age:
Sleep less
REM sleep decreases during infancy and childhood
Time in stage 3 and 4 declines
Chronic sleep deprivation results in:
General depressed state
Lower immune system
Lower ability to concentrate
Higher incidence of accidents
Lower productivity and higher likelihood of making mistakes
Sleep disorders
Insomnia
Chronic difficulty in falling asleep, staying asleep or experiencing restful sleep
Most common sleep disorder
Affects 10-20% of population
Has biological, psychological and environmental causes
Great non-drug treatment based on learning principles
Pair bed with sleep and nothing else
Narcolepsy
Extreme daytime sleepiness and sudden, uncontrollable sleep attacks
Cataplexy (sudden loss of muscle tone)
Cause is unknown
Genetic?
Can be selectively bred in dogs
Sleep apnea
About 1-5% of population
Repeated cycle in which breathing stops and restarts during sleep[
lasts 20-40 seconds up to a minute or two
Severe cases: 400-500 times a night
Most common cause
Obstruction of upper airway
Sleepwalking
Typically occurs during stages 3 or stages 4
More common among children
Causes
Hereditary, stress, alcohol, illness, medications
Treatment:
Psychotherapy, hypnosis, drugs, behavioural (walking before sleepwalking), wait to outgrow it
Myth
Waking a sleepwalker is dangerous
Nightmare disorder
Experience frequent nightmares
Nightmares are more common when stressed and in childhood
Night terrors
Frightening dreams that arouse sleeper to near panic state
Sleeper may flee room yet not remember event in morning
Typically occurs during stages 3 and 4
Most common during childhood
Hypnosis
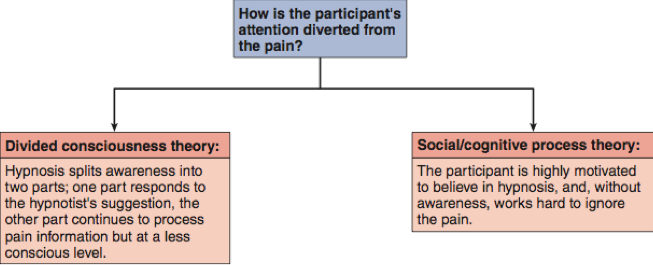
Hypnosis: a state of heightened suggestibility in which some people are able to experience imagined situations as if they were real
Hypnotic induction:
Process by which hypnotist leads person into hypnosis
Hypnotic susceptibility scales:
Series of pass/fail suggestions read after hypnotic induction
Posthypnotic responses:
A behaviour that was suggested while the person was hypnotised, but does not appear until later when a specific signal appears
Posthypnotic amnesia:
When the person who was hypnotised doesn't remember anything from the hypnosis session
Hypnotic hallucinations
Positive hallucinations: when a person is made to perceive something that isn't really there
Negative hallucinations: when a person is made to not perceive something that really is there
Hypnotic involuntary control
No power to get people to act against their will
Amazing feats?
No scientific evidence to support this
Memory enhancement?
Mixed results from controlled experiments
Some memories are pseudomemories
Pain tolerance
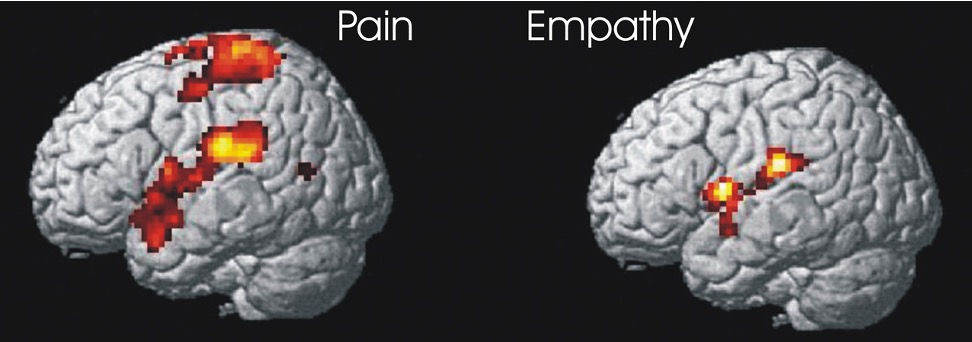
Hypnosis can help relieve pain, but so can mental imagery
Hypnosis and the brain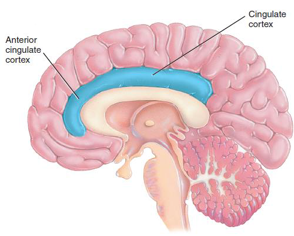
Neuroimaging research suggests that the brain’s anterior cingulate cortex may be particularly involved when hypnosis is used to reduce pain
How hypnosis works
Psychoactive drugs
Psychoactive drugs: any substance that alters mood, perception, awareness or thought
A pervasive part of society
Drugs and the brain
Drugs modify brain chemistry
Cross blood-brain barrier
Alter consciousness by facilitating or inhibiting neural communication
Recall neural communication
Neurotransmitters released into synapse and bind with receptors on the dendrites of the postsynaptic neuron
Neurotransmitters are deactivated (eg: reuptake)
Tolerance and withdrawal
Drug tolerance:
Decrease in responsivity to drug (need larger doses to feel the same effect)
Body attempts to maintain homeostasis
Compensatory responses:
Physiological reactions opposite to that of the drug
Brain is adjusting to body imbalance
Withdrawal
Compensatory responses after drug use is continued
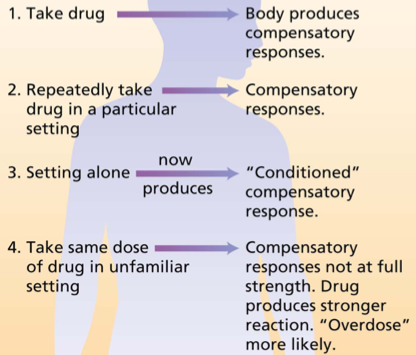
Learning, tolerance and overdose
Environment is powerful influence
Can become associated with drug and trigger compensatory
Conditioned drug responses
Tolerance for drug influenced by familiarity of drug setting
In unfamiliar setting, overdose reaction can occur even when typical amount of drug is used
Myths about substance abuse
Drug tolerance always leads to significant withdrawal
If a drug does not produce tolerance or withdrawal, you cannot become dependent on it
Physiological dependance is the major cause of drug addiction
Three main categories of psychoactive drugs:
Depressants
Stimulants
Hallucinogens
Depressants
Decrease nervous system activity
Moderate doses
Reduce feeling of anxiety
Produce euphoria
High doses
Slow vital life processes
Can be fatal
Alcohol
Nervous system depressants
Initial upper phase then brain centres become depressed
Increases activity of GABA (main inhibitory neurotransmitter)
Decreases activity glutamate (main excitatory neurotransmitter)
Combination creates ‘high’ and then ‘down’ phase
Sedative-hypnotics (benzodiazepines)
Egs: Xanax, ativan, valium
Influence neurons that produce GABA
Produces relaxation and drowsiness, relieves anxiety
Opioids
Egs: opium, heroin, morphine, codeine, methadone
Activates the opioid receptors in the brain, providing an analgesic effect and the related high
Reduces pain and emotional tension, produces pleasurable and calm feelings
Stimulants
Increase neural firing and arouse nervous system
Increase BP, HR, respiration, alertness
Amphetamines
Increase dopamine and norepinephrine activity
Continuous heavy use can produce amphetamine psychosis
Crystal methamphetamine is form of amphetamine
Ecstasy (MDMA): also a form of amphetamine
Interferes with serotonin reuptake
Produces feelings of pleasure, elation, warmth
Cocaine:
Increases activity of norepinephrine and dopamine by blocking reuptake
Chronic use associated with increased risk of cognitive impairment and brain damage
Crack is chemically converted form
Effects are faster and more intense
Caffeine
Works on adenosine neurons, which produces a sensation of increased alertness when stimulated
Nicotine
Influences dopamine and acetylcholine neurons, which increases alertness and reduces stress
Hallucinogens
Produces sensory or perceptual distortions called hallucinations
Many derived from natural sources
Can blur boundaries between fantasy and reality
LSD:
Stimulates dopamine and serotonin receptors
Dramatically strengthens visual perceptions (including hallucinations) song with profound psychological and physical changes
Cannabis (marijuana, THC)
Stimulates release of endorphins and dopamine
Produces a mixture of hallucinogenic, depressant and stimulant effects
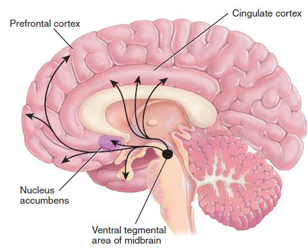
Psychoactive drugs activate a reward learning pathway, or ‘pleasure pathway’, in the brain
Reward-deficiency syndrome = says that people might abuse drugs because their reward centre is not readily activated by usual life events
Chapter 7
What is learning?
Classical conditioning
Operant conditioning
Observational conditioning
Learning and cognition
Factors that facilitate
What is learning?
Two “processes of change” in our development
Maturation and learning
Learning = a lasting change as a result of practice, study or experience
Has to be inferred from behaviour
Allows us to adapt to the environment
Two types of learning:
Associative learning = a change as a result of experience where two or more stimuli become linked
Non-associative learning = learning that does not involve forming associations between stimuli
Involves repeated exposure to only a single stimulus or event
Two types of non-associative learning:
Habituation = a decrease in the response to a stimulus after repeated exposure
Dishabituation = a recovery of the habituated response when exposed to a novel stimulus
Sensitization = an increase in the response to a stimulus after repeated exposure
Types of associative learning:
Classical conditioning = associates stimuli with each other
When two stimuli reliably co-occur, the first stimulus can become a signal for the impending arrival of the second stimulus
Allows the animal to prepare for the second stimulus
Operant conditioning = associating responses with consequences
Learn what consequences are likely to come after specific responses
Allows the animal to adjust responses accordingly
Classical conditioning:
Pavlov’s discovery
While studying digestion in dogs, Ivan pavlov found that salivation came to be triggered by neutral stimuli that reliably predicted the food such as:
Seeing the food or dish
Seeing the person who usually brought the food
Hearing that person’s footsteps
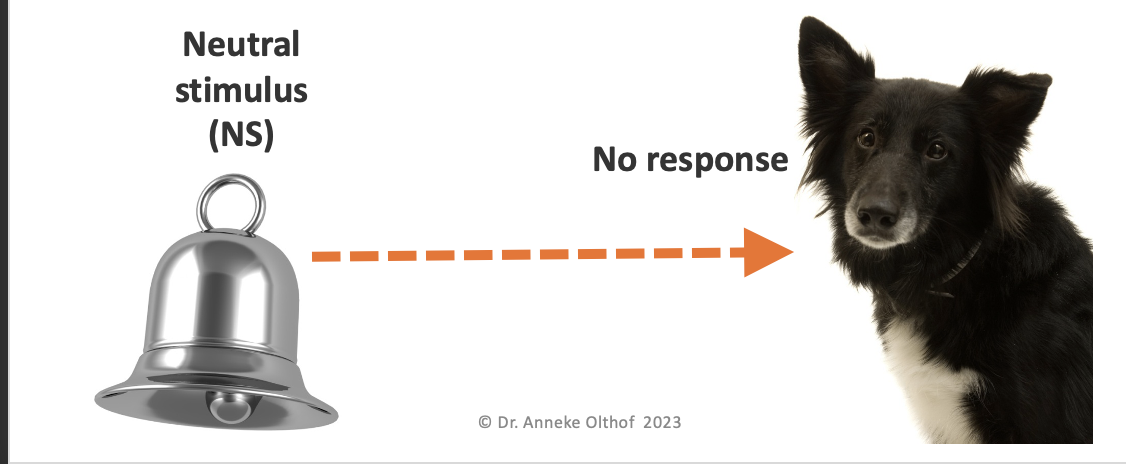
Before conditioning:
Neutral stimulus = a stimulus which does not trigger a response
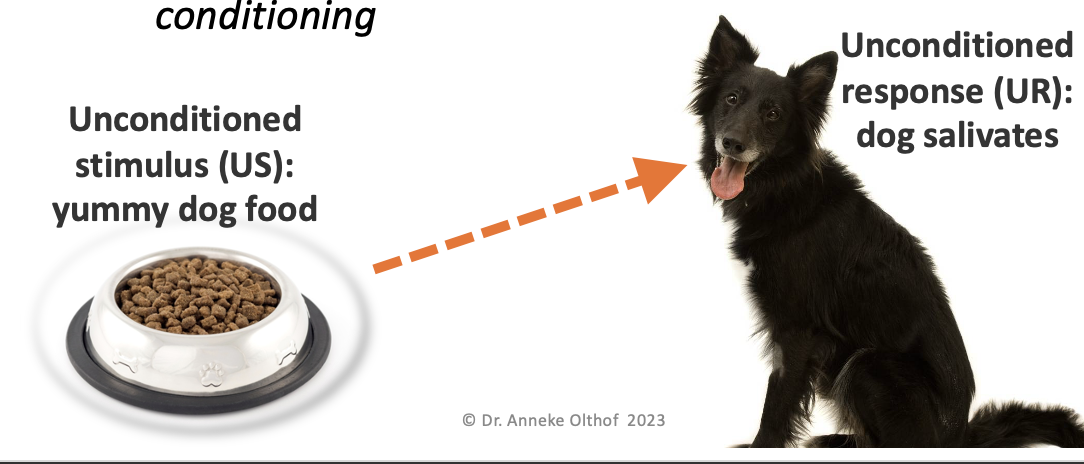
Unconditioned stimulus = a stimulus which triggers a response naturally, before/without any conditioning
During conditioning:
The bell (neutral stimulus) is repeatedly presented with the food (unconditioned stimulus)
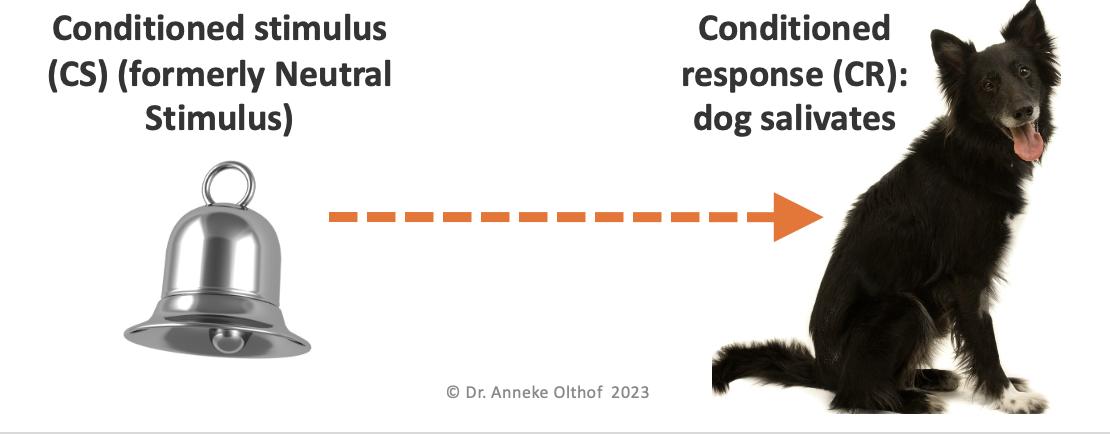
After conditioning

The dog salivates upon hearing the bell, or the neutral stimulus becomes a conditioned stimulus
Activity: your romantic partner always uses the same shampoo. Soon, the smell of that shampoo makes you feel happy.
US- your partner
UR- feeling happy around your partner
CS= smell of shampoo
CR= feeling happy to smell of shampoo
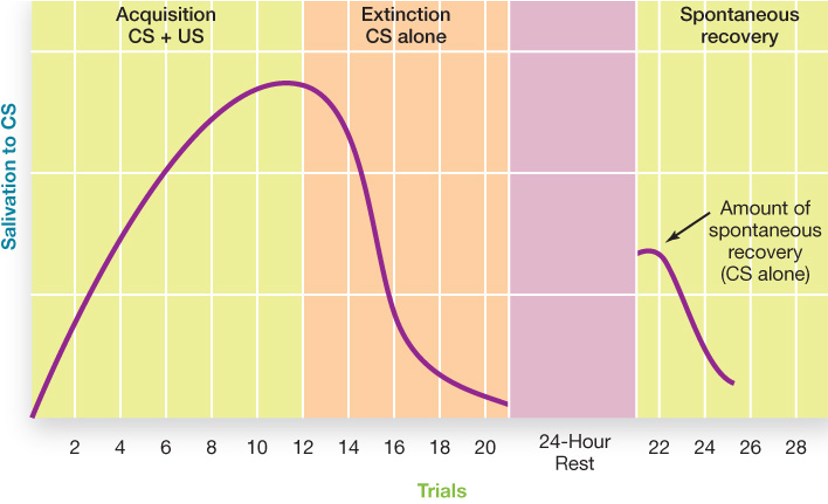
Acquisition = the initial stage of learning/conditioning
As the CS and US are paired, the strength of the CR grows
Timing is important - the CS should appear roughly hald a second before the US for learning to occur
Extinction = the diminishing of a conditioned response
If the US stops appearing after the CS, then the CR decreases
After extinction, may see spontaneous recovery = a return of the CR despite no further conditioning
Very likely to occur following a period of rest
Stimulus generalisation = the tendency to have conditioned responses triggered by similar or related stimuli
Example: a child who learned to fear white rats is also afraid of white rabbits and santa's beard
Responds to MORE stuff
Stimulus discrimination = the learned ability to only respond to a specific stimulus, preventing generalisation
Example: a child who learns to fear white rats is only afraid of white rats and not grey or black rats
Responds to LESS stuff
Higher- order conditioning = when a previously conditioned stimulus functions as if it were a US for further conditioning
Often used in advertising where products (CSs) are paired with sexualLy imagery (US)
Many applications
Phobias
Substance abuse
Immune response
Sexual arousal
Digestion
Reproduction
Territory defence
Learning about good and bad foods
Breast feeding
Advertising
Relaxation or fear
Operant conditioning
Involves adjusting our behaviour according to the consequences
Reinforced behaviour is more likely to be tried again
Example: a child punches another child to get a desired toy and it works; this child will likely try punching again
Punished behaviour is less likely to be tried in the future
Example: a child punches another child to get desired toy and gets sent to their room; this child is less likely to be punching again
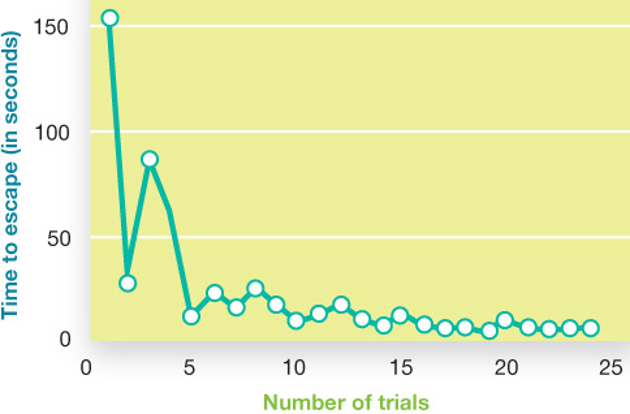
Thorndike’s Law of Effect states that behaviours that are followed by favourable consequences become more likely, and behaviours follows by unfavourable consequences become less likely
Skinner expanded on thorndike’s principles and wondered:
How can we more carefully measure the effect of consequences on behaviour
What else can creatures be taught to do by controlling consequences
What happens when we change the timing of reinforcement
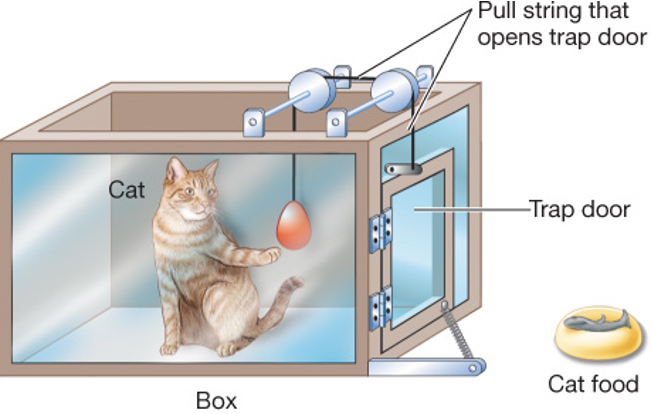
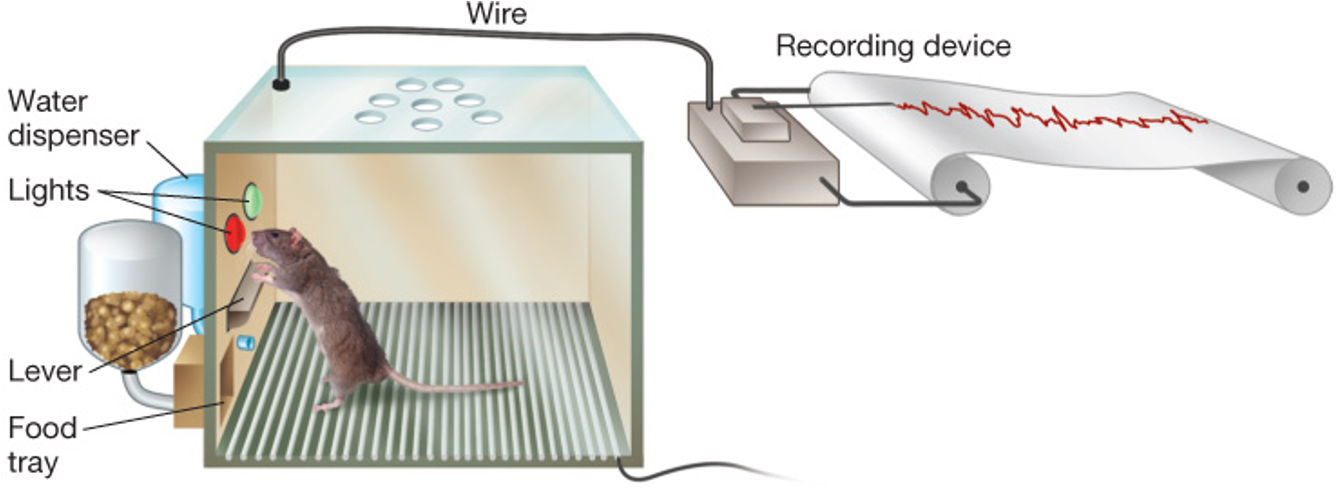
Skinner invented “the skinner box” or “operant chamber”, chich allowed detailed tracking rates of behaviour (lever pressing) over time
Reinforcement refers to any feedback from the environment that makes a behaviour more likely to reoccur
Positive reinforcement: adding something desirable
Negative reinforcement: taking away something unpleasant
A cycle of reinforcement: temper tantrums
What happens if the parent gives in to a temper tantrum???
The child's tantrum is positively reinforced, so the tantrums will get stronger and more frequent
The parent’s giving in behaviour is negatively reinforced, so the parent will give in sooner and more often
Punishment refers to any feedback from the environment that makes a behaviour less likely to recur
Positive punishment is when you ADD something unpleasant/aversive (scold the child)
Negative punishment is when you take away something pleasant/desired (no TV time, a time out)
The severity of punishment is not as helpful in decreasing a behaviour as making the punishments immediate and certain
The search for positives opposites - eg: don't fight becomes play nicely
In order to teach a desired behaviour, reinforce what's right more often than punishing what's wrong
Overview: type of consequences
Adding stimuli | Subtract stimuli | outcome |
|---|---|---|
Positive + reinforcement (you get candy) | Negative reinforcement (i stop yelling) | Strengthens target behaviour (you do chores) |
Positive punishment (you get scolded) | Negative punishment (no cell phone) | Reduces target behaviour (cursing) |
pink= uses desirable stimuli
grey= uses unpleasant stimuli
Schedules of reinforcement= the rules of how often and when reinforcement is delivered
In continuous reinforcement, the subject is rewarded every time they perform the target behaviour
The behaviour is learned very quickly, but also stops quickly if reinforcement is no longer delivered
In partial/intermittent reinforcement, the subject is rewarded only some of the time for doing the target behaviour
It takes longer to learn the behaviour, but it will persist longer without reward
Comparing continuous and partial reinforcement schedules:
Continuous reinforcement
Faster learning and faster extinction
Partial reinforcement:
Slower learning and more resistant to extinction
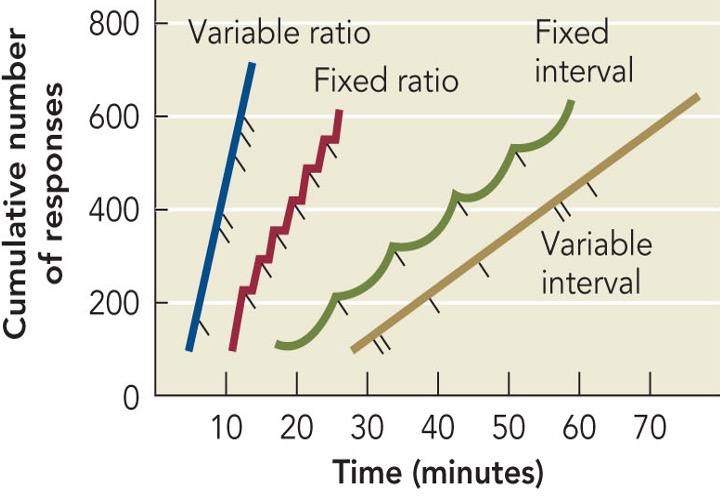
Different schedules of partial/intermittent reinforcement




Which reinforcement schedule produces the most responding (ie, more target behaviour)
Each schedule produces a predictable pattern of responses when number of responses is measured overtime
Shaping a behaviour by rewarding successive approximations to the behaviour is a way to train a new behaviour
Observational learning
Observational learning = learning that occurs by observing the behaviour of a model
Requires several processes:
Attention, memory, motor reproduction of behaviour, motivation
Highly adaptive
If learning were trial and error on our own, we would learn very slowly
From watching others we learn how to do things, when to do things, ect
Bandura’s bobo doll experiment showed that children are ready to learn from others
Children who watched an adult act aggressively towards the doll were more likely to behave aggressively than children who did not watch the adults act aggressively
The presence of mirror neurons also shows that we are wired to learn from others
Mirror neurons fire in the same pattern when we watch others doing or feeling something as if we were doing the action or having the feeling ourselves
Implications of our ‘readiness’ to learn from others in our modern time with ample media violence:
Research shows that viewing media violence leads to increased aggression and reduced prosocial behaviour (such as helping an injured person)
Learning and Cognition
Early behaviourists would argue that learning cannot occur without reinforcement but:
Latent learning = learning that occurs without reinforcement and is not expressed in behaviour until reinforcement is available
Early behaviourists would argue that there is no need to consider cognitive processes; BUT:
Insight learning = a sudden realisation of a solution to a problem or leap in understanding new concepts
Factors that facilitate learning
Timing
Multiple exposures separated by time facilitates learning
Massed studying is ineffective compared to space studying
Context effect:
Studying in several different locations facilitates learning
Minimises context effects
Awareness and attention
Although learning can happen without awareness, it is enhanced by awareness and attention
Attention can be driven by a ‘pop-out’ effect if one stimulus is noticeably different from the rest
Attention can be driven by active searching with more complicated stimuli
Attention can get in the way with stimuli that can be interpreted two ways
Example: the Stroop effect
CHAPTER 12
The nature of personality
Personality = an individual’s unique constellation of consistent behavioural traits
A collection of stable states and characteristics
Varies from one individual to another
Influences choices and actions
The psychodynamic perspective
Freud’s psychodynamic theory focuses on:
Unconscious determinants of behaviour
Constant interplay of unconscious forces that often conflict with one another
Outward expression of this is personality
Structure of personality:
Id
At the unconscious level
Innermost core of personality
Operates according to the pleasure principle
Ego:
At the conscious level (mainly)
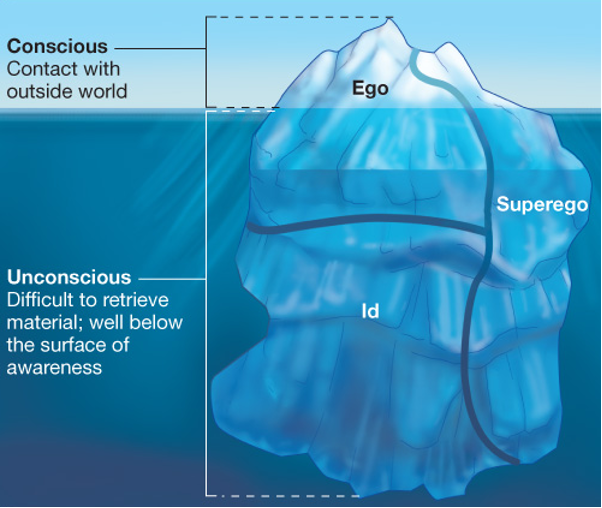
Operates according to the reality principle
Superego:
Moral aspect of personality
The ego functions to keep the impulses of the id under control
The ego feels anxiety if the impulses of the id threaten to get out of control
To deal with anxiety, ego uses:
Realistic strategies
Defence mechanisms = weapons of the ego that operate unconsciously to distort reality
Defence mechanisms:
Repression = thoughts and wishes remain in unconscious
A sexual abuse victim develops amnesia for the event
Sublimation = unacceptable impulses are presented as socially desirable behaviour
A man with hostile impulses becomes a reporter who ruins the careers of others with his stories
Denial = refusal to acknowledge the situation
A terminal cancer patient refuses to believe that won't recover
Displacement = finding a safe target
A man who was yelled at during work comes home and abuses his wife
Identification = unconsciously assuming the characteristics of a more powerful person in order to feel better about oneself
A person bullied as a child may become a bully in other situations in order to feel more powerful
Projection = an unacceptable impulse is attributed to others
A woman with a desire to have an affair represses this and accuses her husband of having an affair
Rationalisation = coming up with reasonable explanations for unacceptable feelings or behaviours to hide true motives
A teenager can justify stealing a shirt from Gap because it was overpriced and used child labour
Reaction formation = an opposite and exaggerated expression of the behaviour associated with the unacceptable impulse occurs
A mom represses her resentful feelings towards her child and becomes over protective
The psychosexual stages of personality development:
Five stages, each focused on a specific pleasure sensitive are of the body
Adult personality is a function of progressing through these stages
Fixation = arrested development where instinct becomes focused on a particular area
The psychosexual stages
Oral stage: 0-2 years
Weaning
Fixation = self indulgence, dependency
Anal stage: 2-3 years
Toilet training
Fixation = compulsive cleanliness and rigid rules or messy and dominant
Phallic stage: 4-6 years
oedipus/electra complex
Move from sexual attachment to opposite sex-parent to identification with same sex parent
Latency stage: 7 years-puberty
Period of dormant sexuality
Genital stage: puberty onwards
Formation of social and sexual relationships
Evaluating freud’s theory:
Inadequate evidence
Small limited sample
Cannot be directly tested by scientific methods
Unconscious processes
Nonconscious processes have been demonstrated
Psychosexual stages
Concept of childhood sexuality rejected
The real issue is the importance of early experiences and emotional attachment
The humanistic perspective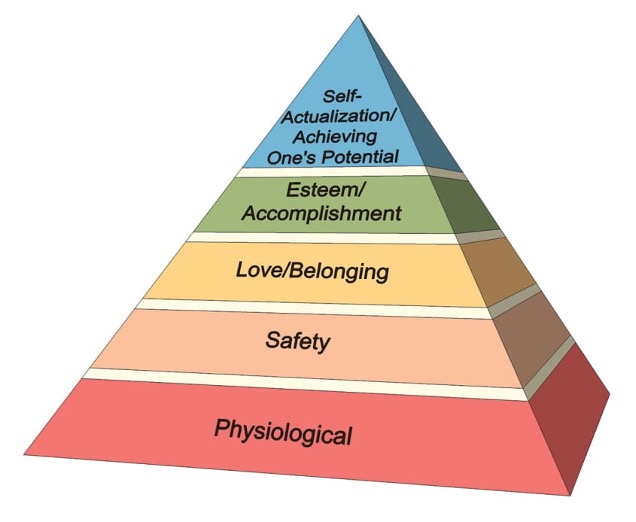
Abraham maslow
Hierarchy of needs
Self-actualization = highest human need to fulfil special potential
Studied healthy, well adjusted people
Led to study of positive psychology
Carl Rogers
Self concept = consistent pattern of self perception describing how we see ourselves
Unconditional positive regard= acceptance without terms or conditions
Client centred therapy = worked on therapeutic atmosphere so client could it aside conditions of worth
Evaluating the humanistic perspective
Not scientific, hard to test
Simplistic view of human nature
Contributions to therapeutic atmosphere
The trait perspective
Personality traits describes an individual’s durable pattern of thinking, feeling and behaving
What is the minimum number of traits that are necessary to describe anyone’s personality?
Use the statistical tool of factor analysis
Hans eysenck
Identified three superfactors or traits that can vary from high to low
Extraversion
High = sociable, outgoing, risk taking
Low = shy, reserved, cautious
Neuroticism
high = emotionally worried, moody, temperamental
Low = emotionally stable, calm, even tempered
Psychoticism
High = impulsive, socially deviant, creative
Low = self controlled, disciplined
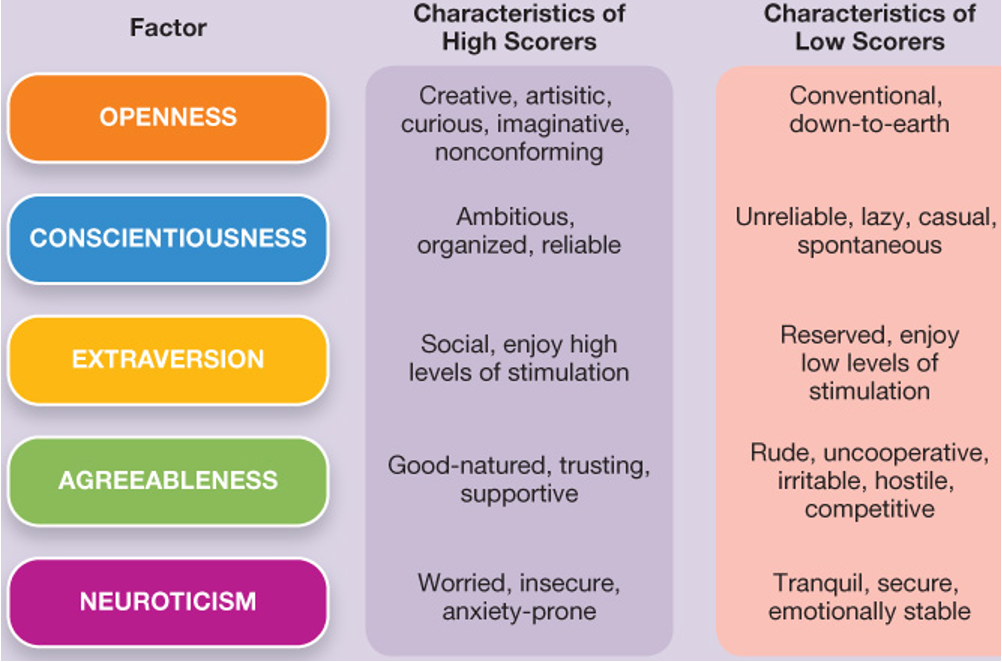
Five factor model

Evaluating the trait perspective: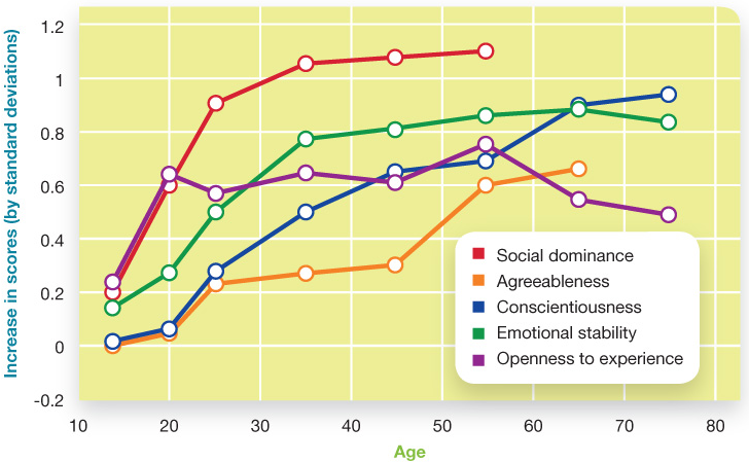
Considerable stability in our personalities
Genetic component to personality
Oversimplify personality
Describes personality but doesn't explain it
The situationist perspective
Situationsim = the view that behaviour is governed by the situation rather than internal traits
Behaviourists would agree - Skinner, Thorndike
Thus, personality is a description of response tendencies that occur to specific environmental stimuli

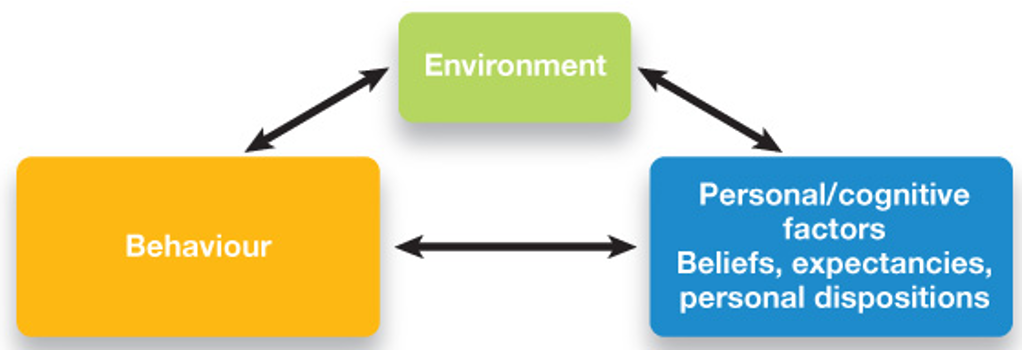
The interactionist perspective
Interactionism = the view that behaviour is governed the interaction between inner traits and the situation
Bandura’s idea of reciprocal determinism = bidirectional links between environment, behaviour and internal mental events
Personality Assessment
Personality inventories = questionnaires used to assess various aspects of personality
Need to worry about social desirability bias = when participant answers in such a way to make themselves look good rather than truthfully
Include questions to look for this
Two ways to develop items on personality inventories:
Rational approach
Based on theoretical conception of the trait
Items seem relevant to the trait
Eg: NEO-PI-R
Evaluates traits compromising three of five superfactors: Neuroticism, extraversion and openness
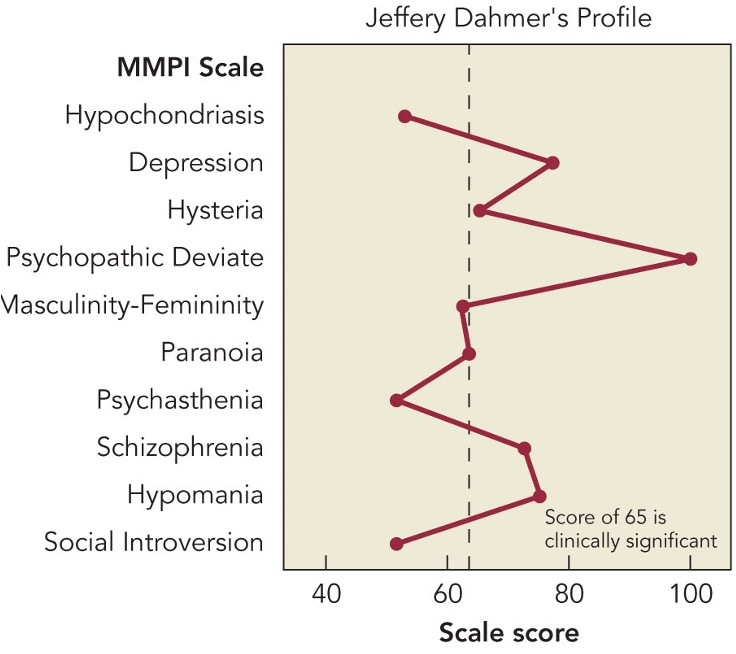
Empirical approach
Based on responses by ‘normals’ and psychiatric patients - items answered differently by these groups
Eg: MMPI-2
Example Jeffrey Dahmer MMPI-2 profile
Protective tests = personality assessment in which the participant interprets ambiguous stimuli as a way to reveal unconscious content
Interpretation = ‘projection’ of inner needs, feelings, ways of viewing the world
Problem :
Different examiners may have different interpretations
Two main types of projective tests:
Rorschach Inkblot test = shown inkblot and have to say what it looks like
Though to reveal underlying personality traits or conflicts
Thematic apperception test (TAT) = show scene and have to create story
Biological foundations of personality
Many core dimensions of personality are influenced by genes
Study this using family studies
Are identical twins raised together more alike than fraternal twins raised together? YES
Suggests genetic component
Are identical twins raised together more alike than identical twins raised apart? NO
Suggests genetic component
Are adoptive siblings raised together more alike than two random people raised apart? NO
Suggest environmental influences are minimal
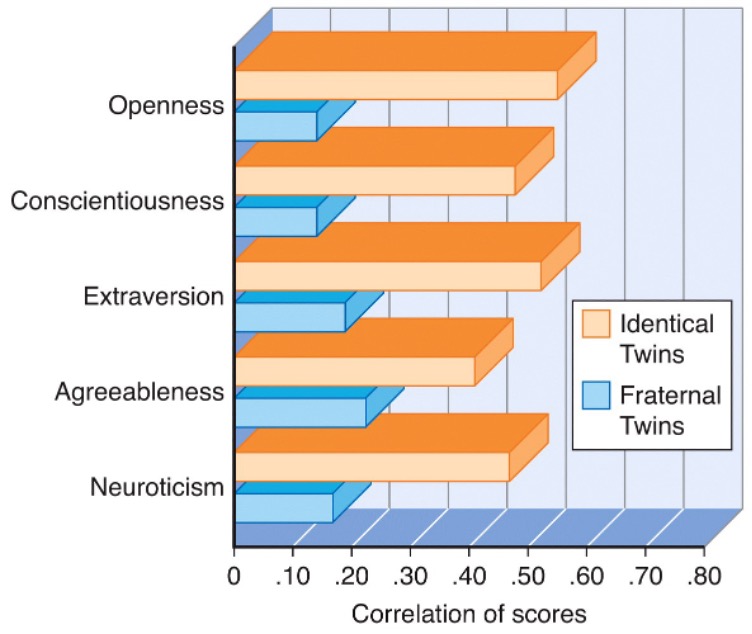
Similarity of pairs of identical and fraternal twins on the big five personality traits:
L
Personality and the brain:
Several brain areas involved
Amygdala - emotionality, fear and avoidance
Inhibited children may have am easily activated amygdala, causing feelings of fear and shyness
Several neurotransmitters involved
Levels of dopamine and serotonin linked with scores on dimensions of temperament
Differences in Personality
Gender differences in personality
Similarities outnumber differences!
Women tend to:
Asses others emotion smore accurately
Score higher on social and connectedness traits
Men tend to:
Exhibit more individuality and autonomy
Show more physical aggression
Challenges of exploring cultural differences in personality:
Translating measures of personality so the same question means the same thing to everyone
Different response styles in different cultures
In collectivist cultures, it is not socially acceptable to say highly positive things about yourself
Cultural differences in personality:
Collectivist cultures consider the needs of the group over that of the individual
Score higher on measures of agreeableness
Value harmony in interpersonal relationships
Describe self as part of a group
Cultural differences in personality:
Individualistic cultures value individual achievement and independence
Score higher on measures of extraversion and openness
Value privacy
Describe self using personal traits
Chapter 15
Overview:
What is abnormal?
Models of abnormal behaviour
Mood disorders
Anxiety disorder
Schizophrenia
Somatic symptom and related disorders
Dissociative disorders
Personality disorders’
What is abnormal?
A lot of grey area between what is normal and abnormal
Varies across individuals and cultures
When discussing psychological disorders, we should keep in mind:
Can we define disorders clearly enough so that we can know that we’re all referring to the same set of symptoms
How do we decide when a set of symptoms crosses the line and becomes a disorder that needs treatment
How can the label of a psychological diagnosis affect people
Abnormal psychology = the scientific study of psychological disorders
No single definition agreed upon by everyone
Most definitions refer to the four D’s:
Devance - thoughts or emotions that fall outside cultural norms
Danger - behaviour increases risk of injury or harm to self or others
Distress - intense negative emotional reaction that doesn’t match the situation
Dysfunction - behaviour interferes with individuals daily functioning
Diagnosing psychological disorders:
One reason to diagnose a disorder is to make decisions about the treatment
In order to treat a disorder, it helps to understand the cause of the psychological symptoms
Classifying psychological disorders:
The diagnostic and statistical manual : DSM-V
The most complete description of over 350 mental disorders and criteria for diagnosing each
Assumes psychological disorders are no different from a physical illness
Symptoms, diagnosis, prognosis
Diagnostic information is represented along 5 dimensions or axes that consider both the person and their life situation
Critiques of diagnosing with the DSM:
The DSM calls too many people ‘disordered’
The border between diagnoses or between disorder and normal, seems arbitrary
Decisions about what is a disorder seem to include value judgements
Is depression necessarily deviant?
Diagnostic labels direct how we view and interpret the world, telling us which behaviour and mental states to see as disordered
Models of Abnormal Behaviour
Today's leading models of abnormality:
Neuroscience model
Psychodynamic approaches
Cognitive behavioural approaches
Socio-cultural approaches
Developmental psychopathology approach
Neuroscience model:
Attributes abnormal functioning to structural or biochemical malfunctions in the brain
Genetic inheritance
Abnormal neurotransmitter levels
Viral infections
Hormones
Brain structure abnormalities
Psychodynamic approaches:
Attributes abnormal functioning to unconscious conflicts that are often rooted in childhood
Defence mechanisms
Fixations
Cognitive behavioural approaches
Attributes abnormal functioning to a mix of conditioning, modelling and cognitive processes
Behavioural perspective - conditioning processes
Classical and operant
Cognitive perspective - maladaptive thinking and beliefs
Selective perception, magnification and overgeneralization
Socio-cultural approaches :
Attributes abnormal functioning to societal, cultural, social, and family pressures or conflict
Relation between abnormal functioning and factors such as:
Widespread social change
Socio-economic class
Social networks and support
Family systems
Developmental psychopathology approach :
Attributes abnormal functioning to early risk factors combined with poor resilience throughout life stages
Risk factors = biological and environmental factors that contribute to problem outcomes
Resilience = the ability to recover from or avoid the serious effects of negative circumstances
Equifinality = children can start from different points and end up at the same outcome
Multifinality = children can start from the same point and end up at different outcomes
Mood Disorders
Two states of mood disorders:
Depression = low, sad state in which people feel overwhelmed
Most people with a mood disorder suffer only from depression
Major depressive disorder is more severe than dysthymic disorder
Mania = elated and frenzied state in which people feel full of energy
People with bipolar disorder or the less severe cyclothymic disorder also experience mania
Major depressive disorder (MDD)
Characterised by a depressed mood that is significantly disabling
Not caused by such factors as drugs or general medical condition
Bipolar Disorder
Dominant mood is depression alternating with periods of mania
Symptoms of MDD
Emotional – depressed mood
Motivational – loss of desire to do activities; lack of drive
Behavioural – less active and productive; may move and speak slowly
Cognitive – negative self-evaluation, self-blame, pessimism, guilt, difficulty concentrating, thoughts of suicide
Physical – fatigue, sleep and eating disturbances, headaches, dizziness, pain
Depression is everywhere :
Per year, 8% of Canadians are diagnosed with MDD
Women are twice as likely
Explanations for MDD:
Genetics:
DNA linkage analysis reveals depressed gene areas
Twin studies:
The brain:
Brain activity is diminished in depression and increased in mania
Brain structure: smaller frontal lobes in depression ad fewer axons in bipolar disorder
Brain chemistry
More norepinephrine (arousing) in mania, less in depression
Reduced serotonin in depression
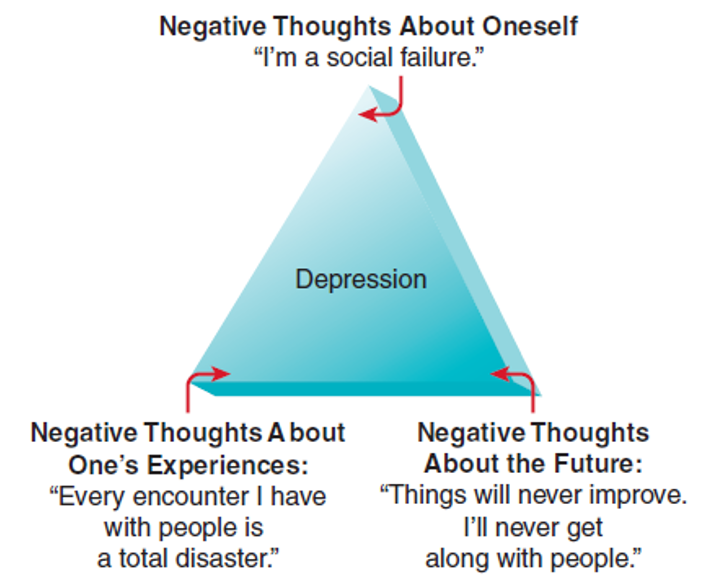
Cognitive-behavioural theorists:
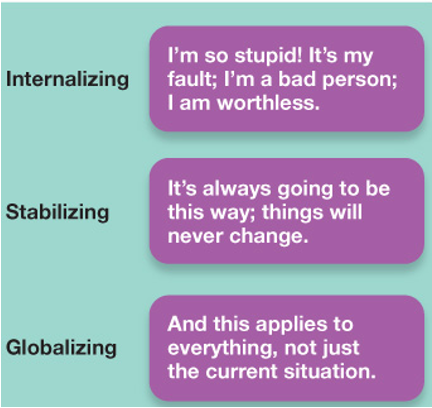
Learned helplessness
Attribution-helplessness theory
Internal + stable + global = depression
Negative thinking and/or dysfunctional attitudes
Magnification, overgeneralization
Automatic thoughts
The cognitive triad
Bipolar disorders:
Involves experiencing repeated periods of two polar opposite moods : depression and mania
Typical pattern is 3-7 weeks of depression followed by 3-7 days of mania
Affects roughly 2% of all adults
Symptoms of mania :
Emotional - powerful highs
Motivational - seeks excitement and companionship
Behavioural - may move and speak quickly
Cognitive - poor judgement, optimism, grandiosity (cannot see the difference between what we can and can't do)
Physical - energetic, requires little sleep
Explanations for bipolar disorder:
Genetics :
Gene abnormalities
Irregularities in ios that allow neurons to communicate (sodium potassium pump not working)
Other causes :
Stress + biological predisposition
Life events - striving, failures
Suicide
3500 suicides every year in Canada, 100x more attempts
2nd most frequent cause of death among high school and college students
Women 3x more attempts than men
Men 3x more success than women (choose more lethal methods than females)
Warning signs
80% of people that attempted to commit have told someone before hand
Verbal or behavioural threat
Detailed plan
Previous attempts
Anxiety disorders
Anxiety disorders = a category of disorders involving fear or nervousness that is out of proportion to the situation and is maladaptive
Six types:
Generalised anxiety disorder
Social anxiety disorder
Phobias
Panic disorder
Obsessive compulsive disorder
Post traumatic stress disorder
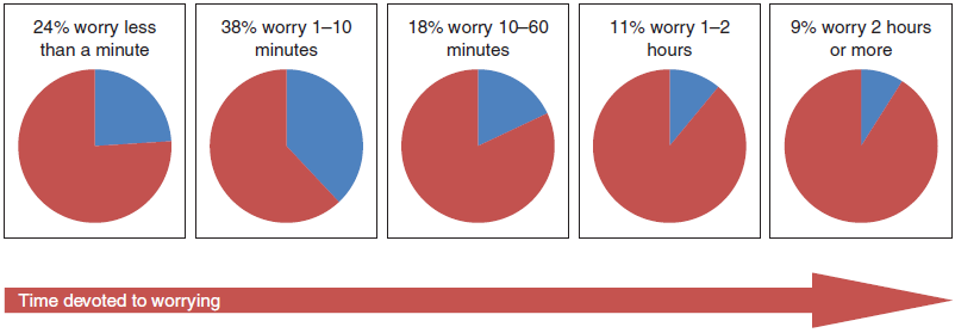
Generalised anxiety disorders
Feeling worried or anxious most of the time
Free-floating anxiety not attached to any subject
Constant worry interferes with ability to concentrate, sleep and eat
Feels restless, edgy and easily tired
Explanations for generalised anxiety disorder:
Cognitive- behavioural theorists:
Assumption that one is in danger
Intolerance of uncertainty theory - unwilling to accept negative events
Neuroscientists:
Malfunctioning GABA feedback system
Malfunctioning emotional brain circuit
Social anxiety disorder:
Severe, persistent fear of embarrassment in social situations
Fear of talking in public, of functioning poorly in front of others
Affects more women than men, more poor people than wealthy people
Roughly 7% of the population will have it in any given year, 12% in their lifetime
Often begins in late childhood or adolescence
Explanation for social anxiety disorder:
Cognitive behavioural theorists:
Dysfunctional cognitions about social situations
Unrealistically high social standards
View oneself as socially unattractive and unskilled
Phobias
Strong, irrational fears of objects or situations
Most develop during childhood, adolescence or young adulthood
Affects roughly 8% of people in Canada in any year
uncontrollable , irrational, intense desire to avoid the object of the phobia
Seldom go away on their own
Can intensify over time
Explanations for phobias:
Classically conditioned fear
Avoidance behaviours are reinforced through operant conditioning
Modelling of fearful behaviour
10 most common phobias:
Spiders – arachnophobia
Heights – acrophobia
Public, social places – agoraphobia
Social situations – social phobia
Flying – aerophobia
Enclosed spaces – claustrophobia
Thunder – brontophobia
Germs – mysophobia
Cancer – carcinophobia
Death – necrophobia
Panic disorder:
Anxiety response occurs suddenly, unpredictably and is very intense
Many minutes of intense dread or terror
Chest mains, choking, numbness
A feeling of need to escape
As a result, the person lives in fear of the next attack and changes their behaviour to avoid panic attacks
Agoraphobia
Explanations for panic disorder:
Malfunctioning brain circuit and excess norepinephrine
Misinterpretation of bodily sensations
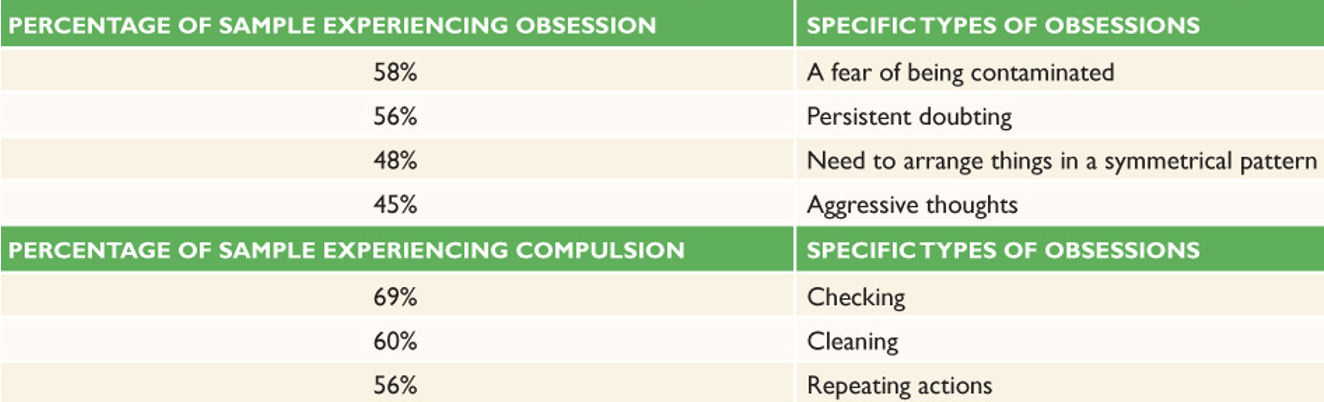
Obsessive-compulsive disorder (OCD)
An anxiety disorder in which individuals are plagued by unwanted repetitive thoughts and tend to engage in repetitive behaviours
Obsessions = cognitive component
Repetitive and unwelcome thoughts
Compulsions = behavioural component
Repetitive behavioural response as an attempt to ease the anxiety from the bad thoughts
Percentage of OCD clients reporting obsessions and compulsions:
Explanations for OCD:
Cognitive behavioural theorists:
Learning that compulsive behaviour relieves distress
Neuroscientists:
Low serotonin activity
Overactive orbitofrontal cortex and caudate nuclei
Cingulate cortex and hypothalamus activate the OCD impulses
Amygdala drives the fear and anxiety components of the OCD response
Post-traumatic stress disorder (PTSD)
Persistent depression and anxiety after a traumatic event
Hyperalertness, easily startled, sleep disturbances, guilt, anxiety, depression, difficulty with concentration
Lasts more than a month, may begin shortly after or years after the event
Acute stress disorder (ASD) = lasts less than a month and begins within 4 weeks of the event
80% of ASD cases develop into PTSD
Explanations for PTSD:
Biological factors
Increased cortisol and norepinephrine
Damaged hippocampus, amygdala
Personality
Perceive negative events as beyond their control
Negative childhood experiences
Poverty, family member with psychological disorder, trauma, parents divorce prior to 10 years
Weak social support
Schizophrenia
Schizophrenia = split mind
A mental disorder characterised by disorganised thought, lack of contact with reality, and sometimes hallucinations
Most characteristic symptoms:
Hallucinations = alterations in perception
Delusions = beliefs that are not based on reality
Disorganised behaviour = ‘all over the place’ to the extent that completing a task is difficult (eg: basic hygiene, cooking, shopping, going places, etc…)
Loose associations or derailment = rapid shifts in topic
Categories of symptoms of schizophrenia:
Positive symptoms: presence of problem behaviours; pathological excess in behaviour
Delusions, disorganised thinking and speech, hallucinations, inappropriate affect
Negative symptoms: absence of healthy behaviours: pathological deficits in behaviour
Lack of speech, flat affect, loss of volition, social withdrawal
Cognitive symptoms: impairment in cognitive functions
Problems with memory, executive function, working memory, intelligence
Psychomotor symptoms: abnormal movements
Awkward movements, odd gestures, catatonia
Onset and development:
Onset: typically, schizophrenic symptoms appear at the end of adolescence and in early adulthood, later for women than for men
Prevalence: roughly 1 out of every 100 people develop schizophrenia, equal men and women
Explanations for schizophrenia:
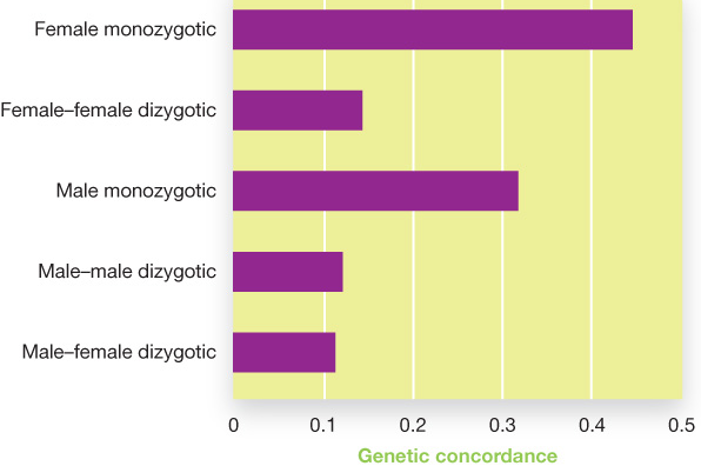
Genetics:
The more genetic similarity an individual has to a person with schizophrenia, the more likely that they will also develop the disorder
Likely a complex genetic combination, not a single gene
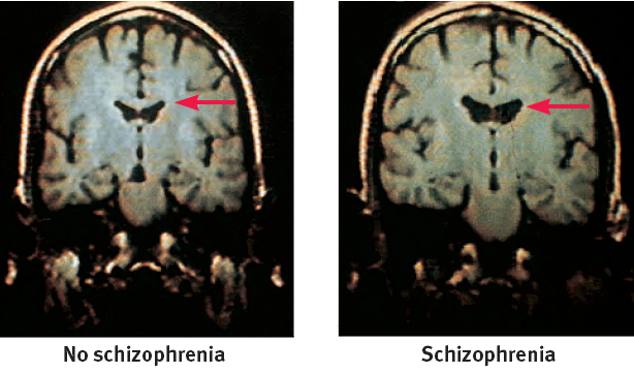
Abnormal brain structure:
Smaller temporal lobes and frontal lobes
Structural abnormalities of the hippocampus, amygdala and thalamus
Cerebral ventricles 20-30% larger in schizophrenics
Biochemical abnormalities:
Too many dopamines receptors help to explain paranoia and hallucinations
Antipsychotic drugs decrease dopamine activity and alleviate symptoms of schizophrenia
Abnormal glutamate and serotonin activity may also play a role
Somatic Symptom and Related Disorders
Somatic symptom and related disorders:
Excessive thought, feelings, and behaviours related to somatic symptoms
Experience genuine symptoms and repeated medical examinations/procedures/treatments, yet no medical explanation for their symptoms
Five types of somatic symptom and related disorders:
Somatic symptom disorder, illness anxiety disorder, conversion disorder, psychological factors affecting other medical conditions, and factitious disorder
Somatic symptom disorder:
Three criteria
One or more somatic symptoms that cause distress and significant disruption in daily life
Symptoms usually include pain, gastrointestinal symptoms, sexual symptoms, and neurological symptoms
Excessive health-related anxiety and time/energy devoted to somatic complaint
Concern has lasted over 6 months
Illness anxiety disorder:
The individual is preoccupied with having a serious disease despite lack of somatic symptoms
Excessive care-seeking for over 6 months
Excessive illness behaviours
Defining feature here is minimal or no symptoms
With symptoms, this would be somatic symptom disorder
Conversion disorder:
The development of sudden symptoms suggestive of neurological damage, yet perfectly healthy
Blindness, paralysis, seizures, loss of feeling
Individual is unconcerned with their symptoms
Onset usually following extreme stress and may last for weeks
Extremely rare, 5 in every 1000 people
Different from malingering – lie about symptoms to avoid an unwanted responsibility
Psychological factors affecting other medical conditions:
When psychological factors adversely affect a documented medical condition
May worsen an existing medical condition or create a new health risk
Factitious disorder:
When an individual purposely assumes physical or psychological symptoms in order to adopt the patient role
May lie about symptoms or take steps to make themselves ill or cause bodily harm
Factitious disorder imposed on another:
When one person deliberately harms another and then presents the harmed one to the doctor and presents themselves as the caregiver (usually parent-child)
Explanations for somatic symptom and related disorders:
Behaviourists – classical conditioning of fears; modelling
Cognitive theorists – misinterpret bodily cues; very sensitive to bodily cues
Socio-cultural theorists – many non-Western cultures transform personal distress into somatic complaints/symptoms
Dissociative Disorders
Dissociation refers to a separation of conscious awareness from thoughts, memory, bodily sensation, feelings, or even from identity
It can serve as a psychological escape from an overwhelmingly stressful situation
A dissociative disorder refers to dysfunction and distress caused by chronic and severe dissociation; three types:
Dissociative amnesia, depersonalization/derealization disorder, dissociative identity disorder
Dissociative amnesia:
Loss of memory with no known physical cause; inability to recall selected memories
Depersonalization/derealization disorder:
A strong feeling of disconnection from one’s regular identity and awareness; usually triggered by stress
Dissociative identity disorder (DID):
Development of separate personalities; formerly called ‘multiple personality disorder’
Each identity is unique
Not in consciousness at the same time
May or may not know about each other
One identity may be protector, another a child
Explanations for dissociative disorders:
Psychoanalytic perspective: repression
Cognitive perspective: coping with abuse
Learning perspective: dissociation pays
Social influence: therapists encourage
Biological approach: smaller hippocampus and amygdala
Personality Disorders
A stable, ingrained, inflexible, and maladaptive way of thinking, feeling, and behaving
Ten specific personality disorders fall into one of three clusters of disorders:
Dramatic & impulsive behaviours *focus here*
*Antisocial*, *borderline*, histrionic, and narcissistic personality disorders
Anxiety & fearfulness
Avoidant, dependent, and obsessive-compulsive personality disorders
Odd & eccentric behaviours
Paranoid, schizoid, and schizotypal personality disorders
Antisocial personality disorder
3 : 1 male – female ratio
Lack a conscience & empathy
Fail to respond to punishment
Disregard for others’ rights or preferences
May be charming & manipulative
Diagnosis – at least 18 years of age with antisocial behaviour before 15
Antisocial personality disorder does not automatically mean criminality!
Many career criminals show empathy and selflessness with family and friends
Many people with APD do not commit crimes
Explanations for antisocial personality disorder:
Behavioural theories:
Modelling – parents have antisocial personalities
Operant conditioning – parents reward the wrong behaviour
Biological factors:
Lower serotonin – linked with impulsivity and aggression
Deficient functioning of the frontal lobes – linked with poor planning, inferior judgments, low empathy
Less anxiety – may be why they don’t learn from negative consequences
Borderline personality disorder:
Intense extremes between positive and negative emotions
Unstable sense of self
Impulsivity and volatility
Difficulty with social relationships
Explanations for borderline personality disorder
Biosocial theory- child has difficulty identifying and controlling emotions, and the emotions are punished or disregarded
Chapter 16
Overview
The nature of therapy
Biological treatments
Psychodynamic therapies
Behaviour therapies
Cognitive-behavioural therapies
Humanistic and existential therapies
Formats of therapy
Does therapy work?
The nature of therapy
Goals of treatment:
To help change maladaptive thoughts, feelings, and/or behaviours
Three features of all therapies:
A sufferer who seeks help
A trained, socially accepted healer
A series of contacts with the goal of changing maladaptive thoughts, feeling, and/or behaviours
Types of treatment:
Psychotherapy
An interactive experience with a trained professional, working understand and changing behaviour, thinking, relationships and emotions
Biological therapy
The use of medications and other procedures acting directly on the body to reduce the symptoms of mental disorders
Who seeks therapy?
30% of North Americans will seek professional counselling at some point in their life
¾ of them will seek help for anxiety or depression
⅔ of them will be women, ⅓ will be men
However, ⅔ of people who would seek help don't, why not?
Stigma about mental illness
Lack of confidence that treatment will help
Who are clinicians?
Clinical psychologists
Psychiatrists
Counsellors
Social workers
Where is the treatment conducted?
Public institutions, such as hospitals and clinics, schools, and private offices
Most people are treated as outpatients
Deinstitutionalization movement began in 1960s
People with severe psychological disorders often face a cycle of in and out of the hospital → the revolving door
Canadian Mental Health Act
Outlines patient rights and conditions for involuntary for admittance to hospitals
Biological Treatments
Interventions in the brain and body can affect mood and behaviour
Biological treatments alter the brain’s functioning by changing its chemistry with medications, or affectug=ng its circuitry with electrical or magnetic impulses or surgery
Drug therapy
Electroconvulsive therapy
Psychosurgery
Drug Therapy:
Psychotropic drug = drug that acts primarily on the brain
Most prescriptions for anti-anxiety drugs, antidepressants, mood stabilisers and antipsychotics
Anti-anxiety drugs:
Valium, Xanax, Prozac
Designed to reduce anxiety without affecting alertness or concentration
Slows down excitatory synaptic activity
Side effects: drowsiness, lethargy, dependance
Newer drugs: enhance inhibitory GABA, fewer side effects
Antidepressants
Elavil, Nardil, prozac, paxil, zoloft
Designed to improve mood and reduce other symptoms of depression
Work by increasing levels of serotonin, norepinephrine and dopamine
Three types of antidepressants:
MAO inhibitors, tricyclics, and selective serotonin reuptake inhibitors (SSRIs)
Mood stabilisers:
Lithonate (lithium)
Standard treatment for bipolar disorder from 1950’s to 1980’s
Many serious side effects
Designed to improve intense shifts in mood from on extreme state to another
Antipsychotics = major tranquilizers
Thorazine, clozaril, risperdal
Designed to reduce symptoms of schizophrenia, especially ‘positive’ symptoms (delusions, hallucinations)
Work by decreasing the action of dopamine
Side effects: obesity, diabetes, movement problems
Tardive dyskinesia = odd facial, tongue and body movements
Keep in mind that drug therapies
Do not cure the disorder
Do not r=teach the client coping and problem solving skills to deal with stress
Can bring symptoms under control and other therapeutic techniques can be incorporated
Electroconvulsive therapy (ECT):
Used to treat depression by sending an electrical current through the brain, producing a brain seizure
Effects can be immediate
60-70% improve
Can cause memory problems
Procedure:
Patient given sedative and muscle relaxant
Placed on well padded mattress
Shocked less than 1 second, causing seizures of CNS
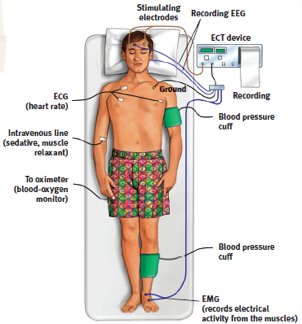
Transcranial magnetic stimulation
A noninvasive procedure used to treat depression
Stimulates a focal area of the frontal lobes with powerful magnetic field

Vagus nerve stimulation
An implanted pulse generator sends electrical signals to a specific region of the brain
Helps reduce depression in many people
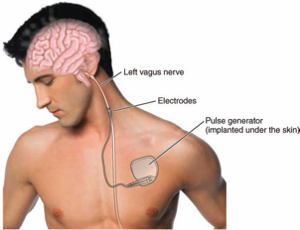
Psychosurgery:
Procedures that remove or destroy parts of the brain
Least used of biomedical procedures
Lobotomy
Destroy nerve tracts to frontal lobes
Treatment for schizophrenia in the 1930’s and 1940s
Strengths
Biological Treatments often work when other treatments have failed
Research offers promising options
Criticism
Undesirable side effects
Ignores environmental effects
Psychodynamic therapies
Several types of psychodynamic therapies:
psychoanalysis , short term psychodynamic therapy, relational psychoanalytic therapy
Goal is to help patients release tension of repression and resolve unconscious inner conflicts
Psychodynamic techniques:
Free association
Uncensored, verbal reports of thoughts, feelings or images that enter awareness
Dream interpretation
Therapist helps client understand the symbolic meaning of their dreams
Resistance
Defensive manoeuvres that hinder the process of therapy are signs that sensitive material is being approached
Transference
When the client shifts feelings for figures from childhood on to the therapist
How do psychodynamic therapies help clients?
Catharsis - reliving of past repressed feelings to resolve conflicts
Must be accompanied by intellectual insight
Very time consuming
Working through - repeatedly examining an issue to improve insight
Strengths:
First to suggest psychological instead of biological treatment
Ie, traumatic childhood events can affect later psychological health
Led to man other psychological treatments
Criticisms:
No empirical support for effectiveness of therapy
Behaviour Therapies
Behavioural therapies focus on behaviour
Abnormal behaviours are learned
Maladaptive behaviours can be unlearned though:
Classical conditioning
Operant conditioning
Modelling
Behavioural therapy is often effective for treating phobias and anxiety issues
Classical conditioning techniques:
Exposure approach:
Treat phobias through exposure to feared CS (stimulus) without being allowed to escape
Eliminate anxiety through extinction
Two types:
Flooding:
Extensive exposure to the feared CS until there is no more fear
Systematic desensitisation:
Progressing through a fear hierarchy while practising at each step
Example of a fear hierarchy for systematic desensitisation
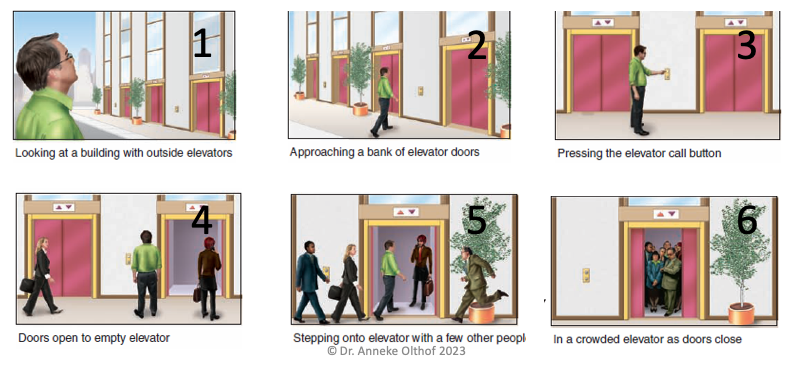
Aversion therapy:
A person learns to associate the stimulus that they desire (alcohol, drugs, source of sexual fetish, etc.) with something aversive
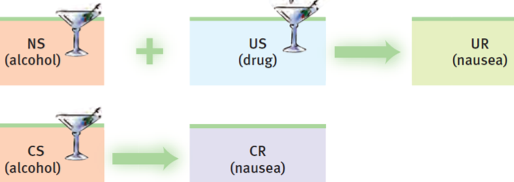
Operant conditioning treatments:
Use positive reinforcement, extinction, negative reinforcement or punishment
Attempt to increase or decrease specific behaviours
Works best in ‘closed systems’ = institutions and schools
Token economies =
System for strengthening desired behaviours through application of positive reinforcement
Tokens given for desirable behaviours
Tokens exchanged for tangible reinforces
Strengths:
A lot of empirical evidence
Effective for many problems
Criticism
Change may not always be long-lasting
Not effective for some disorders
The distress is non-specific (generalised anxiety disorder) schizophrenia
Cognitive-behavioural therapies
Therapy that works on problem thoughts and behaviours
Behavioural - work on gaining skills they may be lacking
Cognitive - work on building more functional thinking habits
Three kinds of therapy :
Ellis’ rational-emotive behavioural therapy
Beck’s cognitive therapy
Second-wave cognitive behavioural therapies
Ellis’ Rational-Emotive Therapy:
Goal is to identify irrational assumptions that lead to disordered emotional and behavioural responses
Point out irrational assumptions
Model the use of alternative assumptions
Uses cognitive restructuring
Effective for anxiety and assertiveness problems

Beck’s Cognitive Therapy:
Widely used for depression
About as effective as drug therapy (⅔ improve)
Also used for panic disorder and social anxiety disorder
Therapist helps client identify negative thoughts and perceptions, and guides them to apply alternative ways of thinking
Second-wave cognitive behavioural therapies:
Recognize problematic thoughts as just thoughts
Learn to accept thoughts rather than try to eliminate them
Mindfulness-based cognitive therapy
Used for treating generalised anxiety disorder
Strengths:
Well supported by research
Good at treating depression, social anxiety disorder, generalised anxiety disorder, panic disorder, sexual dysfunctions and other disorders
Criticism:
Role of cognition unclear (cause or effect?)
Unclear whether cognitive, behavioural, or a combination of both are effective
Humanistic and Existential therapies
Humanists - we are all born with the tools to fulfil our potential
Existentialists - accept responsibility for or lives and choices
Gestalt therapy - guide clients toward self-acceptance by challenging and frustrating them
Rogers' client centred therapy:
How to create a therapeutic environment in which clients can see themselves honestly and with acceptance?
Three important therapist attributes:
•Unconditional positive regard
Total acceptance of client
•Accurate empathy
Willingness and ability to view the world through client’s eyes
Genuineness
Sincere communication
Gestalt Therapy:
Goal is to bring feelings, wishes, and thoughts into immediate awareness
Awareness makes client ‘whole’ again
Methods:
Often carried out in
Uses role-playing
More active and dramatic approaches the client-centred
Strengths:
Appealing to clinicians
Emphasises positive human qualities
Criticism
Difficult to research; little research done
Formats of therapy
Individual therapy - one on one with therapist and client
Group therapy - therapist meets with several clients with similar problems simultaneously
Hope that client benefits from hearing others’ pov
Group therapy, family therapy, couples therapy
Self help groups - people with similar problems meet for support without guidance from clinician
Does therapy work?
Empirically supported treatments should be used
Treatments that have been tested and evaluated
Several problems:
Spontaneous remission
Sometimes people get better with no treatment at all
Difficulties with psychotherapy research:
Ethics of having a control group
Many variables not controlled
Therapist-client interactions varied
Measuring therapeutic effects
Who measures outcomes
Empirically supported treatments come from psychotherapy research that involves randomised clinical trials – APA guidelines:
Random assignments of clients to experimental or control group
Treatment procedures are standardised
Double-blind procedure minimises researcher bias and placebo effects
Some behavioural measures to assess improvement
Need follow-up data
Is therapy generally effective?
Yes! More effective than no treatment or placebo
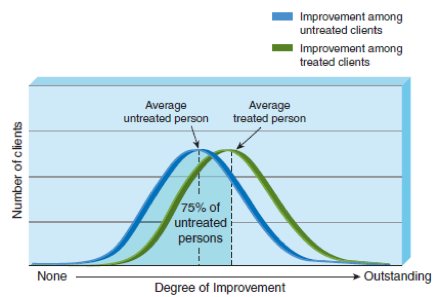
Are particular therapies effective for particular problems?
YES!
Behavioural = phobias
Cognitive-behavioural = social anxiety disorder, generalised anxiety disorder, panic disorder, and depression
Drug therapy = schizophrenia and bipolar disorder
What factors affect the effectiveness of a treatment?
–Client variables:
•Openness to therapy
•Ability to understand own internal states
•Problem needs to ‘fit’ with therapy being used
Therapist variables:
Empathy, genuineness, caring, trust, acceptance
•Eclecticism – willingness to combine treatments for the benefit of a client
Techniques:
Need appropriate technique for client and situation
DONEEEE