Adult Health Exam 3
Hematological Disorders
Hematological Disorders
Anemia:
Patho:
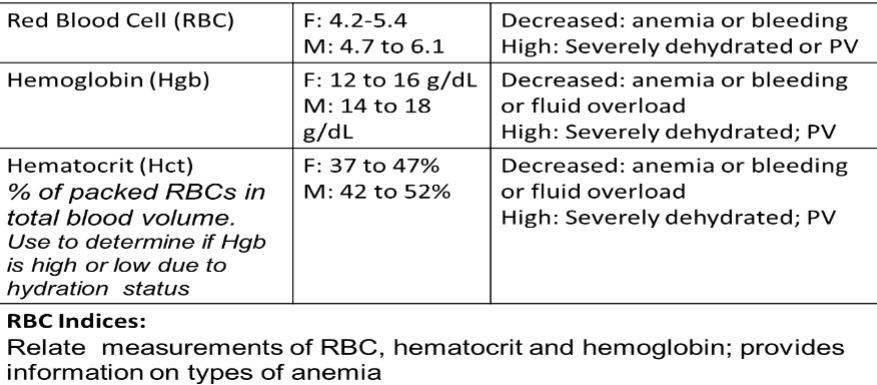
Reduction in RBCs, Hgb, and/or Hct
Clinical Sign - NOT specific disease
Classifications:
Blood loss
Hemolytic
Impaired RBC production
Types:
Iron Deficiency (microcytic)
Blood loss, poor nutrition
Hemolytic
Immune, mechanical trauma, sickle cell
Megaloblastic (macrocytic)
Vitamin B12 deficiency
Pernicious anemia - lack intrinsic factor
Folic acid deficiency
Aplastic anemia (Bone marrow depression)
Chronic disease anemias
Ex: chronic renal failure
CM:
Yellowing of eyes
Skin - Pale, Cold, Yellowing
SOB
Weakness
Changed stool color
Fatigue
Dizziness
Fainting
Low BP
Palpitations
Tachycardia
Chest pain, Heart Attack
Spleen enlargement
Red = Severe anemia
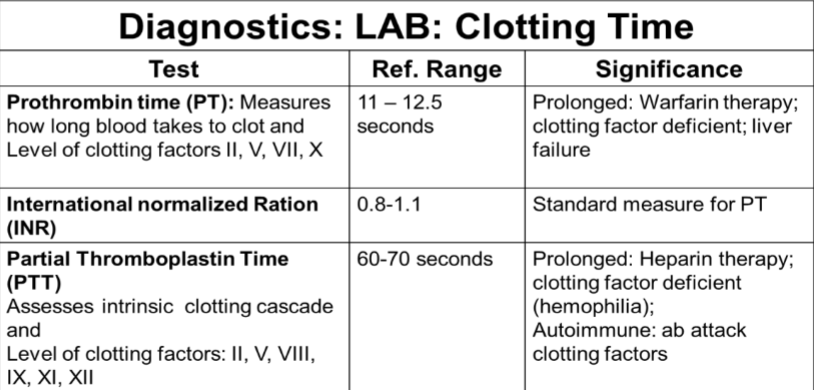
Diagnostics:
CBC with differential and RBC indices
Reticulocyte count
Iron studies
Coomb’s test (Abs on RBCs)
Bone marrow aspiration
Assessment:
Gather history, diet, meds, menstrual flow, symptoms
Assess for:
Fatigue, pallor jaundice, cyanosis, bleeding, dry skin
Mouth ulcers or fissures, smooth tongue (glossitis)
Lymph nodes, resp rate and rhythm, tachycardia
VS, O2 sat, review labs
Treatment:
Determine underlying cause
Iron deficiency
Mild: oral ferrous sulfate
Vit C enhances absorption, take between meals
Hgb should rise 2g in 4 weeks
Severe: IV or IM iron dextran
Z track method
Vitamin B
Diet, oral supplements, injections
Blood loss
Stop bleeding, transfusions
Immune
Immunosuppressive therapies, transfusions, Bone marrow transplant
Chronic Disease - CKD, Cancers
Erythropoietin (Procrit/Epogen) injections SQ weekly
Nursing Diagnosis:
Activity intolerance
Fatigue
Altered tissue perfusion
Impaired gas exchange
Anxiety
Impaired comfort
Risk for bleeding
Risk for injury
Impaired memory
Sickle Cell Anemia
Patho: Genetic disorder of hemoglobin (HgbS) distorting RBC shape (sickle) in response to decreased O2 Hgb cannot carry oxygen well Vaso-occlusive events
CM: Pain Severity varies, and periodic crises Precipitating Conditions:
Complications:
|
Nursing Interventions: Pain management Oxygen Hydration Body positioning (bending = clumping/constriction) Check circulation of peripheral extremeties Assess signs of central claudication
Keep Pt warm Admin IVF or PO fluids Prevent infection Blood transfusion Hydroxyurea (reduces sickling) Teaching:
Nursing Diagnosis: Acute pain (lack of perfusion) Ineffective peripheral tissue perfusion Deficient fluid volume Activity intolerance Risk for decreased cardiac tissue perf Risk for infection Risk for ineffective cerebral tissue perf |
Primary Polycythemia Vera
Patho: Loss of cellular regulation; proliferation of RBCs, WBCs, and platelets Blood is hyperviscous
CM: HTN HAs Dizziness Purple/gray color Itching Dyspnea Complications: bc thick blood
Diagnosis: |
Treatment: Repeated Apheresis 2-5 times/week Medications
Nursing Interventions: Prevent clots Hydration (3 L/day) Stop smoking Promote venous return Elevate feet Avoid tight clothing Support hose Thrombocytopenia precautions Use electric razor, soft toothbrush Neutropenic precautions Contact Dr at first sign of inf or occlusion Exercise slowly
Interdisciplinary
Nursing Diagnosis: Ineffective protection Risk for bleeding Risk ineffective tissue perfusion |
Myelodysplastic Syndrome (MDS)
Patho: Precancerous state – 30% develop acute leukemia Abnormal cell formation in bone marrow; destroyed by body after release; decrease in all blood cell types (pancytopenia) Risk Factors:
Diagnosis: Cytogenetic testing Peripheral blood smears Treatment: Supportive care Blood/platelet transfusions; Epogen (Procrit) injections Allogeneic hematopoietic stem cell transplant only curative treatment Immunomodulatory agents |
Platelet Disorders
Patho: Local bleeding - petechiae Easier to control than clotting factor disorders Reasons: Normal platelets = 150k-400k/mm3
Thrombocytopenia:
Thrombocytosis:
Idiopathic Thrombocytopenic Purpura (ITP): Autoimmune disorder Pts make Abs against own platelets; macrophages destroy
Diagnosis: serial low platelets & Bone marrow Bx Treatment:
Thrombotic Thrombocytopenic Purpura (TTP): Autoimmune disorder Platelets clump together abnormally in capillaries and too few available in circulation
Tissue becomes ischemic → may lead to kidney failure, MI, CVA
Treatment:
|
Clotting Factor Disorders
Patho: Occurs deeper in the body
Disorders:
Hemophilia: Genetic disorder
Type A
Type B
CM:
Joint problems from repeated episodes of bleeding is most common complication Hemophilia Diagnosis: Prolonged PTT Nursing Interventions: Minimize trauma and other causes of bleeding
Assess for s/s of bleeding Interdisciplinary
|
Leukemia
Patho: Acute - sudden onset abnormal blood cells Chronic - abnormal cells replicate slowly Classifications:
Types:
Risk Factors:
CM: Fever Night sweats Easy bleeding and bruising Purplish patches or spots on skin Freq infections Fatigue Loss of appetite Weight loss Swelling Easy SOB Spleen and/or liver enlargement Musc weakness Bone/joint pain or tenderness Treatment: Induction Therapy
Consolidation Therapy
Maintenance Therapy
Diagnosis: CBC
Bone Marrow Bx - Definitive test
Chromosome analysis Other x-rays, CT, MRI |
Lymphoma
Patho: CA of lymphocytes Two main types:
Hodgkins: Starts in single lymph node in neck, underarm, or chest Proceeds in orderly fashion to next Risk Factors:
Fatigue, anorexia, SOB “B” symptoms: sweats, fever, itching, weight loss Pain in node areas after alcohol intake Treatment
Non-Hodgkins: Lymphadenopathy in multiple sites Spread to other organs at diagnosis Risk Factors:
Treatment:
|
Multiple Myeloma
Patho: Overgrowth of plasma cells (PC) PC overproduce gamma globulin (gammopathy)
Produce excess cytokines
CM: Early
Late
Leads to progressive bone destruction, bleeding, kidney failure, immunosuppression, and death Diagnosis: Serum electrophoresis
Bone marrow
Xray
|
Treatment: Chemotherapy agents Bone marrow transplant INCURABLE Nursing Interventions: Care of immunocompromised Pain control Nursing Diagnosis: |
Nursing Care of Leukemia, Lymphoma, & Multiple Myeloma
Infection protection
Prophylactic drugs: antiviral, antibiotic, antifungals
Neutropenic precautions
Monitor labs daily
Monitor for early manifs of infection
Hygiene/skin care
Thrombocytopenia precautions
ENergy conservation
Teach self care
Psychosocial support
Neutropenic Precautions
Avoid crowds, children, ill people - or wear mask
Hand hygiene, Good personal hygiene, Mouth care
Avoid constipation
Use electric razor
Do not handle feces (pet, etc)
No fresh flowers or plants, No gardening
No invasive procedures
No sexual relations
Discuss food safety (no fresh fruits/vegs, raw meat, eggs, some cheeses)
Pt should have thermometer and know how to use
Who to notify and when (Report temp > 100.5 F, chills, or other s/s inf)
Weekly labs
Administer growth factor as directed
Thrombocytopenia precautions
Assess s/s bleeding (bruises, nose, gums, urine, stool, severe HAs)
Avoid IM/SQ/IV or invasive procedures
No aspirin/NSAID
Soft toothbrush, No flossing or dental procedures
Stool softeners & laxatives prevent straining
Hold pressure for 5 min on venipuncture sites
Teach signs of bleeding, When to notify provider
Safe environment, Avoid situations where falls may occur
Transfusion Reactions
Febrile Transfusion Reaction: Occurs most often in pt with anti-WBC Abs, which develop after multiple transfusions Chills Tachycardia Fever Hypotension Tachypnea Giving leukocyte reduced blood, WBC filters, or single-donor reduces risk Hemolytic Transfusion Reaction: Caused by blood type or Rh incompatibility Fever Chills DIC and circulatory collapse Other sx: Apprehension/sense impending doom HA Chest pain Low back pain Tachycardia Tachypnea Hypotension Hemoglobinuria Allergic Transfusion Reaction: Most commonly seen in pts with other allergies Urticaria Itching Bronchospasm Anaphylaxis Onset usually during or 24 hours after Bacterial Transfusion Reaction: Contaminated blood products (esp gram neg organisms) Tachycardia Hypotension Fever Chills Shock Rapid onset Transfusion-related Acute Lung Injury (TRALI): Most commonly when donor blood contains Abs against recipient's neutrophil Ags Dyspnea Hypoxia Rapid onset - within 6 hours Early detection key to survival Most pts need intubation Transfusion-associated Circulatory Overload (TACO): Occurs when transfused too quickly HTN Bounding pulse Distended jugular veins Dyspnea Restlessness Confusion Monitor I&O, infusing blood products more slowly, giving diuretics Transfusion-associated Graft-vs-Host Disease: Most commonly in immunosuppressed pt Thrombocytopenia Anorexia N/v Chronic hepatitis Weight loss Recurrent infection Sx usually within 1-2 weeks Acute Pain Transfusion Reaction: Severe chest pain Back pain Joint pain HTN Anxiety Redness of the head and neck During or shortly after transfusion |
Interventions for reactions during transfusion (Hemolytic, Allergic, and Bacterial)
Stop transfusion and remove blood tubing
Initiate RR
If no other IV access, flush with NS
DO NOT flush the contents of the transfusion tubing
Oxygen usually applied
Diphenhydramine IVP
Shock = fluid resuscitation and hemodynamic monitoring
Vasopressors might be needed
Endocrine Disorders
Pit Gland
Anterior Pituitary:
Adrenocorticotropic hormone (ACTH)
Follicle-stimulating hormone (FSH)
Growth hormone (GH)
Luteinizing hormone (LH): Prolactin
Thyroid-stimulating hormone (TSH)
Posterior Pituitary:
Antidiuretic hormone (ADH)
Oxytocin
Pit Tumors
Most common cause of pituitary disorders (95% benign)
Two types
Secretory - secrete too much hormone
Non-secretory - cause pressure
Posterior
ADH deficiency or excess
Anterior
Hypopituitarism
Deficiency of one or more anterior pituitary hormones results in metabolic problems and sexual dysfunction
Growth hormone stimulates liver
Hyperpituitarism
Hormone oversecretion
Neurologic symptoms may occur - compression of brain tissue (ICP)
Galactorrhea, amenorrhea, and infertility can result
Posterior Pituitary
Diabetes Insipidus: Deficiency of ADH
Cause
Manifestations
Treatment
Nursing (BOTH):
Syndrome of Inappropriate ADH: Excess ADH Water retained, delusional hyponatremia
Cause
Manifestations
Treat
|
Anterior Pituitary
Gigantism: GH hypersecretion before puberty Usually pituitary tumor Sweating, HA, Vision impairment, Weakness, Insomnia, Delayed puberty Dwarfism: GH hyposecretion Suppl GH can be administered for some types Acromegaly: GH hypersecretion after puberty Pituitary adenoma Slow changes over time
Skeletal changes cannot be reversed |
Gigantism/Acromegaly Diagnosis & Treatment:
Diagnosis:
H&P
Visual acuity/visual field tests - tumor can affect optic nerve
CT, MRI
Lab - Pituitary hormones
Measurement of target organ hormones - Thyroid for GH
Treatment:
Remove/destroy tumor
Surgery
Radiation therapy
Replacement hormones required after destruction
Medications
Inhibit production/release GH
Bromocriptine
Octreotide
Hypophysectomy
Complications:
Transient diabetes insipidus - d/t manipulation of posterior pituitary
CSF leakage - observe for clear fluid from nose or continuous post nasal drip, halo pattern, send fluid to lab
Visual disturbances, Post-op meningitis, Pneumocephalus (air in intracranial cavity), and SIADH
Increased risk of meningitis is they have CSF leak
Pre-Op Teaching
Avoid actions that increase intracranial pressure = CSF leakage
Vigorous coughing/blowing nose/sneezing
Sucking through straw
Bending over or straining during urination/defecation
Deep breathing techniques
Dressing and packing nose
Nurse will check visual acuity often - incr pressure on optic nerve
Need for accurate I&O
HOB at least 30 degrees (2 weeks) - elevation decreases ICP
Post-Op Interventions
Monitor
Neuro status including visual acuity and fields
Accurate I&O
Incision/packing (keep dry)
Potential complications
Mouth care every 2-4 hours
Cool vaporizer in room
Hormones and glucocorticoids as ordered
Discharge Instructions
Avoid blowing nose, coughing, sneezing, drinking with straw, or bending over/straining for 4 weeks
Report to surgeon
Hunger, thirst, body swelling, mood swings, increased urine output, weight loss (hormone deficiencies)
Continual postnasal drip, nasal drainage, or excessive swallowing (CSF leakage)
Pain with bending neck (meningitis)
Vision loss (damage to optic chiasm)
Use only nasal medications/rinse as prescribed
Keep follow-up appt 1 week after discharge
Adrenal Glands
Aldosterone
Regulates blood volume
Na reabsorption and K excretion in renal tubules
(AldosteRoNe=Reabsorption Na)
Cortisol
Increases BG level by inhibiting insulin secretion and promoting gluconeogenesis
Increases breakdown of proteins and lipids (gluconeogenesis)
Suppresses the inflam and immune response
Increases sensitivity of vasc musc to norepinephrine and angiotensin II (vasoconstriction)
Increases breakdown of bony matrix
Promotes bronchodilation
Addison’s Disease (Adrenal)
Patho: Decrease ACTH and adrenocortical steroids from adrenal cortex Cause
Low on 3 S’s
CM: Hyperpigmentation (incl gums) Fatigue Weakness Anorexia Weight loss Confusion Emotional lability Hypoglycemia Blood vol depletion Hyperkalemia & hyponatremia
Diagnosis: Early morning plasma cortisol provocation tests
Fasting blood glucose, electrolytes, BUN |
Treatment: Restore blood vol and prevent shock
Replace hormones (hydrocortisone, dexamethasone) Treat hyponatremia and hyperkalemia
Treat hypoglycemia
Administer fluids, Monitor I&O Monitor VS
Vasopressors for hypotension Determine cause Nursing Interventions: Monitor VS q1-4h Assess dysrhythmias or postural hypoTN Daily weight Promote fluid balance
Monitor lab values
Give cortisol and aldost replacement Acute Adrenal Crisis: Life threatening Sudden loss of cortisol and aldosterone Typically occurs after stressful event
Clinical Manifs
|
Cushing’s Syndrome (Adrenal)
Patho: Adrenocortical Excess Cause:
High on 3 S’s
CM: Acne Muscle wasting, Weakness Fragile skin Moon face Buffalo hump Enlarged trunk Virilization:
Retention of Na and water: HTN and HF Hyperglycemia Diagnosis: Three tests (2 must be abnormal for Dx)
|
Treatment: Surgery
Drug therapy: Adrenal enzyme inhibitors
Radiation is an option, but takes long to see effects Nursing Interventions: Decrease risk for injury Decrease risk of infection Prep pt for surgery Encourage rest and activity Promote skin integrity Improve body image Improve coping Monitor for potential complications Promote home and community care Nursing Diagnosis: |
Adrenal Tumor
Patho: Primary Aldosteronism CM: Profound decline in serum K levels (Hypokalemia) and hydrogen ions (Alkalosis) with increase in serum bicarb HTN common universal sign Muscle weakness Cramping Fatigue Excessive urine volume Polyuria Serum concentration - Polydipsia Treatment & Nursing: Surgical removal of adrenal tumor Treat HTN with spironolactone
Nursing
|
Thyroid:
Primary function: Controls cellular metabolic activity
Influences every major organ system
Thyroiditis
Patho: Inflammation, fibrosis, lymphocytic infiltration Types:
CM: Neck pain Swelling Dysphagia Treatment: |
Hyperthyroidism (thyrotoxicosis)
Patho: Thyrotoxicosis Excess thyroid hormones Women > men Graves Disease (most common type)
Other types
Thyroid Storm
CM: Fast forward metabolic processes Nervousness Apprehensive Cannot sit still Tremors Excess perspiration Poor heat tolerance High HR
Flushed, moist skin Increase appetite Weight loss Weakness Amenorrhea Exophthalmos
Thyroid enlargement Bruit over thyroid arteries Diagnosis: TSH low T3 & T4 elevated Radioactive Iodine Uptake
Fine-needle Aspirate Bx
Thyroid scan
|
Treatment: Antithyroid medications
Plasmapheresis or dialysis to remove excessive T3 & T4 Ablation (burn or cauterize) or removal of gland Cardiac monitoring - dysrhythmias Oxygen to treat dyspnea and possible HF Beta blockers to decrease sympathetic activity sx Acetaminophen to reduce temperature Nursing Interventions: Monitor VS
Provide calm and quiet environ to decr anx Maintain cool room Provide eye care (exophthalmos)
Corticosteroids to reduce inflam
Collab with dietician
Teach pt and family need for antithyroid medication Encourage follow-up with HCP Provide info about online resources Treat photophobia with dark glasses
Ablation/Removal: Radioactive Iodine Therapy (I-131)
If I-131 not successful= Surgical removal of the thyroid Total thyroidectomy/Ablation will ness lifelong thyroid hormone replacement Radioactive Iodine Therapy: Ablative dose I-131 administered Causes acute release of thyr hormone
Observe for thyroid storm (thyrotoxic crisis)
Management
Precautions
Post-Op
|
Hypothyroidism
Patho: 95% is primary d/t low levels of thyroid hormones
CM: Early:
TSH high T3 & T4 low Compensatory Mechanism: Enlarged Thyroid Goiter Abnormal enlargement of thyroid Hypothyroid
Hyperthyroid
Rare in US - major cause in lack of iodine |
Treatment: Levothyroxine (synthroid) Nursing Interventions: Modify activity
Monitor physical status
Promote physical comfort
Enhance coping mechanisms
Promote home and community based care
Myxedema Crisis: Can be fatal Tissue and organ failure d/t decreased metabolism Occurs with undiagnosed or poorly treated hypothyroidism Clinical Manifs
Nursing Interventions:
|
Thyroid Cancer
Papillary, Follicular, Medullary, and Anaplastic Surgery Tx of choice: thyroidectomy
Genetic counseling |
Parathyroid:
Regulate Ca and P metabolism
Ca & P = inverse relationship
Hyperparathyroidism
Patho: Excessive secretion of PTH
CM: Fatigue Muscle weakness Constipation Skeletal pain HTN Dysrhythmias Peptic ulcers Pancreatitis Diagnosis: Elevated Ca Xray Scans |
Treatment: Diuretics Fluids Mobility Diet restriction (Ca rich food) Meds:
Surgery Parathyroidectomy: Parathyroidectomy preoperative care:
Post-op Care
|
Hypoparathyroidism
Patho: Decreased PTH secretion
Common cause:
Treatment: Vorrecting hypocalcemia, vitamin D deficiency Keep pt in quiet environment to decrease neurologic stimuli
|
Disaster
Disaster Management
Disaster Definition
An event that causes illness or injury that exceeds the resources of a healthcare facility
Internal
Within a healthcare institution
Can happen same time as external
Ex: Infectious breakout or fire within the institution
External
Outside of the healthcare institution
Can happen at same time as internal
Ex: chemical explosion or major fire
Internal/External Combination
Tornado that causes injuries outside of the healthcare institution and damage to part of the health care institution
Disaster Phases
Mitigation
Predicting possible crisis, Reducing risk
Preparedness
When disaster is imminent
Response
Time right after the disaster, search and rescue, assess initial damage
Recovery
Restoring, when life is normalizing
Triage Under Mass Casualty Conditions
Green Tag - non-urgent, minor injuries that do not require immed treatment
Yellow Tag - urgent, major injuries that require treatment
Red Tag - emergent, immediate threat to life
Black Tag - dead or expected to die
Practice Questions
Practice Questions (look at book for more)
Oxygen first
INR 2.9 because it's the farthest out of range
PCV can be cause by chronic hypoxemia, so COPD can cause it
Flank pain because it is a symptom of an emergent transfusion reaction - rejection (itching is concerning but not the most concerning)
Review blood transfusions
Ch 37, pg 816
Avoid aspirin because it increases bleeding, risk for bleeding is a concern for Bone marrow Bx
Also pain, infection, mobility issues
Check for consent