Pathophysiology Test One Material (copy)
TBW= total body water
makes up 60%
intracellular is 2/3
extracellular is 1/3
there is constant movement happening between the two fluid compartmetns
ECF made up of interstitial fluid and the blood plasma
interstitial fluid lies between the cells and makes up 80% of ECF
this balance can be disrupted
movement between ICF and ECF is due to concentration gradient
if a difference between concentration occurs then the water shifts
remember that these fluids are solutioins with a solvent and a solute
the concentration changes in acccordance with the amount of solutes to solvent
normal range is 280 to 300
280-300 is isotonic
more than 300 is hypertonic
less than 280 is hyptonnic
ECF changes due to either the increase of water or the increase of salt
drinking more water makes solution more dilute
eating more salt makes more concentrated due to addition of solute
water moves from dilute (more h2o) to less dilute (less h2o)
water would shift from an isotonic 290 ICF to a hypertonic 390 ECF
water would shift from a hypotonic 190 ECF to an isotonic 290 ICF
If remain in a hypertonic state, then the water leaves the cells and moves into the ECF so the cells shrink
sodium is a main factor of influence on the movement of fluid between the ICF and ECF because it is very abundant in the ECF/blood
if the ECF is too hypotonic then cells expand and eventually rupture due to the shift of water from ECF to ICF
how do we make a change back to isotonic? get back the normal solute and water level
how do we make a solution hypertonic? decrease the water or increase the solute
how do we make a solution hypotonic? increase the water or decrease the solute
adding sodium makes it more hypertonic
removing sodium makes it more hypotonic
we are most concerned with sodium as it relates to ECF osmolarity
we care about sodium because changes in its levels heavily influences ECF
ECF is too hypo tonic then the cells expand and rupture to due shifting fluid from the ECF into the ICF
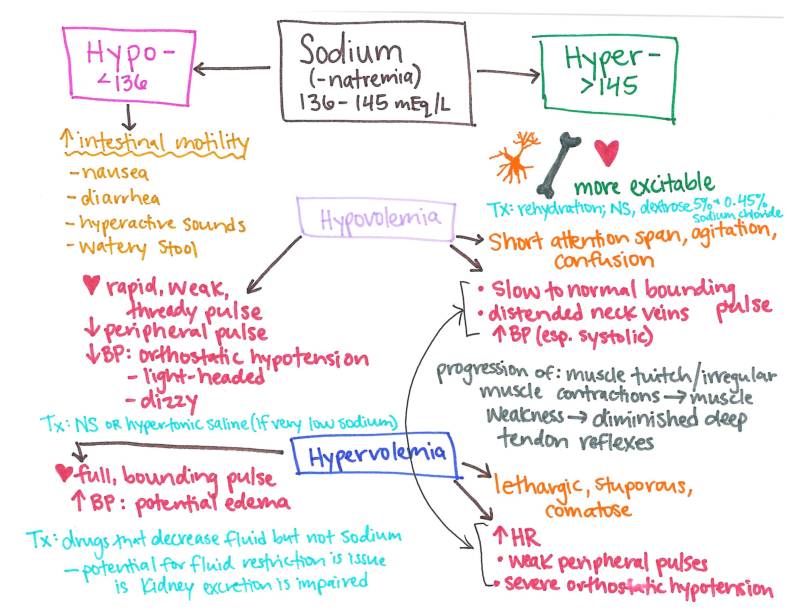
Normal Na is 135-145
sodium levels play a role in blood volume because water follows sodium
How is Na level regulated in the body? kidneys, what we eat, and the hormone aldosterone
aldosterone increases sodium while decreasing potassium '
hypernatremia= more sodium, sodium greater than 145
we base these off of lab work
where will the water shift to? water shifts from the ICF to the ECF because the higher sodium content in the blood means it was become more concentrated
what is the effect of hyper natremia on the cells? it results in cells shrinks because fluid leaves them and enters the blood
what are causes of hypernatremia? decreasing water or increasing sodium intake, too little antidiuretic hormone, too much aldosterone
Na= 152, is this hypernatremia so the blood is hypertonic so water shifts from ICF to the ECF
hyponatremia= less sodium in blood, blood sodium less than 135
the water either decreases or the sodium intake decreases
hyponatremia results in a hypotonic ECF
Na=122, this is severe hyponatremia so the blood is hypotonic resulting in water shifting from the ECF to the ICF and cell expansion
what are causes of hyponatremia? increase intake of water or decrease intake of sodium, too much diuretics, too little aldosterone, too much ADH
Na= 126, due to an increase of water or decreased sodium; blood volume is elevated resulting in elevated blood pressure; we recognize this as hyponatremia where the likely causes is an increase in water intake
Na=153, due to a decrease of water or a increase in sodium; blood volume is elevated resulting in elevated blood pressure; we recognize this is hypernatremia where the likely cause is the increase of sodium in the blood
pressure difference drives the movement within the ECF
two types of pressure= hydrostatic and oncotic
hydrostatic is from the blood into the interstitial fluid (pushing force)
blood volume is the primary determinant of HSP
when BV increases HSP increases
oncotic pressure is the one keeping water in the blood
OC moves water from the IF into plasma (holding force)
water flows according to the greater pressure
arterial pressure is more HSP than OP
venous pressure is more OP than HSP
edema is the build up of fluid in the IF, also called swelling
The four major factors of edema formation are increased plasma HSP, decreased plasma OP, increased cappilary permiablity, and impaired lymph drainage
increased HSP occurs with any increase of BV
BV increase could be caused by endicrine disorders, heart failure, or simply too much IV fluid etc
OP decrease occurs when too much water is kept in the IF
OP decrease could be caused by low albumin levels, liver failure, or protein malnutrition
capillary permiablity is perhaps the most common cause of edema and is often due to inflamation or vessel damage
lymph is where excess IF drains to, so if anything impairs this drainage then the fluid builds up
one common cause of impaired lymph drainage is if someone underwent the removal of lymph nodes
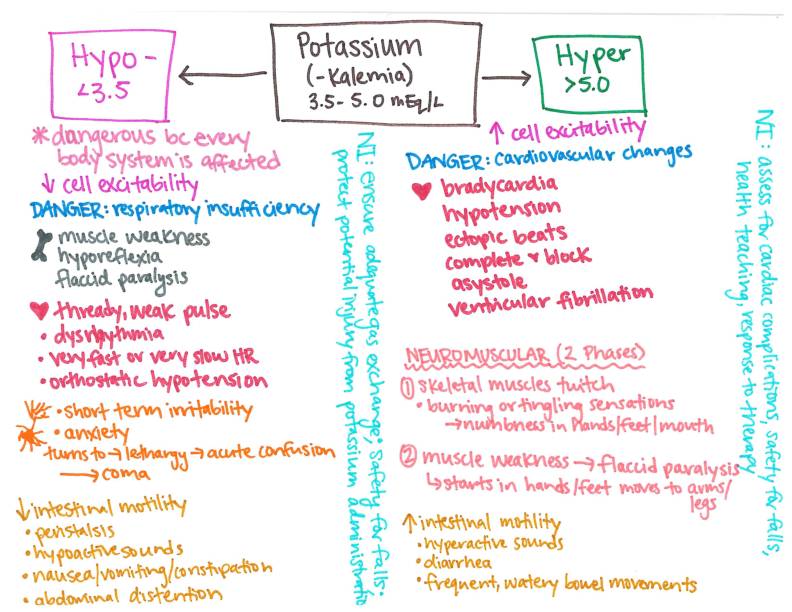
normal blood potassium levels = 3.5 to 5.0
the primary location of potassium in the body is in the cells/ICF
why do we care about potassium? K influences neuromuscular excitability (NMe)
two hormones influence potassium levels: aldosterone is the main one which keeps an in blood and gets rid of K through the kidneys; insulin is the other one which lowers K levels bny shifting it into the cells from the blood
Hyperkalemia= >5.0 and is leveled by mild to severe as well as based on lab values
what are the common causes of hyperkalemia? hypoaldosteronism, increased diet intake of K, kidney disorders, K-sparing drugs
What are the NMe effects of hyperkalemia on the muscles etc? increases because the RMP, which relies on K, gets closer to the threshold
what are the NMe effects of hyperkalemia on the heart? reduces the conduction velocity which can be lethal if the heart stops beating altogether
NMe is controlled by the resting membrane potential (RMP) and threshold
RMP is affected by K
threshold is affected by Ca
rapid changes in K or Ca levels are more lethal/problematic and labeled as acute versus chronic
What are the treatments for hyperkalemia? give Ca gluconate, give insulin, give glucose
we give Ca gluconate during hyperkalemia in order to return NMe back to normal by increasing threshold
we give insulin during hyperkalemia in order to shift the K back into the cells
we give glucose during this treatment in order to maintain blood sugar while administering insulin/prevents hypoglycemia
cell damage by trauma or burns can also cause hyperkalemia
hypokalemia= less K, <3.5
hypokalemia results in a decrease of NMe because the RMP moves further from the threshold
what is the effect of hypokalemia on the heart? it increases conduction velocity which causes fatal arrhythmias such as V-fib and no Cardiac Output which results in no blood pumping
what are the potential causes of hypokalemia? not getting enough K or getting rid of too much; decrease in dietary intake; increase in K output through things such as non K sparing diuretics; aldosterone increase results in increased K output
The effect of K on the heart is what we’re most concerned with!!! It can either cause the heart to stop entirely (hyperkalemia) or cause fatal arrhythmias where heart muscles just twitch without forcefully pumping blood out (hypokalemia)
normal blood calcium=8.5-10.5
why does calcium blood levels matter? influences NMe and establishes threshold
Which hormones influence Ca levels in the blood? PTH and calcitonin
PTH raises the blood calcium and is the most influential on Ca levels
calcitonin decreases the blood calcium (“calcitonin TONES down CALcium”)
Hypercalemia=more Ca, >10.5
What are the common causes of hypercalcemia? hyperparathyroidism and cancers
hyperPTHism results in too much calcium
cancers result in either too much or too little… think about bone cancers and osteoporosis etc
What effect does hypercalcemia have on NMe? it causes to go down because threshold moves away from RMP
Hypocalcemia=less Ca, <8.5
what effect does hypocalcemia have on NMe? it causes it to increase because threshold moves closer to RMP
what are some common causes of hypocalcemia? hypoparathyroidism and vitamin D deficiency
hypoPTHism results in too little calcium
why do we care about hypocalcemia? sustained contranctions with hyperexcitability causes no relaxation and as the threshold gets closer or equal to RMP then NO contraction can occur
normal arterial blood pH=7.35-7.45
alkalosis=>7.45
acidosis=<7.35
metabolic focuses on bicarbonate which is a base
respiratory focuses on CO2 which acts as an acid
Arterial Blood Gas (ABG) is how we make a diagnosis


For the above diagram: note that the norm CO2 and HCO3 or dif from notes because they are the mid values: actual range is 35-45 and 22-28!!!