Abnormal Psychology
Defining Abnormality | ||
|---|---|---|
Terms to Remember | ||
| ||
Abnormal Psychology | ||
| ||
Criteria for Defining Abnormality (4D) | ||
| ||
Biopsychosocial Formulation (What causes abnormality? | ||
| ||
Mental Health | ||
| ||
Mental Disorder (DSM V-TR) | ||
| ||
Basis for Assessing Maladjustment | ||
| ||
HISTORY OF ABNORMAL BEHAVIOR Prehistoric and Ancient Beliefs | ||
| ||
Contemporary Theories On The Causes Of Abnormality | ||
Terms to Remember | ||
| ||
Biological Approaches | ||
| ||
Neurotransmitter Theories | ||
Serotonin | ||
or rewards and it is affected by substances
be associated with:
| ||
Dopamine | ||
or rewards and it is affected by substances
systems
muscle control (Parkinson’s disease)
activity is associated with schizophrenia
are linked to illnesses including:
aggressiveness and having trouble controlling impulses
and addiction | ||
Norepinephrine (noradrenaline) | ||
norepinephrine by slowing its reuptake
neurons are activated for a longer period of time causing stimulating effects
depression | ||
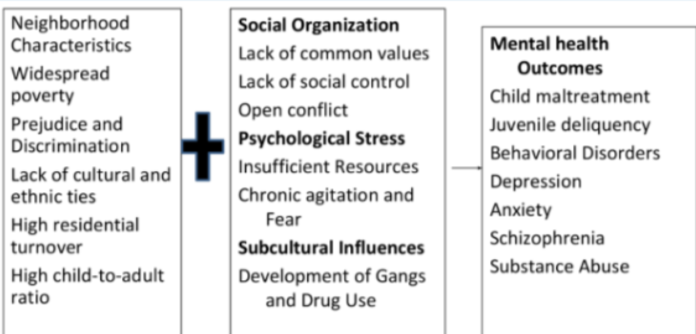
Social Structural Model Of Mental Health | ||
| ||
Models Of Psychopathology | ||
social stimulation that alters cognitive development
| ||
Models In The Study Of Psychopathology | ||
| ||
Biogenic model | ||
brain dysfunction
somatic intervention
dysfunctional behavioral patterns that was learned and placed into practice | ||
Cognitive-behavioral | ||
| ||
Cognitive-neuroscience | ||
system | ||
Biopsychosocial | ||
“Eclectic approach”
and perpetuating factors
| ||
Review Of The Psychological Theories | ||
and forces within individuals that explain human behavior and personality.
Focuses on how people learn through their interactions with the environment.
emotions, body sensations, and behavior are all connected, and that what we think and do affects the way we feel.
individual and stresses concepts such as free will, self-efficacy, and self-actualization
interactions between the patient and other persons in the environment
emotional, interdependent unit. The needs and abilities of one family member will affect all family members
systems that organize and regulate interpersonal phenomena in a group or society | ||
Introduction to DSM 5-TR | ||
Impact of Racism and Discrimination on Psychiatric Diagnosis | ||
| ||
Neurodevelopmental Disorders | ||
developmental period
entering grade school)
impairment of personal, social, or academic functioning
very specific limitations to global impairments of social skills or intelligence
occur | ||
Intellectual Disability (Intellectual Developmental Disorder) | ||
person meets community standards of personal independence and social responsibility compared to others of similar age and sociocultural background
solving, planning, abstract thinking | ||
Criteria | ||
| ||
Relevant Information | ||
retardation to intellectual disability
predispose to disruptive and aggressive behaviors
exploitation
severe intellectual disability: 6 per 1000
intoxication, infection, severe and chronic social deprivation | ||
Global Developmental Delay | ||
developmental milestones in several areas of intellectual functioning
of intellectual functioning including children who are too young to participate in standardized testing
time
age when the clinical severity cannot be reliably assessed during early childhood | ||
Communication Disorders | ||
conventional system of symbols
| ||
Language Disorder | ||
Criteria | ||
and use of language across modalities
(explaining a topic or having conversation)
substantially below those expected for age that limits functioning in effective communication, social participation, academic achievement, and work performance
developmental period
medical or neurological condition | ||
Relevant Information | ||
gestures, or verbal signals
and comprehending language messages | ||
Features | ||
| ||
Development and Course | ||
| ||
Risk and Prognostic Factor | ||
| ||
Speech Sound Disorder | ||
production interferes with speech intelligibility or prevents verbal communication of messages
communication that interfere with social participation, academic achievement, or occupational performance (individually or combined)
developmental period
or acquired conditions | ||
Relevant Information | ||
gestures, or verbal signals
and comprehending language messages | ||
Features | ||
speech production problems
| ||
Childhood-onset Fluency Disorder | ||
Criteria | ||
| ||
Social (Pragmatic) Communication Disorder | ||
Criteria | ||
in effective communication, social participation, social relationships, academic achievement, or work performance (individually or combined)
developmental period
medical or neurological condition | ||
Relevant Information | ||
milestones and structural language problems
communication disorder, or learning disorder | ||
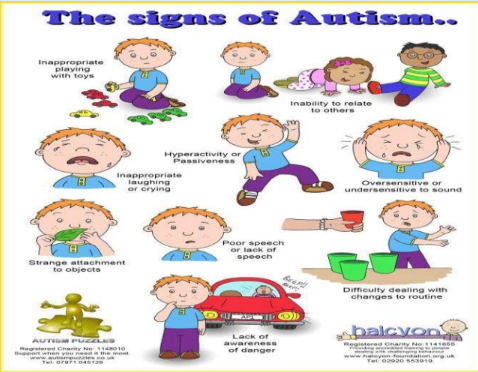
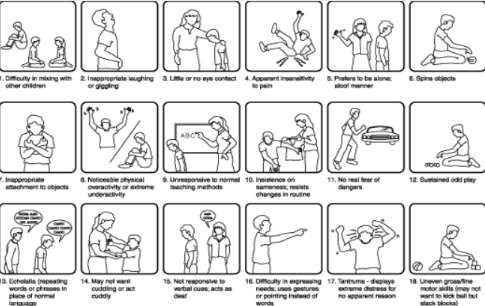
Autism Spectrum Disorder | ||
meaning self
within one’s self”
| ||
Criteria | ||
the early developmental period
| ||
Relevant Information | ||
✓ Early infantile autism ✓ Childhood autism ✓ Kanner’s autism (Leo Kanner, 1943)
| ||
Features | ||
intellectual disability
girls
intellectual disability
dermatoglyphics (adermatoglyphia)
Study of of naturally occurring epidermal ridges Adermatoglyphia Absence of fingerprints
disrupted
second year of lids (12-24 months) ✓ May be seen earlier than 12 months if developmental delays are severe ✓ Can be noted later than 24 months if symptoms are more subtle
| ||
Attention-Deficit/Hyperactivity Disorder (ADHD) | ||
✓ Predominantly inattentive presentation ✓ Predominantly hyperactive/impulsive presentation ✓ Combined presentation
✓ Wandering off task ✓ Failing to follow through on instructions, finishing work or chores ✓ Having difficulty sustaining focus ✓ Being disorganized and is not attributable to defiance or lack of comprehension
→ Excessive motor activity when it is not appropriate → Excessive fidgeting, tapping, or talkativeness
→ Behaviors that are inappropriate, premature, unduly thought out and risky that lead to untoward outcomes
→ Tendency toward repetitive actions and repeated despite adverse consequences | ||
Criteria | ||
✓ Overlooks details ✓ Task inattention ✓ Appears not to listen ✓ Fails to finish tasks ✓ Difficulty in organizing tasks and activities ✓ Avoids tasks requiring sustained mental activity ✓ Often loses things necessary for tasks ✓ Easily distracted ✓ Often forgetful
✓ Often fidgets with or taps hands or feet or squirms in seat ✓ Leaves seat ✓ Runs or climbs ✓ Unable to maintain quiet ✓ Hyperactivity ✓ Talks excessively ✓ Blurts answers ✓ Struggle to take turns ✓ Interrupts or intrudes
to age 12
or more settings
explained by another mental disorder | ||
Relevant Information | ||
age 12 and in two or more settings
(USA)
✓ Unduly sensitive to stimuli and easily upset by noise, light, temperature, and other environmental changes ✓ The child is placid or limp, sleep most of the time and appear to develop slowly ✓ Commonly active in the crib, sleep little and a great deal
✓ May attack a test rapidly ✓ Unable to wait to be called on ✓ They cannot put off for even a minute ✓ Frequently emotionally labile ✓ Impulsive and unable to delay gratification ✓ Susceptible to accidents
✓ May attack a test rapidly ✓ Unable to wait to be called on ✓ They cannot put off for even a minute ✓ Frequently emotionally labile ✓ Impulsive and unable to delay gratification ✓ susceptible to accidents | ||
Development and Course | ||
from normative behaviors before age 4
elementary school years and inattention becomes more prominent and impairing
pregnancy
exposure in utero
grams)
inhibition, effortful control or constraint, negative emotionality, and/or elevated novelty seeking
with a ratio of 2:1 | ||
Specific Learning Disorder | ||
Criteria | ||
| ||
Relevant Information | ||
| ||
Developmental Coordination Disorder | ||
Definition | ||
| ||
Features | ||
| ||
Stereotypic Movement Disorder | ||
Criteria | ||
| ||
Risks | ||
| ||
Tic Disorders | ||
Definition | ||
| ||
Criteria | ||
| ||
Prevalence, Development and Course | ||
| ||
Risk and Prognostic Factors | ||
| ||
SCHIZOPHRENIA SPECTRUM AND OTHER PSYCHOTIC DISORDERS | ||
| ||
Schizophrenia | ||
Etiology
Genetic Factors
Stress-Diathesis Model
Psychological Factors
Social Factors
Risk Factors
Phases of Schizophrenia
| ||
Delusions | ||
| ||
Hallucinations | ||
| ||
Brief Psychotic Disorder | ||
| ||
Schizophreniform | ||
| ||
Schizophrenia | ||
| ||
Schizoaffective | ||
| ||
Psychotic Disorder Due to Another Medical Condition | ||
| ||
Substance/Medication Induced Psychotic Disorder | ||
| ||
Other Specified Schizophrenia Spectrum and Other Psychotic Disorder | ||
| ||
Unspecified Schizophrenia Spectrum and Other Psychotic Disorder | ||
| ||
Delusional Disorder | ||
| ||
Schizotypal (Personality) Disorder | ||
|