ANTH Final
The War on Drugs
Key concepts
Supply side v. demand side in the war on drugs
Addressing the supply of demands (production and sales) rather than addressing the side of those using drugs and reducing the demand.
Creates a Power vacuum - when someone in a position of power has lost control of something and no one has replaced them yet.
Example: Shift between Mexico to Colombia, back to Mexico in terms of the powerful drug cartels
Key concepts
Neocolonialism: post WWII, post decolonization, refers to colonization by other means e.g. existing economic relationships
Internal colonialism: a notion of uneven structural power between areas of a state. The source of exploitation comes from within the state.
The war on drugs: international impacts
Plan Colombia
Hundreds of millions of dollars of military aid, training, & equipment from US to Colombia
Counterinsurgency training at the School of the Americas
Implicated in human rights violations
Clinton administration waived all but one human rights requirements
Widely hailed as a success…
Aerial herbicide application
US regularly sponsors the spraying of large amounts of herbicides over the jungles of south & central America for drug eradication
Glyphosate (produced by Monsanto)
Glyphosate and AMPA accumulate in the environment
Chronic low does effects on humans and animals do occur
Causes shifts in microbial community composition in soil, plant, & animal guts
Glyphosate & antibiotic resistance in fungi and bacteria correlated
May drive antibiotic resistance.
The Mexican drug war
The Mexican theater of the global war on drugs - led by US government
Ongoing, asymmetric, low intensity conflict between Mexican gov. and drug trafficking syndicates.
Massive drug-related violence - means of maintaining power within an underground business
Guadalajara Cartel - First Mexican cartel (an alliance between existing Sinaloa, Juarez, Tijuana, & Sonora Cartels)
Broken up leading to conflict between smaller factions
Mexican cartels now dominate the wholesale elicit drug market
The war on drugs: domestic impacts
The war on drugs: facts
Every 25 seconds someone is arrested in US for drug possession -> 1.3 million arrests per year in 2015
1/5th of incarcerated population is serving time for a drug charge
1.5 million on parole for drug offense
Incarceration has little impact on substance abuse rates and is instead linked to increased mortality from overdose
Incarceration has a negligible effect on public safety
Racial disparities: the new Jim Crow
Black Americans are 4x more likely to be arrested for marijuana charges
Black Americans make up 30% of all drug related arrests, they represent only 12.5% of users
Black Americans are 6x more likely to be incarcerated despite equal use rates
80% of people serving time for fed. Drug offense are Black or Latinx
Black defendants serve similar time for drug offense as white defendants do for violent crime
Prosecutors are 2x likely to pursue a mandatory minimum for Black defendants as white
Those with mandatory mins serve 5x longer
Economic impacts
Since 1971, the War on Drugs has cost the use ~$1 trillion.
In 2015, Fed spend ~9.2 million every day to incarcerate people w/ drug offenses
State govs. Spent another $7 billion on incarceration for drugs in 2015
Marijuana legalization would save ~$7.7 billion per year and yield an additional $6 billion in tax revenue
Impact of interventions: drug courts
More than 3,100 drug courts in US
Specialized court programs that sentence defendants to substance use treatment, supportive services, & supervision instead of incarceration
Linked with lower rates of reoffending
National evaluation found participants were 26% less likely to report substance abuse after completion
Completion rates vary by program (30-70%)
Impact of interventions: law enforcement assisted diversion
Law Enforcement Assisted Diversion (LEAD) programs allow officers to divert people to treatment of social services rather than making low level arrests
Pioneered in Seattle
LEAD associated with increases in housing and economic stability
After referral, participants 33% more likely to
Immigration to the United States from central and south America
Much of the immigration to the US
What are pharmaceutical drugs?
Drugs used to diagnose, cure, treat, or prevent disease
Pharmaceutical drugs vary in and can be
Drug scheduling
Based upon the acceptable medical use and the drug's abuse or dependence potential
Determined by DEA, US Department of Health and Human Services,
Drug Tiers
Under a healthcare (insurance) plan, the list of covered prescription drugs is called a formulary.
The formulary is usually divided into tiers or levels of coverage based on the type or usage of the medication
Each tier will have a defined out-of-pocked cost that the patient must pay before receiving the drug.
Insulin
What is insulin? & how does it work?
Insulin is a hormone (protein) secreted from beta-cells of the pancreas
It has multiple functions throughout the body but one of the main functions is related to glucose
It signal cells to store glucose (skeletal muscle & fat) or turn glucose into glycogen and reduce glucose release (liver).
3 main types of diabetes*
*There are many more types of diabetes!
All types require blood glucose monitoring
Type 1 (T1D)
Body cannot make insulin -> Fully dependent on exogenous insulin injections
Autoimmune disease: The immune system targets & destroys pancreatic beta cells
Onset commonly occurs at ages 0 - 40 but can occur at any age (more diagnoses are occurring at later ages)
Estimated 5 - 10% of people with diabetes have T1D
Type 2 (T2D)
Body can make insulin but it does not work properly in the body (insulin resistance) or your pancreas cannot make enough insulin
Onset typically occurs in adulthood (but this is changing)
Can be managed with changes to lifestyle (diet,
Diabetes globally
Diabetes in the US
History of insulin as a drug
Discovered in 1923 by Frederick Banting, James Collip, Charles Best, and John MacLeod
First synthesized from animal insulin (cows and pigs)
Collip and Best sold the patent for $1 to the University of Toronto
They believed that people who needed insulin should be able to afford it
Banting did not list his name
1970s scientists discovered how to fully synthesize insulin in a lab
More effective than animal insulin
Continued innovate to get faster and better insulin than previous versions
1921: Insulin isolation
1922: First usage of insulin in clinic
Ways to administer insulin
Syringe & needle
Insulin pen
Insulin pump
Insulin inhaler
5 Suppliers:
MannKind
Viatris
Eli Lilly*
Sanofi*
US insulin pricing
From 1996 - 2016 the price of insulin* in the US has increased by over >1100%
This increase in insulin
Why is insulin so expensive in the US? Because it can be.
These 3 manufacturers supply nearly all US insulin
They raised insulin prices to fund research and development
Minor tweaks to drugs (or synthesis process) over time = extended patents that prevent competition
Relationships with pharmacy benefit
Issues with health insurance
Tiering issues
Insurance plans do not always cover every type of available insulin (they may prefer a specific brand of a particular type of insulin)
Differences in tiers can alter out-of-pocket costs for consumers
Insurance companies can change tiers or preferred brands from one year to the next -> causing individuals to have to switch medications or pay more for the particular type or brand of insulin they need
Some insulins may be the same general type by impact individuals differently
Variation in cost by pharmacy type
Trouble aligning prescription needs - how much insulin insurance will cover
Individuals need varying amounts of insulin (and this may change over time)
More than just insulin
Syringes
Insulin pen needles
Insulin pump supplies
Glucose monitor
Glucose test strips
Lancets
Continuous Glucose Monitor (CGM) supplies
Alcohol swabs
Tapes or sprays to help with pump or CGM adherence
Ketone meter & strips
Ketone urine strips
Sugar/glucose tablets
Glucagon (for hypoglycemic emergencies)
Rationing insulin
The process of cutting back/reducing the amount of insulin used to delay buying insulin (prolonging time between purchases)
It is estimated that 1.3 million Americans (16.5%) ration their insulin
Leaves people vulnerable diabetes related complications in the short term (diabetic ketoacidosis) and long term (kidney disease, vascular disease, neuropaythy)
Crowdfunding & social media
Many people (mostly with T1D) turn to crowdfunding and/or social media to
Generic insulin
Slowly, some generic insulins are becoming available, but they are not as widely available as name brand insulins (number of pharmacies that carry them or stock
Definitions: biologics
Biologics generally come from living organisms, including animal cells or microorganisms such as bacteria and yeast. Biologics include a wide range
Homemade insulin (biohacking)
Develop both the methodology and hardware to allow communities and individuals to produce medical-grade
Trips to Canada
Individuals and groups (caravans) travel to Canada
Progress?
Eli Lilly (one of the big 3 suppliers) announced a cost cap on their name brand insulin after a fake Twitter post announced they were making insulin free
Novo Nordisk and Sanofi followed and also changed their prices of some of their name brand insulin
It is not simply $35 for everyone - it depends on individuals insurance coverage and those without insurance coverage and those without insurance
History of ADHD
Early years of ADHD
1798 Sir Alexander Crichton noticed some people were more easily distracted and unable to focus in the way that others could --> symptoms beginning early in life
1902 British pediatrician Sir George Frederick Still described the condition noting that it was "an abnormal defect of moral control in children"
Children were intelligent but could not control their behavior in ways others could
1932: Discovery of hyperkinetic disease by German Doctors Kramer and Pollnow: children who had difficulty staying still
Early medication for ADHD: Benzedrine
Some say Amphetamine discovered in late 1880s by a Romanian chemist
Other sources say it was discovered in the 1910s
1936 Benzedrine (name for amphetamine) is approved by the FDA
Introduced in 1930s for narcolepsy
Widely available as an inhaled decongestant
Available without a prescription increase in popularity
1937: Charles Bradley in East Providence, RI noticed that a stimulant called Benzedrine caused some children's behavior to improve -> also improved school performance
Bradley's findings were not widely accepted for quite some time
The introduction of Ritalin
Ritalin is methylphenidate
Psychostimulant
Developed in 1944 - intended to treat chronic fatigue and depression
FDA approved in 1955
Became a popular treatment for ADHD
Is it still the stimulant doctors most often prescribe for children with ADHD
From ADD to ADHD
The APA issued the first "Diagnostic and Statistical Manual of Mental Disorders" (the DSM) in 1952.
No form of ADHD was recognized
DSM II was published in 1968 and included hyperkinetic reaction of childhood
DSM III released in 1980. Hyperkinetic reaction of childhood renamed to attention deficit disorder (ADD)
Hyperactivity was not a considered a common symptom
Finally ADHD
1987 - released a revised version of the DSM-III
Removed hyperactivity distinction and changed name to attention deficit hyperactivity disorder
Included three symptoms: inattentiveness, impulsivity, and hyperactivity
2000 DSM IV released
Includes three subtypes of ADHD: 1) combined type; 2) predominantly inattentive type; 3) predominantly hyperactive/impulse type
Rise in diagnosis
ADHD cases began to climb significantly in the 1990s
Increase from 6.1% to 10.2% between 1997 and 2016
Potential factors in these increases include:
Doctors were able to diagnose more efficiently
More parents become aware and reported symptoms
More children were actually developing ADHD
Increasing availability of accommodations & destigmatization
Is ASHS a culture-bound syndrome?
Culture-bound syndrome
AKA a culture specific syndrome sometimes known as a folk illness
A combination of psychiatric and somatic symptoms that is considered to be a recognizable disease only within a specific society or culture. Often there are no biochemical or structural alterations of body organs or functions, and the disease is not recognized in other Cultures.
Examples?
IV
Examples of culturally-specific syndromes included in DSM<IV
Medicalization
They process by which human conditions and problems come to be defined and treated as medical conditions
Thus they become the of medical study, diagnosis, prevention, or treatment
Originated in sociology in 1970s
Normal human variation is medicalized and pathologized
ADHD in the US
9.8% of US children ages 3-17 have ever been diagnosed with ADHD between 2016-2019
Boys are more likely to be diagnosed (13%) that girls (6%)
Black, non-Hispanic children and which non-Hispanic children are more often diagnosed (12% and 10%), than Hispanic children (8%) or Asian, non-Hispanic children (3%)
ADHD estimates vary widely by state (6%-16%)
Contemporary
What is an amphetamine?
Speed, Uppers
Dexmethylphenidate
Non-stimulant medication for ADHD
Wellbutrin
What caused the Adderall shortage?
Started with a disruption in manufacturing at a plant run by Teva Pharmaceuticals, the largest supplier of Adderall in the U.S.
Increased Demand: Massive increase in the number of adults with adult diagnosed ADHD -> seek out treatment
Increased Access: Rise of companies like Cerebral during the pandemic - diagnosis and treatment online -> operating like pill mills for Adderall.
Part of the issue is limits on how much you can get at a time (only a 30 day supply) -> means people can't get more until they are already out.
Global Spread of Slim Ideals and Fat Stigma
Slim-body ideals have become widespread globally over recent decades, but the spread of fat-stigmatizing beliefs hasn't been as closely studied.
Using surveys and body mass data from 680 adults in urban areas across 10 countries, the study investigates how people perceive and stigmatize obesity.
Cultural Consensus on Obesity
The study found a shared cultural model of obesity across diverse populations, including traditionally fat-positive societies.
Key elements of this model include viewing obesity as a disease, attributing weight gain to individual responsibility, recognizing fat as socially undesirable, and acknowledging the inappropriateness of open prejudice against fat individuals.
Fat Stigma is Prevalent in Middle-Income and Developing Countries
Fat-stigmatizing views are especially common in middle-income and developing countries, suggesting a global diffusion of negative ideas about obesity.
Culture constructs ideas of health
Historical Shifts in Ideas of Fatness
In the European Context
Pre-19th Cent.: potential signifier of health & social privilege ("well fed")
19th C.: more class stratification relating to food quality.
E.g., "corpulent" vs. "plump," "guant" vs. "lean."
Present: potential signifier of illness & social stigma.
Michel Foucault
Philosopher interested in power and knowledge in societies
Previous lectures have discussed biopower…
Power knowledge - knowledge is not just a tool for understanding the world but also a mechanism of power that shapes and controls societies
Panopticon Metaphor
Individuals internalize surveillance and regulate their own behavior, because they don't know if they are being watched.
This system creates an illusion of free choice, as people adapt their behavior to fit norms, in reality, their actions are shaped by the pervasive influence of power and surveillance embedded in society.
Knowledge
Observation
Internalization of norms
Fatphobia & Fat-related Stigma
Fatphobia-systematic bias against and anxieties about fatness
Fat stigma-negative values placed on fat or large bodies that are socially discrediting
Examples of fat-related stigma in slim idealism:
Moral (sloth, lacking will power, and expense on society)
Class (poor, lazy, stupid)
Sex/Gender (selfish, unattractive, fetishized)
Globalization of Fat Stigma
Brewis et al discusses how many cultures in the 1980s and 1990s had documented positive views on fatness as a beauty standard
Proposed that this changed with globalization, what did they find?
Something to think about: How does this relate to a culture bound syndrome from last class? (We can discuss more in recitation)
Weight and Health are often Conflated
What does fat do in our body?
Crucial component of the body that serves many important functions
Energy storage
Vitamin absorption & storage
Insulation
Immune function
Regulate blood sugar
Cell membranes
Defining Obesity
CDC - "Weight that is higher than what is considered as a healthy weight for a given height is described as overweight or obese."
Harvard School of Public Health - "At their most basic, the words "overweight" and "obesity" are ways to describe having too much body fat."
BMI=Body Mass Index
Body Fat is most commonly measured through calculating BMI
BMI is a measure that uses weight and height
Created to be a population level measure
One pro is that it is easy to calculate!
What are some of the problems of this measure?
Limitations of BMI
BMI does not account for body composition
BMI does not account for healthy variation in body proportions
A paradox for body types and BMI
Body mass index may not be the best way to measure risk of death from obesity. New research shows that people with a normal body mass index but a large belly, which is known as central obesity, are at greater risk of dying from heart disease than those with more evenly distributed weight.
BMI was created not as a measure of individual health but a statistic that could be looked at in the aggregate to screen for possible health issues
Regular BMI categories assumes certain ranges are always better
Aesthetics does not equal Health
The Mechanism of Diet Drugs
For any weight loss, including wt loss from drugs, you need to be in a calorie deficit.
This means you are burning more calories than you consume.
This can occur through
Increasing metabolism or differential use of tissues in metabolic processes
Decreasing appetite
Both!
Long History of Diet Drugs
People have been trying to address body weight with drugs for centuries!
Late 1800s thyroid extract - speeds of metabolism…serious consequences
1930s-dinitrophenol (compound in explosives and pesticides) was observed to have wt loss properties in factory workers, then utilized as a diet drug
Uncouples oxidative phosphorylation which leads to heightened metabolic rate and increased fat metabolism
Symptoms of Graves' Disease
Graves' disease is the most common cause of hyperthyroidism, which causes the following symptoms
Rapid heartbeat (palpitation)
Amphetamine & Fen-Phen
Amphetamines became a popular diet drug after WWII
Soldiers used it to stay awake, habit forming
Aggressive marketing was utilized by the medical community, including making the pills in a rainbow color
Crackdown starting in 1959 through the 1960s on the dangers
Fen-Phen (phentermine and fenfluramine) comes to market in the 1980s after NIH declares obesity to be a chronic disease
Release norepinephrine and suppresses appetite = wt loss fast! Hailed a miracle drug
However, long term users were found to develop heart valve abnormalities (removed from market in 1997)
Oh, Oh, Oh, Ozempic
Ozempic (semaglutide) was approved for use in adults with T2DM in 2017
Wegovy (semaglutide) was approved for chronic wt management in 2021
Mounjaro (semaglutide + tirzepatide) was approved for use in T2DM in 2023
Many more, all in the GLP-1 class of drugs.
Glucagon-like peptide-1 receptor antagonist (GLP-1)-selectively binds and activates the GLP1-receptor, the target for native GLP-1 (more on next slide)
Most common
What’s the hype?
Significant decrease of HbA1c (T2DM pts only) or improved maintenance of blood sugar
Significant decrease of weight (around 5-10% of body weight, dependent on dose and other factors, up to 20% decrease in body weight)
Significant decrease in systolic blood pressure.
Been found to reduce risk of cardiovascular events (strokes, heart attacks) and some evidence found in helping heart failure and chronic kidney disease
More studies are being conducted, current longest study is the SELECT study which is
What's the backlash?
Adverse Events:
Nausea, Vomiting, Diarrhea are very common side effects
20% Dropped out of SELECT study
Access!
Off label use
Price: The current Ozempic list price for each pen is $936 (1 pen = 4 doses).
Increase in demand: The number of semaglutide fills increased by 442% between January 2021 and December 2023 (from 471,876 to 2,555,308), with Ozempic accounting for over 70% or more of semaglutide fills during this period.
These increases, which primarily occurred following increased awareness of weight-loss benefits in late 2022, are likely contributing to the FDA-reported shortage of Ozempic and Wegovy first issued in March 202.
One study found despite
Longevity
Just like diets, once a patient stops intervention, all "benefits" rebound
Some argue that semaglutide
So… is ozempic good
No drugs will not SOLVE any systematic problem
Drugs are not solving root cause health related problems
Large structural change is needed
The problem is not obesity, we have a health crisis. Our system is not working because it does not allow equitable access to:
Nutritious food
Diet Culture is a Panopticon
Stigma
Moral (sloth, lacking will power, an expense on society
Class (poor, lazy, stupid)
Sex/Gender (selfish, unattractive, fetishized)
Access to preventative health measures
Nutritious food
Safe areas to play & exercise
Where does Ozempic fit in this system?
Ozempic seems to work for many people that are victims of our current system, improving health. We should not stigmatize the use of these drugs. Time will show long term health benefits/consequences.
These drugs do not work for everyone and should not be hailed as a miracle drug. A larger focus on
On a Positive Note…
The Principles of
Health at Every Size
Weight Inclusivity
Accept and respect the inherent diversity of body shapes and sizes. Reject the idealizing or pathologizing of specific weights.
Health Enhancement
Overview of Key Themes:
Marginality and Pharmaceuticals: The concept of marginalization in biomedicine often relates to a lack of access to medications, particularly antidepressants, which are marketed as means to reintegrate individuals into society, particularly middle-class consumer society.
Pharmaceutical Citizenship: The paper introduces the notion of "pharmaceutical citizenship," which examines how access to drugs can define an individual's citizenship status and how pharmaceuticals might be perceived as a means of gaining or regaining societal belonging.
Context and Background:
Global Mental Health Trends: The World Health Organization recognizes depression as a significant global health issue, especially with the rise of SSRIs (selective serotonin reuptake inhibitors) in the 1990s.
Pharmaceutical Industry in India: India's pharmaceutical sector has grown significantly, producing generic medications and increasingly targeting the domestic market with a focus on antidepressants.
Marginality as a Social Construct:
The WHO and other organizations define marginality as social inequality that should be addressed. Marginalized individuals are often viewed as deprived of necessary medications.
Depression is viewed not only as a clinical issue but also as a symptom of social marginality, creating a cycle where untreated mental health issues perpetuate social exclusion.
Pharmaceutical Marketing Strategies:
Antidepressants in India: Ecks analyzes advertisements for Indian antidepressants, revealing a consistent marketing theme that promotes the idea of demarginalization. The imagery used in ads typically features happy, affluent families and individuals, indicating a lifestyle associated with middle-class success and happiness.
Self-Diagnosis Initiatives: The marketing of antidepressants includes self-diagnosis tools that encourage individuals to see themselves as depressed, thus framing them as marginal unless they seek treatment.
Pharmaceutical Citizenship Defined:
Conceptual Framework: Pharmaceutical citizenship extends beyond traditional notions of citizenship to include access to medicines and the societal implications of medication use.
Two Models of Citizenship: There are two competing narratives within the Indian context:
Citizen-as-Patient: Recognizes individuals as citizens deserving of medical care.
Not-Yet-Citizen Patient: Suggests that access to medicines is a means of achieving full citizenship, implying a hierarchy based on medical consumption.
Advertising Analysis:
Ecks provides detailed descriptions of antidepressant advertisements that emphasize the positive transformations associated with medication, often neglecting any acknowledgement of the complexities of mental health issues or social status.
The advertisements consistently depict successful, happy individuals, devoid of any visible signs of marginality. This imagery promotes the idea that antidepressants can seamlessly reintegrate individuals into a socially acceptable middle-class life.
Critical Observations:
Global vs. Local Narratives: The marketing strategy often ignores local cultural contexts and definitions of distress, instead promoting a universalized concept of depression that aligns with Western models.
Normalization of Depression: By framing normal emotional responses as pathological, the marketing campaigns can create a larger consumer base for antidepressants, equating medication with social belonging and happiness.
Conclusions:
Ecks argues that the commodification of antidepressants within Indian society reflects broader global trends in mental health and consumerism, where happiness is increasingly linked to medication consumption and the markers of middle-class identity.
The paper prompts readers to consider the implications of defining citizenship through pharmaceutical access and the potential ethical concerns surrounding such narratives in the context of global health and local realities.
Overview
Rates of depression and anxiety rose significantly during the COVID-19 pandemic.
As of 2020, 1 in 8 American adults were taking antidepressants, with usage increasing by 18.6% during the pandemic.
Zoloft has become the 12th most prescribed medication in the U.S.
There is an ongoing debate about the efficacy of antidepressants, with some studies suggesting they are only marginally more effective than placebos.
Efficacy of Antidepressants
Selective Serotonin Reuptake Inhibitors (SSRIs), like Prozac and Zoloft, are the most commonly prescribed antidepressants, increasing serotonin availability in the brain.
The STAR*D trial is the largest study on antidepressants, involving nearly 3,000 participants:
50% showed significant improvement after one or two medications.
About 70% became symptom-free after trying up to four different medications.
Critiques of the STAR*D trial include the lack of a placebo comparison, raising questions about the true efficacy of the drugs versus placebo effects.
Placebo Effect
Research indicates that much of the improvement attributed to antidepressants could be a placebo effect. For instance:
Antidepressant users improved 9.6 points on a depression scale, while placebo users improved 7.8 points.
Approximately 80% of the antidepressant benefit may stem from placebo effects.
Overall, antidepressants are about 25% more effective than placebos.
Mechanism of Action
Traditional views suggested depression was caused by low neurotransmitter levels, particularly serotonin.
More recent research indicates depression is complex, with serotonin playing a limited role.
Antidepressants may help regenerate synapses in the hippocampus, an area affected by depression.
There is skepticism regarding genetic tests predicting antidepressant responses; current tests primarily assess metabolism for adverse reactions.
Alternative Treatments
Emerging alternatives include ketamine and psychedelic therapy, showing effectiveness in about 60% of patients, especially those resistant to traditional antidepressants.
Non-pharmaceutical approaches, including exercise, diet, therapy, and meditation, are increasingly being recommended as first-line treatments.
Research indicates exercise can help promote brain connectivity and has been shown to be as effective as antidepressants for some patients.
Conclusion
While antidepressants are not perfect and there is hope for better options in the future, they currently remain the best available treatments for many individuals with depression.
A holistic approach to treatment, considering lifestyle factors and non-pharmaceutical interventions, is encouraged for effective management of depression.
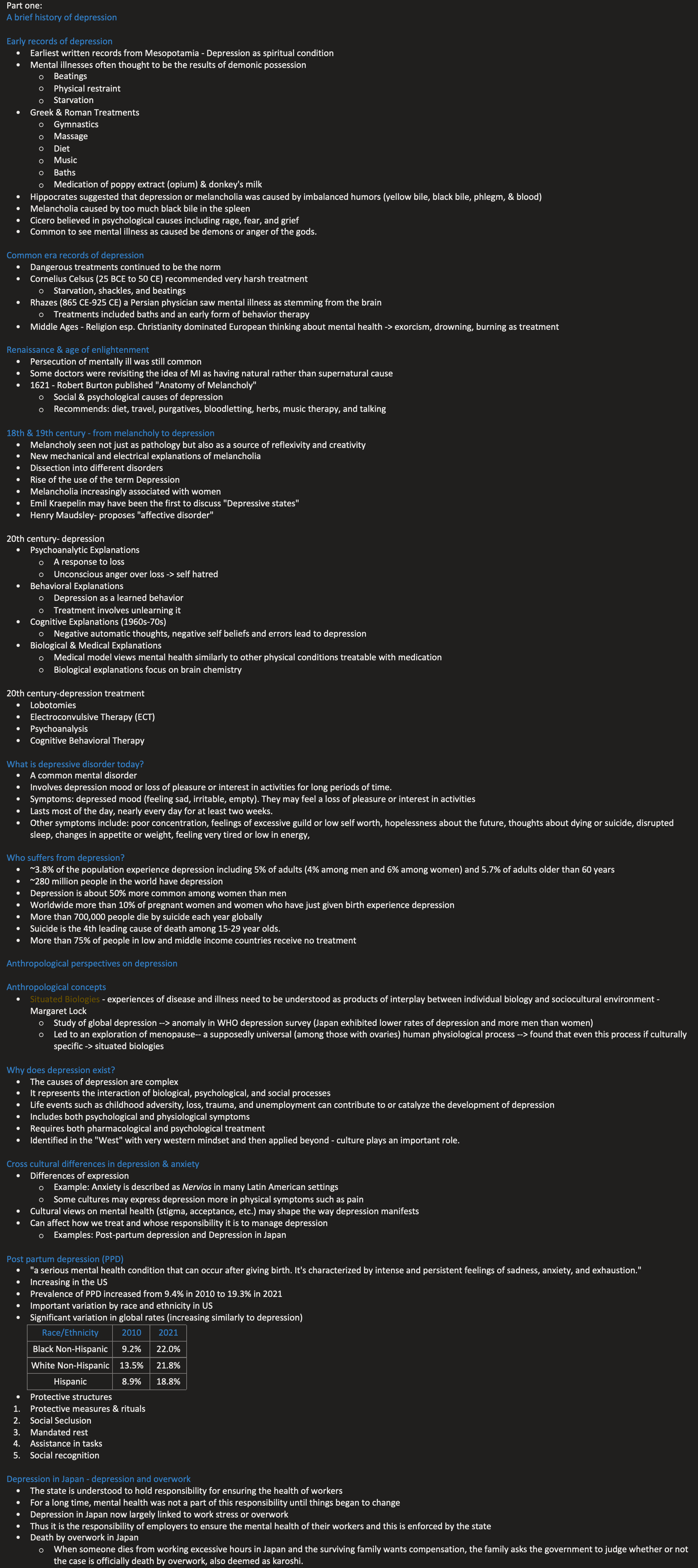
Part one:
A brief history of depression
Early records of depression
Earliest written records from Mesopotamia - Depression as spiritual condition
Mental illnesses often thought to be the results of demonic possession
Beatings
Physical restraint
Starvation
Greek & Roman Treatments
Gymnastics
Massage
Diet
Music
Baths
Medication of poppy extract (opium) & donkey's milk
Hippocrates suggested that depression or melancholia was caused by imbalanced humors (yellow bile, black bile, phlegm, & blood)
Melancholia caused by too much black bile in the spleen
Cicero believed in psychological causes including rage, fear, and grief
Common to see mental illness as caused be demons or anger of the gods.
Common era records of depression
Dangerous treatments continued to be the norm
Cornelius Celsus (25 BCE to 50 CE) recommended very harsh treatment
Starvation, shackles, and beatings
Rhazes (865 CE-925 CE) a Persian physician saw mental illness as stemming from the brain
Treatments included baths and an early form of behavior therapy
Middle Ages - Religion esp. Christianity dominated European thinking about mental health -> exorcism, drowning, burning as treatment
Renaissance & age of enlightenment
Persecution of mentally ill was still common
Some doctors were revisiting the idea of MI as having natural rather than supernatural cause
1621 - Robert Burton published "Anatomy of Melancholy"
Social & psychological causes of depression
Recommends: diet, travel, purgatives, bloodletting, herbs, music therapy, and talking
18th & 19th century - from melancholy to depression
Melancholy seen not just as pathology but also as a source of reflexivity and creativity
New mechanical and electrical explanations of melancholia
Dissection into different disorders
Rise of the use of the term Depression
Melancholia increasingly associated with women
Emil Kraepelin may have been the first to discuss "Depressive states"
Henry Maudsley- proposes "affective disorder"
20th century- depression
Psychoanalytic Explanations
A response to loss
Unconscious anger over loss -> self hatred
Behavioral Explanations
Depression as a learned behavior
Treatment involves unlearning it
Cognitive Explanations (1960s-70s)
Negative automatic thoughts, negative self beliefs and errors lead to depression
Biological & Medical Explanations
Medical model views mental health similarly to other physical conditions treatable with medication
Biological explanations focus on brain chemistry
20th century-depression treatment
Lobotomies
Electroconvulsive Therapy (ECT)
Psychoanalysis
Cognitive Behavioral Therapy
What is depressive disorder today?
A common mental disorder
Involves depression mood or loss of pleasure or interest in activities for long periods of time.
Symptoms: depressed mood (feeling sad, irritable, empty). They may feel a loss of pleasure or interest in activities
Lasts most of the day, nearly every day for at least two weeks.
Other symptoms include: poor concentration, feelings of excessive guild or low self worth, hopelessness about the future, thoughts about dying or suicide, disrupted sleep, changes in appetite or weight, feeling very tired or low in energy,
Who suffers from depression?
~3.8% of the population experience depression including 5% of adults (4% among men and 6% among women) and 5.7% of adults older than 60 years
~280 million people in the world have depression
Depression is about 50% more common among women than men
Worldwide more than 10% of pregnant women and women who have just given birth experience depression
More than 700,000 people die by suicide each year globally
Suicide is the 4th leading cause of death among 15-29 year olds.
More than 75% of people in low and middle income countries receive no treatment
Anthropological perspectives on depression
Anthropological concepts
Situated Biologies - experiences of disease and illness need to be understood as products of interplay between individual biology and sociocultural environment - Margaret Lock
Study of global depression --> anomaly in WHO depression survey (Japan exhibited lower rates of depression and more men than women)
Led to an exploration of menopause-- a supposedly universal (among those with ovaries) human physiological process --> found that even this process if culturally specific -> situated biologies
Why does depression exist?
The causes of depression are complex
It represents the interaction of biological, psychological, and social processes
Life events such as childhood adversity, loss, trauma, and unemployment can contribute to or catalyze the development of depression
Includes both psychological and physiological symptoms
Requires both pharmacological and psychological treatment
Identified in the "West" with very western mindset and then applied beyond - culture plays an important role.
Cross cultural differences in depression & anxiety
Differences of expression
Example: Anxiety is described as Nervios in many Latin American settings
Some cultures may express depression more in physical symptoms such as pain
Cultural views on mental health (stigma, acceptance, etc.) may shape the way depression manifests
Can affect how we treat and whose responsibility it is to manage depression
Examples: Post-partum depression and Depression in Japan
Post partum depression (PPD)
"a serious mental health condition that can occur after giving birth. It's characterized by intense and persistent feelings of sadness, anxiety, and exhaustion."
Increasing in the US
Prevalence of PPD increased from 9.4% in 2010 to 19.3% in 2021
Important variation by race and ethnicity in US
Significant variation in global rates (increasing similarly to depression)
Race/Ethnicity | 2010 | 2021 |
Black Non-Hispanic | 9.2% | 22.0% |
White Non-Hispanic | 13.5% | 21.8% |
Hispanic | 8.9% | 18.8% |
Protective structures
Protective measures & rituals
Social Seclusion
Mandated rest
Assistance in tasks
Social recognition
Depression in Japan - depression and overwork
The state is understood to hold responsibility for ensuring the health of workers
For a long time, mental health was not a part of this responsibility until things began to change
Depression in Japan now largely linked to work stress or overwork
Thus it is the responsibility of employers to ensure the mental health of their workers and this is enforced by the state
Death by overwork in Japan
When someone dies from working excessive hours in Japan and the surviving family wants compensation, the family asks the government to judge whether or not the case is officially death by overwork, also deemed as karoshi.
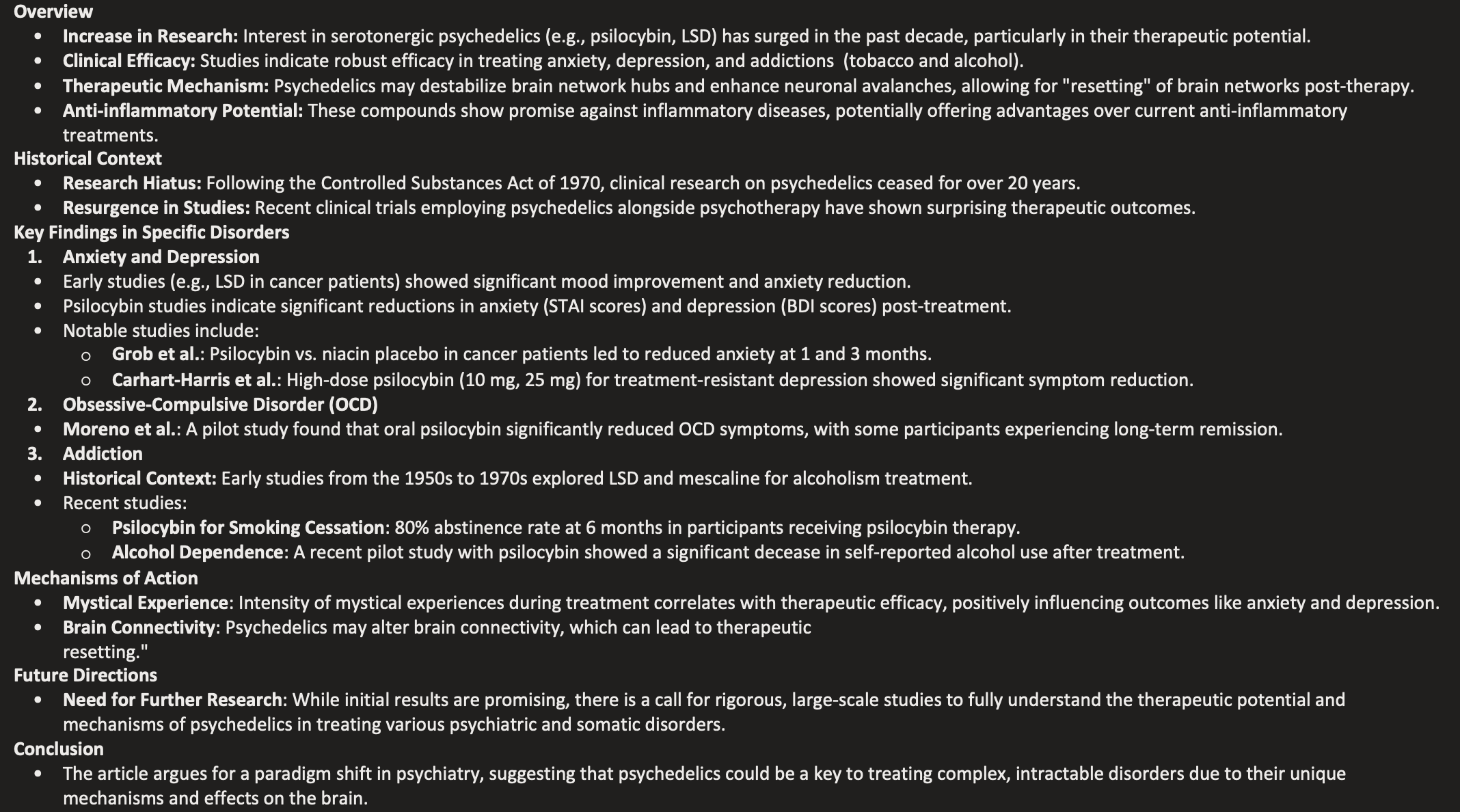
Overview
Increase in Research: Interest in serotonergic psychedelics (e.g., psilocybin, LSD) has surged in the past decade, particularly in their therapeutic potential.
Clinical Efficacy: Studies indicate robust efficacy in treating anxiety, depression, and addictions (tobacco and alcohol).
Therapeutic Mechanism: Psychedelics may destabilize brain network hubs and enhance neuronal avalanches, allowing for "resetting" of brain networks post-therapy.
Anti-inflammatory Potential: These compounds show promise against inflammatory diseases, potentially offering advantages over current anti-inflammatory treatments.
Historical Context
Research Hiatus: Following the Controlled Substances Act of 1970, clinical research on psychedelics ceased for over 20 years.
Resurgence in Studies: Recent clinical trials employing psychedelics alongside psychotherapy have shown surprising therapeutic outcomes.
Key Findings in Specific Disorders
Anxiety and Depression
Early studies (e.g., LSD in cancer patients) showed significant mood improvement and anxiety reduction.
Psilocybin studies indicate significant reductions in anxiety (STAI scores) and depression (BDI scores) post-treatment.
Notable studies include:
Grob et al.: Psilocybin vs. niacin placebo in cancer patients led to reduced anxiety at 1 and 3 months.
Carhart-Harris et al.: High-dose psilocybin (10 mg, 25 mg) for treatment-resistant depression showed significant symptom reduction.
Obsessive-Compulsive Disorder (OCD)
Moreno et al.: A pilot study found that oral psilocybin significantly reduced OCD symptoms, with some participants experiencing long-term remission.
Addiction
Historical Context: Early studies from the 1950s to 1970s explored LSD and mescaline for alcoholism treatment.
Recent studies:
Psilocybin for Smoking Cessation: 80% abstinence rate at 6 months in participants receiving psilocybin therapy.
Alcohol Dependence: A recent pilot study with psilocybin showed a significant decease in self-reported alcohol use after treatment.
Mechanisms of Action
Mystical Experience: Intensity of mystical experiences during treatment correlates with therapeutic efficacy, positively influencing outcomes like anxiety and depression.
Brain Connectivity: Psychedelics may alter brain connectivity, which can lead to therapeutic
resetting."
Future Directions
Need for Further Research: While initial results are promising, there is a call for rigorous, large-scale studies to fully understand the therapeutic potential and mechanisms of psychedelics in treating various psychiatric and somatic disorders.
Conclusion
The article argues for a paradigm shift in psychiatry, suggesting that psychedelics could be a key to treating complex, intractable disorders due to their unique mechanisms and effects on the brain.
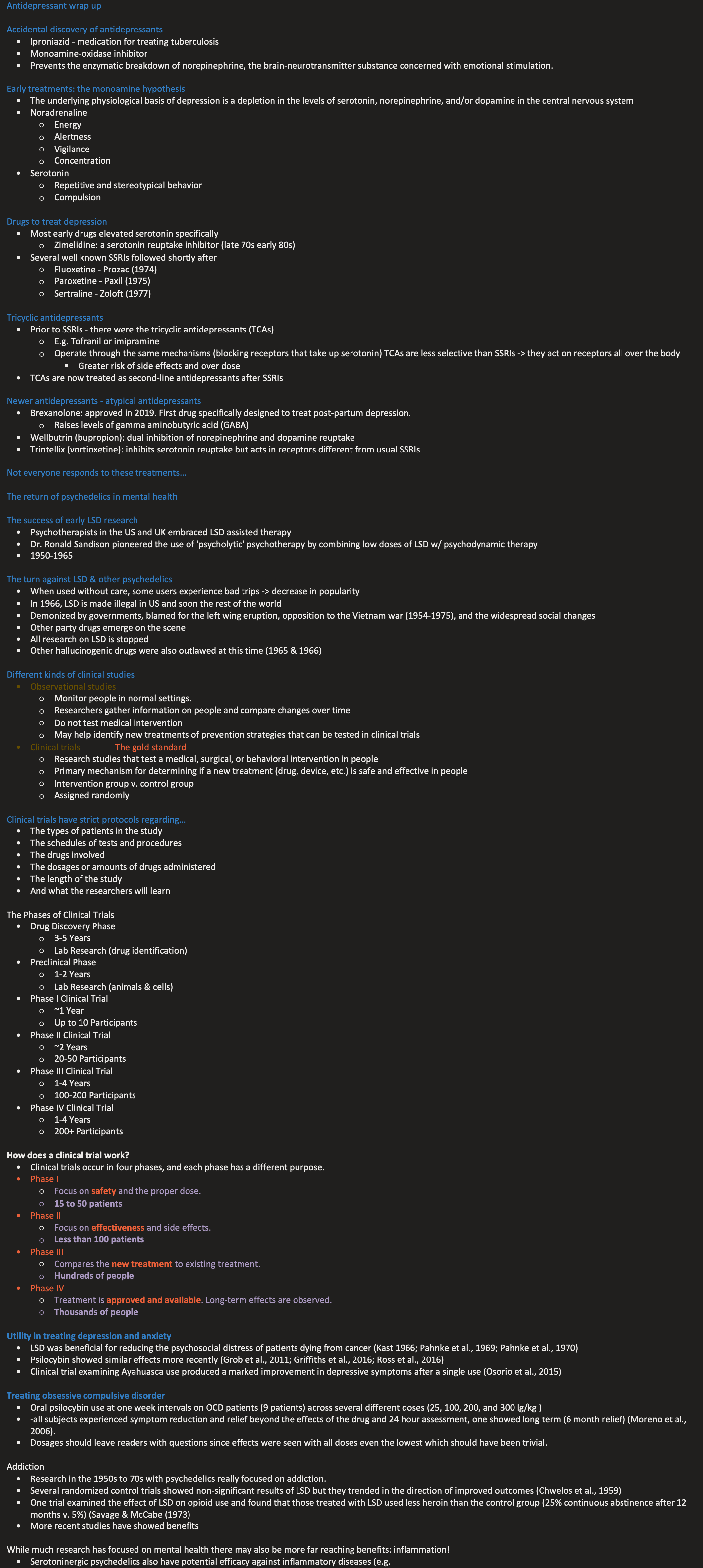
Antidepressant wrap up
Accidental discovery of antidepressants
Iproniazid - medication for treating tuberculosis
Monoamine-oxidase inhibitor
Prevents the enzymatic breakdown of norepinephrine, the brain-neurotransmitter substance concerned with emotional stimulation.
Early treatments: the monoamine hypothesis
The underlying physiological basis of depression is a depletion in the levels of serotonin, norepinephrine, and/or dopamine in the central nervous system
Noradrenaline
Energy
Alertness
Vigilance
Concentration
Serotonin
Repetitive and stereotypical behavior
Compulsion
Drugs to treat depression
Most early drugs elevated serotonin specifically
Zimelidine: a serotonin reuptake inhibitor (late 70s early 80s)
Several well known SSRIs followed shortly after
Fluoxetine - Prozac (1974)
Paroxetine - Paxil (1975)
Sertraline - Zoloft (1977)
Tricyclic antidepressants
Prior to SSRIs - there were the tricyclic antidepressants (TCAs)
E.g. Tofranil or imipramine
Operate through the same mechanisms (blocking receptors that take up serotonin) TCAs are less selective than SSRIs -> they act on receptors all over the body
Greater risk of side effects and over dose
TCAs are now treated as second-line antidepressants after SSRIs
Newer antidepressants - atypical antidepressants
Brexanolone: approved in 2019. First drug specifically designed to treat post-partum depression.
Raises levels of gamma aminobutyric acid (GABA)
Wellbutrin (bupropion): dual inhibition of norepinephrine and dopamine reuptake
Trintellix (vortioxetine): inhibits serotonin reuptake but acts in receptors different from usual SSRIs
Not everyone responds to these treatments…
The return of psychedelics in mental health
The success of early LSD research
Psychotherapists in the US and UK embraced LSD assisted therapy
Dr. Ronald Sandison pioneered the use of 'psycholytic' psychotherapy by combining low doses of LSD w/ psychodynamic therapy
1950-1965
The turn against LSD & other psychedelics
When used without care, some users experience bad trips -> decrease in popularity
In 1966, LSD is made illegal in US and soon the rest of the world
Demonized by governments, blamed for the left wing eruption, opposition to the Vietnam war (1954-1975), and the widespread social changes
Other party drugs emerge on the scene
All research on LSD is stopped
Other hallucinogenic drugs were also outlawed at this time (1965 & 1966)
Different kinds of clinical studies
Observational studies
Monitor people in normal settings.
Researchers gather information on people and compare changes over time
Do not test medical intervention
May help identify new treatments of prevention strategies that can be tested in clinical trials
Clinical trials The gold standard
Research studies that test a medical, surgical, or behavioral intervention in people
Primary mechanism for determining if a new treatment (drug, device, etc.) is safe and effective in people
Intervention group v. control group
Assigned randomly
Clinical trials have strict protocols regarding…
The types of patients in the study
The schedules of tests and procedures
The drugs involved
The dosages or amounts of drugs administered
The length of the study
And what the researchers will learn
The Phases of Clinical Trials
Drug Discovery Phase
3-5 Years
Lab Research (drug identification)
Preclinical Phase
1-2 Years
Lab Research (animals & cells)
Phase I Clinical Trial
~1 Year
Up to 10 Participants
Phase II Clinical Trial
~2 Years
20-50 Participants
Phase III Clinical Trial
1-4 Years
100-200 Participants
Phase IV Clinical Trial
1-4 Years
200+ Participants
How does a clinical trial work?
Clinical trials occur in four phases, and each phase has a different purpose.
Phase I
Focus on safety and the proper dose.
15 to 50 patients
Phase II
Focus on effectiveness and side effects.
Less than 100 patients
Phase III
Compares the new treatment to existing treatment.
Hundreds of people
Phase IV
Treatment is approved and available. Long-term effects are observed.
Thousands of people
Utility in treating depression and anxiety
LSD was beneficial for reducing the psychosocial distress of patients dying from cancer (Kast 1966; Pahnke et al., 1969; Pahnke et al., 1970)
Psilocybin showed similar effects more recently (Grob et al., 2011; Griffiths et al., 2016; Ross et al., 2016)
Clinical trial examining Ayahuasca use produced a marked improvement in depressive symptoms after a single use (Osorio et al., 2015)
Treating obsessive compulsive disorder
Oral psilocybin use at one week intervals on OCD patients (9 patients) across several different doses (25, 100, 200, and 300 lg/kg )
-all subjects experienced symptom reduction and relief beyond the effects of the drug and 24 hour assessment, one showed long term (6 month relief) (Moreno et al., 2006).
Dosages should leave readers with questions since effects were seen with all doses even the lowest which should have been trivial.
Addiction
Research in the 1950s to 70s with psychedelics really focused on addiction.
Several randomized control trials showed non-significant results of LSD but they trended in the direction of improved outcomes (Chwelos et al., 1959)
One trial examined the effect of LSD on opioid use and found that those treated with LSD used less heroin than the control group (25% continuous abstinence after 12 months v. 5%) (Savage & McCabe (1973)
More recent studies have showed benefits
While much research has focused on mental health there may also be more far reaching benefits: inflammation!
Serotoninergic psychedelics also have potential efficacy against inflammatory diseases (e.g.
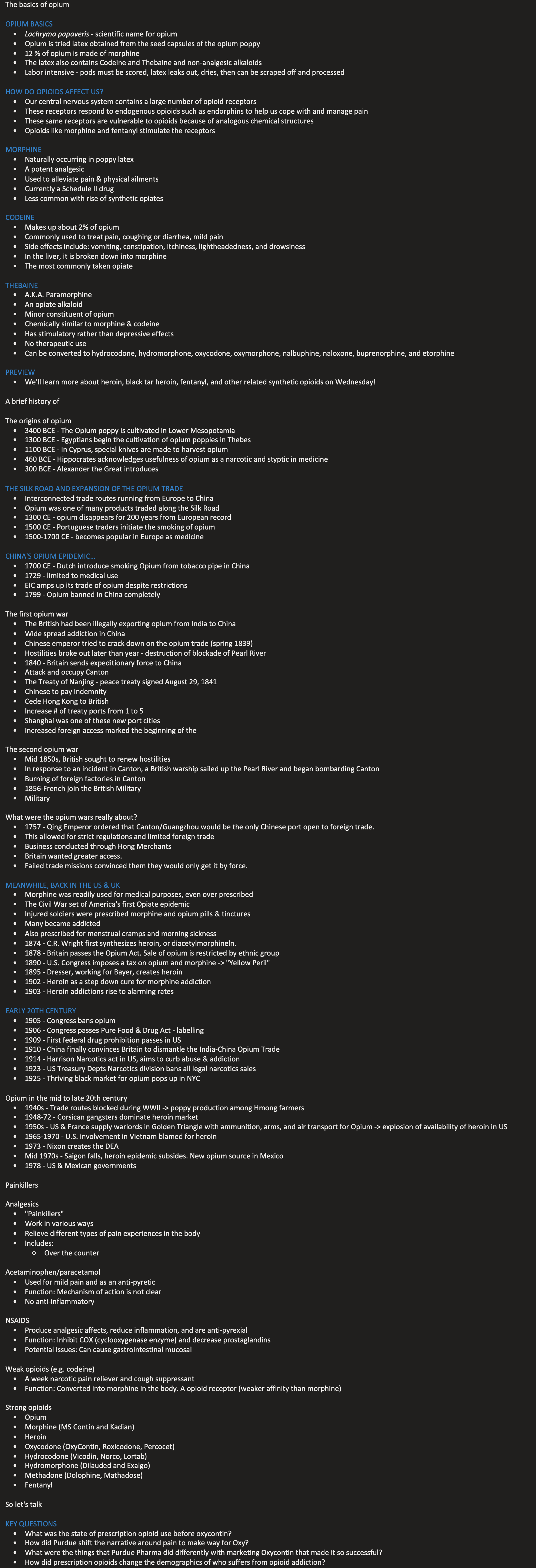
The basics of opium
OPIUM BASICS
Lachryma papaveris - scientific name for opium
Opium is tried latex obtained from the seed capsules of the opium poppy
12 % of opium is made of morphine
The latex also contains Codeine and Thebaine and non-analgesic alkaloids
Labor intensive - pods must be scored, latex leaks out, dries, then can be scraped off and processed
HOW DO OPIOIDS AFFECT US?
Our central nervous system contains a large number of opioid receptors
These receptors respond to endogenous opioids such as endorphins to help us cope with and manage pain
These same receptors are vulnerable to opioids because of analogous chemical structures
Opioids like morphine and fentanyl stimulate the receptors
MORPHINE
Naturally occurring in poppy latex
A potent analgesic
Used to alleviate pain & physical ailments
Currently a Schedule II drug
Less common with rise of synthetic opiates
CODEINE
Makes up about 2% of opium
Commonly used to treat pain, coughing or diarrhea, mild pain
Side effects include: vomiting, constipation, itchiness, lightheadedness, and drowsiness
In the liver, it is broken down into morphine
The most commonly taken opiate
THEBAINE
A.K.A. Paramorphine
An opiate alkaloid
Minor constituent of opium
Chemically similar to morphine & codeine
Has stimulatory rather than depressive effects
No therapeutic use
Can be converted to hydrocodone, hydromorphone, oxycodone, oxymorphone, nalbuphine, naloxone, buprenorphine, and etorphine
PREVIEW
We'll learn more about heroin, black tar heroin, fentanyl, and other related synthetic opioids on Wednesday!
A brief history of
The origins of opium
3400 BCE - The Opium poppy is cultivated in Lower Mesopotamia
1300 BCE - Egyptians begin the cultivation of opium poppies in Thebes
1100 BCE - In Cyprus, special knives are made to harvest opium
460 BCE - Hippocrates acknowledges usefulness of opium as a narcotic and styptic in medicine
300 BCE - Alexander the Great introduces
THE SILK ROAD AND EXPANSION OF THE OPIUM TRADE
Interconnected trade routes running from Europe to China
Opium was one of many products traded along the Silk Road
1300 CE - opium disappears for 200 years from European record
1500 CE - Portuguese traders initiate the smoking of opium
1500-1700 CE - becomes popular in Europe as medicine
CHINA'S OPIUM EPIDEMIC…
1700 CE - Dutch introduce smoking Opium from tobacco pipe in China
1729 - limited to medical use
EIC amps up its trade of opium despite restrictions
1799 - Opium banned in China completely
The first opium war
The British had been illegally exporting opium from India to China
Wide spread addiction in China
Chinese emperor tried to crack down on the opium trade (spring 1839)
Hostilities broke out later than year - destruction of blockade of Pearl River
1840 - Britain sends expeditionary force to China
Attack and occupy Canton
The Treaty of Nanjing - peace treaty signed August 29, 1841
Chinese to pay indemnity
Cede Hong Kong to British
Increase # of treaty ports from 1 to 5
Shanghai was one of these new port cities
Increased foreign access marked the beginning of the
The second opium war
Mid 1850s, British sought to renew hostilities
In response to an incident in Canton, a British warship sailed up the Pearl River and began bombarding Canton
Burning of foreign factories in Canton
1856-French join the British Military
Military
What were the opium wars really about?
1757 - Qing Emperor ordered that Canton/Guangzhou would be the only Chinese port open to foreign trade.
This allowed for strict regulations and limited foreign trade
Business conducted through Hong Merchants
Britain wanted greater access.
Failed trade missions convinced them they would only get it by force.
MEANWHILE, BACK IN THE US & UK
Morphine was readily used for medical purposes, even over prescribed
The Civil War set of America's first Opiate epidemic
Injured soldiers were prescribed morphine and opium pills & tinctures
Many became addicted
Also prescribed for menstrual cramps and morning sickness
1874 - C.R. Wright first synthesizes heroin, or diacetylmorphineln.
1878 - Britain passes the Opium Act. Sale of opium is restricted by ethnic group
1890 - U.S. Congress imposes a tax on opium and morphine -> "Yellow Peril"
1895 - Dresser, working for Bayer, creates heroin
1902 - Heroin as a step down cure for morphine addiction
1903 - Heroin addictions rise to alarming rates
EARLY 20TH CENTURY
1905 - Congress bans opium
1906 - Congress passes Pure Food & Drug Act - labelling
1909 - First federal drug prohibition passes in US
1910 - China finally convinces Britain to dismantle the India-China Opium Trade
1914 - Harrison Narcotics act in US, aims to curb abuse & addiction
1923 - US Treasury Depts Narcotics division bans all legal narcotics sales
1925 - Thriving black market for opium pops up in NYC
Opium in the mid to late 20th century
1940s - Trade routes blocked during WWII -> poppy production among Hmong farmers
1948-72 - Corsican gangsters dominate heroin market
1950s - US & France supply warlords in Golden Triangle with ammunition, arms, and air transport for Opium -> explosion of availability of heroin in US
1965-1970 - U.S. involvement in Vietnam blamed for heroin
1973 - Nixon creates the DEA
Mid 1970s - Saigon falls, heroin epidemic subsides. New opium source in Mexico
1978 - US & Mexican governments
Painkillers
Analgesics
"Painkillers"
Work in various ways
Relieve different types of pain experiences in the body
Includes:
Over the counter
Acetaminophen/paracetamol
Used for mild pain and as an anti-pyretic
Function: Mechanism of action is not clear
No anti-inflammatory
NSAIDS
Produce analgesic affects, reduce inflammation, and are anti-pyrexial
Function: Inhibit COX (cyclooxygenase enzyme) and decrease prostaglandins
Potential Issues: Can cause gastrointestinal mucosal
Weak opioids (e.g. codeine)
A week narcotic pain reliever and cough suppressant
Function: Converted into morphine in the body. A opioid receptor (weaker affinity than morphine)
Strong opioids
Opium
Morphine (MS Contin and Kadian)
Heroin
Oxycodone (OxyContin, Roxicodone, Percocet)
Hydrocodone (Vicodin, Norco, Lortab)
Hydromorphone (Dilauded and Exalgo)
Methadone (Dolophine, Mathadose)
Fentanyl
So let's talk
KEY QUESTIONS
What was the state of prescription opioid use before oxycontin?
How did Purdue shift the narrative around pain to make way for Oxy?
What were the things that Purdue Pharma did differently with marketing Oxycontin that made it so successful?
How did prescription opioids change the demographics of who suffers from opioid addiction?
Key Themes
Differences in Framing:
Opioid Epidemic (2016-2017): Primarily framed using medical/public health terminology (e.g., treatment, health).
Crack Cocaine Epidemic (1988-1989): Framed with criminal justice terminology (e.g., enforcement, arrest), portraying addiction as a criminal act.
The framing aligns with racial demographics-opioids are associated with white users, while crack cocaine is associated with African Americans.
Policy Implications:
Media narratives influenced public policy responses:
Medical framing (opioids): Encouraged public health measures like treatment access, drug courts, and prevention programs.
Criminal framing (crack): Promoted punitive measures such as mandatory sentencing, "three strikes" laws, and mass incarceration.
Public health approaches to opioids focused on rehabilitation and systemic blame (e.g., pharmaceutical companies), contrasting with crack's criminalization model.
Media's Role in Shaping Public Perception:
Media has a dual role in setting the public agenda and framing issues, often emphasizing certain narratives that resonate with societal biases.
The crack cocaine epidemic was framed to suggest violence and criminality, influencing harsher public policies.
Historical and Structural Factors:
The Reagan administration's "War on Drugs" strategically linked substance use to criminality and race, disproportionately targeting African Americans.
Race played a significant role in public perceptions and responses:
Crack cocaine was predominantly associated with Black communities, fueling punitive measures.
Opioids, associated with white communities, received a compassionate, health-focused response.
Racial Disparities:
African Americans faced disproportionate incarceration rates for drug-related offenses despite similar substance use rates to whites.
Collateral consequences of mass incarceration included exclusion from housing, education, and employment, reinforcing systemic inequality (Michelle Alexander's "new racial caste system").
Evolution of Media Narratives:
Changes in media language over time do not fully explain the differences in responses to these epidemics.
Substance type (stimulants vs. opioids) and racial associations were likely critical factors in shaping media narratives and public policy.
Findings:
Critics' hypotheses that racial demographics influenced the divergent responses to the epidemics are supported.
Methamphetamine (1992-1993) and heroin (1988-2017) analyses suggest that substance legality and associated racial identities influenced media framing and subsequent policy.
Implications:
The study underscores the importance of equitable media framing to ensure just public health responses to substance use.
It highlights how structural and racial biases can permeate policy through media influence.
Key Themes
Racial Disparities in Responses to Drug Epidemics
Crack epidemic (1980s-1990s) disproportionately affected Black communities; it was met with criminalization and harsh punishment.
Opioid epidemic (2000s-present) affects predominately white communities and is met with sympathy, treatment, and understanding.
White drug users are often framed as victims needing help, while Black users were demonized as criminals.
Media Representation and Compassion
Media coverage of the opioid crisis often humanizes addicts and their families, portraying their struggles with sympathy (e.g., photos of innocent children, narratives about addicted mothers' challenges).
Coverage of the crack crisis emphasized crime and violence, showing images of arrests and drug use without compassion or context.
Historical and Social Context
Structural factors such as poverty, systemic racism, and housing discrimination exacerbated the crack epidemic's effects in Black communities.
These communities were already vulnerable due to decades of marginalization, making the violence and addiction associated with crack worse.
Policy and Political Response
Politicians like Donald Trump and Chris Christie expressed deep sympathy for opioid addiction victims, framing it as an uncontrollable tragedy.
During the crack epidemic, policymakers responded with punitive measures, such as mandatory minimum sentencing laws and "War on Drugs" rhetoric, leading to mass incarceration of Black Americans.
Impact on Families and Generations
Bailey's family experienced profound losses due to drug-related violence and incarceration.
Generational trauma: Children born into drug-affected families, like Bailey's nieces and nephews, suffered developmental issues, instability, and exposure to violence.
Inequities in Treatment and Resources
Black families like Bailey's lacked access to appropriate treatment for addiction or resources to combat systemic challenges.
Instead, they were stigmatized and left to fend for themselves, perpetuating cycles of poverty and incarceration.
Personal Anecdotes:
The author recalls visiting the grave of his almost sister-in-law, who was a bystander killed in a drug-related drive-by shooting. Her children narrowly survived and bear lifelong scars.
Bailey's brother, Jordan, was imprisoned for drug-related crimes despite his family's efforts to intervene early.
His oldest brother, Moochie, is serving life for a murder committed under the influence of drugs, showing the compounding effects of untreated addiction and systemic neglect.
Critical Points:
Uneven Media Narratives: The crack epidemic's victims, especially children, were rarely portrayed sympathetically, unlike children affected by the opioid epidemic today.
Systemic Racism: Black families faced systemic barriers to education, healthcare, and economic opportunity, making them more vulnerable to the devastating effects of addiction.
Society's Role: Bailey argues society failed Black communities by criminalizing addiction rather than addressing its root causes.
Conclusion:
Bailey's article underscore the stark racial disparities in how American society has addressed drug epidemics, showing the need for equitable responses that prioritize compassion and systemic reform.
Crisis
People
Problem
Epidemic
Drug
Medicalized
THE CRACK CRISIS
Surge of crack cocaine use in major cities in the US in 1980s-1990s
Most users were Black
Resulted in increases in crime & violence in inner cities
Significant backlash in form of "tough on crime" policies
Large spike in incarceration rates
Escalation in the War on drugs
CRACK CRISIS IS SEEN AS A CRIMINAL ISSUE, OPIOID EPIDEMIC IS SEEN AS A PUBLIC HEALTH ISSUE
DEPICTIONS OF USERS
Criminals v. victims
People without morals or work ethic v. people who got swept up
Problems v. people who need to be helped
RESPONSES
Demonize users v. expressions of empathy and sympathy
Criminalize, prosecute, & punish v/. Search for answers, try to get help for users, increase treatment options
A RETURN TO CRIMINALIZATION?
How has the Biden administration addressed fentanyl overdoses?
Framed opioid use, addiction, and overdose as a public health issue
This includes more treatment Better medications
Some accessible through the ACA
In the last year we have seen the first decrease in overdose deaths since (2018)
Saving some 16,000 people (according to CDC)
PROMISES FROM THE INCOMING ADMINISTRATION
Promises of cracking down on fentanyl traffickers & dealers
Securing the border
Has proposed the death penalty for drug dealers
Tom Homan (the US Border Tsar) promises US military action against Mexican drug cartels
Most experts believe that these policies will not be effective and or result in major diplomatic issues and destabilize Mexico
DEATHS OF DESPAIR:
Deaths attributable to suicide, drug overdose, and alcohol-related liver disease
WHAT ARE DEATHS OF DESPAIR?
Deaths attributed to alcohol, drugs, or suicide
Rising in white, working class
Education plays a major role
Similar patterns observed among Black Americans in 1980s & 1990s
ECONOMIC TIES?
Linked with decline in household income
Loss of working class jobs
Shuttering of factories
Exportation of Labor
Shift in industry
IS IT GLOBAL?
Not really
Seeing some increase in Australia & Canada
Was an increase in UK but seems to be flattening
Criticisms of deaths of despair
Not limited to white Americans - Ignores ongoing disparities and changes among other groups
Black Americans were still dying at much higher rates than white Americans even with the rises of DODs
Actually during the same period, premature deaths among Native Americans increased by a much greater margin
Midlife mortality is still significantly lower for White Americans than for Black
WHAT IS RESPONSIBLE FOR THIS PHENOMENON?
What is neoliberalism?
NEOLIBERALISM
An economic philosophy and political ideology that embraces largely unregulated free market capitalism.
Emphasis on personal responsibility and individualization of risk and reward.
Tends to transfer responsibility of economic factors from the public sector (government) to the private sector (corporations).
Economic policies include: privatization, austerity, deregulation, free trade, and reductions in government spending in order to increase the role of the private sector.
Reductions in social services and social spending.
THE CONSEQUENCES OF NEOLIBERALISM
Economic Growth
Increase in Policing & Military
Reduction of social safety net
Reduction in manufacturing
Rise in Inequality
Stagnation in household income
NEOLIBRALISM IS NOT LIMITED TO ONE POLITICAL PARTY
THE CONSEQUENCES OF NEOLIBERALISM
Economic Growth
Increase in Policing & Military
Reduction of social safety net
Reduction in manufacturing
Rise in Inequality
Stagnation in household income
NEOLIBERAL POLICIES + INCREASINGLY LETHAL DRUGS -> RISE IN DEATHS OF DESPAIR AMONG AMERICANS
KEY CONCEPTS
BASIC DEFINITIONS
Sex: the different biological and physiological characteristics of males and females, such as reproductive organs, chromosomes, hormones, etc.
Usually synonymous with "assigned sex" or "biological sex"
Often dichotomized as male/female but also includes intersex individuals
Gender: refers to the cultural constructions and expectations we have that are often observed, performed and understood in a given society.
Gender Identity: how a person identifies their own gender, may be different than how they are perceived
Sexuality: 1) The capacity for sexual feelings 2) a person's identity in relation to the gender or genders to which they are typically attracted; sexual orientation.
Sexual orientation/identity: who you are attracted to or drawn to romantically, emotionally, or sexually
LET'S TALK ABOUT SEX & DRUGS…
Chem sex
Divine connection
Via sex & drugs
(e.g. Hinduism)
Drugs & sex work
Coerced & otherwise
Alcohol & sex
Gendered expectations
Around use
Libido & sex drive
Issues - men get
Viagra women get
Wine
Gender affirming care
Birth
Control
SSRI's & libido
Drugs
& gender performance
Use of drugs to
Facilitate sexual
Assault
ANTHROPOLOGICAL PERSPECTIVES ON SEX/GENDER
HISTORY OF GENDER IN ANTHROPOLOGY
Early ethnographic studies: gender = kinship or family
1970s & 1980s - rise of feminist anthropology --> gender its own area
Focus on division of domestic & public, drawing attention to structural inequalities, role of economic disparities, global dimensions of gender politics, role language, sexuality, & masculinity studies, health and human rights
Challenges Western/monolithic assumptions
Incorporating queer perspectives and moving beyond both sex and gender binaries
GLOBAL & TEMPORAL GENDER VARIATION
EXAMPLES OF GENDER VARIATION
Travesti - a word which can refer to transgender individuals in Latin America
Assigned male at birth, adopt feminine, transfeminine or femme gender identity
In Brazil, they do not identify as women
May represent a third gender
ZAPOTEC - MUXE
Assigned male at birth, dresses, behaves, and is associated with female gender
Often seen as a third gender
Third gender predates colonization
Phenomenon of Muxe seems more recent
BUGIS - 5 GENDERS
Ethinc group from Indonesia's 3rd largest island Sulawesi
They see sex as a spectrum from which 5 socioculturally salient genders emerge
Makkunrai (~cis women)
Oroané (~cis man)
Calabai (~trans women)
Calalai (~trans men)
Bissu (~intersex)
Gender is a social construct that sits on a spectrum.
Underlying this notion of gender as a spectrum has been the idea
that biological sex is a fixed dichotomy: male/female
This represents a fundamental misunderstanding about the
nature of biological sex.
HORMONE BASICS
What is a
Hormone?
A hormone is any member of a class of signaling molecules, produced by glands in multicellular organisms, that are transported by the circulatory system to target distant organs to regulate physiology and behavior.
"Pharmacologic dose" - amount greater
ALL PEOPLE NEED BOTH ESTROGEN AND TESTOSTERONE TO
FUNCTION!
USES OF HORMONE THERAPY - HORMONES AS DRUGS!
Birth control (progesterone & estrogens)
Treat hormone deficiencies (all kinds of hormones)
Facilitate sex/gender transitions
Treat cancers (reproductive hormones)
Improve growth (growth hormone)
Treatment of auto-immune diseases & respiratory disorders (Steroids)
Diabetes treatment (insulin)
GENDER AND DRUG USE:
BASIC STATS
According to the NIH, men are more likely to use almost all types of illicit drugs than women
Illicit drug use is more likely to result in emergency room visits or OD deaths for men
For most age groups man have higher rates of use or dependence on illicit drugs and alcohol than do women
Women are just as likely to develop a substance use disorder
CANNABIS AND GENDER
Fewer women report use
Reported effects are different from male users
Different highs
Different performance effects
Different risks
Some variation may be linked to sex hormones
STIMULANTS (COCAINE & METHAMPHETAMINE)
Research suggests that people with more estrogen may be more vulnerable to the reinforcing effects of stimulants)
Women may be more sensitive to effects of cocaine
Amphetamines and weight loss -> more use by women
Women may be more receptive to treatment
MDMA (ECSTASY & MOLLY)
May produce stronger hallucinatory effects in women though men have higher blood pressure increases
Young women are more likely to die from MDMA related complications having to do with
WHAT DOES HARM REDUCTION LOOK LIKE?
SO WHAT IS HARM REDUCTION WHEN IT COMES TO DRUGS?
HARM REDUCTION IS A SET OF PRACTICAL STRATEGIES AND IDEAS AIMED AT REDUCING NEGATIVE CONSEQUENCES ASSOCIATED WITH DRUG USE. HARM REDUCTION IS ALSO A MOVEMENT FOR SOCIAL JUSTICE BUILT ON A BELIEF IN, AND RESPECT FOR, THE RIGHTS OF PEOPLE WHO USE DRUGS.
KEY PRINCIPLES OF HARM REDUCTION
Accepts, for better or worse, that licit or illicit drug use is part of our world and chooses to work to minimize its harmful effects rather than simply ignore or condemn them
Establishes quality of individual and
Ensures that people who use drugs and those with a history of drug use routinely have a real voice in the creation of programs and policies designed to serve them
Recognizes that the realities of poverty, class, racism, social isolation,
Understands drug use as a complex, multi-faceted phenomenon that encompasses a continuum of behaviors from severe use to total abstinence, and acknowledges that some ways of using drugs are clearly safer than others
Calls for the non-judgemental, non-coercive provision of services
Affirms people who use drugs (PWUD) themselves as the primary agents of reducing the harms of their drug use and seeks to empower PWUD to share information and support each other in strategies
HARM REDUCTION INTERVENTIONS
(H)arm (R)eduction:
A philosophical
A FRAME FOR THINKING ABOUT HARM REDUCTION
RISK
What issue is being presented?
What other possible sources of harm might be connected to the main issue?
What drug is being used? What is the risk of overdose?
SET
How are they feeling? Confident? Angry? Anxious?
Are they physically in pain or hurt? Do they need to get well?
Can they engage with you fully? Are their basic needs being met?
HARM REDUCTION AND CURRENT US DRUG POLICY
Harm Reduction
Harm reduction is an evidence-based approach that is critical to engaging with people who use drugs and equipping them with life-saving tools and information to create positive change in their lives and potentially save their lives. Harm reduction is a key pillar in the U.S. Department of Health and Human Services' Overdose Prevention Strategy.
HOW DOES SAMHSA HELP?
Mostly through funding and grants for organizations doing hard reduction
Grants can be used for
Harm reduction supplies
E.g. overdose reversal supplies, substance test kits, food, condoms, etc. Does not include drug paraphernalia such as clean needles
Some Harm reduction services (not all)
E.g. overdose reversal education and training services, referrals to Hep vaccinations, information on local resources and referrals for prep, provision of education
WHAT ARE THE EFFECTS OF THESE RELATIVELY MODEST HARM REDUCTION POLICIES?
This includes more treatment
Better medications
Some accessible through the ACA
In the last year we have seen the first decrease in overdose deaths since 2018
Saving some 16,000 people (according to CDC)
KEY TERMS
Decriminalization: The process through which the legislature removes criminal sanctions against an act, omission, article, or behavior which is considered a crime. --there is no punishment or prosecution, no consequences are enacted even though it remains technically illegal.
Legalization: The process whereby the use, possession, or production of a substance or a behavior is permitted by law and thus is subject to regulation.
DECRIMINALIZATION: WHAT DOES THIS LOOK LIKE?
Examples: Portugal, the Netherlands, some US states such as Oregon
Possession and use are technically illegal but…
No criminal penalties for possession or use
May be civil or administrative penalties
Does not change production, distribution, or supply of drugs - drugs are still procured through the black market, underground trade, etc.
Does not appear to increase drug use
LEGALIZATION
Drug possession and use are legal
Regulations control production, distribution, and supply (age limits, purchasing limitations, quality control, etc. e.g. alcohol, cigarettes, etc.)
No penalties if regulations are complied with
May be criminal penalties if regulations are not followed
Dramatically alters drug production, supply, etc. brings drug production and sale under purview of government and regulatory bodies
Increases safety may lead to some increased use…
SOME OF THE EFFECTS OF LEGALIZING CANNABIS
Several studies have shown that in places where cannabis has been legalized, its use has increased (Martins et al. 2021)
Legalization DID NOT lead to more frequent use or higher rates of cannabis misuse disorder (Martins et al. 2021)
Legalization has not been associated with an increase in the use of other drugs (Zellers et al., 2023).
PORTUGAL: ONE POTENTIAL SUCCESS STORY
PORTUGAL STORY
By the late 1980s, one in every 10 Portuguese was struggling with heroin addiction, overdose-related deaths were on the rise, and the rate of HIV infection in the country was the highest in the European Union
In 2001, Portugal took a radical approach to the problem: it decriminalized all illicit substances, even heroin and other opiates, and implemented harm reduction policies to help addicts get treatment.
Portugal's policy rests on three pillars:
There's no such thing as a soft or hard drug, only healthy and unhealthy relationships with drugs;
An individual's unhealthy relationship with drugs often conceals frayed relationships with loved ones, with the world around them, and with themselves;
The eradication of all drugs is an impossible goal.
The effects of these policies depend on how you look at the outcomes (e.g. Hughes & Stevens 2012 reading)
However, the consensus is there were:
Reductions in drug-related deaths
Reductions in drug-related infectious disease incidence
Reductions in rates of problematic drug usage
Reductions of the burden of drug-related crimes on the criminal justice system
Slight increases in recreational drug use (but now when compared to other European countries)
KEY TAKEAWAYS FROM PORTUGAL STORY
Enormous Cultural Shift aka shift in Language
Transformation of law to echo societal shifts
Officially adopting the policy of decriminalization
Better coordination of health, housing, and drug management departments of the government
ABOVE ALL, A willingness to rise above the view that harm reduction methods are state-sponsored drug addiction strategies
WHICH DRUGS SHOULD BE LEGAL AND WHY?
Historical & cultural patterns of use
Mechanism of action
Comorbidities
Risk of addiction
Associated mortality
Medical benefits
Synthetic v. naturally occurring
"SOFT" V. "HARD" DRUGS
Many draw the lines of what should be legal at hard v. soft drugs
These are arbitrary categories
Often soft drugs include: cannabis, mushrooms, some organic hallucinogens (psilocybin, DMT from plant products, etc.)
Hard drugs usually include: cocaine and its derivatives, opioids (heroin, fentanyl, etc.), meth, PCP, ketamine, ecstasy, hallucinogens like LSD
NATURAL V. HUMAN-MADE
"Natural" - drugs available in nature without significant processing or human handling
E.g. cannabis, mushrooms, salvia, peyote, ayahuasca, other plant or animal-based hallucinogens
Would opium count?
Human-made - Synthetic versions or heavily processed drugs
BIG PHARMA
Scientific difficulties including identifying new chemical matter with unique properties required and funding and lack of financial incentives are two explanations for…
WHAT IS THE LACK OF DEVELOPMENT OF NEW ANTIBIOTICS?
THIS MARKETING
WHAT IS DIRECT TO CONSUMER ADVERTISING?
The high price of insulin that causes low-income families in the US to choose between life-saving medicine and food
WHAT IS STRUCTURAL VIOLENCE?
The use of any of various legal, business, and technological strategies by which producers extend the lifetime
WHAT IS EVERGREENING?
This drug is what keeps diabetics alive but costs an exorbitant amount in the US
What is insulin?
ALL ABOUT OPIOIDS
The deaths of Black folks associated with crack in the 80s & 90s and opioid
WHAT ARE DEATHS OF DESPAIR?
Naming this as a sixth vital sign helped set the stage for the opioid crisis
WHAT IS PAIN?
Despite its origins in the Middle East and its earlier presence in India, Opium has
WHAT IS CHINA?
This opiate alkaloid is chemically similar to morphine and codeine but can be used to product naloxone
WHAT IS THEBAINE?
This synthetic opioid has led to a surge in deaths since its introduction
WHAT IS FENTANYL?
Sex/gender & diet drugs
This measure does not assess body fat
WHAT IS BODY MASS INDEX (BMI)
The cultural constructions and expectations we have that are often observed, performed
WHAT IS GENDER?
The fact that people internalize surveillance and self-regulate is a lesson of this metaphor from Foucault
WHAT IS THE PANOPTICON?
Because we don't know their long-term effects, it is possible that Ozempic and Wegovy can be considered in this phase of clinical trials which can take place after the drug is available
WHAT IS PHASE 4?
The birth control pill, insulin, and growth hormone treatment all show that hormones can be…
WHAT ARE DRUGS?
DEPRESSION & ADHD MEDs
A combination of psychiatric and somatic symptoms that is considered to be a recognizable
WHAT IS A CULTURE-BOUND SYNDOME?
WHAT NEUROTRANSMITTER DO MOST ANTIDEPRESSANTS WORK TO INCREASE?
WHAT IS SEROTONIN?
IN JAPAN DEPRESSION MANIFESTS IN A UNIQUE FORM ANS IS ASSOCIATED WITH…
WHAT IS OVERWORK?
The underlying physiological basis of depression is a depletion in the levels of serotonin, norepinephrine, and/or dopamine in the central nervous system is called
WHAT IS THE MONOAMINE HYPOTHESIS
WHAT TYPE OF DRUG IS USUALLY TREATED TO TREAT ADHD?
WHAT ARE AMPHETAMINES?
Addiction & Drug Policies
THIS IS THE PLEASURE CENTER OF THE BRAIN THAT IS IMPLICATED IN ADDICTION
WHAT IS THE NUCLEUS ACUMBENS?
THIS CONDITION PUTS PEOPLE AT RISK OF DRUG RELAPSE
WHAT IS STRESS?
THIS UNDERSTANDING OF ADDICTION SEES DRUG USE AS A DISTINCTIVE SUBCULTURE
WHAT IS THE LIFE STYLE MODEL?
NALOXONE DISTRIBUTION AND NEEDLE EXHCHANGES
WHAT IS HARM REDUCTION?
THESE TWO NEUROTRANSMITTERS ARE INVOLVED IN THE BIOLOGY OF ADDICTION
WHAT ARE DOPAMINE AND GLUTAMATE
The War on Drugs
This president officially started the War on Drugs
WHO IS RICHARD NIXON?
THIS REPRESENTS ONE OF THE MOST SIGNIFICANT DOMESTIC IMPACTS OF THE WAR ON DRUGS
WHAT IS MASS INCARCERATION
THIS US INSTITUTION WAS USED TO TRAIN MILITARY PERSONAL WHO WENT ON TO COMMIT
WHAT IS THE SCHOOL OF THE AMERICAS?
The disproportionate penalties for these two drugs are examples of how the drug war was used to oppress certain segments of the US population, specifically
WHAT ARE CRACK AND COCAINE?
The largest and most troublesome domestic effect of the US war on drugs that has a negligible effect on public safety
Mass incarceration