bpk110 final
Chapter 1
1.2 - nutrients and non-nutrients
Nutrition is the scientific study of food and nutrients and their effects on body structure, function and health.
Some of these nutrients are essential, meaning that the body cannot make them itself and that they must be obtained from the diet. For example, essential amino acids, essential fatty acids, vitamins, minerals and water are all essential nutrients
Carbohydrates, lipids, protein and vitamins are organic nutrients. water and minerals are inorganic because they do not contain carbon.
Phytochemicals, alcohol, caffeine and toxins are naturally found in some of the foods and beverages we consume. They are sometimes referred to as non-nutrients because they are not required for the growth and survival of the organism but are nonetheless found in
Food.
Phytochemicals, or plant chemicals, are non-nutrients found in plants that may have positive health effects. For instance, they are believed to be partly responsible for the reduced risk of cardiovascular disease and cancer in those who consume higher amounts of fruits and vegetables
Flavonoids tend to promote a bright blue, red or dark colour pigmentation in plants. They are abundant in parsley, blueberries, black tea, citrus fruits, wine and cocoa
Carotenoids contribute to the yellow, orange and red colours found in plants such as pumpkins, sweet potatoes, carrots and squash. Like flavonoids, they have antioxidant effects
Toxins are naturally occurring substances found in plants and animals that can have harmful effects on the body. These include discarding old, moldy, bruised, damaged or discolored food or food that does not smell fresh or has an unusual taste
1.3 - whole foods vs. processed foods
fortified, which involves increasing the amount of nutrients in the food beyond what was there originally.
whole foods are those that remain as close to their natural form as possible. These foods have had little to no refinement and/or processing as well as few or no additives and/or preservatives. Conversely, processed foods are those that have undergone significant changes to their original form.
ultra-processed foods have been linked with several health concerns. For instance, one study found that Canadians that consumed the highest amounts of ultra-processed foods had a 31% increased risk of obesity, a 37% increased risk of type 2 diabetes and a 60% higher risk of high blood pressure
Group 1: Unprocessed or Minimally Processed Foods
These include plants and animals that have had minimal alterations. They are typically found intact and with minimal packaging. They are often found in meals cooked at home or in restaurant kitchens. These foods may still have been dried, crushed, roasted, boiled, refrigerated or pasteurized, which are processes meant to preserve foods as close to their natural form as possible.
Group 2: Processed Culinary Ingredients
These include oils, butter, sugar and salt. They are made from foods found in the first category by pressing, refining and grinding them. These are typically used in combination with foods from group 1 and are not typically consumed on their own.
Group 3: Processed Foods
These are typically made from combining group 1 and group 2 foods. They include canned foods, cheese, breads and fruits in syrup. Typically, processed foods have more than one processed culinary ingredient added to a formerly unprocessed or minimally processed food. These foods are typically made to enhance shelf life, taste and marketability.
Group 4: Ultra-processed Foods
These foods have minimal amounts of group 1 ingredients. Instead, they are made almost entirely from the processed ingredients found in group 2 and group 3 foods. They include lower-cost ingredients such as sugar and salt. They are often found in brightly coloured packages and sold in convenience stores. Sugar-sweetened beverages, chocolate bars, candy,
pre-packaged frozen dinners and deli meats are all examples of ultra-processed foods. Manufacturers make these foods to improve shelf life, taste, marketability and ultimately profit.
1.4 - organic foods
organic means that a substance contains carbon.
Organic foods are foods that have minimal synthetic or artificial inputs and are grown, raised and harvested in a way that preserves biodiversity. organic foods are not genetically modified and are farmed without the use of hormones and unnecessary antibiotics.
there has been to correlation that organic foods help you lose weight organic foods can be found in each NOVA category
1.5 - genetically modified foods
Genetically modified foods, also known as genetically engineered foods or genetically modified organisms, are foods that have undergone alterations to their DNA through the process of genetic engineering.
There are many other foods that are genetically modified, such as so-called cash crops. Cash crops are those that are heavily produced, sold and traded, such as corn and soy. Soy alone accounts for about half of all commercially available genetically modified foods worldwide
The high profit potential of genetically modified foods means that they are often favored and less varieties of plants may be planted.
Food additives are substances added to food for the purpose of taste, appearance, safety, freshness or other factors. There is a wide range of food additives, including preserving agents like sodium nitrate, thickening agents like guar gum and sweeteners like high-fructose corn syrup.
Food additives are typically found in processed and ultra-processed foods. Anyone concerned about the effects food additives might have on health can easily minimize them by consuming more unprocessed NOVA group 1 foods.
1.6 - why do we eat
Nutrients contribute to our anatomy in various ways. Except for vitamins, nutrients can be found within most body cells
The body is 60–70% water by weight, most of which provides structure to cells.
not all nutrients promote body structure (like vitamins)
The study of body functions is called physiology.
Homeostasis is a state of dynamic equilibrium that allows our bodies to function optimally.
The body needs energy in order to perform its various functions and keep us alive. This is known as basal metabolism. In addition, the body needs energy to be able to perform the various activities we do throughout the day. The more active an individual is, the more energy they require
Carbohydrates, lipids and proteins are the energy-yielding nutrients, providing 4, 9 and 4 kilocalories
In addition to eating to support structure, function and energy needs, we also eat because we simply enjoy it
1.7 - diet and health
There are many other modifiable and nonmodifiable factors that also affect our disease risk. Modifiable risk factors include whether a person smokes, is inactive or experiences a high degree of stress in their life. Unmodifiable risk factors include gender, age and genetics.
Though diet cannot change the sequence of DNA we inherently have in our cells, it can affect the way genes are expressed. The study of this interaction is called nutritional epigenetics. Nutritional epigenetics explores how the foods we eat can change DNA expression, even
if the DNA code stays the same.
Agouti mice have an altered version of the agouti gene. This genetic change causes the mouse to have both a yellow coat colour and obesity. Researchers fed pregnant agouti mice either a normal diet or one that was rich in something called methyl groups. The litter of mice from the mother who was fed the normal diet were like their mother – yellow, obese and prone to disease. However, the pregnant mice that were fed the methyl-rich diet produced a litter that
was more brown, lean and not prone to disease
Balance means consuming foods in the right proportions. Dietary balance means to have things in the right proportions. This applies to the nutrients and energy we consume but also to the general choices we make.
This means that 80% of our nutritional decisions should be ones that promote health, while
20% can be less healthy
1.8 - choosing a healthy diet
Dietary variety means consuming a diversity of foods.
Moderation means not too much and not too little. In other words, it ensures that our diets are adequate, so we do not develop nutritional deficiencies, but not excessive to the point where they promote complications.
Nutrient density refers to the amount of nutrients in a food or meal as compared to a reference amount. Typically, a 100 kcal reference amount of food is used.
The science of ranking foods based on nutrient density is called nutrient profiling.Consuming more of these NOVA group 1 foods and less of the group 3 and 4 foods, can increase the nutrient density and healthfulness of our diets
1.9 - the study of nutrition
Experimental studies are often called randomized control trials. They are the gold standard for making inferences from research. This is because they control all variables, except for the one factor that is being studied.
Using this controlled procedure means that when an effect is seen after a study, it is most
likely due to that one variable that was changed, the group receiving the dietary supplement is the experimental group, while the one that didn’t receive the supplement that was used for comparison purposes is the control group. To reduce the risk of intentional or unintentional bias that could affect the results, control groups are often given a placebo.
A blind study means that neither the experimental nor control group knows
which group they are in. They just know what the experiment is about and that they might receive an active treatment or a placebo.
A double-blind study is one where neither the scientists nor the subjects know which group is receiving the experimental treatment and which is receiving the placebo
While experimental studies are best at establishing causality, human nutrition studies are difficult to perform and have several limitations
Epidemiological studies, also known as population-based studies, look at trends in populations without manipulating any variables. A critical point to understand about epidemiological studies is that association does not equal causation. For instance, just because a link was found between two factors (i.e., saturated fat and cardiovascular disease) it does not mean one leads to the other (i.e., high saturated fat intake leads to cardiovascular disease). In epidemiological studies, We cannot control all the variables that may influence disease.
prospective epidemiological design, where a large, similar group is followed forward through time. Another major weakness of epidemiological studies is the lack of accuracy in determining a population's diet. For instance, how do we accurately gauge the quality and quantity of a person’s diet?
Anecdotal evidence is what is typically used to sell products and sway opinions. Anecdotes
are personal testimonies drawn from direct or indirect casual experiences. For instance, an Instagram post may feature an influencer selling a weight loss supplement with a before and after photo stating how well the supplement worked for them.
it is also imperative that this data is analyzed properly and thoroughly evaluated, and that
accurate conclusions are drawn. This typically takes the work of a skilled research team whose work is further reviewed and assessed through a process called peer review. Before a scientific article can be published, it must be reviewed by experts in the field who were not involved in the study process to make sure the study was properly conducted, the results were properly analyzed, and conclusions were properly drawn
Primary journal articles, those that summarize a scientific study, are often highly specific and it may be challenging to find more general answers.
Review articles may be more helpful for general questions,
Systemac reviews involve a panel of topic experts reviewing a wide range of primary research studies and evaluating the strength of evidence to support or not support a phenomenon.
in Western science we reduce food to its nutrient content and then study the effects of individual nutrients on the body. We see food as a non-living thing that we take from the earth for our own benefit. Conversely, traditional and modern Indigenous cultures typically see food as a dynamic, living entity, one that forms part of our relationship with each other and the land. They may give to their food system as much or more than they take from it.
Chapter 2
2.2 - determining nutrition status
Nutritional status is the condition of the body with respect to nutrition. It helps us determine whether a person has the appropriate level of nutrients to meet their needs.
A dietary analysis typically involves three main steps:
1. Recording everything a person ate for a period.
2. Comparing recorded intake levels to specific recommendations.
3. Determining whether the person’s nutrient status is adequate, deficient or excessive.
To get an accurate diet analysis, we must be as specific as possible with respect to the amounts and types of foods we eat.
Laboratory tests use blood samples to determine nutritional status. For instance, a test called a blood lipid panel looks at the levels of certain lipid-based compounds in the body to see if they are within a healthy range
2.3 - dietary reference intakes
The dietary reference intakes (DRIs) are a set of scientifically determined reference values for nutrient requirements. They tell us how much of a nutrient is required to meet the needs of an individual. These requirements vary depending on gender and stage of life.
At the population level, they can be used to inform dietary recommendations. Canada and the USA use the same four DRIs.
The estimated average requirement (EAR) is the amount of a nutrient that will meet the needs of 50% of the population. For example, the EAR for calcium for those aged 19–50 is 800 mg/day. If a population consumes the estimated average requirement of a nutrient, the vast majority will not be adequate for that nutrient. (EAR meets the needs of only 50% of the population)
The recommended dietary allowance (RDA) is the amount of a nutrient that meets the needs of 97% of the population. The RDA is set at two standard deviations, about 20–25%, higher than the EAR. For example, the RDA for calcium for those aged 19–50 is 1000 mg/day, 25% higher than the EAR of 800 mg/day.
If we cannot determine the EAR, then an RDA cannot be set.
there is not enough scientific data to establish the EAR and RDA. In such cases, an adequate intake (AI) value is used. The AI is typically determined by observing how much of that nutrient healthy people eat. Since these individuals do not show signs of deficiency, it is assumed that this amount is adequate for most healthy people.
The tolerable upper limit (TUL), or upper limit (UL) is focused on excess. If we consume an
amount of nutrient in excess of its UL, we are more likely to show signs of toxicity. Many nutrients do not have an upper limit - meaning we do not have sufficient evidence to show that they cause symptoms of toxicity above a certain level
2.4 - energy recommendations
Energy intake recommendations come in two main forms. The estimated energy requirement estimates the total amount of energy needed to maintain a person’s current size. In contrast, the acceptable macronutrient distribution range gives recommendations for the percentage of energy to come from each of the three energy-yielding nutrients.
Energy needs vary by person. To maintain energy balance, energy intake and energy expenditure need to match. Our EER does not increases with age
Energy expenditure can also be estimated using the EER calculation
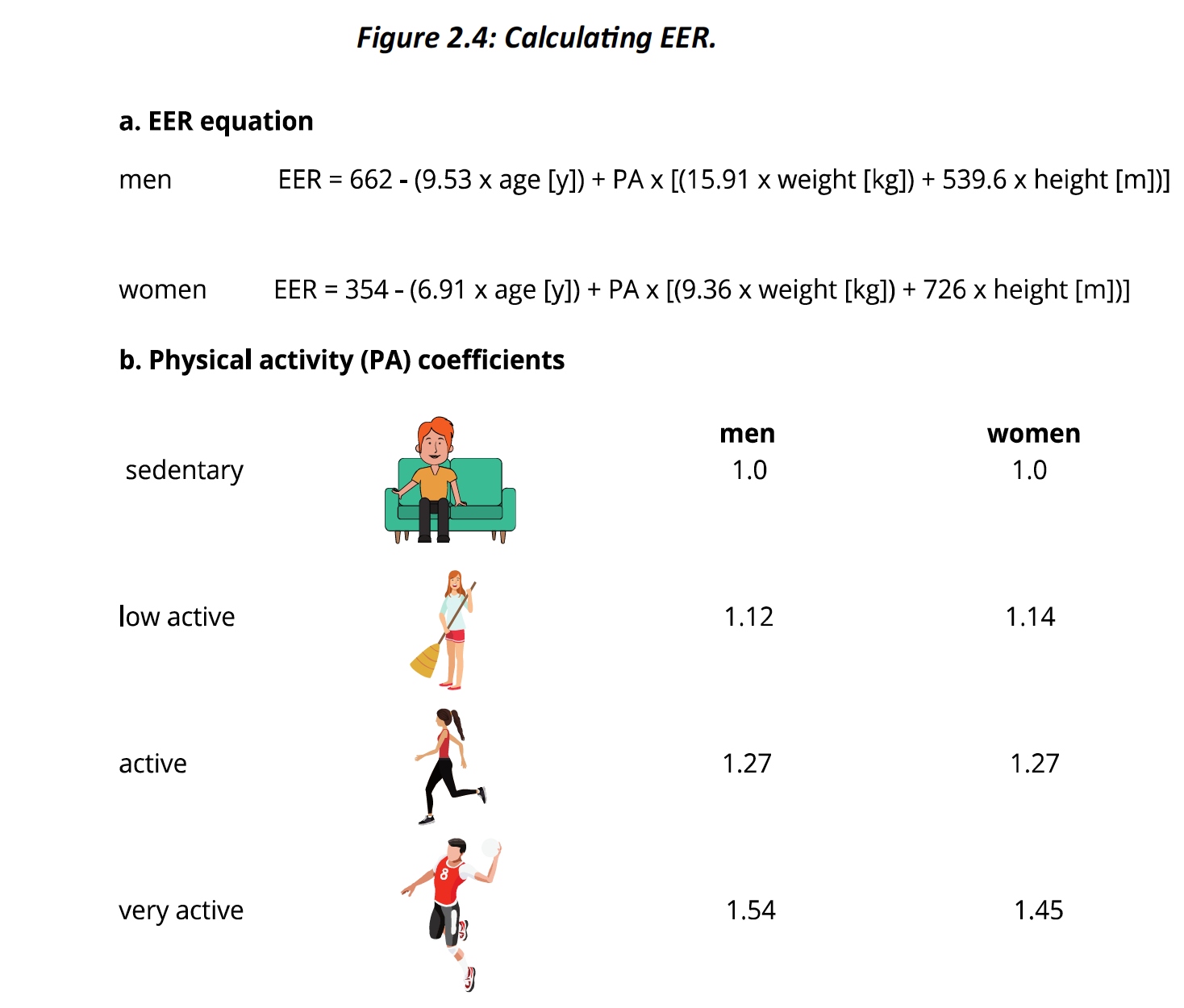
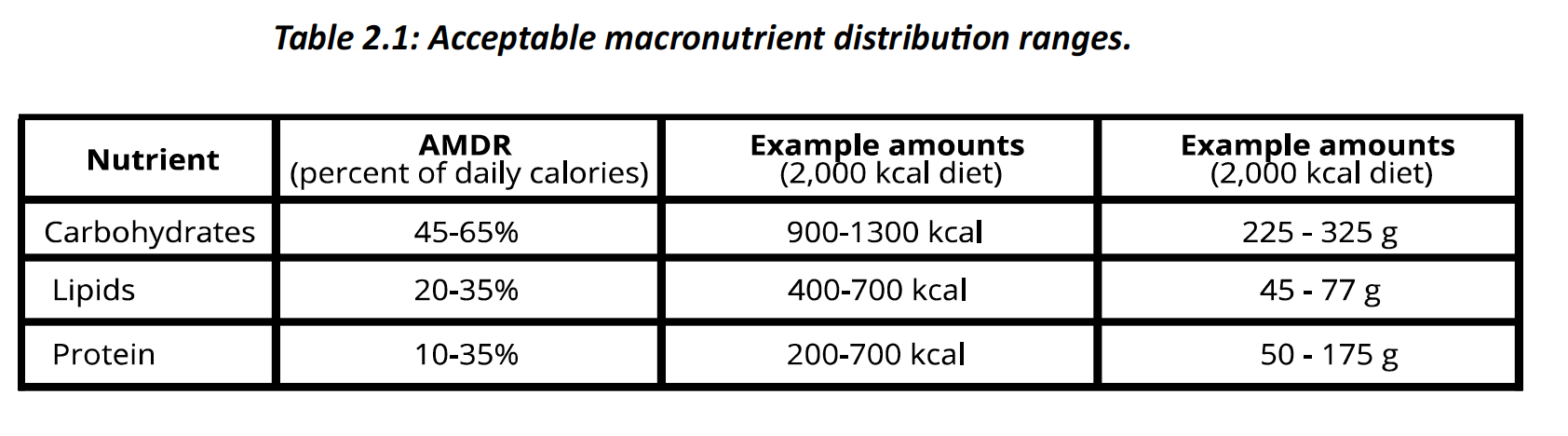
The acceptable macronutrient distribution range outlines the recommended percentage of energy that should come from each of the three energy-yielding nutrients: carbohydrates, lipids and proteins.
2.5 - canada’s food guide
Canada was one of the first countries to have a food guide. The newest Canadian food guide was released in early 2019. It has since been translated into many languages, including several Indigenous languages to reflect the diversity of Canadians.
50% of the plate is vegetables and fruits. Note that the word vegetable comes before the word fruit. This is meant to communicate the foundational role of these plants in the diet.
The food guide recommends consuming whole vegetables and fruits over juices
and concentrates, which tend to be processed and high in added sugar.
25% of the plate is whole grains. These foods are the staples in many diets and the guide communicates the importance of consuming unrefined versions of them. Whole grains are those that have had been minimally processed and make use of the entire grain in food
prepatiraon. They include whole-grain wheat, whole-grain bran and whole-grain rye. Whole-grain foods are a good source of fiber, vitamins and minerals
25% of the plate is protein-rich foods. While protein can be found in all sections of the plate, the foods in this quadrant are especially high in protein. These protein-rich options are of both animal and plant origin, so both vegetarians and omnivores can build a healthy plate that fits their lifestyle. It prioritizes beans, peas, lentils, nuts and seeds over animal-based protein
The 2019 Canadian food guide does not organize foods into four groups; the food groups concept was found on previous guides, not the newest edition.
The guide also has several key themes:
Variety. The plate has a wide range of foods in each second.
Accessibility. The plate features foods that are relatively inexpensive for most people.
Cultural relevance. Given the diversity of the Canadian population, there are foods that are key staples to many ethnic diets, such as rice and beans.
Availability. The guide features options that are available at times of year in different forms, either fresh, frozen, canned or dried.
Being mindful of our eating habits means being aware of how, why, when, how much and where we eat. This recommendation is meant to help us develop a more positive relationship with foods and to be aware of the feelings, thoughts, emotions and behaviors that are associated with food intake
Cooking more often can help us include more whole foods in our diet, while also improving the experience we have with food
Eating meals with others can not only improve our experience with food but can also promote social and mental health
Reading labels can help us compare products and be aware of the types of ingredients and nutrients in foods. This can help us make more informed and healthy food decisions
Limit foods high in sugar, sodium fat.
Be aware of food marketing. Advertising’s main goal is to sell products, not to promote health
2.6 - other food guides
Within the First Nations group, there is a wide diversity of nations, each with their own cultural practices and beliefs. As such, there is not a single set of traditional or current dietary practices. That said, there is consensus that traditional aboriginal diets had many healthy principles. For one, they were environmentally sustainable, as they focused on local seasonal plants and animals.
For instance, the American Dietary Guidelines (U.S. Department of Health and
Human Services & U.S. Department of Agriculture, 2015) focus on the following key messages:
• Follow a healthy diet across the lifespan.
• Focus on variety, nutrient density and amount.
• Limit calories from added sugars and saturated fats and reduce sodium intake.
• Shift to healthier food and beverage choices.
• Support healthy eating patterns for all.
Some inspiration for the Canadian food guide came from the 2014 Brazilian Dietary Guidelines. This set of recommendations was the first country-level dietary advice to focus more on food behaviors than on the specific content of the diet.
2.7 - canadian food policy
Food labels communicate information about packaged foods so consumers can make informed decisions.
These labels must adhere to requirements stipulated by the Food and Drug Regulations. The regulations were amended in 2016 and have undergone significant changes as compared to previous labeling guidelines
Required components of a canadian food label: (6)
The common name of the food. This name must appropriately represent the food. For instance, a food cannot claim to be apple juice if it is made from apple flavoring and sugar. A brand name may also appear on a food label, but this is not mandatory. The brand name must not mislead the consumer in any way.
Net quantity. This tells the consumer the total weight, volume and/or contents of the entire package. The common name and net quantity must appear on the primary display panel of the package – the part of the package that is primarily displayed or visible to the consumer.
Name and address of the producer and/or distributor. This is meant to provide accountability for the product, so the consumer can contact them if necessary.
Date marking. Also known as the best-before date, the date marking tells the consumer the date after which the product will lose its quality characteristics. This includes the time it might take for freshness, taste and appearance to diminish. These are mandatory on foods with a shelf life of less than 90 days.
Ingredients list. Ingredients must be written in descending order of each ingredient’s weight before being combined with any other ingredients during preparation.
Nutrient facts box. This outlines the nutritional composition of the food according to the key nutrients mandated by Health Canada. New labeling requirements have shied which nutrients are included and how the box is represented. The nutrient amounts are often expressed in grams and daily values. The daily value compares the amount of nutrient in a serving size to an appropriate DRI.
Food packaging may also display certain claims to highlight a nutrient, health-associated factor or the nature of a food. These claims are voluntary, cannot purposely deceive consumers and must abide by the regulations set out by the Food and Drug Regulations of Canada
Nutrient content claims describe the amount of energy or specific nutrient in a food. These include statements such as low in fat, lower in Calories and high in fiber. Ex: to state that a product is low in fat, it must contain 3 g or less of fat per serving and 30% or less of the energy in that product can come from fat.
There are two general categories of health claims: disease reduction claims and function
Claims.
Disease reduction claims link a food or its ingredients with a reduced risk of developing a specific disease. In order to make these claims, a prescribed type of wording must be used, and the food must meet the criteria set out by the
Food and Drug Act.

Function claims note the association between consuming a nutrient or diet factor with its role in the normal biological function of the body. There are two permitted nutrient function claims that can be used for all nutrients: Energy (or name of the nutrient) is a factor in the maintenance of good health and Energy (or name of the nutrient) is a factor in normal growth and development.

mandatory front-of-package labeling for foods high in sodium, sugar and saturated fat.
Symptoms of foodborne illness, often called food poisoning, are unpleasant and can involve nausea, diarrhea, vomiting, abdominal cramps and fatigue. In some cases, as in the case of E. coli or botulism poisoning, it can be fatal. Foodborne illness occurs due to harmful infectious agents that can sometimes be present in food.
Items sold as vitamins, minerals, multivitamins, probiotics, amino acids and essential fatty acids, as well as homeopathic and traditional medicines are considered natural health products (NHPs) They are naturally occurring substances that may be used to address health needs.
In order to receive a license, the manufacturer must provide safety and efficacy evidence to the government. Clinical trials and studies published in reputable scientific journals or publications are permitted types of evidence. A list of medicinal and non-medicinal ingredients, as well as the source, dose, strength and recommended uses must also be provided
Menu labeling - There is currently no Canada-wide regulation requiring restaurants and other eateries to list nutritional information on their menus.
Partially hydrogenated oils are now prohibited in food processing. As per the newest food policy they are not prohibited and are being phased out of the food supply
In addition to grams, nutrient amounts on a nutrient facts box may also be expressed in daily value
The micro nutrient potassium was not found on previous nutrient facts box, but must listed in the updated versions
“Contains strawberries” is an example of a highlighted ingredients claim
Chapter 3 - part 1
3.2 - digestion
For the body to use these nutrients, they must be broken down into their subunits
Digestion separates the nutrients in food and breaks larger molecules into smaller ones. Polysaccharides (long chain carbohydrates), triglycerides and proteins cannot be absorbed as they are found in food. They must be broken down into sugars, fatty acids and amino acids, respectively, in order to pass through the membranes of internal cells.
Mechanical digestion, also known as physical digestion, uses physical process like our teeth chewing and stomach churning to break food apart
chemical digestion uses enzymes to alter the chemical structure of nutrients and reduces them to their building blocks
Enzymes allow reactions to occur quick enough to meet the body’s needs. Various enzymes facilitate the breakdown of energy-yielding nutrients. For example, when the enzyme sucrase is present in the small intestine, the two-sugar molecule sucrose is broken down more quickly into its building blocks, glucose and fructose
This suffix tells us that a structure is an enzyme -ase
hydrolysis reaction, where the input of water (hydro) helps to break down (lysis) the molecule.
Unlike hydrolysis reactions, condensation reactions combine molecules by liberating a water molecule
Hormones are chemical messengers that are required for many physiological processes, including digestion. During digestion, hormones communicate information about specific parts of the digestive tract to the brain and other digestive structures.
3.3 - the digestive system
Sphincters are found between certain organs and regulate passage from one organ to the next. They are composed of circular muscle that contracts to close openings and relaxes to open them.
The lumen is the inner cavity of the small intestine tube; it is where you will find food and digestive secretions
Transit time through the digestive tract is ~2+ days. The bulk of this time is due to time spent in the: large intestine
If the lower esophageal sphincter does not properly close, acid can spill into the esophagus
Hydrochloric acid denatures protein and activates the enzyme pepsin. Pepsinogen is not a functional enzyme - needs to be activated into pepsin by HCl
Mouth
Saliva is secreted into the mouth to facilitate digestion
significant mechanical digestion. Our tongue is a powerful muscle that helps mix foodstuffs with saliva and water and helps to push this food forward towards our teeth.
Once food has been chewed and mixed with saliva, it forms a uniform cohesive
structure called a bolus.
Pharynx
commonly known as the throat. When we swallow, the pharynx moves to receive the bolus
of food from the mouth. If we put our hand on our throat and swallow, we might feel this upward movement. The pharynx is a common passageway for both food and air
When we are not eating, the pharynx opens to the trachea, allowing air to flow in and out of our lungs. However, when we are eating, we want the food to move from the pharynx into the more posteriorly oriented esophagus. This process involves a flap of tissue called the epiglottis.
Esophagus
It is merely a conduit for food from the pharynx to the stomach. peristalsis uses waves of muscle contraction to move a bolus of food forward. Gravity also aids in the downward movement of food towards the stomach.
Stomach
The stomach is also where the chemical digestion of protein begins. A small amount of absorption occurs here, but it is limited to the partial absorption of water and amino acids. Most digestion and absorption occur further down in the small intestine. By the time food leaves the stomach, it is no longer a solid bolus, but a semiliquid substance called chyme
churning. Stomach churning promotes mechanical digestion. It also facilitates chemical digestion by mixing foodstuffs with enzymes.
Gastric juice contains several substances that facilitate digestion, while protecting the stomach walls:
Mucus provides lubrication and a medium in which chemical reactions can occur.
Hydrochloric acid (HCl) is a highly corrosive acid (pH = 2). It is used to unravel proteins, exposing sites where enzymes can further break them down. It also has a role in activating the enzyme pepsin
Pepsinogen is a proenzyme that is secreted by certain stomach cells. It only becomes an active enzyme when it is acted upon by HCl, which converts pepsinogen into its active form, pepsin. This protease acts on specific sites in amino acid chains, breaking them down into smaller chains.
Small intestine
Large circular folds can be seen along the small intestine’s innermost walls, facing the lumen.These increase the surface area and slow the passage of food along its path. To the naked eye, the surface of these circular folds looks slightly fuzzy. This fussiness is due to millions of villi (singular = villus) – invaginations of the small intestine membrane.
Further adding to the small intesne’s surface area are tiny finger-like projections called microvilli Accordingly, the microvilli are collectively known as the brush border. The brush border is particularly important because it is where certain digestive enzymes are stored, such as lactase, sucrase and maltase
The majority of absorption occurs in the: small intestine
Accordingly, small intestine cells are also secretory cells.
Large intestine
where a minimal amount of further digestion and absorption occur. One of the large intesne’s main functions is to package wastes for easy removal
material moves into the ascending, transverse, descending and sigmoid colons. Collectively, these are referred to as the colon, which makes up the bulk of the large intestine
segmentation also occurs, which breaks material into smaller components while mixing it with digestive juices.
Waste is then held in the rectum, which stores feces until it is ready to be excreted.
Microbiome
microbiome refers to the large variety of non-human genetic material within our bodies due to the presence of these microorganisms. Our microbiome contains about 150 times more genes than human DNA
The term microbiome refers to the different genetic material found in our body due to the presence of microorganisms such as bacteria
microbiota refers to the total composite of microorganisms found in our bodies. While the microbiota includes viruses, fungi and other microorganisms, it is mainly composed of bacteria. There are about 300–500 different species of microorganisms living in our large intestine, totalling about a trillion cells!
3.4 - accessory digestive structures
Pancreas
The pancreas is a gland with two types of functions. It has a blood glucose-regulating function, due to the production and secretion of the hormones insulin and glucagon. Endocrine function of the pancreas. Exocrine function: pancreas secretions that are deposited into the digestive tract
Pancreatic juice contains several digestive enzymes, including protein-digesting protease, lipid-digestion lipase and carbohydrate-digesting amylase.
Bicarbonate (important buffer) neutralizes chyme, making it less acidic and more conducive
to physiological processes.
Liver and gallbladder
The liver has many roles in the body, including metabolism, detoxification and digestion. Its digestive role relates to the production of bile, which promotes lipid digestion.
bile is stored in the gallbladder for quick secretion when needed.
Bile is a lipid emulsifier.
The process of emulsification allows hydrophobic lipids to be suspended in a watery environment; bile salts are required for this process
Chapter 3 - part 2
4.2 - digestive tract in health and disease
Probiotics are found in certain supplements and are also found naturally in foods such as yogurt and kombucha.
Prebiotics are typically medium-length carbohydrates (3–10 carbons in length) that our gut microbes ferment. Sources of prebiotics include asparagus, beet sugar, garlic, onion, wheat, honey, banana, barley, tomato, rye, soymilk, peas, beans and seaweed. They act as food for these bacteria
Ulcers are open sores that can occur along the lining of a body structure. They can occur at multiple points of the digestive tract, including the mouth, esophagus, stomach and small intestine.
Ulcers in the mouth are commonly called canker sores. They are often caused by biting the cheek, eating a lot of acidic food or burning the inside of the mouth.
Peptic ulcers occur in the esophagus, stomach or small intestine. These ulcers are typically related to infection with H. pylori bacteria. In these cases, doctors may prescribe antibiotics.
The lower esophageal sphincter between the esophagus and the stomach can weaken over time. When this occurs, stomach acid can spill upward into the esophagus resulting in a burning feeling called gastroesophageal reflux aka heartburn. If GERD continues, it can lead to the narrowing of the esophagus. It can also promote an esophageal ulcer, which can then lead to a precancerous condition called Barrett’’s esophagus
Irritable bowel syndrome (IBS) affects the large intestine and is associated with symptoms such as abdominal pain, bloating, cramping, diarrhea, constipation and flatulence. Managing stress, finding and avoiding triggers, drinking plenty of fluids, getting adequate sleep and exercising are all recommended. Avoiding foods that promote gas, such as carbonated and alcoholic beverages as well as certain vegetables like broccoli, cauliflower and cabbage, may minimize symptoms
Foods such as broccoli, cauliflower and cabbage may trigger IBS symptoms
Sometimes, the walls of the digestive tract become weakened, leading to the formation of outpouchings called diverticula (singular = diverticulum)
Gallstones are hardened bile deposits that accumulate in the gallbladder or bile duct, the vessel that drains the gallbladder They occur due to an overabundance of cholesterol as compared
to bile salts in bile.
Cancer involves the uncontrolled multiplication and spread of cells. The digestive tract has multiple sites where cancer can occur – both along the tract itself, or within accessory digestive structures. Cancer compromises organ function by blocking important structures from performing and by consuming valuable energy required for proper tissue function
Colorectal cancer occurs in the colon or rectum of the large intestine.
Constipation can be a temporary or chronic condition. It refers to bowel movements that are difficult to pass or less frequent. When these stools are passed, they are typically dry, hard and can be painful to excrete
Chronic constipation can increase the chance of hemorrhoids – swollen blood vessels in the anus and rectum that can become inflamed and painful. Constipation is more likely to occur when matter passes through the large intestine more slowly
When matter passes quickly through the large intestine, a condition called diarrhea can result. Diarrhea is evidenced by loose stools that have a liquid-like consistency. Bacterial and viral infections are the most common causes of diarrhea
4.3 - delivering absorbed nutrients
The liver is a gatekeeper that will do one of four things with these nutrients: use them, store them, send them to the rest of the body or detoxify them
Our liver is also our main detoxification center, neutralizing toxins that enter via the digestive tract or are otherwise found in the blood. Unlike other nutrients, large lipids and fat-soluble vitamins are packaged and enter the lacteal vessels in the small intestine villi. These move through lymphatic vessels, which drain into the blood around the level of the collarbone. They accordingly bypass the liver.
Toxins are substances that can damage our bodies and cause disease. They are found in the environment and the foods we eat
The skin, kidneys, lungs, digestive tract and liver all eliminate toxins. For instance, the liver can convert arsenic to a non-toxic form
There is a lack of quality clinical and randomized-control trial evidence to support the purported health effects of detox diets. While some studies have suggested improvements in symptoms after a commercial detox supplement or program, these studies did not have control groups and had very small sample sizes
4.4 - energy metabolism
Metabolism is the sum of all the chemical reactions that occur in an organism.
Anabolism involves smaller molecules coming together to make larger ones. Anabolic reactions require a net input of energy. Protein synthesis, which combines amino acids into specific chains, is an example of an anabolic reaction that requires an input of energy
Catabolism involves larger molecules breaking down into smaller ones. Catabolic reactions lead to a net release of energy
The released energy from the metabolism of sugars, fats and amino acids is captured by a key molecule called adenosine triphosphate (ATP). ATP can then use this stored energy to fuel chemical reactions ATP is the body’s energy currency. It is the main molecule that provides energy to fuel the body’s various needs.
The cellular respiration of glucose can be summarized by the following equation: C6H12O6 + 6 O2 ——> 6 CO2+ 6 H2O + ATP
Cellular respiration metabolizes these nutrients to capture their stored energy within the bonds of ATP – the body’s energy currency.
The four main steps of the cellular respiration of glucose:
Glycolysis of glucose
Glycolysis, or sugar splitting, is the first step of cellular respiration. In this process, six-carbon glucose is broken down into two molecules of three-carbon pyruvate. Since bonds are broken in this process, energy is released and then captured in two molecules of ATP.
Doesn't require oxygen
Aerobic means with oxygen while anaerobic means without oxygen. During high intensity activities oxygen levels are insufficient to meet the needs of all cells. In such cases, cells can make ATP anaerobically through glycolysis.
Breakdown of pyruvate
Anaerobic metabolism of pyruvate, pyruvate is oxidized to lactate. This produces an acidic environment in the blood that is not sustainable. Luckily, this process is reversible. Most lactate that is produced during anaerobic conditions can be converted back to pyruvate when oxygen is available again. Pyruvate can then proceed through its aerobic breakdown.
Aerobic metabolism of pyruvate, pyruvate forms acetyl CoA with the addition of coenzyme A. This process also leads to the loss of some electrons, which are captured by an electron transporter called NADH+H+. Some carbon dioxide is also released in this process.
The citric acid cycle
The citric acid cycle is a series of chemical reactions that occur under aerobic conditions. acetyl CoA reacts with oxaloacetate to form citrate (the conjugate base of citric acid). This is how the cycle gets its name. Citrate will then go through a sequence of alterations to form eight different molecules in total. During this process, some energy is captured within GTP, an energy currency like ATP. The waste product carbon dioxide is also produced.
electrons are lost and then captured within the electron transporters NADH+H+ and FADH2. These electron transporters then move to the membrane of the mitochondria, where the last and
the most productive stage of cellular respiration can occur.
Electron transport chain
The electron transporters NADH+H+ and FADH2 exchange electrons with these membrane-bound proteins in a series of reactions known as reduction-oxidation
The main function of this process is to create a buildup of protons (H+) on one side of the membrane. As these protons flow back through the membrane, the ATP-creating enzyme ATP synthase is active. ATP synthase promotes the bonding of the phosphate group onto ADP, regenerating ATP. Cellular respiration leads to the production of more than 30 molecules of ATP per molecule of glucose, most of which are synthesized in this last step.
Lipid metabolism
A triglyceride molecule has three fatty acids attached to a glycerol backbone. To metabolize triglycerides, the glycerol and fatty acids first need to be separated
The bulk of the energy derived from lipids comes from fatty acids. Fatty acids are broken down two carbons at a time to form acetyl CoA. This process is called beta-oxidation. Once acetyl CoA is formed, it can enter the citric acid cycle and the remaining steps of cellular respiration occur from there.
Amino acid metabolism
only 5–10% of our energy needs are met through the metabolism of amino acids. Unlike sugars and fatty acids, amino acids have a nitrogen-containing amine group. The first step in using amino acids for energy is the removal of this nitrogen group through deamination
There are 21 amino acids in the human diet, each with a unique side chain. Therefore, after an amino acid is deaminated, there are 21 possible products. These remaining chains can either be used to form glucose, pyruvate or certain citric acid cycle intermediates, which will proceed through the appropriate steps of cellular respiration.
Chapter 4 - Water
5.2 - water overview
A water molecule is composed of two hydrogen atoms attached to an oxygen atom, giving it the chemical formula H2O.the molecule has a V-shape, due to the respective slightly positive (δ+), and slightly negative (δ–) charges of the hydrogen and oxygen atoms
polar molecule - The negative charge forms one pole of the molecule, while the positive charge forms the other pole
Polar molecules that are attracted to and dissolve easily in water are hydrophilic, or water loving.
Those that are not polar and not attracted to water are hydrophobic, or water hating.
The human body is 60–70% water by weight Approximately two thirds of this water is found within cells, or intracellularly, and the remainder is found outside of cells, or extracellularly
The water in cytoplasm therefore accounts for the majority of the body’s water.
Most extracellular water is found within blood. Red blood cells give blood its characteristic colour, however, more than 90% of the volume of blood is water. Water can be exchanged
between this extracellular space and the blood. Certain factors regulate this exchange and the content of water in the blood versus the extracellular space.
Osmosis drives water to move across semi-permeable membranes, like blood capillaries, with the goal of evening out concentration differences.
That is one function of protein: to maintain fluid balance and make sure that water doesn’t build up in the extracellular space.
If there is an area with more dissolved polar substances, water will move towards these.
When blood pressure is higher, there is a greater chance the water will move from blood vessels to the extracellular space
5.3 - water functions
Water helps structures maintain their form. For instance, the water within cells gives them the three-dimensional shape necessary for cellular organelle to function properly.
The eye also maintains its structure because of the fluid, or humour, found within
Water is the most important biological solvent because of the variety of polar substances it can dissolve This is important for moving things around the body via blood vessels or the digestive tract
hydrolysis reactions use water to split larger molecules into smaller ones. An example of a hydrolysis reaction is the breakdown of the double-sugar maltose into two molecules of single-sugar glucose.
Help with defense from infection. Within the lymph you will find many immune cells suspended within a watery environment. If an infectious agent gets into the body, it can be moved to the lymph, where these immune cells can act on it for removal. Furthermore, mucus, which is mostly water, helps trap and gather pathogens together for removal.
Protection from injury - Water can reduce the friction and damage from movement or trauma that can negatively affect our tissues. For instance, the water found in synovial fluid helps protect bones that articulate from scraping against each other
Our bodies accordingly use two main strategies to maintain internal temperature; both involve water. Sweating involves the release of watery sweat from our sweat glands. When this sweat evaporates, it cools down our skin and bodies.
Sweating in a humid environment compromises this process, as the air’s high water content does not let sweat evaporate. This leaves us feeling hot, sticky and uncomfortable
When body temperature increases, as is the case during strenuous exercise, the face often becomes redder. This is because the body tries to maintain its temperature by opening blood vessels close to the skin. This allows blood to shunt some of the heat from the body’s core to the skin’s surface.
Heat stroke occurs when the body temperature rises above 40˚C.
Since the body does not store water, we must constantly replenish this water. Beverages account for most of the water we take in, though foods also provide water.
5.4 - water balance
Water homeostasis is one of the body’s main priorities. To this end, there is a tightly regulated feedback process in place to make sure that water is maintained at desirable levels.
two main mechanisms are employed to help maintain water levels. First, our thirst increases. This is due to several body sensors that indicate to the brain that the concentration of dissolved particles in the blood is high, meaning that the concentration of water is low. Thirst is the body’s way of telling us it is deficient in water. The kidneys also play a key role in regulating water
levels. They decide what stays in the blood and what is excreted in urine
Dehydration can be caused by not consuming enough water or by an excessive loss of water, potentially due to sweating, diarrhea or vomiting.
Symptoms of dehydration include increased thirst, dry mouth, headaches, fatigue, dizziness, irritability and dark urine. Chronic dehydration can lead to more severe complications, including kidney damage, seizures and hypovolemic shock.
Kidney disease
Dehydration puts extra stress on the kidneys, as they do not have enough water to help excrete waste products. This increases the risk of urinary tract infections, kidney stones, and in extreme cases can lead to chronic kidney disease and even death.
Seizures
Excessive sweating not only promotes water loss, but important electrolytes can also be lost in this process. Electrolyte imbalance can compromise the body’s electrical activity, potentially promoting seizures. Those with sodium and other electrolyte disorders are more susceptible to these dehydration-induced seizures.
Hypovolemic shock
Dehydration increases the risk for hypovolemic shock, which occurs when the body loses a lot of blood or extracellular fluid. Low blood volume and pressure can compromise oxygen and nutrient delivery to the tissues.
Symptoms of hypovolemic shock include increased heart rate, low blood pressure, blue skin colour, cool and clammy skin and mental status changes. The symptoms and severity depend on the health of the person and the length of time the person stays in hypovolemic shock. If untreated, it can be fatal.
Water intoxication
Water intoxication, also known as water poisoning, is a potentially fatal condition where the content of water in the body is too high with respect to the level of electrolytes
Water intoxication can occur when an individual consumes excessive amounts of water in a short period of time and does not excrete it through urination. However, most cases of water intoxication occur when a significant amount of water is lost due to excessive sweating, diarrhea or vomiting.
Both water and electrolytes are lost in sweat, diarrhea and vomit. If these losses are replaced by only drinking water, it dilutes the electrolytes in the body.This can result in a condition called hyponatremia, or low sodium in the blood.
5.5 - diuretics
Diuretics are substances that promote water losses through urination. Certain medications act as diuretics, as do certain psychoactive drugs like caffeine and alcohol.
Diuretic pills, sometimes called water pills, are prescribed for conditions such as high blood pressure, kidney stones and tissue swelling. They work by promoting sodium excretion at the kidney, which also promotes water excretion
Caffeine is a psychoactive drug found in certain foods and beverages.While caffeine acts as a diuretic, it is typically consumed for its effects on the central nervous system, as it can promote alertness, while reducing fatigue and drowsiness.
Coffee is believed to have anti-oxidant and an-inflammatory properties that perhaps contribute to the observed effects. While it is generally recognized as safe, caffeine has some potential side effects. The authors of the above study found an increased risk of miscarriage with coffee consumption.
Alcohol is a psychoactive drug found in certain foods and beverages. It has diuretic properties and can affect hydration levels if over consumed. Alcohol also provides energy to the body; each gram provides 7 kcal.
High alcohol intakes significantly increase the risk of liver cirrhosis and cancers of the liver and digestive systems. Alcohol also increases the risk of neurological deficits such as confusion and dementia.
Interestingly, epidemiological evidence suggests that light to moderate drinkers (1–2 servings of alcohol per day) have a lower risk of cardiovascular disease compared to non-drinkers.
Women and smaller individuals have lower total blood volume; thus, alcohol is concentrated more quickly. Blood alcohol also tends to concentrate more before menstruation and during ovulation.
If alcohol is consumed in excess of our energy needs, it will be converted into lipids and stored in our fat cells.
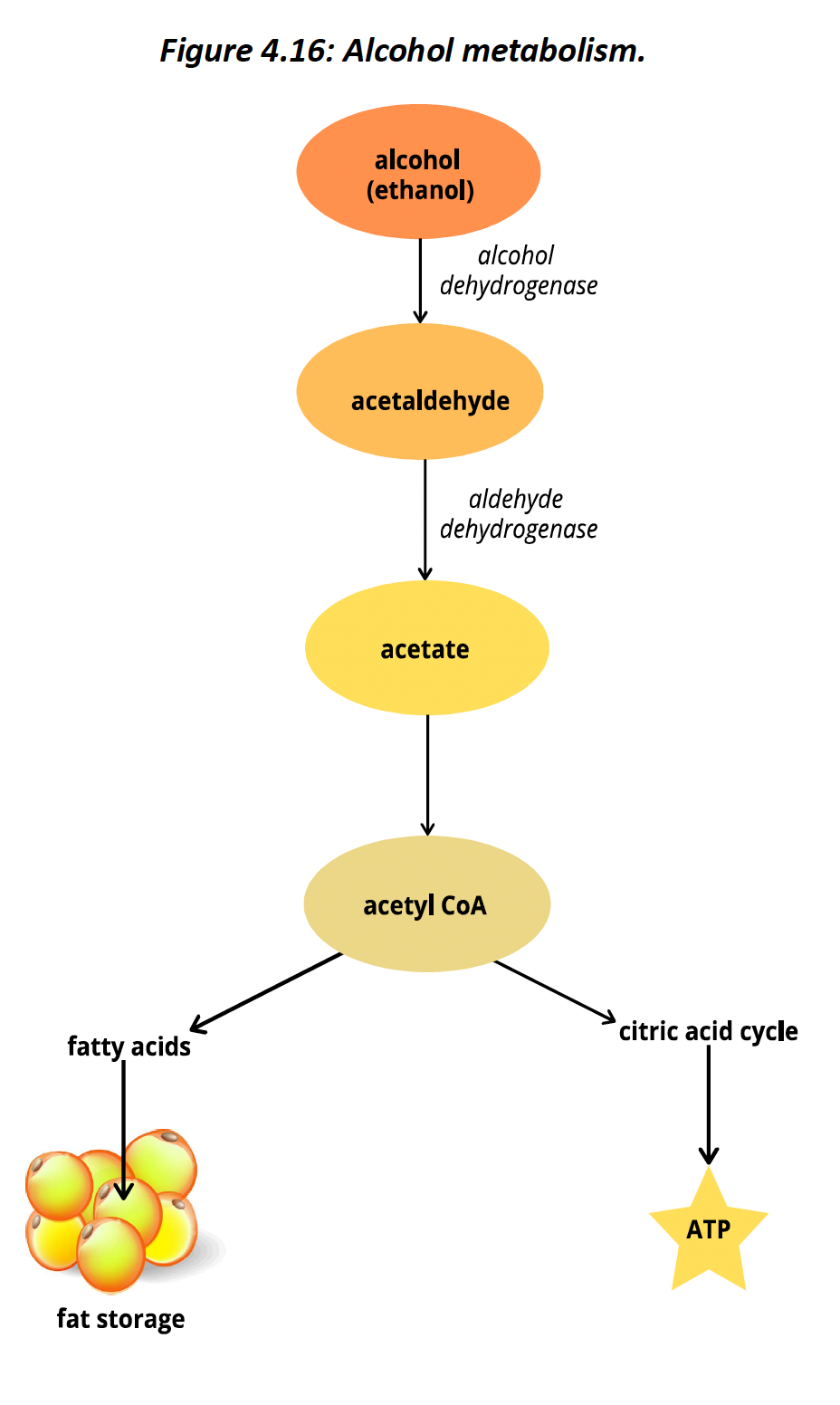
Approximately 90% of alcohol is metabolized and eliminated in the liver. The enzymes alcohol dehydrogenase and aldehyde dehydrogenase modify alcohol in a two-step process that leads to the formation of acetate.
acetyl CoA can enter the citric acid cycle and continue through cellular respiration
to create ATP, the body’s energy currency. Acetyl CoA can also be used to synthesize fatty acids.
One genetic variation of the enzyme aldehyde dehydrogenase leads to slower metabolism and lower risk for dependence. People with these genetic differences experience facial redness, nausea, sweating, dizziness and a racing heart rate due to the buildup of acetaldehyde.
Many people experience hangovers several (6+) hours after drinking – especially after high levels of consumption. Symptoms of a hangover vary, but may include vomiting, tiredness, decreased attention, decreased concentration,stomach pain and disturbed sleep.
It is also proposed that it is not the alcohol itself that produces hangover symptoms, but the presence of congeners, substances added during the fermentation process.
an adequate intake (AI) level of 2.7 L/day for women and 3.7 L/day for men is typically used.
Chapter 5
6.2 - types of carbohydrates
Carbohydrates are organic molecules whose primary role is to provide energy. There are three main types of carbohydrates: sugars, starches and fibers.
Sugars
monosaccharides, or single sugars. Carbohydrates vary in the types and number of monosaccharides they have in their structure.
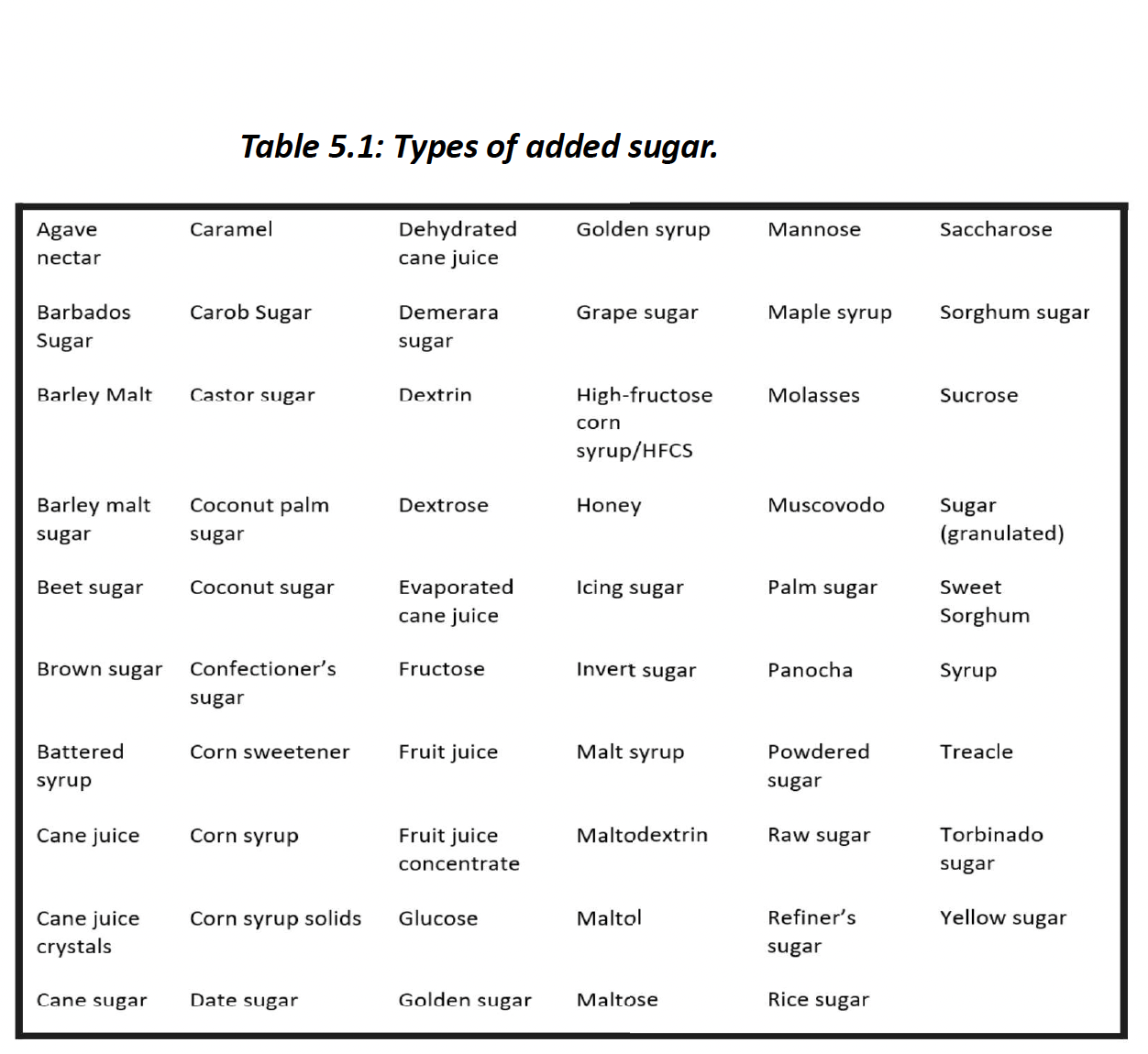
Sugars are found naturally in many foods including fruits and milk. These are known as intrinsic sugars. Sugars are also added to foods by the food industry to enhance the flavor of processed foods. These are known as extrinsic sugars or added sugar.
Glucose is the most common monosaccharide. It is the building block of most other longer carbohydrates like starch and fibre. Glucose can be metabolized into ATP, the body’s main
energy currency.
Fructose is often referred to as fruit sugar because it is found in many fruits as well as some vegetables and honey.
Galactose is often called milk sugar because it is found in milk. It is similar in sweetness to glucose.
Disaccharides are sugars with two monosaccharide units.
Sucrose, or table sugar, is what most people think of when they think of sugar. It is what we put in our coffee and use in baking. Sucrose is made up of a glucose molecule bound to a molecule of fructose.
The enzyme sucrase breaks down sucrose into its respective two sugars.
Maltose, or malt sugar, is the reason bread tastes sweeter as it is chewed. One of the main nutrients found in bread is starch, which is formed from a long chain of glucose molecules.
Lactose, or milk sugar, is the main sugar found in milk, which is why coffee tastes sweeter when milk is added. Lactose is composed of a glucose and a galactose molecule. Note that galactose is also referred to as milk sugar, however, this term is most often used to refer to lactose.
Oligosaccharide have a few monosaccharides in their chains – between 3 and 10. The main oligosaccharides found in the diet are considered fibres because humans lack the enzymes needed to break them down.
Polysaccharides are chains of monosaccharides greater than 10 units in length. We can further divide these into two categories – starches and fibre. The human body has enzymes that can break down starches but lacks those that break down fibre.
fructooligosaccharides is most likely to function as a prebiotic.
Starch
Starch is composed of long chains of glucose molecules in either a straight-chain (amylose) or branched-chain (amylopectin) formaon.
Amylopectin is the most common carbohydrate in the human diet. Most foods that contain starch have a greater degree of amylopectin than amylose. During digestion, starch is first broken down into oligosaccharides, then into disaccharides and eventually into
the monosaccharide glucose, which is then absorbed.
Fibre
fibre is a collective term for plant substances such as cellulose, dextrin and inulin that human enzymes cannot break down. These carbohydrates are mainly in the rougher parts of plants, such as their outer casing. Vegetables, fruits, whole grains and legumes are all good sources of fibre.
fibre is composed of long chains of glucose molecules. However, the bonds that hold adjacent glucose molecules together in fibre are different from those in starch and the human body lacks the enzymes needed to break these bonds.
Whether fibre can or cannot be fermented into short chain fatty acids primarily depends on whether it is soluble or insoluble fibre.
Soluble fiber dissolves in water to form a gelatinous solution, which adds bulk and viscosity to ingested food. Oats, apples, beans, peas, citrus fruits, barley and psyllium are all good sources of soluble fibre. Each gram of soluble fibre provides around 2–3 kcal of energy. Soluble fibre consumption may improve cardiovascular health.
Insoluble fibre does not dissolve readily in water and is best known for its ability to facilitate the passage of food material through the digestive tract. This contributes to the health of the digestive system.
The bran layer is the outer, waxy cover on the grain. It tends to be high in fibre and has calcium, iron and B vitamins. Most of the grain is the endosperm layer. It is mainly composed of starch and tends to be lower in other nutrients. The germ layer, or embryo, is the smaller inner part of the grain. It has the highest protein content of the three. It also contains more fibre than the endosperm, as well as B vitamins and vitamin E.
Bacteria ferment certain fibres into short-chain fatty acids, which can be absorbed and used for energy.
Following the refinement of a grain, which is the main remaining component? Endosperm. 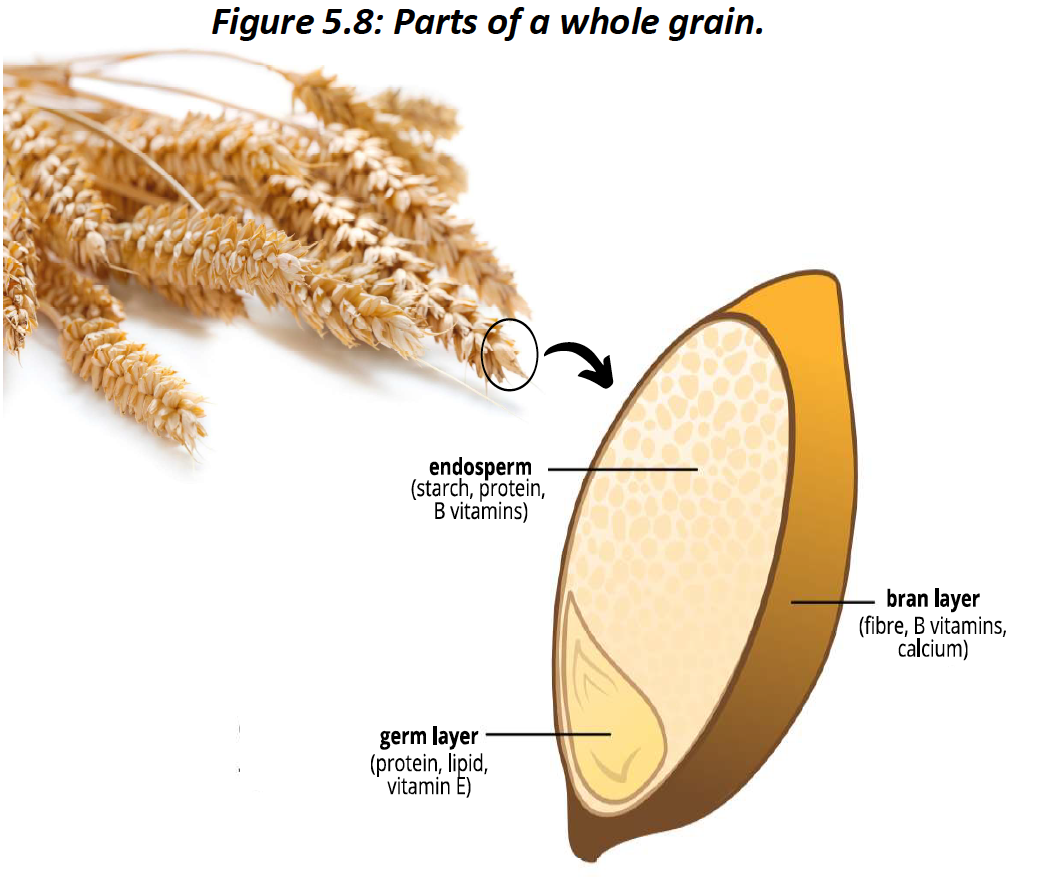
Glycogen
Glycogen, like amylose, is a large, unbranched chain of glucose units. Unlike amylose, it is found in negligible amounts in the human diet. Small pockets of glycogen are found around our liver and our muscles.
Unrefined sources of carbohydrates are those consumed in their entire form; the main edible parts of the plant have not been changed or removed These are often called whole sources, such as whole grain wheat and whole grain oats.
refined sources of carbohydrates have part of the plant – typically the bran and germ layer – removed. This usually lowers the nutrient density of that plant.
6.3 - digestion and absorption of carbohydrates
Most carbohydrate digestion occurs in the small intestine. Once carbohydrates are detected here, the hormone cholecystokinin (CCK) is released from duodenum cells. This hormone acts on receptors in the pancreas to promote the release of pancreatic juice into the small intestine. Pancreatic juice contains pancreatic amylase, which further digests starch into shorter and shorter saccharide chains.
Lactase is a brush border enzyme, which means it is secreted by the microvilli which are collectively known as the brush border.
The microvilli provide another source of carbohydrate-digesting enzymes. The brush border contains an essential set of carbohydrate-digesting enzymes that are released by internal cells to finish off the digesting job that the amylases started. Lactase, maltase and sucrase, which respectively break down lactose, maltose, and sucrose are all brush border enzymes.
Glucose, fructose and galactose are absorbed across the walls of small intestine cells into blood capillaries. They then go to the liver.
Some individuals have a compromised secretion of lactase, leading to a condition known as lactose intolerance.
Individuals who are lactose intolerant may experience symptoms such as cramps, bloating, diarrhea and pain in the abdomen when they consume the lactose found in milk products. Lactose intolerance is caused by insufficient secretion of the brush border enzyme lactase. This leads to an inability to digest lactose and absorb its glucose and galactose components. These sugars pass on to the large intestine, where bacteria can ferment them. This process leads to the production of methane gas, which is responsible for many of the symptoms noted above.
An option is to take lactase tablets. There are various options on the market, with varying degrees of lactose digestion. Too much stomach acid could inactivate the enzymes found in these tablets, so they tend to work more effectively in some people compared to others.
The glycemic response is the spike in blood glucose that follows a meal once glucose enters the general circulation.
Diets that produce a lower glycemic response are associated with improved insulin sensitivity, lower body weight and may decrease the risk of diabetes, cardiovascular disease (CVD) and obesity. The glycemic index and glycemic load can help us determine the glycemic response of foods.
The glycemic index (GI) is the relative ranking of a food’s potential to spike blood sugar on a 100-point scale. Pure sugar, glucose, is given a score of 100 as a benchmark. Low-GI foods score 55 or less, mid-GI foods score between 56 and 69 and high-GI foods score above 70.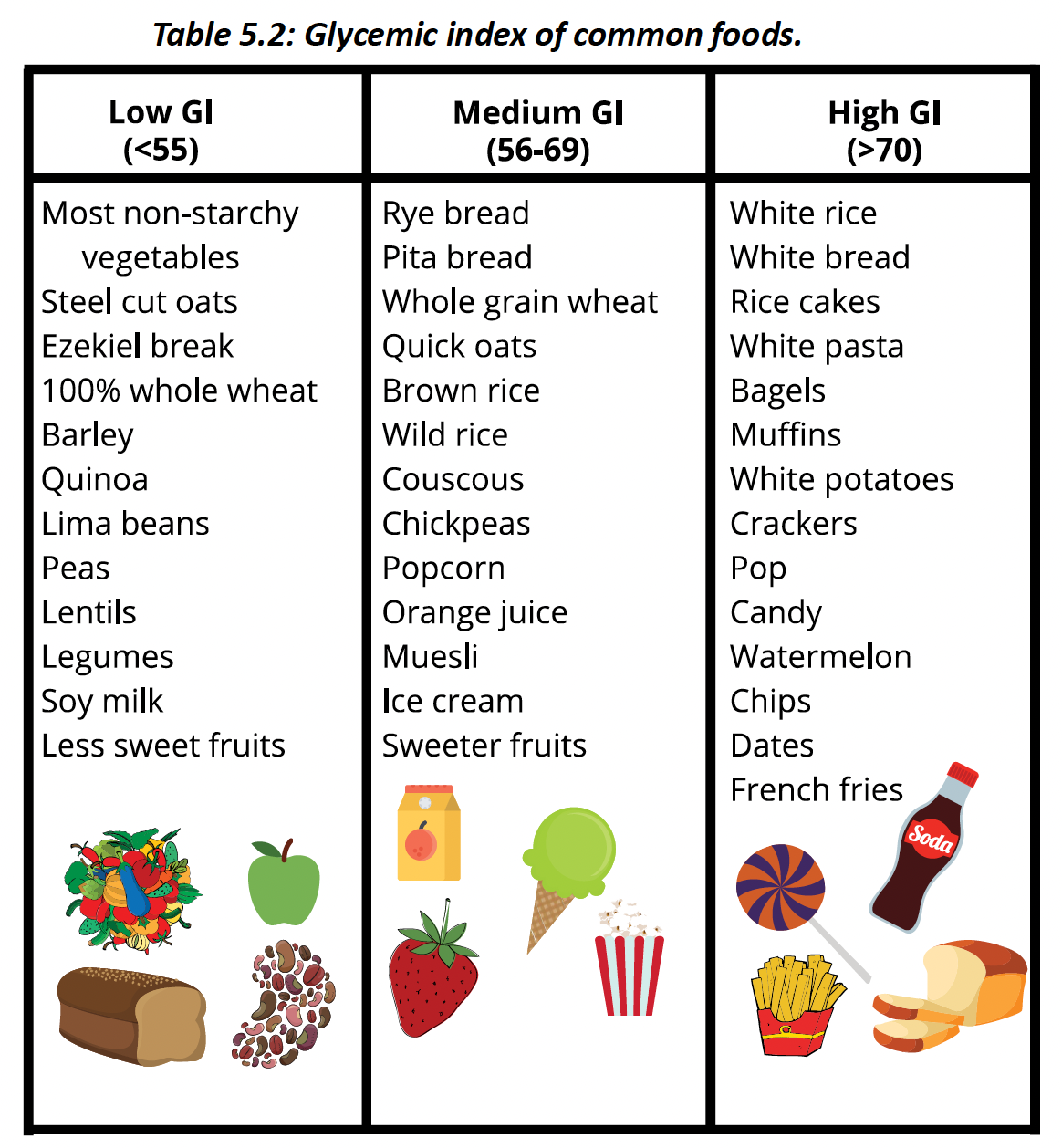
glycemic load (GL) is believed to be a more accurate assessment of how much blood glucose will spike since it considers the food’s GI plus the actual amount of carbohydrate within the food.
The GI of watermelon is 72 – which makes it a high GI food. However, since a serving of watermelon contains only a small amount of carbohydrate, its glycemic load is 7. Low-GL foods score less than 10, moderate-GI foods score 10–20, and high-GL foods score above 20.
Low blood glucose levels result in a state known as hypoglycemia, in which an individual may experience tiredness, lethargy and irritability.
Excessive pancreatic secretion of the hormone insulin can lead to hypoglycemia.
chronic hyperglycemia, or elevated blood sugar levels, can damage blood vessels and the kidneys and promote diabetes.
The pancreas has two very important yet very different functions. Exocrine means outside of the body and typically refers to secreons that occur into the digestive tract. The digestive tract is technically outside of the body since it is a long tube that runs through us. The pancreas secretes enzyme-containing pancreatic juice into the small intestine. Pancreatic amylase, lipase and protease promote the digestion of carbohydrates, lipids and proteins, respectively. Endocrine refers to the secretion of substances into the bloodstream, specifically hormones. The secretion of the hormones insulin and glucagon into the blood to regulate blood glucose is the main endocrine role of the pancreas.
insulin regulates blood glucose levels. When blood glucose levels spike after a meal, insulin secretion from the pancreas also rises. Once insulin allows glucose to enter the cell, blood glucose levels normalize. Once in the cell, glucose can then be stored, converted into fat or used for energy, depending on the body’s needs.
If insulin cannot allow glucose into the cell, glucose remains in the blood and blood glucose levels remain high. This can occur if insulin is not being secreted (insulin deficiency) or if the cell’s response to insulin is compromised (insulin resistance). These are the hallmarks of type 1 and type 2 diabetes, respectively.
Glucagon increases blood glucose by promoting three main processes:
1. Glycogenolysis: the conversion of glycogen to glucose.
2. Gluconeogenesis: the conversion of certain amino acids into glucose.
3. Lipolysis: the breakdown of stored lipids. Glycerol from triglycerides can then be used to make glucose.
6.4 - carbohydrates function
Carbohydrates have one main role in the body – to provide a source of energy. Glucose is the main carbohydrate in the body and is used as a source of energy by all body tissues.
Certain amino acids are used to make glucose through gluconeogenesis. However, this leads to the breakdown of body protein to provide these amino acids. Getting enough carbohydrates in the diet spares this from happening and helps maintain protein in tissues such as the muscles.
This can occur during periods of carbohydrate and/or caloric restriction. Getting enough carbohydrates in the diet spares this from happening and helps maintain protein in tissues such as the muscles.
Carbohydrates are involved in the metabolism of lipids. The metabolism of the glycerol and fatty acids that make up a triglyceride molecule leads to the production of acetyl CoA. Acetyl CoA can only enter the next stage, the citric acid cycle, if there is enough oxaloacetate present.
A high-fat, low-carbohydrate diet will not provide enough carbohydrates to metabolize fats this way. Instead, acetyl-CoA is used to form molecules called ketone bodies, which are used to fuel the body’s needs.
The main role of carbohydrates in the human body is fueling body needs.
6.5 - Diabetes
Diabetes is a disease characterized by chronically elevated blood glucose levels, due to the body’s inability to regulate them.
Elevated blood glucose levels can have a wide range of negative health effects. In the acute, or earlier, stages of diabetes a range of symptoms are seen.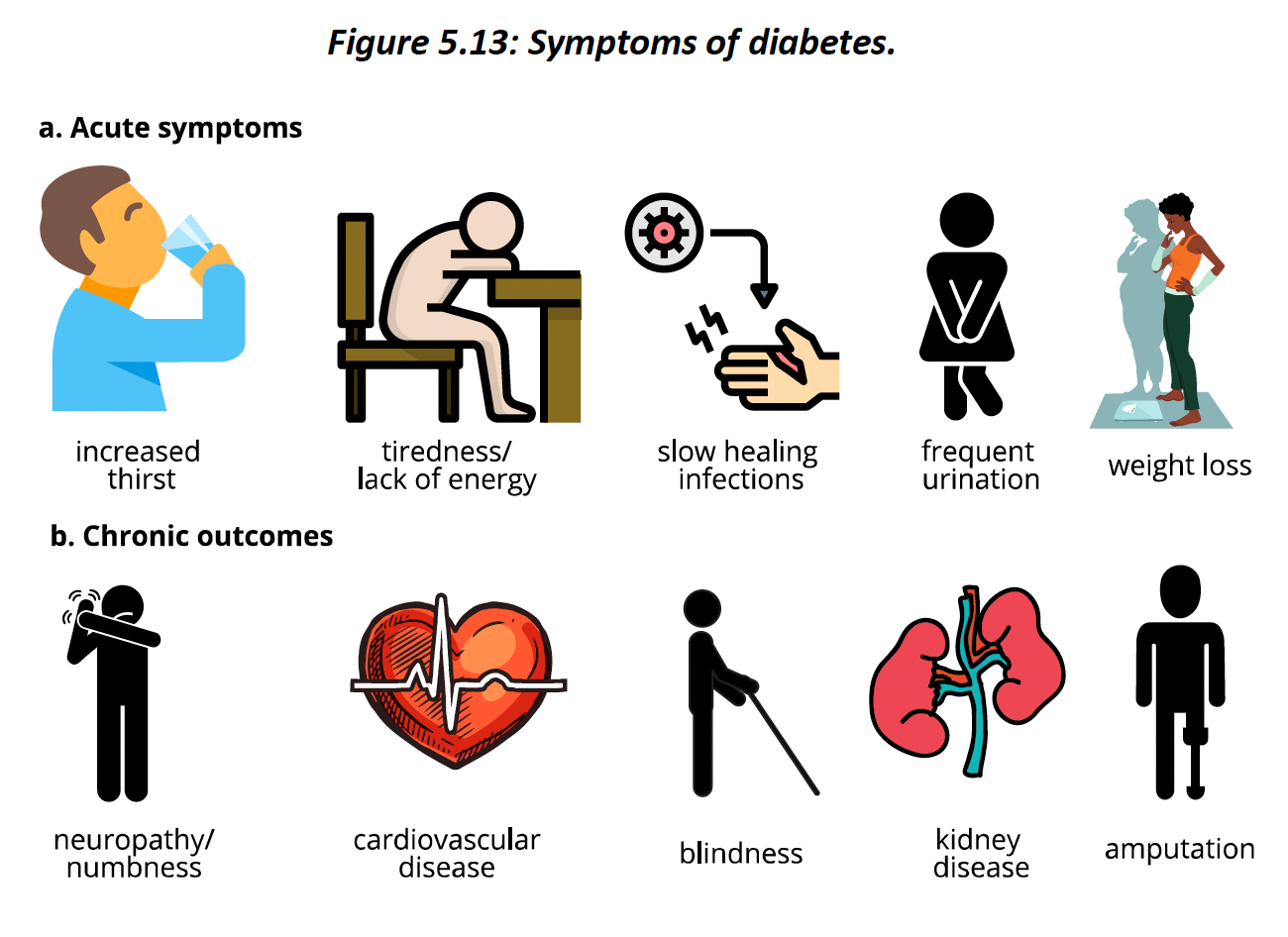
The high mortality rate seen in diabetes is related to its tendency to increase risk of CVD.
obesity is a risk factor, not an outcome of diabetes.
In Canada, First Nations living off -reserve and on-reserve have a diabetes incidence of 10% and 17%, respectively This is two to three times higher than the non-aboriginal population in Canada. This striking difference has led to examinations as to why the disparity exists and how to reduce it.
According to the study discussed in the Indigenous Lens section, preservation of Indigenous languages was associated with a lower risk for diabetes in the Aboriginal population that was studied.
Type 1 diabetes accounts for approximately 10% of diabetes cases. The immune system attacks the insulin- secreting cells of the pancreas. There is accordingly no insulin to promote glucose’s uptake into the cells and out of the blood. Presently, we are not entirely sure why our immune system attacks our own body. This is an active area of research. Regardless of the cause, individuals with type 1 diabetes develop toxic levels of blood glucose.
Type 2 diabetes accounts for the remainder of cases of diabetes. In type 2 diabetes, the pancreas cell secretes insulin, but the cells lose their sensitivity to it – that is, they don’t respond to it as well as they should.
Gestational diabetes is elevated blood glucose and impaired glucose management that first occurs during pregnancy (Diabetes Canada, 2020). Of women who have given birth, approximately 5% developed gestational diabetes – a number that has risen over time (Diabetes Canada, 2020). It is more common in older mothers, perhaps due to higher weights at time of pregnancy.
women who develop gestational diabetes are at a higher risk for developing type 2 diabetes.
The risk factors for type 1 diabetes are not fully established. Environmental factors, including early infection with pathogens such as rubella, have been suggested. There is also likely a genetic factor at play. Genetic studies of people with type 1 diabetes have found more than 40 changes in their DNA compared to people without this condition.
The risk factors for type 2 diabetes are more well established. Obesity, a lack of physical activity, family history and a previous case of gestational diabetes all increase risk. Again, there is also likely a genetic component.
The cause of type 1 diabetes is unclear, there is also no known way to prevent it. Currently, the cause of insulin resistance is still unclear. While a high carb diet may increase risk, it is not the sole cause.
The causes of type 2 diabetes are obesity and being overweight. Therefore, strategies that aim at reducing these conditions are recommended. A renowned study called the Diabetes Prevention Program (DPP) showed that the risk of type 2 diabetes can be significantly reduced with intensive lifestyle modification or medication use.
6.6 - carbohydrates in health and disease
Hypoglycemia, or low blood glucose, can lead to symptoms that include dizziness, extreme hunger, headache, irritability, tiredness and mental confusion. Diabec hypoglycemia occurs in individuals with either type 1 or type 2 diabetes who take too much insulin.
Reactive hypoglycemia is low blood glucose due to an excessively high release
of insulin. It occurs 2–5 h after a meal. The later hypoglycemia is experienced may suggest an abnormal insulin response and an increased risk of diabetes.
Non-reactive hypoglycemia, formerly called fasting hypoglycemia, is low blood sugar that may or may not be related to meals. It can occur in people who eat very little, such as in conditions like anorexia, but can also be caused by certain medications, pregnancy, alcohol abuse or liver,
heart and kidney disorders.
Sugars are not inherently bad or good. They are a source of energy that the body can use to fuel its many needs
Intrinsic sugars and extrinsic sugars are chemically identical, but the sources of these sugars are often very different, with potential nutritional consequences.
Diets high in extrinsic sugars are associated with a higher risk of CVD, diabetes and obesity
Since most studies on the link between SSBs and health outcomes are Sugar-sweetened beverages are high in extrinsic sugar and low in nutrient density. epidemiological in nature, caution should be taken in not assuming causation: we cannot say for sure that SSBs cause
cardiovascular events and obesity. However, most studies and reviews point to an association between these factors, suggesting that reducing consumption could improve health. Indeed, Canada’s Food Guide recommends replacing sugary drinks with water when possible.
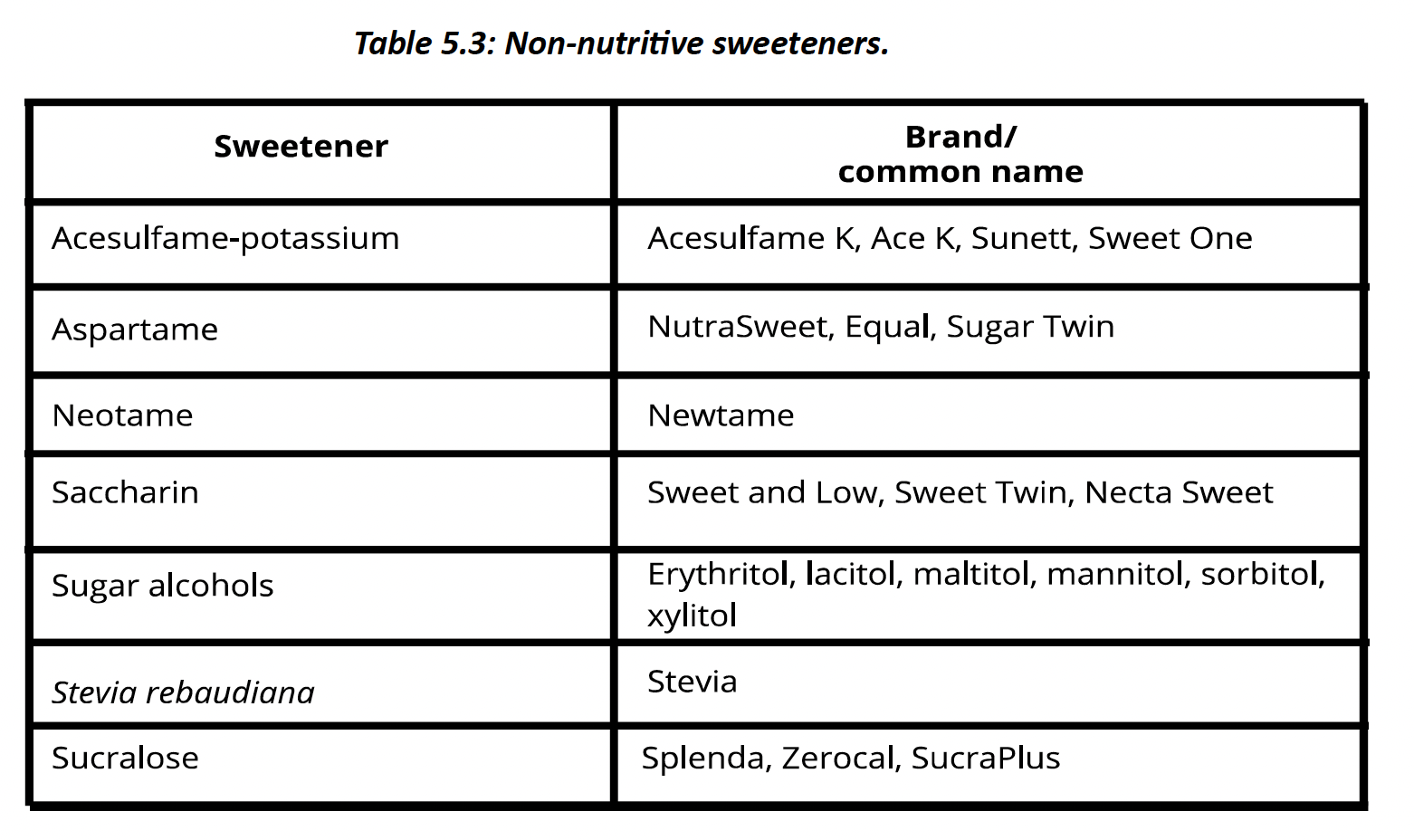
Non-nutritive sweeteners (NNSs) are also known as sugar substitutes or artificial sweeteners. They have a negligible number of calories and nutrients yet have a sweet-thang flavor. Depending on the sweetener, they are 30–1300 times sweeter than sugar, therefore a much smaller amount is required for a sweetening effect.
Since NNSs provide negligible calories and can replace calorie-laden sugar-sweetened products, it stands to reason that their consumption would be associated with a lower weight. The evidence to support this claim is conflicting.
In humans, prospective epidemiological studies have found an increase in body mass index (BMI) with the consumption of NNSs (Sylvetsky & Rother, 2018). The potential reason for this increase is that sensing sweetness without the delivery of calories may compromise our appetite regulation pattern and promote more food consumption.
there is currently not enough evidence to support the inclusion or elimination of NNSs from the
diet, since their benefits and disadvantages are not clear. A take-home message is to again focus on reducing the amount of processed foods in the diet, which are more likely to contain added sugars and artificial sweeteners.
A dietary factor that determines whether an individual will store energy in the body is the total number of calories they take in, regardless of the source of those calories, be it from carbohydrates, fats or protein.
A strong argument against the sweeping generalization that carbohydrates promote weight gain is that fibre is well established to have a role in reducing energy intake and promoting a healthier weight. Epidemiological evidence has long supported a link between dietary fibre intake and reduced risk for obesity
Dental caries, or cavies, are holes that develop in the teeth. They can promote pain and lead to more serious issues, even tooth loss, a strong link between the consumption of sugar and the development of dental caries (Gustafsson et al., 1954). Sugars provide food for bacteria in the mouth to grow and thrive.
diets that are high in added sugars and refined carbohydrates pose a greater cardiovascular risk. Conversely, foods that are high in fibre, such as fruits, vegetables and whole grains, are associated with a decreased risk of CVD.
Refined carbohydrates and added sugars promote a higher glycemic response. A high-GI diet has been associated with an increase in cardiovascular risk factors such as high blood triglyceride levels,
dietary fibre has a beneficial effect on cardiovascular risk. epidemiological studies and randomized control studies found a 15–30% decrease in CVD-related deaths, heart disease, stroke and type 2 diabetes among those with higher fibre consumption.
Soluble fibre lowers LDL (“bad”) cholesterol Meta-analyses of randomized control trials have shown that soluble fibre decreases LDL and total cholesterol levels in the blood (
Soluble fibre regulates blood sugar Diabetes is one of the main risk factors for CVD. Blood glucose regulation is important for decreasing the risk of as well as managing type 2 diabetes. Soluble fibre has been shown to decrease glucose spikes
Dietary fibre intake may reduce the risk of developing cancers of the large intestine. fibre had the lowest risk of developing cancers in different parts of the Colon. Fibre’s potential to reduce colon cancer incidence may be due to its ability to dilute the concentrations of cancer-causing agents in the large intestine, thus lowering their potency.
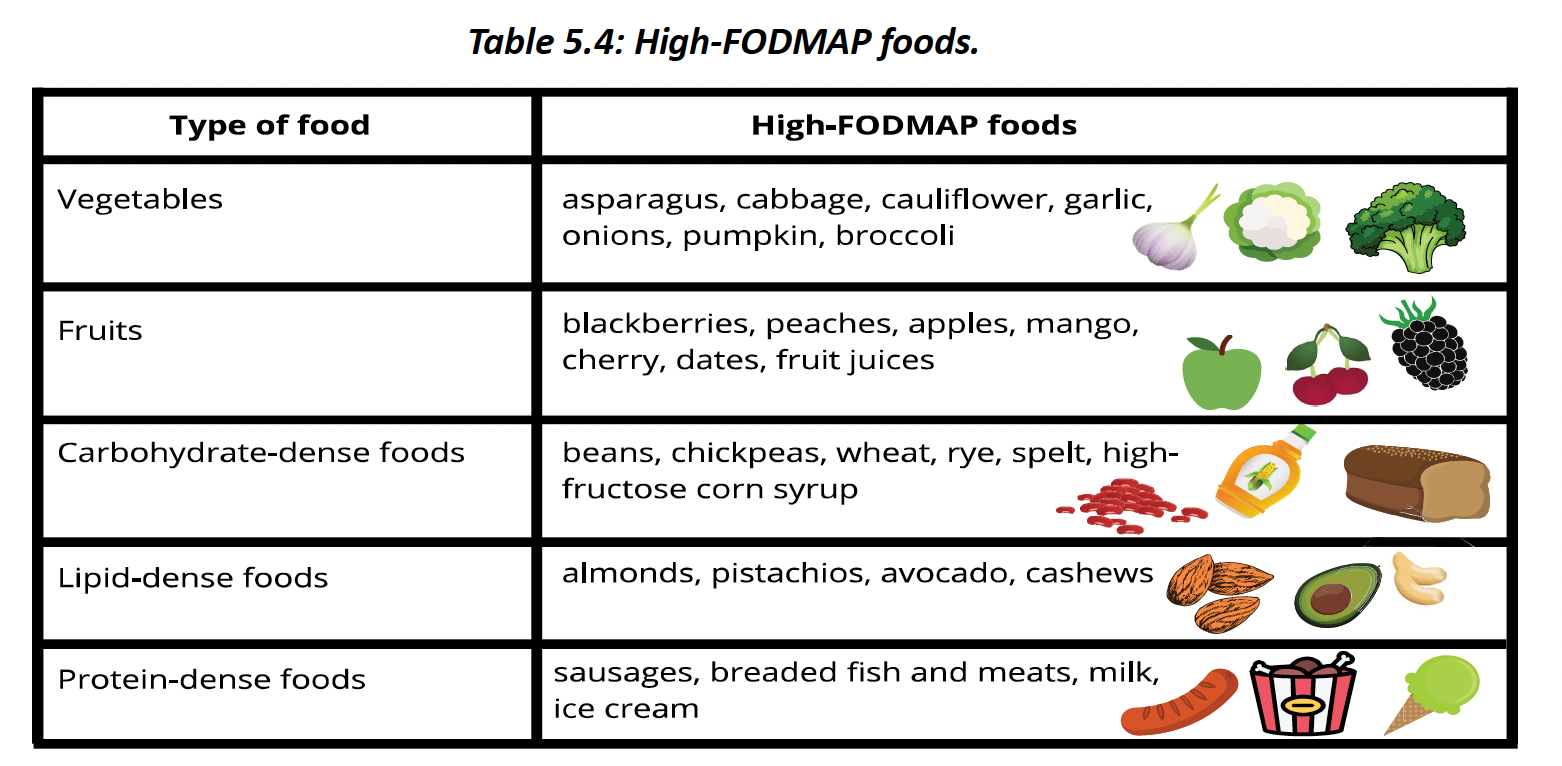
Irritable bowel syndrome (IBS) is a chronic condition that promotes symptoms such as abdominal pain, diarrhea, constipation, gas and bloating.
Accordingly, a diet low in fermentable oligosaccharides, disaccharide, monosaccharide
and polyols (FODMAPs) are often recommended.
Health effects of carbohydrates depend on the type and quantity that is consumed. Consuming carbohydrates from whole foods and plants is associated with positive health outcomes.
Chapter 6
7.2 - types of lipids
Lipids are molecules that are partly or en rely hydrophobic, meaning that they do not dissolve readily in water.
Triglycerides
Triglycerides are the main dietary lipids. They consist of a glycerol backbone with three fatty acids attached to it
triglycerides are completely hydrophobic
Fay acids differ in their degree of saturation.shows both a saturated fatty acid as well as three unsaturated fatty acids. The ends of both types of fats are the same. One end has a –CH3 group (represented by the end of the line). This is the fatty acid’s methyl, or omega end. The other end has a carboxylic acid group (–COOH). This is the acid end
The main difference between saturated and unsaturated fatty acids is that unsaturated fa y acids have one or more double bonds in their chain. The presence of a double bond kinks the chain, so it is no longer a straight-chain fatty acid.
fundamental rule in nature is that structure dictates function
Fay acids with one double bond are called monounsaturated fatty acids (MUFAs) Unsaturated fatty acids with two or more double bonds are polyunsaturated fatty acids (PUFAs)
The human body cannot synthesize PUFAs with the double bond before the ninth position. Accordingly, omega-3 and omega-6 fatty acids are essential fatty acids, but omega-9 fatty acids
are not.
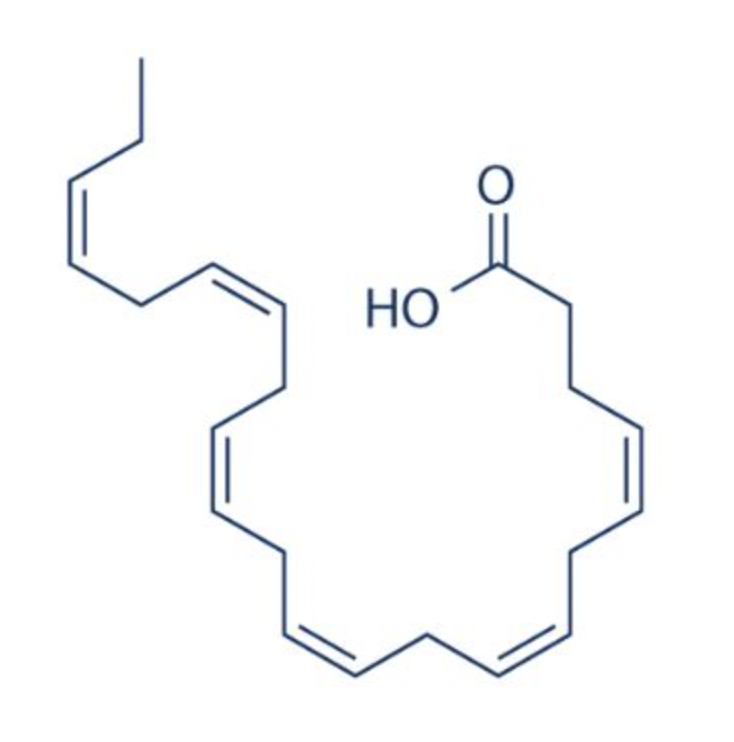
The above image is omega-6 fatty acid.
alpha-linolenic acid (omega-3) and linoleic acid (omega-6). They cannot be synthesized by the human body and must be consumed from the diet
Alpha-linolenic acid can be used to synthesize two other important omega-3 fatty acids, docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA
Both omega-3 fatty acids and omega-6 fatty acids can be used to synthesize signaling molecules called eicosanoids. Eicosanoids derived from omega-3 fatty acids have anti-infl ammatory properties, while those derived from omega-6 fatty acids have pro-infl ammatory properties
Long-chain fatty acids have a chain of 14 or more carbon atoms). Most fay acids we consume have 18–22 carbon atoms. Medium-chain fatty acids, like those found in tropical oils, have between 6 and 12 carbon atoms in their length
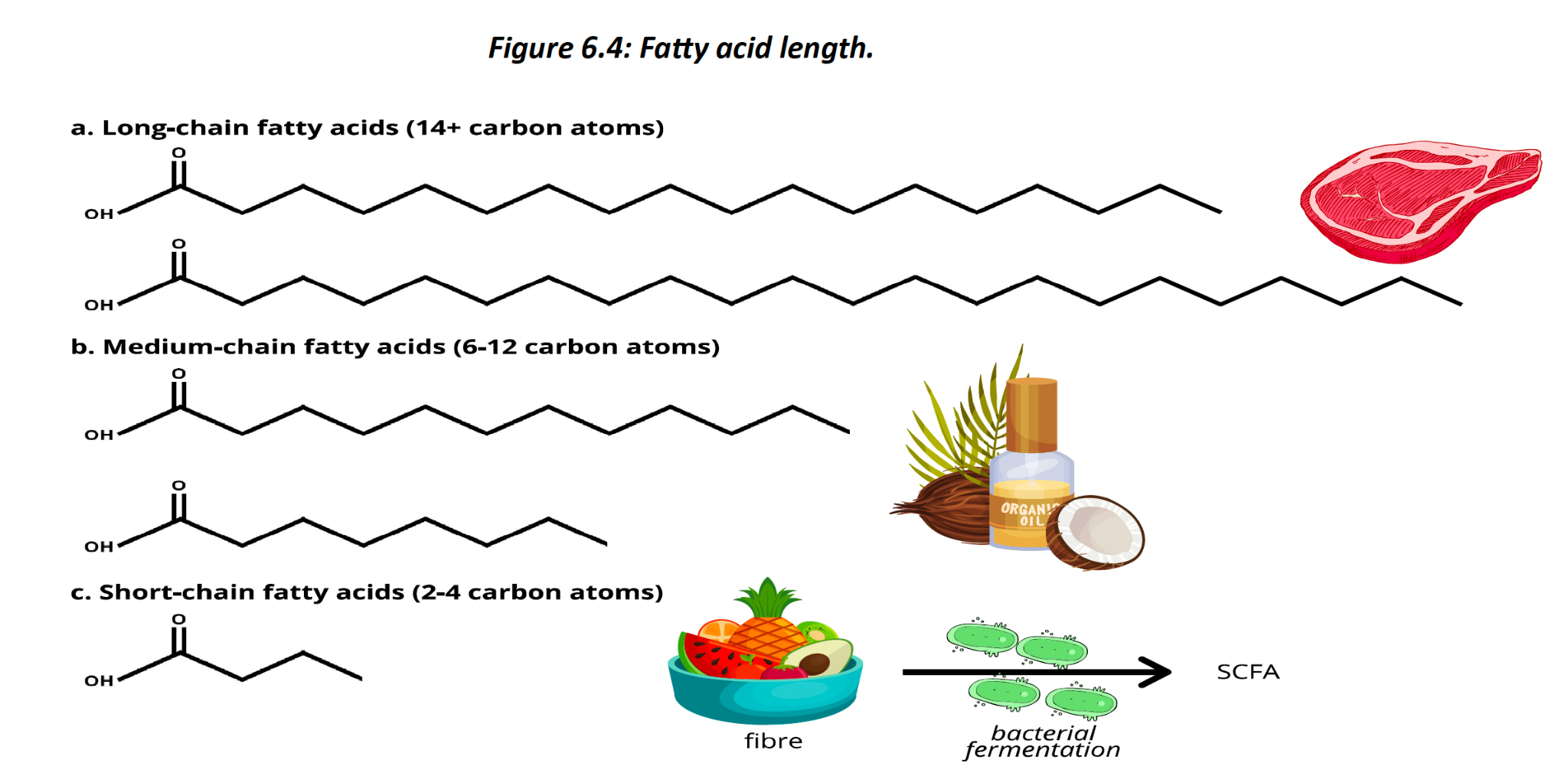
best source of short-chain fatty acids is in fiber
fatty acids are named according to their geometric organization. Unsaturated fatty acids can be either cis- or trans-fatty acids.
cis configuration, the hydrogens are on the same side of the double bond. This creates a small
force that pushes the rest of the chain away and produces the observed kink. In the trans fatty acid, the hydrogen atoms are on opposite sides of the double bond.
The food industry converts cis-fay acids into trans-fatty acids through a process called hydrogenation. This is done because trans-fatty acids are more stable and therefore have a longer shelf life. known to significantly increase the risk of cardiovascular disease (CVD) and other health issues
Sterols
Another group of lipids is the sterol group. Sterols have a ring formation made up of a hydrocarbon chain
sterols are considered lipids because they are also hydrophobic. Some sterols provide structure to the cell membrane, while other sterols can be used to form the hormones that facilitate body functions.
Sterols can be consumed from both plant and animal products.
The most common animal-derived sterol is cholesterol. Cholesterol is a crucial molecule. About a third of the human cell membrane is composed of cholesterol. Its presence in the outer layer of cells promotes membrane structure, while also helping to control what can enter and exit cells. not considered an essential nutrient.
Plant-derived sterols are also known as plant sterols or phytosterols. These sterols are similar to the animal-derived sterol cholesterol but have a slightly different molecular structure. Vegetable oils are the richest source of plant sterols.
found in nuts, seeds and fruits
Phospholipids
Phospholipids are a critical component of the outer surface of every human cell – the cell membrane. The body can make phospholipids itself, so they are not essen al from the diet
phospholipid has two fatty acids; in the place of the third fatty acid there is a phosphate group
phospholipids are amphiphilic – meaning they have both a hydrophobic (water-hating) and hydrophilic (water-loving) end.
phosphate heads facing the watery environment and their fatty acid tails facing each other. The membrane of each cell is composed of this phospholipid bilayer. This membrane is quite special as it allows the water content within the cell to be fully separated from the water content outside the cell. Only water and non-polar substances like fats can readily pass through this membrane.
Phospholipids also have an important role in the food industry, as they help form emulsions
Vitamins A, D, E and K are all technically lipids since they are hydrophobic. Unlike triglycerides, however, they do not provide energy to the body. Instead, they are responsible for several important physiological processes. In nutrition, we typically do not classify these as lipids and instead categorize them as fat-soluble vitamins
7.3 lipid digestion, absorption and transport
Triglycerides cannot be absorbed as ingested; they must first be broken down into fatty acids and their glycerol backbone.
Lipid digestion begins in the mouth with the release of lingual lipase. This enzyme removes a fay acid from the triglyceride. The release of lingual lipase continues as we swallow the
lipid-containing food into our esophagus. T
The stomach's acidic environment stops the activity of this enzyme, but lipid digestion continues here due to the secretion of gastric lipase by the stomach’s cells. Lingual and gastric lipase are particularly important for digesting small- and medium-chain fatty acids and act to begin lipid digestion.
If lipids are not digested by lipases, they cannot be digested, nor absorbed
bile is secreted into the duodenum to begin emulsifying these fats. Bile has an amphiphilic structure, making it an excellent emulsifier.
bile salts, the main components of bile, arrange themselves with their hydrophobic tails pointing towards the lipid center and their hydrophilic heads facing the watery environment of the small intestine, forming a micelle. Sterols, fat-soluble vitamins and other hydrophobic structures can also be found within micelles.
The liver synthesizes bile.
absorption villi of the small intestine, the micelle breaks down. It's digested fat components pass through the small intestine-facing membranes of the internal cells
Since the cell membrane is composed of phospholipids, lipids can easily pass through the spaces between them through passive diffusion. Once inside the small intestine cells, long-chain fatty acids bond with a glycerol molecule to reassemble into triglycerides.
As these and other lipid components move out of the small intestine cell, they become wrapped in a membrane mainly composed of phospholipids, but also containing protein and cholesterol. This new structure is called a lipoprotein. This specific lipoprotein is called a chylomicron.
Transporting lipids requires a series of lipoprotein molecules. main purpose of a lipoprotein is to carry lipids around the body
The outer shell of a lipoprotein is composed of phospholipids with embedded large proteins. Since most lipids are hydrophobic, the hydrophilic shell provides a structure that allows them to dissolve and move readily through watery environments such as the blood and lymph.
The more lipids there are in a lipoprotein, the less dense they are.
As lipoproteins lose triglycerides, their density increases. Therefore, very low-density
lipoproteins (VLDL) have the most triglycerides, while high-density lipoproteins have the least triglycerides.
Chylomicrons transport lipids between the small intestine and the liver. Unlike most other absorbed dietary components, these chylomicrons and the lipids they contain are too large to enter the blood vessels of the villi. absorbed into lacteals – the one-way lymphatic vessels found within the villi
Blood vessels near lipid-desiring tissues, such as muscle and fat tissue, express an enzyme called lipoprotein lipase (LPL) on their surface. LPL promotes the uptake of lipoprotein contents, particularly fatty acids, into cells
The liver makes a lipoprotein called very low-density lipoprotein (VLDL) that is low in density because it is mainly composed of triglycerides. VLDL is the main triglyceride delivery system from the liver
low-density lipoprotein (LDL). LDL has far fewer relative triglycerides compared to VLDL and is proportionally higher in cholesterol. LDL is thus the body’s primary cholesterol-delivery structure, delivering this sterol where it is needed. As we will learn later, LDL can potentially become quite reactive and even build up in artery walls, promo ng cardiovascular tissues
bad cholesterol. LDL is not intrinsically bad, but chronically high levels may increase the risk of CVD
The liver also makes high-density lipoprotein (HDL). HDL has a higher protein content and a lower lipid content, making it higher in density. HDL can pick up cholesterol as it travels through the bloodstream and return it to the liver, thus lowering the amount of cholesterol circula ng in the blood. Higher levels of HDL are associated with a lower risk of CVD, which is why it is o en referred to as good cholesterol.
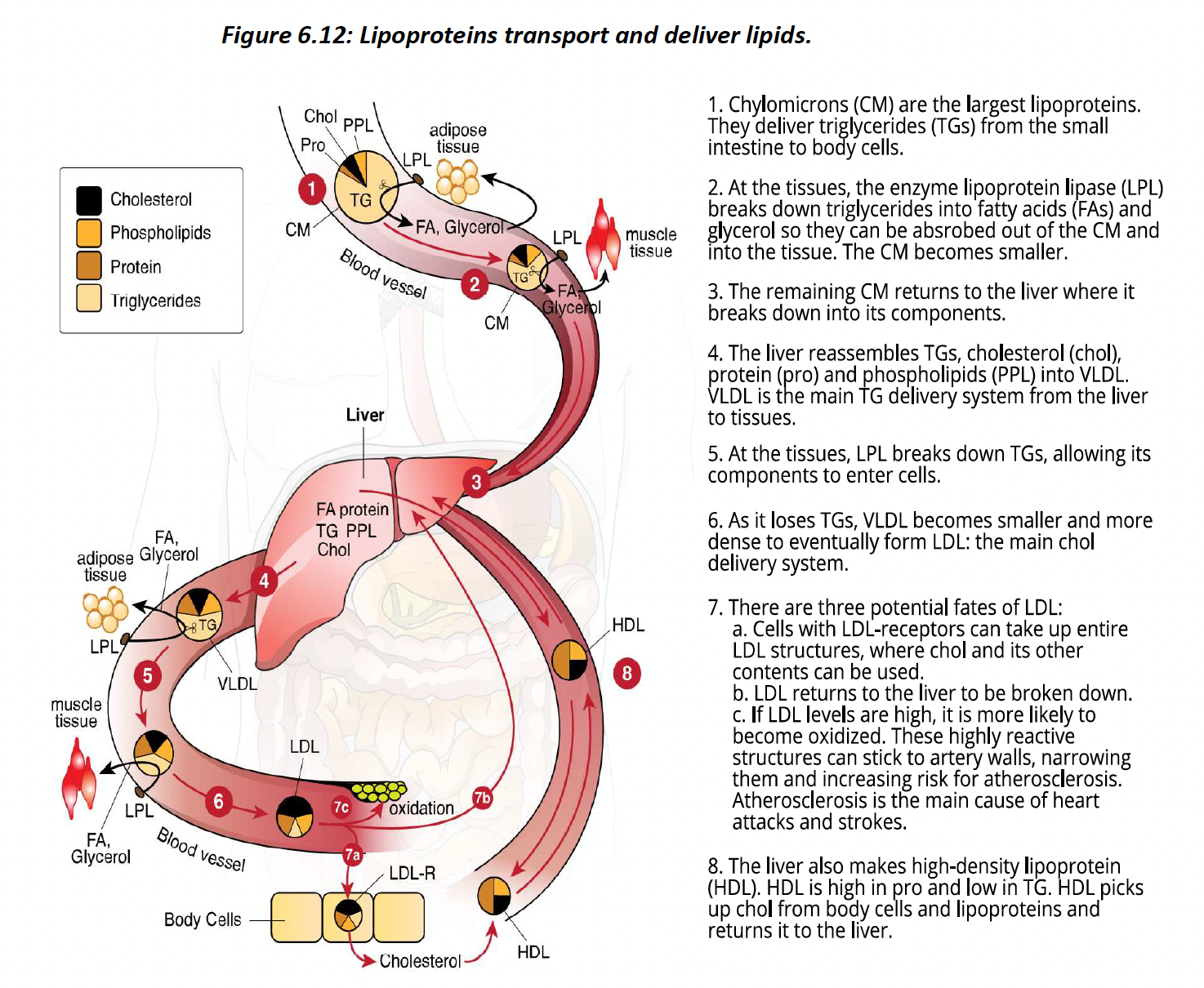
7.4 - lipid functions
Low density lipoprotein is the main cholesterol-delivering lipoprotein.
Very low-density lipoproteins promote the uptake of lipoprotein contents, particularly fatty acids, into cells.
Lipids are one of the three energy- yielding nutrients, affording 9 kcal of energy per gram. The main lipid we use for energy is the triglyceride
glycerol backbone can be used to synthesize glucose, which can then be metabolized into acetyl CoA. Fay acids also form acetyl CoA by breaking down two carbon atoms at a time through beta-oxidation.
an individual consumes a diet that contains sufficient carbohydrates (>~130 g/day), acetyl CoA enters the citric acid cycle, and cellular respiration proceeds as was first described in Chapter 3. Adequate carbohydrate intake is required to maintain oxaloacetate levels. This is what is meant by the phrase, fat burns in a carbohydrate flame.
low-carbohydrate diet and during times of fasting, oxaloacetate levels are insufficient, and lipid-derived acetyl CoA is metabolized differently. alternative metabolism produces ketones, through ketogenesis. The body can adapt to preferentially use ketones instead of carbohydrates as a primary energy source
excess lipids will be stored in our fat cells for later use. Together, our fat cells make up our adipose tissue, or fat tissue.
Chylomicrons deliver excess lipids from the small intestine to adipose tissue. Conversely, VLDL is the primary system that delivers lipids from the liver to adipose tissue. In an energy positive state, excess dietary carbohydrates and proteins that are not otherwise required will be converted into lipids and then also stored in our fat cells.
Our energy status determines whether our lipids are stored or metabolized.
When we are in an energy deficit, our bodies break down lipids from adipose tissue. These can then be metabolized to capture energy as ATP in order to fuel the body’s needs.
Human cell membranes are primarily composed of phospholipids. These phospholipids are also found in the structure of key cellular organelle such as the nucleus, mitochondria and endoplasmic reticulum.
We require dietary lipids to facilitate the absorption of vitamins A, D, E and K – the fat-soluble vitamins. These vitamins are packaged, absorbed and transported along with other dietary lipids within micelles (small intestine) and lipoproteins (blood).
Fat cells are also responsible for fat-soluble vitamin storage. Individuals who
do not consume enough fat or have issues with fat absorption are at risk for fat-soluble vitamin deficiencies.
Lipids form the precursors for several key molecules in the body.
Cholesterol is the precursor for a wide-range of important signaling molecules, including steroid hormones, bile salts, vitamin-D, and the sex hormones estrogen and testosterone.
Omega-3 and omega-6 fatty acids can be used to synthesize a wide range of eicosanoids. These signaling molecules have diverse roles in the body, including effects on blood vessels, blood clotting and inflammation. Essential fatty acids can also be used to synthesize endocannabinoids. These signaling molecules have effects throughout the body, but
their receptors are highly expressed in the brain. They have potential effects on cognitive function, appetite, mood and memory.
7.5 - lipids in health and disease
One of the cardiovascular system’s main roles is to carry oxygen and nutrient-rich blood to tissues so they can fuel themselves. It also removes waste products, so they do not build up. CVD compromises this delivery system and can have profound effects on the health and wellbeing of individuals.
Heart attacks and most strokes occur due, in part, to day materials building up in artery walls, narrowing the arteries and restricting blood flow. This artery narrowing is called atherosclerosis.
The risk for this disease can be greatly reduced by modifying specific lifestyle factors. It is well established that not smoking, consistent exercise, maintaining a healthy weight and managing stress levels decrease the risk for CVD.
Diet also plays a critical role in determining the risk. Consuming a diet rich in whole foods with lots of vegetables and fruits is recommended
Trans-fay acids are well established to increase the rao of LDL to HDL and increase the risk of CVD as well as all-cause mortality.
Diets that are higher in saturated fats are associated with higher levels of LDL. Decades of evidence has shown that higher levels of and more years of exposure to LDL are associated with a higher risk for CVD.
A reduction in LDL levels has been shown to reverse the development of atherosclerosis.
link between high LDL and atherosclerosis was causal, This has been referred to
as the lipid hypothesis, which suggests that one of the main drivers of CVD are the lipids found in our diet and blood.
It is important to note that the lipid hypothesis and specifically the link between dietary saturated fat intake and CVD is not a clear-cut case
A direct link between saturated fat and CVD mortality has not been established.
Contrary to the CVD-promoting effects of saturated fats, PUFAs may afford protection. Several studies have found that when saturated fats in the diet were replaced with PUFAs, LDL levels and the risk of CVD decreased
To minimize the amount of saturated fat in our diets but also include more PUFAs, a sound option is to consume a whole foods-based diet that is rich in plants. Plants, such as nuts, seeds and vegetable oils, as well as fatty fish like salmon and trout tend to be higher in PUFAs.
essential fatty acids can be used to synthesize hormone-like molecules called eicosanoids. The effects of eicosanoids depend on whether they were derived from omega-3 or omega-6 fatty acids
Eicosanoids derived from omega-3 fatty acids have been touted for their cardioprotective benefits such as decreasing inflammation, blood cholesterol, vasoconstriction and blood clotting. However, scientists are still debating whether supplementing omega-3 fatty acids promotes a decreased risk of CVD.
The ability to independently decrease the risk of CVD is still a topic of debate and research, though they are not believed to increase the risk.
Eicosanoids derived from omega-6 fatty acids have been thought for some time to increase the risk of CVD due to their potential to increase inflammation and blood clotting. However, results of randomized control trials have been mixed, either showing a reduction in CVD risk or no effect
They also found that increasing omega-6 fatty acids is linked with a decrease in blood cholesterol.
There has also been extensive study into the effects of omega-3 fatty acids on healthy brain aging.
DHA is particularly important in the brain and contributes to the structure and function of neuron membranes as well as neuron growth. Their anti-inflammatory effects may also contribute to brain health
fay acid’s potential to reduce the risk of Alzheimer’s disease is the topic of much
research. Systematic reviews of the evidence have found that DHA levels correlate with delaying Alzheimer’s onset
We do not eat LDL; the liver makes it from available lipids. For most people, dietary cholesterol has a minimal effect on increasing LDL and cardiovascular risk. This is because the body seems to produce less cholesterol when it is consumed from the diet, thus maintaining cholesterol levels despite dietary intake.
cholesterol hyper-responders. In about 25–30% of the population, cholesterol consumption does lead to increases in LDL. This is believed to be due to genetic differences in these individuals.
What is recommended is that most of our food choices come from plant products, with a reduction in animal products.
Eggs are very nutrient dense, having a high amount of protein, fat, vitamins and minerals for about 75 kcal per egg.
Some eggs are also a good source of omega-3 fatty acids. Omega-3 fatty acids are not added to the eggs, as typically happens in food fortification. Instead, when chickens are fed flaxseeds, they convert the alpha-linolenic acid into DHA, and both of these omega-3 fatty acids are incorporated into the egg yolk, making these eggs even more nutrient dense.
The egg contains about 225 mg of cholesterol. egg consumption did not increase CVD risk or mortality.
Nuts are high in fatty acids as well as plant sterols. Plant sterols, also known as phytosterols, are similar to animal-derived cholesterol, but are found in plants such as nuts, fruits and seeds. They are known to reduce low density lipoprotein levels by competing with cholesterol for absorption and altering cholesterol metabolism.
systematic review and meta-analysis that evaluated 17 epidemiological studies found no association between plant sterol levels in the blood and CVD risk.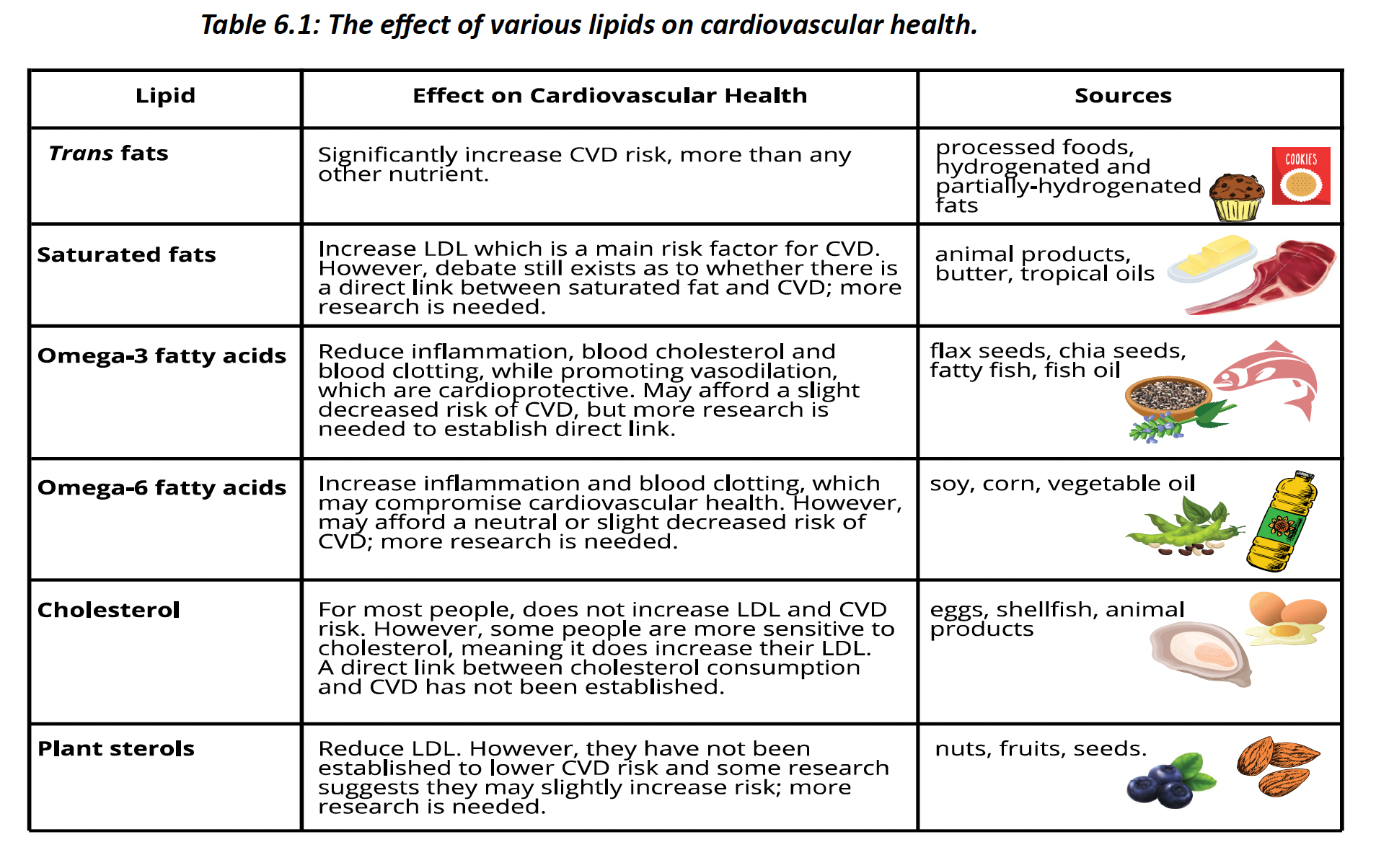
Body fat and dietary fat are not the same thing and no single nutrient causes obesity. While lipids offer more calories per gram than protein and carbohydrates, it is the total amount of energy consumed from all sources that determines whether body fat is gained, not the energy source.
Chapter 7
8.2 - protein structure
Proteins are organic molecules composed of a folded chain of amino acids. They are an energy-yielding nutrient, but their main roles relate to tissue growth and repair.
Proteins are long chains of amino acids.
Each amino acid has a nitrogen-containing amine group on one side and a carboxylic acid group on the other side. There are 21 amino acids found in our foods and bodies; they are structurally identical except for their side chains.
Of the 21 amino acids, nine are essential. These are absolutely required from
the diet because the body cannot make them itself.
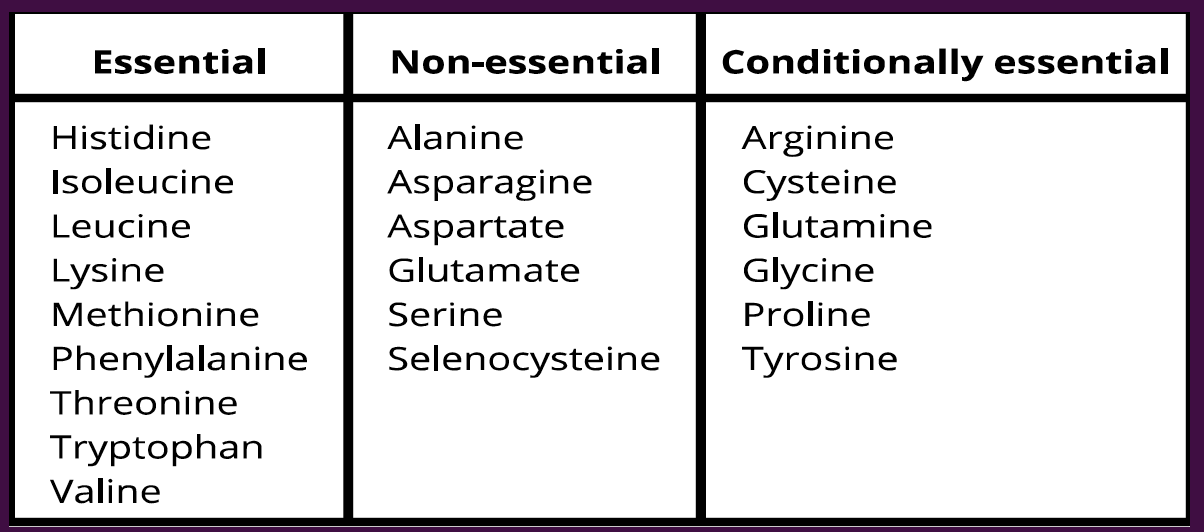
A food is considered a complete protein if it has all nine essential amino acids. Animal products are complete proteins, while plant products are typically incomplete proteins.
Essential amino acids missing from incomplete proteins are called limiting amino acids. Individuals who eat little or no animal products can ensure their diet includes all the essential amino acids by eating the few plant sources of protein that are complete.
Another option is eating a variety of plant products so the amino acids complement each other. This concept is called complementing proteins or mutual complementation.
those that consume a plant-based diet can meet protein needs by eating a variety of plant protein sources; these do not have to be consumed at the same meal
Our DNA holds the instructions for the sequence of amino acids needed in order to build specific proteins. To make these chains, the body draws on the amino acid pool, a reservoir of amino acids that are available for making protein. If the diet lacks an-essential amino acid, the liver can make it from another one through transamination.
Genes are sections of DNA that have the specific instructions for building a polypeptide chain, including instructions about the order of amino acids and chain length. When we say that DNA has the blueprints for life, we mean that DNA has the blueprints for making the various proteins
All proteins are polypeptides.
The first level of protein structure arises from adjacent amino acids bonding to each other. This occurs through a condensation reaction and leads to the formation of a peptide bond
These peptide bonds help build the polypeptide chain. The amino acid order in the polypeptide chain (i.e., which amino acids are located where) and the chain length determine how the protein folds to form its secondary,tertiary and potentially quaternary structures. This, in turn, determines the protein’s function
The secondary structure of a protein is evidenced by the presence of alpha-helices and beta-pleated sheets.These folds occur when non-adjacent amino acids form hydrogen bonds with each other.
Tertiary structure is formed after secondary structure and arises from interactions between amino acid side chains.
Some proteins have a quaternary structure. In this case, several proteins with a tertiary structure bind together to form the final protein.
referred to as protein subunits. Most quaternary proteins are made up of eight or less protein subunits.
A protein is denatured when it loses its folded three-dimensional structure. This change in structure also alters the protein’s function.
Digestion of protein begins with denaturation. The acid in our stomachs unfolds protein units, allowing enzymes to work on the primary structure of a protein, separating off amino acids for absorption.
Once this has occurred, it is impossible to go back because the protein has been unraveled
8.3 - protein digestion and absorption
The mechanical digestion of protein begins in the mouth as the teeth rip apart protein-containing structures from the rest of food. The mouth and saliva do not contain any protein-digesting enzymes, so chemical digestion does not begin until food reaches the stomach
hydrochloric acid released into the stomach lumen unravels proteins and activates the enzyme pepsin. Pepsin helps break the bonds between specific amino acids, further breaking down the unraveled polypeptide chain.
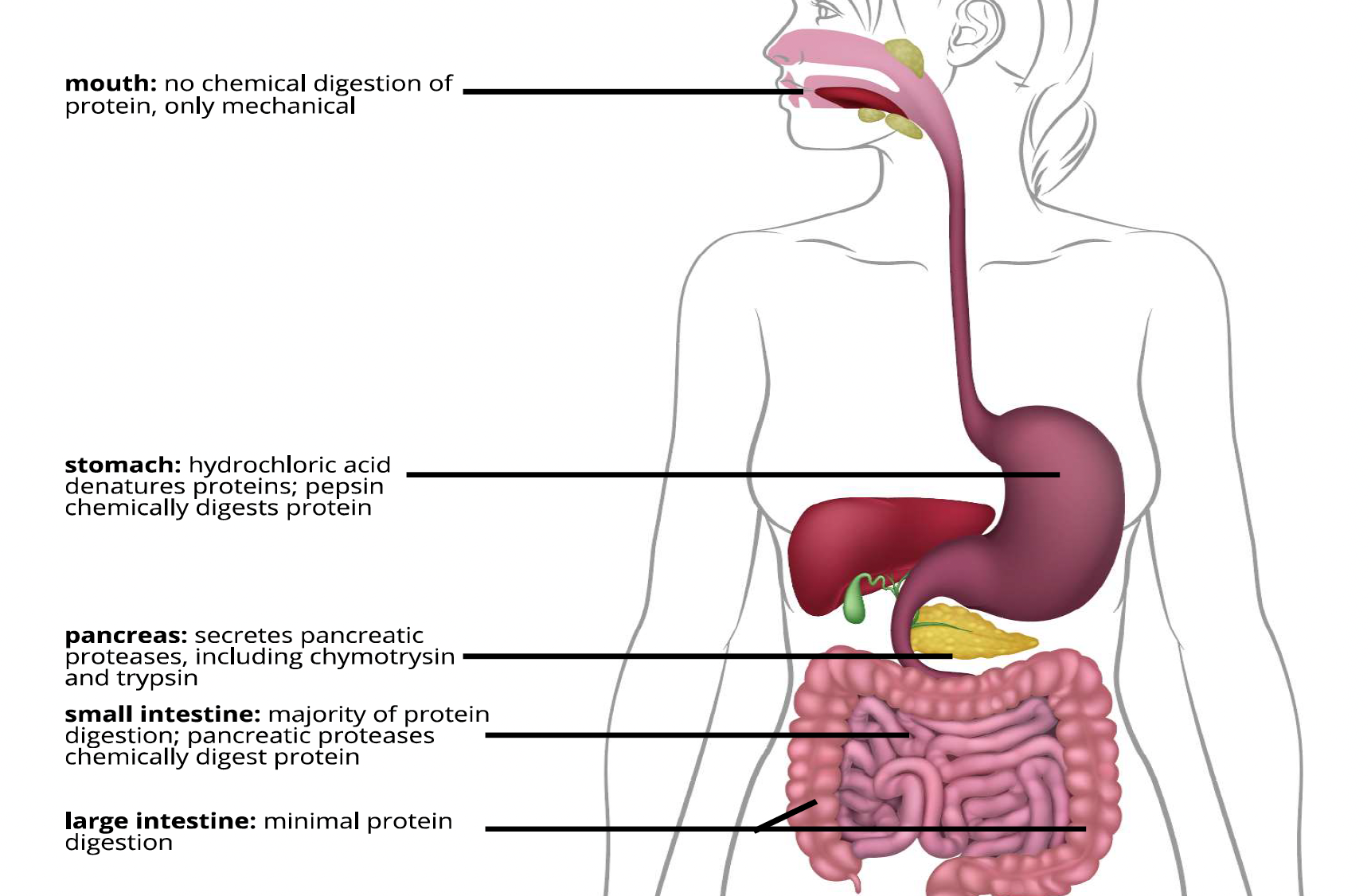
The main site of protein digestion is the small intestine. Here, the proteases (protein-digesting enzymes) trypsin and chymotrypsin, which are secreted by the pancreas, act on the remaining polypeptide structures. Proteases act on different amino acid sites to further break polypeptides into single, double (dipeptides) or triple (tripeptides) amino acids.
absorbed through active transport into the center of the small intestine villus.
Once the amino acids enter the villus space, they pass into the bloodstream via capillaries and then proceed to the liver. Amino acids that are not metabolized at the liver are released into the general blood circulation. Our tissues can then pick up amino acids from the blood and use them for various functions.
8.4 - protein functions
protein’s importance to body structure – bones, muscles, skin as well as every organ
in the body contain protein.
The protein's structural role is the protein collagen. Collagen is a protein found in bone, skin and connective tissue; it is the most abundant protein in humans and other mammals. In bone, collagen organizes itself into a rigid matrix that calcium and phosphate then harden. In skin, collagen promotes firmness and strength. found in the connective tissue of ligaments and tendons
elastin. As its name implies, this protein adds elasticity and can allow a structure to be slightly deformed and then resume its shape. The outside of our ears have both collagen and elastin.
Collagen allows the outer ear to maintain its shape, while elastin permits its flexibility.
Transport - our cells contain protein tracks that allow other proteins to “walk” along
them, carrying things around the cell. In cell membranes, there are protein transporters that extend from one side of the membrane to the other
In the blood, proteins can also be used to transport substances. For example, the blood protein hemoglobin picks up oxygen at our lungs and delivers it where it is needed
enzymes speed up the rate of cellular reactions by providing a site for reasons to occur. Most enzymes, like lipases, amylases and proteases are proteins. After a reaction has occurred, enzymes maintain their structure and can go on to catalyze other similar reasons
Two proteins are critical for moving us around our world. Myosin and actin are muscle proteins that interact to shorten our muscles so they can move our skeleton.
During muscle contraction, millions of myosin proteins bind to actin chains and then kink their heads to shorten the overall muscle length. When many acton- and myosin-containing muscle cells shorten in a coordinated way, the body can produce complex movements like walking or picking something up from the ground.
The amino acids found in blood proteins can carry positive or negative charges. Water is attracted to these charges and moves from the extracellular space into the bloodstream due to the draw of these proteins. This ensures that water does not build up in the extracellular space, reducing the risk for edema.
Certain proteins protect us from infectious agents such as bacteria and viruses.
Collagen in skin promotes structural integrity and allows skin to act as a barrier, stopping
infectious agents from entering and causing harm.
Antibodies are Y-shaped proteins that stick to the outside of pathogens, labeling them for removal and restricting the harm they can cause the body.
Amino acids can also be used to synthesize substances that are not classified as proteins. For instance, creatine, DNA, RNA and the neurotransmitters dopamine and serotonin can all be synthesized from amino acids.
Only 5–10% of the energy we use each day is derived from amino acids. This is partly because using amino acids for energy is a wasteful process.
The first step in using amino acids for energy involves deamination. Deamination removes the nitrogen-containing amine group so that the remaining structure can be used to form pyruvate, acetyl CoA or citric acid cycle intermediates. Which reactant of cellular respiration is formed depends on the side chain of the original amino acid before it was deaminated.
A product of deamination is ammonia, which is toxic to humans. Ammonia is thus converted into urea and excreted. The body prefers to be efficient, so it would rather use all parts of an amino acid to make necessary body proteins instead of excreting part of it in the urine. Accordingly, proteins are not a preferenal fuel source.
8.5 - protein in health and disease
no upper limit for protein consumption because complications from excessive protein intake
are uncommon in the general population. Protein deficiency, however, is linked with compromised growth and development and is a significant problem in parts of the world where poverty leads to undernutrition.
Marasmus is a wasting syndrome and occurs when energy from all sources, including protein, is inadequate. In addition to very low body weight, symptoms include difficulty managing body temperature, anemia, dehydration and heart irregularities. Marasmus can occur at any age but is most common in children and infants.
Kwashiorkor is a form of protein malnutrition that occurs in young children. It is believed to be associated with inadequate protein intake when energy needs are all being met. These diets are low in protein and essential amino acids, leading to protein deficiency. Kwashiorkor is typically evidenced by a distended, swollen abdomen and swollen legs and feet, but an otherwise slim appearance. The distended belly is partly due to edema.cause is believed to be decreased protein in the blood, but the exact mechanism by which kwashiorkor develops is unclear.
A high-protein diet that exceeds caloric needs can therefore promote fat gain. The converse is also true.
Diets that are higher in protein are sometimes recommended. This stems from the fact that a high-protein diet may favor a caloric deficit and has been associated with increased weight loss.
• Protein-rich foods tend to be more filling compared to foods higher in carbohydrates and fat . Therefore, eating protein-rich foods may promote a lower overall caloric intake because hunger is more satisfied, and the individual may consume less overall.
• A protein-rich diet may also help with energy balance since protein has a higher thermic effect which increases total energy expenditure. More calories are required to digest and absorb protein as compared to carbohydrates and lipids, again promong a caloric deficit.
• Lastly, amino acids may also play an important role in the metabolism of lipids and carbohydrates, further promoting an energy deficit.
The main role of protein is to promote the growth and repair of tissues. Therefore, it is particularly important when the body is repairing from exercise and rebuilding tissue, specifically muscle
Muscle protein synthesis increases in the 24 hours following resistance training and dietary protein can facilitate this process.
athletes increase their protein intake from 0.8 g/kg body weight to 1.2–2.0 g/kg body weight, depending on the intensity and load of training.
About half of the volume of bone and a third of its mass is composed of protein. Collagen is the main bone protein, providing the structural matrix that calcium and other minerals bind to and harden.
While protein is essential for bone structure, a high-protein diet has been associated with calcium excretion. overall, higher protein intake did not negatively affect bone health. They also found moderate evidence of increased bone density in the lower spine at higher protein intakes.
Dietary protein can impact the health of the kidneys, especially in those who have kidney disease. Filtration rates at the kidney increase following dietary intake of protein. kidneys must work harder to excrete the waste products produced when protein intake is higher
Patients with reduced kidney function could decrease their risk of further kidney decline, while also avoiding potential negative effects of excessively low protein intake, by consuming 0.8 g/kg body weight of protein per day.
Protein quality typically refers to two factors: how well a protein is digested and how the types and queens of amino acids in that protein source match the body’s requirements.
8.6 - protein quality
The United Nations recommended that the protein digestibility corrected amino acid score (PDCAAS) become the industry standard for assessing protein quality; it is still used today.
PDCAAS compares the amino acid content of a food against a standard amino acid
profile. The highest score that can be achieved is 1.0. Having a PDCAAS of 1.0 means that, following digestion, each unit of protein meets or exceeds the human requirement for essential amino acids.
digestible indispensable amino acid score (DIAAS). This score measures how well amino acids are digested in the ileum and more closely estimates the amount of amino acids absorbed by the body. This method is also better at determining the protein quality of mixed meals, not just ones with single ingredients.
PDCASS remains the preferred method.
Protein efficiency ratio (PER) is calculated in a laboratory setting by determining how much weight an animal gains when consuming a specific amount of protein, divided by the amount of food it consumes.
Canadian Food Inspection uses the PER to make sure that the food industry is making appropriate claims about a product’s protein content and/or quality.
The traditional diets of Indigenous people were very rich in protein. To assess the change in protein quality, researchers compared the composition of the amino acid tryptophan in the wild meat found in a traditional Indigenous diet to the composition found in processed meats. It was found that in addition to having higher total protein content, wild meats also had significantly higher tryptophan levels compared to processed meats.
Protein needs can be met by consuming whole food sources of protein. Some people also supplement their diet with processed protein supplements (e.g., protein powders, shakes and bars) or extra whole food supplementation (e.g., animal products, milk and tofu) in order to meet their needs and/or promote specific goals
supplementation beyond 1.62 g/kg body weight per day did not produce further gains. Thus, protein supplementation may improve muscle-related gains, but only up to a certain amount of protein intake, and both whole and processed protein sources can provide this gain.
processed sources of protein are typically low in phytochemicals and fiber and they can also be expensive.
Branched-chain amino acids (BCAAs) are essential amino acids that have a branched side chain. They are key components of the amino acid pool, accounting for 35–40% of the dietary essential amino acids that are found in body protein.
BCAAs are metabolized in the muscle instead of the liver.
Since these amino acids are essential, consuming enough of them is critical for the repair of protein-based tissue such as muscle. However, BCAAs can be consumed through whole sources of protein, like chicken, salmon and yogurt. To date, there is no evidence to show an
advantage to consuming BCAAs from supplement capsules or powders compared to whole foods.
8.7 - vegetarian diets
Compared to plants, animal sources of protein tend to have more total protein as well as a higher PDCAAS. They are also all complete sources of protein, having all the essential amino acids. In addition, they are higher in vitamin B12, vitamin D, iron, zinc and omega-3 fatty acids
also higher in saturated fat and absent in fiber and phytochemicals. Also, consuming processed animal products may lead to a higher health risk.
Diets that include animal products also provide a significantly higher environmental impact compared to plant based diets
Plant sources of protein, such as beans, nuts and lentils, offer less total protein and are more likely to be incomplete proteins. However, a well-planned plant-based diet may provide the same protein-related benefits as animal protein if a proper combination of sources is used.
Vegetarians are individuals who avoid some or all animal-related foods. People choose to become vegetarians for a variety of reasons.
veganism can sometimes also apply to more than just nutrition. For instance, the Vegan Society defines veganism as a lifestyle that excludes all types of cruelty and exploitation of
animals for food, clothing or other purposes.
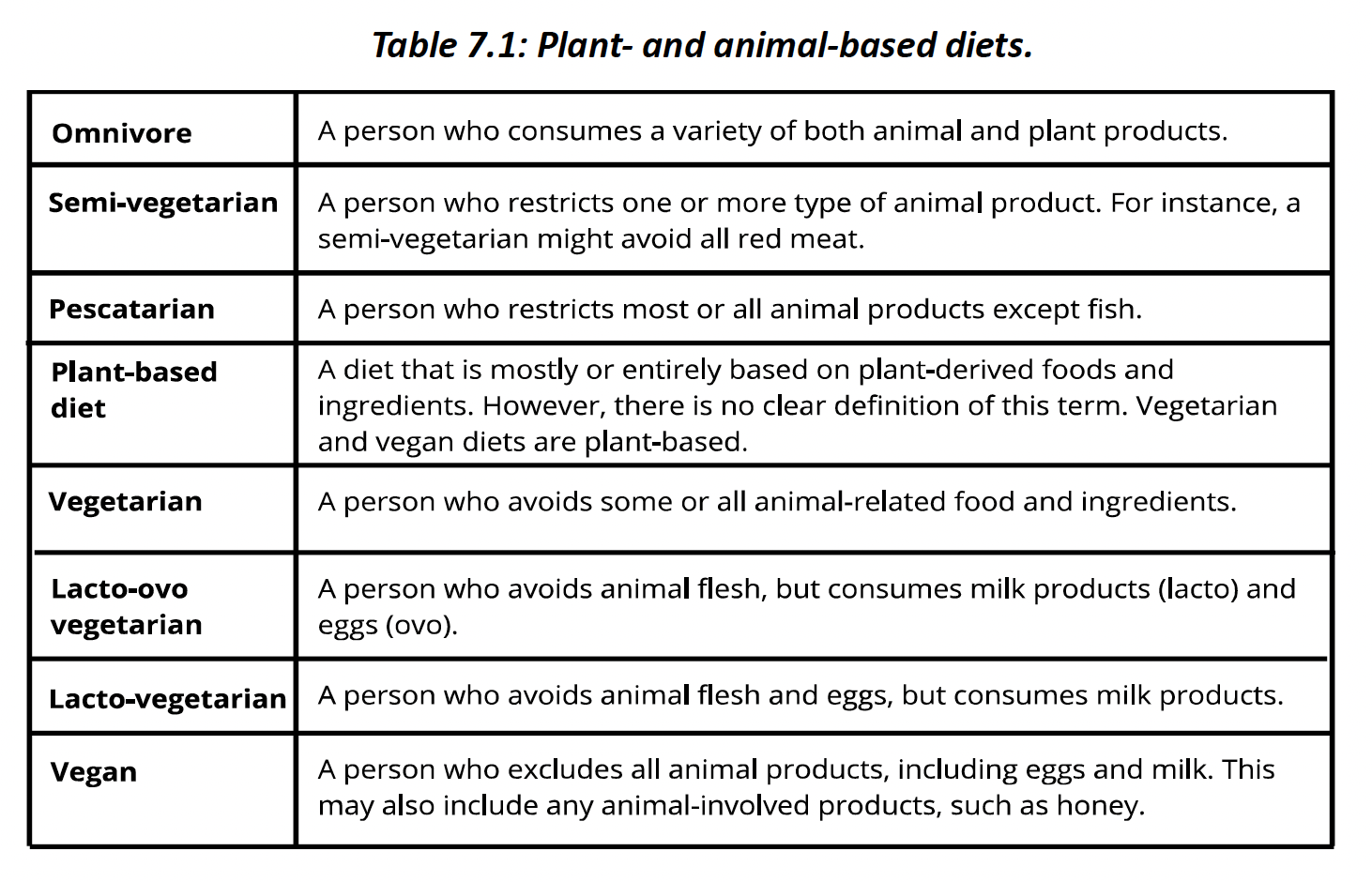
Vegetarian and vegan diets may have several health-related strengths. These diets are higher in fiber and phytochemicals and lower in saturated fats. In addition, they may reduce disease risk.
vegetarians are more likely to have lower body mass indexes, total cholesterol and LDL cholesterol. reduced risk of ischemic heart disease, cancer and cardiovascular-related deaths.
a reduced risk in these cardiovascular outcomes with a vegetarian diet.
All vegetarian and vegan diet health research comes from epidemiological studies. We cannot ethically or logically ask a certain group of people to become vegetarian and vegan for a long period of time in a controlled fashion and then compare this to another group whose diet is also controlled. Thus, randomized control trials, the gold-standard for establishing cause and effect, cannot be used to study human vegetarian diets and health.
Vegetarian diets tend to be lower in vitamin B12, vitamin D, omega-3 fatty acids, calcium,
iron and zinc. Searching out plant foods that are higher in these nutrients may prevent deficiency. The one exception is vitamin B12, which is absent in almost all plant products, with the exception of nutritional yeast.
Chapter 8
9.2 - vitamin overview
Vitamins are organic micronutrients. They do not provide energy, nor contribute to body structure, but are involved in numerous important biochemical processes.
If a diet lacks enough of a particular vitamin, certain biochemical processes may be compromised, which can lead to symptoms of deficiency. Conversely, some vitamins have an upper limit and if we consume them in excess, they can be toxic.
The body requires 13 vitamins to survive and thrive. They are classified as either water- or fat-soluble vitamins according to their behavior in water.
Provides 0 kcal of energy.
Water-soluble vitamins are hydrophilic and dissolve readily in water.
fat-soluble vitamins are hydrophobic and require a lipoprotein transporter to move around the watery environments of the body.
Whether a vitamin is water- or fat-soluble is also correlated with how often it is needed in the
body and how likely it is to be toxic. Excess water-soluble vitamins are excreted in urine, while fat-soluble vitamins are stored in adipose tissue, where they can build-up and lead to toxicity.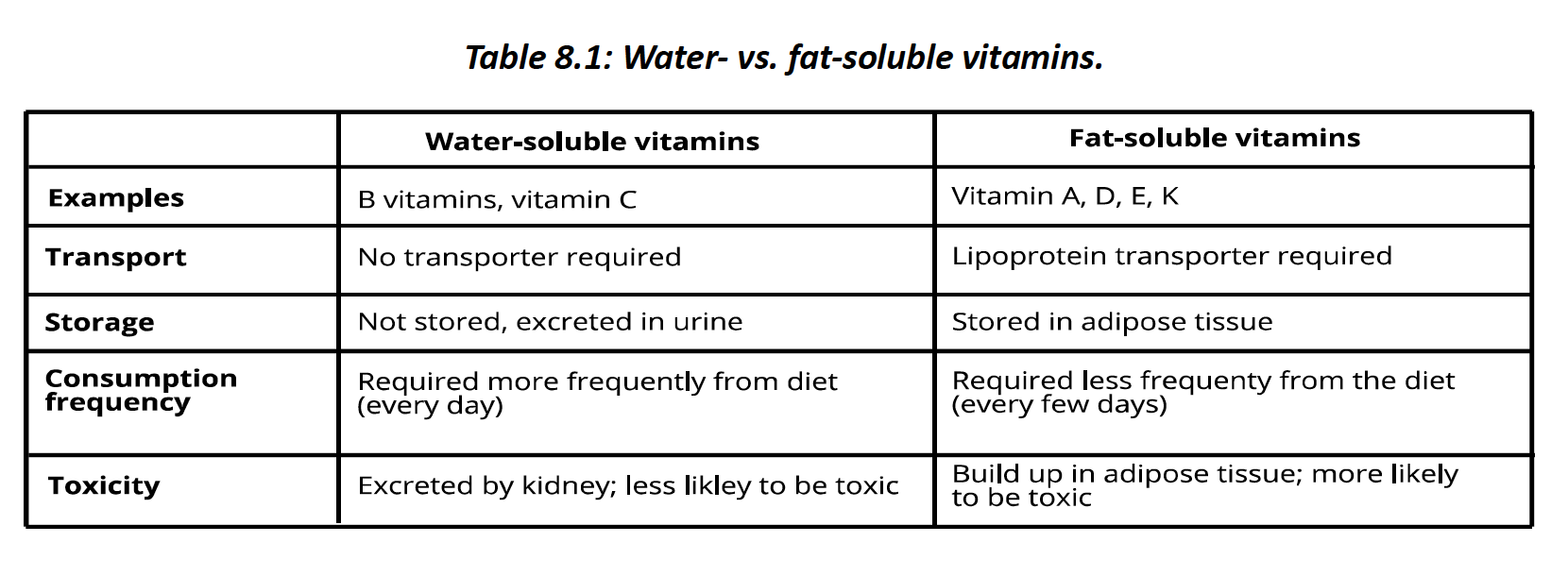
Many vitamins achieve their function by acting as coenzymes. Coenzymes are non-protein factors required for enzyme function. When coenzymes bind to enzymes, they can activate the enzymes and allow them to function. Vitamins are therefore important because they facilitate many enzyme-dependent body reactions.
Our daily vitamin needs depend on our age and life stage. For instance, younger individuals often have a lower RDA/AI for the various vitamins, while pregnancy and lactation typically increase needs.
9.3 - water soluble vitamins
The B vitamins are a group of eight vitamins that facilitate energy metabolism through their coenzyme functions. To be clear, the B vitamins do not provide energy. They support the enzymatic activity that promotes energy metabolism.
only nine B vitamins even though vitamin B12 exists. Many foods naturally contain B vitamins; they are also fortified into foods such as grains and cereals.
Vitamin B1: Thiamine
RDA: 1.2 mg (M); 1.1 mg (F).
Function: Thiamine is required by all body tissues. It plays a role in muscular contraction, nerve conduction and the synthesis of ATP. Thiamine is also part of thiamine pyrophosphate (TPP), a coenzyme involved in many cellular reactions.
TPP is required for the citric acid cycle of cellular respiration and is particularly important for carbohydrate metabolism
Source: Thiamine is abundant in many foods. Nuts, seeds, eggs, milk, poultry and for fi ed cereals are all high in thiamine.
Deficiency: Thiamine deficiency negatively affects the activity of thiamine-dependent enzymes. The brain is particularly susceptible to thiamine deficiency, where it can lead to neuronal death in areas with a higher thiamine requirement. Pregnant and breastfeeding women have a higher need for thiamine, which can be provided through food or through a prenatal vitamin supplement.
rare in Canada and the USA since it is so abundant in the food supply. thiamine deficiency can occur in those with restricted eating patterns, who have undergone gastric bypass surgery or with gastrointestinal cancers. most typically associated with alcoholism
Alcohol-related cases of severe thiamine deficiency can lead to Wernicke’s syndrome
– a potentially life-threatening disease that compromises the central and peripheral nervous systems. It is associated with short-term memory loss, confusion, disorientation and changes in eye movements
Beriberi is another condition associated with thiamine deficiency. It is divided into two types: wet and dry.
Wet beriberi negatively impacts the cardiovascular system and can lead to heart failure.Dry beriberi negatively impacts the nervous and muscular systems, potentially leading to muscle paralysis.
Toxicity: Thiamine is well tolerated and excess amounts can be secreted by the kidneys. Dietary toxicity is rare and there is no upper limit.
Vitamin B2: Riboflavin
RDA: 1.3 mg (M); 1.1 mg (F)
Function: Riboflavin helps form two important coenzymes: flavin mononucleotide (FMN) and flavin adenine dinucleotide (FAD)
These coenzymes are also involved in the conversion of the amino acid tryptophan to niacin. They are further involved in maintaining appropriate levels of homocysteine, a risk factor for cardiovascular disease.
Sources: Egg yolks, organ meats, fortified breakfast cereals, oats, milk, salmon, tuna, soybeans and almonds are all high in riboflavin. Dairy products are also high in riboflavin and are typically packaged in opaque containers to preserve their riboflavin content, as riboflavin is sensitive to light.
Deficiency: Riboflavin deficiency is called ariboflavinosis. It is characterized by skin disorders, swelling in the mouth and throat, dry and cracked lips, red eyes and hair loss.
Riboflavin deficiency is rare, though hormonal abnormality- es such as thyroid hormone deficiency may promote it. Animal products are better sources of riboflavin, so a meat-free diet may lead to deficiency. Vegans and vegetarians can meet needs by increasing the intake of vegetables higher in riboflavin or by taking supplements.
Toxicity: Riboflavin toxicity is rare because the body does not absorb more than a certain level and the kidneys excrete excess amounts.. Excess intake from food or supplements have not been observed to promote toxicity. Accordingly, there is no upper limit.
Vitamin B3: Niacin
RDA: 16 mg (M), 14 mg (F); UL: 35 mg.
Function: Niacin’s func ons are exerted by its main metabolically active form: the coenzyme nicotinamide adenine dinucleotide (NAD). It is accordingly critical to the metabolism of carbohydrates, lipids and proteins. This is just one of the reduction and oxidation reactions in which NADH is involved. NAD is critical to many metabolic reactions since more than 400 enzymes require it to function properly.
Niacin helps form the electron transport NADH + H+, which is critical for energy metabolism.
improving the blood lipids associated with CVD. High doses of niacin (>2000 mg) have been shown to reduce triglycerides and the lipid transporters VLDL and LDL.
niacin megadoses have also been shown to increase HDL, so-called good cholesterol. Since these megadoses improve CVD risk factors.
niacin megadoses did not reduce overall mortality or heart attack and stroke incidence. They further found that people in niacin treatment groups were more likely to discontinue treatment due to side effects such as niacin flush.
Sources: Animal products such as chicken, beef and fish are high in niacin. Plant products such as nuts, legumes and grains are also high in niacin, but have about half the niacin content of animal products by mass.
Getting adequate amounts of both protein and riboflavin can help promote niacin levels.
Deficiency: Niacin deficiency causes pellagra. Symptoms of pellagra are some me called the three Ds: dermatitis, diarrhea and dementia. In severe cases, pellagra can lead to another D: death. While rare today, in the early 1900s, pellagra plagued the southern USA before its cause was determined
toxicity: is rare from food. It is typically evidenced in those taking high doses for the management of blood lipids and/or CVD. Doses of 30 mg or more can cause niacin flush, which is the flushing, or reddening, of the skin accompanied by burning and itching sensations.
Consuming niacin in its niacinamide form instead of its nicotinic acid form can reduce symptoms of toxicity.
pellagra plagued the southern USA, leading to about 7,000 deaths per year. It caused a butterfly-like skin rash, negative mental effects and had a mortality rate of 40%.
Vitamin B5: Pantothenic Acid
AI: 5 mg.
Function: Pantothenic acid helps form coenzyme A. Coenzyme A is required for lipid, carbohydrate and certain amino acid metabolites to enter the citric acid cycle as acetyl CoA.
Pantothenic acid helps form coenzyme A.
Sources: Pantothen is Greek for everywhere. Indeed, pantothenic acid is widely available in a wide variety of both animal and plant products. Fortified cereals, beef, chicken, grains and vegetables are rich sources of pantothenic acid.
Deficiency: Due to its abundance in a variety of foods, pantothenic acid deficiency is rare. If present, it is often associated with malnutrition and other micronutrient deficiencies, making it difficult to establish symptoms of deficiency
deficiency may lead to numbness in the hands and feet, headache, tiredness, disturbed sleep and gastrointestinal issues.
Toxicity: There has been no reported human toxicity from high amounts of pantothenic acid from foods. Accordingly, there is no established upper limit. However, megadoses (10,000 mg) of pantothenic acid supplements have been associated with diarrhea and digestive tract distress
Vitamin B6
RDA: 1.3 mg; UL: 100 mg.
Function: Vitamin B6 is the generic name for six different vitamers. Vitamers are different forms of the same vitamin that have a common function. These vitamins act as coenzymes in the catalyzation of more than 100 enzymatic reactions, including the metabolism of carbohydrates, lipids and amino acids.
help form certain neurotransmitters, such as serotonin and norepinephrine, which support cognitive function.
Vitamin B6, B9 and B12 are involved in regula ng homocysteine levels
It has been implicated in improving cognitive function and reducing cancer risk. However, there is currently insufficient evidence to support these proposed effects.
Since vitamin B6 is associated with lower levels of homocysteine – a marker for CVD – it has also been suggested that supplementation may decrease risk. However, vitamin B6 supplementation has not been shown to decrease CVD incidence.
Sources: Vitamin B6 is found in many animal and plant foods. Chickpeas are the best plant sources of vitamin B6, while beef liver, tuna, salmon and chicken are excellent animal sources.
also found in fortified cereals and grains, as well as potatoes, bananas, squash and rice. Pyridoxine is the form of vitamin B6 that is typically found in supplements.
deficiency: is rare in isolation and is often found in combina on with other B vitamin deficiencies. In more pronounced cases, vitamin B6 deficiency can lead to macrocytic anemia, a condi on in which red blood cells are small and do not properly transport oxygen.
Symptoms include fatigue, lethargy, dry and cracked lips, and a swollen tongue. Individuals with kidney issues, alcohol dependency and certain autoimmune disorders tend to have lower vitamin B6 levels and have an increased risk for deficiency.
Toxicity: High vitamin B6 intake from food has not been shown to have adverse effects. However, prolonged supplementation of more than 1000 mg per day of pyridoxine, the supplement form of vitamin B6, can lead to a loss of control over body movements. High supplement doses should be taken only under the advice of a medical doctor and closely monitored.
Vitamin B7: Biotin
AI: 30 mcg
Function: Biotin is the generic name for five vitamins that function as coenzymes. These coenzymes are involved in the metabolism of carbohydrates, lipids and proteins. They are also involved in cell signaling and DNA structure and function.
Because deficiency is associated with compromised hair, nail and skin health, supplements of B7 are sometimes sold to improve these conditions. However, the results of studies into the ability of bi n to improve these tissues are mixed. More research is needed before supplementation can be recommended
Sources: Bion is abundant in many foods (Figure 8.14). One serving of beef liver affords 100% of the RDA. Other animal products such as chicken, tuna and pork are also excellent sources. Plant products such as sunflower seeds, sweet potatoes, almonds, spinach and broccoli are also high in bion.
Deficiency: Biotin deficiency is rare but may occur with certain conditions biotinidase deficiency negatively affects bioavailability and can lead to deficiency. Chronic alcohol
abuse can also lead to deficiency since it negatively affects bone absorption.
Signs and symptoms of deficiency include hair loss, red eyes and rashes around the eyes, nose and mouth. More serious cases may progress to seizures, depression and decreased muscle tone and strength.
Toxicity: High intakes of bion from food do not lead to symptoms of toxicity and there is no set upper limit.
Those who supplement with biotin should inform their doctor before laboratory tests are administered.
Vitamin B9: Folate
RDA: 400 mcg; UL: 1000 mcg.
Vitamin B9 can exist in a basic form as folate or in an acidic form as folic acid. Folate is predominant in food sources, while vitamin supplements and fortified foods typically have folic acid, which is more stable.
Function: Folate and folic acid function as coenzymes in the synthesis of DNA and RNA. They are also involved in the metabolism of amino acids. Further, they are involved in the conversion of homocysteine to methi.
Sources: Beef liver is in the most concentrated source of folate, with one serving providing more than half of the RDA. Spinach, legumes, asparagus, Brussels sprouts and avocados are also high in folate.
addition of folic acid to cereal grains. Accordingly, these are also good sources of folic acid.
Deficiency: Folate deficiency in non-pregnant individuals is rare. If it does occur, it is typically associated with other micronutrient deficiencies that might occur due to poor diet, alcohol dependency or absorption issues.
Pregnant women with inadequate folate levels are more likely to have offspring that develop neural tube defects. Folate is necessary for the synthesis of DNA in a developing embryo and fetus. Accordingly, deficiency can compromise the development of the neural tube.
embryonic structure that develops into the brain and spinal cord.
Spina bifida leads to physical problems, such as leg weakness, scoliosis and bladder and bowel issues, as well as neurological problems in which planning, organizing and attention are compromised.
anencephaly, which is when a child is born missing major parts of their brain. This defect typically results in infant death within a few hours of birth.
Folate deficiency can also lead to megaloblastic anemia – a disorder in which red blood cells are immature, large, misshapen and unable to properly carry oxygen.
inability to properly synthesize DNA during red blood cell production. Both folate and vitamin B12 deficiency can cause this type of anemia, which leads to tiredness, weakness and heart irregularities.
Autism is a complex disorder whose causes are not fully understood. An interesting newer area of research explores whether folic acid supplementation before and during pregnancy lowers the risk of autism in children.
Toxicity: Folate is generally well tolerated. Symptoms of toxicity are uncommon, but may include nausea, bloating, decreased appetite and difficulty sleeping.
folate and vitamin B12 are involved in the conversion of homocysteine to methionine as well as in the prevention of megaloblastic anemia. If folate intake is high, it can accordingly mask a vitamin B12 deficiency. While folate supplementation can correct the neurological damage of megaloblastic anemia, it cannot correct the neurological damage from a vitamin B12 deficiency.
Vitamin B12 Cobalamin
RDA: 2.4 mcg.
Functions: Vitamin B12 has various vitamins that are collectively known as cobalamins. These are required for DNA synthesis, the formation of mature red blood cells and brain function. Vitamin B12 also acts as a coenzyme in the conversion of homocysteine to methionine.
involved in fat and protein metabolism.
Vitamin B12 has been proposed as a way to decrease the risk of dementia. While research is ongoing, the evidence
is currently insufficient to recommend supplements digestion and absorption of vitamin B12 relies on stomach secretions. The process begins with the activity of hydrochloric acid in the stomach, which helps release vitamin B12 from food.
The stomach also releases intrinsic factor (IF), which is needed later in the small intestine for vitamin B12 absorption. Vitamin B12 cannot be absorbed in free form, and thus binds to IF, which allows it to enter the villi of the ileum.
atrophic gastritis, an autoimmune disorder that results in the breakdown of the stomach’s lining, restricts intrinsic factor secretion and significantly increases the risk for vitamin B12 deficiency.
Intrinsic factor is required for B12 absorption.
Sources: Vitamin B12 is found in a wide variety of animal products. Shellfish, fish and beef liver are particularly high in vitamin B12. Plant foods do not typically contain vitamin B12 unless they are fortified. Nutritional yeast is another potential source that can supplement vitamin B12 into the vegetarian or vegan diet.
Vitamin B12 supplementation is one of the most common recommenda-ons for those who follow a partial or fully plant-based diet.
Deficiency: Megaloblastic anemia is the main outcome of vitamin B12 deficiency. Accordingly, individuals with vitamin B12 deficiency may experience fatigue, weakness and lethargy, constipation and loss of appetite
deficiency can also lead to balance issues, depression, poor memory and confusion.
Toxicity: There are no reported adverse effects of excess vitamin B12 intake, either from supplements or food. There is therefore no upper limit for vitamin B12. However, B12 can interact with certain medications and higher intake levels from supplements should be mentioned to doctors and pharmacists.
Vitamin C: Ascorbic Acid
RDA: 90 mg (M), 75 mg (F); UL: 2000 mg.
The first known cure is attributed to Iroquois who lived in present day Quebec city and who cured Jacques Cartier's crew of the condition
Functions:Ascorbic acid, L-ascorbic acid or simply vitamin C is involved in a wide range of body processes. It is critical in the formation of the protein collagen, which forms the main structure of bones, ligaments, skin and a variety of other body structures.
Vitamin C is also involved in the metabolism of protein. In addition, it is well known for its antioxidant fun. Another well-known benefit of vitamin C is its ability to increase the absorption of iron, reducing the risk for iron-deficiency anemia. It is also one of the body’s key antioxidants.
Vitamin C promotes collagen cross-linking.
Antioxidants are substances that help reduce the activity of free radicals.
Free radicals are reactive molecules that have an unpaired electron. They accordingly steal these electrons from other molecules such as DNA and cell membranes. When a molecule loses an electron, it is oxidized, which often damages it. Antioxidants stop oxidation by dona ng their extra electrons to free radicals, neutralizing them so they cannot cause damage.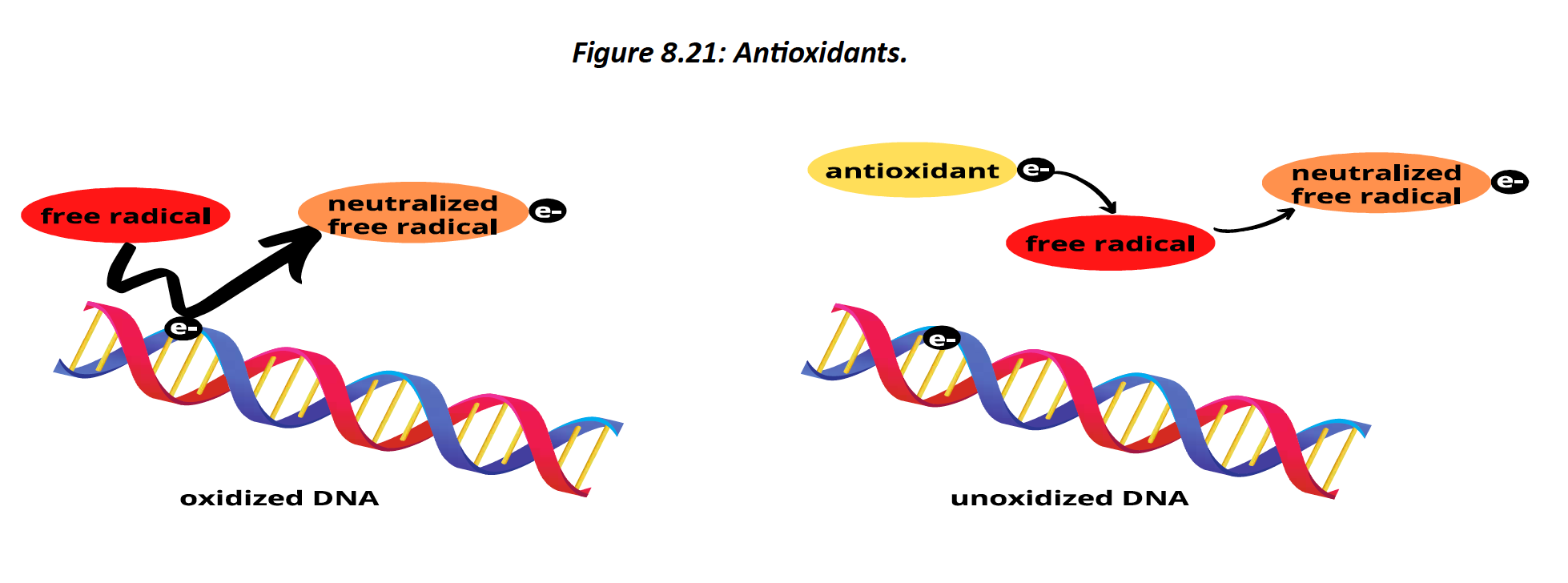
Vitamin C has long-been suggested as a treatment for the common cold and other infections. While vitamin C does support the proper function of the immune system, it does not cure the common cold, which has no cure.
In studies involving athletes, such as marathon runners and skiers, a 50% decrease in cold incidence was observed, but only if the supplement was taken before the cold began.
increased consumption of foods that contain vitamin C – like many fruits and vegetables is associated with a lower risk of both diseases.
Sources: Vitamin C is synthesized by most animals except for humans. We therefore must consume this vitamin from food or supplements to meet our needs. Vitamin C is abundant in
fruits and vegetables. Just half a cup of raw red peppers or ¾ of a cup of orange juice provides more than 100% of the RDA.
abundant in citrus fruits, such as oranges, grapefruits, kiwis and lemons, as well as tomatoes
and strawberries. The vegetables broccoli, Brussels sprouts and cauliflower are also quality sources.
Deficiency: Scurvy is evidenced by fatigue and gum inflammation. If deficiency is prolonged,
It can negatively affect collagen formation, wound healing and joint integrity leading to bleeding gums and loss of hair and teeth. Nowadays, scurvy is rare in populations that consume a variety of fruits and vegetables.
Toxicity: Though an upper limit of 2000 mg is set, toxicity from vitamin C is relatively mild. Gastrointestinal effects such as diarrhea, nausea and abdominal cramps may occur in those who consume too much. Like other supplements, vitamin C may interact with medications.
9.4 - fat soluble vitamins
There are four fat-soluble vitamins – vitamins A, D, E and K
unlike the water-soluble vitamins, these vitamins are stored in fat tissue, so we need
them less often. Since they are stored, they are also more likely to lead to symptoms of toxicity
absorption and transport are dependent on lipid carriers such as micelles and lipoproteins.
When the body is deficient in lipids, or if there are issues with lipid absorption, the bioavailability of fat-soluble vitamins suffers, and deficiency can occur.
Vitamin A
RDA: 900 mcg (M), 700 mcg (F); UL: 3000 mcg.
Vitamin A has several vitamers that include retinol, retinol and retinyl esters. As a group, they are referred to as retinoids. We consume vitamin A in one of two forms: provitamin A and preformed vitamin A.
Provitamin A is found in plants and its vitamins are collectively known as carotenoids. Carotenoids are not in their active form of vitamin A and must be converted into retinoids before they can be further modified into their active form.
most well-known carotenoid is beta-carotene, which helps give certain plants their orange colour
Preformed vitamin A is found in its almost-acve forms: retinol and retinyl ester. These retinoids are found in animal products including dairy. Animal products also contain provitamin A, but to a lesser degree.
For retinoids to become fully active, the body must metabolize them into retinal and retinoic acid – the active forms of vitamin A.
Functions: most known for its role in the visual pathway. Vitamin A-derived retinal binds to the protein opsin to form the visual pigment rhodopsin, found in the rods of the eye’s re na. When rhodopsin absorbs light, a message is sent along the visual pathway to help us interpret what was seen. This helps improve our vision at night or in low light
claim that vitamin A improves our ability to see at night is not true
involved in gene expression, helping to turn certain genes on or off . This affects whether DNA
is transcribed into proteins.
Vitamin A is also involved in immune function, specifically by contributing to the formation of infection-fighting T-cells. The carotenoid form of vitamin A found in plants further acts as an antioxidant, helping to reduce the activity of potentially harmful free radicals.

Many people believe that vitamin A helps us see deer at night. However, we might be surprised to learn that this false rumor was started by the British Air Force during the
Second World War. To hide the development and use of radar technology, the British started a propaganda campaign to convince people that eating carrots helped them see better at night
Vitamin A promotes skin health by switching on the genes that cause immature skin cells to become mature and healthy
individuals who overuse retinoids may experience skin irritation, burning, scaling and dermas. Products with higher retinoid doses, such as the retinoic acid product Accutane, are also sometimes prescribed for the treatment of severe acne. While effective, this product can have severe skin, gastrointestinal, nervous system and cardiovascular side effects
Sources: Preformed vitamin A is available in many animal products, while provitamin A is found in many orange and leafy green plants. both humans and other animals, most vitamin A is
stored in the liver. Other animal products that are good sources include fish oils, milk and eggs
The provitamin form of vitamin A is found in many plant products. A single serving of sweet potatoes has more than the RDA. Spinach, carrots, pumpkin, cantaloupes,
red peppers and other orange and leafy green vegetables are also excellent sources of provitamin A.
Deficiency: rare in Canada and the USA, vitamin A deficiency is common in developing countries. It is typically due to poverty leading to a less varied diet that is low in both preformed and provitamin A.
deficiency in children and pregnant women is typically evidenced by xerophthalmia – abnormal dryness of the eye that affects the body’s ability to form tears. If untreated it can lead to breaks in the cornea of the eye, leading to further damage and potentially blindness. Night blindness is an early sign of xerophthalmia.
Toxicity: no reported negative health effects of consuming carotenoids from plant products. In some cases, the skin may turn slightly orange due to the extra pigments consumed, high intakes of preformed vitamin A from animal products can lead to serious side effects. Prolonged excessive preformed vitamin A intake increases the risk of elevated pressure around the brain, dizziness, nausea, headaches and can be fatal.
This is almost always due to overconsuming supplements
Vitamin D
RDA: 15 mcg; UL: 100 mcg
Functions: most important ones being vitamin D3 (cholecalciferol)
and vitamin D2 (ergocalciferol). These compounds are critical to maintaining calcium homeostasis. Specifically, they increase calcium absorption in the digestive tract, while also contributing to the absorption of other bone-mineralizing minerals like magnesium and phosphate
Vitamin D supplementation does not reduce risk of colon cancer
Sources: Vitamin D is not widely available in foods. Fatty fish such as salmon, tuna and mackerel as well as fish oils are naturally high in vitamin D. Certain foods like orange
juice and milk products are also sometimes fortified with vitamin D, but do not contain significant amounts naturally.
In Canada, food and drug regulations mandate the for fi canon of vitamin D into fluid milk.
Sun exposure is our main source. To be clear, vitamin D is not absorbed through the skin from the sun. Instead, ultraviolet B (UVB) light penetrates the skin and promotes the conversion of vitamin D precursors to its fully active form.
Generally advised to limit sun exposure during peak UV times of the day to between 10 and 30 minutes.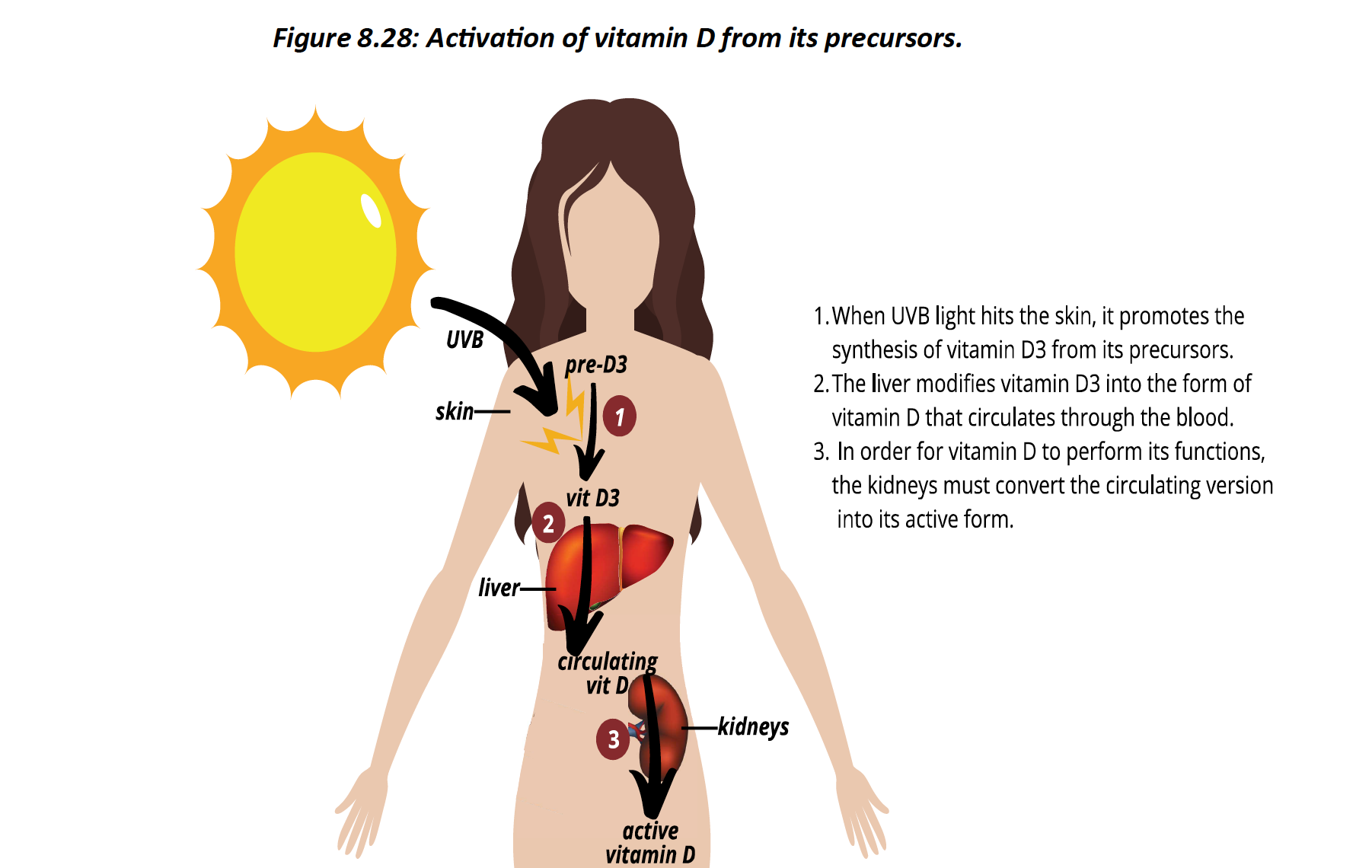
Deficiency: Vitamin D deficiency is common and can be due to both inadequate vitamin D from the diet or limited sun exposure
vitamin D deficiency can lead to rickets. Rickets is associated with a lack of bone mineral density that leads to soft bones. Accordingly, legs that curve outwards is a characteristic sign of rickets. This occurs because vitamin D deficiency impairs bone mineral availability,
and the weight of the growing body causes weakened bones to bow outwards.
vitamin D deficiency can lead to osteomalacia – a softening of the bones due to decreases in bone mineralization. While calcium deficiency can also lead to osteomalacia, its most common cause is vitamin D deficiency.
Prolonged vitamin D and calcium deficiency may progress to osteoporosis, a condition in which bones are not only weakened but have less hardened bone tissue, making them more likely to break.
The RDA for vitamin D increases by more than 30% after the age of 80.
Those who have darker skin are more likely to be deficient since dark skin limits the ability to produce vitamin D precursors.
Toxicity: typically due to over-supplementation. Anorexia, weight loss, increased urination and irregular heart rhythms are poten al symptoms of toxicity.
excessive vitamin D intake can increase calcium levels to a harmful level. Excessively high blood calcium can harden blood vessels and eyes and can negatively affect the kidneys and heart. Vitamin D toxicity may also increase the risk of kidney stones due to the high mineral concentration of the blood
Vitamin D toxicity can lead to the hardening of the kidneys and heart
Vitamin E
RDA: 15 mg; UL: 1000 mg
Vitamin E is the generic term for a group of eight vitamers. These are further divided into tocotrienols and tocopherols, the most notable and nutritionally relevant of which is alpha tocopherol.
Function: Vitamin E exerts its main effects through its antioxidant role. It can help protect cells from the harmful effects of free radicals by donating electrons and neutralizing them. Vitamin E is further involved in immune function, cell signaling and gene expression.
Sources: Vitamin E is found primarily in the oily germ of cereal grains. Accordingly, the richest sources of vitamin E are vegetable oils. Fatty shellfish and fatty plants such as nuts, seeds, fortified cereals and nut butter are also good sources.
Deficiency: Vitamin E deficiency is rare in Canada and the USA. If found, it is often associated with compromised fat absorption, such as in individuals who have had gastric surgery or in individuals with Crohn's disease or cystic fibrosis. Symptoms may include peripheral neuropathy, movement difficulties, muscle disorders and an impaired immune response.
Toxicity: Vitamin E toxicity has not been established from food consumption. However, supplements of vitamin E may lead to a higher mortality risk. Indeed, two clinical trials both found that prolonged intake of high levels of vitamin E increased the risk of stroke.
Vitamin E has also been linked with lung issues in those who vape. Accordingly, caution should be taken with supplementation.
Vaping: Laboratory assessments performed by the American Center
for Disease Control found elevated levels of vitamin E acetate in the blood samples of the affected people
Vitamin K
Functions: Danish word koagulation, whose English translation coagulation refers to
blood clotting. Indeed, the vitamin K family of vitamins function as coenzymes in the pathway that leads to blood coagulation
synthesis of the protein prothrombin is dependent on a vitamin K coenzyme.
Prothrombin is a proenzyme that is activated into thrombin. Thrombin, in turn, helps convert the proenzyme fibrinogen into fibrin.
Fibrin fibres are sky and link together to help the blood clump together, causing it to coagulate. Without this ability, we are more likely to have thinner blood and have an increased risk of bleeding and hemorrhage.
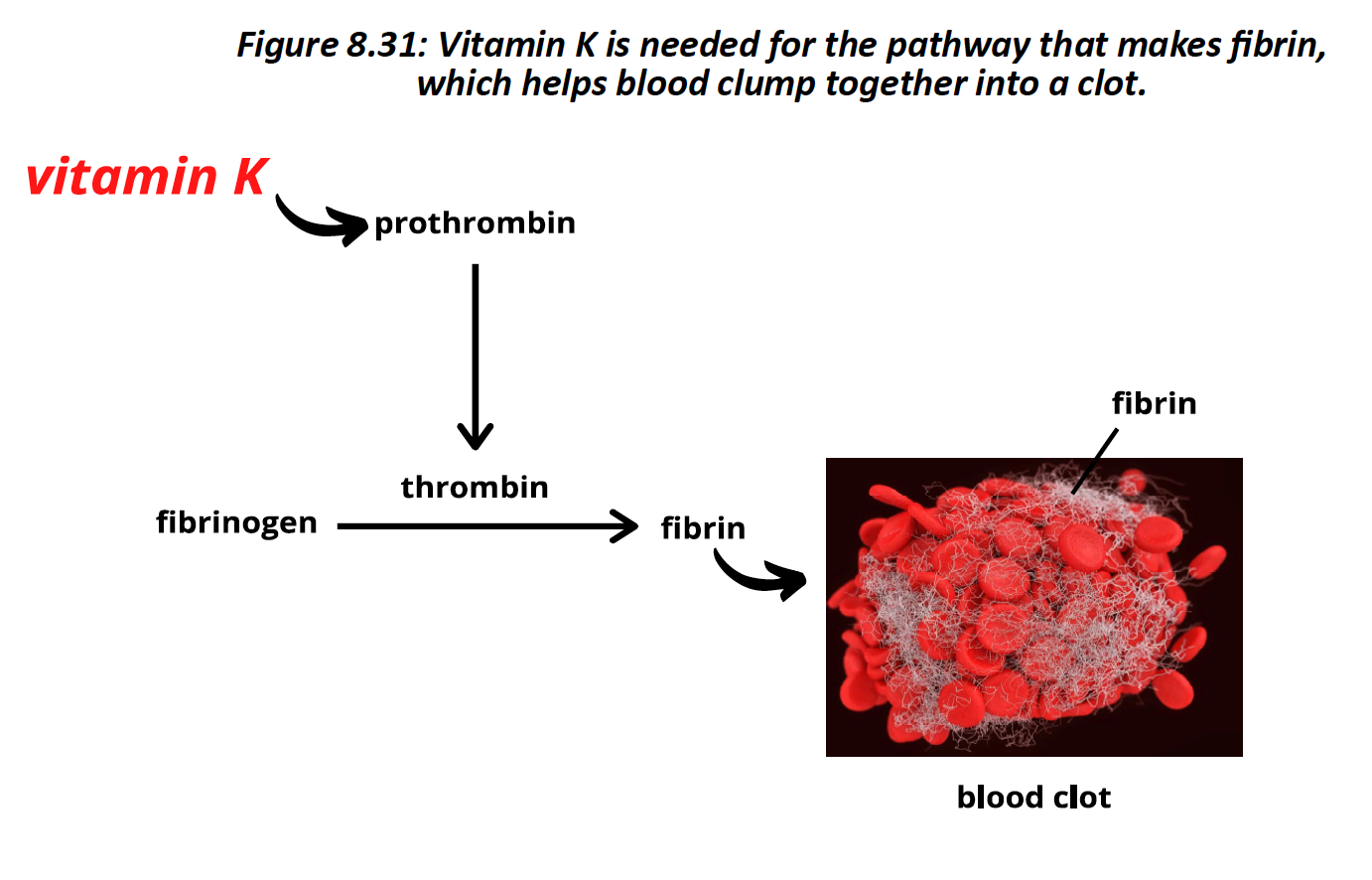
Sources: Vitamin K is found in leafy-green vegetables, such as spinach and broccoli, as well as oils and nuts. attained from animal products such as liver, ham, cheese and milk. A healthy gut microbiota contributes to vitamin K bioavailability, as certain organisms can synthesize different forms of vitamin K
Deficiency: rare in healthy adults unless they have an issue with vitamin K absorption. Initial symptoms of vitamin K deficiency may not be evidenced until it progresses to more severe clinical symptoms such as increased bleeding and hemorrhaging.
Newborns are at high risk for vitamin K deficiency since it is poorly delivered via the placenta Accordingly, the Canadian Pediatric Society and the American Academy of Pediatrics recommend a single dose of 0.5 to 1.0 mg of vitamin K to all newborns
Breast milk is low in vitamin K thus a shot of this vitamin is typically administered to newborns
Vitamin K is also involved in bone mineralization, so deficiency may lead to decreased bone density and even osteoporosis. Vitamin K deficiency can sometimes be discovered through a prothrombin time test – an exam that evaluates how well the blood coagulates.
Warfarin is a drug sold under the brand name coumadin. It is prescribed to individuals with a high risk for heart attacks and strokes, conditions in which a blood clot can block an important
artery in the heart or brain, respectively. Warfarin is an anticoagulant that blocks the vitamin K-dependent coagulation pathway, decreasing the formation of blood clots.
Warfarin first came to the market as a rat poison.
Toxicity: Vitamin K does not have an upper limit – no adverse effects from foods or supplements have been observed
Vitamin infused beverages
In Canada, vitamin-infused beverages are considered natural health products, not foods.
Since these beverages have a water base, they can only contain water-soluble vitamins – those that are less likely to be deficient in the North American diet. Furthermore, drinking these beverages may provide a false sense of healthfulness to someone with a less healthy diet.
9.5 - an indigenous lens
James Lind, a Scottish doctor, is well-known for identifying citrus fruits as a cure for scurvy. This discovery helped ensure that British sailors had enough lime juice to last their months at sea, during which they were more likely to develop the disease.
The first known remedies for scurvy were identified. The Iroquois of what is now Quebec City had a cure for scurvy since at least the 1500s. They shared this cure with the invading French explorers commanded by Jacques Cartier.
The concoction is believed to have been made from boiling winter leaves plus the bark of what they called the annedda tree.
It has since been discovered that the concoction made by the Iroquois was both high in vitamin C and several amino acids, including arginine and proline. It really was a miracle cure, because it not only contained vitamin C, but also essential amino acids, which are both needed for collagen synthesis.
Cartier did not repay the Iroquois for the lifesaving favors given to him. Instead, he kidnapped Donnacona, the Iroquois chief, and members of his tribe and took them to France where they could tell of the riches found in Canada.
Chapter 9
10.2 - overview of minerals
Minerals are solid, naturally occurring, inorganic substances. They are found throughout nature, often bound to other minerals or substances, such as in rocks. The human body requires certain minerals to sustain life
they do not provide energy, minerals are essential structural and functional nutrients. Accordingly, mineral deficiencies are associated with a range of complications.
Carbon, oxygen, hydrogen and nitrogen are sometimes called the basic organic elements because they are found within the molecules that make up living things, such as carbohydrates, lipids and proteins.
minerals are elements that form solid compounds and are not bound to carbon. They are therefore inorganic.
Minerals are further classified based on how much of that mineral is required from the diet. Major minerals are those required in higher amounts, while minor minerals, also known as trace minerals, are needed in smaller amounts.
Major minerals make up about 3% of the body’s weight and include calcium, phosphorus, potassium, sodium, chloride, sulfur and magnesium
Trace minerals make up about 0.15% of the body’s weight. They include iron, copper, zinc, molybdenum, manganese and selenium
Indigenous lens: Western science defines organic matter as that which contains carbon and comes from living things. Minerals do not contain carbon, which according to a Western science lens, makes them non-living, inorganic things. If you talk about a rock in English, you are thinking about it being something static, something fixed…but in Ojibway, when you’re talking about asin or asiniig, you’re talking about something that is alive, something that has a spirit, something that is in motion. And if you can start to conceive of things around you in a different way, I think it’s going to open up your worldview…
The bioavailability of a mineral refers to its availability in food as well as its propensity to be absorbed and available for use within the body. Both plants and animals are a source of minerals.
The quantity and diversity of minerals found in plants depends on the mineral composition of the soil in which they are grown. The mineral content of animal products depends on what the animal consumes. The more an animal eats, the more concentrated in minerals they become.
Plant compounds, such as phytates, oxalates, tannins and glucosinolates, can negatively affect mineral absorption sometimes referred to as anti-nutrients because their presence in foods reduces the amount of minerals absorbed.
Phytates are found in plant seeds and are abundant in nuts, legumes and grains. Plant foods can vary a lot in their phytate composition, with nuts and beans tending to contain especially high amounts.
Phytates impair iron and zinc absorption. They also negatively affect calcium absorption, but to a lesser extent. Phytate levels can sometimes be reduced by soaking certain foods overnight.
Oxalates are found in leafy green vegetables, nuts and seeds. Oxalates bind to minerals, forming compounds that cannot be absorbed. Specifically, oxalates decrease calcium and iron bioavailability. Boiling foods high in oxalates can significantly reduce their oxalate content.
Tannins are found in tea, coffee, red wine and legumes. Tannins interfere with iron absorption. Those prone to iron-deficiency are advised to avoid consuming tannin-rich foods and beverages with meals that contain iron. tannins have also been studied for a wide range of disease-reducing effects. Specifically, they have been shown to have anti-cancer, antioxidant, antimicrobial and anti-inflammatory properties.
Glucosinolates are found in cruciferous vegetables such as broccoli, Brussels sprouts and cabbage. They compromise iodine absorption.
Many minerals achieve their functions because they act as cofactors. Cofactors are inorganic metals that bind to enzymes, often acting them and thus improving the rate of reaction.
proteins may require an inorganic (cofactor) or organic (coenzyme) substance in their structure to become active. In other words, cofactors and coenzymes are needed to help enzymes do their work. facilitate the enzymatic processes necessary for life.
10.3 - major minerals
Calcium
RDA: 1000 mg; UL: 2500 mg
Calcium is the most abundant mineral in the human body. accounting for approximately 1.5% of the body’s weight
Functions: calcium is a key signaling molecule; it helps send nerve signals and is an important messenger within cells. It is also needed for muscle and heart contraction and for securing substances from gland.
99% of the body’s calcium is stored within the bones and teeth (Institute of Medicine, 2011). This, in turn, promotes their structure and stability.
Calcium supplementation may help moderately reduce the risk of colorectal cancer. quality of evidence was not high enough to suggest recommending calcium supplements on to reduce cancer risk. Same with decreasing the risk of cardiovascular disease (CVD) and obesity.
Homeostasis: When calcium levels are too low, body processes that require calcium are compromised. Conversely, when blood calcium is too high, it can deposit in tissues, hardening and damaging them.
When calcium levels drop, parathyroid hormone (PTH) is released. PTH restores calcium levels through three mechanisms.
- PTH promotes calcium release from bones by activating bone breaking cells called osteoclasts.
- PTH decreases calcium excretion at the kidneys, so more is kept within the blood and less is lost in urine.
- PTH promotes the action of vitamin D at the kidneys. Vitamin D then promotes calcium absorption at the small intestine.
blood calcium is high, the hormone calcitonin is released. Calcitonin opposes the actions of
PTH leading to a decrease in blood calcium. Indeed, calcitonin impairs osteoclast activity in bone, leading to less being released into blood.
It promotes calcium excretion at the kidneys and a decrease in calcium absorption at the
small intestines.
Parathyroid hormone maintains adequate blood calcium levels.
Sources: The main sources of calcium are dairy products. It can also be found in eggs, canned
fish with bones, fortified milk alternatives and leafy green vegetables.
Deficiency: if we are consistently at a calcium deficit, our ability to achieve peak bone mass decreases, and our risk of osteoporosis increases. Peak bone mass is typically achieved within our 20s, after which it decreases over time.
Until approximately age 30 bone density increases. Following this age, bone mass tends to decrease.
Achieving a higher peak bone mass and maintaining bone density throughout life are key to reducing our risk of osteoporosis.
Bone mass decreases after peak bone mass is achieved.
Osteoporosis is a lack of bone mineralization and density and is the main cause of bone fractures in older adults. It is caused by an imbalance in bone remodeling favoring the breakdown of bone by osteoclasts. Peak bone mass influences risk for osteoporosis, as do factors that negatively affect bone mineralization.
Women are at higher risk for osteoporosis since their peak bone mass is not as high as males Also, hormonal changes around menopause further promote decreases in bone density, further increasing risk for osteoporosis
modifiable risk factors include physical inactivity, smoking, alcohol consumption and a lower body weight. Non-modifi able risk factors include female gender, age and family history. In addition to its effects on bones, severe calcium deficiency can lead to numbness, muscle spasms, seizures and confusion.
Toxicity: Minor increases in blood calcium often present no symptoms. chronically elevated levels or a quick increase in calcium levels may be evidenced by abdominal pain, bone pain and mental confusion. Consistently high levels of calcium can be fatal as they can lead to the calcification, or hardening, of the tissues
Calcification of the tissues is typically due to other conditions such as an overactive parathyroid gland or cancer.
Phosphorus
RDA: 700 mg; UL 4000 mg
Phosphorus is the second most abundant dietary mineral in the human body and has both structural and functional roles
Functions: Phosphorus is found within hydroxyapatite – a crystal that contains both calcium and phosphorus. This crystal mineralizes bones and teeth, hardening them and promoting their strong structure.
a critical component of all cells, as it is needed to form the phospholipids that make up the cell membrane. It is also part of the key physiological molecule ATP (adenosine triphosphate) as well as DNA and RNA, which have a sugar-phosphate backbone.
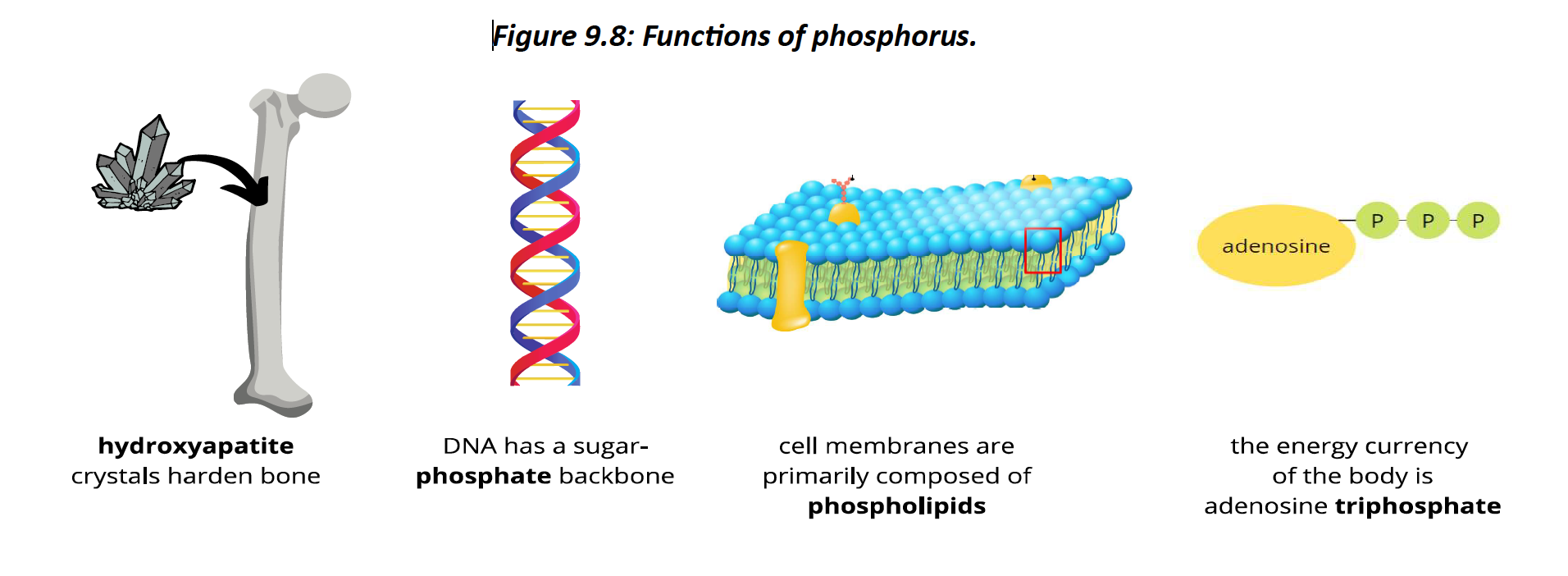
Sources: Phosphorus is abundant in animal products such as salmon, cheese, milk, eggs and beef. Plant sources include boiled lentils, cashews, potatoes, kidney beans, rice and oatmeal.
Deficiency: phosphorus is abundant in many foods, dietary deficiency is rare; it typically occurs with severe malnutrition. Phosphorus deficiency can increase the risk for osteoporosis, seizures and coma. Symptoms of deficiency include anorexia, muscle weakness, anemia and an increased risk of infection.
Toxicity: Phosphorus toxicity is rare in healthy individuals. High levels can lead to the hardening of the tissues.
Sodium
AI: 1500 mg; UL 2300 mg
Function: Sodium, potassium and chloride are collectively known as the electrolytes, meaning they are involved in the body’s electrical activity .
sodium is the main electrolyte found in the extracellular space.
electrolytes are minerals that become charged when dissolved in water. They are responsible for the electrical activity of the body.
electrolytes become ions – atoms that carry a positive or negative charge. Their movement therefore leads to the creation of an electrical current, which facilitates the electrical activity and function of our nerves, heart and muscles.
Electrolytes are responsible for the body’s electrical activity. The movement of sodium into a cell is part of what leads to the transmission of an electrical signal.
important role in regulating fluid balance in the body. Water moves across a semipermeable membrane to equal out concentration differences. Without this fluid balance, water can
build up in a tissue, causing it to swell.
Sources: found naturally in many foods and is also added during food processi. three
quarters of the sodium we consume comes from the sodium added to processed foods
Smoked, cured and salted animal products, as well as canned entrees, salted nuts and many prepackaged foods are all high in sodium. Table salt, or simply salt, is sodium chloride (NaCl). The salt we add to our food at the dinner table contributes only about 5% to our sodium intake.
Deficiency: hyponatremia, which typically arises due to excessive vomiting, sweating or diarrhea situa ons in which the body loses a large number of electrolytes, including sodium. Symptoms of hyponatremia include nausea, vomiting, irritability, fatigue, loss of appetite, confusion, muscle weakness and spasm. In more extreme cases, it can lead to loss of consciousness and coma.
Toxicity: caused by the excessive loss of body water, which concentrates the amount of
sodium in the blood. At higher and chronic levels, sodium toxicity can lead to confusion, muscle twitching and brain hemorrhages. People who regularly consume high levels of sodium may also be at higher risk for hypertension, or high blood pressure.
when blood pressure is chronically elevated – especially above values of 140/90 mmHg, which are considered hypertensive. Hypertension is a main risk factor for CVD since it increases the risk for heart attacks and strokes.
diets that are high in whole foods, potassium and fibre, moderate in
calories and low sodium are associated with a decreased risk. These are the foundations of the Dietary Approaches to Stop Hypertension (DASH) eating plan, which is recommended to reduce the risk for, as well as in the management of, hypertension.
DASH eating plan emphasizes whole foods, particularly fruits, vegetables, whole
grains, low-fat dairy, poultry, fish and nuts and is high in fibre, potassium, magnesium, calcium and protein
Potassium
AI: 3400 mg (M), 2600 mg (F)
Function: main role of potassium is as an electrolyte. In water, potassium also becomes a positively charged ion. While sodium is the main ion found in the extracellular space, potassium is the main ion found in the intracellular space – that is, within the cytoplasm of a cell
Potassium and sodium also share the role of maintaining fluid balance.
diets higher in potassium promoted lower blood pressure
The government of Canada allows health claims on food labels stating, “A healthy diet containing foods high in potassium and low in sodium may reduce the risk of high blood pressure, a risk factor for stroke and heart disease.
Sources: Potassium is abundant in many whole foods but is often removed during food processing. Dried apricots, lentils, squash, potatoes, kidney beans, bananas, dairy products and salmon are all naturally high in potassium.
deficiency: no obvious symptoms
If individuals do show symptoms, they may feel tired, have weakness or experience cramps. Low blood potassium can further increase the risk of an irregular heart rhythm, promoting a slower heart rate that can lead to cardiac arrest. Clinical potassium deficiency is typically caused by excessive vomiting, diarrhea or certain medications.
Toxicity: so higher intakes do not pose a health risk in healthy individuals. Those with impaired kidney function, who are on certain medications, or who have type 1 diabetes may have limited potassium excretion potential, increasing their risk for toxicity.
severe cases it can promote muscle weakness, heart irregularities and paralysis through over supplementation
Chloride
AI: 2300 mg; UL: 3600 mg
Function: mineral that functions as an electrolyte chloride is essential for the body’s electrical activity as well as for maintaining fluid balance. It is also part of hydrochloric acid, which is secreted by the stomach and contributes to protein digestion.
Sources: Table salt – sodium chloride – is our main dietary source of chloride
Deficiency: salt is so abundant in the North American diet, chloride deficiency is rarely due to low dietary intake. Conversely, respiratory issues, vomiting and kidney malfunction are the main causes of chloride deficiency
no symptoms, though in some individuals it can promote weakness, difficulty breathing, diarrhea and vomiting.
Toxicity: typically asymptomatic. Since it can accompany other electrolyte toxicities, similar symptoms such as tiredness and muscle weakness may occur. Again, this electrolyte imbalance is not typically due to dietary excess, but to irregular fluid balance in the body, which can concentrate chloride.
Magnesium
RDA: 400-420 mg (M), 310-320 mg (F); UL: 350* mg
*from supplements
Function: cofactor for more than 600 enzymes, promong many physiological movies. involved in enzymatic reactions including energy metabolism and protein synthesis. Magnesium also helps DNA and RNA form their three-dimensional structure. healthy brain development and maintaining a healthy heart bone density by supporting the formation of hydroxyapatite crystals
The body's magnesium content is stored in bone.
Magnesium may help prevent migraine headaches. Randomized control trials have found modest reduction in migraine occurrence with a 600 mg/day magnesium supplement
Sources: Magnesium is plentiful in many foods including nuts, spinach, soymilk, black beans, edamame, bananas and avocado.
Deficiency: kidneys tightly regulate magnesium levels, dietary magnesium deficiency is rare
kidney malfunction, chronic alcoholism or who consistently consume low levels of magnesium may experience certain symptoms. Loss of appetite, nausea, vomiting, fatigue and weakness are early signs of magnesium deficiency. Symptoms can progress to more severe ones such as cramping, numbness, tingling, heart irregularities and seizures.
Toxicity: kidneys regulate magnesium levels so that they do not reach toxic states. Rare in healthy individuals
due to dietary supplements or medicines can lead to gastrointestinal issues such as diarrhea, nausea and abdominal cramping.
Magnesium toxicity can promote low blood pressure, depression, muscle weakness and tiredness. It can progress to heartbeat irregularity, difficulty breathing and heart failure. Supplement intake should accordingly be closely monitored.
Sulfur
RDA/UL: Not determine
Sulfur is the third most abundant mineral in the human body.
Function: synthesis of the amino acids methionine and cysteine, whose side chains contain sulfur atoms. The presence of sulfur in these amino acids is cri cal to the three-dimensional structure of proteins, as bonds between sulfur groups help the amino acid chain fold into a
functional protein
formation of the enzyme glutathione peroxidase, an important antioxidant
that can decrease cellular damage. Other minerals and vitamins also promote glutathione peroxidase function by acting as cofactors and coenzymes.
Glutathione peroxidase neutralizes the free radical hydrogen peroxide.
Sources: Protein-rich foods supply the body with ample sulfur through the sulfur-containing amino acids methionine and cysteine.
Cruciferous vegetables like cauliflower, cabbage, kale, broccoli as well as leafy vegetables are
naturally high in sulfur. Tap water and other beverages may also help us meet sulfur needs.
Deficiency: Most Canadians consume adequate protein, which is our main source of sulfur, so sulfur deficiency is rare. In populations with inadequate protein intake, sulfur deficiency can contribute to protein-energy malnutrition.
Toxicity: Sulfur toxicity from dietary consumption is rare. However, excessive supplementa on, consuming tap water with high sulfate levels or kidney malfunc on can increase risk. Excess sulfur can promote diarrhea and perhaps colitis, though more research into this potential risk is needed.
10.4 - minor minerals
minor minerals are required in much smaller amounts. Like the major minerals, they are critical for the proper structure and function of the human body
Iron
RDA: 8 mg (M), 18 mg (F); UL: 45 mg
Functions: Iron is essential for the structure and function of many proteins and enzymes. It is particularly critical for the formation of functional hemoglobin – the oxygen-carrying protein found in red blood cells. This protein has four iron ions in its structure, making it a bonding site for oxygen molecules
Myoglobin, also known as myo hemoglobin, is another oxygen-transporting compound that requires iron. It is found in muscle cells and contributes to their energy metabolism.
Red blood cell showing hemoglobin protein and iron-dependent heme group.
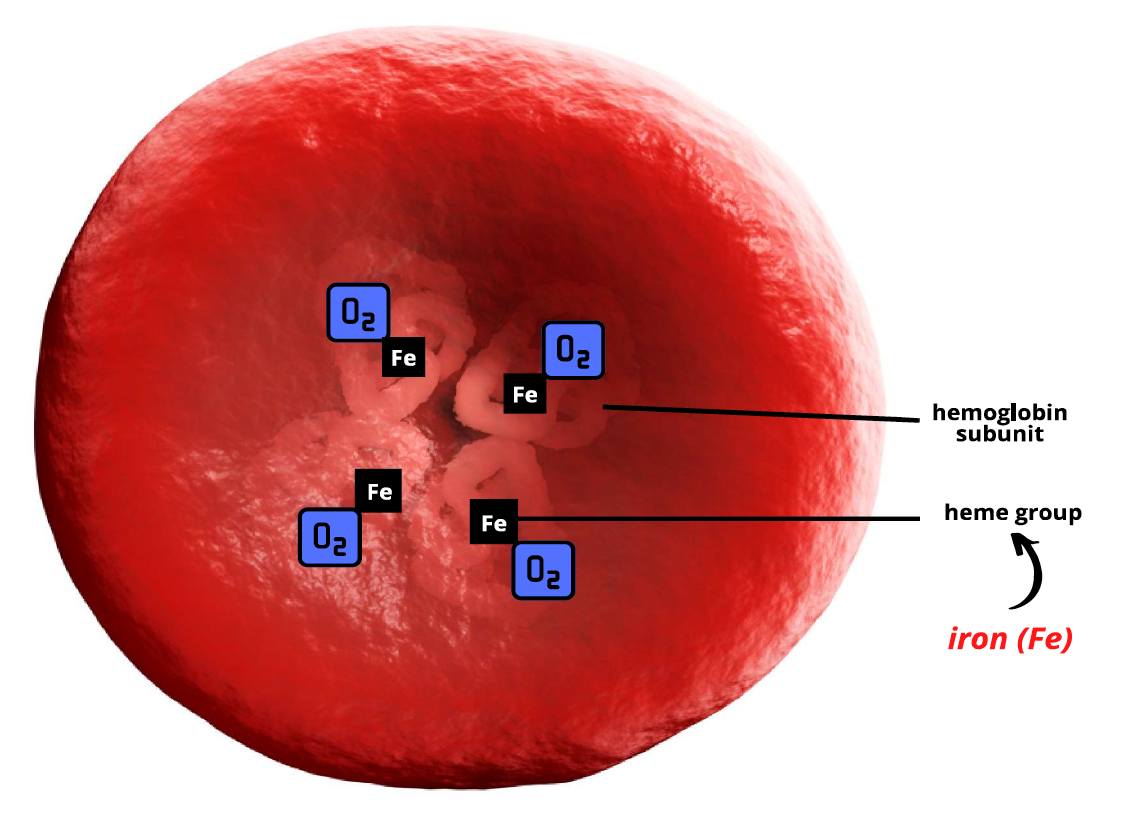
Sources: Iron is found in both animal and plant products.. Dietary sources of iron are divided into two categories: sources of heme iron and sources of nonheme iron.
Heme iron is the form that exists in blood and is accordingly only found in animal products such as red meat, poultry and seafood.
Non heme iron is found in plant products, but also in animal products, making animal products a source of both heme and nonheme iron. Plant sources of nonheme iron include lentils, beans, chickpeas, tofu, cashews and chia seeds.
a fraction of dietary iron is available for use in the body. Iron bioavailability is approximately 14–18% for mixed diets and 5–12% for vegetarian di
Other dietary factors can also impact iron bioavailability. For instance, caffeine and calcium negatively impact iron absorption. Conversely, vitamin C competes with the negative effects of iron inhibitors, promong absorption.
Deficiency: Iron deficiency is one of the most common dietary deficiencies in the world. Its most serious outcome is iron-deficiency anemia. Iron-deficiency anemia occurs when there are not enough functional red blood cells due to low iron status, negatively impacting oxygen delivery to the tissues.
Milder cases occur when iron levels in the blood and bone marrow are low. This is known as mild iron deficiency.
Marginal iron deficiency occurs when blood levels as well as stores in the liver, muscle, spleen and bone marrow become depleted.
Iron-deficiency anemia is the final stage and negatively impacts the iron levels in hemoglobin and the production of healthy red blood cells. Earlier stages may show no symptoms, but symptoms can progress to lethargy, tiredness, weakness, hair loss and thinning, and pale-coloured skin. Severe levels, iron-deficiency anemia can lead to an irregular heartbeat and delayed growth in infants and children.
women lose blood due to menstruation, they are at a higher risk for iron-deficiency anemia, especially if they are consuming less iron due to a vegetarian diet or have higher iron needs.
Athletes are at a higher risk of iron deficiency as they lose iron through sweat and urine and have a higher degree of hemolysis – the breakdown of red blood
cells due to physical impact.
Pregnancy also increases the risk for iron-deficiency anemia, as iron requirements increase to support blood volume development in the fetus.
Toxicity: Iron can be very toxic at higher levels. Accordingly, the body controls iron intake by regulating its absorption in the digestive tract.
Hepcidin, the body’s iron-regulatory hormone, is responsible for keeping iron stores in balance. Its main function is to suppress the absorption of iron when levels are high.
Iron toxicity is typically due to genetic conditions or the overconsumption of iron supplements.
Supplemental iron of more than twice the RDA can promote faintness as well as gastrointestinal issues such as nausea, vomiting and constipation. Excessive iron supplementation can also reduce zinc absorption and bioavailability
consumption of 60 mg/kg of iron or more can lead to iron poisoning, which can cause organ failure, coma and death. Children are at highest risk for iron poisoning, as they may mistake their caregivers’ iron supplements for candies
Hemochromatosis has dysregulated iron absorption and high levels of internal iron.
Zinc
RDA: 11 mg (M), 8 mg (F); UL: 40 mg
Functions: Zinc is a ubiquitous mineral that acts as a cofactor for more than 100 different enzymes. gene expression, enzyme and immune function, protein and DNA synthesis, wound healing, and growth and development.
structure of the antioxidants superoxide dismutase and glutathione peroxidase. It is present in every cell of the body and is the second-most abundant trace mineral after iron.
Sources: abundant in the diet as it is found in a wide variety of foods (Figure 9.21). Good sources of zinc include shellfish, animal products, legumes, dairy products, whole
grains and certain vegetables like mushrooms, kale, peas, spinach and asparagus.
Absorption of zinc from plant sources is more difficult because plant compounds such as phytates can inhibit absorption. Many foods are also fortified with zinc,
Deficiency: Zinc deficiency is rare due to dietary insufficiency but may occur due to certain genetic mutations or in individuals with alcoholism who are malnourished. Vegetarians and vegans are also at higher risk, though this can be mitigated with a well-planned and varied diet. Mild zinc deficiency can promote slowed growth, erectile dysfunction, diarrhea, thinning hair and impaired immunity.
Toxicity: Zinc toxicity may occur due to excessive supplementa on but is rare from dietary sources. Symptoms include nausea and vomiting, a metallic taste in the mouth, loss of appetite, diarrhea, abdominal cramps and headaches. High dietary intake of zinc can also limit the absorption of copper and iron and promote their deficiency.
Manganese
Functions: is a cofactor for several enzymes in the body. It facilitates enzymatic reactions involved in carbohydrate, protein and lipid metabolism, bone development and wound healing. It is also part of the antioxidant superoxide dismutase.
Sources: Manganese is abundant in shellfish and plant products. Good sources include mussels, oysters, nuts, beans, chickpeas, whole wheat bread and leafy green vegetables. Foods that are higher in iron can slow its absorption.
Deficiency: Manganese deficiency rarely results from dietary insufficiency. Conditions such as epilepsy, osteoporosis and diabetes may increase risk.. Deficient individuals may experience poor growth, compromised fertility and abnormal carbohydrate and lipid metabolism.
Toxicity: no established side effects of excessive manganese intake from food. Toxic levels can result from excessive supplementa on, occupational inhalation or if tap water has excessively high manganese levels. Toxicity promotes neurological symptoms including tremors, muscle spasms, muscular weakness and hearing loss.
Copper
RDA: 900 mcg; UL: 10000 mcg
Functions: Copper plays a key role in red blood cell production, is involved in iron absorption and is a cofactor for many enzymatic reactions. Enzymes involved in energy metabolism, DNA synthesis and connective tissues synthesis all require copper. Part of the antioxidant superoxide dismutase. required for iron absorption.
Magnetic therapy bracelets, which often contain copper, have long been promoted as a wearable treatment for arthritic pain. However, their use is not fully supported by evidence.
Sources: Copper is found in a wide variety of animal and plant products. Beef liver, oysters, crab and salmon are all high in copper. Plant products, such as potatoes, mushrooms, cashew nuts and sunflower seeds, are also high in the mineral.
Deficiency: dietary copper intake has been decreasing since the 1930s. Approximately one in four Canadians are well below the RDA for copper. deficiency include tremors, tingling sensations, awkward walking patterns, numbness and fatigue. Digestive conditions, such as celiac disease as well as bariatric surgery, may increase risk for deficiency.
get enough iron but are lacking in copper may experience iron-deficiency anemia
Toxicity: toxicity is rare from food but can occur due to over-supplementation or due to certain genetic conditions.
can also occur due to a tainted water supply. Milder cases can result in vomiting, diarrhea, yellowing of skin and muscle pain. More serious cases can result in liver damage, heart failure, kidney failure and even death.
Wilson’s disease, a condition in which the liver is unable to remove excess copper, leading to its accumulation in the brain, liver and eyes.
Iodine
RDA: 150 mcg; UL: 1100 mcg
Functions: Iodine is an essential component of the two thyroid hormones: thyroxine (T4) and triiodothyronine (T3). These two hormones, secreted by the thyroid gland, have metabolic effects all over the body. They are involved in the regulation of fuel use, protein synthesis, heartbeat, body temperature regulation, muscle contraction and cell turnover.
Iodine is required for the synthesis of the thyroid hormones T4 and T3.
Sources: All table salt in Canada is iodized – that is, fortified with iodine. also found naturally in fish, dairy products and eggs, as well as plant products such as seaweed, nuts and enriched bread
Deficiency: Iodine deficiency compromises the thyroid gland’s ability to make thyroid
hormones. It is common in areas where food is scarcer and salt is not iodized. lead to hypothyroidism, which typically manifests as a goiter
goiter is an enlargement of the thyroid gland, which is located at the base of the neck. Iodine is needed to make thyroid hormones, but if iodine is insufficient, the thyroid gland enlarges as it tries harder to make these hormones. This condition is mostly reversible with iodine supplementation.
goiter is a physical sign of iodine deficiency,
Congenital iodine deficiency syndrome, previously known as cretinism, occurs when iodine is deficient in the prenatal or postnatal nutrition of a child. Pregnant women have a higher need for iodine; if it is lacking, several neurological issues can arise in the child.
Mental deficiencies, deaf mutism, difficulties with muscular control and slowed growth can result due to congenital iodine deficiency.
Toxicity: Iodine poisoning, which typically results from excessive supplementation, can promote diarrhea, nausea and vomiting. In severe cases it can lead to the swelling of airways, liming breathing, a lowered heart rate and even Coma. Also lead to iodine-induced hyperthyroidism, which can promote an accelerated heart rate, muscle weakness and unexplained weight loss.
cause goiters as the thyroid gland swells in an attempt to produce more thyroid hormones
Selenium
RDA: 55 mcg; UL: 400 mcg
functions: Selenium has roles in reproduction, the production and metabolism of the thyroid hormones, as well as in the synthesis of DNA. Its most known role, however, is as an essential component of the an oxidant glutathione peroxidase
no strong evidence base to support the use of selenium supplements ons in the prevention or management of CVD, but obtaining adequate amounts through the diet is recommended.
Sources: both plant and animal products. Fish, shellfish, eggs and chicken are high in
selenium, as are plants such as brazil nuts, sunflower seeds and shiitake mushrooms.
selenium in plant foods depends on the quality of the soil in which they were grown
Deifmecy: increases the risk of male infertility, muscle weakness, fatigue, hair loss and a weakened immune system.
selenium deficient and experience a secondary stress such as a viral infection, have
a higher risk for Keshan disease. Keshan disease is a potentially fatal disease of the heart muscle. It was first evidenced in the Keshan province of China, but has been found all over the country, as well as in other areas of the world where selenium content in the soil is low.
Toxicity: increase the risk of hair loss, nail discoloration, muscle and joint pain, headache and gastrointestinal symptoms. Early symptoms may include a metallic taste in the mouth and breath that smells like garlic.
selenium poisoning. This can promote neurological symptoms, breathing problems, kidney failure, heart attack and, though rare, even death.
Molybdenum
RDA: 45 mcg; UL: 2000 mcg
functions: Molybdenum is a cofactor in certain enzymatic reactions. Molybdenum enzymes help break down sulfites, which can promote allergic reactions, diarrhea, and breathing difficulties if they build up in the blood.
Molybdenum is a cofactor in the breakdown of sulfites.
Sources: The molybdenum content of plants varies depending on soil quality. Legumes are the best sources of molybdenum, while lentils are also rich in the mineral. Organ meats, such as liver and kidney, as well as dairy products are good animal sources of molybdenum.
Deficiency: Since molybdenum is abundant in a lot of foods and we only need a trace amount, deficiency is rare.
Toxicity: Molybdenum toxicity is rare and is typically due to over-supplementation. Excessive intake may affect growth, promote kidney failure or promote the development of seizures and brain damage. However, since deficiency is rare, not enough data has been collected to know the true symptoms of toxicity.
Fluoride
AI: 4 mg; (M), 3 mg (F) UL: 10 mg
Fluoride is an ion of the naturally occurring mineral fluorine. It is not typically deemed essential because it is not required for growth or to sustain life
functions: health-promoting effects through its well-established ability to strengthen bones and teeth. With calcium and phosphorus, fluoride forms a crystal structure called fluorapatite, which hardens tooth enamel. Fluoride therefore contributes to tooth integrity and health.
water fluoridation was effective at reducing tooth decay by 35%
Toxicity: fluorosis, which is most common in children under eight. Fluorosis negatively affects tooth enamel, promoting tooth discoloration. In rare cases it can lead to tooth damage
Chapter 10
11.2 - overview of energy balance
Energy is the ability to do work. Our bodies must perform a lot of work each day in order to survive and thrive.
The energy we obtain from the food we eat is our energy intake. We use this energy to fuel basal metabolism, physical activity and food processing.
This is collectively referred to as our energy expenditure. We achieve energy balance when
our energy intake equals our energy expenditure.
Carbohydrates, lipids and proteins are our three energy-yielding nutrients Cellular respiration breaks these bonds, releasing energy that can be captured in the bonds of ATP, the body’s energy currency
not a nutrient, alcohol also provides energy and contributes to our net energy intake
Recall that carbohydrates and proteins provide 4 kcal/g, whereas lipids provide 9 kcal/g and alcohol provides 7 kcal/g. However, the total number of calories consumed each day, not the source of the calories, determines our net energy intake.
Energy expenditure - We burn energy for three purposes: basal metabolic rate, physical activity and thermogenesis
Basal metabolic rate (BMR) is the amount of energy the body needs to perform its most basic, life-sustaining functions over a period of time. This energy helps us breath, pump blood and send nerve messages, among countless other critical functions.
accounts for 60–75% of the energy we burn. When we say someone has a fast metabolism,
we typically mean that they burn a lot of calories to sustain their body, even before physical activity is factored in
Compared to the other nutrients, more energy is required to process protein
On the other hand, some people are said to have a slow metabolism, meaning that they expend fewer calories on foundational life-sustaining processes. These individuals might have a harder time achieving and maintaining energy balance and may need to consume fewer calories or burn more to achieve energy balance.
determined by factors out of our control. Organ size also plays a large role in determining
BMR (Müller et al., 2011); the larger the organs, the higher the BMR
most significant determinant of BMR within our control is lean body mass
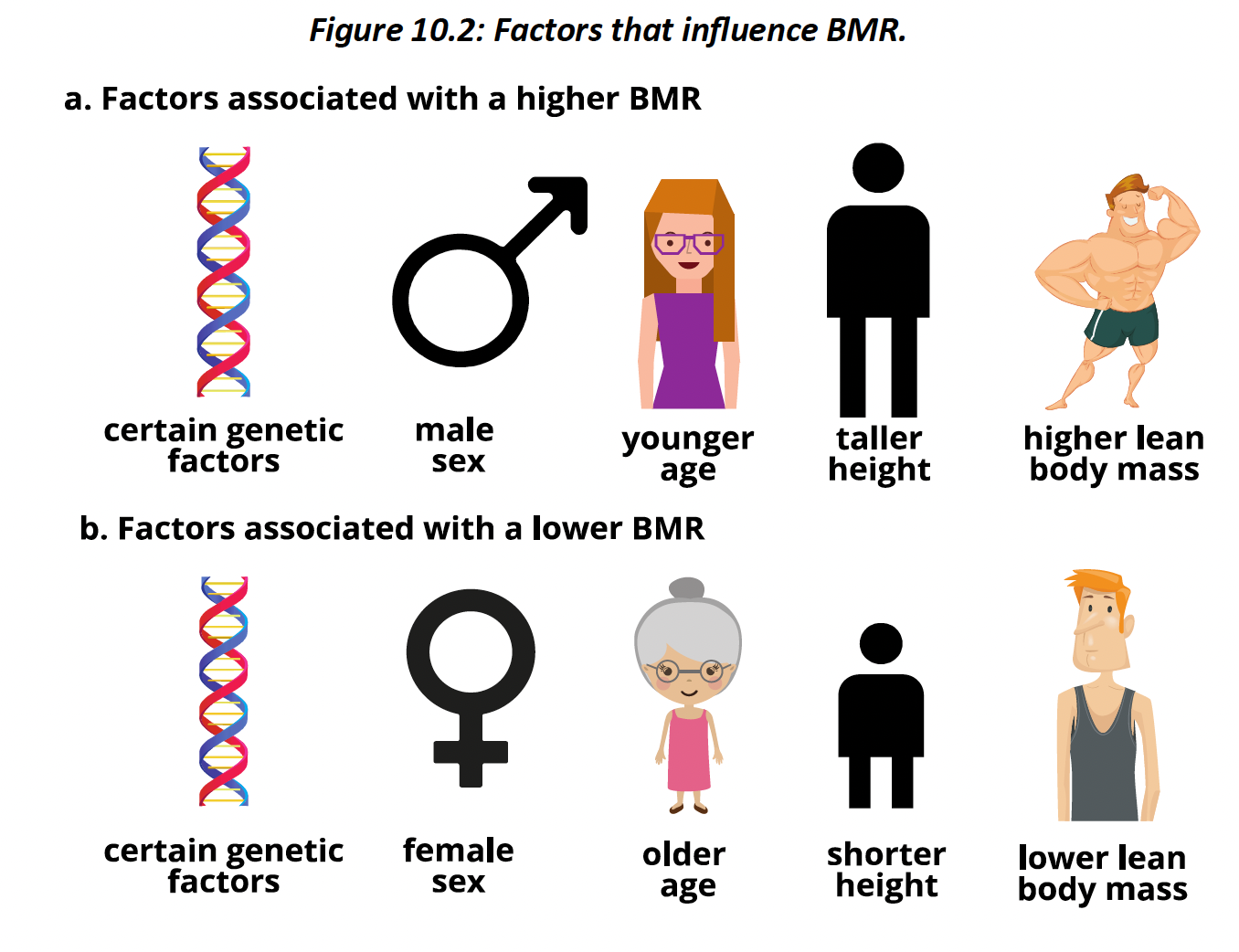
Diet-induced thermogenesis, also known as specific dynamic action or the thermic effect of food, also contributes to energy expenditure. It is the energy that is used and dissipated as heat following food intake. While food brings energy into the body, we also need energy to process it.
Diet-induced thermogenesis accounts for about 10% of energy expenditure.
diets high in protein promote a higher thermic effect, while those high in fat promote a lower thermic effect
diet-induced thermogenesis accounts for no more than 15% of our total energy expenditure.
The element of energy expenditure that is most under our control is physical activity. Physical activity is the body’s voluntary movement that leads to the expenditure of calories
Energy balance is achieved when the number of calories taken in from carbohydrates, lipids, protein and alcohol matches the energy we expend through BMR, diet-induced thermogenesis and physical activity.
consistent energy excess or energy deficit will lead to a gain or loss of energy, respectively. Since most of the body’s energy is stored as fat, and fat has weight, a consistent energy excess will lead to fat and weight gain, whereas a consistent energy deficit will lead to loss of fat and
weight.
some energy is stored as carbohydrate in the form of glycogen, most is stored as fat within adipocytes, or fat cells
Adipocytes are obvious under a microscope due to their empty-looking appearance. The part that looks empty is a vacuole and is where energy is stored. Adipocyte vacuoles contain triglycerides, fatty acids and fat-soluble vitamins.
lipids are stored in these vacuoles, adipocytes become larger. This increases body fat and weight. We are born with a certain number of adipocytes with a reserve of fat-storing potential. When adipocytes reach their maximum size, they can divide, increasing the total number of adipocytes. We can accordingly continue to add more and more energy to our bodies beyond our current capacity.
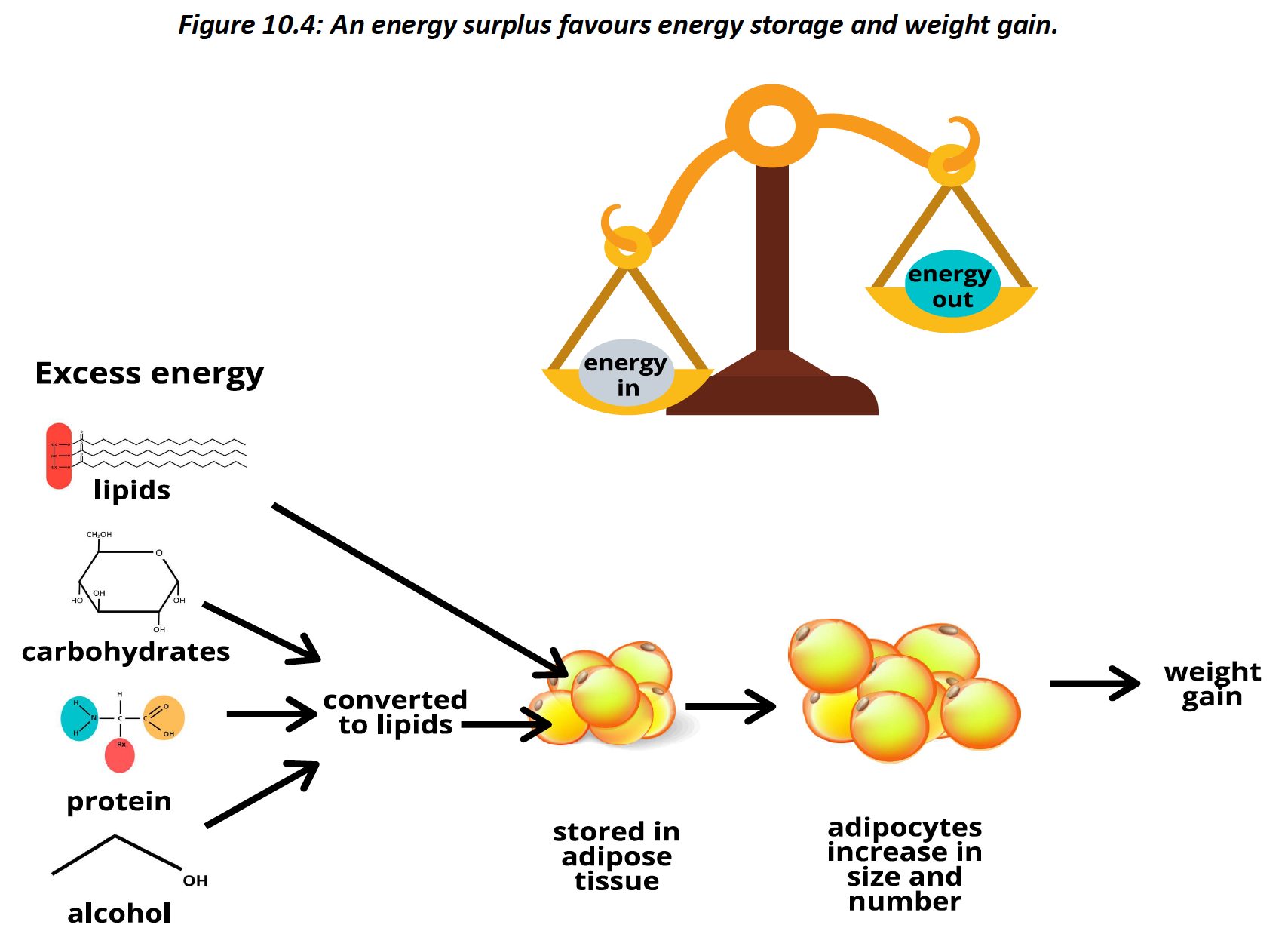
Energy deficit is reached when we consume less energy than our bodies need to perform its various func-ons. If the diet is inadequate to meet current energy requirements, it turns to its energy reserves.
Most energy retrieval comes from our adipocytes. Here, fatty acids and triglycerides are released and enter the blood. At the cells, these can then be metabolized to form ATP
consistently at an energy deficit, our adipocytes become smaller and smaller, leading to a loss of body fat and weight
Therefore, maintaining lean mass through physical activity is recommended while at an energy deficit.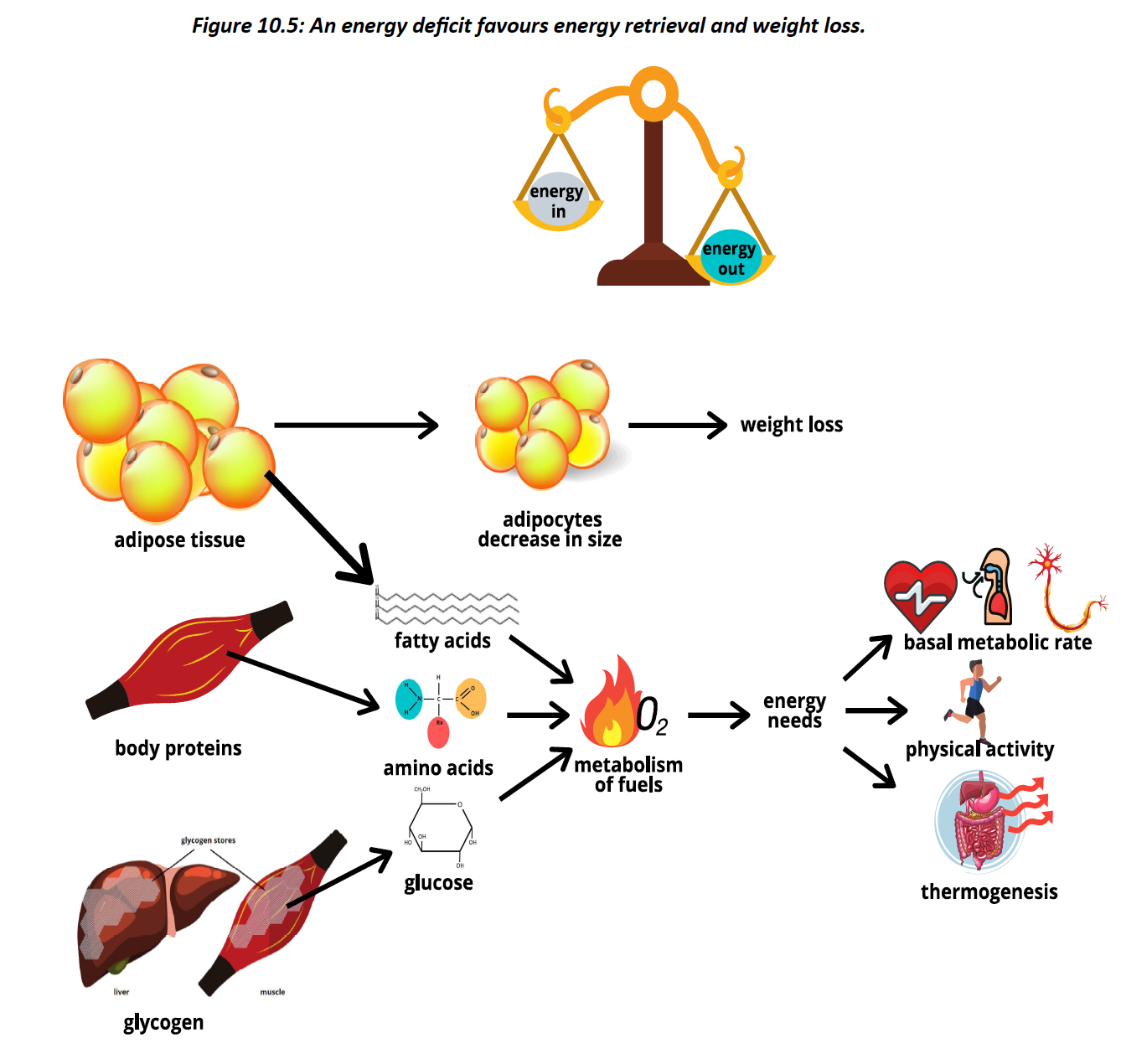
Weight is typically gained when lean mass or fat mass increase
Lean mass can be increased by increasing muscle and bone mass through resistance exercises
Fat mass is gained when we are at an energy surplus over a longer period of time
Some individuals may also notice a shifting in weight of a half or full kilogram in as little as
a day or two. This is rarely due to major changes in lean or fat mass. Minor daily weight fluctuations are typically due to changes in the body’s water content. The more cells an individual has, the greater room for water volume in the extracellular space.
Weight loss typically occurs when we lose lean mass or fat mass. Lean mass can decrease if our muscle or bone mass decrease, for instance if resistance exercises are discontinued.
Having enough lean body mass supports the structure and function of our bodies, while promoting health. Even if resistance activities are continued, we may still lose lean body mass when we are at a caloric deficit, as some body proteins will be broken down for energy
A major determinant of weight loss is the loss of energy stored as fat. This occurs at an energy deficit. Interestingly, most of this weight is lost in the air we breathe out. In addition to ATP, recall that the metabolism of fuels leads to the production of water and carbon dioxide
Every 10 kg of metabolized body fat, 1.6 kg are lost as water and 8.4 kg are lost as carbon dioxide, which is expelled from the lungs.
11.3 - Obesity
Leptin is secreted by adipocytes and communicates with the brain and other organs. It promotes fullness and energy expenditure and helps promote healthy energy balance
hundreds of adipokines – messengers released from our fat cells – have been identified. Each communicates with one or more tissues and helps maintain homeostasis.
Adipocytes communicate with the body by releasing adipokines.
Below a certain level of fat mass, adipokines produce a health-promoting effect on the body. Specifically, they tend to decrease the total amount of inflammation. However, above this threshold, adipokine secretion shifts towards a net negative effect on the body, increasing inflammation and the risk of disease
having too much of it can promote both physiological and structural consequences
researchers identified an obese mouse within a litter of otherwise lean mice.
Genetic analysis found that this mouse had a spontaneous mutation in a region they called the ob gene – ob for obese Jeff rey Friedman found that leptin is secreted by our adipocytes.
This was a major discovery because until then it was believed that our fat cells didn’t interact with the bod
Obesity is the state of having an excessive amount of fat stored in the body.Obesity meets the definition of disease because it takes years to develop and, once established, it compromises our anatomy and physiology and is often difficult to manage.
Individuals with obesity are more likely to have leptin resistance. Whereby their hypothalamus does not properly respond to this adipokine
These are outcomes associated with lifestyle factors that lead to a disease state. In 2015, the Canadian Medical Association recognized obesity as a chronic medical disease.
Obesity can affect the physical, mental and social wellbeing of an individual. Its physical effects are sometimes categorized into two categories: sick fat disease and fat mass disease
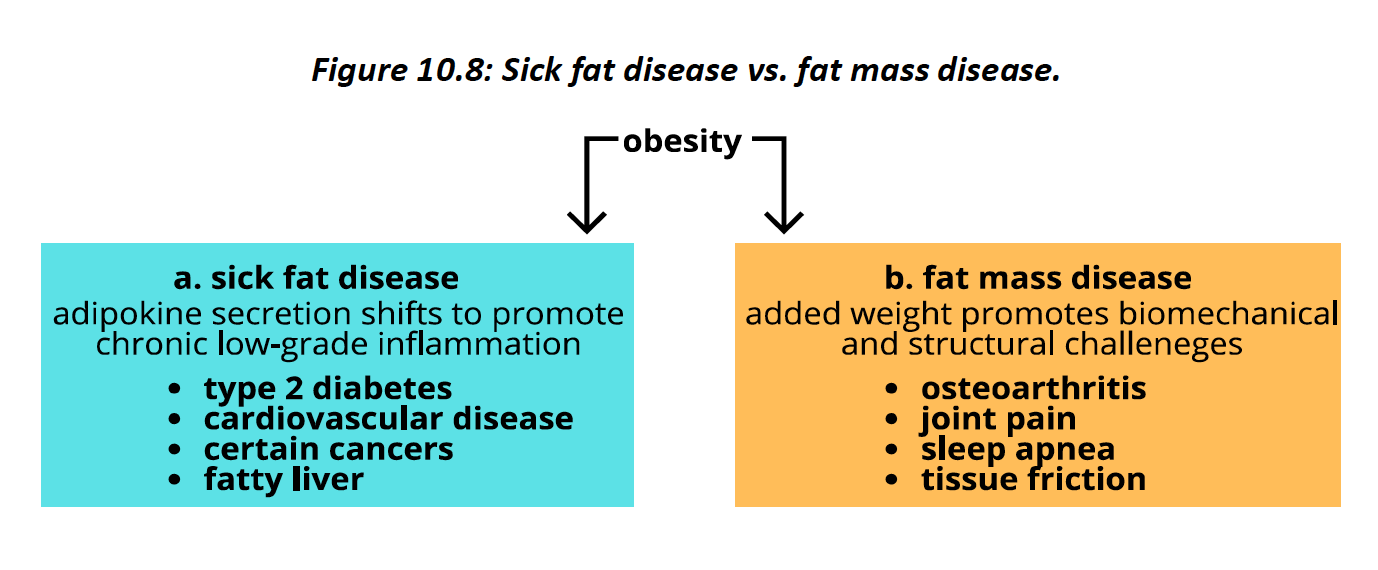
Sick fat disease refers to the negative physiological effects excess body fat can have once it passes a certain threshold. Past this point, fat cells interact with the body in a way that promotes chronic low-grade inflammation. This inflammation promotes several negative health effects.
Fat mass disease refers to the biomechanical and structural challenges that excess weight places on the body. In addition to the negative effects these can have on quality of life, they can also compromise obesity interventions. For example, added joint stress can make exercise painful for an individual with obesity.
increased risk for certain mental health effects, such as depression, low self-esteem and negative self talk. Furthermore, obesity is a common cause of discrimination in both adults and children.
The main take home message of the Foresight map of obesity is that the causes of obesity are complex and caused by many interrelated factors.
11.4 - determinants of body size
One of the key determinants of body size is genetics. Indeed, identical twins (same genes) have a much stronger correlation in body mass index (BMI) compared to fraternal twins
The genetic causes of obesity are typically polygenic, that is, caused by a combination of small effects in several different genes. A technique called genome-wide association studies has examined the genetic makeup of millions of individuals around the world and found approximately 100 sites in the human genome that promote an increased risk for obesity.
rates of obesity in First Nations people who live off reserve is 26%, while the rates in the Métis and Inuit samples they assessed were 22% and 26% respectively. These rates are significantly higher than the 16% rate of obesity evidenced in non-Indigenous people.
One potential reason is the higher rates of food insecurity. Food insecurity is the state where some or all members of a household have compromised access to food in sufficient quantity or quality, A potential outcome of severe undernutrition is height stunting, which may prioritize towards gains in fat mass over lean mass
appetite plays a key role in determining how much food we consume. Appetite is the drive to consume food.
It can be influenced by hunger, the physiological drive to consume. However, it is possible to have an appetite without being hungry – as anyone who has eaten past the point of fullness can attest to.
Satiety is the sense of fullness that promotes the cessation of eating and keeps us feeling full after a meal.
Our appetite and satiety centers are found beside each other in the brain’s hypothalamus.
The digestive tract, microbiome and fat cells tell our brain about our energy and nutrient status. These feedback cues are meant to keep our bodies in energy balance.
Individuals with obesity are more likely to have a higher amount of the gut bacteria that are able to extract more calories out of the food they eat
Other signals to the appetite center can override them. The brain’s limbic system, which is associated with emotions, reward and learning, as well as its prefrontal cortex, associated with our thoughts, also communicate with our appetite center.
Our appetite center receives various cues that influence appetite.
individuals with obesity are more likely to have genetic changes around their appetite-associated genes. This may affect the ability of these genes to properly interpret the signals the body sends, promoting higher food consumption
Large portion sizes, brightly coloured food packaging, constant advertising and cheap food are just some of the messages that our brains need to interpret. These signals compete with our internal appetite signals and often override them
the high energy availability and low demand for physical exertion in our surroundings is referred to as our obesogenic environment
Psychology can also have a significant effect on our energy status. Stress, mental health status and the way we think about ourselves and our bodies can affect both how much we eat and how much we exercise.
A major effect of our social psychology is the rush, rush, rush culture we live in – one that gives many a perceived lack of time. Our busy lifestyles prioritize other movies over cooking, grocery shopping and exercise.
The amount of physical activity we participate in is the main controllable factor that affects energy expenditure.
Both the natural and built environment can affect how much physical activity we engage in
Our built environment can also affect activity levels. This includes whether there are opportunities for being active that are free, safe and built into the existing infrastructure. Local, territorial, provincial and federal governments can influence the physical activity environment by improving transit opportunities, bike routes and hiking trails.
Physiology- we each have different BMRs, hormonal activity, genetics and various other biological factors that affect our energy balance. This partly explains the differences in fat and weight status between people who eat and move similarly
individuals with obesity are more likely to have a higher proportion of a phylum of bacteria called Firmicutes. Firmicutes are beer at harvesting energy from otherwise indigestible carbohydrates and metabolizing them into short-chain fatty acids, which contribute to our energy intake.
gut-brain axis – a communication system between the organisms in our digestive tract and the brain. We are all researching all the various ways this can affect health, including the ability of these organisms to affect appetite
Our adipocytes get larger due to more fat storage, leptin acts on the appetite center, promoting satiety and energy expenditure. This leads to a caloric deficit, which can help shrink these fat cells to their former size
Ghrelin is secreted by the stomach and has many targets around the body, including the hypothalamus. Ghrelin levels have been shown to spike before meals, promoting appetite (
over-secretion of ghrelin is implicated in the development and maintenance of obesity. Indeed,
levels of ghrelin often rise following weight loss, which may promote weight regain
Glucagon-like peptide 1 (GLP-1) is secreted by internal cells in response to food intake. It signals to the brain that the intestines have food in them, promoting satiety. Individuals with obesity may have impaired GLP-1 signaling, which can decrease satiety and promote higher energy consumption.
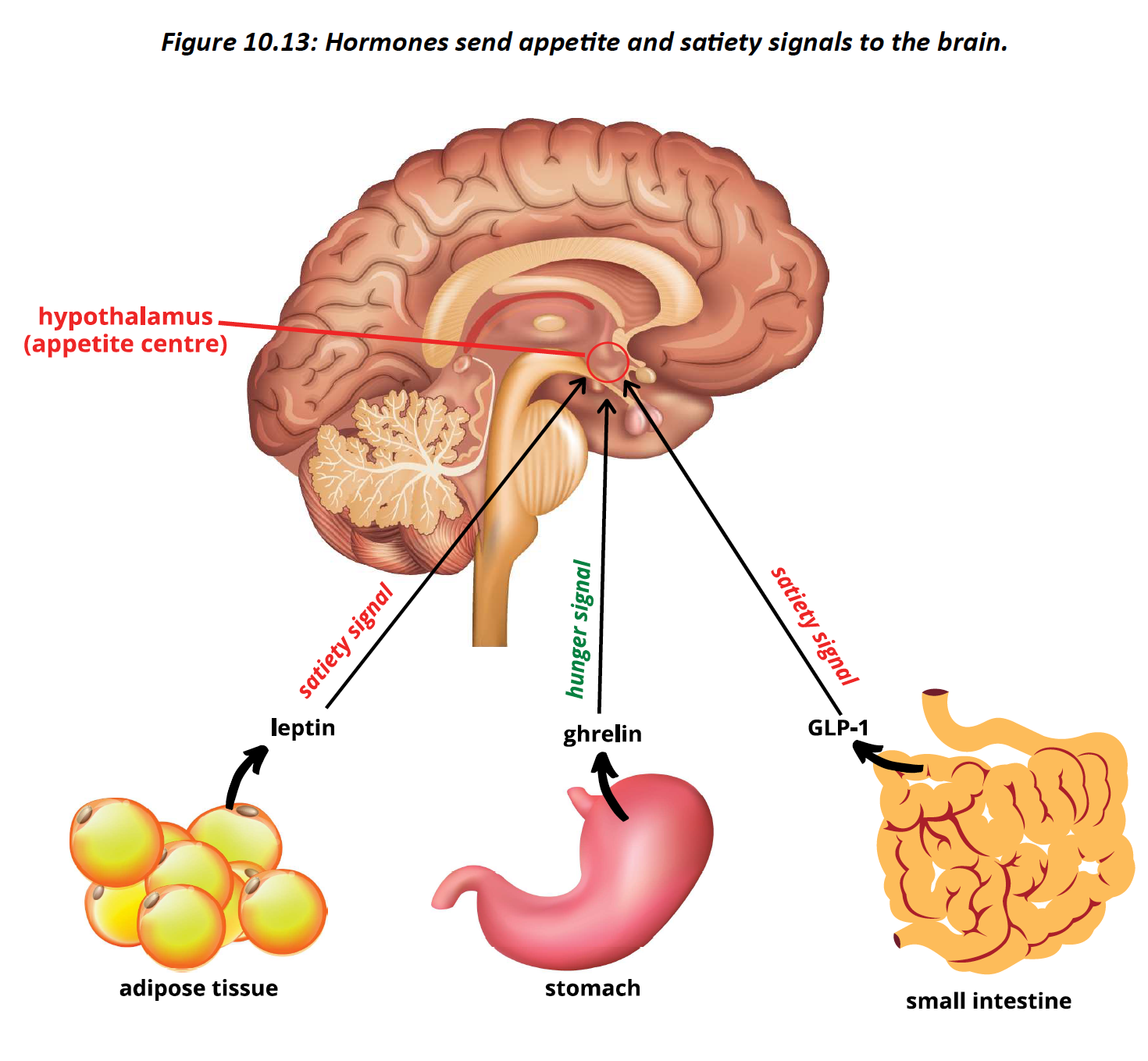
12.2 - body composition
Body composition is the proportion of fat mass versus lean mass in the body. A body that is higher in lean mass and lower in fat mass is associated with health.
Weight gives an indication of body composition, but doesn’t fully capture it. Weight can vary significantly with height, for instance. That is why BMI, which considers both weight and height, is often used instead of weight alone.
percent body fat is considered the gold standard for indicating how much fat a person has on their body. It expresses a person’s fat mass as a percentage of their entire body mass
The amount of fat a person has on their body affects health, as does where this fat is primarily located
Subcutaneous fat is located just below the skin, while visceral fat is located within the abdominal cavity, where many internal organs are found
Visceral fat is associated with higher risk of disease compared to subcutaneous fat
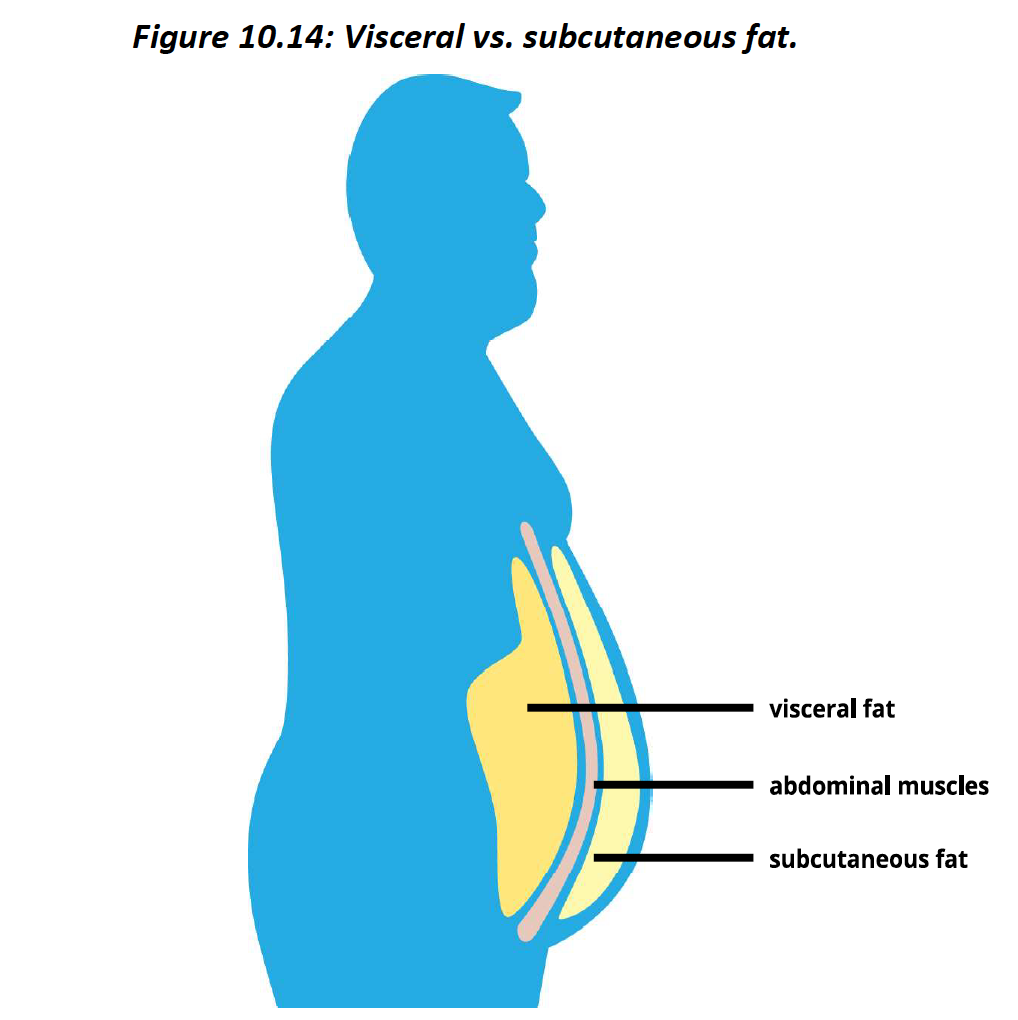
Dual X-ray absorptiometry (DEXA) is a low-dose x-ray that scans the body in two planes. An image of the body is produced that illustrates body composition. indicates bone density and muscle mass at various locations
can also discern between visceral and subcutaneous fat
DEXA is a non-invasive procedure as well as quick and easy for the technician and subject to perform. However, the DEXA machine is extremely costly and paying for a scan out of pocket can cost over 100 dollar
Body fat percentage can be estimated from body density. The body’s density is determined by dividing its mass by its volume. On earth, our mass is represented by our weight. However, the body’s volume is trickier to determine
We used to perform this water displacement technique to determine body fat percentage, but it is costly, time consuming and requires a person to submerge themselves under water.
A newer technique, commonly known as the Bod Pod, uses air displacement to measure body volume. A person places themselves in a small pod and the volume of air in the pod before they enter is compared with the volume after they entered.
It also requires the person to sit still and be in a confined space, which may make some people uncomfortable.
Skin fold analysis involves the use of calipers that pinch and measure folds of skin and the fat that lies underneath them. Using specific sites on the body, these measurements
are then put into an equation that is used to predict body fat percentage
Not performed properly, inaccurate results are obtained. Another limitation is that some people may feel uncomfortable
handheld devices estimate body fat percentage through bioelectrical impedance. This technique measures the rate at which electrical current passes through the body and determines its voltage. Voltage is calculated by multiplying current by resistance.
body fat produces greater resistance to current, the measured voltage can estimate
how much body fat a person has. fast, non-invasive and inexpensive to use.
accuracy is quite variable and can fluctuate significantly based on hydration levels. As much as a 5 kg decrease in fat-free mass is found in those who are dehydrated, leading to an overestimation of body fat percent
Individuals with a higher BMI are more likely to have an increased risk of health issues. Conversely, an underweight BMI may also be associated with health complications
Many countries have used BMI for decades, it is useful for comparing different populations over time. It is also a popular tool because it is easy to calculate from either measured or self-reported data.
a weak determinant of individual body composition compared to the other methods. A lean person could have a higher weight due to more muscle or bone mass, but that person might be incorrectly placed in the overweight or obese category.
BMI is that it does not differentiate between visceral and subcutaneous fat.
To help make BMI data more accurate, many newer studies of populations and individuals
often use waist circumference in addition to BMI. Waist circumference is measured a few cen meters above the hip bones with a measuring tape.
A waist circumference of more than 88 cm for women or 102 cm for men is considered high risk, especially if that person has an obese BM.
12.3 - weight management
There is a range of weights for which health is promoted and disease risk is minimized. However, when a high or low weight starts negatively affecting us, reaching a healthier size may be indicated
a person's best weight is, “…whatever weight they achieve while living the healthiest lifestyle they can truly enjoy. There comes a point when a person cannot simply eat less or exercise more and still like their life
Losing fat and weight boils down to one key concept: maintaining a consistent caloric deficit.
All diets work on that same principle
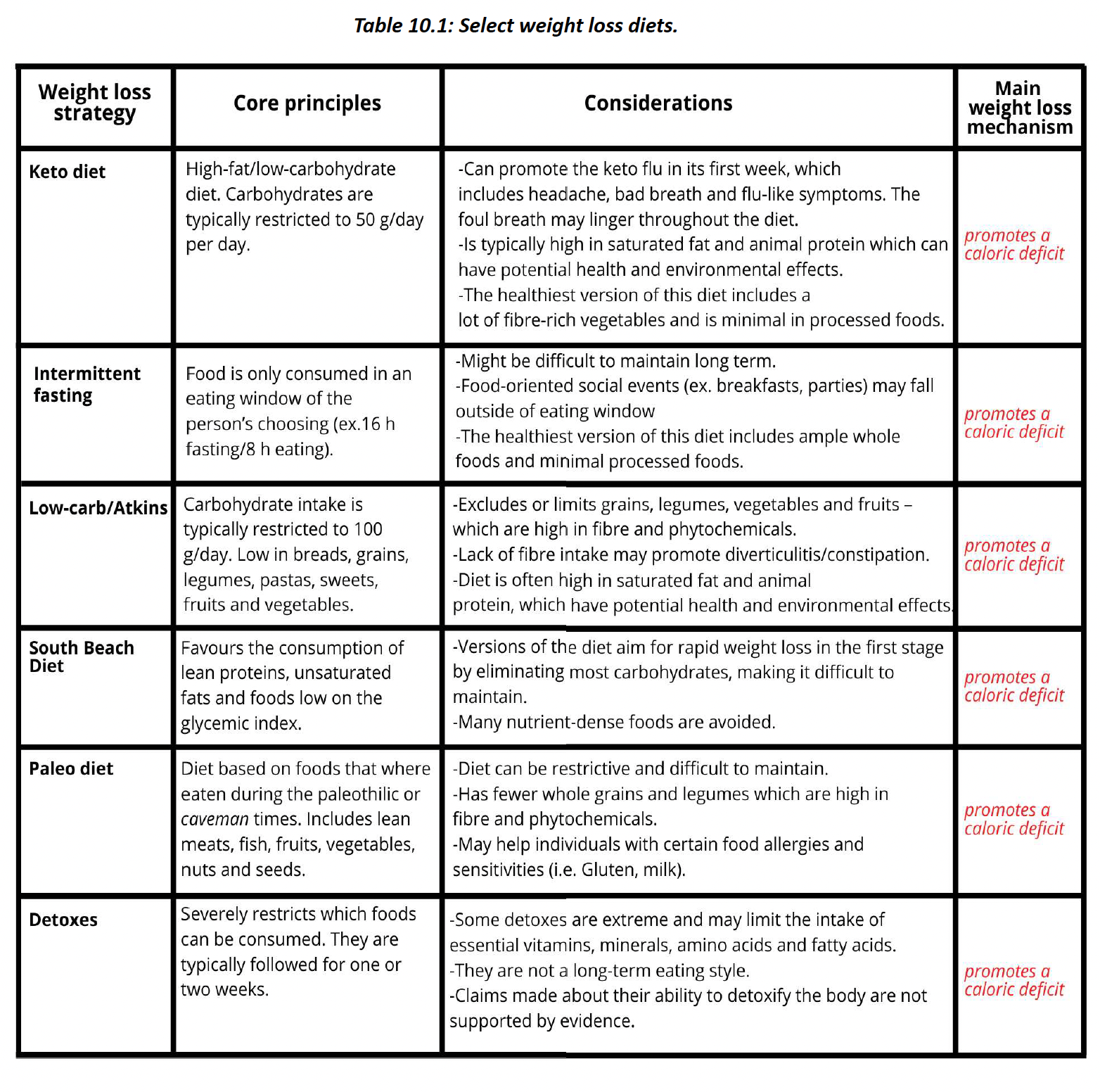
the National Weight Control Registry. This database collects information from individuals who have lost at least 30 pounds (13.6 kg) and kept it off for at least a year. It contains data from more than 10,000 people, 80% of which are women, mostly in their 40s.
achieving a caloric deficit is consuming less calories than we currently consume. A good place to start is to assess current intake levels, perhaps through a dietary analysis or through food journaling
A modest caloric deficit of 500–1000 kcal per day can lead to significant changes
in fat mass over time. more likely to be sustainable compared to more drastic caloric deficits
Tracking our daily intake can help provide accountability and a realistic goal to strive for. Furthermore, feedback is a powerful behavior-change tool
caution should be taken with respect to how food tracking affects mental health and quality of life. Some individuals find it demanding and guilt-promong
When portion sizes double, energy intake increases by 35% on average. While we cannot control the size of protons in restaurants, we can control how we respond to them. We can
split an entrée with a friend, package part of our meal for later or simply not finish what’s on our plate if we are full.
changes to the size of our portions at home by using smaller plates or putting less food on them. A small change can have a large impact.
Controlling our hunger may help us consume a more modest number of calories. We can decrease our hunger and appetite by eating in a way that promotes satiety. Protein-rich food and fibre-rich foods are well established to promote satiety
When we eat more slowly, we give the brain enough time to receive this message so we don’t overeat.
Willpower is our thinking brain’s ability to override other signals. For instance, we may really want to eat, but our thoughts could override this drive and stop us from eating. When it comes to moderang food intake, willpower can help, but it is not typically sufficient to sustainably change behavior.
use it too much, our willpower depletes and making healthy decisions may become more difficult
skillpower is recommended in addition to willpower. Skillpower means making the healthy decision, the obvious and easy one.
Energy expenditure that is most under our control is physical activity, and being physically active is one of the best things we can do for our overall health.
may also promote fat loss by increasing energy expenditure and BMR. This is typically more evident at higher intensities, longer durations and with exercise consistency over time.
Physical activity, especially resistance exercises, can also preserve lean body mass while at a caloric deficit.
evidence found that most long-term physical activity programs only promoted a weight loss
of approximately 2 kg on average
physical activity does not correlate with increased energy expenditure or weight loss. The body may adapt to long-term increases in activity by either moving less in other
areas, or by decreasing energy expenditure elsewhere.
Self-efficacy is our belief in our ability to achieve a certain task. If we do not believe we can eat less, move more or change body composition, that makes it more difficult to do.
Setting small, achievable goals, celebrating ourselves when we make a healthy choice and giving ourselves affirming thoughts may help improve self-efficacy with respect to weight-related behaviors.
individuals exhibit emotional eating to cope with the stressors in their lives. Finding positive coping mechanisms, such as talking to others, spending time in nature, journaling, crying or speaking to a counselor, may help to deal with the emotional triggers that promote overeating.
Mindfulness is the practice of being aware of and experiencing the present moment, including its thoughts, emotions and sensations with a judgment-free, curious approach
help us promote a healthy weight by regulating our emotions and improving our relationship with food, activity and our bodies
Mindful eating means being aware of what we are eating and thinking about each
bite. It may also mean an awareness of the various sensations our bodies experience while eating.
Fad diets are ones that are popular for a limited time. They often promise quick results, are endorsed by celebrities and influencers, and are not based on sound dietary recommendations.
Many fad diets are nutrient poor, which can compromise health. The other problem with many of these diets, is that they are so extreme that they cannot be maintained long-term, leading to weight regain. Many people who use fad diets get stuck on a never-ending fad diet cycle
lifestyle management alone may not be enough to improve physical and mental health.
Doctors might then be consulted for potential medical interventions.
Orlistat blocks the activity of the lipid-digesting enzyme lipase in the small intestine. Accordingly, lipids cannot be digested into free fatty acids and absorption is limited. This promotes weight loss as fewer total calories are absorbed from food.
fat-soluble vitamins are not readily absorbed and deficiency is more likely. Further, unabsorbed fat can pass into the large intestine, promong oily stools, fecal incontinence and gastrointestinal issues
Liraglutide (brand name = Saxenda) increases the activity of the signaling molecule GLP-1. Recall that the presence of food in the small intestine leads to the release of GLP-1, which acts on the hypothalamus to promote satiety.
The main limitation is that it is expensive and not covered by most extended medical plans. Also, it can promote nausea and vomiting, although this can typically be mitigated by altering the dose
Naltrexone/Bupropion (brand name = Contrave) It is a combination of two drugs that have historically been used to treat certain drug dependencies as well as depression. Together, these drugs reduce food cravings by altering the reward circuit in the brain that drives food-seeking
behavior.
expensive and not covered by most extended medical plans. Nausea is the most commonly
reported side effect, though some people also experience headache, constipation, dizziness, vomiting and dry mouth
Bariatric surgeries promote weight loss by altering the stomach. One of the main ways they promote weight loss is due to a smaller stomach size that can receive less food. This promotes satiety and a decrease in energy intake
Roux-en-y and sleeve gastrectomy typically produce the greatest amount of weight loss – typically between 50 and 70% of a person’s highest weight
lower body weight and struggle to gain weight. This is often due to physiological reasons such as a higher BMR or genetic factors that promote a lower appetite
If we want to increase lean mass, the best way to do so is with consistent resistance exercises that focus on building muscle, which in turn also build bone mass. they will need to consume more calories than they burn. If they are also exercising, this might mean that energy intake may have to increase dramatically
12.4 - eating disorders
Eating disorders (EDs) are not about food. The relationship with food is often indicative of another underlying cause.
Women, especially younger women, are far more likely to experience eating disorders than men. Socio-cultural factors, such as the pressure to be thin, are believed to contribute to this disparity. Perfectionism, obsessive tendencies and sensitivity to reward and punishment are also more common in individuals with EDs
People who have bulimia nervosa and binge eating disorder both experienced recurrent episodes of binge eating
Binge eating involves a loss of control, where the conscious regulation of eating is severely
compromised and a person cannot stop themselves from overconsuming. A binging episode is one that occurs in a specific amount of time
This binging typically occurs in the absence of hunger, at a fast rate, while the person is alone, and with feelings of guilt and shame
Bulimia nervosa affects 1.9% of women and 0.6% of men (Galmiche et al., 2019). It is evidenced by episodes of binge eating followed by compensation. This compensation is typically vomiting but may also include fasting, excessive exercising, or using laxatives or diuretics.
This behavior must occur at least once a week for three months. People who have other psychological disorders such as depression and who diet frequently are at higher risk for bulimia
mental effects, bulimia that includes vomiting has other potential complications. Stomach acid that is vomited can lead to stomach rupture, tears in the esophagus and gastroesophageal reflux.
One of the hallmarks of bulimia with vomiting is deteriora on of the teeth due to stomach acid.
lead to electrolyte imbalances, which can negatively impact the heart and other tissues
Binge eating disorder is the most common eating disorder, aff ec ng approximately 2.8% of women and 1% of men. Like bulimia, binge eating disorder involves episodes of binge eating. Unlike bulimia, there is no post-binge compensation
promote obesity and its related complications. However, binge eating disorder can also occur in individuals who are not obese. Binge eating disorder is more likely to occur in individuals who diet
Approximately 1.4% of women and 0.2% of men experience anorexia nervosa during their lives
involves a significant restriction in energy intake leading to a unhealthily low body weight. Individuals with anorexia typically have an intense fear of weight gain and spend a lot of effort to avoid it.
individuals with anorexia may exercise excessively or consume laxatives. There is also a binging/purging subcategory of anorexia, which involves episodes of binge eating followed by vomiting or excessive exercise
Anorexia is the psychiatric condition with the highest mortality rate
Nutrient deficiencies are common in anorexia, as are fatigue, hair loss, insomnia, dizziness and fainting
also develop amenorrhea – a cession in menstruation
In the purging type of anorexia, there is an increased risk of tooth decay, ulcers and electrolyte imbalances. Treatment is imperative for all forms of this disorder.
Night eating syndrome is found in the DSM-5 under Other Specified Feeding or Eating Disorders. It does not have diagnostic criteria
include an abnormal increase in food intake at night resulting in at least 25% of total calories being consumed after dinner. It could also include the person waking up in the middle of the night to eat.
features include a lack of appetite and food intake in the morning and/or insomnia at night.
Some who experience the condition might exhibit a belief that they need to eat in order to go to sleep or return to sleep
increases the risk for obesity. Those who are not overweight or obese might purposely delay their food intake throughout the day to eat more at nighttime.
Orthorexia nervosa is an obsession with eating healthy that has negative psychological implications. Individuals with orthorexia may severely restrict food intake for the sake of promoting health, though it may have the opposite effect.
might compulsively check nutrient facts boxes and ingredients lists and be preoccupied with the health of a food’s constituents. They may limit food intake to a narrow number of foods or food
groups and cut out others, including sugar, carbohydrates, dairy or animal products
may consume a less varied diet, they may also be at higher risk for micronutrient deficiencies. They may also experience higher levels of stress and their obsessive behavior may compromise their social, academic and work functions.
Treatment of EDs typically begins with proper diagnosis by a healthcare professional. This presents a challenge, however, as symptoms often go unrecognized. Bulimia
The most common psychological treatment is cognitive behavioral therapy (CBT). CBT is a type of talk therapy aimed at identifying thought patterns and behaviors that are unhelpful
Medication may also help certain individuals regulate their appetite and/or manage the other psychiatric conditions that might accompany an ED.
Chapter 11
13.2 - physical activity overview
Physical activity is an umbrella term for voluntary body movements that expend energy. There are several different forms of physical activity
Exercise is a type of physical activity that is planned and structured and whose goal is to enhance fitness.
Fitness is the body’s ability to respond to tasks that are physically demanding without being
exhausted. The more challenging an activity is, the more likely it is to build fitness
Sport is also planned, structured and can promote fitness, but has a competitive element and fitness may not be its main objective.
We may also participate in occupational activities to support the demands of our job or leisure activities.
Active living can further support fitness and overall health. Active living is a lifestyle that includes multiple opportunities for engagement in physical activity throughout the day. Cleaning the house, walking the dog, taking the stairs, dancing to our favorite song and gardening
Gardening is an excellent example of a practice that promotes both mental health and active living. Beyond its impact on physical activity levels, the direct interaction with natural environments that occurs during gardening may have further health benefits including reducing
the risk of depression and anxiety
The garden, much like other community gardens, shows how the various factors that affect health, such as physical activity, diet, mental health, community and relationships are interconnected.
For adults aged 18–64, the World Health Organization (WHO) recommends 150 min of moderate physical activity or 75 min of vigorous physical activity per week in intervals of 10 min or more. For further benefits, moderate-intensity activities can be increased to 300 min per week and vigorous activities to 150 min.
also recommends incorporating muscle-strengthening activities at least two times per week
13.3 - fuel use during physical activity
Energy intake provides fuel for our exercising muscles
Aerobic activities are moderate-intensity activities that can typically be performed for longer periods of time. They increase our heart and breathing rates, but not so much that the activity is unsustainable
Aerobic means with oxygen. Since these are moderate-intensity activities, after an initial adjustment the body can adequately deliver enough oxygen to meet the demands of aerobic metabolism.
Aerobic metabolism is the cellular respiration pathway discussed in Chapter 3 that leads to the production of more than 30 molecules of ATP. Carbohydrates, lipids and proteins can all be used for aerobic metabolism
anaerobic activities use anaerobic metabolism.
Anaerobic metabolism is the metabolic pathway that can occur without oxygen and that leads to the production of lactate and a small amount of ATP. Anaerobic metabolism is required in the first couple minutes of exercise as the body adjusts to adequately deliver oxygen to the tissues.
only dietary fuel that can be used for anaerobic metabolism is glucose
The body simultaneously uses multiple fuel sources. However, depending on the stage of exercise, one fuel will be used preferentially over others.
Aerobic zone - After exercise begins, it takes our bodies a couple of minutes to determine how much oxygen to send to which tissues. This stage is accordingly anaerobic, which limits the fuels that can be used
Anaerobic fuel use during the first two minutes of exercise:
0-2 seconds - Our muscle cells have a minimal amount of ready-to-go ATP that can be used for fuel when exercise begins. leads to the release of energy that can fuel muscle contraction. This ATP is used up within the first 2 seconds of exercise
3-10 seconds - Creatine phosphate, also known as phosphocreatine, can replenish ATP by transferring its high-energy phosphate group to ADP.
creatine system is the main energy pathway that fuels movies from the point
ATP is depleted to approximately the first 10 seconds of exercise. ATP and the creatine phosphate-ATP energy systems provide a quick, maximal burst of ATP before other long-term fuels are recruited
Creatine phosphate replenishes ATP.
11-120 seconds - body is in an anaerobic state for approximately the first 2 minutes of exercise. Anaerobic glycolysis, the anaerobic metabolism of glucose, takes up this role. This process is also known as the short-term energy system and the lactic acid system.
Pyruvate instead produces lactate (the conjugate base of lactic acid) and ATP. While this process produces much less ATP, it does so quickly and much faster than the aerobic fuel systems.
promotes an acidic environment that cannot be sustained. This is experienced as a burning sensation when spring or weightlifting. Due to the limits of anaerobic glycolysis, the body ships into aerobic metabolism as oxygen becomes sufficient.
After the first 2 minutes of moderate-intensity activity, the body is delivering an appropriate amount of oxygen to meet its energy demands.
two new fuel systems dominate: aerobic glycolysis and lipid metabolism.
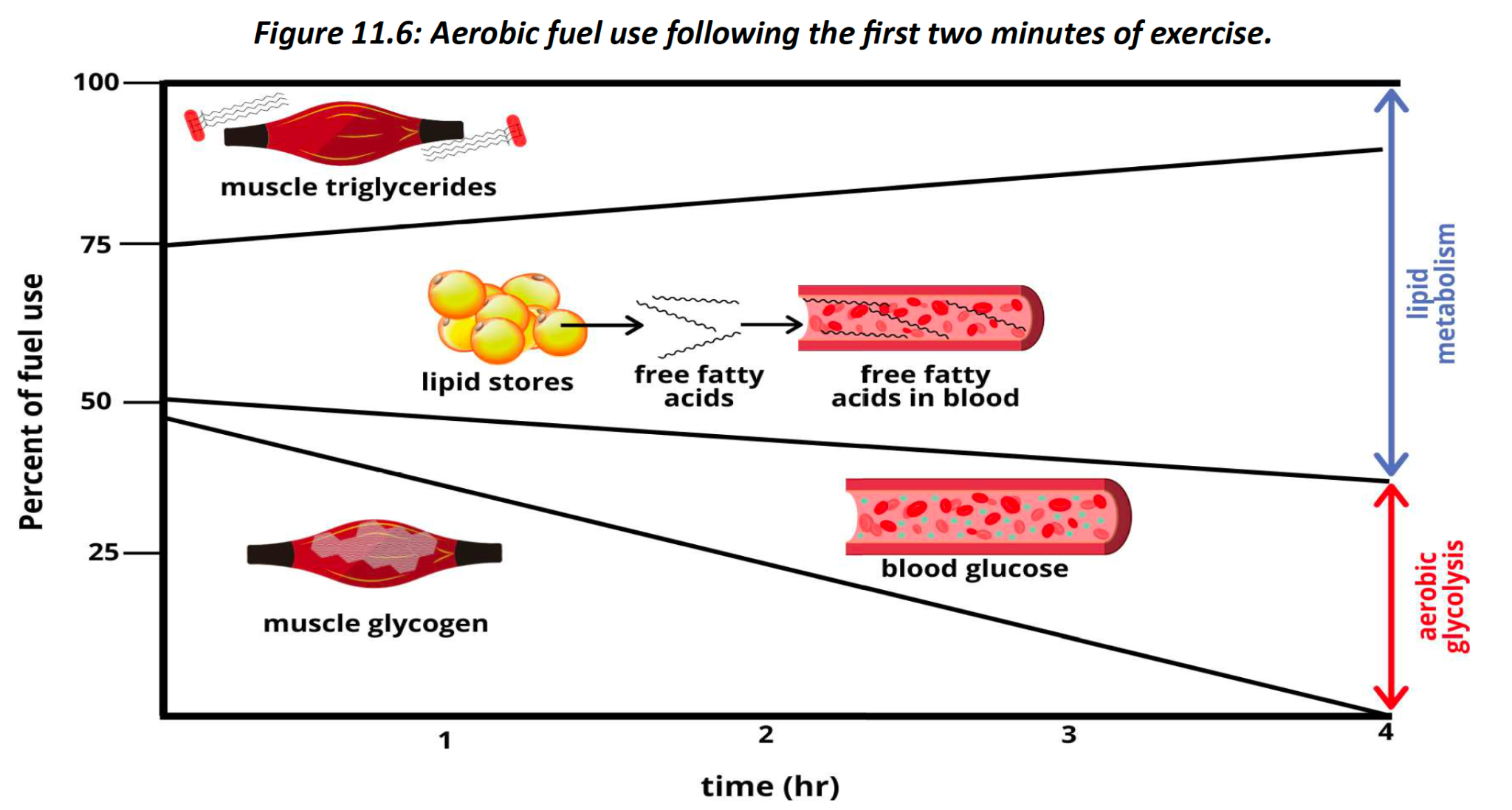
2 - 20 minutes - minutes 2–20 of moderate-intensity exercise, aerobic glycolysis is the dominant fuel source. Blood glucose and muscle glycogen supply this need for glucose. During this time, the body starts ramping up lipid metabolism, which will become the preferred fuel source after 20 minutes of exercise.
After 2o minutes - we start dipping into our main fuel source for extended activities: the aerobic metabolism of lipids. Some of these lipids come from our intramuscular fat – triglycerides stored within muscle.
most lipids used for lipid metabolism come from our fat cells, which release free fatty acids into
the blood. Since fatty acids are continuously supplied by our fat cells, we can continue to fuel exercise for an extended period
provides about 9 kcal of energy, compared to the 4 kcal of energy that is generated from carbohydrate and protein metabolism.
Protein can help fuel aerobic activities, but it is never the main fuel source. In general, protein only generates a maximum of 10% of the total energy needed for prolonged exercise
body would rather use an entire amino acid for the growth and repair of tissues than remove part of an amino acid and use it for fuel
Protein is an important part of an athlete’s diet for tissue recovery and growth, but not as a fuel source.
intensity of exercise can affect the preferred fuel source
Low- to moderate- intensity activities put us in the aerobic zone. That means that the preferred fuel source will depend on the duration of the activity, as discussed above. For moderate activities lasting longer than 20 minutes, lipids are the preferred fuel
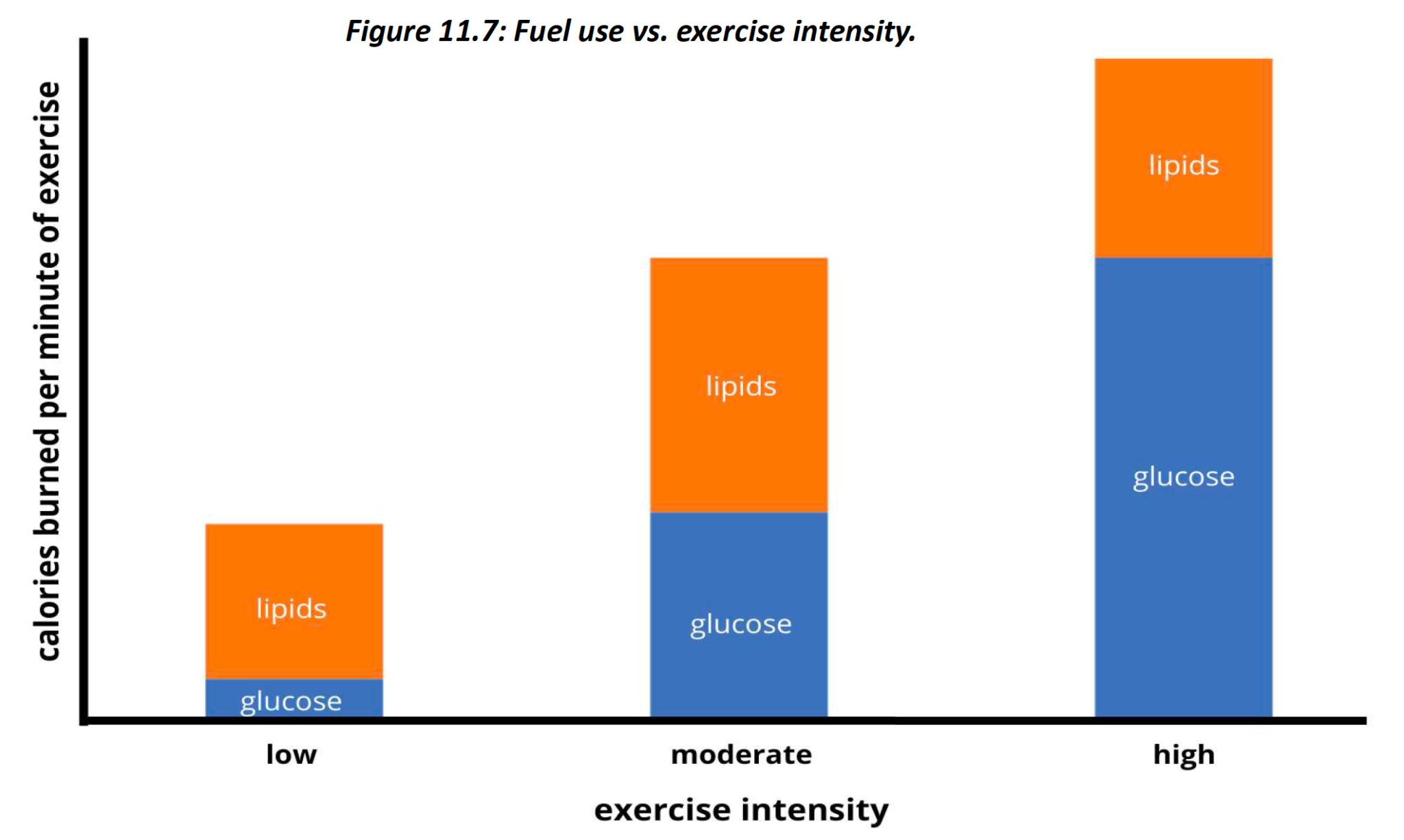
High-intensity activities, such as spring, weight lifting and plyometrics, are considered anaerobic activities. While aerobic metabolism still occurs during these activities, anaerobic glycolysis is the main energy source.
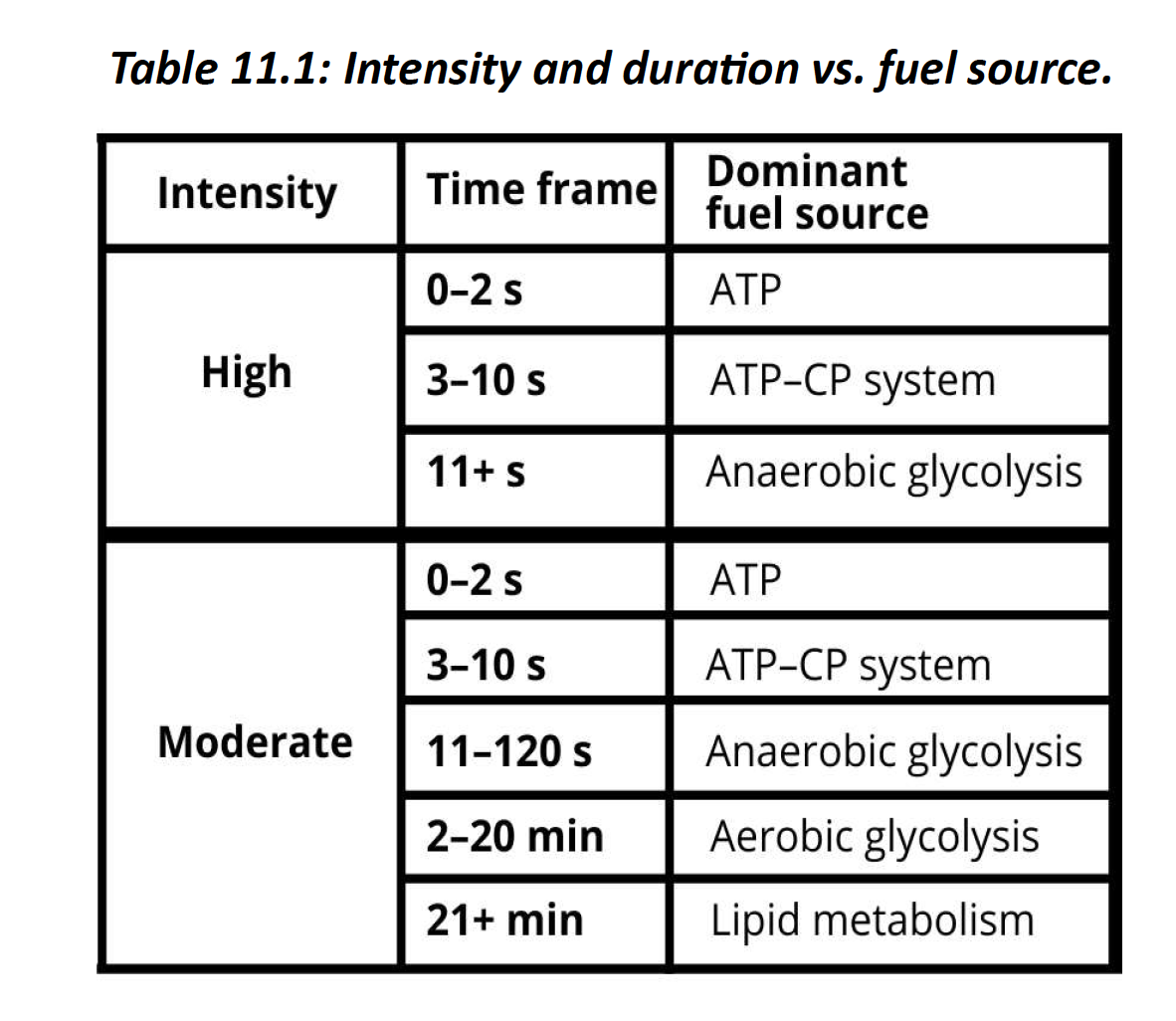
On treadmills,The fat-burning/weight-loss zone is a moderate-intensity zone in which lipid metabolism is the preferred fuel source. However, this does not mean that we will burn more body fat in this zone.
Energy availability is calculated by subtracting energy expenditure from energy intake - it considers how much energy is remaining following exercise.
Consuming adequate carbohydrates can maximize glycogen stores.
13.4 - nutritional considerations for athletes 
Sufficient energy intake is required to fuel activities. However, when planning for energy intake, we might also need to consider an athlete’s preferred energy balance
a good place to begin is for an athlete to determine how much energy they burn each day using the estimated energy requirement (EER) calculator
If a person is trying to gain weight, they should consume energy in excess of their EER. If they are trying to lose weight, they should consume energy at a deficit to their EER.
maintain weight, their energy intake should closely match their EER. While BEER is helpful for estimating energy requirements
Another method that can be used to explore the energy needs of athletes is the concept of energy availability (EA). EA is calculated by subtracting our exercise expenditure from our energy intake.
if a person ate 2000 kcal in a day and burned 500 kcal through exercise, their EA would be 1500 kcal. This concept is important because it considers how much energy is left over to meet our other needs once we take exercise into account
Carbohydrates are a key fuel for both aerobic and anaerobic exercise. Recall that muscles use glucose for both types of activity, but a limited amount is available.
Consuming adequate carbohydrates can maximize glycogen stores and contribute to exercise performance. Indeed, glucose provides a higher yield of ATP over other fuels per volume of oxygen.
the brain and red blood cells, both of which are important for performance, rely on glucose as a fuel
Meeting carbohydrate recommendations for different levels of activities can help athletes replenish and maximize their glycogen stores, which many athletes fail to do.
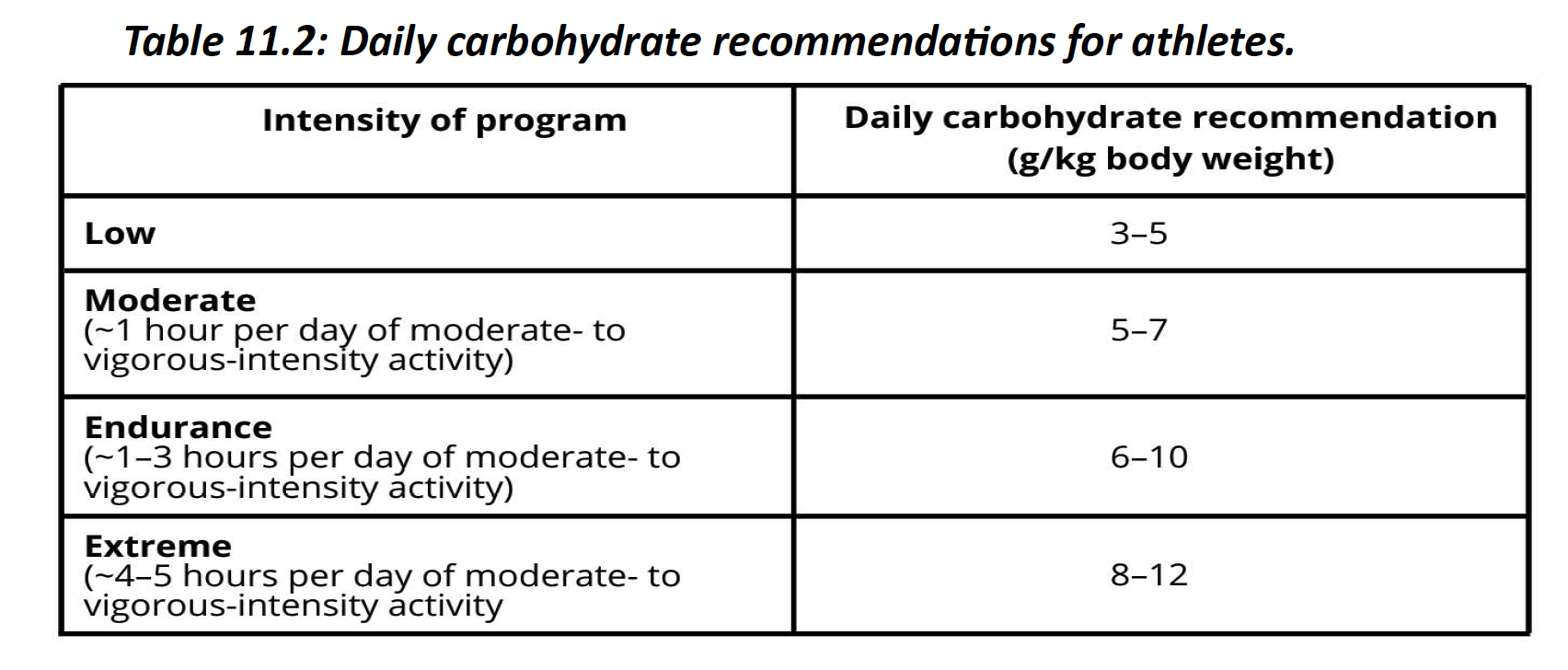
Protein is essential for the growth and repair of tissue, including the synthesis of muscle. In the 24 hours following resistance exercise, muscle protein synthesis increases, which is coupled with an increased need for dietary protein
athletes require sufficient dietary protein to facilitate the repair and growth of these and other body proteins
Protein recommendations increase from an RDA of 0.8 g/kg/day up to a range of 1.2–2.0 g/kg/day for athletes. depends on training duration and intensity.
lipids are the primary fuel source for activities lasting more than 20 minutes, the body stores lipids and extra dietary consumption is not typically recommended for an athlete, especially if it displaces carbohydrates in the diet
fat restriction below the lower end of the acceptable macronutrient range for fat (20% of calories) is also not recommended, as it can impair the bioavailability of fat-soluble vitamins and essential fatty acids
Vitamins and minerals regulate many physiological processes that are critical for exercise. Accordingly, micronutrient deficiencies can compromise athletic performance and recovery.
vitamin D both contribute to bone health. Exercise, especially resistance exercise, promotes the mineralization of bones, which requires an adequate supply of these micronutrients. to support bone health, athletes should ensure adequate intake of both calcium and vitamin D
important for those with lower EA who may be lacking in these and other micronutrients
vitamin D has emerged as a potential mediator of muscle health
Iron is an essential component of the two proteins hemoglobin and myoglobin, which help transport oxygen in blood and muscle, respectively. Iron deficiency compromises oxygen delivery and can progress to iron deficiency anemia, promotes tiredness and decreased exercise capacity.
iron deficiency can compromise muscle function and athletic ability
higher risk for iron deficiency, especially if their heme iron intake is low. Accordingly, it is imperative that athletes achieve adequate iron status to support performance and health
Iron from animal products is more bioavailable than non heme iron found in plant products. Animal products are also advantageous because they do not contain phytates, oxalates or tannins, which can compromise iron absorption in plants.
Consuming iron sources with vitamin C can improve iron absorption. Iron supplements may also be used, but they are recommended as a second course of action due, in part, to their ability to promote gastrointestinal distress
Exercise increases the production of free radicals. Free radicals can oxidize and damage muscles and impair their function
An oxidant activity can mitigate this damage. However, athletes may have lower total antioxidant capacity.
Foods rich in vitamins E, C, provitamin A, selenium, zinc, sulfur, magnesium and the
B vitamins can help increase an athlete’s total antioxidant capacity.
13.5 - nutritional considerations for before, during and after exercise
The timing of nutrient intake is an important determinant of exercise performance and recovery.
for those who exercise for longer, a pre-exercise meal that contains carbohydrates is
the best established way to promote exercise performance recommend consuming 1–4 g/kg body weight of carbohydrate 1–4 hours before exercising for more than 60 minutes
These maximize performance while lowering the potential for digestive stress. For those competing in longer events, glycogen supercompensation may be indicated.
common for marathoners and those participating in endurance competitions to load up on pasta or pancakes the night before their big event. This is glycogen supercompensation, commonly known as carbo-loading.
maximize glycogen stores to promote optimal carbohydrate fuel use during endurance events. Indeed, this strategy has been shown to increase the time to exhaustion as well as overall performance.
10–12 g/kg body weight of carbohydrate is recommended per day for the two days preceding the activity.
To reduce the risk of dehydration, sufficient water intake is also recommended before exercise. Individual water needs vary according to physiology and the environmental temperature.
5–7 mL/kg body weight of water at least 4 hours prior to exercise can help prevent dehydration in most individuals.
we lose water through sweat and exhalation, and we must rehydrate to maintain water balance. Regardless of duration, water intake during activity is recommended to prevent dehydration, which can negatively affect both performance and health.
weigh ourselves before and after exercise to determine our level of dehydration. Every kilogram of weight lost is equal to a liter of water lost.
If athletes only replace water and not electrolytes, they are at higher risk for hyponatremia and other electrolyte imbalances
For longer activities, especially those in a hotter environment, both fluid and electrolyte replacement is imperative. Since sweating rates vary dramatically, so will water and electrolyte needs. Consuming 375–500 mL of water every 10–15 minutes will typically be enough to reduce dehydration
who exercise for a moderate amount of time (e.g., 30–60 minutes) or at a lower intensity do not usually require extra fuel during exercise
Eating during exercise can promote gastrointestinal side effects such as indigestion.
However, for endurance activities lasting more than 60 minutes, including stop and start events like soccer, 30–60 g/hour of easily digested carbohydrate is recommended
Following exercise, we have three nutritional priorities: promoting the growth and repair of muscles, replenishing lost fluids and electrolytes, and refilling glycogen stores
24 hours following an exercise session, muscle protein synthesis increases, as does our sensitivity to dietary protein. In the first two hours following exercise, consuming high-quality protein sources maximizes muscle protein synthesis
Milk-based protein is often recommended as a high-quality protein source following exercise. It is easily digested, contains water, electrolytes and carbohydrates and is especially high in the branched-chain amino acid leucine.
branched chain amino acids improve aerobic capacity, they may be useful for muscle recovery, not performance
Caffeine is most effective as an ergogenic aid when it consumed in a form that does not include water
30–40 minutes following exercise, both glucose transport into muscle cells and glycogen synthesis increase. Consuming a post-exercise meal that includes whole sources of carbohydrate can help promote this glycogen synthesis.
Sources with a high glycemic index can be included to maximize glycogen recovery.
If a meal that contains whole foods is consumed following exercise, it will most likely replace electrolyte loss. To replenish fluids, any post-exercise drop in body weight should be addressed by consuming the appropriate amount of water lost.
13.2 - ergogenic aids
Athletes, especially those competing in elite sports, are more likely to use ergogenic aids, which are commonly known as performance enhancers
products are taken in order to improve output, muscular gains and/or recovery. While some ergogenic aids may be beneficial to an athlete, a discussion with a sports nutritionist or dietician should precede consumption so the potential for negative side effects is minimized
Creatine supplements are one of the most popular nutritional supplements for athletes. They help maximize muscle creatine stores, which are not typically saturated.
shown to boost the levels of creatine within muscles, thus providing more fuel for anaerobic activities. Creane supplement may promote performance in high-intensity activities, especially those performed in short intervals
recommends a supplementation protocol of 5 g of creatine monophosphate four times per day for five to seven days to fill creatine stores. Following this, 3–5 g
of creatine monophosphate a day can be continuously taken to maintain store
The most common side effect of creatine use is weight gain due to water retention. Muscle cramps and gastrointestinal symptoms, such as diarrhea and abdominal discomfort may also occur,
Protein supplements are consumed as protein powders or as individual or grouped amino acid supplements. They are mainly taken to enhance recovery and promote muscle growth and repair
adequate protein intake can easily be achieved through diet alone. However, commercial protein supplements are typically easy to consume and are open mixed with other nutrients that may be lacking in an athlete’s diet.
branched-chain amino acids leucine, isoleucine and valine are sometimes taken for their ergogenic potential. Indeed, they have been shown to reduce low to moderate amounts of
muscle damage in resistance athletes.
shown to improve muscle protein synthesis as well as reduce soreness after more demanding bouts of exercise
We can purchase branched-chain amino acids at supplement stores, or we can simply consume a diet that contains high-quality protein to meet our needs
Caffeine is not a nutrient; it is a psychoactive drug. For decades, it has been used within sport for its mild stimulating effects
caffeine improves exercise performance in a number of ways. Muscular strength and endurance, aerobic endurance and anaerobic power all improve with caffeine intake. Benefits are more significant with aerobic activities as compared to anaerobic ones.
caffeine has an enhancing effect when consumed in doses of 3–6 mg/kg. They further assert that caff eine’s ergogenic effect is most pronounced when consumed
in a state that does not include water
Hydroxymethylbutyrate (HMB) is a compound produced by the breakdown of the essential amino acid leucine. It has been shown to decrease protein breakdown while increasing protein synthesis
potential effects on athletic performance, muscular growth and recovery, lean body mass, strength, power and aerobic performance
HMB may improve recovery by decreasing muscular damage. Further, they deemed this supplement as safe for use at a range of ages.
An athlete suffering from a vitamin or mineral deficiency may see a significant improvement in their performance when vitamin and mineral intakes are increased to adequate levels. This can be done through a well-planned and varied diet. However, little to no change will be seen in athletes who over consume vitamin and mineral supplements beyond adequacy levels
Anabolic steroids, also known as anabolic-androgenic steroids, are synthetic compounds similar to the male hormone testosterone. They are taken by some athletes to increase muscle mass, strength and performance, but are not recommended
Steroids promote a wide range of negative side effects, including severe acne, increased risk of tendon issues and aggressive behaviors. There are also cardiovascular risks such as increased LDL, decreased HDL and increased blood pressure. They are also associated with psychiatric symptoms such as mood and schizophrenia-related disorders.
they can promote fertility consequences, such as shrinking testes and decreased testosterone
levels, which can last for months
cannabis is legal in Canada, there is an increased focus on its effects on a range of outcomes, including athletic performance. However, there are very few studies that examine these potential effects
no significant improvement in athletic performance with cannabis use
negative side effects such as chest pain and a reduction in strength. More research is needed to establish the relationship between cannabis and athletic performance
Nutrition needs will vary depending on the individual and the specific activity being performed. People who exercise at lower frequencies, intensities and durations may not need to significantly alter their nutrition
Athletes have higher requirements for energy, carbohydrate, protein, antioxidants, fluids and micronutrients. Also, the timing of their consumption can provide an added benefit to performance and recovery.