Orbital Nerves: Cranial Nerves II, III, IV and VI
Learning Objectives
Understand the visual field and the different components of CN II
Isolate the cranial nerves that innervate the skeletal and smooth muscles of the orbit
Apply this information in a clinical context
Review
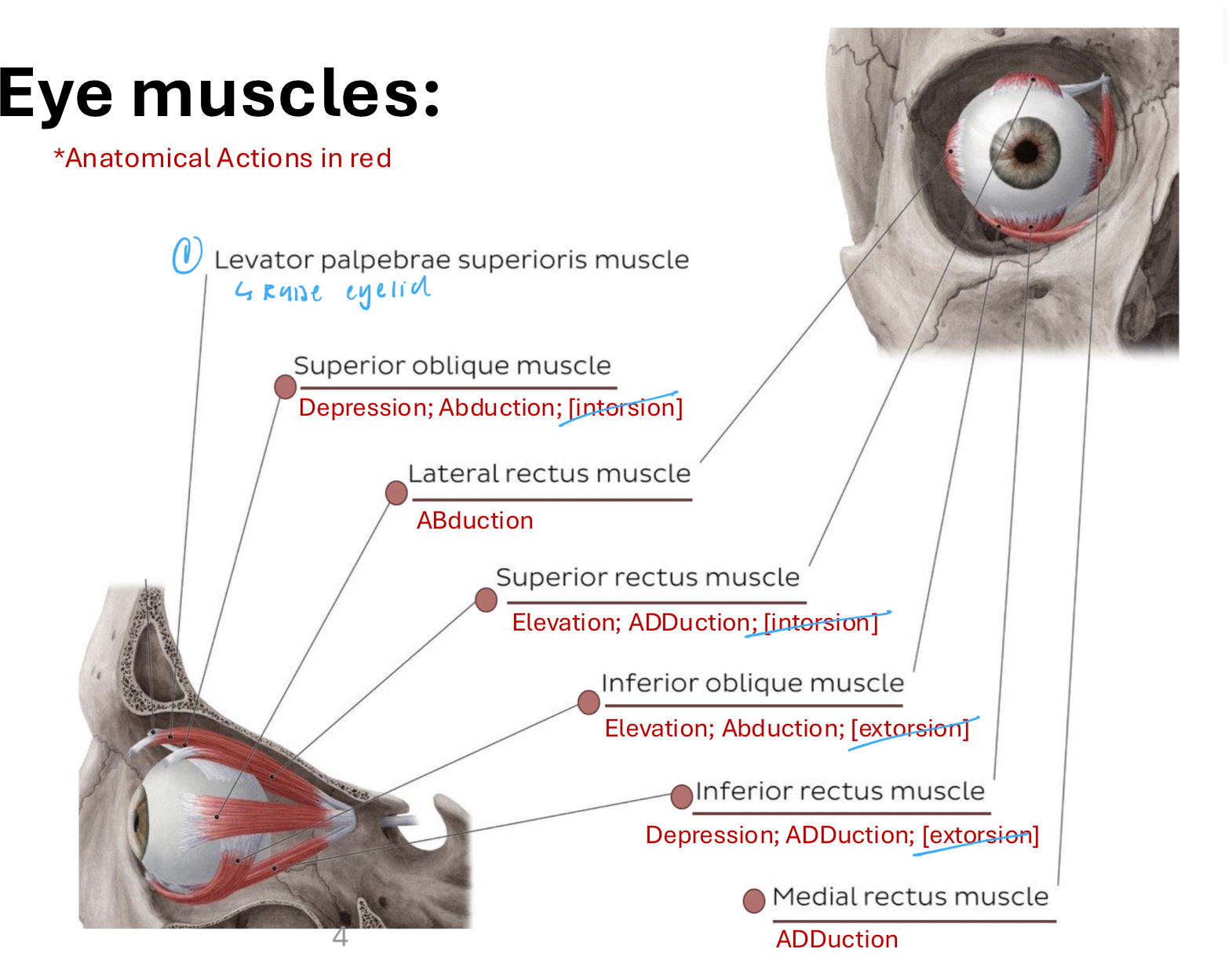
Eye muscles
Extrinsic muscles: Extraocular muscles
Involved in movement of the eyeball or raising the upper eyelid
Levator palpebrae superioris m.: Raise eyelid
Superior oblique m.: Depression; ABduction
Lateral rectus m.: ABduction
Superior rectus m.: Elevation; ADduction
Inferior oblique m.: Elevation: ABduction
Inferior rectus m.: Depression; ADduction
Medial rectus m.: ADduction
All muscles with “rectus” originate from the common tendinous ring
Intrinsic muscles: Muscles within the eyeball
Control lens shape and pupil size
Orbital Nerves
CN | Name | Fiber | Function/Innervation |
CN II | Optic n. | SSA (Special sensory afferent) | Special sense of vision |
CN III | Oculomotor n. | Somatomotor (GSE) and Parasympathetic (GVE) | GSE: Levator palpebrae superioris; Superior rectus; Inferior rectus; Medial rectus; Inferior oblique GVE: Sphincter pupillae; Ciliary m. |
CN IV | Trochlear n. | Somatomotor (GSE) | Superior oblique |
CN V1 | Ophthalmic division of CN V | Somatosensory (GSA) | Skin around the ey; eyelid; lacrimal gland (sensory only); conjunctiva |
CN VI | Abducent n. | Somatomotor GSE | Lateral rectus |
N. that run along the lateral wall of cavernous sinus (inferior → superior): Ophthalmic n (V1), Trochlear n. (IV), oculomotor n. (III)
N. that travel through cavernous sinus: Abducens n. (VI)
CN II - Optic n.
SSA: Special sense of sight
Function: transmits info from the world → brain about brightness color, and contrast (visual acuity)
Pathway: Originate from retina and move distally into brain proper
Retina → L and R optic n. → Optic canal → R and L optic n. join at optic chiasm (in chiasnatic groove) → Optic tract → Midbrain (synapse) → Visual cortex (in occipital lobe)
Covered by pia, arachnoid, and dura mater
Central retinal a. (from opthalmic ← branch of ICA) pops through dura and follows optic nerve to pierce the back of the eye
Optic n. technically a myelinated tract from the CNS (not a true CN)
Limited regeneration → Damage results in blindness
Permanent regeneration
Reflexes (response to light)
Pupillary light reflex: Change how much light enters eye
Accommodation reflex: Changes focus with distance
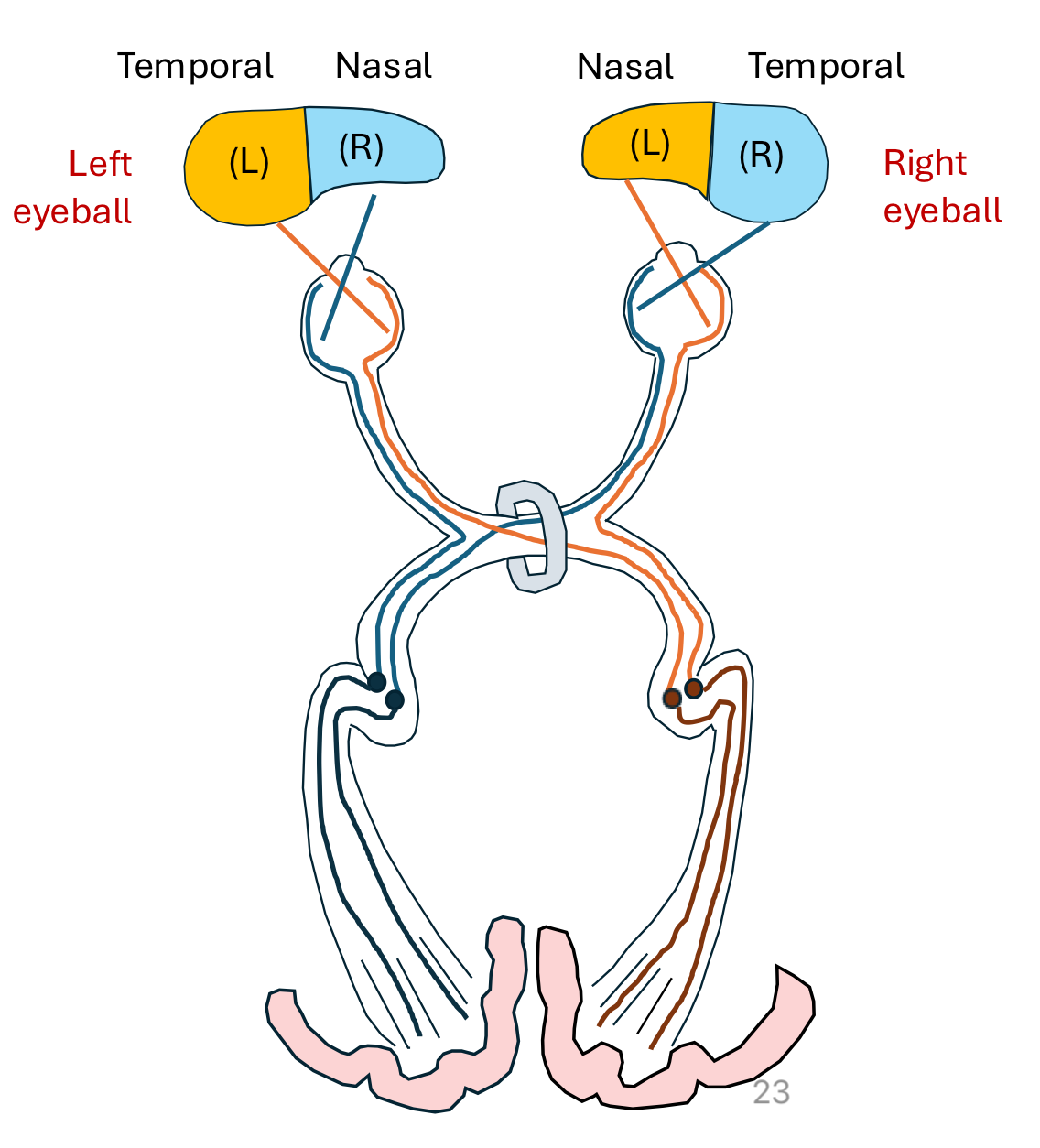
Optic chiasm
Optic n. cross each other
In humans small part stays on ipsilateral side
Visual field covered by both eye = binocular depth perception
Remember…. LEFT goes to right and RIGHT goes to left
Visual field
Info from the RIGHT half of the visual field of both eyes are carried in the left optic tract
Info from the LEFT half of the visual field of both eyes are carried in the right optic tract
Nasal component: closest to nose
Path of light from LEFT nasal field: Light captured by R side of R eyeball → R optic nerve (stays on R side) → R Lateral geniculate body continue down the R optic tract → Occipital lobe
Path of light from RIGHT nasal field: Light captured by L side of L eyeball → L optic nerve (stays on L side) → L lateral geniculate body continue down the L optic tract → Occipital lobe
Temporal component: closest to temple
Path of light from the LEFT temporal field: Light captured by R side of L eyeball → Cross over at optic chiasm (to R side) → R lateral geniculate body continue down the R optic tract → Occipital lobe
Path of light from the RIGHT temporal field: Light captured by L side of R eyeball → Cross over at optic chiasm (to L side) → L lateral geniculate body continue down the L optic tract → Occipital lobe
Clinical considerations
Prechiasmatic lesion: Retina or optic n. damage
If the lesion to the nerve is incomplete, blind spot in that eye’s visual field results
Ex/ damage to R optic n. means no info from R eyeball
Chiasmatic lesion: Optic chiasm
Temporal visual fields loss (tunnel vision)
Info from temporal visual fields cannot cross to opposing optic tract
Postchiasmatic lesion: Optic tract
Loss of input from the contralateral visual field from both eyes
Ex/ damage to R optic tract means that you lose vision from L temporal and nasal visual fields
Ophthalmic Division of Trigeminal (V1)
Branches of V1 (superior → inferior)
Lacrimal n. → Frontal n. → Nasociliary n.
Frontal n → Supraorbital n. and Supratrochlear n.
Nasociliary n. → Infrotrochlear n.
Oculomotor n. (CN III) - SM and Parasymp/Pre
Upper division: Innervates levator palpebrae superioris and superior rectus
Lower division: innervates inferior rectus and inferior oblique
Trochlear n. (CN IV) - SM ONLY
Innervates superior oblique m.
Trochlear swing before turning onto eye
Abducent n. (CN VI) - SM ONLY
Innervates lateral rectus
Sympathetic and Parasympathetic Pathways
Sympathetics
Synapse at superior cervical ganglion (right next to ICA)
Post-synaptic sympathetics carried by the ICA into the head via the carotid plexus
Sympathetics to vessels within the eye
ICA → Nasociliary n. (V1) → Ciliary ganglion → Short ciliary nn.
ICA → Plexus branch → Ciliary ganglion → Short ciliary nn.
Sympathetics from carotid plexus innervate dilator pupillae m.
Dilates pupil to bring in more light
ICA → Nasociliary n. (V1) → Long ciliary n. → Sclera → Dilator pupillary
Bypass the ciliary ganglion
Parasympathetics
Parasymoathetics innervate….
Sphinctor pupillae: Constricts pupil
Ciliary m.: Controls lens thickness for accomodation/focus
Zonular fibers attach lens from ciliary m.
Relaxed ciliary m. = flatten lens (unaccommodated)
Contracting ciliary m. = thickened lens (accommodated)
Clinical Correlations
Pupillary Light Reflex
Afferent limb: CN II from stimulation to retinal ganglion cells
Efferent limb: CN III parasympathetics via short ciliary nn. to sphincter pupillae
Clinically test by shining bright light and observing if the pupil changes size
Constrict in bright light
Dilate in dim light
Accommodation Reflex
Afferent limb: CN II from stimulation of retinal ganglion cells
Efferent limb: CN III parasympathetics via short ciliary nn. to ciliary body (m.) and sphincter pupillae
Clinically test by asking patient to converge eyes (bring object closer)
Observe convergence, pupil constriction, lens gets thicker
Aid in near focus
Horner’s Syndrome
Neurologic disorder that affects the sympathetics
More specifically, the sympathetics to the head
Lesion in sympathetic ganglion/sympathetic chain
Clinical manifestations: Ptosis, miosis, and anhidrosis
Ptosis: drooping eyelid
Result from loss of control of superior tarsal muscle (smooth muscle under autonomic control) therefore can’t assist levator palperae superioris
Miosis: constricting pupil
Result from loss of control of pupillary dilator m.
Anhidrosis: lack of sweating on the face
Result from loss of control of the smooth muscle within the aa. of the forehead (supraorbital and supratrochlear aa.)
Clinical Testing (“H Test”)
Goal: Isolate actions to isolate specific nerves
Ex/ Testing trochlear n.
Innervates: Superior oblique
Actions of SO: Depression, ABduction
Depression is primary action → look medially (ADduction) and downwards
Ex/ Testing oculomotor n.
Innervates: Superior rectus; Inferior rectus; Medial rectus; Inferior oblique
Actions of SR: Elevation, ADduction
Elevation is primary action → look laterally (ABduction) and upwards
Actions of IR: Depression, ADduction
Look laterally and downwards
Actions of MR: ADduction
Look medially (ADduction)
Actions of IO: Elevation, ABduction
Look medially (ADduction) and upwards